
Effects of occupational health promotion interventions on health-related outcomes among employees of small businesses and self-employed individuals: A systematic review
Abstract
BACKGROUND:
Compared to workers of larger companies it is less clear what health promoting interventions might be beneficial for employees of small businesses and self-employed individuals.
OBJECTIVE:
Our aim was to critically appraise trials investigating health promotion programs among small business workers and self-employed individuals, by means of a systematic review.
METHODS:
We conducted a search of primary studies using MEDLINE, Web of Science, LIVIVO and the Cochrane library. Our assessment followed the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions and PRISMA.
RESULTS:
We identified six trials including 5,854 participants from Asia, North America and Australia. Most were of moderate methodological quality, only one was of low quality. Some of the supervised psycho-educational lifestyle programs focusing on individual behavior changes showed benefits in terms of stress reduction and increased physical activity levels among small enterprise employees.
CONCLUSIONS:
There is a huge knowledge gap on evidence-based health promotion interventions for self-employed and for small business workers, especially in Europe.
1Introduction
Absenteeism, presentism (i.e. working while sick, but not 100% productive), and early retirement due to ill health are associated with high economic costs in many countries [1]. Andreyeva et al. estimated for the U.S. that 8.65 billion dollars per year were attributable to absenteeism caused by obesity [2]. Presenteeism also has considerable economic implications. Goetzel et al. evaluated that 25% of the total costs caused by respiratory infections result from presenteeism, whereas the proportion of costs due to presenteeism in migraine/headache is estimated at 89% [3]. In case of fatigue, they are even higher than the direct healthcare costs. For the UK, it was estimated that lost productivity due to presenteeism for mental health reasons alone may cost UK employers between 26–29 billion Pounds per year [4]. Schultz et al. reported in their literature review that health conditions are associated with a loss of productivity in the workplace and presenteeism is a large component of the employer cost of these health conditions [5]. The high economic costs place a strain on businesses as well as governments and individuals, and will probably increase in the future due to aging workforces [1]. Studies in large companies have demonstrated that health promotion programs at the workplace that focused on changes in lifestyle and disease management (e.g. nutrition, or physical activity and overweight, or high blood pressure), can improve employees’ health and result in economic benefits [6–8]. Specific wellness programs at the workplace are designed to improve the health and wellbeing of workers. Employers who integrate workplace wellness may have a greater positive impact on healthy lifestyles and absenteeism, for example, and therefore might reduce healthcare costs [9]. As the recent COVID pandemic showed, enterprises can use their settings and contribute to preventive and health promoting activities. For instance, workplace vaccination campaigns represent a great opportunity to prevent the spreading of infectious diseases and thus complement other useful public health tools. Employers offering free on-site vaccination may be particularly helpful during pandemics to ensure adherence to vaccination campaigns [10].
Self-employed individuals and employees of small and medium-sized enterprises (SME) suffer from mental and physical diseases at least as often as, or even more frequently, than employees of large enterprises [11–14]. Furthermore, there have been indications that unhealthy lifestyle behaviors, including smoking as well as low fruit and vegetable consumption, might be associated with self-employment [15]. However, workplace health promotion programs are less often implemented by self-employed individuals and in SMEs than in large enterprises [16–18], although these companies account for a considerable share of the economy [19, 20]. Self-employed individuals are less likely to use cost-free preventive health services as compared to standard workers [21]. Time constraints and staffing are the most common barriers to implementation of workplace health strategies [22, 23]. These aspects result in psychological pressure by SME owners and lower their engagement in creating wellbeing interventions for their employees. [24]. Additionally, SME owners, who play an important role in implementing workplace health promotion, often do not consider health promotion as a serious issue with regard to their activities. However, some research has found that workplace health promotion was successful regardless of the size of the businesses [25]. For example, low-activity employees of a SME improved their body mass index, stress levels and levels of presentism after taking part in a physical activity intervention program for three months [26]. Furthermore, a large Korean study with over 20,000 participants showed significant improvements regarding hyperlipidemia, obesity, and smoking after a government-supported prevention program for SME employees was implemented [27]. This is consistent with an older work-site health promoting intervention in larger enterprises in the US. The evaluation by Jeffrey et al. showed a reduced smoking prevalence among the employees [28]. By contrast, a previous study reported only little or no changes in absenteeism, presentism, stress and depression [29]. Since no comprehensive overview of the effects of these programs is available, the first systematic review was conducted to provide a summary of trials that evaluated health promotion interventions for SME employees in order to determine their benefits and any harm caused regarding health-related outcomes.
2Methods
For this systematic review, we followed the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions version 6.0 [30] and the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [31]. This study, as a literature review, is exempt from Institutional Review Board approval.
2.1Search strategy
We searched PubMed (i), Web of Science (ii), LIVIVO (iii) and Cochrane library (iv) databases up to November 2021 using the following search strings:
(i) (“Small Business”[Mesh]) OR “self-employed”;
(ii) “self-employ*” (All Fields) or “freelanc*” (All Fields) or “free agent*” (All Fields) or “small business*” (All Fields) or “small enterprise*” (All Fields) or “micro business*” (All Fields) or “small and medium-sized enterprise*” (All Fields) AND TS=“health promotion*” or TS=“occupational health*” or TS=“intervention*” or TS=“promotion of health*” or TS=“health support*” or TS=“excercise*” or TS=“workplace health*” or TS=“health campain*” or TS=“prevention*” or TS=“preventive*” or TS=“health education*” or TS=“health literacy*”;
(iii) “self-employ*” OR “freelanc*” OR “free agent*” OR “small business*” OR “small enterprise*” OR “micro business*” OR “small and medium-sized enterprise*”[Keywords];
(iv) “self-employ*” OR freelanc* OR “free agent*” OR “small business*” OR “small enterprise*” OR “micro business*” OR “small- and medium-sized enterprise*”
To complement the systematic search across the major literature databases for health sciences as described above, we screened all the references from the included studies and searched the internet (e.g. scientific conferences) for additional publications. We did not exclude any study based on language or year of publication.
2.2Inclusion and exclusion criteria
The inclusion criteria were specified using PICO model (Population, Intervention, Comparison, and Outcome). Previous researchers have used several definitions for both self-employment and small enterprises. Therefore, we did not define the size of small businesses, and included all definitions of self-employed individuals (sole proprietors, or entrepreneurs with own personnel) according to the definition used by the authors of identified studies. Thus, studies examining entrepreneurs or employees of small businesses were included (P).
We included only intervention studies with comparison groups, additionally we searched for systematic reviews with or without meta-analysis. Articles were identified as being eligible if any health intervention program was applied to self-employed sole proprietors, entrepreneurs of small businesses, or their employees (I). The included study designs required one or more interventions and at least one unexposed control group (C). The health outcomes included were improvements or deteriorations in physical and mental disorders, general health, as well as risky health behaviors, e.g. physical inactivity (O).
We excluded the following study designs and publication types: before-after intervention studies (i.e. studies without a separate control group); case reports and series; observational studies (cross-sectional, cohort and case-control studies); qualitative studies; narrative reviews; book chapters; editorials; and letters. In terms of the intervention, we excluded studies that only investigated an occupational safety program. Furthermore, we excluded studies that examined employees or self-employed individuals on sick leave, and studies that did not assess patient-relevant health outcomes but rather endpoints, such as return on investment.
2.3Assessment of studies
In compliance with the inclusion and exclusion criteria, the first author (K.W.) screened the titles and abstracts of the identified articles. We did not observe any duplicates of studies. All studies of interest that were not published as open access were available via the German library network ‘subito’.
An external professional translator translated one Korean publication into German to be included in the full-text screening. Two of three authors (P.J., C.T., A.D.) evaluated all the full texts independently, and if their assessments did not match, a third author was contacted (T.K.). Accordingly, a quality assessment was carried out by two of three authors independently (P.J., C.T., A.D.) using the Quality Assessment of Controlled Intervention Studies by the National Heart, Lung, and Blood Institute, U.S.A. (see quality assessment below) [32].
