
Reliability of scapular position and periscapular muscle strength tests in healthy subjects with forward neck and rounded shoulder posture
Abstract
BACKGROUND:
People with forward head posture (FHP) and rounded shoulder posture (RSP) may experience shifts in scapular position and alterations in the strength of the muscles surrounding the scapula. Therefore, a reliable scapula position and scapula muscle strength test are required to identified scapula problem and provided appropriate intervention programs.
OBJECTIVE:
This study aimed to determine the reliability of scapular position measurements obtained using a modified digital inclinometer and palpation meter, as well as muscle strength using a hand-held dynamometer (HHD) in individuals with FHP and RSP.
METHODS:
Thirty healthy subjects underwent scapular position tests (upward rotation, anterior tilt, depression, and protraction) and strength tests of periscapular muscles (serratus anterior, upper trapezius, middle trapezius, and lower trapezius) on both the dominant and non-dominant sides. The reliability of the measurements was confirmed by computing the intraclass correlation coefficient (ICC), standard error of measurement (SEM), and minimal clinically important difference (MCID). Test and re-tests were conducted over a period of one week and actual values for each measurement were also obtained and assessed.
RESULTS:
The ICC ranged from 0.802 to 0.935 for the scapular position tests and from 0.808 to 0.949 for muscle strength tests on the dominant and non-dominant sides. For scapular position tests, SEM values ranged from 0.3 cm to 0.6 cm (protraction and depression), from 1.0∘ to 1.7∘ (upward rotation and anterior tilt) and MCID values ranged from 0.7 cm to 1.6 cm (protraction and depression), from 2.8∘ to 4.7∘ (upward rotation and anterior tilt). Regarding muscle strength tests, SEM and MCID values were in the range 14.4N–27.3N and 39.9N–75.7N, respectively.
CONCLUSIONS:
Scapular position and periscapular muscle strength can be reproducibly measured in healthy subjects individuals with FHP and RSP. These instruments can hence be recommended for evaluating these functional traits in subjects with FHP and RSP.
1.Introduction
Forward head posture (FHP) and rounded shoulder posture (RSP) are prevalent musculoskeletal disorders that can lead to dysfunction and pain in the cervical and shoulder regions. Such neck and shoulder pain often stem from imbalances in the muscles surrounding these areas due to changes in FHP and RSP [1]. The upper crossed syndrome (UCS), which induces alterations in the muscles around the cervical and shoulder region, is marked by FHP, RSP, and an enhanced kyphotic curve in the thoracic region [2, 3]. In this syndrome, the upper trapezius (UT), levator scapula (LS), and pectoralis major (PM) muscles tend to become taut, while the serratus anterior (SA), middle trapezius (MT), and lower trapezius (LT) muscles tend to elongate in the shoulder region. Changes in these muscles (elongation or tightness) can alter scapular positioning [2].
It is recognized that FHP and RSP not only influence the neck muscles but also affect the scapular position and strength of surrounding muscles. In individuals with FHP, scapular positioning can shift, tilting anteriorly, rotating downwardly and interally, elevation and medial bordoer of scapula protruding backward during arm elevation [1]. Additionally, RSP is often associated with both FHP [4, 5] and thoracic kyphosis [6, 7, 8]. Such static postural adjustments lead to changes in scapular positioning and muscle length imbalances, where the UT muscle shortens while the MT, LT, and rhomboid muscles lengthen [6, 9]. Based on the length-tension relationship, these muscle length changes can influence muscle strength [10]. Variations in scapular position can result in changes in the length of periscapular muscles, subsequently altering muscle strength. Consequently, a reliable test of measuring the scapular position and the strength of the periscapular muscles is needed to evaluate scapula problems and provide intervention for FHP and RSP subjects.
Various methods can assess shifts in scapular positioning. Past studies have employed 3D motion analysis to determine shoulder position and movement, and demonstrated its reliability. For instance, it was confirmed that patients with subacromial impingement syndrome (SIS) had reduced scapular posterior tilt or upward scapular rotation compared to healthy individuals [11, 12]. However, 3D motion analysis equipment is costly and not easily applicable in a clinical setting. As an alternative, tools such as the modified digital inclinometer and palpation meter have recently been introduced. These devices are both economical and portable, displaying high reliability for measuring scapular positioning in previous studies. Kim et al. utilized a modified digital inclinometer to gauge the scapular position during upward rotation and anterior-posterior tilt in patients with SIS [13], revealing that this measurement technique was highly reliable. Another study highlighted the high reliability of scapula protraction measurements obtained using a palpation meter in healthy subjects [14]. Additionally, the hand-held dynamometer (HHD) is a straightforward tool for measuring muscle strength in clinical settings and has demonstrated high reliability in past research [15].
