
Real-World Outcomes in Patients with Advanced/Metastatic Renal Cell Carcinoma Receiving Cabozantinib or Other Tyrosine Kinase Inhibitors After Checkpoint Inhibitor-Based Therapy
Abstract
BACKGROUND:
Checkpoint inhibitor (CPI)-based therapy is recommended for first-line treatment of advanced/metastatic renal cell carcinoma (mRCC). Cabozantinib is a tyrosine kinase inhibitor (TKI) approved in the USA for treating mRCC, including after CPI-based therapy. However, data on the benefits of subsequent TKI therapy are limited.
OBJECTIVE:
To study the real-world use and outcomes of cabozantinib versus other TKIs after CPI-based therapy for mRCC.
METHODS:
This retrospective study used data from the US Oncology Network electronic health record database supplemented by chart review. Patients initiated TKI therapy between 2016 and 2021 after CPI-based therapy. The primary endpoint was real-world response rate in the first 6 months of treatment (RR-6m; physician assessment). Secondary endpoints included overall response rate (ORR), progression-free survival (PFS) and overall survival (OS). Covariates were adjusted by inverse probability of treatment weighting.
RESULTS:
Of 485 included patients, 331 received cabozantinib and 154 another TKI. Baseline characteristics were generally similar between arms. For cabozantinib versus other TKIs, adjusted RR-6m (available for 69.3% of patients) was 62.5% versus 46.0% (rate difference: superiority, 16.5% [95% CI: 7.8–25.1], p = 0.0002), adjusted ORR was 62.4% versus 49.4% (p = 0.0020), adjusted median OS was 19.2 versus 19.1 months (p = 0.7353) and adjusted median PFS was 7.9 versus 9.2 months (p = 0.8752).
CONCLUSIONS:
Cabozantinib following CPI-based therapy was effective for treating mRCC in the US real-world setting. Differences in adjusted RR-6m and ORR significantly favored cabozantinib versus other TKIs. The lack of OS difference may reflect differences in post-index therapy.
INTRODUCTION
Significant advances in the therapeutic management of advanced/metastatic renal cell carcinoma (mRCC), including the introduction of vascular endothelial growth factor receptor (VEGFR)-targeted tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (CPIs), have contributed to declining RCC mortality despite increasing incidence [1–3]. CPI-based combination therapy is now recommended as a front-line standard of care in mRCC clinical guidelines [4, 5]. Ipilimumab plus nivolumab was the first CPI-based combination to be approved by the Food and Drug Administration (FDA), the European Medicines Agency (EMA) and Health Canada for the treatment of patients with intermediate- or poor-risk mRCC [6–8]. Between 2018 and 2020, ipilimumab plus nivolumab accounted for 36–47% of first-line (1L) mRCC therapy in the USA [9]. While the use of ipilimumab plus nivolumab is restricted to patients with intermediate- or poor-risk disease, several TKI–CPI combinations are now indicated as 1L mRCC therapies across all risk categories, including pembrolizumab plus axitinib, nivolumab plus cabozantinib and pembrolizumab plus lenvatinib [4, 5].
CPI and VEGFR TKI monotherapies also play an important role in the mRCC treatment landscape, with clinical guidelines generally recommending their use after 1L treatment [4, 5]. Cabozantinib is a multi-targeted TKI with activity against tyrosine kinases including MET, VEGFR-1-3 and AXL [10]. In the USA, cabozantinib monotherapy is indicated for the treatment of adults with advanced RCC; in Canada and Europe, it is approved for the 1L treatment of adults with intermediate- or poor-risk advanced RCC, or for≥second-line (2L) treatment following prior VEGF-targeted therapy [10–12].
Prospective data on the use of VEGFR TKIs, including cabozantinib, after CPI-based therapy remain limited [13–19]. BREAKPOINT was one of a few clinical trials to assess cabozantinib following CPI-based therapy. This open-label, phase 2 trial showed that 2L cabozantinib was active in patients with mRCC who had received prior CPI-based therapy, with a median progression-free survival (PFS) of 8.3 months (N = 30) [19]. In addition to limited clinical trial data, the feasibility of retrospective, real-world analyses of cabozantinib use after 1L CPI-based therapy is restricted by the variations in the approved use of cabozantinib in different regions [10–12].
Recent systematic literature reviews of the available evidence for cabozantinib use after CPI-based therapy in patients with mRCC report consistent antitumor activity and real-world effectiveness of cabozantinib, regardless of treatment line [20, 21]. Conversely, emerging data suggest that prior therapy may influence subsequent TKI effectiveness [15]. In this context, our objective was to study the real-world use and outcomes of cabozantinib versus other VEGFR TKIs in patients with mRCC who had received prior CPI-based therapy.
METHODS
We performed a retrospective, observational study of patients with mRCC who initiated index treatment (cabozantinib or other TKI therapy) after prior CPI therapy, in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The Institutional Review Board approved a waiver for informed consent and authorized the study; exemption status was approved before the initiation of retrospective data extraction and analysis. This study used only anonymized secondary data.
Data sources
Study data were primarily derived from the US Oncology Network (USON) electronic health record (EHR) system, iKnowMed (iKM), which captures patient demographics, clinical information and treatment information for patients receiving community-based care in the USA. Structured EHR data were supplemented by unstructured data collected through chart review by healthcare professionals with oncology experience. For elements captured by both iKM and chart review, data were compared to identify differences between sources, with chart review data taking precedence. The Limited Access Death Master File and publicly available obituary databases were used to capture death data.
Study design
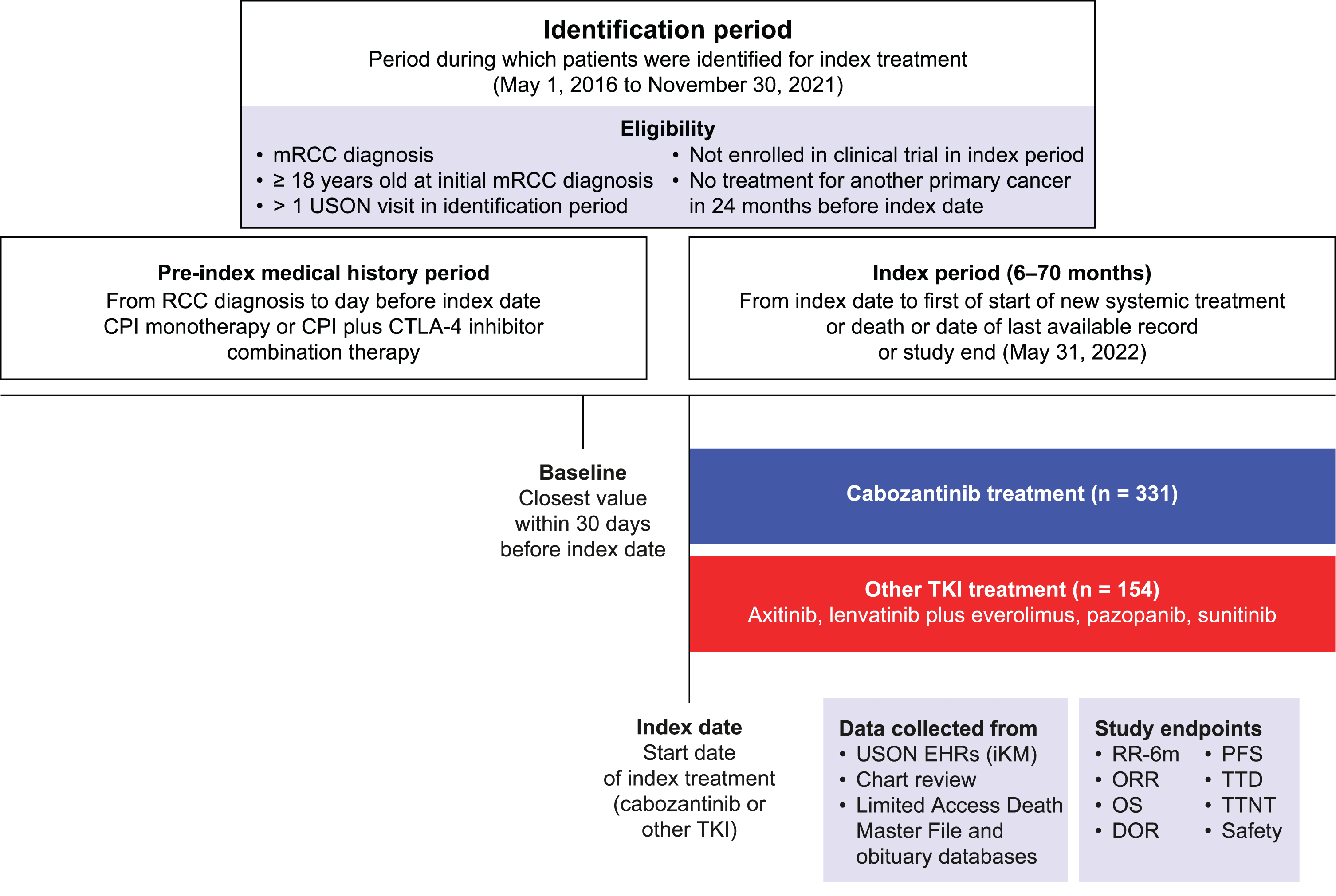
The study period ran from May 1, 2016 to May 31, 2022 and comprised an identification period for eligible patient identification (May 1, 2016 to November 30, 2021), an index date at which eligible patients initiated cabozantinib or other TKI therapy and an index period (from index date to the first of: start of new systemic treatment, death, date of last available record or study end) during which eligible patients received cabozantinib or other TKI therapy (Fig. 1). Patients were followed until the end of the observation period (May 31, 2022) or the date of last record, allowing a minimum of 6 months follow-up.
