
Effectiveness of Second-Line Cabozantinib in Metastatic Clear Cell Renal Cell Carcinoma Patients After First-Line Treatment with Immune Checkpoint Inhibitor-based Combinations
Abstract
Background:
Cabozantinib, a tyrosine kinase inhibitor (TKI), is a prevalent second-line (2 L) therapy and was approved for use after progression on TKIs. However, the 1 L treatment setting has changed since the approval of cabozantinib monotherapy in salvage therapy settings.
Objective:
To assess the differential effectiveness of cabozantinib after prior progression on 1 L ipilimumab with nivolumab (IPI + NIVO) compared to programmed death receptor-1 (PD-1) or PD-1 ligand (PD-L1) inhibitors (PD1/L1i) with TKIs.
Methods:
Utilizing a nationwide electronic health record (EHR)-derived de-identified database, we included patients with metastatic clear cell renal cell carcinoma (mccRCC) who received 1 L treatment with an immune checkpoint inhibitor (ICI)-based combination and 2 L treatment with cabozantinib monotherapy. These patients were categorized based on the type of 1 L ICI-based combination received: IPI + NIVO vs. PD1/L1i with TKI. Real-world time to next therapy (rwTTNT) and real-world overall survival (rwOS) were summarized using Kaplan-Meier curves and compared using Cox-proportional hazard models adjusted for International mRCC Database Consortium (IMDC) risk groups.
Results:
Among 12,285 patients with metastatic renal cell carcinoma, 237 were eligible and included. Median rwTTNT was 8 months for the IPI + NIVO subgroup and 7.5 months for the PD1/L1i + TKI subgroup (HR 1.05, 95% CI: 0.74–1.49, p = 0.8). Median rwOS was 17 months for IPI + NIVO and 16 months for PD1/L1i + TKI subgroup (HR 0.79, 95% CI: 0.52–1.20, p = 0.3).
Conclusions:
Cabozantinib remains effective as a 2 L therapy for mccRCC independent of the type of prior 1 L ICI-based combination. Further research is needed to validate these findings and explore the ideal sequencing of therapies.
INTRODUCTION
The therapeutic landscape of metastatic clear cell renal cell carcinoma (mccRCC) has significantly changed in the last decade. Currently, immune-checkpoint inhibitors (ICIs)-based combinations represent the first-line standard of care for mccRCC, which is either ipilimumab with nivolumab (IPI + NIVO) or programmed death receptor-1 (PD-1) or PD-1 ligand (PD-L1) inhibitors (PD1/L1i) with vascular endothelial growth factor (VEGF) tyrosine kinase inhibitor (TKIs) (i.e., axitinib and avelumab, axitinib and pembrolizumab, cabozantinib and nivolumab, and lenvatinib and pembrolizumab) [1–6]. However, data is limited to select the best second-line therapy after progression on first-line ICI-based combinations. Cabozantinib is among the available options and is one of the most commonly used agents in a second-line treatment setting [7]. Cabozantinib is an oral receptor TKI that is active against several receptor tyrosine kinases, including VEGFR2, MET, and AXL [8]. In the METEOR trial, which investigated cabozantinib in the second-line treatment setting, patients experienced disease progression on first-line VEGF TKIs and not ICI-based combinations [9]. However, it is currently unknown whether cabozantinib activity in the second line treatment setting differs by prior treatment with IPI + NIVO vs VEGF-TKIs in the first line treatment setting. There is limited preclinical evidence [10] and only few clinical studies have investigated the effectiveness of a VEGF-TKI in a second-line treatment setting in patients who progressed on prior ICI-based combinations [11–19]. Herein, we sought to investigate the effectiveness of second-line cabozantinib in patients who received prior first-line IPI + NIVO versus PD1/L1i with TKI in a large real-world database. We hypothesize that cabozantinib will have similar effectiveness independent of the prior ICI-based combination type.
METHODS
Cohorts and exposure
This cohort study was approved by the institutional review board at the University of Utah and adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines and used the nationwide Flatiron Health electronic health record (EHR)-derived de-identified database. The Flatiron Health database is a longitudinal database comprising de-identified patient-level structured and unstructured data curated via technology-enabled abstraction from >280 cancer clinics (∼800 sites of care) [20, 21]. The data are de-identified and subject to obligations to prevent re-identification and protect patient confidentiality. The present cohort study included adult patients (aged≥18 years at diagnosis) with mccRCC treated with IPI + NIVO or PD1/L1i with TKI as a first-line therapy, followed by second-line therapy with single-agent cabozantinib. Patients received the first-line treatment from 3/10/2017 to 7/20/2022 and the second-line treatment from 1/16/2018 to 9/26/2022. Lines of therapy were defined by clinical oncology experts’ rules. Patients treated with first-line cabozantinib, those enrolled in clinical trials, and patients without documentation of first-line treatment were excluded.