Fig. 1
PRISMA Flow Chart showing the selection process of trials on health promoting and preventive interventions in small businesses and self-employed individuals [31].
![PRISMA Flow Chart showing the selection process of trials on health promoting and preventive interventions in small businesses and self-employed individuals [31].](https://ip.ios.semcs.net:443/media/wor/2024/79-2/wor-79-2-wor230441/wor-79-wor230441-g001.jpg)
The first author (K.W.) performed data extraction for all the studies included, and a second author (P.J.) reviewed all the extracted data. The following parameters from each of the included studies were extracted: first author, publication data, country, study design, sample size, response rate, percentage of female participants, age of the study population, origin and main characteristics of the target group, occupational status, assessment tools, intervention strategy and main results.
2.4Quality assessment
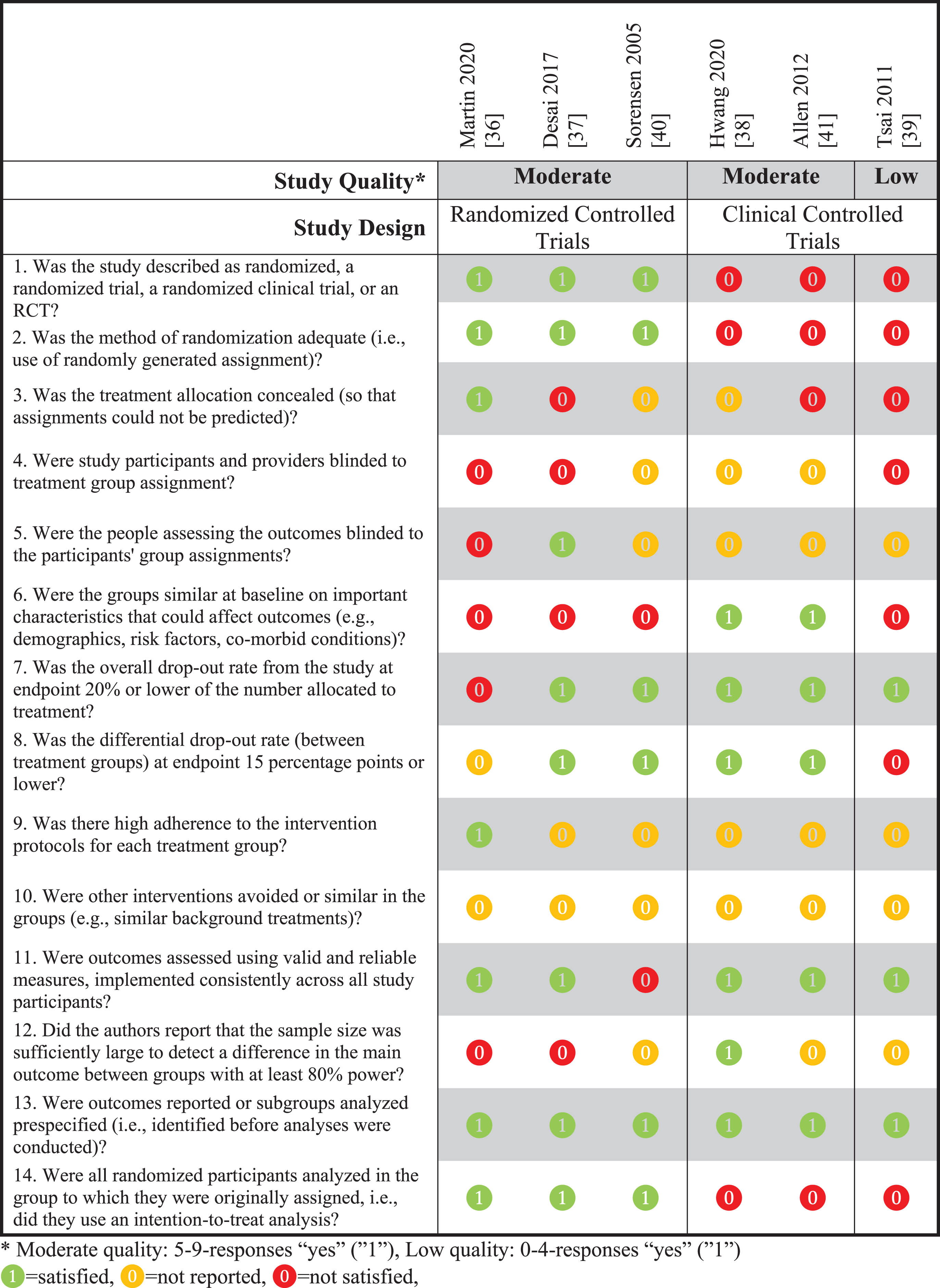
The assessment of methodological quality of the studies was performed using the Quality Assessment of Controlled Intervention Studies by the National Heart, Lung, and Blood Institute, U.S.A. [32], for which a high level of interrater agreement has been demonstrated (kappa = 0.82) [33]. The tool contains 14 items (Supplementary Table S1) that critically appraise the internal validity of the studies by asking questions, e.g. about randomization, blinding, and power. Rather than providing a numerical evaluation, each question is answered with “yes”, “no”, “not reported”, “cannot determine” or “not applicable”. In this way, we classified the quality of the studies as follows: low quality (0–4 responses of ‘yes’); moderate quality (5–9); and high quality (10–14) (Table 1).
Table 1
Quality assessment of the included trials
 |
2.5Synthesis methods
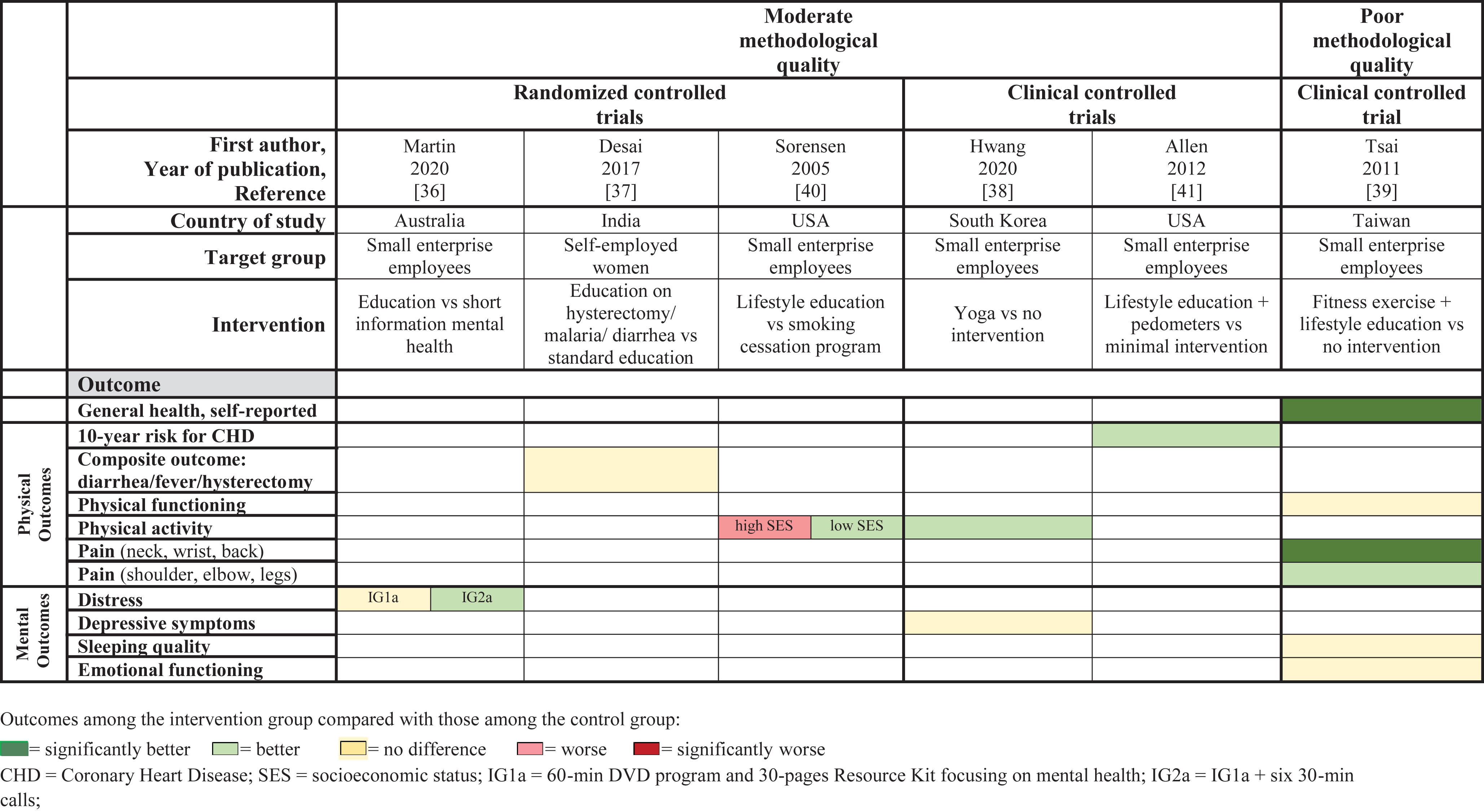
Due to the limited number of included studies with heterogeneous interventions and outcomes, we decided to present the results graphically using a non-standardized table. Table 2 summarizes the extracted data for each study, such as publication year, intervention strategy, outcome measures, and results. In Table 3, the trends in the results from the studies have been presented in color. Within this representation, studies were grouped according to study quality and design, as well as physical and psychological outcomes. The colored representation showed the following outcomes among the intervention group compared with those among the control group: dark green = significantly better; green = better; red = worse; dark red = significantly worse; yellow = no difference.