Fig. 1
Study design. CPI, checkpoint inhibitor; DOR, duration of response; EHR, electronic health record; iKM, iKnowMed; mRCC, advanced/metastatic renal cell carcinoma; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; RR-6m, response rate in the first 6 months of treatment; TKI, tyrosine kinase inhibitor; TTD, time to discontinuation; TTNT, time to next treatment; USON, US Oncology Network.
Study population
Patients who met the following criteria were included: a documented diagnosis of mRCC; aged≥18 years old at initial mRCC diagnosis; more than one recorded healthcare contact within USON during the identification period; receipt of prior CPI monotherapy (atezolizumab, avelumab, pembrolizumab, nivolumab) or CPI plus CTLA-4 inhibitor combination therapy (ipilimumab plus nivolumab); and initiation of cabozantinib or another TKI therapy as their next treatment after their CPI-based regimen during the identification period.
Patients were excluded if they had been enrolled in a clinical trial at any time during the index period or had received treatment for another documented primary cancer diagnosis during the 24-month period before the index date.
Endpoints
Because this was a real-world study, all endpoints were assessments of real-world treatment response.
Primary endpoint
The primary endpoint was response rate (complete or partial response) in the first 6 months of treatment (RR-6m) among patients receiving cabozantinib versus other TKIs. RR-6m was based on physician-documented assessment of response. Response assessments were captured by chart review, with no attempts made to mimic Response Evaluation Criteria in Solid Tumors (RECIST) assessment guidelines. Tumor response assessments documented during the study observation period were abstracted and classified by healthcare professionals trained in medical data extraction. Based on chart review, a complete response was defined as the patient being in remission, that all lesions had disappeared or that there was no evidence of the disease. Partial response was defined as improved or responding disease. Mixed response was defined as a combination of improved and worsened disease (different results in different lesions). Stable disease was defined as the disease being stable, not progressed or not improved. Progressive disease was defined as the disease having ‘progressed’, worsened, relapsed or recurred.
Secondary endpoints
Secondary endpoints included: overall response rate (ORR) in the full index period; duration of response in the index period only (DOR; defined as the time between first documented tumor response to the date of documented progression); PFS (defined as the time from index date to the earliest date of progression or death owing to any cause during the index period only, not including events occurring during subsequent therapy); overall survival (OS; defined as the time between index treatment initiation and date of death); time to next treatment (TTNT; measured from the initiation of index treatment to the start date of the next treatment); time to treatment discontinuation (TTD; the time from index treatment initiation to discontinuation, defined as a treatment interruption of more than 40 days, or the start of a new treatment); baseline demographics and clinical characteristics; and safety/tolerability, including dose reduction, treatment discontinuation, discontinuation owing to adverse events (AEs), rate and reason for hospitalization and AEs.
Statistical analysis
All statistical analyses were performed using SAS® version 9.4 (SAS Institute, Inc., Cary, NC, USA) and R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna, Austria).
Primary endpoint
The primary endpoint analysis tested the non-inferiority of cabozantinib versus other TKIs based on RR-6m. RR-6m was reported for each index treatment group and compared using a Chi-square test. Non-inferiority was assessed using a 90% confidence interval (CI) approach with a non-inferiority margin of 10%. Cabozantinib was considered non-inferior to other TKIs if the lower bound of the 2-sided 90% CI of the difference (cabozantinib – other TKIs) in the proportion of responder patients was greater than –10%. As per FDA guidance on the conduct of non-inferiority studies [22], the non-inferiority margin was set at half of the clinically significant difference between treatment groups. A margin of 10% was selected based on the METEOR study, which demonstrated an ORR of 22% with cabozantinib in a small subgroup of patients who had received prior CPI therapy [14]. Non-inferiority testing could be switched to superiority testing if the lower bound of the 90% CI for the treatment effect lay above –10%. In this instance, a p value associated with a test of superiority was provided. No multiplicity argument affected this interpretation because, in statistical terms, it equates to a simple closed test procedure.
Propensity scores were calculated for each patient based on a generalized boosting model that included the following covariates: age, sex, index treatment start year, time from mRCC diagnosis to index date, stage at diagnosis, history of nephrectomy, number of prior systemic treatments before index, type of CPI therapy prior to index, duration of prior CPI therapy, count of metastatic site(s) at index, reason for CPI therapy discontinuation and International mRCC Database Consortium (IMDC)/Memorial Sloan Kettering Cancer Center (MSKCC) composite score (covariates including missing values without data imputations were balanced between groups). Propensity scores were then used by inverse probability of treatment weighting (IPTW) for covariate adjustment between the cabozantinib and other TKI arms. Adjusted and unadjusted data are presented for RR-6m and ORR.
The IMDC/MSKCC composite score was based on the combination of individual IMDC and MSKCC risk categories. If a patient was missing only one score, the other documented score was used. If a patient had both IMDC and MSKCC scores, the more favorable score was used. If a patient did not have either IMDC or MSKCC scores, the score was considered missing. Patients with no risk factors documented in the EHR were categorized as having favorable risk, those with 1–2 documented risk factors as having intermediate risk and those with 3 or more documented risk factors as having poor risk.
Secondary endpoints
ORR was analyzed using a similar methodology to that for the primary endpoint analysis. Time-to-event outcomes, including DOR, PFS, OS, TTNT and TTD, were assessed using the IPTW-adjusted Kaplan–Meier plots, and IPTW-adjusted hazard ratio (HR) were calculated with Cox’s proportional hazard models. Other secondary outcomes were analyzed by descriptive statistics and reported for each treatment arm. No multiplicity adjustments were performed; all secondary endpoint analyses were hypothesis generating.
Sample size
Based on the feasibility assessment, 618 participants (421 for cabozantinib and 197 for non-cabozantinib TKI) were estimated for inclusion, which would provide a power of 85.5% (using a one-sided alpha of 0.05) to reject the null hypothesis of RR-6m lower than 12% in favor of an alternative hypothesis of RR-6m greater or equal to 12%, which correspond to the minimal acceptable RR-6m according to the non-inferiority margin of 10% and the observed ORR of 22%. This sample size was not reached owing to limited availability of data.
RESULTS
Demographics and clinical characteristics
Overall, 485 patients met the study inclusion criteria. Of these, 331 patients received cabozantinib, while 154 received another TKI as index treatment (axitinib, n = 58; lenvatinib plus everolimus, n = 25; pazopanib, n = 49; sunitinib, n = 22).
Mean (standard deviation [SD]) age was 66 (10.7) years, 74% were male and 42% had IMDC intermediate- or poor-risk disease, while 54% of patients had missing IMDC data. Of those with available data (n = 223), 67% and 25% had intermediate- and poor-risk disease, respectively. Baseline demographics and disease characteristics were generally similar between treatment arms (Table 1). Prior to IPTW, there were significant differences with regard to IMDC/MSKCC composite score, type of CPI therapy prior to index, duration of prior CPI therapy and time from mRCC diagnosis to the index date. After IPTW, there were no significant differences between the two groups for these variables (p > 0.2 for all).
Table 1
Demographics and characteristics at initiation of index therapy
| Cabozantinib (n = 331) | Other TKI (n = 154) | Overall (N = 485) | |
| Age, years, mean (SD) | 65.9 (10.5) | 67.2 (11.0) | 66.3 (10.7) |
| Sex, male, n (%) | 241 (72.8) | 116 (75.3) | 357 (73.6) |
| IMDC risk, n (%) | |||
| Poor | 44 (13.3) | 12 (7.8) | 56 (11.5) |
| Intermediate | 105 (31.7) | 45 (29.2) | 150 (30.9) |
| Favorable | 14 (4.2) | 3 (1.9) | 17 (3.5) |
| Missing | 168 (50.8) | 94 (61.0) | 262 (54.0) |
| MSKCC risk, n (%) | |||
| Poor | 56 (16.9) | 13 (8.4) | 69 (14.2) |
| Intermediate | 112 (33.8) | 49 (31.8) | 161 (33.2) |
| Favorable | 13 (3.9) | 1 (0.6) | 14 (2.9) |
| Missing | 150 (45.3) | 91 (59.1) | 241 (49.7) |
| Composite IMDC/MSKCC score, n (%) | |||
| Poor | 45 (13.6) | 9 (5.8) | 54 (11.1) |
| Intermediate | 121 (36.6) | 51 (33.1) | 172 (35.5) |
| Favorable | 15 (4.5) | 3 (1.9) | 18 (3.7) |
| Missing | 150 (45.3) | 91 (59.1) | 241 (49.7) |
| Number of metastatic site(s) at initiation of index treatment, n (%) | |||
| 0 | 1 (0.3) | 1 (0.6) | 2 (0.4) |
| 1 | 83 (25.1) | 48 (31.2) | 131 (27.0) |
| ≥2 | 247 (74.6) | 105 (68.2) | 352 (72.6) |
| Distant metastatic sites, n (%) | |||
| Bone | 149 (45.0) | 67 (43.5) | 216 (44.5) |
| Brain | 29 (8.8) | 11 (7.1) | 40 (8.2) |
| Liver | 60 (18.1) | 30 (19.5) | 90 (18.6) |
| Lung | 116 (35.0) | 68 (44.2) | 184 (37.9) |
| Lymph nodes | 128 (38.7) | 49 (31.8) | 177 (36.5) |
| Other | 143 (43.2) | 73 (47.4) | 216 (44.5) |
| Prior nephrectomy, n (%) | |||
| Yes | 238 (71.9) | 108 (70.1) | 346 (71.3) |
| Time from mRCC diagnosis to first systemic mRCC therapy, mo | |||
| Median (95% CI) | 1.2 (1.1–1.5) | 1.1 (0.9–1.4) | 1.2 (1.1–1.4) |
| Index treatment line, n (%) | |||
| 2L | 107 (32.3) | 56 (36.4) | 163 (33.6) |
| 3L | 154 (46.5) | 74 (48.1) | 228 (47.0) |
| ≥4L | 70 (21.1) | 24 (15.6) | 94 (19.4) |
| Follow-up from TKI initiation, mo | |||
| Median (95% CI) | 13.2 (11.4–15.2) | 12.4 (10.2–16.7) | 13.1 (11.5–14.3) |
2L, second line; 3L, third line; 4L, fourth line; CI, confidence interval; IMDC, International mRCC Database Consortium; mo, months; mRCC, advanced/metastatic renal cell carcinoma; MSKCC, Memorial Sloan-Kettering Cancer Center; RCC, renal cell carcinoma; SD, standard deviation; TKI, tyrosine kinase inhibitor.