Baseline variables prior to initiation of the second line, such as age, race, practice type, insurance, IMDC risk, and prior nephrectomy, were collected. Insurance status for each patient was derived using the imputed coverage window method, assuming calendar-year coverage. IMDC risk scores were calculated based on six prognostic variables, namely time to start of first-line treatment after initial diagnosis, performance status, hemoglobin, calcium, neutrophil, and platelet counts (22). IMDC risk was categorized as follows: patients with three or more negative prognostic variables were categorized as poor risk, patients with 1 or 2 negative prognostic variables, or patients with 2 negative prognostic variables and non-missing values in all remaining score criteria or patients with 1 negative prognostic variable and 0 or 1 missing values were categorized as intermediate risk, patients with 1 or 2 negative prognostic variables but failed to be categorized as intermediate risk category due to missingness were categorized as poor/intermediate risk, patients with 0 negative prognostic variables and non-missing values in all prognostic variables were categorized as favorable risk, and patients with 0 negative prognostic variables and at least one missingness value were categorized as unknown. For the analysis purpose, patients were categorized into two groups – favorable risk and intermediate/poor risk – by merging patients who were in poor risk, intermediate risk, poor/intermediate risk into intermediate/poor risk.
Outcomes and analyses
Endpoints were real-world time to next therapy (rwTTNT) and real-world overall survival (rwOS). rwTTNT was measured from the start of the second line to the start of the third line, and rwOS was measured from the start of the second line to death from any cause or loss to follow-up. rwTTNT and rwOS were summarized via Kaplan-Meier survival estimates with a 95% confidence interval (CI) and compared in the context of the multivariable Cox proportional hazard model. In the multivariable analysis, we adjusted for the IMDC risk group. All analyses were done using R version 4.2.3.
RESULTS