Table 2
Basic characteristics and results of included trials examining health promotion in small/medium sized enterprises
| Author, publication year, country [reference] | Study design, setting, year(s) | Business size, Source population | Sample, size, age, females (baseline) | Intervention duration and type | Follow-up, Response | Health outcome definition/assessment | Main Health Outcomes |
| Trials with moderate quality | |||||||
| Martin 2020 Australia [36] | RCT whole country before 2020 | 0-200 employees, SME owners/ managers/ sole traders from health, service, retail, building/ construction, or transport/ finance sector (recruitment source not described) | N= 297 18+ y 63% (IG1) 71% (IG2) 57% (CG) | 4 months IG1 : 60-min DVD program (5 psycho-educational and cognitive behavior chapters) and accompanying 30-page resource kit “Promoting Mental Health in SMEs” IG2: same as IG1 + six 30-min telephone calls in 4 months by psychologist CG: only 1st chapter from intervention DVD (15 min, psycho-educational) | Immediately after intervention 49.50% | Psychological distress: Kessler 10 (k10) (10 = lowest, 50 = highest stress level) | IG1 vs IG2 vs CG Psychological Distress Baseline-Post-Intervention Change (Mean; 95% CI); Ratio (95% CI): IG1 (n (baseline) = 104 –> n (4 mo) = 46): – 1.3 (–2.9, 0.4); Ratio 0.9 (–0.5, 2.2) IG2 (n (baseline) = 115 –> n (4 mo) = 46): – 2.5 (–4.1, –0.9); Ratio 1.7 (–0.1, 3.5) CG (n (baseline) = 78 –> n (4 mo) = 55): –1.5 (–2.7, –0.2); Ratio 1.0 (Ref) (intention-to-treat linear regression, log-transformed k10 scores, adjusted for baseline differences regarding sex, age, educational level) |
| Desai 2017 India (Asia) [37] | Cluster-RCT Urban and rural (Ahmedabad district) 2010 | n.r. Self–Employed Women’s Association (SEWA) | N= 1,839 (IG) N= 1,719 (CG) 37.7 y (IG) 37.1 y (CG) 100% | 18 months IG: Group education sessions on hysterectomy/ fever/malaria/ diarrhea and sanitation linkages and programs, tools/handouts, wall paintings, monthly refresher training for community health worker plus CG CG: home visits and group education on common illnesses, accompanied referral to health services, medicine sales and insurance promotion, activate village health and sanitation committees | Immediately after intervention n.r. | Diarrhea, fever and hysterectomy as the leading reasons of hospitalisation claims among SEWA members: Primary outcome: insurance claims rate based on VimoSEWA insurance scheme database Secondary outcomes: Hospitalisation, Morbidity (both for the three conditions) | IG (n (baseline) = 975 –>n (18 mo) = 833) vs CG (n (baseline) = 959 –>n (18 mo) = 783) Insurance claims: Claims rates/100 person-years: 5.5 vs 5.0 Effect estimate (95% -CI): 1.0 (0.8, 1.3), p= 0.81 Hospitalization: Hospitalization rates/100 person-years: 2.7 vs 2.4 Effect estimate (95% -CI): 1.1 (0.6, 1.9), p= 0.88 Morbidity: Morbidity rate/100 person-months: 5.8 vs 5.4 Effect estimate (95% -CI): 1.1 (0.9, 1.4), p= 0.46 (intention to treat analysis, using a poisson regression model) |
| Sorensen 2005 USA (North-America) [40] | RCT (Healthy Directions – Small Business Study) Urban area (Greater Boston, Massachusetts) 1999-2003 | 50-150 employees, Dun and Bradstreet database: manufacturing industries | 26 sites, N= 1,737 44.1 y (IG) 42.8 y (CG) 44.0 % (IG) 24.6 % (CG) | 18 months (1 session/month) IG: complex lifestyle intervention focused on individual behavior change including smoking cessation program CG: only smoking cessation program | Immediately after intervention 77% | Physical activity: hours per week | Physical activity ≥2.5 hours/week: IG vs CG Whole sample Baseline (n= 719 vs 805) 69.6% vs 75.2% Follow-up (n= 571 vs 734) 75.0% vs 74.3%, p= 0.23 Subgroup Analysis Managers: Baseline (n= 101 vs 105) 79.6% vs 78.4% Follow-up (n= 72 vs 84) 77.6% vs 82.1% Workers: Baseline (n= 397 vs 502) 64.6% vs 71.7% Follow-up (n= 353 vs 451) 71.7% vs 69.6% p=0.09 for difference between intervention and control group for both managers and workers (adjusted for poverty status) (Reported results from per protocol analysis, but intention to treat analysis not different according to authors.) |
| Hwang 2020 South Korea (Asia) [38] | Clinical Controlled Trial | <300 employees, Participants with CVD risk factors* from small manufacturing enterprises (recruitment source not described) | 4 sites N= 31 (IG) N= 38 (CG) 48.2 y (IG) 47.7 y (CG) 45.8 % (IG) 47.4 % (CG) | 12 weeks IG: yoga program twice a week for 30 min CG: instructed to maintain their normal life without participating in regular physical activity programs | One month after intervention | 1. Depressive symptoms: Center for Epidemiologic Studies Depression (CES-D) Scale (0 = best, 60 = worst) Physical activity: Health Promoting Lifestyle Profile II (HPLP II) (32 = best, 8 = worst) | IG vs CG 1. Depressive symptoms Mean (SD): Baseline: 19.4 (8.1) vs 21.4 (6.9) Follow-up: 19.8 (3.6) vs 20.2 (6.9) Physical activity Mean (SD): Baseline: 15.1 (6.2) vs 14.0 (4.7) Follow-up: 17.1 (5.9) vs 14.2 (3.8) |
| Allen 2012 USA (North-America) [41] | Clinical Controlled Trial (only partly randomized) | n.r., University of New Hampshire Cooperative Extension | 10 sites N= 29 (IG) N= 31 (CG) 51.7 (10.4) y (IG) 48.5 (10.1) y (CG) 93.1% (IG) 87.1% (CG) | 10 months IG: Lifestyle education program (videoconference) + distribution of pedometers (aim: 10.000 steps/day) CG: minimal intervention | Two months after intervention 94% (CG) 90% (IG) of baseline participants | 10-year CHD-risk: Framingham Risk Score (1.4 equals a 1.4% risk of developing CHD in 10 years) | IG vs CG 10-year risk for CHD Baseline: 1.8 (3.4) vs 1.4 (2.1) Follow-up: 1.9 (2.9) vs 1.8 (2.6) |
| Trial with low quality | |||||||
| Tsai 2011 Taiwan (Asia) [39] | Clinical Controlled Trial | <100 employees, Large local office building that housed multiple SMEs | n.r., N= 85 (IG) N= 48 (CG) 36.5 y (IG) 34.2 y (CG) 82.6% (IG) 41.7% (CG) | IG: exercise program with instructions promoting lifestyle and exercise for individual health (3 x 60 min /week for 3 months) CG: no intervention (not interested to participate in intervention but in study) | One week after intervention 81.2% (IG) 100% (CG) | 1. Self-reported health status: based on Short Form-36 Health Survey (higher score = better health) 2. Sleeping assessment 3. Body pain: Nordic Musculoskeletal Questionnaire (yes = improvement from pain condition) | IG vs CG General health, Mean(SD)* Baseline: 35.5 (22.8) vs 38.0 (20.6) Follow-up: 50.7 (21.8) vs 40.6 (22.2), p= 0.019 Physical functioning, Mean(SD)* Baseline: 89.5 (13.1) vs 91.8 (11.9) Follow-up: 92.2 (9.6) vs 94.0 (8.3), p= 0.883 Emotional functioning, Mean(SD)* Baseline: 76.3 (34.8) vs 66.6 (42.3) Follow-up: 78.7 (32.7) vs 77.7 (38.4), p= 0.239 Sleeping quality, Mean(SD)* Baseline: 63.1 (20.7) vs 55.4 (17.1) Follow-up: 63.4 (16.4) vs 57.0 (17.9), p= 0.551 *adjusted for age, sex, smoking status, and coffee drinking Neck pain (yes, %): 18.8 vs 2.1, p= 0.006 Shoulder pain (yes, %): 20.3 vs 8.3, p= 0.078 Elbow pain (yes, %): 5.8 vs 2.1, p= 0.329 Wrist pain (yes, %): 17.4 vs 4.2, p= 0.030 Upper back pain (yes, %): 8.7 vs 0.0, p= 0.036 Lower back pain (yes, %): 21.7 vs 6.3, p= 0.022 Thigh/Buttock pain (yes, %): 8.7 vs 2.1, p= 0.138 Knee pain (yes, %): 4.3 vs 4.2, p= 0.962 Ankles/Feet pain (yes, %): 7.2 vs 0.0, p= 0.057 |