Measurements of scapular position using a modified digital inclinometer and palpation meter have been shown to be reliable and easily applicable in clinical practice. However, there is a limited body of research regarding the reliability of the scapular position test in FHP and RSP subjects. Moreover, despite potential alterations in muscle strength due to changes in the scapular position of FHP and RSP subjects, no study has assessed the reliability of the periscapular muscle strength test.
Thus, this study’s objective was to assess the reliability of scapular position measurements obtained using a modified digital inclinometer and palpation meter, and of scapular muscle strength tests performed using an HHD, in individuals with FHP and RSP.
2.Methods
2.1Subjects
Thirty healthy male subjects (mean age
Table 1
Reliability values for scapular position and muscle strength tests on the dominant side
| ICC | SEM | MCID | |
|---|---|---|---|
| Scapula position test | |||
| Protraction (cm) | 0.911 | 0.3 | 0.7 |
| Upward rotation (∘) | 0.802 | 1.0 | 2.8 |
| Anterior tilt (∘) | 0.902 | 1.1 | 3.0 |
| Depression (cm) | 0.821 | 0.6 | 1.6 |
| Scapula muscle strength test | |||
| Serratus anterior (N) | 0.887 | 18 | 49.9 |
| Upper trapezius (N) | 0.949 | 18 | 49.9 |
| Middle trapezius (N) | 0.858 | 23.8 | 66.1 |
| Lower trapezius (N) | 0.836 | 15.7 | 43.7 |
Abbreviations: ICC, intraclass correlation coefficient; SEM, standard error of measurement; MCID, minimal clinically important difference.
Participants were drawn from a pool of individuals who voluntarily responded to a public advertisement. Only those who contacted the primary investigator and experiment supervisor were considered. All participants received detailed information about the study before taking part and provided consent via forms endorsed by the KAYA University Ethics Committee for Human Investigation (No. KAYA IRB-359). This study was registered in the Clinical Research Information Service, with reg-istration number KCT0008700.
2.2Experimental procedures
Prior to the assessment of scapular position and periscapular muscle strength, each subject completed a demographic questionnaire providing information such as age, weight, and height.
To determine the intra-rater reliability of the scapular position test and periscapular muscle strength, evaluations were conducted twice within a week by examiners with a decade of clinical experience. Following the scapular position test, the strength of the periscapular muscle was determined. Markers were positioned by the examiner on the inferior angle of the scapula, the posterolateral side of the acromion, and the scapular spine’s root before scapular position measurements. Protraction, upward rotation, anterior tilt, and depression were measured on the dominant and non-dominant sides in different scapular positions. Subsequent to these measurements, after a 30-minute interval to avoid muscle fatigue, the strength of the periscapular muscles was measured. The dominant side was evaluated first, followed by the non-dominant side. A second round of measurements was performed a week later. If a subject engaged in sporting activities within the week after the initial test, they were omitted, because such activities might influence the results.
2.3Measurement of scapular position
Figure 1.
Scapula position tests: upward rotation (A), anterior tilt (B), depression (C), protraction (D).