Of the 12285 patients with metastatic renal cell carcinoma (mRCC) in the database, 237 met eligibility criteria and were included in the analysis. In the first-line treatment setting, 145 patients were treated with IPI + NIVO and 92 patients with PD1/L1i with TKI. Out of the 92 patients, 92.4% received pembrolizumab with axitinib (Fig. 1). The median age of the overall cohort was 65 years (IQR 50–80), 64 (IQR 49–79) for the IPI + NIVO group, and 68 (IQR 54–82) for the PD1/L1i with TKI group. In the IPI + NIVO cohort and the PD1/L1i cohort, 6.9% and 14.1% of patients had IMDC favorable risk, respectively. The median duration of first-line treatment was 162 days (IQR 110–285) for the IPI + NIVO group and 304 days (IQR 178–482) for the PD1/L1i with TKI group. The majority of patients in this study originated from community oncology practices. Baseline characteristics of the study population by treatment are summarized in Table 1.
Fig. 1
Schematic representation of patient selection for the study. Abbreviations: ICI: immune checkpoint inhibitor. IPI + NIVO: ipilimumab with nivolumab. PD1/L1i with TKI: PD1/L1 inhibitor with tyrosine kinase inhibitor. mRCC: metastatic renal cell carcinoma. mccRCC: metastatic clear cell renal cell carcinoma. 1L: first-line. 2L: second-line. Created with Biorender®.
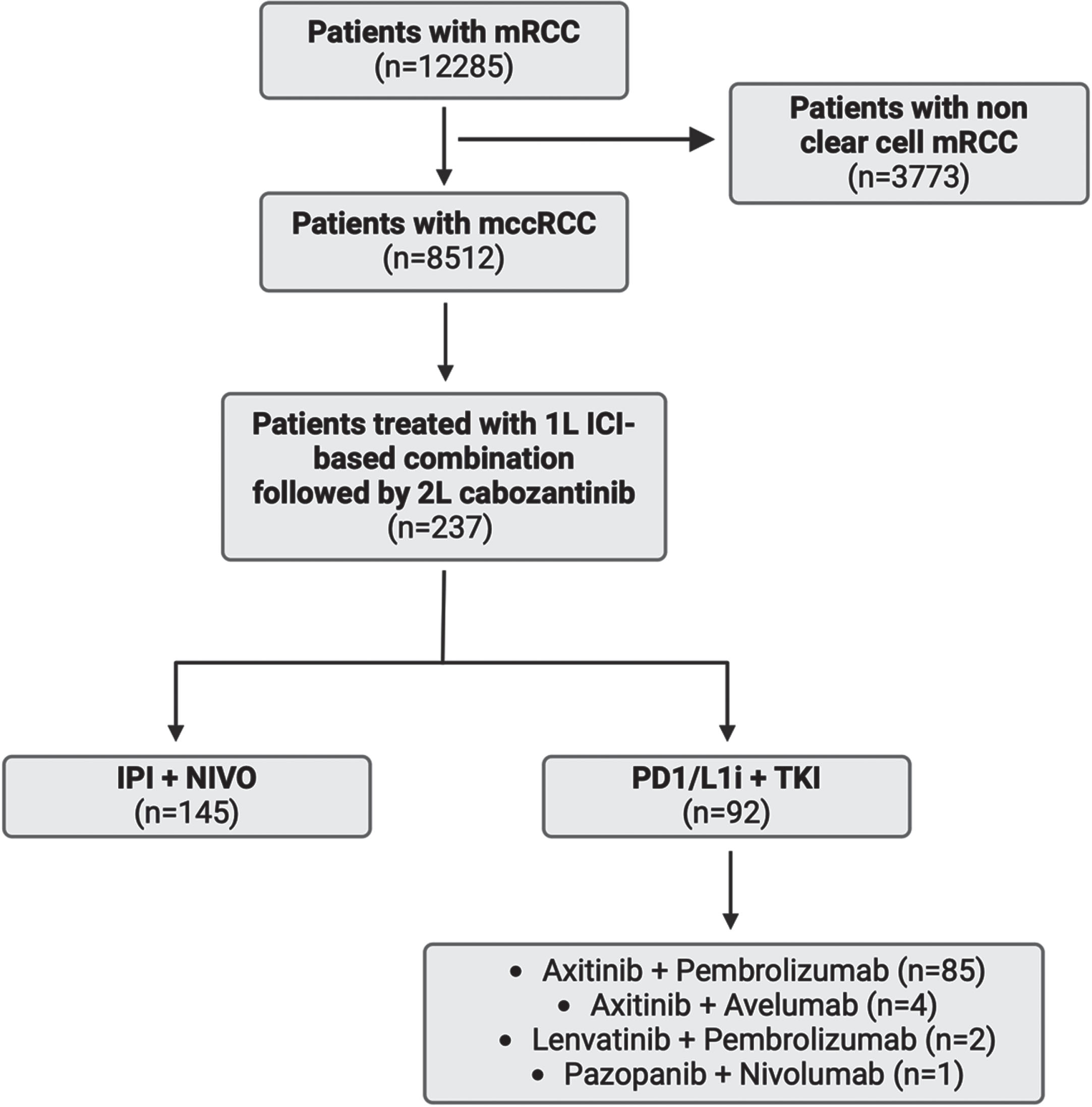
Table 1
Baseline characteristics
| Variable | IPI + NIVO (145) | PD1/L1i + TKI (92) | |
| Age, n (%) | <65 | 75 (51.7) | 33 (35.9) |
| 65–75 | 43 (29.7) | 31 (33.7) | |
| ≥75 | 27 (18.6) | 28 (30.4) | |
| Gender, n (%) | Male | 106 (73.1) | 62 (67.4) |
| Female | 39 (26.9) | 30 (32.6) | |
| Race/Ethnicity, n (%) | White Non-Hispanic | 94 (71.2) | 57 (67.1) |
| Black Non-Hispanic | 11 (8.3) | < =5 (5.9) | |
| Hispanic/Latino | 11 (8.3) | < =5 (5.9) | |
| Other | 16 (12.1) | 19 (22.4) | |
| Practice Type, n (%) | Community | 121 (85.2) | 80 (88.9) |
| Academic | 21 (14.8) | 10 (11.1) | |
| Insurance Type, n (%) | Commercial Health Plan | 87 (64.9) | 59 (65.6) |
| Medicare/Medicaid | 19 (14.2) | 13 (14.4) | |
| Others | 28 (20.9) | 18 (20) | |
| IMDC Risk Group, n (%) | Favorable Risk | 10 (6.9) | 13 (14.1) |
| Poor/Intermediate Risk | 128 (88.3) | 74 (80.4) | |
| Unknown | 7 (4.8) | 5 (5.4) | |
| Prior Nephrectomy, n (%) | No | 55 (37.9) | 35 (38) |
| Yes | 90 (62.1) | 57 (62) | |
| Total number of lines of therapy received, n (%) | 2 | 73 (50.3) | 63 (68.5) |
| 3 | 50 (34.5) | 17 (18.5) | |
| 4 | 14 (9.7) | 9 (9.8) | |
| 5 | 7 (4.8) | 3 (3.3) | |
| 6 | 1 (0.7) | 0 (0) |
Abbreviations: IPI + NIVO: ipilimumab with nivolumab; PD1/L1i: PD1/L1 inhibitor; TKI: tyrosine kinase inhibitor.