N= number, CG = control group, IG = intervention group, y = years, vs = versus, SD = standard deviation, SE = standard error, MET = metabolic equivalents, CI = confidence interval, n.s. = not significant, n.r. = not reported; mo = months
Table 3
Patient-relevant outcomes among trials with moderate and poor quality
 |
3Results
3.1Study characteristics
Our search identified 7,789 publications. After eliminating duplicates and following screening of titles and abstracts, 54 full-text articles were obtained and assessed for eligibility. Two trials were excluded because they only examined surrogate outcomes and no patient-relevant outcomes [34, 35]. Six trials met our inclusion criteria: five were of moderate methodological quality, and one was of low quality (Table 1).
The six included trials encompassed 5,854 subjects, ranging from 60 to 3,558 participants per study. With the exception of one study from Australia [36], the included studies were conducted in Asia [37–39] and North America [40, 41]. Five studies were carried out in small business settings (with less than 300 employees) [36, 38–41] and one investigated self-employed women only [37]. All included studies were published between 2005 and 2020 (Table 2).
Most of the trials did not describe the recruitment strategy in detail. Four studies included a higher proportion of women in the intervention group than in the control group [36, 39–41]. All participants had a mean age of 34 to 52 years. The occupational groups included varied from study to study (Table 2). Family status or ethnicity was not reported in most of the included studies.
3.2Assessment of employment categories
The trials used different definitions of a small business, which ranged from less than 100 to less than 300 employees. Only one study examined self-employed individuals [37]. Most of the trials combined workers of different sectors, e.g. health service, transportation, manufacturing, or office workers, and only analyzed them together, not separately [36, 39]. Two studies did not report any information on a specific industrial sector [37, 39] (Table 2).
3.3Intervention strategies
Various strategies for complex lifestyle interventions were examined in the included studies. Two trials developed weekly exercise sessions, which included educational measures, such as lifestyle education, implemented to a varying degree [38, 39]. Four trials examined educational interventions, such as lectures or video materials related to mental health, education on hysterectomy, malaria, and diarrhea, or lifestyle education [36, 37, 40, 41]. Educational elements were supplemented by telephone calls or using pedometers in two programs [36, 41]. The duration of the interventions ranged from twelve weeks [38] to 18 months [37] (Table 2).
3.4Quality assessment
None of the six trials were of good methodological quality, with five being of moderate quality [36–38, 40, 41], and one of poor quality [39]. Most frequently they lacked information as to whether participants participated in additional interventions or whether they received background treatments (in all studies), and whether participants adhered to the intervention protocol (in all but one study) [36]. Additionally, information on the blinding of study participants and providers to the assignment of treatment groups was lacking in all studies, and a description of blinding of persons who assessed the outcomes was lacking in all but one study [37]. Only three out of the six studies randomized their participants to an intervention or control group respectively [36, 37, 40] (Table 1).
3.5Outcome measures
In order to focus on the patient/participant perspective, only patient-relevant outcomes have been presented. Some trials also [36, 38, 40, 41] or exclusively [34, 35] examined surrogate parameters (e.g. biomarkers) as outcomes to explain potential mechanisms. These are listed in the supplement (Tables S2 and S3). We identified only one outcome (physical activity) examined by more than one trial (Tables 2 and 3).
3.5.1Randomized controlled trials
A randomized trial in Australia examining workers from a small enterprise with less than 200 employees found considerably reduced stress levels in one intervention group also receiving 30-minute-phone calls for four months in comparison to the other intervention group (without phone calls) or the control group receiving minimal intervention [36].
A randomized trial from India (RCT) recruiting only female subjects from the Self-Employed Women's Association (SEWA) investigated the effect of monthly education sessions on the main reasons for local hospital admissions (hysterectomy, fever, malaria and diarrhea) over 18 months. The authors did not identify any effect of their education program for self-employed women in terms of hospitalization for hysterectomy, fever, malaria and diarrhea [37].
Participants in the intervention group of a randomized controlled trial in Massachusetts (USA) received monthly educational sessions on behavioral change over a period of 18 months. Sorensen et al. found increased levels of physical activity in their intervention group among workers of low socioeconomic status, but not among those of higher socioeconomic status [40].
All randomized controlled trials included in this systematic review were of moderate methodological quality.
3.5.2Non-randomized controlled trials
The following two non-randomized trials were of moderate methodological quality. Hwang et al. applied a 12-week yoga program in a non-randomized trial including manufacturing workers from a small enterprise (less than 300 employees) in South Korea. For depressive symptoms as their main outcome the authors found no clinically relevant difference between the intervention and control groups (receiving no intervention) 16 weeks after the study started. However, there was a trend toward increased levels of physical activity in the intervention group compared to the control group [38].