Treatment sequence
With regard to CPI therapy prior to index treatment, 64.1% of patients had received nivolumab, 33.4% ipilimumab plus nivolumab and 2.5% pembrolizumab (Fig. 2). Among those receiving index treatment as their 2L of therapy (n = 163; 33.6%), 76.7% had received ipilimumab plus nivolumab, 19.0% had received nivolumab and 4.3% had received pembrolizumab for 1L treatment. Among those receiving index treatment as their third line of therapy (n = 228; 47.0%), 86.0% had received nivolumab, 12.7% had received ipilimumab plus nivolumab and 1.3% had received pembrolizumab for 2L treatment.
Fig. 2
Sankey diagram of treatment sequence. 1L, first line; 2L, second line; 3L, third line; CPI, checkpoint inhibitor; mTOR, mammalian target of rapamycin; TKI, tyrosine kinase inhibitor.
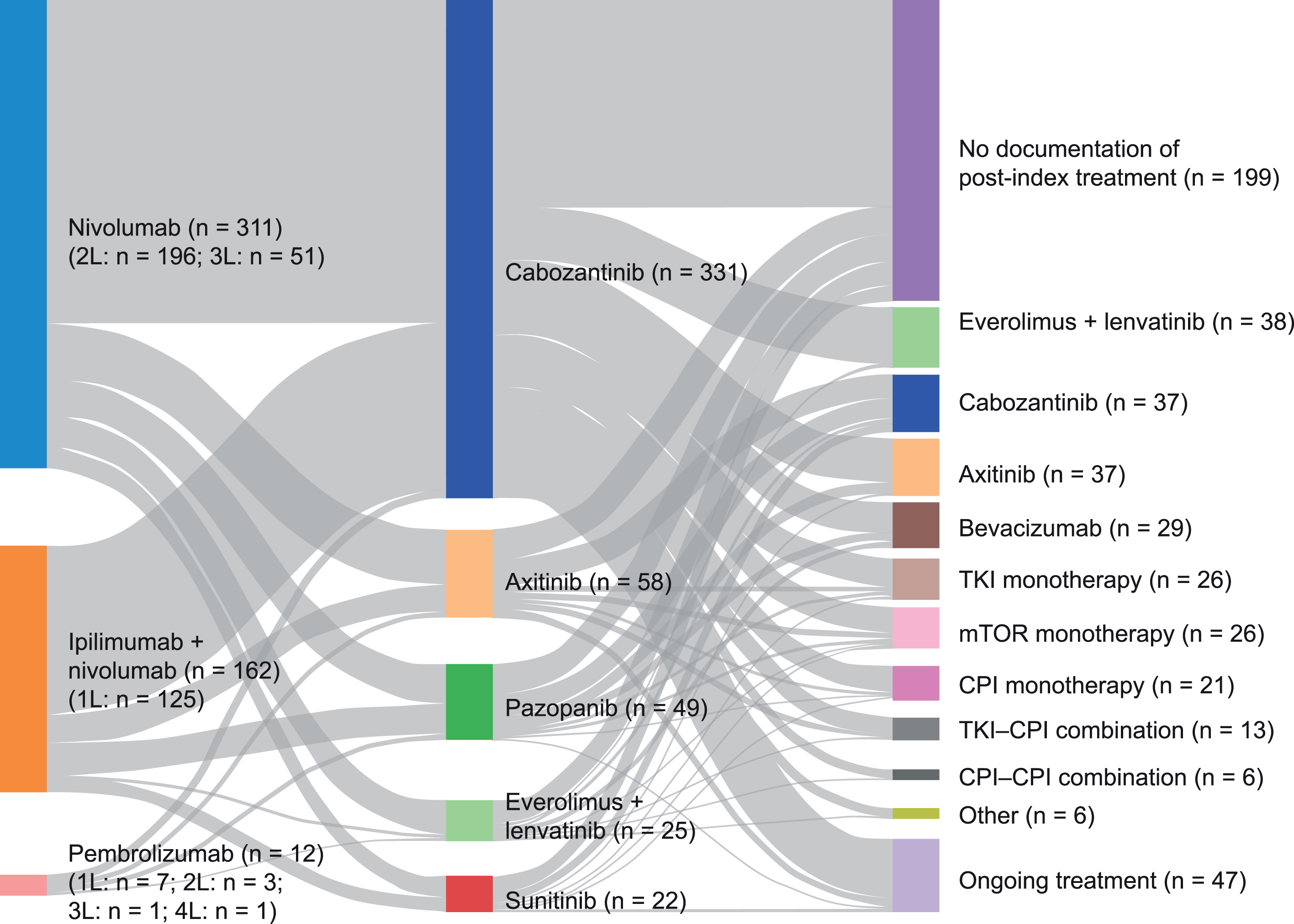
Overall, 41.0% of patients had no documentation of post-index treatment (Fig. 2).
Effectiveness
Primary endpoint: RR-6m
At the 6-month time point, 69.3% of patients (336/485) had tumor response data available (cabozantinib arm, 73.7% ; other TKI arm, 59.7%). Non-inferiority was met for RR-6m and cabozantinib was superior to other TKIs in both the unadjusted analysis and the analysis adjusted for potential confounders (Table 2). Adjusted RR-6m was 62.5% and 46.0% for patients receiving cabozantinib and other TKIs, respectively (rate difference: superiority, 16.5% [95% CI: 7.8–25.1], p = 0.0002).
Table 2
Response rate at 6 months
| Unadjusted | Adjusted | |||
| Cabozantinib | Other TKIs | Cabozantinib | Other TKIs | |
| Patients with evaluable responses | 244 | 92 | 322.3a | 206.0a |
| Patients with no post-index tumor assessment during the first 6 months of the index period, n (%) | 87 (26.3) | 62 (40.3) | – | – |
| RR-6m, n (%)b | 153 (62.7) | 43 (46.7) | 201.3 (62.5) | 94.8 (46.0) |
| Rate difference (90% CI [non-inferiority]) | 16.0% (6.3–25.7); | 16.5% (9.3–23.7); | ||
| p < 0.0001 | p < 0.0001 | |||
| Rate difference (95% CI [superiority])c | 16.0% (4.1–27.8); | 16.5% (7.8–25.1); | ||
| p = 0.0081 | p = 0.0002 | |||
| BOR-6 m, n (%) | ||||
| Complete response | 3 (1.2) | 0 | 4.3 (1.3) | 0 |
| Partial response | 150 (61.5) | 43 (46.7) | 197 (61.1) | 94.8 (46.0) |
| Stable disease | 36 (14.8) | 21 (22.8) | 45.6 (14.2) | 48.1 (23.3) |
| Mixed responsed | 7 (2.9) | 5 (5.4) | 9.2 (2.8) | 14.4 (7.0) |
| Progressive disease | 48 (19.7) | 23 (25.0) | 66.2 (20.5) | 48.8 (23.7) |
aCounts were weighted by IPTW; bProportion of the final study population with at least one complete or partial response; cWhen the lower bound CI exceeded the 10% non-inferiority margin (Δ= –10%), superiority testing was performed; dCombination of improved and worsened disease (different results in different lesions). BOR-6 m, best overall response at 6 months; CI, confidence interval; IPTW, inverse probability of treatment weighting; RR-6m, response rate in the first 6 months of treatment; TKI, tyrosine kinase inhibitor.
In a preplanned subgroup analysis of 125 patients who had received 1L ipilimumab plus nivolumab (prior to cabozantinib for 87 patients and prior to other TKIs for 38 patients), cabozantinib was non-inferior to other TKIs for adjusted RR-6m. Adjusted RR-6m was 58.2% and 49.2% for patients receiving cabozantinib and other TKIs, respectively (rate difference: non-inferiority, 9.0% [90% CI: –5.6 to 23.6], p = 0.0159; superiority, 9.0% [95% CI: –8.5 to 26.6], p = 0.3141).