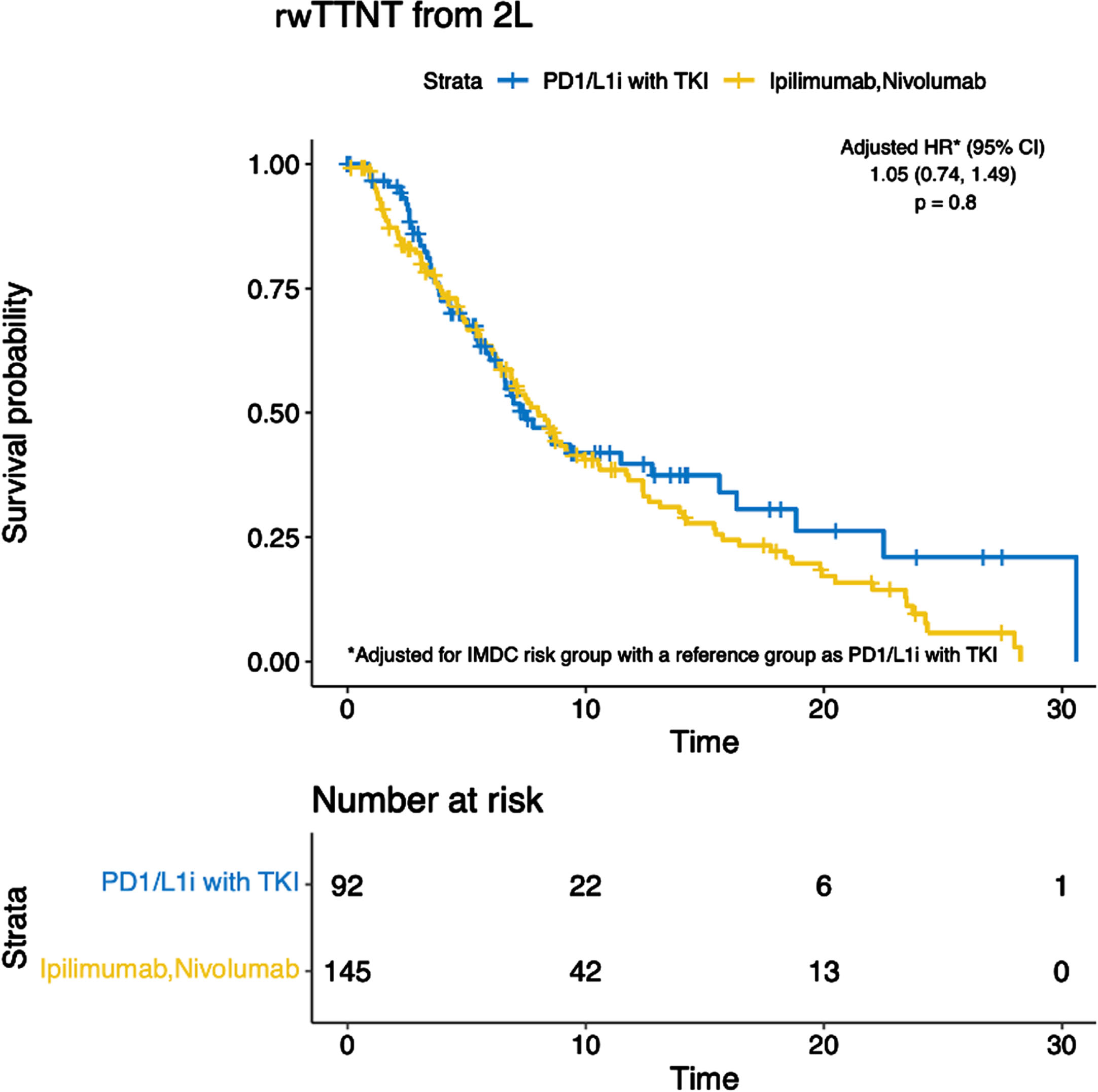
The median rwTTNT was 8 months (95% CI 6.9–11) for patients treated with IPI + NIVO and 7.5 months (95% CI 6.3–16) for patients treated with PD1/L1i with TKI (ref. group) (HR 1.21, 95% CI 0.87–1.70, p = 0.3). On the multivariable analysis, rwTTNT remained similar between the two groups (HR 1.05, 95% CI 0.74–1.49, p = 0.8) (Fig. 2).
Fig. 2
Kaplan-Meier curves demonstrating real-world time to next therapy (rwTTNT). Abbreviations: PD1/L1i with TKI: PD1/L1 inhibitor with tyrosine kinase inhibitor. 2L: second-line.