Another non-randomized trial examined the effects of a lifestyle education program using pedometers on the 10-year risk of coronary heart disease among workers from an enterprise with 172 employees in New Hampshire (USA). The authors found a reduced risk of coronary heart disease in the intervention group in comparison with the control group after the 10-month education program [41] (Tables 2 and 3).
The only trial included of poor quality was from Taiwan (Asia). Participants of this study performed an exercise program including lifestyle and exercise promotion three times weekly for one hour. After three months of intervention participants of the intervention group had a significant reduction in neck, wrist and back pain, a non-significant reduction in shoulder and elbow pain, as well as a significantly improved perception of their general health. No differences were found regarding physical and emotional functioning and quality of sleep [39] (Tables 2 and 3).
3.5.3Adverse events
Adverse events were not specifically reported in the publications for the six trials. However, one of the large trials showed a decreased average physical activity level in the intervention group compared to the control group among the subgroup of workers of a higher socioeconomic status following monthly educational sessions on behavior change over a period of 18 months [40].
4Discussion
4.1Main findings
Our comprehensive systematic literature review identified only three randomized and two non-randomized trials of moderate methodological quality, and one non-randomized trial of poor quality. All were conducted in Asia or North America, except one (in Australia). Most of the trials examined the effects of workplace health promotion in small businesses with less than 300 employees.
Trials of moderate quality showed a slight decrease in distress, which was defined as a feeling of extreme worry, sadness, or pain [42], if the intervention group was actively supervised over the entire intervention period. No effects on distress were found for a one-time educational intervention. The results from two trials that examined physical activity were inconsistent. After monthly complex lifestyle interventions over a period of 18 months, workers of a high socioeconomic status showed decreased levels of physical activity, whereas workers of low socioeconomic status showed increased levels.
4.2Comparison of studies
Therapeutic trials, which we purposely excluded from our systematic review on preventive interventions, have shown that supervised interventions seem more effective than when unsupervised. Actively guided cognitive behavioral therapy among employees of six SMEs in Denmark, defined as subclinical cases of mental diseases, was successful in reducing stress levels compared to controls without any intervention of this type [43]. A further study was excluded from our systematic review because it included workers suffering from acute illnesses. It found significantly decreased stress levels in the intervention group (one-week multimodal prevention program for stress reduction) in the short-term, and slightly decreased stress levels for this group over long-term follow-up, although the intervention did not include any further regular elements [44]. Our review showed similar preventive effects in generally healthy workers at small businesses in Australia. Martin et al. reported that a complex lifestyle intervention for small business owners and employees in Australia was more effective when the participants were actively guided. The intervention group, which applied supervision by psychologists by means of six phone calls over 4 months, performed considerably better than the other groups with no active guidance [36]. This is in line with another trial from our review conducted in South Korea. The authors reported reduced job stress for the intervention group who received twice-weekly yoga sessions, compared to a group that only received advice as a minimal intervention. However, this study by Hwang et al. was not randomized and thus may have been prone to bias [38]. A study that we excluded due to lack of a control group did not find improvements in stress levels following four telephone-coaching sessions. This study only compared the results with another intervention group who did not receive telephone calls, but it did not evaluate a control group with no interventions. In this trial, all participating entrepreneurs from green professions (e.g. farmers, foresters, gardeners etc.) completed a 12-day stress-prevention program. One group subsequently received four telephone-coaching sessions, including psychoeducation, which the other group did not receive. All of the participants saw an improvement in their stress levels to a similar extent after a follow-up period of nine months [45]. The decreased stress levels could be the result of the interventions which included active participation, such as exercise sessions, or mindful-based stress reduction [38, 39, 44–46]. In contrast, Martin et al. provided only educational material in the form of a DVD program and a written document [36]. In this case, which did not apply active sessions, there may be the need for further active therapeutic support to achieve a decrease in distress, given that a key issue for improving behavioral change in self-care is motivation by means of human contact and empathy [47]. Furthermore, it may be the case that it is easier for workers to relax if they had fixed intervention dates instead of organizing relaxation time themselves [48]. Behavior-oriented prevention will reach a limit if there is no change in the social framework conditions (structural prevention). Whereas behavioral prevention targets a change in the individual’s behavior, structural prevention deals with working and living conditions [49]. Even if cognitive information is accepted and retrievable, analogous behavioral adaption does not necessarily follow without environmental changes [50]. Findings from studies included in our review suggested that, for example, regular group exercises or contact with peers at the workplace might represent a necessary change in the working conditions.
Another example of poor implementation of newly acquired knowledge can be seen in the study included from India. The authors reported no effects as a result of monthly education sessions on the most common reasons for hospital admissions – hysterectomy, fever, malaria and diarrhea [37]. However, the authors found some improvements in health knowledge after the interventions [37], which was in line with findings by Kroeger et al, who reported improvements in health knowledge on malaria control of 33–61% through health education among people living in rural communities of the Pacific coast of Ecuador [51]. Although behavioral change is associated with improved knowledge [37], behavioral change does not always seem to follow an increase in knowledge [50]. In the study by Desai et al, one reason for not applying acquired knowledge could have been that the malaria prevention intervention only involved group education and providing handouts [37]. Previous research on this topic applied to mothers and children suggested “regular supervisory visits, frequent auditing of resources, steady supplies, community promotion policies [\dots] and strict and enforced regulations” to achieve improvements in malaria prevention [52]. Consequently, the interventions in the study by Desai et al. may have been too weak to achieve behavioral changes.
Regarding physical activity, Hwang et al. reported an increase following a 16-week yoga program in their non-randomized trial [38]; whereas Sorensen et al. (RCT) showed that the results of a lifestyle education program depended on the socioeconomic status of the small business workers [40]. The two studies might show different results and inconsistent outcomes due to sampling bias and a lack of randomization in the study by Hwang et al, because the authors of this study examined a very small sample size of only 69 participants [38]. On the contrary, the study by Sorensen et al. (the more convincing of the two studies, with a sample size of 1,737) reported increased physical activity following intervention among workers of low socioeconomic status, whereas decreased physical activity was reported among workers of high socioeconomic status [40]. This is in line with Hwang et al, who investigated participants with cardiovascular risk factors from small manufacturing enterprises and reported an increase in physical activity following intervention among this sample of low socioeconomic status [38]. This would seem to contrast with findings from previous research showing generally higher levels of physical activity among people of high socioeconomic status than among those of low socioeconomic status [53]. A reason for the positive effects among workers of low socioeconomic status in the trial by Sorensen et al. could be their low activity levels prior to the intervention [40]. This was also shown in a study by Edmunds et al. who reported increased physical activity following intervention among low-activity employees [26]. In contrast, overworking due to the implementation of workplace health interventions could have decreased the time available for physical activity among managers. A large Korean study including over 20,000 participants examined a state financed and organized prevention program and reported significant improvements regarding cardiovascular risk factors including physical activity. These positive effects were achieved by means of just four visits to each company per year. For the current review, we had to exclude this trial due to a lack of control group [27].
A controlled clinical trial of moderate quality examined a 12-week yoga intervention among small enterprise employees from South Korea. It reported no change in depressive symptoms among the participants [38]. However, results from further literature reviews that were not included in our systematic review because they did not investigate either participants from small enterprises or the self-employed, suggest positive effects of yoga on depressive symptoms [54, 55]. These reviews reported a moderate reduction in depressive symptoms as a result of yoga intervention programs lasting up to one year [54, 55]. A possible reason for the lack of an effect in the trial included by Hwang et al. might be their short intervention period, and, additionally, the different stages of depression [38]. Two studies that investigated worksite wellness confirmed that depressive symptoms only subside after a longer period of intervention. However, they were not included in our review due to a lack of control group [26, 29].