A total of 163 patients received index treatment as 2L therapy (cabozantinib, n = 107; other TKIs, n = 56). In the preplanned analysis of adjusted RR-6m for this subgroup, cabozantinib was non-inferior to other 2L therapies (55.8% vs 48.4% ; rate difference: 7.4% [90% CI –5.6 to 20.3], p = 0.0137; Supplementary Table S1).
Secondary endpoints
ORR. ORR data for the index period were available for 75.5% of patients (366/485) (cabozantinib arm, 79.8% ; other TKI arm, 66.2%). ORR was statistically significantly higher among patients receiving cabozantinib compared with those receiving other TKIs, irrespective of adjustment (Table 3). Adjusted real-world ORR was 62.4% in the cabozantinib arm and 49.4% in the other TKI arm (rate difference: superiority, 13.0% [95% CI: 4.8–21.1], p = 0.0020).
Table 3
Overall response rate during the index period
| Unadjusted | Adjusted | |||
| Cabozantinib | Other TKIs | Cabozantinib | Other TKIs | |
| Patients with evaluable responses | 264 | 102 | 349.5a | 232.3a |
| Patients with no post-index tumor assessment during the index period, n (%) | 67 (20.2) | 52 (33.8) | – | – |
| ORR, n (%)b | 165 (62.5) | 52 (51.0) | 218.0 (62.4) | 114.8 (49.4) |
| Rate difference (90% CI [non-inferiority]) | 11.5% (2.3–20.7); | 13.0% (6.1–19.8); | ||
| p < 0.0001 | p < 0.0001 | |||
| Rate difference (95% CI [superiority])c | 11.5% (0.2–22.8); | 13.0% (4.8–21.1); | ||
| p = 0.0443 | p = 0.0020 | |||
| BOR, n (%) | ||||
| Complete response | 8 (3.0) | 2 (2.0) | 11.1 (3.2) | 3.1 (1.4) |
| Partial response | 157 (59.5) | 50 (49.0) | 206.9 (59.2) | 111.7 (48.1) |
| Stable disease | 39 (14.8) | 20 (19.6) | 48.6 (13.9) | 52.7 (22.7) |
| Mixed responsed | 7 (2.7) | 4 (3.9) | 9.2 (2.6) | 9.2 (4.0) |
| Progressive disease | 53 (20.1) | 26 (25.5) | 73.7 (21.1) | 55.6 (23.9) |
aCounts were weighted by IPTW; bProportion of the final study population with at least one complete or partial response; cWhen the lower bound CI exceeded the 10% non-inferiority margin (Δ= –10%), superiority testing was performed; dCombination of improved and worsened disease (different results in different lesions). BOR, best overall response; CI, confidence interval; IPTW, inverse probability of treatment weighting; ORR, overall response rate; TKI, tyrosine kinase inhibitor.
In the preplanned analysis of the 1L ipilimumab plus nivolumab subgroup, the adjusted real-world ORR was 62.4% for cabozantinib (n = 69) and 54.3% for other TKIs (n = 25) (rate difference: non-inferiority, 8.1% [90% CI: –5.6 to 21.8], p = 0.0151; superiority, 8.1% [95% CI: –8.5 to 24.7], p = 0.3386).
In the 2L TKI subgroup, adjusted ORR was non-inferior for cabozantinib versus other TKIs (59.2% vs. 52.9% ; rate difference: non-inferiority, 6.3% [90% CI: –6.0 to 18.7], p = 0.0146; Supplementary Table S1).
DOR. There was no significant difference in median DOR for patients in the cabozantinib arm versus those in the other TKI arm in both the unadjusted (n = 165 vs. n = 52, respectively) and adjusted (n = 218 vs. n = 115, respectively [weighted]) analyses (Supplementary Fig. S1). Adjusted median DOR was 8.1 months and 9.3 months (HR 1.19 [95% CI: 0.89–1.59]; p = 0.4171) for cabozantinib and other TKIs, respectively.
Among patients who received 2L TKI therapy, adjusted median DOR was not significantly different with 2L cabozantinib than with other 2L TKIs (9.2 months vs. 10.6 months; log-rank p = 0.3900; Supplementary Table S1).
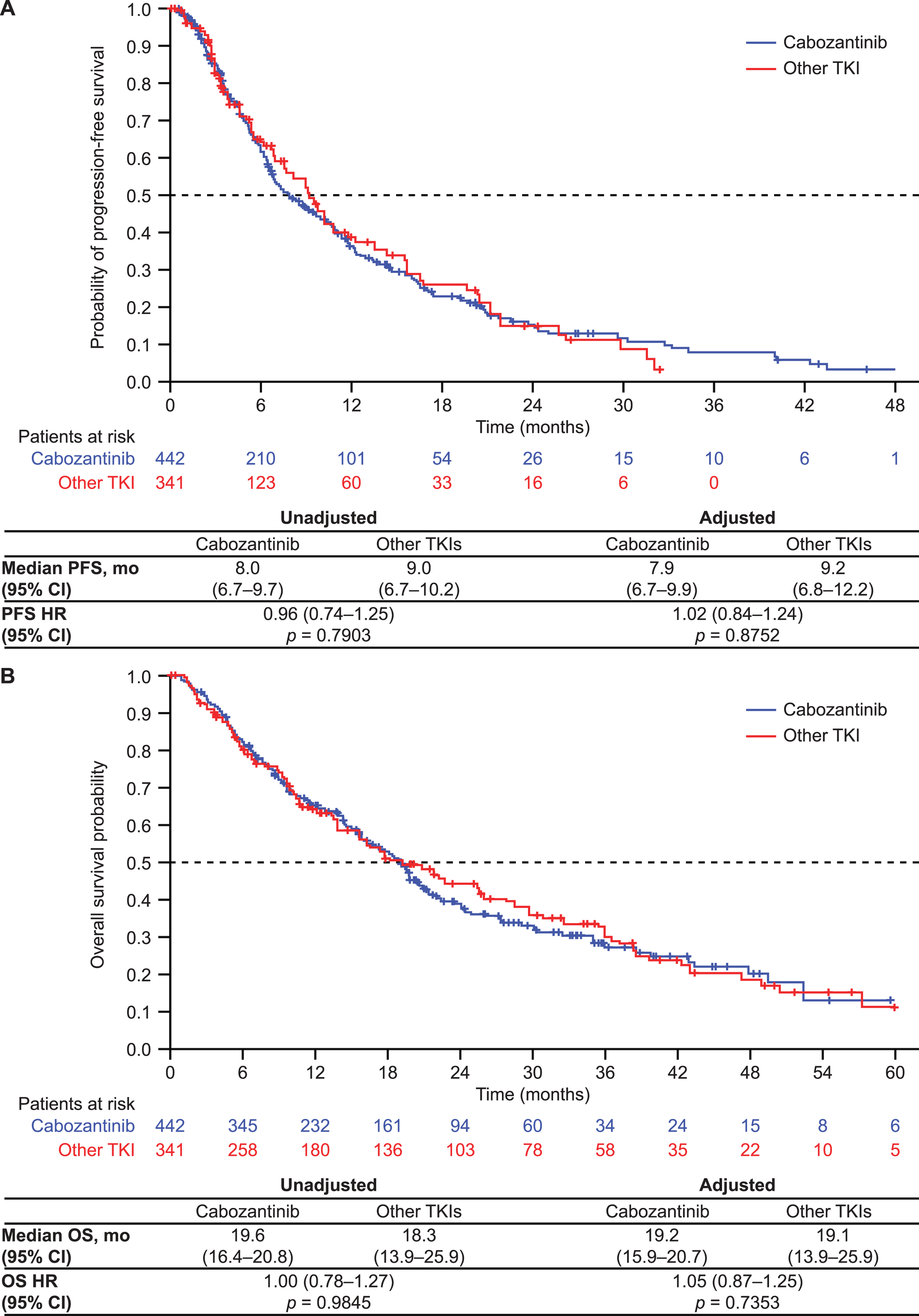
PFS. There was no significant difference in median PFS (during the index period) for patients receiving cabozantinib versus other TKIs in both the unadjusted and adjusted analyses (Fig. 3A). Adjusted median PFS was 7.9 months and 9.2 months (HR 1.02 [95% CI: 0.84–1.24]; p = 0.8752) for cabozantinib and other TKIs, respectively.
Fig. 3
IPTW-adjusted progression-free survival (A) and overall survival (B). CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; mo, months; OS, overall survival; PFS, progression-free survival; TKI, tyrosine kinase inhibitor.
Adjusted median PFS was not significantly different with 2L cabozantinib than with other 2L TKIs (9.6 months vs. 8.2 months; log-rank p = 0.3407; Supplementary Table S1).
OS. Median OS was similar for cabozantinib and other TKIs in both the unadjusted and adjusted analyses (Fig. 3B). Adjusted median OS was 19.2 months and 19.1 months (HR 1.05 [95% CI: 0.87–1.25]; p = 0.7353) for cabozantinib and other TKIs, respectively.
In the 2L TKI subgroup, adjusted median OS was not significantly different with 2L cabozantinib than with other 2L TKIs (19.4 months vs. 16.3 months; log-rank p = 0.5065; Supplementary Table S1).
