
The Prevalence of Parkinson’s Disease in Poland: Regional and Sex-Related Differences
Abstract
Background:
Given the growing evidence for an environmental contribution to the etiology of Parkinson’s disease (PD), searching for local and regional differences in PD prevalence in multiple areas across the world may further clarify the role of environmental toxins.
Objective:
To provide local and regional prevalence estimates of PD in Poland.
Methods:
We analyzed the prevalence of PD and its trend over the last decade (2010 to 2019) based on data from the National Health Fund in Poland. We specifically examined sex differences in PD prevalence, as well as differences across Polish regions.
Results:
During the above period, the prevalence of PD in Poland increased from 226 per 100,000 to 269 per 100,000 inhabitants. Unexpectedly, we found that PD was 1.2-times more common in women than men. The increase in prevalence over the past decade was different between both sexes: an increase from 250 to 283 per 100,000 for women (13.3% increase), and from 200 to 254 per 100,000 for men (27.1% increase). In addition, we observed differences in prevalence across different Polish regions, with some regions having up to 51% lower prevalence rates than others.
Conclusions:
The prevalence of PD in Poland is in line with previously reported prevalence rates across Europe. However, unlike the situation in most of the world, PD was more prevalent in women than men. We discuss several possible explanations as well as potential measures that might help to reduce the growth of PD.
INTRODUCTION
Parkinson’s disease (PD) is a complex neurodegenerative disease presenting with motor and non-motor symptoms [1, 2]. Typically, the prevalence of PD increases with age, and its incidence rises sharply after the age of 60 years, with a projected exponential growth in subsequent decades. For a large part of the history of humankind, PD was presumably a rare disorder, certainly prior to 1817 when the disease was meticulously described for the first time by James Parkinson. The severe air pollution that arose at the beginning of the 19th century in London may have contributed to the appearance of PD during this time [3]. Based on the available resources in the early 19th century, the prevalence reported in, for example, England and Wales, was approximately 22 people in a population of 15 million [4]. These numbers have grown rapidly since, and currently PD is the world’s fastest-growing neurological disorder, with over six million individuals affected with the disease globally, having more than doubled since 1990, thus becoming a leading cause of neurological disability [5]. Overall age-standardized PD prevalence rates have increased worldwide by nearly 22% [6] and based on prevalence data from a 2014 meta-analysis, the number of people with PD will have more than doubled again to 14.2 million in 2040 [7]. Nonetheless, these estimates probably represent an underestimate of the future prevalence due to underreporting of PD in current datasets [8].
The rapid growth in PD prevalence could be driven by multiple factors, including aging of the population, increasing longevity, declining smoking rates (smoking has been associated with a 50% decreased risk of developing PD), reduced mortality from PD due to better care, and increasing industrialization [8, 9]. There are growing concerns that the increased PD prevalence rates may be explained, at least in part, by exposure to environmental toxins, including chemicals such as pesticides and trichloroethylene [10–12]. Here, studies of differences in the regional prevalence of PD may be of particular help to clarify the possible role of environmental toxins in the etiology of this disease. For example, studies in France have highlighted that the prevalence of PD shows marked regional differences, the prevalence being considerably higher in areas with intensive wine culture, and with somewhat of a dose-response relationship to the concentration of pesticides [13]. Other countries where such regional differences have been identified include Canada [14] and the United States [15]. In order to provide prevalence estimates of PD and aid in better understanding the local situation in Poland, we aimed to analyze the prevalence rates of PD and its trend over the last decade (2010 to 2019). In addition, we sought to determine whether regional differences in PD prevalence across Poland were present.
METHODS
The analyses described here were based on data available in the database of the National Health Fund in Poland (NHF) (https://www.nfz.gov.pl). Population size estimates were obtained from the Central Statistical Office of Poland (https://stat.gov.pl). The NHF is a public organ, financed by compulsory health insurance contributions, which finances health services provided to individuals and reimburses the cost of medicines in Poland. Therefore, the NHF databases contain data of all patients who received healthcare services financed from public funds related to a diagnosis of PD. It does not include those diagnosed and treated entirely within private healthcare, but due to the general structure of the healthcare system and services in Poland, such cases are likely to be incidental as nearly all patients who have private insurance (around 11% of all patients) are also seen in public healthcare facilities. In our analyses, we limited the data to the last decade, spanning the years 2010 to 2019 (inclusive). The data obtained from the NHF database were all in anonymized form, in compliance with the Polish Act on the Protection of Personal Data.