The final trial included was of moderate methodological quality, and showed a decreased 10-year risk of coronary heart disease after 10 monthly lifestyle education videoconference sessions in addition to the use of pedometers over the same time period [41]. These results are consistent with the results of a study by Salinardi et al. who investigated cardio-metabolic risk factors in office workers from the U.S. [56]. The authors of this study evaluated the effects of a lifestyle intervention on weight loss and prevention of regaining weight [56]. Additionally, a systematic review on the effectiveness of lifestyle health promotion-interventions for nurses suggested that interventions targeting behavioral changes are more effective than interventions that focused solely on education [57]. Consequently, in the trial by Allen et al, the combination of the educational videoconferences and the use of the pedometers seem to be an effective approach to successfully establishing new behaviors. This theory is also supported by a systematic review that examined the effectiveness of using pedometers. Its authors reported an association between the use of a pedometer and significant increases in physical activity as well as decreases in body mass index and blood pressure [58]. Nevertheless, it should be noted that the subjects in the trial by Allen et al. volunteered for the intervention and therefore subjects who were relatively highly motivated for lifestyle changes may have been examined.
The only trial included of poor methodological quality showed significant improvements of self-reported general health and various pain conditions among Taiwanese SME workers. They had received three months of fitness exercises and lifestyle education in comparison with control subjects who did not receive any intervention [39]. The results were consistent with a cluster-randomized controlled study in nursery schoolteachers from Italy. The authors reported significant improvements in pain after an extension-oriented exercise program [59]. However, the trial from Taiwan did not find any changes with respect to physical function, sleep quality and emotional function [39]. The latter was in contrast to a previous Taiwanese study that showed positive effects of exercise programs on mental health among middle-aged women with cardiovascular disease risk factors from the general population [60]. A possible explanation for the results by Tsai et al. could be the fact that the participants in both the intervention and control groups were all involved in a course promoting the importance of lifestyle and exercise before the initial trial [39]. As such, both groups received a relevant health promoting intervention prior to the actual trial, which could have had an impact on the study participants’ behavior and thus influenced the results. Additionally, the intervention period may have been too short to substantially influence sleep quality, as well as emotional and physical functioning.
New trends and changes in working conditions due to the aftermath of the pandemic or pandemic-related changes should be considered in the planning of future observational and intervention studies [61]. In addition, the business size could be an advantage of small businesses achieving higher participation rates and more health improvements of their employees than larger businesses [29].
4.3Strengths and limitations
The current study has several strengths. It represents the first systematic review applying standardized criteria to examine the effects of health promoting and preventive occupational interventions on health-related outcomes of workers in small businesses or self-employed individuals. To ensure a comprehensive overview, we did not exclude any language, country or year of publication in our search. We only included intervention studies with comparison groups and study designs of higher quality with the aim of obtaining meaningful results. Additionally, we performed a stringent methodological quality assessment of the included studies using a validated assessment tool, which showed a high interrater agreement in a previous study [33].
Nevertheless, our study also had some limitations. First, although we searched four major medical and health science databases supplemented by a manual search, we may have missed some publications. Furthermore, we were not able to obtain the full texts for four studies which we identified from the title-abstract-screening as being potentially eligible.
Second, the six included trials examined different interventions (e.g. physical activity, or lifestyle education programs) aiming to improve various outcomes. Therefore, comparability between the different studies is limited. Since there was excessive heterogeneity with regard to the interventions, outcomes as well as the assessment tools used in the trials included in our systematic review, we did not conduct a meta-analysis.
Third, the trials investigated heterogeneous populations. Most of the studies assessed several sectors and occupations together, although previous research demonstrated different needs across diverse professions (e.g. blue- and white-collar workers) [11]. Sorensen et al. 2005 reported contradictory outcomes among managers and employees who joined the same intervention [40], but none of the other studies included investigated these groups separately. Additionally, the studies reported different definitions of small businesses and therefore investigated businesses sizes varying from one to 300 employees.
Fourth, because of the different countries of origin and corresponding work cultures, the comparability of the trials was further hampered. For example, the decision latitude of workers in Asia is considerably lower and working hours are longer than in other parts of the world [62]. Previous research has demonstrated a strong association between decision latitude and the wellbeing of workers [63].
Fifth, we did not identify any trial of a quality level higher than moderate. Most of the studies included did not assess workers’ adherence to the interventions offered, although improvements in health outcomes strongly depend on frequency of participation [39]. Further research on the effects of occupational health promotion should include evaluations on workers’ compliance and adherence in order to avoid compliance bias [64]. Additionally, the attrition rate varied from 0 [37] up to 51% [36] among the subjects of the trials included. Therefore, comparability of the studies may also have been limited due to attrition bias [65]. Furthermore, none of the studies included used a fully blinded design.
Sixth, we were not able to consider the possible changes in working conditions related to the Covid-19 pandemic and specific interventions for the self-employed or small enterprises in this systematic review, since no intervention studies that met our inclusion criteria were published by the time when we conducted the literature search.
5Conclusions
Compared to workers in larger companies it is less clear what health promoting interventions are beneficial for employees in small businesses and the self-employed. Although employees in small businesses and the self-employed are a considerable part of the global workforce, there is a lack of good quality prevention research focusing on them.
Despite an extensive literature search, we identified only three randomized and three non-randomized trials on occupational health promotion and prevention for workers of SMEs or the self-employed. Five were of moderate methodological quality, and one of the non-randomized trials was of only low quality. We found some indications that supervised health promoting programs with educational lifestyle interventions or yoga may have the potential to decrease stress levels and increase physical activity levels among workers of SMEs.
However, to fill the huge knowledge gaps with respect to the health of this large occupational group, good/high quality randomized controlled trials are urgently needed to examine the sustainable effects of mental and physical health promotion programs at work. Moreover, it is conceivable that intervention effects may vary by age, sex and occupation. Additionally, the effects of interventions at the workplace may differ from the effects of interventions conducted outside of work, e.g. within the environment of a complex health promotion program at a specialized location.
This systematic review can provide the basis for new health promotion strategies in small business settings to prevent work-related chronic mental and physical disorders.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Acknowledgments
The authors thank Caroline Bauer (Bad Kissingen, Germany) for supporting the literature search.
Conflicts of interest
The authors declare that they have no conflict of interest.
Funding
The authors report no funding.
Supplementary materials
The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/WOR-230441.