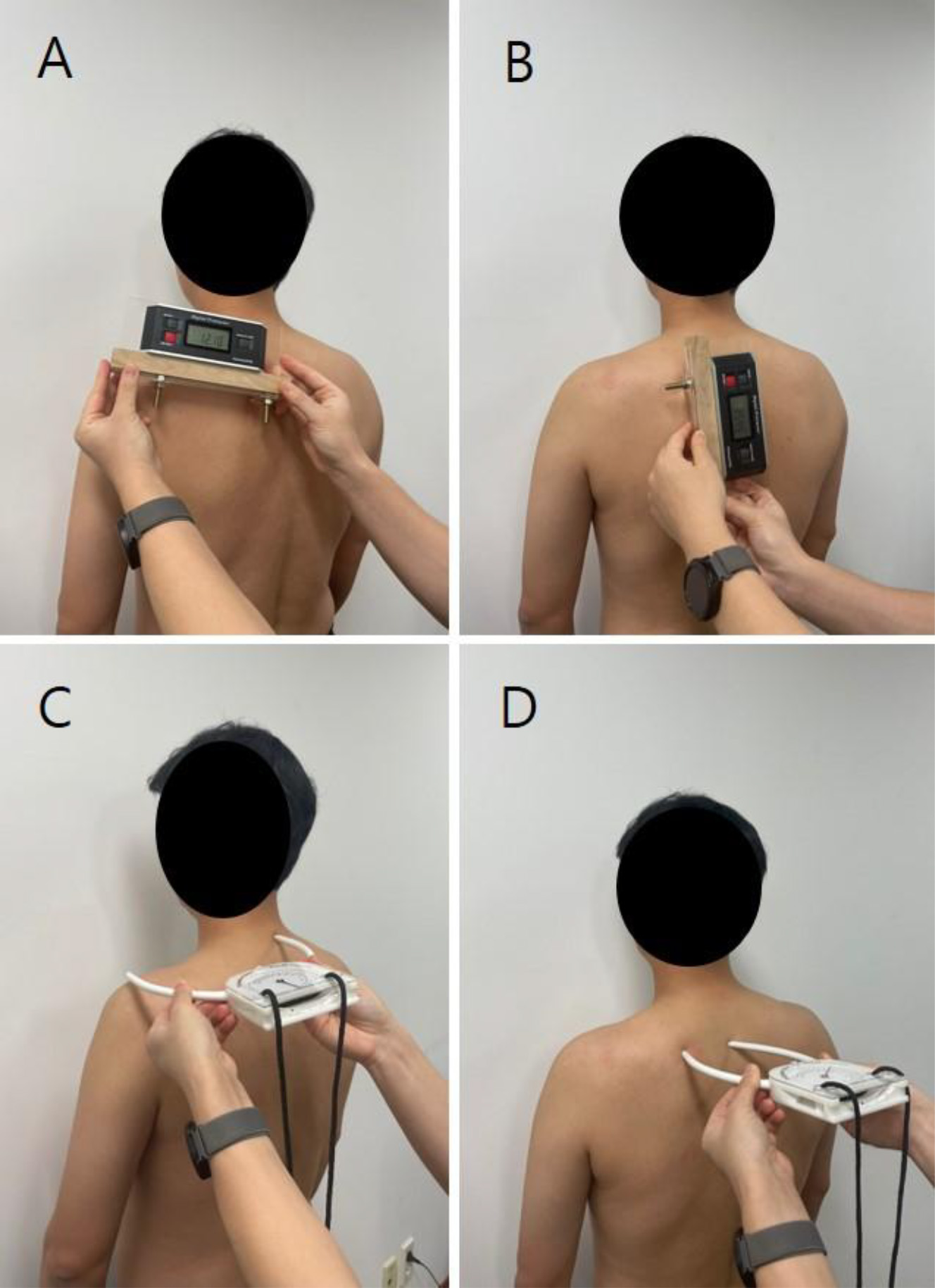
In a static standing pose, the subject’s scapular position was measured during protraction, upward rotation, anterior tilt, and depression. To determine upward rotation and anterior tilt of the scapula, a modified digital inclinometer was utilized, which has previously demonstrated high reliability [13]. This digital inclinometer was modified based on past studies [18, 19]. Two “locator rods,” each around 7 cm in length, were affixed to a customized plate attached to the primary body of the digital inclinometer (Pro 360, Baseline; Fabrication Enterprises, White Plains, NY, USA) using cylindrical screws 1 cm in diameter and 2 cm in length. Utilizing the locator rods, the device was aligned with the scapula’s bony landmarks to measure angles in each scapular position in a static stance. A “bubble indicator” was attached to the inclinometer’s body to ensure accurate measurement while maintaining vertical alignment of the inclinometer’s horizontal surface. For upward scapula rotation measurement, subjects stood upright, markers were positioned over the acromion process and the root of the scapular spine, and the angle of inclination was measured using the inclinometer (Fig. 1A). To assess scapular anterior tilt, subjects stood with their arms in a natural position by the sides, and markers were placed on the scapula’s inferior angle and spine root. The angle between the device and the thoracic wall was then measured (Fig. 1B). Scapular depression and protraction were quantified using a palpation meter (PALM; Performance Attainment Associates, St. Paul MN, USA). To measure scapular depression, the palpation meter was positioned on the C7 spinous process (SP) and the acromion while the subject’s arm was relaxed (Fig. 1C). To measure scapular protraction, the palpation meter was aligned with the scapular spine root and the corresponding thoracic SP (Fig. 1D). There was a 10-second rest period between trials and a 10-minute rest between tests, and the mean of three measurements was analyzed.