We defined PD by its relevant ICD-10 diagnosis code “G20 –Parkinson’s disease” as the principal diagnosis or comorbidity for any person who was identified in the NHF database as having received care for this diagnosis during a given calendar year. From the database, it was not possible to ascertain whether this diagnosis had been made within a primary or secondary/tertiary care setting, so a certain rate of misclassification (e.g., atypical parkinsonism) can be expected, although this would be unlikely to affect the time trends or the differences between sexes or regions.
The primary aim of the current analyses was to estimate the prevalence of PD in Poland over the period 2010–2019. To this aim, we divided the number of patients with ICD-10 code G20 for each year by the average population for that year. Additionally, we repeated this separately for male and female patients to obtain sex-specific PD prevalence estimates. Further stratification was performed by analyzing the prevalence estimates per age group as provided by the NHF: 1) 0–17 years; 2) 18–20 years; 3) 21–50 years; 4) 51–70 years; and 5) 71 years and over. Finally, we performed separate analyses to determine the PD prevalence across the different Polish regions (called Voivodships; Fig. 1) and explored possible reasons explaining regional differences in PD prevalence. For the latter, we obtained data on the number of neurologists per region from the Polish Chamber of Physicians and Dentists (https://nil.org.pl), the percentage of people who never smoked [16], and regional life expectancy at birth from the Statista website (https://www.statista.com). Regional data on the number of movement disorders neurologists were not available.
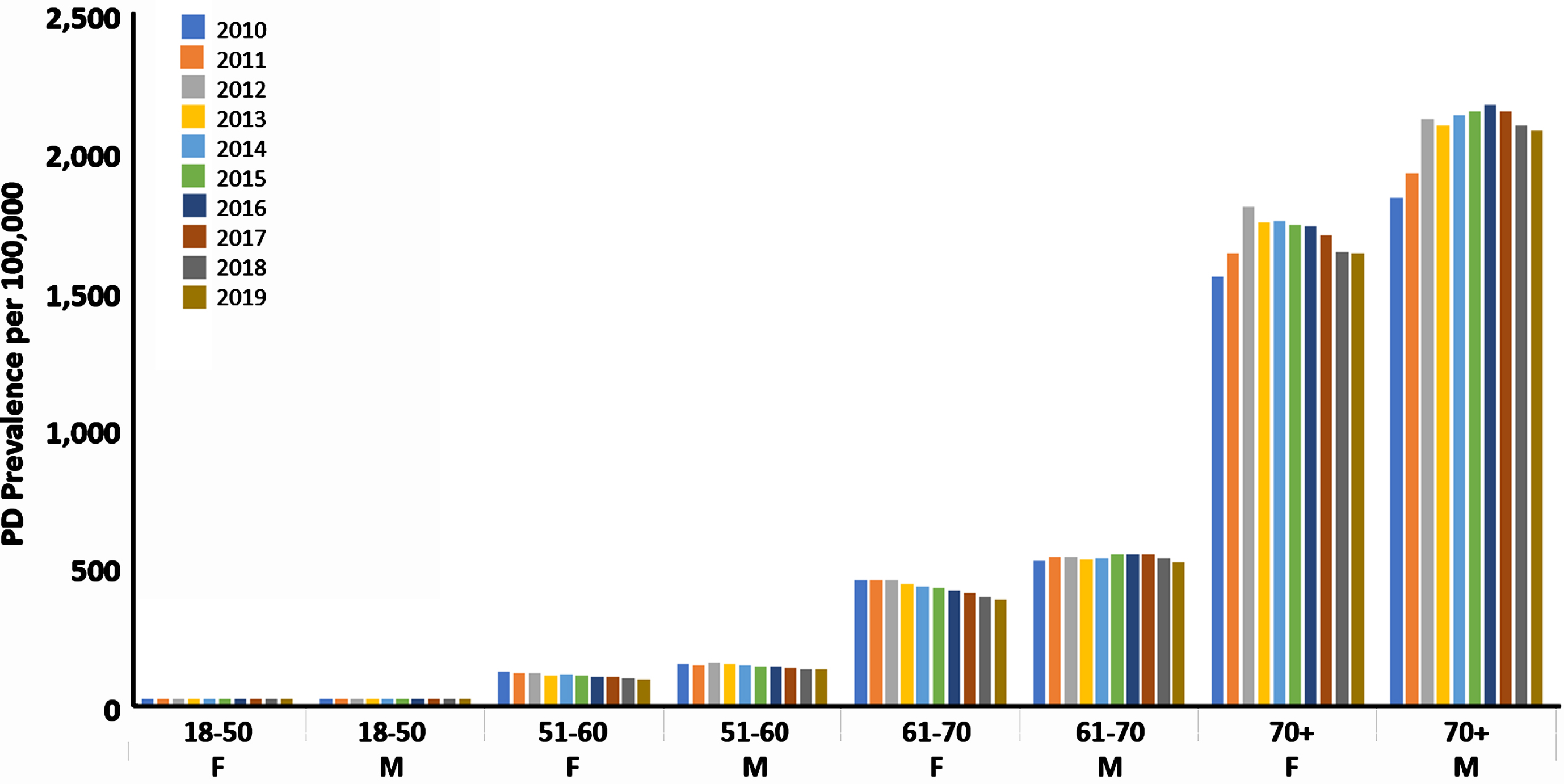
Fig. 1
Sex-specific Parkinson’s disease prevalence in Poland for the years 2010–2019. PD, Parkinson’s disease; F, female; M, male.