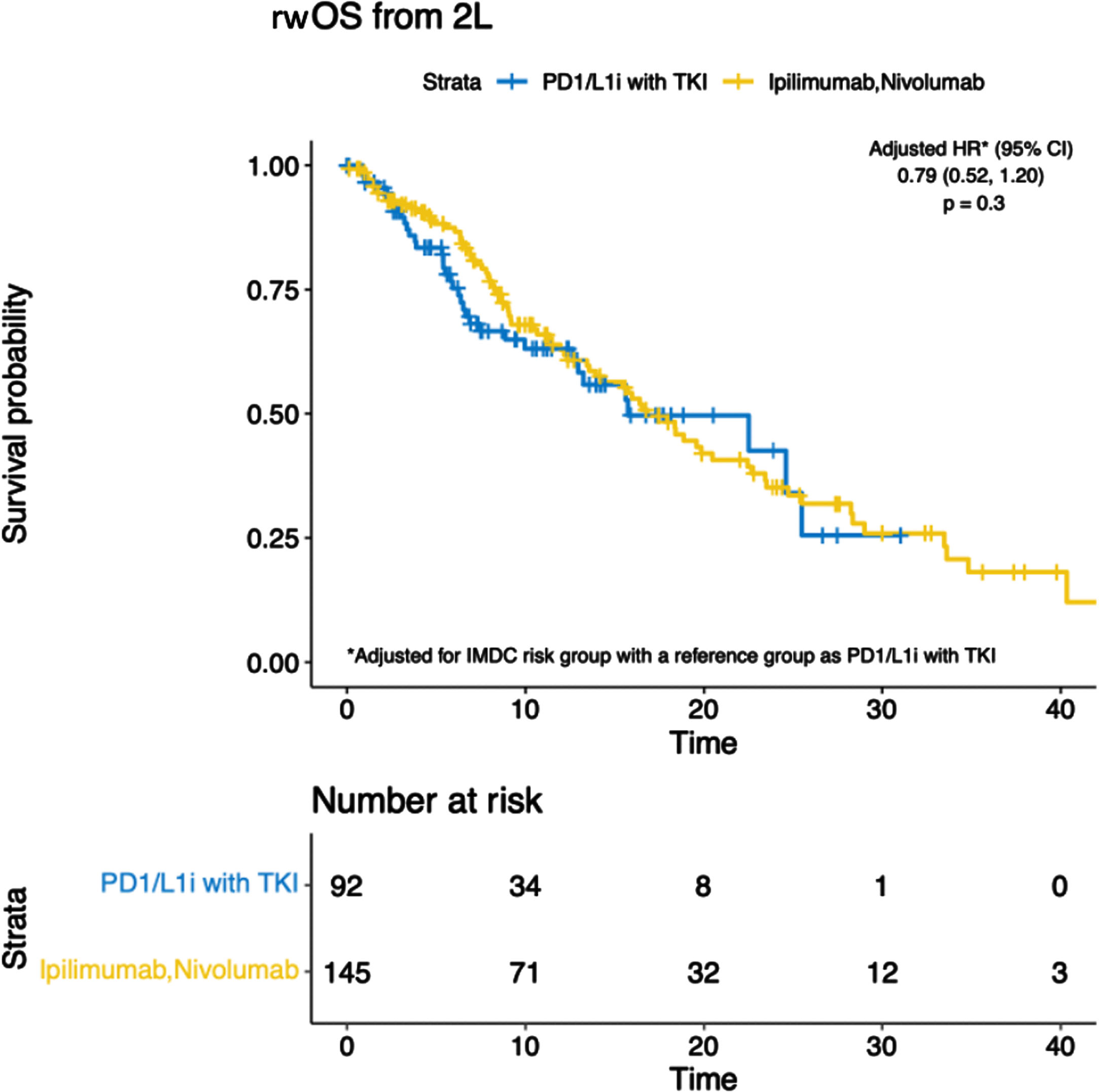
The median rwOS from the start of second-line therapy was 17 months (95% CI 14–23) and 16 months (95% CI 13 – Not reached) for patients treated with IPI + NIVO and PD1/L1i with TKI (ref. group), respectively (HR 0.89, 95% CI 0.59–1.33, p = 0.6). Similarly, rwOS remained similar across both groups on the multivariable analysis (HR 0.79, 95% CI 0.52–1.20, p = 0.3) (Fig. 3).
Fig. 3
Kaplan-Meier curves demonstrating the real-world overall survival (rwOS). Abbreviations: PD1/L1i with TKI: PD1/L1 inhibitor with tyrosine kinase inhibitor. 2L: second-line.
DISCUSSION
In this large real-world study of patients who received cabozantinib in the second line treatment setting, there was no statistical difference in rwTTNT and rwOS between the groups who received IPI + NIVO or PD1/L1i with TKI in the first line treatment setting. This suggests that cabozantinib’s effectiveness is similar as a second line agent, independent of the type of first-line therapy received by the patients.
The BREAKPOINT study was the first phase 2 clinical trial evaluating the effectiveness and safety of cabozantinib in patients with mRCC who previously received adjuvant or first-line ICI-based immunotherapy. The study enrolled 31 patients, 63% receiving IPI + NIVO as first-line therapy, and 26% treated with a PD1/L1i with TKI combination. At a median follow-up of 11.9 months, the median PFS was 8.3 months. The median OS was 13.8 months and 37.9% achieved an objective response rate. The study met its primary endpoint of detecting an increment of the median PFS from 3.8 to 7.4 months, confirming the effectiveness of cabozantinib following progression on first-line ICI therapy [19].