Figure 2.
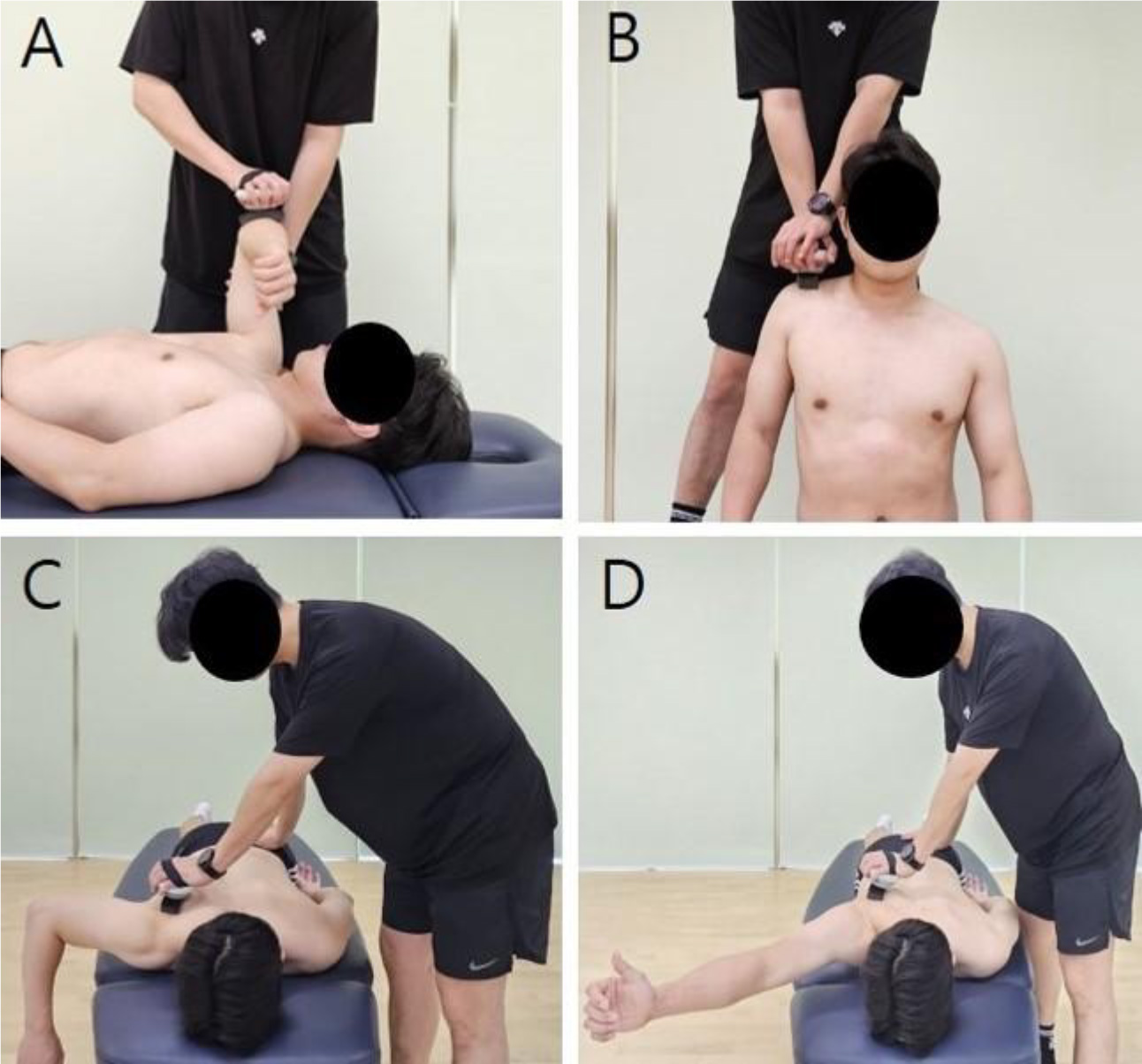
Techniques for measuring the strength of muscles around the scapula: serratus anterior (A), upper trapezius (B), middle trapezius (C), and lower trapezius (D).