Statistical analysis
Data were summarized descriptively and were presented as numbers (percentages) unless otherwise specified. For group comparisons, we used the Kruskal-Wallis test with a Bonferroni correction for multiple testing, where relevant. For the comparison of prevalence figures between men and women, the prevalence rate ratio (PRR) was used with a corresponding 95% confidence interval (CI) and p-value. The sex-specific prevalence was compared with the crude odds ratios (OR) as well as with the odds ratios based on the Mantel-Haenschel method of stratification (by age group) and presented with a 95% CI and p-value. The Breslow-Day test was used to assess the homogeneity for a 2 by 2 by k table in order to investigate whether all k strata have the same OR. For univariate analyses, we used the non-parametric Spearman’s rank correlation coefficient. Where relevant, we corrected the effects of multiple testing using the Bonferroni-Holmes technique. All analyses were performed using SPSS Version 27 (IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp.) and MedCalc (Version 22.006).
RESULTS
Over the period 2010 to 2019, the crude prevalence of PD in Poland increased from 226 per 100,000 to 269 per 100,000 (prevalence rate ratio (PRR) of 1.19, 95% CI: 1.18 –1.20,p < 0.001;Table 1). We also observed that the prevalence of PD over the decade that we investigated increased more for men than for women (from 200 to 254 for men, and from 250 to 283 per 100,000 for women). This corresponded to a PRR of 1.27 (95% CI: 1.25 –1.29, p < 0.001) for men and 1.13 (95% CI: 1.12 –1.15, p < 0.001) for women. Analysis of the sex-specific prevalence during follow-up showed that PD was more prevalent among women than men (Table 1). The crude odds ratio of PD for women, compared to men, varied slightly throughout the decade between 1.11 and 1.25, and the unadjusted odds ratio stratified by years was 1.20 (95% CI: 1.19 –1.20; p < 0.001). However, taking age groups into account, the age-adjusted odds ratios of PD for women, compared to men, were in the opposite direction, varying slightly between 0.84 and 0.77. The mean magnitude of the ageing effect was 32%. In addition, we noted that in those over 70 years, the prevalence during follow-up increased more for men than for women (from 1,844 to 2,091 and from 1,560 to 1,644 per 100,000, respectively), which corresponds to a PRR of 1.13 (95% CI: 1.12 –1.15, p < 0.001) for men and 1.05 (95% CI: 1.04 –1.07, p < 0.001) for women (Table 2; Fig. 1).