References
[1] | Rasmussen B , Sweeny K , Sheehan P . Economic costs of absenteeism, presenteeism and early retirement due to ill health: A focus on Indonesia. Report of the US Chamber of Commerce. (2016) . |
[2] | Andreyeva T , Luedicke J , Wang YC . State-level estimates of obesity-attributable costs of absenteeism. Journal of Occupational and Environmental Medicine. (2014) ;56: (11):1120–7. PubMed PMID: 25376405; PubMed Central PMCID: PMC4225558. |
[3] | Goetzel RZ , Long SR , Ozminkowski RJ , et al. Health, absence, disability, and presenteeism cost estimates of certain physical and mental health conditions affecting US employers. J Occup Environ Med. (2004) (46):398–412. |
[4] | Hampson E . Mental health and employers: Refreshing the case for investment. [Internet] 2020 [cited 2024 Mar 11]. Available from: https://www2.deloitte.com/uk/en/pages/consulting/articles/mental-health-and-employers-r5/31/2024efreshing-the-case-for-investment.html |
[5] | Schultz AB , Chen C-Y , Edington DW . The cost and impact of health conditions on presenteeism to employers: A review of the literature. Pharmacoeconomics. (2009) ;27: (5):365–78. PubMed PMID: 19586075. |
[6] | Goetzel RZ , Liss-Levinson RC , Goodman N , Kennedy JX . Development of a community-wide cardiovascular risk reduction assessment tool for small rural employers in upstate New York. Preventing Chronic Disease. (2009) . 6(2). |
[7] | Jacobs JC , Yaquian E , Burke SM , Rouse M , Zaric G . The economic impact of workplace wellness programmes in Canada. Occupational Medicine (Oxford, England). (2017) ;67: (6):429–34. PubMed PMID: 28898961. |
[8] | Astrella JA . Return on investment: Evaluating the evidence regarding financial outcomes of workplace wellness programs. J Nurs Adm. (2017) ;47: (7-8):379–83. PubMed PMID 28727623. |
[9] | Meyers AR , Al-Tarawneh IS , Bushnell PT , Wurzelbacher SJ , Lampl MP , Tseng C-Y , et al. Degree of integration between occupational safety and health programs and wellness programs: First-year results from an insurer-sponsored wellness grant for smaller employers. Journal of Occupational and Environmental Medicine. (2019) ;61: (9):704–17. PubMed PMID: 31205207. |
[10] | Gualano MR , Santoro PE , Borrelli I , Rossi MF , Amantea C , Tumminello A , et al. Employee participation in workplace vaccination campaigns: A systematic review and meta-analysis. Vaccines (Basel). (2022) ;10: (211). PubMed PMID: 36366407; PubMed Central PMCID: PMC9698273. |
[11] | Willeke K , Janson P , Zink K , Stupp C , Kittel-Schneider S , Berghöfer A , et al. Occurrence of mental illness and mental health risks among the self-employed: A systematic review. International Journal of Environmental Research and Public Health. (2021) ;18: (16). PubMed PMID: 34444369; PubMed Central PMCID: PMC8393630. |
[12] | Ipsen C , Gish L , Poulsen S . Organizational-level interventions in small and medium-sized enterprises: Enabling and inhibiting factors in the PoWRS program. Safety Science. (2015) ;71: (2):264–274. |
[13] | Freeman MA , Staudenmaier PJ , Zisser MR , Andresen LA . The prevalence and co-occurrence of psychiatric conditions among entrepreneurs and their families. Small Bus Econ. (2019) ;53: (2):323–42. |
[14] | Willeke K , Janson P , Zink K , Tischer C , Heuschmann PU , Zapf A , Wildner M , Stupp C , Keil T . Comparing the occurrence of chronic physical disorders in self-employed individuals with that of employees: A systematic review. Work. (2023) ;75: (4):1179–1198. 10.3233/WOR-220145. PMID: 36710710; PMCID: PMC10473076. |
[15] | Al-Hanawi MK , Keetile M . Socio-economic and demographic correlates of non-communicable disease risk factors among adults in Saudi Arabia. Front Med (Lausanne). (2021) ;8. PubMed PMID: 33889582; PubMed Central PMCID: PMC8055828. |
[16] | Tenney L , Fan W , Dally M , Scott J , Haan M , Rivera K , et al. Health Linkstrademark Assessment of Total Worker Health® Practices as Indicators of Organizational Behavior in Small Business. Journal of Occupational and Environmental Medicine. (2019) ;61: (8):623–34. PubMed PMID: 31045750; PubMed Central PMCID: PMC6748381. |
[17] | Zelfel RC , Alles T , Weber A . Gesundheitsmanagement in kleinen und mittleren Unternehmen – Ergebnisse einer repräsentativen Unternehmensbefragung. Gesundheitswesen. (2011) ;73: (8-9):515–9. PubMed PMID: 21387215. |
[18] | Gunnarsson K , Andersson I-M , Josephson M . Swedish entrepreneurs’ use of occupational health services. AAOHN J. (2011) ;59: (10):437–45. PubMed PMID: 21973286. |
[19] | International Labour Organization, ILOSTAT database. Self-employed, total (% of total employment) (modeled ILO estimate) [Internet]; 2021 [cited 2022 Nov 9]. Available from: https://data.worldbank.org/indicator/SL.EMP.SELF.ZS |
[20] | The World Bank. Small and Medium Enterprises (SMEs) Finance [Internet] [cited 2022 Nov 9]. Available from: https://www.worldbank.org/en/topic/smefinance |
[21] | Kim S , Song JH , Oh YM , Park SM . Disparities in the utilisation of preventive health services by the employment status: An analysis of 2007–2012 South Korean national survey. PLoS One. (2018) ;13: (12):e0207737. PubMed PMID: 30586360; PubMed Central PMCID: PMC6306253. |
[22] | Nelson CC , Allen JD , McLellan D , Pronk N , Davis KL . Integrating health promotion and occupational safety and health in manufacturing worksites: Perspectives of leaders in small-to-medium sized businesses. Work (Reading, Mass.). (2015) ;52: (1):169–76. PubMed PMID: 26410231. |
[23] | Sedani A , Stover D , Coyle B , Wani RJ . Assessing workplace health and safety strategies, trends, and barriers through a statewide worksite survey. International Journal of Environmental Research and Public Health. (2019) ;16: (14). PubMed PMID: 31336749; PubMed Central PMCID: PMC6678341 |
[24] | Dawkins S , Martin A , Kilpatrick M , Scott J . Reasons for engagement: SME owner-manager motivations for engaging in a workplace mental health and wellbeing intervention. Journal of Occupational and Environmental Medicine. (2018) ;60: (10):917–27. PubMed PMID: 29851735. |
[25] | Taylor AW , Pilkington R , Montgomerie A , Feist H . The role of business size in assessing the uptake of health promoting workplace initiatives in Australia. BMC Public Health. (2016) ;16: :353. PubMed PMID: 27097738; PubMed Central PMCID: PMC4839116 |
[26] | Edmunds S , Stephenson D , Clow A . The effects of a physical activity intervention on employees in small and medium enterprises: A mixed methods study. Work (Reading, Mass.). (2013) ;46: (1):39–49. PubMed PMID: 23241703 |
[27] | Kim S-L , Jung H-S , Lee J-E , Yi Y , Kim Y , Lee S-S , et al. Cardiovascular disease management among workers in small-sized enterprise using community-based approach. (2010) ;19: (1):70–7. |
[28] | Jeffery RW , Forster JL , French SA , Kelder SH , Lando HA , McGovern PG , et al. The Healthy Worker Project: A work-site intervention for weight control and smoking cessation. American Journal of Public Health. (1993) ;83: (3):395–401. PubMed PMID: 8438979; PubMed Central PMCID: PMC1694637. |
[29] | Schwatka NV , Smith D , Weitzenkamp D , Atherly A , Dally MJ , Brockbank CVS , et al. The impact of worksite wellness programs by size of business: A 3-year longitudinal study of participation, health benefits, absenteeism, and presenteeism. Annals of Work Exposures and Health. (2018) ;62: (suppl_1):S42–S54. PubMed PMID: 30212884. |
[30] | Higgins J , Thomas J , Chandler J , Cumpston M , Li T , Page MJ , et al. Cochrane handbook for systematic reviews of interventions: Version 6.2 (updated February 2021); Available from: www.training.cochrane.org/handbook. |
[31] | Page MJ , McKenzie JE , Bossuyt PM , Boutron I , Hoffmann TC , Mulrow CD , et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. (2021) ;18: (3):e1003583. PubMed PMID: 33780438; PubMed Central PMCID: PMC8007028. |