2.4Measurement of periscapular muscle strength
The strength of the SA, UT, MT, and LT muscles was assessed. For the SA, subjects were positioned supine with 90∘ of shoulder and elbow flexion and forearm pronation. The examiner positioned a HHD on the subject’s elbow, instructing the subject to push forward with maximum effort. The HHD reading was then recorded (Fig. 2A). For the UT measurement, subjects were seated, and the HHD was placed midway between the C7 and acromion process. Each subject was instructed to elevate the shoulder maximally, and the HHD value was recorded (Fig. 2B). The strength of the MT was measured with subjects in a prone position and the shoulder joint of the assessed side abducted to 90∘. The examiner positioned the HHD above the scapula, instructing the subject to horizontally abduct the scapula to the maximum extent. The HHD reading was recorded (Fig. 2C). For the LT measurement, subjects were prone with the shoulder joint abducted 120∘. The HHD was placed on the scapula. Subjects were instructed to horizontally abduct the shoulder joint fully, and the value displayed on the HHD was recorded (Fig. 2D). If force equilibrium between the examiner and subject was not achieved during measurement or if the subject experienced pain, the test was halted and resumed after a brief rest. A 2-minute rest was provided between each muscle strength test. Each muscle strength assessment was repeated three times, and the average of the three maximum force values was analyzed.
2.5Statistical analysis
The Kolmogorov-Smirnov test was employed to verify the normality of the data distribution. Reliability was estimated using the intraclass correlation coefficient (ICC), with values of
3.Results
Tables 1 and 2 present the ICC, SEM, and MCID values for the entire scapular position test on both the dominant and non-dominant sides. On the dominant side, ICC values (upward rotation, anterior tilt, depression, and protraction) ranged from 0.802 to 0.911, falling within the high and excellent categories. The SEM on the dominant side were in the range of 0.3 cm–0.6 cm (protraction and depression), 1.0∘–1.1∘ (upward rotation and anterior tilt) and MCID were in the range of 0.7 cm–1.6 cm (protraction and depression) and 2.8∘–4.7∘ (upward rotation and anterior tilt). The intra-rater reliability for the scapular position test on the non-dominant side was also high to excellent, with ICC values ranging from 0.816 to 0.935. On the non-dominant side, the SEM values were in the range of 0.3 cm–0.5 cm (protraction and depression), 1.3∘–1.7∘ (upward rotation and anterior tilt) and MCID values were in the range of 0.7 cm–1.5 cm (protraction and depression)and 3.6∘–4.7∘ (upward rotation and anterior tilt).
Table 2
Reliability values for scapular position and muscle strength tests on the non-dominant side
| ICC | SEM | MCID | |
|---|---|---|---|
| Scapula position test | |||
| Protraction (cm) | 0.935 | 0.3 | 0.7 |
| Upward rotation (∘) | 0.816 | 1.7 | 4.7 |
| Anterior tilt (∘) | 0.884 | 1.3 | 3.6 |
| Depression (cm) | 0.845 | 0.5 | 1.5 |
| Scapula muscle strength test | |||
| Serratus anterior (N) | 0.918 | 14.4 | 39.9 |
| Upper trapezius (N) | 0.886 | 27.3 | 75.7 |
| Middle trapezius (N) | 0.935 | 14.6 | 40.6 |
| Lower trapezius (N) | 0.808 | 16.7 | 46.2 |
Abbreviations: ICC, intraclass correlation coefficient; SEM, standard error of measurement; MCID, minimal clinically important difference.
For the muscle strength test, encompassing measurements of SA, UT, MT, and LT, the intra-rater reliability was high to excellent on both the dominant (range: 0.836–0.949) and non-dominant sides (range: 0.808–0.935). The SEM values for the periscapular muscle strength test ranged from 15.7N to 23.8N, while the MCID ranged from 43.7N to 66.1N, as depicted in Tables 1 and 2.
Table 3
Scapular position and muscle strength data on the dominant and non-dominant sides
| Dominant | Non-Dominant | |||
| Trial 1 | Trial 2 | Trial 1 | Trial 2 | |
| Scapula position | ||||
| Protraction (cm) | 7.19 | 7.18 | 7.35 | 7.26 |
| Upward rotation (∘) | 3.71 | 4.42 | 4.60 | 4.06 |
| Anterior tilt (∘) | 6.06 | 6.26 | 3.98 | 4.94 |
| Depression (cm) | 6.05 | 5.91 | 5.77 | 5.67 |
| Scapula muscle strength test | ||||
| Serratus anterior (N) | 224.21 | 225.21 | 214.38 | 224.46 |
| Upper trapezius (N) | 279.99 | 288.73 | 279.89 | 285.93 |
| Middle trapezius (N) | 162.25 | 175.94 | 165.31 | 175.19 |
| Lower trapezius (N) | 137.78 | 143.12 | 141.10 | 144.88 |
Table 3 shows the mean and standard deviation values for the entire scapula position and muscle strength (SA, UT, MT, and LT) on the dominant and non-dominant sides.