The question of whether the prior receipt of IPI + NIVO versus PD1/L1i with TKI could impact the effectiveness of subsequent cabozantinib has been explored in some previous retrospective studies. A study from the IMDC database indicated that the activity of cabozantinib as a second-line treatment is comparable, irrespective of the type of first-line therapy administered. However, in this study, only 13% (n = 46) of patients progressed on prior PD1/L1i with TKI and 22% (n = 78) on IPI + NIVO. When comparing those two groups, time to treatment failure and OS were similar without statistically significant differences [23]. Another real-world retrospective study that included 86 patients treated with cabozantinib post-ICI progression showed that the 12-month OS rates were 63% for the ICI cohort (which included ICI monotherapy and ICI-ICI combination) and 40% for the PD1/L1i with TKI group, with overlapping confidence intervals, suggesting no statistical difference [17]. These findings align with our study and indicate that the effectiveness of cabozantinib as a second-line therapy remains consistent irrespective of the specific first-line ICI combination utilized. The ongoing prospective phase 2 CABOPOINT trial [NCT03945773] will provide valuable data on the effectiveness of cabozantinib as a second-line treatment in this setting. In the interim analysis of 88 patients at 3-month follow-up, 68.2% of patients were in the IPI + NIVO subgroup and 31.8% in the PD1/L1i with TKI subgroup, the objective response rate was 31.7% and 25.0%, respectively, showing preliminary effectiveness of cabozantinib, regardless of the inclusion of a VEGF TKI in the first-line regimen [24].
In patients who progressed on prior ICI-based combinations, several completed or ongoing clinical trials have investigated the benefits of adding various therapeutic agents to cabozantinib, compared to cabozantinib monotherapy in the second-line treatment setting. For example, the CONTACT-03 trial investigating the addition of atezolizumab to cabozantinib compared to cabozantinib alone, resulted in no additional progression-free survival or OS benefit [25]. Similarly, the phase 3 CANTATA trial aimed to compare the effectiveness and safety of combining a glutaminase inhibitor, telaglenastat, with cabozantinib versus placebo with cabozantinib in patients with mRCC who progressed on either IPI + NIVO or PD1/L1i with TKI. The median PFS was 9.2 months in the telaglenastat with cabozantinib arm, compared to 9.3 months in the placebo with cabozantinib arm, also showing that adding telaglenastat did not enhance the effectiveness of cabozantinib [26].
Currently, the phase 3 LITESPARK 011 [NCT04586231] trial is evaluating the effectiveness and safety of belzutifan, a hypoxia-inducible factor 2 alpha (HIF-2α) inhibitor with lenvatinib compared to cabozantinib monotherapy in patients with mRCC progressing after prior ICI therapy. One study investigated the efficacy of post-lenvatinib therapies in patients with advanced RCC. Results showed modest activity of TKI-based therapy post-lenvatinib, with a need for improved treatment options for patients progressing on lenvatinib-based therapies [27]. In a more upfront approach, PDIGREE [NCT03793166] is an ongoing response-adaptive phase 3 trial that is investigating the benefit of adding cabozantinib to nivolumab versus nivolumab alone in patients who experience partial response or stable disease to first-line IPI + NIVO. This trial will provide additional data on the benefits of administering cabozantinib at an earlier stage of the disease, specifically before the onset of progressive disease on first-line ICI-based combination [28].
Our study is the largest, multicenter, real-world experience reporting the effectiveness of cabozantinib based on the type of first-line contemporary ICI-based combination received. Second-line cabozantinib appears to be associated with similar survival outcomes in patients who received either first-line IPI + NIVO or PD1/L1i with TKI. We acknowledge that the study’s retrospective nature, residual confounding including lack of information regarding metastasis directed therapy and delayed nephrectomy to extend TTNT, the patient and physician preferences, and access to healthcare could limit our study findings.
CONCLUSION
In patients with mRCC who progressed on first-line ICI-based combinations and were treated with second-line cabozantinib monotherapy, there was no evidence found for different survival outcomes whether they progressed on first-line IPI + NIVO versus PD1/L1i with TKI. These results align with the results of prior studies and might assist clinicians in treatment selection, supporting the use of cabozantinib independently of the type of prior ICI-based combination received.
ACKNOWLEDGMENTS
Research reported in this publication utilized cancer biostatistics at Huntsman Cancer Institute at the University of Utah and was supported by the National Cancer Institute of the National Institutes of Health under Award Number P30CA042014. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
FUNDING
National Cancer Institute of the National Institutes of Health under Award Number P30CA042014.
AUTHOR CONTRIBUTIONS
A.N., Y.J., G.G.: Conceptualization, writing original draft, writing-review, and editing; Y.J.: formal analysis, methodology, writing-review and editing, visualization, and software; V.M.T, G.G.F., C.T., N.S., N.T., C.H.C., B.C., B.N., A.S.: Data collection and writing-review and editing; H.L.: writing-review and editing; B.L.M., U.S., N.A.: Conceptualization, data curation, formal analysis, methodology, investigation, supervision, writing-review and editing, visualization, and project administration.