TTNT. Median TTNT was numerically, but not statistically significantly, longer in the cabozantinib arm than in the other TKI arm in both the unadjusted (n = 155 vs. n = 84, respectively) and adjusted (n = 206 vs. n = 191, respectively [weighted]) analyses (Fig. 4A). Adjusted median TTNT was 7.1 months and 5.6 months (p = 0.0607) for cabozantinib and other TKIs, respectively.
Fig. 4
IPTW-adjusted time to next treatment (A) and time to discontinuation (B). CI, confidence interval; HR, hazard ratio; IPTW, inverse probability of treatment weighting; mo, months; TKI, tyrosine kinase inhibitor; TTD, time to discontinuation; TTNT, time to next treatment.
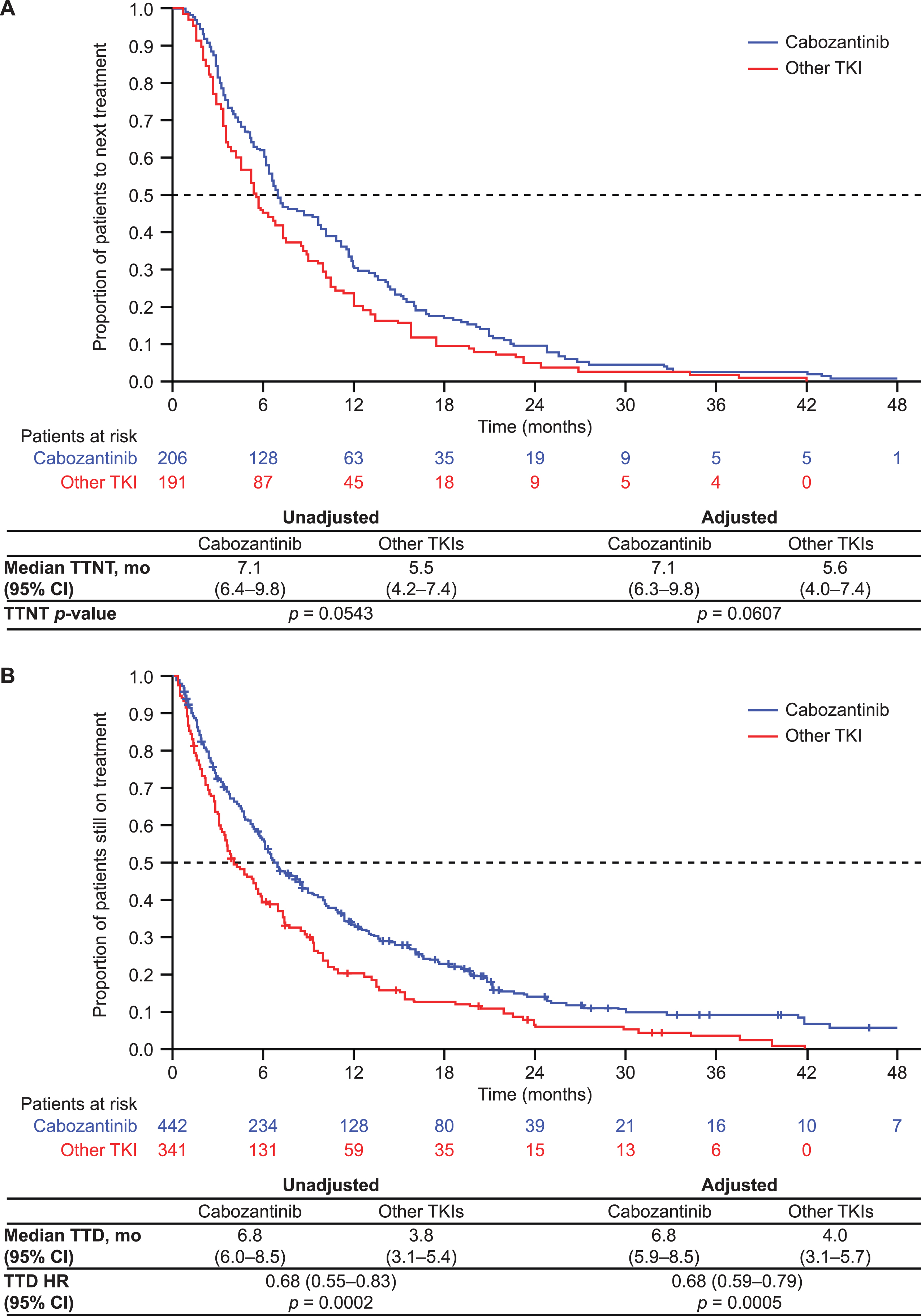
TTD. Median TTD was significantly longer for patients in the cabozantinib arm than in those in the other TKI arm in both the unadjusted and adjusted analyses (Fig. 4B). Adjusted median TTD was 6.8 months and 4.0 months (HR 0.68 [95% CI: 0.59–0.79]; p = 0.0005) for cabozantinib and other TKIs, respectively.
Safety/tolerability outcomes
Dosing
Dose information at the time of index therapy initiation is summarized in Supplementary Table S2. Among patients in the cabozantinib arm, 61.6% initiated therapy at the recommended dose (60 mg once daily) compared with 63.6–80.0% for those in the other TKI arm. A numerically higher percentage of patients in the cabozantinib arm experienced a dose reduction compared with those in the other TKI arm (44.7% vs. 33.8%, respectively). In the cabozantinib arm, 81.6% of patients discontinued index treatment compared with 90.3% of patients in the other TKI arm.
AEs related to index treatment
The rate of treatment-related AEs (TRAEs) was numerically lower in the cabozantinib arm than in the other TKI arm (25.7% vs. 34.4%, respectively), as were discontinuation rates of index therapy owing to AEs (21.8% vs. 26.0%, respectively) (Table 4). The percentage of patients experiencing at least one hospitalization during the index period was numerically higher in the cabozantinib arm than in the other TKI arm (36.0% vs. 28.6%, respectively). The most commonly reported TRAEs in both the cabozantinib and the other TKI arms were fatigue (24.7% vs. 17.0%, respectively), diarrhea (22.4% vs. 18.9%, respectively), nausea (11.8% vs. 15.1%, respectively) and palmar–plantar erythrodysesthesia (11.8% vs. 3.8%, respectively).
Table 4
Treatment-related adverse events
| Cabozantinib (n = 331) | Other TKIs (n = 154) | |
| Patients with at least one TRAE, n (%) | 85 (25.7) | 53 (34.4) |
| TRAEs occurring in≥5% of patients in either group, n (%) | ||
| Fatigue | 21 (24.7) | 9 (17.0) |
| Diarrhea | 19 (22.4) | 10 (18.9) |
| Nausea | 10 (11.8) | 8 (15.1) |
| PPE | 10 (11.8) | 2 (3.8) |
| Rash | 8 (9.4) | 4 (7.5) |
| Decreased appetite | 8 (9.4) | 3 (5.7) |
| Weakness | 6 (7.1) | 5 (9.4) |
| Vomiting | 6 (7.1) | 3 (5.7) |
| Stomatitis | 5 (5.9) | 1 (1.9) |
| Hypertension | 3 (3.5) | 5 (9.4) |
| Patients with an index treatment dose reduction, n (%) | 148 (44.7) | 52 (33.8) |
| Patients who discontinued index treatment owing to AEs, n (%) | 72 (21.8) | 40 (26.0) |
| Patients with at least one hospitalization during the index period, n (%) | 119 (36.0) | 44 (28.6) |
AE, adverse event; PPE, palmar–plantar erythrodysesthesia; TRAE, treatment-related adverse event.
DISCUSSION
The findings of this retrospective study of nearly 500 patients with mRCC demonstrate the activity of cabozantinib in the real-world setting. We retrospectively assessed patient characteristics, treatment patterns, effectiveness and safety/tolerability outcomes among patients with mRCC receiving cabozantinib or other TKI therapy after prior CPI-based treatment in the USA between 2016 and 2022. Importantly, our data demonstrate the effectiveness of cabozantinib treatment after CPI-based therapy in patients without prior TKI exposure.
While cabozantinib monotherapy is commonly used after 1L CPI-based regimens in the USA (based on its broad indication for the treatment of adults with advanced RCC), it is restricted to 1L use or following other VEGF-targeted therapies in Europe and Canada; it is not approved for use following CPI-based therapy in these regions [10–12]. Our objective was to compare the US real-world outcomes of post-CPI VEGF-targeted TKIs (cabozantinib versus axitinib, pazopanib, lenvatinib plus everolimus and sunitinib) to assess whether cabozantinib is non-inferior to other TKIs following CPI-based therapy, to inform global authorities regarding its use in this treatment setting. Based on results from previous randomized, controlled trials, the hypothesis for sample size computation was that post-CPI cabozantinib would demonstrate non-inferiority versus other TKIs post CPI in RR-6m (non-inferiority was met if the lower bound of the 2-sided 90% CI of the difference in the proportions of responders was greater than –10%); superiority was tested when non-inferiority was met.