4.Discussion
To the best of our knowledge, this is the first study to examine the reliability of strength measurements of the scapular muscles in individuals with FHP and RSP. Our investigation aimed to confirm the reliability of scapula position and periscapular muscle strength measurements obtained on both the dominant and non-dominant sides. Both measurements demonstrated high to excellent reliability.
The ICC values for the scapular position test were high for both the dominant and non-dominant sides, in line with previous studies. Two factors can account for the high ICC values for scapular position measurements. First, the scapular position was ascertained using skin palpation. A previous study that used a method similar to ours, marking the scapula with pins to measure its position and movement, confirmed the validity of the approach [21]. Another study, which utilized a modified digital inclinometer with locator rods, proposed that identifying the scapula through skin palpation and subsequently measuring its position is valid and reliable. The second reason for the high ICC values for scapular position measurements relates to the equipment used to measure the scapular position. Given the slight curvature of the scapula, measuring its upward rotation and anterior tilt using a standard digital inclinometer can be challenging. However, our modified inclinometer equipped with two locator rods can measure the scapular position with greater precision. Scapula protraction, which is determined by the distance between the scapula spine root and the corresponding thoracic SP, can be influenced by muscle bulk if measured using a tape. However, the palpation meter, with its two locator rods, eliminates interference by muscle bulk during scapula protraction measurement, as indicated by prior studies. For instance, high ICC values were reported for scapula upward rotation and anterior tilt measurements using a modified digital inclinometer in patients with SIS [13]. Similarly, Johnson et al. found that the ICC for scapula upward rotation measurements was high (0.89–0.96) in participants both with and without shoulder pain [18]. Another study reported high ICC values when measuring scapula protraction in healthy subjects using a palpation meter [14]. Our results suggest that the modified digital inclinometer and palpation meter are useful devices for assessing scapular position in subjects with forward neck posture. The high to excellent ICC values observed in our study further underscore the precision of our measurement method, which directly palpates the scapula.
Regarding the strength of the muscles around the scapula, all ICC values in this study were excellent for both the dominant and non-dominant sides. In prior research, the reliability of UT, MT, LT, and SA muscle strength measurements (ICC values of 0.89–0.96) obtained using an HHD in patients with shoulder pain was high to excellent. Other studies examining the reliability of the MT muscle strength tested using an HHD, such as those by DiVeta et al. (ICC: 0.96) [22], and Zmierski et al. (ICC: 0.96–0.98) [23], also reported excellent results, in line with our data. The position used in our study for measuring strength was selected to allow the primary mover to be more active than the synergistic muscle [15]. Additionally, resistance was provided by the examiner at a point that maximized the primary mover’s activity, which might have contributed to the high reliability.
Although ICC values are useful, the insight they provide into errors or variations in measurement methods can be limited. Nevertheless, they can be useful for assessing the reliability of equipment or measurement techniques [24]. SEM indicates measurement imprecision or variability due to errors [25] for a particular apparatus. In our study, the SEM values for scapular protraction and depression ranged from 0.3 to 1.0 cm, and upward rotation (1.0∘) and anterior tilt (1.1∘) were lower compared to past studies [13, 18, 26, 27]. The SEM for muscle strength was similar to that reported previously [15]. Discrepancies may have arisen because we used static postures when measuring upward rotation and anterior tilt, while earlier studies performed dynamic position evaluations. Compared to SEM, MCID is a more valuable estimate of error; it helps determine whether observed changes in scapular position and periscapular muscle strength result from errors or genuine changes [15]. In our study, the MCID values varied across measurements, with those for scapula protraction, rounded shoulder, and depression ranging from 0.7 to 1.6 cm, and those of upward rotation and anterior tilt ranging between 2.8∘ and 3.0∘. The MCID values for periscapular muscle strength varied from 43.7 to 66.1N. Given that alterations in neck and shoulder posture can lead to functional issues by altering the scapula’s position and the strength of periscapular muscles, these metrics can serve as benchmark data for evaluating FHP and RSP.