Table 1
The number of people with Parkinson’s disease and the estimated prevalence of the disease in Poland over the period 2010–2019
| People with ICD-10 diagnosis G20 (Parkinson’s disease) in Poland | |||||||||||
| All | Men | Women | Female vs. Male | ||||||||
| OR (±95% CI) | |||||||||||
| Year | Population | Parkinson’s | Crude prevalence* | Population | Parkinson’s | Crude prevalence | Population | Parkinson’s | Crude prevalence | Crude | Age-adjusted |
| 2010 | 38,529,866 | 87,034 | 226 | 18,653,125 | 37,313 | 200 | 19,876,741 | 49,721 | 250 | 1.251# (1.234 –1.268) | 0.842# (0.831 –0.854) |
| 2011 | 38,538,447 | 91,561 | 238 | 18,654,577 | 39,192 | 210 | 19,883,870 | 52,369 | 263 | 1.254# (1.238 –1.271) | 0.842# (0.831 –0.854) |
| 2012 | 38,533,299 | 99,660 | 258 | 18,649,334 | 42,662 | 229 | 19,883,965 | 56,938 | 286 | 1.252# (1.237 –1.268) | 0.836# (0.826 –0.847) |
| 2013 | 38,495,659 | 97,906 | 254 | 18,629,535 | 42,353 | 227 | 19,866,124 | 55,553 | 280 | 1.231# (1.215 –1.246) | 0.823# (0.813 –0.834) |
| 2014 | 38,478,602 | 99,420 | 258 | 18,619,809 | 43,418 | 233 | 19,858,793 | 56,002 | 282 | 1.212# (1.197 –1.227) | 0.822# (0.812 –0.833) |
| 2015 | 38,437,239 | 100,485 | 261 | 18,597,991 | 44,438 | 239 | 19,839,248 | 56,047 | 283 | 1.183# (1.168 –1.198) | 0.796# (0.786 –0.807) |
| 2016 | 38,432,992 | 101,348 | 264 | 18,593,166 | 45,366 | 244 | 19,839,826 | 55,982 | 282 | 1.189# (1.174 –1.204) | 0.782# (0.772 –0.792) |
| 2017 | 38,433,558 | 102,236 | 266 | 18,593,175 | 46,167 | 248 | 19,840,383 | 56,069 | 283 | 1.105# (1.092 –1.119) | 0.774# (0.764 –0.783) |
| 2018 | 38,411,148 | 101,432 | 264 | 18,581,886 | 46,264 | 249 | 19,829,262 | 55,168 | 278 | 1.155# (1.141 –1.170) | 0.806# (0.796 –0.817) |
| 2019 | 38,382,576 | 103,331 | 269 | 18,567,052 | 47,190 | 254 | 19,815,524 | 56,141 | 283 | 1.115# (1.101 –1.129) | 0.769# (0.759 –0.778) |
*The prevalence calculated per 100,000. #p < 0.001.
Table 2
Prevalence of Parkinson’s disease across different age groups for men and women in Poland
| Year | Sex | Age | Population | Number of people with | Estimated |
| group | ICD-10 code G20 | prevalence per | |||
| (Parkinson’s disease) | 100,000 population | ||||
| 2010 | F | 0–17 | 3,531,399 | 107 | 3 |
| 18–20 | 774,383 | 75 | 10 | ||
| 21–50 | 8,338,237 | 1,528 | 18 | ||
| 51–60 | 3,015,180 | 3,491 | 116 | ||
| 61–70 | 1,916,945 | 8,622 | 450 | ||