[32] | National Heart, Lung and Blood Institute . Study Quality Assessment Tools [Internet] [cited 2021 Dec 29]. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools |
[33] | Lai S-T , Lim K-S , Low W-Y , Tang V . Positive psychological interventions for neurological disorders: A systematic review. Clin Neuropsychol. (2019) ;33: (3):490–518. PubMed PMID: 29938575. |
[34] | Reynolds GS , Bennet JB . A cluster randomized trial of alcohol prevention in small businesses: A cascade model of help seeking and risk reduction. American Journal of Health Promotion. (2015) ;29: (3):182–91. |
[35] | Patterson CR , Bennett JB , Wiitala WL . Healthy and Unhealthy Stress Unwinding: Promoting Health in Small Businesses. J Bus Psychol. (2005) ;20: (2):221–47. |
[36] | Martin A , Kilpatrick M , Scott J , Cocker F , Dawkins S , Brough P , et al.. Protecting the mental health of small-to-medium enterprise owners: A randomized control trial evaluating a self-administered versus telephone supported intervention. Journal of Occupational and Environmental Medicine. (2020) ;62: (7):503–10. PubMed PMID: 32730026. |
[37] | Desai S , Mahal A , Sinha T , Schellenberg J , Cousens S . The effect of community health worker-led education on women’s health and treatment-seeking: A cluster randomised trial and nested process evaluation in Gujarat, India. Journal of Global Health. (2017) ;7: (2):20404. PubMed PMID: 28959438 |
[38] | Hwang WJ , Kim JA , Ha JS . Effects of a Yoga program in reducing cardiovascular disease risk factors in workers of small workplaces: A pilot test. Sustainability. (2020) ;12: (23):10038. |
[39] | Tsai HH , Peng SM , Yeh CY , Chen CJ , Chen RY . An effective physical fitness programm for small and medium-sized enterprises. Industrial Health. (2011) (49):311–20. |
[40] | Sorensen G , Barbeau EM , Stoddard AM , Hunt MK , Kaphingst K , Wallace L . Promoting behavior change among working-class, multiethnic workers: Results of the healthy directions-small business study. American Journal of Public Health [Internet]. (2005) ;95: (8):1389–95. Available from: http://arxiv.org/pdf/2004.03874v1 |
[41] | Allen JC , Lewis JB , Tagliaferro AR . Cost-effectiveness of health risk reduction after lifestyle education in the small workplace. Preventing Chronic Disease. (2012) ;9: , 1–8. PubMed PMID: 22575081; PubMed Central PMCID: PMC3431951. |
[42] | Cambridge Dictionary [Internet] [cited 2024 Mar 7]. Available from: https://dictionary.cambridge.org/de/worterbuch/englisch/distress |
[43] | Sørensen HØ , Valentin JB , Bording MK , Larsen JI , Larsen A , Omland Ø . An outreach collaborative model for early identification and treatment of mental disorder in Danish workplaces. BMC Psychiatry. (2019) ;19: (1). PubMed PMID: 30678679; PubMed Central PMCID: PMC6345055. |
[44] | Kus S , Immich G , Oberhauser C , Frisch D , Schuh A . Evaluierung der Wirksamkeit eines einwöchigen multimodalen Präventionsprogramms zur Entschleunigung und Stressreduzierung, durchgeführt in einem deutschen Kurort: Ergebnisse einer randomisiert kontrollierten Studie. Complement Med Res. (2021) :1–11. PubMed PMID: 33951633. |
[45] | Stier-Jarmer M , Oberhauser C , Frisch D , Berberich G , Loew T , Schels-Klemens C , et al. A multimodal stress-prevention program supplemented by telephone-coaching sessions to reduce perceived stress among German farmers: Results from a randomized controlled trial. International Journal of Environmental Research and Public Health. (2020) ;17: (24). PubMed PMID: 33321849; PubMed Central PMCID: PMC7763316. |
[46] | Ryu H , Jung J , Moon J . Health promotion program for office workers with SEM based on the WHO’s healthy workplace framework. Health Promotion International. (2020) ;35: (6):1369–82. PubMed PMID: 32068840. |
[47] | Riegel B , Dunbar SB , Fitzsimons D , Freedland KE , Lee CS , Middleton S , et al.. Self-care research: Where are we now? Where are we going? Int J Nurs Stud. (2021) ;116: :103402. PubMed PMID: 31630807; PubMed Central PMCID: PMC7035984. |
[48] | Miller AL , Gearhardt AN , Fredericks EM , Katz B , Shapiro LF , Holden K , et al. Targeting self-regulation to promote health behaviors in children. Behav Res Ther. (2018) ;101: , 71–81. PubMed PMID: 29050636; PubMed Central PMCID: PMC5801044. |
[49] | Kempf HD . Die neue Rückenschule: Verhältnispreävention und Verhaltensprävention: Springer, Berlin, Heidelberg; (2010) . |
[50] | Hartung A , Schorb B , Niesyto H , Moser H , Grell P . Jahrbuch Medienpädagogik 10: Methodologie und Methoden medienpädagogischer Forschung: Springer VS, Wiesbaden; (2014) . |
[51] | Kroeger A , Meyer R , Mancheno M , Gonzalez M . Health education for community-based malaria control: An intervention study in Ecuador, Colombia and Nicaragua. Tropical Medicine and International Health. (1996) ;1: (6):836–46. |
[52] | Gilmore B , McAuliffe E . Effectiveness of community health workers delivering preventive interventions for maternal and child health in low- and middle-income countries: A systematic review. BMC Public Health. (2013) ;13: , 847. |
[53] | Varo JJ , Martínez-González MA , Irala-Estévez J , Kearney J , Gibney M , Martínez JA . Distribution and determinants of sedentary lifestyles in the European Union. Int J Epidemiol. (2003) ;32: , 138–46. PubMed PMID: 12690003. |
[54] | Weber M , Schnorr T , Morat M , Morat T , Donath L . Effects of mind-body interventions involving meditative movements on quality of life, depressive symptoms, fear of falling and sleep quality in older adults: A systematic review with meta-analysis. International Journal of Environmental Research and Public Health. (2020) ;17: (18). PubMed PMID: 32916879; PubMed Central PMCID: PMC7559727. |
[55] | Meister K , Becker S . Yoga bei psychischen Störungen. Nervenarzt. (2018) ;89: (9):994–8. PubMed PMID: 29858642. |
[56] | Salinardi TC , Batra P , Roberts SB , Urban LE , Robinson LM , Pittas AG , et al. Lifestyle intervention reduces body weight and improves cardiometabolic risk factors in worksites. Am J Clin Nutr. (2013) ;97: (4):667–76. PubMed PMID: 23426035; PubMed Central PMCID: PMC3607649. |
[57] | Stanulewicz N , Knox E , Narayanasamy M , Shivji N , Khunti K , Blake H . Effectiveness of lifestyle health promotion interventions for nurses: A systematic review. International Journal of Environmental Research and Public Health. (2019) ;17: (1). PubMed PMID: 31861367; PubMed Central PMCID: PMC6981404. |
[58] | Bravata DM , Smith-Spangler C , Sundaram V . Using pedometers to increase physical activity and improve health: A systematic review. JAMA. (2007) ;298: (19):2296–304. |
[59] | Pillastrini P , Mugnai R , Bertozzi L , Costi S , Curti S , Mattioli S , Violante FS . Effectiveness of an at-work exercise program in the prevention and management of neck and low back complaints in nursery school teachers. Ind Health. (2009) ;47: (4):349–54. PubMed PMID: 19672007. |
[60] | Wu T-Y , Yeh H-I , Chan P , Chiou Y-F , Tsai J-C . The effects of simple eight-week regular exercise on cardiovascular disease risk factors in middle-aged women at risk in Taiwan. Acta Cardiologica Sinica. (2007) ;23: (3):169–76. |
[61] | Peters SE , Dennerlein JT , Wagner GR , Sorensen G . Work and worker health in the post-pandemic world: A public health perspective. The Lancet Public Health. (2022) ;7: (2):e188–e194. |
[62] | Eurofound and International Labour Organization. Working Conditions in a Global Perspective; (2019) . |
[63] | Karasek RA . Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative Science Quarterly. (1979) ;24: (2):285–308 . |
[64] | Delgado-Rodríguez M , Llorca J . Bias. J Epidemiol Community Health. (2004) ;58: (8):635–41. PubMed PMID: 15252064; PubMed Central PMCID: PMC1732856. |
[65] | Sedgwick P . Questionnaire surveys: Sources of bias. BMJ. (2013) ;347: (1):f5265–f5265. |