Our study had some limitations. First, as the upward rotation angle might influence the ICC value or SEM of the scapula [26, 28], future studies should assess the scapular position at various shoulder angles. Second, our sample size was relatively small; larger studies are therefore needed. Lastly, our study did not explore interrater reliability. Future studies should focus on this metric, particularly in measurements of forward neck posture.
In clinical settings, pinpointing the scapula’s location and accurately measuring the strength of the muscles around it is crucial for effective treatment of patients with neck and scapular postural deviations. The methodology employed in this study to measure the scapular position and assess the strength of surrounding muscles exhibited high reliability and low SEM values. Furthermore, the modified digital inclinometer has proven to be a dependable measurement tool irrespective of the therapist’s experience [13].
5.Conclusions
In subjects with FHP and RSP, the measurement of scapular position and periscapular muscle strength measurements obtained using a modified digital inclinometer and HHD, respectively, proved to be clinically reproducible. We suggest that the SEM and MCID data obtained frpm this study can serve as reference for clinical tests and treatments in these cohorts.
Author contributions
CONCEPTION: Soo-Yong Kim, Tae-Gyu Kim, Jun-Seok Kim, Haimin Zhang.
PERFORMANCE OF WORK: Soo-Yong Kim, Tae-Gyu Kim, Jun-Seok Kim, Haimin Zhang.
INTERPRETATION OR ANALYSIS OF DATA: Soo-Yong Kim, Tae-Gyu Kim.
PREPARATION OF THE MANUSCRIPT: Soo-Yong Kim, Tae-Gyu Kim, Jun-Seok Kim.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Soo-Yong Kim, Tae-Gyu Kim.
SUPERVISION: Soo-Yong Kim, Tae-Gyu Kim.
Ethical considerations
Ethical approval of our work was obtained from KAYA (KAYA IRB-359) University Ethics Committee for Human Investigation., and the subjects signed a statement of informed consent prior to participation and this study from July 2022 to July 2023 (a period of 12 months).
Funding
The authors report no funding.
Conflict of interest
The authors have no conflict of interest to report.
References
[1] | Singla D, Veqar Z. Association between forward head, rounded shoulders, and increased thoracic kyphosis: a review of the literature. J Chiropr Med. (2017) ; 16: : 220-229. doi: 10.1016/j.jcm.2017.03.004. |
[2] | Page P, Frank C, Lardner R. Assessment and treatment of muscle imbalance: the Janda approach; Human Kinetics: Champaign. (2010) . |
[3] | Janda V. Muscles and motor control in cervicogenic disorders: assessment and management: Physical therapy of the cervical and thoracic spine; Churchill Livingstone: New York. (1994) ; 195-216. |
[4] | Thigpen CA, Padua DA, Michener LA, Guskiewicz K, Giuliani C, Keener JD, et al. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J Electromyogr Kinesiol. (2010) ; 20: : 701-709. doi: 10.1016/j.jelekin.2009.12.003. |
[5] | Kwon JW, Son SM, Lee NK. Changes in upper-extremity muscle activities due to head position in subjects with a forward head posture and rounded shoulders. J Phys Ther Sci. (2015) ; 27: : 1739-1742. |
[6] | Ghanbari A, Ghaffarinejad F, Mohammadi F, Khorrami M, Sobhani S. Effect of forward shoulder posture on pulmonary capacities of women. Sports Med. (2008) ; 42: : 622-623. doi: 10.1136/bjsm.2007.040915. |
[7] | Kebaetse M, McClure P, Pratt NA. Thoracic position effect on shoulder range of motion, strength, and three-dimensional scapular kinematics. Arch Phys Med Rehabil. (1999) ; 80: : 945-950. doi: 10.1016/s0003-9993(99)90088-6. |
[8] | Lee JH, Cynn HS, Yi CH, Kwon OY, Yoon TL. Predictor variables for forward scapular posture including posterior shoulder tightness. J Bodyw Mov Ther. (2015) ; 19: : 253-260. doi: 10.1016/j.jbmt.2014.04.010. |
[9] | Levangie PK, Norkin CC. Joint structure and function: a comprehensive analysis, 3rd ed;. Jaypee Brothers: New Delhi, India. (2001) . |