The primary study endpoint was met and maintained when adjustments for potential confounders were taken into account: at 6 months, response rate with cabozantinib was superior to that for other TKIs (63% vs. 46%, respectively); in the subgroup of 163 patients who received 2L index treatment, RR-6m was non-inferior with 2L cabozantinib versus other 2L TKIs (56% vs. 48%, respectively). In the subgroup analysis of 125 patients who had received 1L ipilimumab plus nivolumab, RR-6m with cabozantinib was also non-inferior to that for other TKIs (58% vs. 49%, respectively). Our RR-6m with cabozantinib (63%) was substantially higher than the ORR reported for cabozantinib after prior CPI therapy in the phase 3 METEOR study (22% ; median duration of cabozantinib exposure, 11.4 months) [14, 23]. Our RR-6m was also higher than the ORR for cabozantinib monotherapy or cabozantinib combined with atezolizumab after prior CPI therapy in the phase 3 CONTACT-03 trial (41% ; median duration of follow-up, 15.2 months) [13]. Furthermore, our RR-6m was higher than the ORR for cabozantinib monotherapy (28%) or cabozantinib plus telaglenastat (31%) after prior antiangiogenic therapy or nivolumab plus ipilimumab in the phase 2 CANTATA trial (median duration of follow-up, 11.7 months) [16].
Ongoing trials, such as the phase 2 CaboPoint study, will provide additional insights on the use of cabozantinib following CPI-based therapy [24]; at interim analysis, the CaboPoint study showed preliminary cabozantinib efficacy in patients with advanced RCC who had received prior 1L CPI–CPI and TKI–CPI combinations [15]. However, owing to the geographical variations in indications, there are currently limited data on the real-world use and effectiveness of cabozantinib after CPI-based therapy, particularly in comparison with other TKI regimens [10–15].
The notably higher response rate reported in our study than in the METEOR, CONTACT-03 and CANTATA trials may reflect the use of physician assessment or chart documentation of response in real-world settings (with partial response defined as any improvement or response) instead of RECIST-based tumor assessments (in which partial response is defined as reduction in tumor size of at least 30% [25]), as used in clinical trials, which may also employ a centralized review committee. Physician-based assessments are open to greater potential subjectivity and between-center heterogeneity than objective RECIST-based assessments [26]. Although these differences limit the extent to which our findings can be compared with those of published studies, particularly interventional trials using RECIST-based assessments, it should not prohibit within-study comparison between treatment arms, for which tumor response was assessed in the same way.
Despite the potential heterogeneity in physician assessments for all index treatments in real-world studies, real-world ORR and TTD significantly favored cabozantinib over other TKIs in our study, and TTNT was numerically longer with cabozantinib than with other TKIs. ORR was superior for cabozantinib versus other TKI therapies in both adjusted and unadjusted analyses, and was non-inferior for 2L cabozantinib versus other 2L TKIs. In a preplanned subgroup analysis of patients who had received 1L ipilimumab plus nivolumab in our study, the adjusted ORR with cabozantinib remained unchanged at 62% and was shown to be non-inferior to other TKIs. Other published real-world studies of cabozantinib after CPI-based therapy have reported more modest response rates around this time point (20–52% vs. 62% in our study) [27–33]. For example, in the UK CARINA study, which evaluated cabozantinib after CPI-based combination therapy, the ORR at ∼5.5 months of treatment was 32% [33]. Interestingly, in this study, ORR for cabozantinib was numerically higher after CPI–CPI therapy than after TKI–CPI therapy (36% vs. 16%) [34]. Although the CARINA study was similar to the present study in its requirement for evidence of prior CPI-based therapy, there are some important differences: prior CPI-based therapy in CARINA was restricted to the 1L setting and did not include CPI monotherapy (79% of patients in the CARINA study received 1L ipilimumab plus nivolumab vs. 26% in our study) [33].
There were no differences in DOR, PFS or OS for patients receiving cabozantinib versus other TKIs in our study. The lack of significant difference in median PFS between cabozantinib and other TKI therapies may be partly explained by the imbalance in the percentage of patients who were censored versus those with events between the two groups (for cabozantinib, 36% of patients were censored and 64% had an event, whereas for other TKIs, 50% of patients were censored and 50% had an event). The lack of significant difference in median OS for cabozantinib and other TKI therapies, despite differences in tumor response rates, may reflect the effects of post-index therapy treatments that confound the OS analysis; 59% of patients had documentation of post-index therapy. The median OS for cabozantinib was consistent with that reported in the METEOR study (19.2 vs. 21.4 months) [35] and real-world studies of cabozantinib after CPI-based combination therapy (13.1–21.4 months) [27–30, 33].
The majority of patients in the cabozantinib arm commenced treatment at the recommended dose of 60 mg/day, which was slightly higher than that reported in a similar real-world study conducted in the USA (62% vs. 52%, respectively) [27]. Dose reductions occurred for a higher proportion of patients in the cabozantinib arm than in the other TKI arm; however, TRAEs and discontinuations owing to AEs were less frequent. In this study, all data, including for TRAEs, were analyzed by treatment group (cabozantinib versus other TKIs); differences in TRAEs between the other TKIs were therefore not analyzed, but were not anticipated.
The safety/tolerability and effectiveness of cabozantinib were consistent with both the phase 3 METEOR study, which supported the initial approval of cabozantinib for patients with advanced RCC, and with other small real-world studies of cabozantinib after CPI-based therapy [14, 23, 27–30, 33, 36]. The findings of the present study should be generalizable to European and Canadian populations because the benefit–risk profile of cabozantinib is not expected to differ notably between theseregions.
Strengths and limitations
These study results should be interpreted within the context of its retrospective design and the use of secondary-source EHR data, the quality of which depends upon accurate and complete physician documentation. Precise histology data were not available given the study design; therefore, the proportion of patients with non-clear cell RCC, and specific sub-types, could not be further described. In addition, the iKM EHR did not include any medical history prior to a patient’s first encounter at a USON practice, or services and procedures performed outside of the USON; these data may therefore provide an incomplete picture of the patient experience.
RR-6m based on chart review was used instead of RECIST-based ORR. Differences in partial response definitions between these assessment methods limit the comparison of our real-world data with other clinical data. In addition, data availability and quality were impacted by the data collection methods and reporting practices of individual physicians.
Owing to the dates of the study period and the exclusion of patients with a history of clinical trial participation, few patients received TKI–CPI combination therapy prior to index treatment, which may affect comparisons with future real-world studies that include patients with prior TKI–CPI treatment. In addition, only one third of the study population had previously received CPI–CPI combination therapy (ipilimumab plus nivolumab). While this may limit the applicability of our results in regions with significant use of such combinations as a 1L regimen, this treatment pattern may broadly reflect its real-world use in many jurisdictions given the uptake of 1L TKI–CPI therapies overtime [4, 5].
The final sample size was smaller than anticipated during protocol development owing to differences between the feasibility eligibility criteria and completeness of the preliminary versus final chart review. However, updated power calculations confirmed that the analysis retained statistical validity.
Within the context of this study design, this study is one of the largest analyses of cabozantinib use in the real-world setting. Real-world studies tend to feature broader inclusion criteria than those employed in clinical trials and are more representative of routine clinical practice. Additionally, this study provides an accurate reflection of real-world tumor response assessment. Furthermore, our large study population (N = 485) comprises a wide variety of patients receiving treatment in community oncology practice, in contrast to the populations of retrospective studies performed at single academic institutions, which typically comprise fewer than 100 patients (range, 30–87 [37–42]) and have limited geographic diversity. It is also larger than other multi-center, real-world cabozantinib studies (for example, CABOREAL [N = 410], the 2021 IMDC study [N = 413], CABOSEQ [N = 346] [28, 29, 43]).
Finally, data from this study robustly describe patient characteristics, treatment patterns and outcomes among patients with mRCC treated in community oncology settings and offer insights to help clinicians seeking to optimize treatment outcomes in routine clinical practice.
CONCLUSIONS
In this large, real-world study, cabozantinib was an effective and well-tolerated therapy for patients with mRCC in the post-CPI setting. These data build on the existing pool of real-world evidence to support the tolerability and effectiveness of cabozantinib monotherapy after CPI-based therapy, including for patients without prior TKI exposure, and may inform global authorities regarding the use of cabozantinib in this treatment setting. Prospective studies, including the ongoing phase 2 CaboPoint study will generate additional data to guide the use of cabozantinib in the post-CPI setting.
ACKNOWLEDGMENTS
The authors thank all patients involved in the study, as well as their caregivers, care team, investigators and research staff in participating institutions. The authors thank Amber Tear (MRes) and Alison Chisholm (MPH) of Oxford PharmaGenesis, Oxford, UK for providing medical writing support, which was sponsored by Ipsen in accordance with Good Publication Practice guidelines (GPP 2022).
FUNDING
This study was sponsored by Ipsen.
AUTHOR CONTRIBUTIONS
All authors had access to the study data, reviewed and edited the manuscript, and had final responsibility for the decision to submit.
DH: study design, investigation, data gathering, analysis and interpretation, writing – reviewing and editing.
GD: study design, investigation, data gathering, curation, analysis and interpretation, writing – reviewing and editing.
PD: investigation, supervision, writing – reviewing and editing.
AH: conceptualization, investigation, methodology, supervision, writing – reviewing and editing.
ML: conceptualization, funding acquisition, investigation, methodology, supervision, writing – reviewing and editing.
AM: conceptualization, data curation, investigation, methodology, project administration, resources, writing – reviewing and editing.
YW: formal analysis, investigation, methodology, software, writing – reviewing and editing.
VP: conceptualization, investigation, methodology, supervision, writing – reviewing and editing.