| 70+ | 2,300,597 | 35,898 | 1,560 | ||
| M | 0–17 | 3,711,840 | 152 | 4 | |
| 18–20 | 808,656 | 75 | 9 | ||
| 21–50 | 8,523,326 | 1,819 | 21 | ||
| 51–60 | 2,810,128 | 4,114 | 146 | ||
| 61–70 | 1,548,909 | 8,102 | 523 | ||
| 70+ | 1,250,266 | 23,051 | 1,844 | ||
| 2011 | F | 0–17 | 3,483,048 | 122 | 4 |
| 18–20 | 743,535 | 78 | 10 | ||
| 21–50 | 8,317,206 | 1,459 | 18 | ||
| 51–60 | 2,998,319 | 3,367 | 112 | ||
| 61–70 | 2,011,278 | 9,057 | 450 | ||
| 70+ | 2,330,484 | 38,286 | 1,643 | ||
| M | 0–17 | 3,663,503 | 142 | 4 | |
| 18–20 | 776,615 | 75 | 10 | ||
| 21–50 | 8,508,594 | 1,702 | 20 | ||
| 51–60 | 2,798,446 | 3,923 | 140 | ||
| 61–70 | 1,638,346 | 8,773 | 535 | ||
| 70+ | 1,269,073 | 24,577 | 1,937 | ||
| 2012 | F | 0–17 | 3,442,368 | 87 | 3 |
| 18–20 | 710,611 | 56 | 8 | ||
| 21–50 | 8,306,388 | 1,393 | 17 | ||
| 51–60 | 2,951,924 | 3,272 | 111 | ||
| 61–70 | 2,125,690 | 9,615 | 452 | ||
| 70+ | 2,346,984 | 42,515 | 1,811 | ||
| M | 0–17 | 3,624,400 | 124 | 3 | |
| 18–20 | 740,198 | 61 | 8 | ||
| 21–50 | 8,502,210 | 1,705 | 20 | ||
| 51–60 | 2,763,303 | 4,136 | 150 | ||
| 61–70 | 1,738,778 | 9,344 | 537 | ||
| 70+ | 1,280,445 | 27,292 | 2,131 | ||
| 2013 | F | 0–17 | 3,406,419 | 70 | 2 |
| 18–20 | 677,799 | 43 | 6 | ||
| 21–50 | 8,288,324 | 1,263 | 15 | ||
| 51–60 | 2,892,464 | 3,078 | 106 | ||
| 61–70 | 2,251,310 | 9,824 | 436 | ||
| 70+ | 2,349,808 | 41,275 | 1,757 | ||
| M | 0–17 | 3,588,943 | 72 | 2 | |
| 18–20 | 705,642 | 48 | 7 | ||
| 21–50 | 8,487,592 | 1,478 | 17 | ||
| 51–60 | 2,715,033 | 3,961 | 146 | ||
| 61–70 | 1,848,933 | 9,747 | 527 | ||
| 70+ | 1,283,392 | 27,047 | 2,107 | ||
| 2014 | F | 0–17 | 3,380,346 | 87 | 3 |
| 18–20 | 647,744 | 44 | 7 | ||
| 21–50 | 8,266,258 | 1,220 | 15 | ||
| 51–60 | 2,828,145 | 3,034 | 107 | ||
| 61–70 | 2,378,158 | 10,125 | 426 | ||
| 70+ | 2,358,142 | 41,492 | 1,760 | ||
| M | 0–17 | 3,562,650 | 89 | 2 | |
| 18–20 | 675,325 | 44 | 7 | ||
| 21–50 | 8,468,003 | 1,462 | 17 | ||
| 51–60 | 2,662,799 | 3,740 | 140 | ||
| 61–70 | 1,959,960 | 10,393 | 530 | ||
| 70+ | 1,291,072 | 27,690 | 2,145 | ||
| 2015 | F | 0–17 | 3,359,862 | 89 | 3 |
| 18–20 | 618,627 | 35 | 6 | ||
| 21–50 | 8,242,307 | 1,138 | 14 | ||
| 51–60 | 2,757,525 | 2,854 | 103 | ||
| 61–70 | 2,499,417 | 10,622 | 425 | ||
| 70+ | 2,361,510 | 41,309 | 1,749 | ||
| M | 0–17 | 3,541,933 | 87 | 2 | |
| 18–20 | 646,907 | 46 | 7 | ||