[10] | Neumann DA. Kinesiology of the musculoskeletal system: foundations for physical rehabilitation; Mosby: Philadelphia. (2002) . |
[11] | Lukasiewicz AC, McClure P, Michener L, Pratt N, Sennett B. Comparison of three-dimensional scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. (1999) ; 29: : 574-583. doi: 10.2519/jospt.1999.29.10.574. |
[12] | McClure PW, Bialker J, Neff N, Williams G, Karduna A. Shoulder function and 3-dimensional kinematics in people with shoulder impingement syndrome before and after a 6-week exercise program. Phys Ther. (2004) ; 84: : 832-848. doi: 10.1093/ptj/84.9.832. |
[13] | An DI, Park JE, Lee CH, Kim SY. Reliability of scapular upward rotation and anterior-posterior tilt measurements using a modified digital inclinometer in patients with subacromial impingement syndrome. J Back Musculoskelet Rehabil. (2021) ; 34: : 837-843. doi: 10.3233/bmr-200080. |
[14] | Da Costa BR, Armijo-Olivo S, Gadotti I, Warren S, Reid DC, Magee DJ. Reliability of scapular positioning measurement procedure using the palpation meter. Physiotherapy. (2010) ; 96: : 59-67. doi: 10.1016/j.physio.2009.06.007. |
[15] | Michener LA, Boardman ND, Pidcoe PE, Frith AM. Scapular muscle tests in subjects with shoulder pain and functional loss: reliability and construct validity. Phys Ther. (2005) ; 85: : 1128-1136 doi: 10.1093/ptj/85.11.1128. |
[16] | Ruivo RM, Pezarat-Correia P, Carita AI. Intrarater and interrater reliability of photographic measurement of upper body standing posture of adolescents. J Manip Physiol Ther. (2015) ; 38: : 74-80. doi: 10.1016/j.jmpt.2014.10.009. |
[17] | Falla D, Jull G, Russell T, Vicenzino B, Hodges P. Effect of neck exercise on sitting posture in patients with chronic neck pain. Phys Ther. (2007) ; 87: : 408-417. doi: 10.2522/ptj.20060009. |
[18] | Johnson MP, McClure PW, Karduna AR. New method to assess scapular upward rotation in subjects with shoulder pathology. J Orthop Sports Phys Ther. (2001) ; 31: : 81-89. doi: 10.2519/jospt.2001.31.2.81. |
[19] | Scibek JS, Carcia CR. Assessment of scapulohumeral rhythm for scapular plane shoulder elevation using a modified digital inclinometer. World J Orthop. (2012) ; 3: : 87-94. doi: 10.5312/wjo.v3.i6.87. |
[20] | Munro BH, Visintainer MA, Page EB. Statistical methods for health care research. JB Lippincott: Philadelphia. (1986) . |
[21] | Lewis J, Green A, Reichard Z, Wright C. Scapula position: the validity of skin surface palpation. Man Ther. (2022) ; 7: : 26-30. doi: 10.1054/math.2001.0405. |
[22] | DiVeta J, Walker ML, Skibinski B. Relationship between performance of selected scapular muscles and scapular abduction in standing subjects. Phys Ther. (1990) ; 70: : 470-476. doi: 10.1093/ptj/70.8.470. |
[23] | Zmierski T, Kegerreis S, Scarpaci J. Scapular muscle strengthening. J Sport Rehab. (1995) ; 4: : 244-252. |
[24] | Edouard P, Samozino P, Julia M, Gleizes Cervera S, Van-biervliet W, Calmels P, et al. Reliability of isokinetic assessment of shoulder-rotator strength: a systematic review of the effect of position. J Sport Rehabil. (2011) ; 20: : 367-383. doi: 10.1123/jsr.20.3.367. |
[25] | Hopkins WG. Measures of reliability in sports medicine and science. Sports Med. (2000) ; 30: : 1-15. doi: 10.2165/00007256-200030010-00001. |
[26] | Tucker WS, Ingram RL. Reliability and validity of measuring scapular upward rotation using an electrical inclinometer. J Electromyogr Kinesiol. (2012) ; 22: : 419-423. doi: 10.1016/j.jelekin.2012.02.013. |
[27] | Tangrood ZJ, Sole G, Ribeiro DC. Between-day reliability of scapular locator for measuring scapular position during arm elevation in asymptomatic participants. J Manip Physiol Ther. (2020) ; 43: : 276-283. doi: 10.1016/j.jmpt.2019.03.014. |
[28] | Larsen CM, Søgaard K, Eshoj H, Ingwersen K, Juul-Kristensen B. Clinical assessment methods for scapular position and function: An inter-rater reliability study. Physiother Theory Pract. (2020) ; 36: : 1399-1420. doi: 10.1080/09593985.2019.1579284. |