AL: study design, investigation, data gathering, analysis and interpretation, writing – reviewing and editing.
CONFLICT OF INTEREST
DH: Editorial board member of Kidney Cancer but not involved in the peer-review process of this paper, and did not have access to any information regarding its peer review; Consulting or advisory role – Astellas Pharma, Bristol Myers Squibb, Eisai, Ipsen, Janssen, Merck, Novartis, Pfizer; Research funding – Bristol Myers Squibb, Exelixis, Ipsen, Novartis, Pfizer. GD: Nothing to disclose. PD: Full- or part-time employment – Ipsen. AH: Full- or part-time employment – Ipsen; Travel, accommodation, expenses – Ipsen; Stock and other ownership interests – Ipsen. ML: Full- or part-time employment – Ipsen; Stock and other ownership interests – Amgen. AM: Full- or part-time employment – Ontada/McKesson; Stock and other ownership interests – McKesson. YW: Full- or part-time employment – Ontada/McKesson; Stock and other ownership interests – McKesson. VP: Full- or part-time employment – Ipsen; Travel, accommodation, expenses – Ipsen; Stock and other ownership interests – Ipsen. AL: Consulting or advisory role – AbbVie, Astellas Pharma, Bayer, Bristol Myers Squibb, Eisai, Ipsen, Janssen, Merck, Pfizer, Roche/Genentech; Honoraria – Astellas Pharma, Bayer, Bristol Myers Squibb, Eisai, Ipsen, Merck, Novartis, Pfizer, Roche/Genentech; Research funding – BioCanRx, Bristol Myers Squibb, EMD Serono, Ipsen, Novartis, Roche.
DATA AVAILABILITY
The health data used to support the findings of this study are restricted by the US Oncology Institutional Review Board in order to protect patient privacy. For this reason, data used to support the findings of this study have not been made available. These health data were accessed for this study by Ontada who were contracted to support Ipsen with this research.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/KCA-240005.
REFERENCES
[1] | Padala SA , Barsouk A , Thandra KC , Saginala K , Mohammed A , Vakiti A , Rawla P , Barsouk A . Epidemiology of renal cell carcinoma. World J Oncol. (2020) ;11: (3):79–87. |
[2] | Lalani AA , Heng DYC , Basappa NS , Wood L , Iqbal N , McLeod D , Soulieres D , Kollmannsberger C . Evolving landscape of first-line combination therapy in advanced renal cancer: A systematic review. Ther Adv Med Oncol. (2022) ;14: :17588359221108685. |
[3] | National Cancer Institute Surveillance Epidemiology and End Results Program. Cancer Stat Facts: Kidney and renal pelvis cancer [accessed April 2023]. Available from: https://seer.cancer.gov/statfacts/html/kidrp.html. |
[4] | Rathmell WK , Rumble RB , Van Veldhuizen PJ , Al-Ahmadie H , Emamekhoo H , Hauke RJ , Louie AV , Milowsky MI , Molina AM , Rose TL , Siva S , Zaorsky NG , Zhang T , Qamar R , Kungel TM , Lewis B , Singer EA . Management of metastatic clear cell renal cell carcinoma: ASCO guideline. J Clin Oncol. (2022) ;40: (25):2957–95. |
[5] | Powles T , ESMO Guidelines Committee. Recent eUpdate to the ESMO Clinical Practice Guidelines on renal cell carcinoma on cabozantinib and nivolumab for first-line clear cell renal cancer: Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2021) ;32: (3):422–3. |
[6] | US Food and Drug Administration. Opdivo Prescribing Information; 2022 [updated March 2022; accessed July 2023]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/125554s112lbl.pdf. |
[7] | European Medicinces Agency. Yervoy Summary of Product Characteristics; 2016 [updated October 16, 2023; accessed January 29, 2024]. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/yervoy#authorisation-details-section. |
[8] | Health Canada.Yervoy® (ipilimumab) Product Monograph; 2012 [updated November 24, 2022; accessed July 2023]. Available from: https://pdf.hres.ca/dpd_pm/00068433.PDF. |
[9] | Shah NJ , Sura S , Shinde R , Shi J , Perini RF , Puneet S , Robert NJ , Vogelzang NJ , Motzer RJ . Real-world assessment of changing treatment patterns and sequence for patients with metastatic renal cell carcinoma (mRCC) in the first-line (1L) setting [abstract]. Presented at 2022 ASCO Genitourinary Cancers Symposium. J Clin Oncol. (2022) ;40: (6_suppl):302. |
[10] | US Food and Drug Administration. Exelixis, Inc. Prescribing information, CABOMETYX; 2021 [updated January 2021; accessed July 2023]. Available from: www.accessdata.fda.gov/drugsatfda_docs/label/2021/208692s010lbl.pdf. |
[11] | European Medicines Agency. Cabometyx® (cabozantinib) EU Summary of Product Characteristics; 2016 [updated April 21, 2021; accessed September 2022]. Available from: https://www.ema.europa.eu/en/documents/product-information/cabometyx-epar-product-information_en.pdf |
[12] | Health Canada. Cabometyx® (cabozantinib) Product Monograph; 2022 [updated September 14, 2022; accessed May 2023]. Available from: https://pdf.hres.ca/dpd_pm/00067411.PDF. |
[13] | Pal SK , Albiges L , Tomczak P , Suarez C , Voss MH , de Velasco G , Chahoud J , Mochalova A , Procopio G , Mahammedi H , Zengerling F , Kim C , Osawa T , Angel M , Gupta S , Khan O , Bergthold G , Liu B , Kalaitzidou M , Huseni M , Scheffold C , Powles T , Choueiri TK . Atezolizumab plus cabozantinib versus cabozantinib monotherapy for patients with renal cell carcinoma after progression with previous immune checkpoint inhibitor treatment (CONTACT-03): A multicentre, randomised, open-label, phase 3 trial. Lancet. (2023) ;402: :185–95. |
[14] | Powles T , Motzer RJ , Escudier B , Pal S , Kollmannsberger C , Pikiel J , Gurney H , Rha SY , Park SH , Geertsen PF , Gross-Goupil M , Grande E , Suarez C , Markby DW , Arroyo A , Dean M , Choueiri TK , George D . Outcomes based on prior therapy in the phase 3 METEOR trial of cabozantinib versus everolimus in advanced renal cell carcinoma. Br J Cancer. (2018) ;119: (6):663–9. |
[15] | Albiges L , Powles T , Sharma A , Venugopal B , Bedke J , Dutailly P , Qvick B , Martin-Couce L , Perrot V , Grünwald V . CaboPoint: Interim results from a phase 2 study of cabozantinib after checkpoint inhibitor (CPI) therapy in patients with advanced renal cell carcinoma (RCC). J Clin Oncol. (2023) ;41: (6_suppl):606. |
[16] | Tannir NM , Agarwal N , Porta C , Lawrence NJ , Motzer R , McGregor B , Lee RJ , Jain RK , Davis N , Appleman LJ , Goodman O Jr , Stadler WM, Gandhi S, Geynisman DM, Iacovelli R, Mellado B, Sepúlveda Sánchez JM, Figlin R, Powles T, Akella L, Orford K, Escudier B. Efficacy and safety of telaglenastat plus cabozantinib vs. placebo plus cabozantinib in patients with advanced renal cell carcinoma: The CANTATA randomized clinical trial. JAMA Oncol. (2022) ;8: (10):1411–8. |
[17] | Ornstein MC , Pal SK , Wood LS , Tomer JM , Hobbs BP , Jia XS , Allman KD , Martin A , Olencki T , Davis NB , Gilligan TD , Mortazavi A , Rathmell WK , Garcia JA , Rini BI . Individualised axitinib regimen for patients with metastatic renal cell carcinoma after treatment with checkpoint inhibitors: A multicentre, single-arm, phase 2 study. Lancet Oncol. (2019) ;20: (10):1386–94. |
[18] | Grande E , Alonso-Gordoa T , Reig O , Esteban E , Castellano D , Garcia-Del-Muro X , Mendez MJ , Garcia-Donas J , Gonzalez Rodriguez M , Arranz-Arija JA , Lopez-Criado P , Molina-Cerrillo J , Mellado B , Alvarez-Fernandez C , De Velasco G , Cuellar-Rivas MA , Rodriguez-Alonso RM , Rodriguez-Moreno JF , Suarez-Rodriguez C . Results from the INMUNOSUN-SOGUG trial: A prospective phase II study of sunitinib as a second-line therapy in patients with metastatic renal cell carcinoma after immune checkpoint-based combination therapy. ESMO Open. (2022) ;7: (2):100463. |
[19] | Procopio G , Claps M , Pircher C , Porcu L , Sepe P , Guadalupi V , De Giorgi U , Bimbatti D , Nole F , Carrozza F , Buti S , Iacovelli R , Ciccarese C , Masini C , Baldessari C , Doni L , Cusmai A , Gernone A , Scagliarini S , Pignata S , de Braud F , Verzoni E . A multicenter phase 2 single arm study of cabozantinib in patients with advanced or unresectable renal cell carcinoma pre-treated with one immune-checkpoint inhibitor: The BREAKPOINT trial (Meet-Uro trial 03). Tumori. (2023) ;109: (1):129–37. |