| 21–50 | 8,442,872 | 1,408 | 17 | ||
| 51–60 | 2,604,223 | 3,629 | 139 | ||
| 61–70 | 2,065,314 | 11,247 | 545 | ||
| 70+ | 1,296,742 | 28,021 | 2,161 | ||
| 2016 | F | 0–17 | 3,357,327 | 50 | 1 |
| 18–20 | 595,320 | 28 | 5 | ||
| 21–50 | 8,215,290 | 1,074 | 13 | ||
| 51–60 | 2,672,915 | 2,695 | 101 | ||
| 61–70 | 2,629,497 | 10,838 | 412 | ||
| 70+ | 2,369,477 | 41,297 | 1,743 | ||
| M | 0–17 | 3,538,551 | 61 | 2 | |
| 18–20 | 624,889 | 33 | 5 | ||
| 21–50 | 8,413,904 | 1,361 | 16 | ||
| 51–60 | 2,531,344 | 3,465 | 137 | ||
| 61–70 | 2,178,337 | 11,904 | 546 | ||
| 70+ | 1,306,141 | 28,542 | 2,185 | ||
| 2017 | F | 0–17 | 3,369,155 | 47 | 1 |
| 18–20 | 573,746 | 25 | 4 | ||
| 21–50 | 8,184,624 | 1,008 | 12 | ||
| 51–60 | 2,590,117 | 2,575 | 99 | ||
| 61–70 | 2,698,214 | 10,959 | 406 | ||
| 70+ | 2,424,527 | 41,455 | 1,710 | ||
| M | 0–17 | 3,551,497 | 54 | 2 | |
| 18–20 | 601,860 | 26 | 4 | ||
| 21–50 | 8,383,366 | 1,349 | 16 | ||
| 51–60 | 2,459,724 | 3,273 | 133 | ||
| 61–70 | 2,243,591 | 12,217 | 545 | ||
| 70+ | 1,353,137 | 29,248 | 2,161 | ||
| 2018 | F | 0–17 | 3,375,681 | 37 | 1 |
| 18–20 | 558,244 | 19 | 3 | ||
| 21–50 | 8,149,016 | 919 | 11 | ||
| 51–60 | 2,504,043 | 2,332 | 93 | ||
| 61–70 | 2,748,915 | 10,759 | 391 | ||
| 70+ | 2,493,363 | 41,102 | 1,648 | ||
| M | 0–17 | 3,559,842 | 43 | 1 | |
| 18–20 | 586,060 | 22 | 4 | ||
| 21–50 | 8,345,961 | 1,192 | 14 | ||
| 51–60 | 2,386,330 | 3,080 | 129 | ||
| 61–70 | 2,292,062 | 12,179 | 531 | ||
| 70+ | 1,411,631 | 29,748 | 2,107 | ||
| 2019 | F | 0–17 | 3,381,734 | 31 | 1 |
| 18–20 | 546,554 | 22 | 4 | ||
| 21–50 | 8,103,468 | 896 | 11 | ||
| 51–60 | 2,427,490 | 2,153 | 89 | ||
| 61–70 | 2,778,757 | 10,654 | 383 | ||
| 70+ | 2,577,521 | 42,385 | 1,644 | ||
| M | 0–17 | 3,566,972 | 45 | 1 | |
| 18–20 | 573,176 | 14 | 2 | ||
| 21–50 | 8,299,910 | 1,123 | 14 | ||
| 51–60 | 2,320,514 | 2,948 | 127 | ||
| 61–70 | 2,323,615 | 12,056 | 519 | ||
| 70+ | 1,482,865 | 31,004 | 2,091 |
M, male; F, female.
In 2019, the prevalence of early-onset PD, defined as an age of onset between 21 and 50 years, was 11 per 100,000 for women and 14 per 100,000 for men, representing 2.0% of all PD cases with an overall prevalence of 12.3 per 100,000. In contrast, in 2010 the prevalence was 18 per 100,000 for women and 21 per 100,000 for men, representing 3.8% of all PD cases, with an overall prevalence of 19.8 per 100,000. The PRR was 0.63 (95% CI: 0.59 –0.68, p < 0.001) for men and 0.60 (95% CI: 0.56 –0.66, p < 0.001) for women.