CONFLICTS OF INTEREST
Dr. Agarwal: NA has received honorarium before May 2021 and during his lifetime for consulting to Astellas, AstraZeneca, Aveo, Bayer, Bristol Myers Squibb, Calithera, Clovis, Eisai, Eli Lilly, EMD Serono, Exelixis, Foundation Medicine, Genentech, Gilead, Janssen, Merck, MEI Pharma, Nektar, Novartis, Pfizer, Pharmacyclics, and Seattle Genetics; and NA’s institution has received research funding during his lifetime from Arnivas, Astellas, AstraZeneca, Bavarian Nordic, Bayer, Bristol Meyers Squibb, Calithera, Celldex, Clovis, CRISPR Therapeutics, Eisai, Eli Lilly, EMD Serono, Exelixis, Genentech, Gilead, Glaxo Smith Kline, Immunomedics, Janssen, Lava, Medivation, Merck, Nektar, Neoleukin, New Link Genetics, Novartis, Oric, Pfizer, Prometheus, Rexahn, Roche, Sanofi, Seattle Genetics, Takeda, and Tracon. NA is a member of the editorial board of Kidney Cancer but was not involved in the peer-review process of this paper, nor had access to any information regarding its peer-review.
Umang Swami, MD: US reports consultancy to Astellas, AstraZeneca, Adaptimmune, Exelixis, Gilead, Imvax, Pfizer, Seattle Genetics and Sanofi and research funding to institute from Janssen, Exelixis and Astellas/Seattle Genetics.
Benjamin L. Maughan, MD: BLM has received financial compensation as a paid consultant/advisor to Abbive, Pfizer, AVEO oncology, Janssen, Astellas, Bristol-Myers Squibb, Clovis, Tempus, Merck, Exelixis, Bayer Oncology, Lilly, Sanofi, Telix, Xencor, NCCN and Peloton Therapeutics. Huntsman Cancer Institute has received research funding from Exelixis, Bavarian-Nordic, Clovis and Bristol-Myers Squibb on his behalf.
AN, GB, NJ, VMT, HL, GGF, NS, CT, NT, BC, AS, CHC and BN have no conflicts of interest to report
DATA AVAILABILITY
The data that support the findings of this study have been originated by Flatiron Health, Inc. Requests for data sharing by license or by permission for the specific purpose of replicating results in this manuscript can be submitted to E-mail: .
REFERENCES
[1] | kidney.pdf [Internet]. [cited 2024 Feb 23]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf |
[2] | Motzer RJ , Tannir NM , McDermott DF , et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. (2018) ;378: (14):1277–90. |
[3] | Choueiri TK , Larkin J , Oya M , et al. Preliminary results for avelumab plus axitinib as first-line therapy in patients with advanced clear-cell renal-cell carcinoma (JAVELIN Renal 100): An open-label, dose-finding and dose-expansion, phase 1b trial. Lancet Oncol. (2018) ;19: (4):451–60. |
[4] | Choueiri TK , Powles T , Burotto M , et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2021) ;384: (9):829–41. |
[5] | Motzer R , Alekseev B , Rha SY , et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. (2021) ;384: (14):1289–300. |
[6] | Rini Brian I , Plimack Elizabeth R, Viktor Stus, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. New England Journal of Medicine. (2019) ;380: (12):1116–27. |
[7] | Shaw T , Lee H , Figlin R . Second-Line Therapies in the Changing Landscape of First-Line Therapies for Metastatic Clear Cell Renal Cell Cancer. Oncology (Williston Park). (2021) ;35: (6):306–10. |
[8] | Abdelaziz A , Vaishampayan U . Cabozantinib for the treatment of kidney cancer. Expert Rev Anticancer Ther. (2017) ;17: (7):577–84. |
[9] | Choueiri TK , Escudier B , Powles T , et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): Final results from a randomised, open-label, phase 3 trial. Lancet Oncol. (2016) ;17: (7):917–27. |
[10] | Mennitto A , Huber V , Ratta R , et al. Angiogenesis and Immunity in Renal Carcinoma: Can We Turn an Unhappy Relationship into a Happy Marriage? J Clin Med. (2020) ;9: (4):930. |
[11] | Auvray M , Auclin E , Barthelemy P , et al. Second-line targeted therapies after nivolumab-ipilimumab failure in metastatic renal cell carcinoma. Eur J Cancer. (2019) ;108: :33–40. |
[12] | Albiges L , Fay AP , Xie W , et al. Efficacy of targeted therapies after PD-1/PD-L1 blockade in metastatic renal cell carcinoma. Eur J Cancer. (2015) ;51: (17):2580–6. |