[20] | Graham J , Vogel A , Cheng AL , Bjarnason GA , Neal JW . Cabozantinib after prior checkpoint inhibitor therapy in patients with solid tumors: A systematic literature review. Cancer Treat Rev. (2022) ;110: :102453. |
[21] | Albiges L , McGregor BA , Heng DYC , Procopio G , de Velasco G , Taguieva-Pioger N , Martin-Couce L , Tannir NM , Powles T . Vascular endothelial growth factor-targeted therapy in patients with renal cell carcinoma pretreated with immune checkpoint inhibitors: A systematic literature review. Cancer Treat Rev. (2024) ;122: :102652. |
[22] | US Food and Drug Administration. US Department of Health and Human Services, Food and Drug Administration. Non-inferiority clinical trials to establish effectiveness - guidance for industry; 2016 [published November 2016; accessed April 2023]. Available from: https://www.fda.gov/media/78504/download. |
[23] | Choueiri TK , Escudier B , Powles T , Mainwaring PN , Rini BI , Donskov F , Hammers H , Hutson TE , Lee JL , Peltola K , Roth BJ , Bjarnason GA , Géczi L , Keam B , Maroto P , Heng DY , Schmidinger M , Kantoff PW , Borgman-Hagey A , Hessel C , Scheffold C , Schwab GM , Tannir NM , Motzer RJ . Cabozantinib versus everolimus in advanced renal-cell carcinoma. N Engl J Med. (2015) ;373: (19):1814–23. |
[24] | Albiges L , Schmidinger M , Taguieva-Pioger N , Perol D , Grünwald V , Guemas E . CaboPoint: A phase II study of cabozantinib as second-line treatment in patients with metastatic renal cell carcinoma. Future Oncol. (2022) ;18: (8):915–26. |
[25] | Eisenhauer EA , Therasse P , Bogaerts J , Schwartz LH , Sargent D , Ford R , Dancey J , Arbuck S , Gwyther S , Mooney M , Rubinstein L , Shankar L , Dodd L , Kaplan R , Lacombe D , Verweij J . New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer. (2009) ;45: (2):228–47. |
[26] | Feinberg BA , Zettler ME , Klink AJ , Lee CH , Gajra A , Kish JK . Comparison of solid tumor treatment response observed in clinical practice with response reported in clinical trials. JAMA Netw Open. (2021) ;4: (2):e2036741. |
[27] | McGregor BA , Lalani A-KA , Xie W , Steinharter JA , Bakouny ZE , Martini DJ , Fleischer JH , Abou-Alaiwi S , Nassar A , Nuzzo PV , Kaymakcalan MD , Braun DA , Wei XX , Harshman LC , Bilen MA , Choueiri TK . Activity of cabozantinib after immune checkpoint blockade in metastatic clear-cell renal cell carcinoma. Eur J Cancer. (2020) ;135: :203–10. |
[28] | Navani V , Wells JC , Boyne DJ , Cheung WY , Brenner DM , McGregor BA , Labaki C , Schmidt AL , McKay RR , Meza L , Pal SK , Donskov F , Beuselinck B , Otiato M , Ludwig L , Powles T , Szabados BE , Choueiri TK , Heng DYC . CABOSEQ: The effectiveness of cabozantinib in patients with treatment refractory advanced renal cell carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC). Clin Genitourin Cancer. (2023) ;21: (1):106.e1–e8. |
[29] | Gan CL , Dudani S , Wells JC , Donskov F , Pal SK , Dizman N , Rathi N , Beuselinck B , Yan F , Lalani A-KA , Hansen A , Szabados B , de Velasco G , Tran B , Lee JL , Vaishampayan UN , Bjarnason GA , Subasri M , Choueiri TK , Heng DYC . Cabozantinib real-world effectiveness in the first- through fourth-line settings for the treatment of metastatic renal cell carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium. Cancer Med. (2021) ;10: (4):1212–21. |
[30] | Zhang H , Basappa NS , Ghosh S , Joy I , Lalani A-KA , Hansen AR , Heng DYC , Castonguay V , Kollmannsberger CK , Winquist E , Wood L , Bjarnason GA , Breau RH , Kapoor A , Graham J . Real-world experience of cabozantinib in metastatic renal cell carcinoma (mRCC): Results from the Canadian Kidney Cancer information system (CKCis). Kidney Cancer. (2021) ;5: :21–9. |
[31] | Iacovelli R , Ciccarese C , Facchini G , Milella M , Urbano F , Basso U , De Giorgi U , Sabbatini R , Santini D , Berardi R , Santoni M , Bracarda S , Massari F , Masini C , De Tursi M , Ricotta R , Buti S , Zustovich F , Sepe P , Rossetti S , Maruzzo M , Cortesi E , Tortora G , Procopio G . Cabozantinib after a previous immune checkpoint inhibitor in metastatic renal cell carcinoma: A retrospective multi-institutional analysis. Target Oncol. (2020) ;15: (4):495–501. |
[32] | Derosa L , Rouche JA , Colomba E , Baciarello G , Routy B , Albiges L , Escudier B . Efficacy of cabozantinib (C) after PD-1/PD-L1 checkpoint inhibitors in metastatic renal cell carcinoma (mRCC): The Gustave Roussy experience. Ann Oncol. (2017) ;28: :v309. |
[33] | Nathan PD , Allison J , Charnley N , Griffiths R , Michael A , Moore K , Sharma A , Szabados B , Venugopal B , Ali J , Perrot V , Prendergast A , Klair B , Larkin J . Real-world treatment sequencing and outcomes for patients with advanced renal cell carcinoma treated with cabozantinib after first-line checkpoint inhibitor-based combination therapy: Results from the CARINA study [abstract]. Presented at ASCO Annual Meeting. J Clin Oncol. (2023) ;41: (16 SUPPL):e16512. |
[34] | Nathan P , Allison J , Charnley N , Griffiths R , Michael A , Moore K , Sharma A , Venugopal B , Ali J , Perrot V , Prendergast A , Ceruso M , Larkin J . Real-world outcomes of cabozantinib treatment after first-line checkpoint inhibitor-based combination therapy for patients with advanced renal cell carcinoma: CARINA study results. Eur Urol Open Sci. (2023) ;57: :S238–S9. |
[35] | Motzer RJ , Escudier B , Powles T , Scheffold C , Choueiri TK . Long-term follow-up of overall survival for cabozantinib versus everolimus in advanced renal cell carcinoma. Br J Cancer. (2018) ;118: (9):1176–8. |
[36] | Choueiri TK , Escudier B , Powles T , Tannir NM , Mainwaring PN , Rini BI , Hammers HJ , Donskov F , Roth BJ , Peltola K , Lee JL , Heng DYC , Schmidinger M , Agarwal N , Sternberg CN , McDermott DF , Aftab DT , Hessel C , Scheffold C , Schwab G , Hutson TE , Pal S , Motzer RJ . Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): Final results from a randomised, open-label, phase 3 trial. Lancet Oncol. (2016) ;17: (7):917–27. |
[37] | Campbell MT , Bilen MA , Shah AY , Lemke E , Jonasch E , Venkatesan AM , Altinmakas E , Duran C , Msaouel P , Tannir NM . Cabozantinib for the treatment of patients with metastatic non-clear cell renal cell carcinoma: A retrospective analysis. Eur J Cancer. (2018) ;104: :188–94. |
[38] | Cerbone L , Nunno VD , Carril Ajuria L , Alves Costa Silva C , Colomba E , Guida A , Salviat F , Hirsch L , Benchimol-Zouari A , Flippot R , Escudier B , Albiges L . Activity of systemic treatments after cabozantinib failure in advanced metastatic renal cell carcinoma. Clin Genitourin Cancer. (2022) ;20: (1):80–7. |
[39] | Kucharz J , Dumnicka P , Kusnierz-Cabala B , Demkow T , Wiechno P . The correlation between the incidence of adverse events and progression-free survival in patients treated with cabozantinib for metastatic renal cell carcinoma (mRCC). Med Oncol. (2019) ;36: (2):19. |
[40] | Lemke EA , Shah AY , Campbell M , Tannir NM . Real-world experience with cabozantinib in metastatic clear cell renal cell carcinoma: A retrospective analysis. J Adv Pract Oncol. (2019) ;10: (4):333–9. |
[41] | Martini DJ , Kline MR , Liu Y , Shabto JM , Carthon BC , Russler GA , Yantorni L , Hitron EE , Caulfield S , Goldman JM , Harris WB , Kucuk O , Master VA , Bilen MA . Novel risk scoring system for metastatic renal cell carcinoma patients treated with cabozantinib. Cancer Treat Res Commun. (2021) ;28: :100393. |
[42] | McElwee JH , Gourdin TS , Mikoll J , Weeda E , Sion AM . Cabozantinib use in metastatic renal cell carcinoma patients in clinical practice: Evaluation of dosing patterns, tolerability, and outcomes compared to clinical trials. J Oncol Pharm Pract. (2020) ;26: (4):861–5. |
[43] | Albiges L, Flechon A, Chevreau C, Topart D, Gravis G, Oudard S, Tourani JM, Geoffrois L, Meriaux E, Thiery-Vuillemin A, Barthelemy P, Ladoire S, Laguerre B, Perrot V, Billard A, Escudier B, Gross-Goupil M. Real-world evidence of cabozantinib in patients with metastatic renal cell carcinoma: Results from the CABOREAL Early Access Program. Eur J Cancer. (2021) ;142: :102–11. |