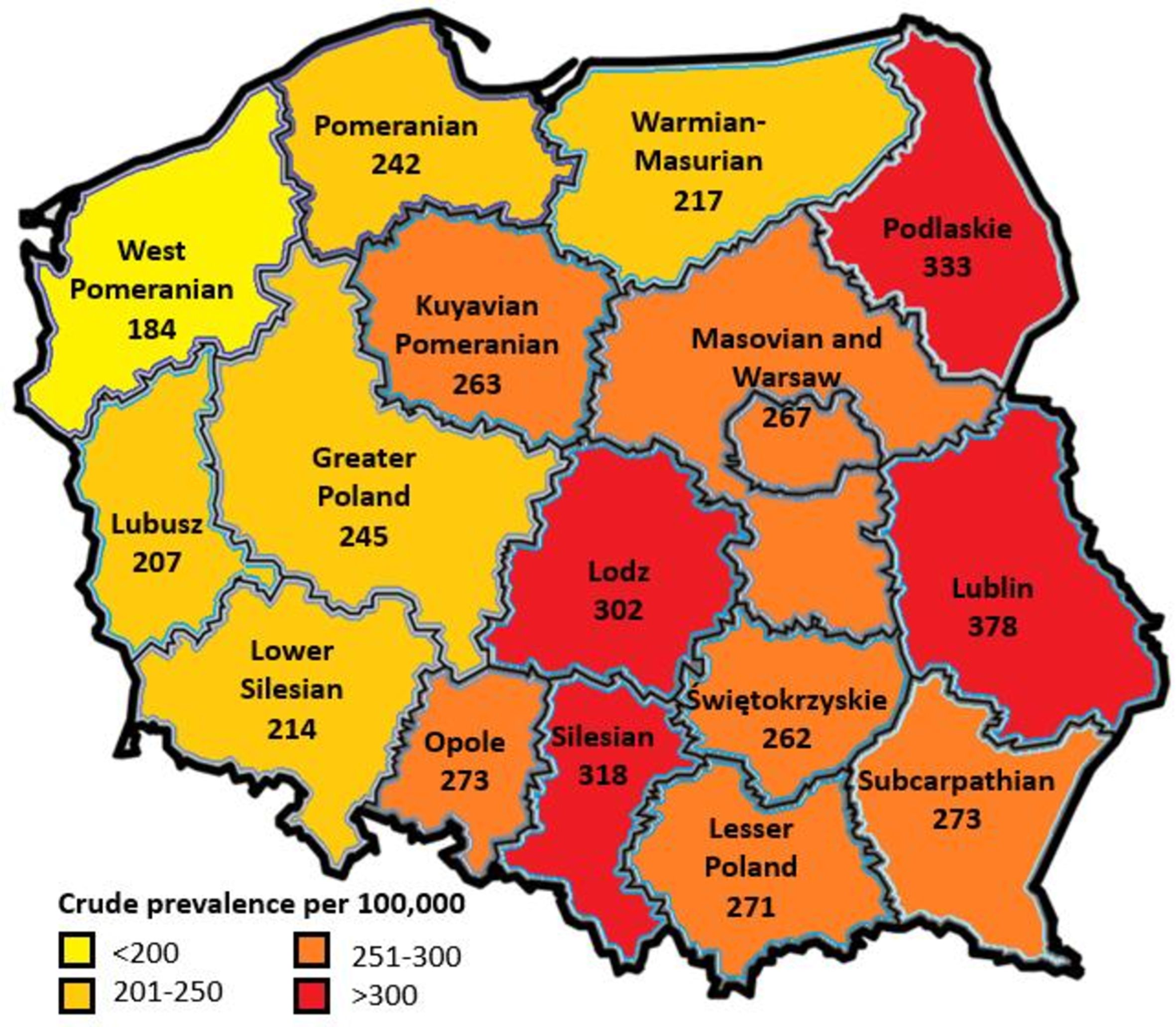
Finally, we looked at regional differences in PD prevalence in 2019. Although we did not observe differences at a group level (p = 0.45), post-hoc analysis showed that the crude PD prevalence was significantly different between the regions with the highest prevalence (the Lublin and Podlaskie regions) compared to regions with the lowest prevalence (the West Pomeranian and Lubusz regions) (p≤0.05; Fig. 2). To explore possible reasons behind these regional differences we performed univariate analyses looking at the relationship between regional PD prevalence rates and regional percentage of people who never smoked (stratified for sex), regional life expectancy, as well as the number of neurologists per region (to identify possible diagnostic bias). After correction for multiple testing (p = 0.05/5 = 0.01) we did not observe significant correlations between regional PD prevalence figures and the number of neurologists per region (β= 0.327; p = 0.217), regional life expectancy (β= 0.267, p = 0.318 for men, and β= 0.359, p = 0.172 for women), or percentage of male non-smokers (β= 0.083, p = 0.761), although a trend towards statistical significance was observed for female non-smokers (β= 0.558, p = 0.025).
Fig. 2
Regional distribution of Parkinson’s disease crude prevalence in Poland for the year 2019. Numbers represent prevalence per 100,000 inhabitants. The map used in this figure was created through MapChart (https://www.mapchart.net).
DISCUSSION
This is the first study aiming to assess the overall and region-specific prevalence of PD in Poland. The main findings from this data analysis are: 1) the data suggest that PD prevalence in Poland has increased over the period 2010 to 2019; 2) PD appears to be more prevalent in women in Poland than in men; and 3) PD prevalence shows regional differences across Poland. While our analyses have not provided a clear rationale for these three observations, they do point out an interesting trend. If we assume that PD prevalence in Poland follows the broader pattern seen in other European countries, the unique nature of points 2 and 3 becomes more pronounced. This divergence from the common European trends adds to the distinctiveness of the situation in Poland.