[13] | Nadal R , Amin A , Geynisman DM , et al. Safety and clinical activity of vascular endothelial growth factor receptor (VEGFR)–tyrosine kinase inhibitors after programmed cell death 1 inhibitor treatment in patients with metastatic clear cell renal cell carcinoma. Ann Oncol. (2016) ;27: (7):1304–11. |
[14] | Shah AY , Kotecha RR , Lemke EA , et al. Outcomes of patients with metastatic clear-cell renal cell carcinoma treated with second-line VEGFR-TKI after first-line immune checkpoint inhibitors. Eur J Cancer. (2019) ;114: :67–75. |
[15] | Dudani S , Graham J , Wells JC , et al. First-line Immuno-Oncology Combination Therapies in Metastatic Renal-cell Carcinoma: Results from the International Metastatic Renal-cell Carcinoma Database Consortium. Eur Urol. (2019) ;76: (6):861–7. |
[16] | Ornstein MC , Pal SK , Wood LS , et al. Individualised axitinib regimen for patients with metastatic renal cell carcinoma after treatment with checkpoint inhibitors: A multicentre, single-arm, phase 2 study. Lancet Oncol. (2019) ;20: (10):1386–94. |
[17] | McGregor BA , Lalani AKA , Xie W , et al. Activity of cabozantinib after immune checkpoint blockade in metastatic clear-cell renal cell carcinoma. Eur J Cancer. (2020) ;135: :203–10. |
[18] | Gan CL , Dudani S , Wells JC , et al. Cabozantinib real-world effectiveness in the first-through fourth-line settings for the treatment of metastatic renal cell carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium. Cancer Med. (2021) ;10: (4):1212–21. |
[19] | Procopio G , Claps M , Pircher C , et al. A multicenter phase 2 single arm study of cabozantinib in patients with advanced or unresectable renal cell carcinoma pre-treated with one immune-checkpoint inhibitor: The BREAKPOINT trial (Meet-Uro trial 03). Tumori. (2023) ;109: (1):129–37. |
[20] | Ma X , Long L , Moon S , et al. Comparison of Population Characteristics in Real-World Clinical Oncology Databases in the US: Flatiron Health, SEER, and NPCR [Internet]. medRxiv; 2020 [cited 2024 Mar 2]. p. 2020.03.16.20037143. Available from: https://www.medrxiv.org/content/10.1101/2020.03.16.20037143v2 |
[21] | Birnbaum B , Nussbaum N , Seidl-Rathkopf K , et al. Model-assisted cohort selection with bias analysis for generating large-scale cohorts from the EHR for oncology research [Internet]. arXiv; 2020 [cited 2024 Mar 2]. Available from: http://arxiv.org/abs/2001.09765 |
[22] | IMDC (International Metastatic RCC Database Consortium) Risk Model for Metastatic Renal Cell Carcinoma [Internet]. [cited 2024 Mar 9]. Available from: https://www.mdcalc.com/calc/3008/imdc-international-metastatic-rcc-database-consortium-risk-model-metastatic-renal-cell-carcinoma |
[23] | Navani V , Wells JC , Boyne DJ , et al. CABOSEQ: The Effectiveness of Cabozantinib in Patients With Treatment Refractory Advanced Renal Cell Carcinoma: Results From the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC). Clin Genitourin Cancer. (2023) ;21: (1):106.e1–106.e8. |
[24] | Albiges L , Powles T , Sharma A , et al. CaboPoint: Interim results from a phase 2 study of cabozantinib after checkpoint inhibitor (CPI) therapy in patients with advanced renal cell carcinoma (RCC). JCO. (2023) ;41: (6_suppl):606. |
[25] | Pal SK , Albiges L , Tomczak P , et al. Atezolizumab plus cabozantinib versus cabozantinib monotherapy for patients with renal cell carcinoma after progression with previous immune checkpoint inhibitor treatment (CONTACT-03): a multicentre, randomised, open-label, phase 3 trial. Lancet. (2023) ;402: (10397):185–95. |
[26] | Tannir NM , Agarwal N , Porta C , et al. Efficacy and Safety of Telaglenastat Plus Cabozantinib vs Placebo Plus Cabozantinib in Patients With Advanced Renal Cell Carcinoma: The CANTATA Randomized Clinical Trial. JAMA Oncology. (2022) ;8: (10):1411–8. |
[27] | Panian J , Zhong C , Choi S , et al. Efficacy of post-lenvatinib treatments in patients (pts) with advanced renal cell carcinoma (aRCC). JCO. (2024) ;42: (16_suppl):4538. |
[28] | Zhang T , Ballman KV , Choudhury AD , et al. PDIGREE: An adaptive phase III trial of PD-inhibitor nivolumab and ipilimumab (IPI-NIVO) with VEGF TKI cabozantinib (CABO) in metastatic untreated renal cell cancer (Alliance A04). JCO. (2020) ;38: (6_suppl):TPS760. |