The prevalence of PD generally ranges from between 1 and 2 per 1,000 in unselected populations [17]. Other estimates put the PD prevalence around 0.3% of the entire population and around 1% of the population above 60 years [18, 19]. These estimates are in line with our findings for Poland where we showed an estimated crude prevalence ranging between 226 (for men) and 269 (for women) per 100,000 inhabitants over the years 2010–2019. Moreover, in 2019, approximately 0.8% (for men) to 0.9% (for women) of those aged 60 or above were affected. Notably, PD prevalence increased consistently for both genders during this period. Are findings related to early onset PD are similar to other European countries [20]. Whether these might have been related to specific gene mutations remains unclear due to the nature of the data used. In the Polish population, only a limited number of positive results have been reported in genes that have previously been associated with PD. Notably, in genetic studies involving 150 patients with early-onset Parkinson’s disease (defined as the onset of PD before the age of 45), mutations were exclusively identified in the PARK2 and PINK1 genes, with frequencies of 4.7% and 2.7%, respectively [21, 22]. Therefore, environmental factors may be of greater importance for PD prevalence in general, particularly when it comes to gene-environment interactions (virtually all known Parkinson genes interact in some way with environmental toxicants such as pesticides) [23]. As PD links to heightened pesticide usage [2, 24], it is interesting to note that the use of pesticides in Poland has increased significantly substantially over the last 20 years. Specifically, according to the Food and Agriculture Organization of the United Nations, pesticide use in kilogram per capita in Poland increased from approximately 0.15 in 1990 to 0.7 in 2021, in line with an increase in Eastern Europe overall from 0.3 to 0.6, while the use of pesticide in Western Europe decreased from 0.8 to 0.7 [25]. It may be assumed that, based on this rise, a further in PD prevalence is likely to occur in the future. Of note, better diagnostic skills appear not to be a good explanation for the rise in PD, because other neurological conditions for which the diagnostic ancillary tests have changed dramatically in the past decades (such as multiple sclerosis) do not show such a rise in incidence or prevalence, in contrast to PD which is still largely diagnosed in very much the way it was diagnosed over 200 years ago by James Parkinson [3, 26].
Another intriguing observation is the elevated PD prevalence among women in comparison to men. However, within the 70+ age group, females outnumbered males (1.73 times more in 2010 and 1.62 times more in 2019). Conversely, among younger groups, gender ratios were similar, necessitating consideration of a possible Simpson Paradox [27]. Similar trends have been noted in East Asian countries like Japan, South Korea, and Kazakhstan in Central Asia [28–31], challenging the assumption that PD prevalence is invariably 1.5 times higher in men [7]. Our analyses do not unravel the reasons behind these sex-specific disparities, but multiple factors might contribute. Local variations in occupational distribution could play a role, such as a relatively high percentage of female farmers in Poland. In fact, Poland is 4th among the European countries with the highest number of female farmers (over 40% of the farming work force) [32], aligning with findings in Japan and South Korea, and suggesting a higher proportionate exposure to pesticides among Polish women compared to other countries. Furthermore, the higher proportion of women (110 : 100 ratio) in many post-communist countries in Eastern Europe due to significantly shorter male lifespans might also be a contributing factor [33], although we did not find an association between life expectancy and PD prevalence across regions. Significantly, considering the regional disparities we have observed, the degree of feminization in densely populated regions in southern Poland and the Mazovian region is of interest. Conversely, the eastern regions, characterized by rural dominance and the absence of major cities, exhibit lower levels of feminization [34].
Taking into consideration the hypothesis that the higher prevalence of PD in rural areas is related to pesticides, air pollution may play a similar role in urban settings. According to the World Bank Group, 36 of the 50 most polluted cities in the European Union are in Poland [35]. Moreover, Polish cities are among the urban areas with the highest estimated mortality due to particulate matter pollution [36]. Air pollution is a significant risk factor for various diseases, including PD, and it might contribute significantly to global cases. Recent epidemiological studies support a link between PD and air pollution, prompting further investigation into a potential cause. Multiple potential mechanisms are being explored to understand how air pollution could facilitate neurodegeneration, and it is probable that multiple disease-related pathways are implicated. Given the widespread impact on individuals worldwide and the likelihood of shared pathological pathways with other disorders like Alzheimer’s disease, a deeper comprehension of this field is imperative. This should include factors that we were not able to include in the current analyses, such as caffeine intake, diet, and head trauma. Such insights can play a pivotal role due to the extensive global prevalence of these conditions and can lead to enhanced strategies for reducing incidence rates and developing more effective therapies that target the underlying causes [37].
The other observation of note in our findings is the regional difference in PD prevalence, with variation between different Polish regions. We have to interpret this finding cautiously as the primary analysis showed no overall regional difference, and the regional disparity was only found in a post-hoc analysis comparing the regions with the highest versus the lowest prevalence. Here, environmental pollution, as already outlined above, might play a role in the occurrence of PD [38], coinciding with high pollution rates in the Polish regions of Silesia, Lesser Poland, Lower Silesia, Ł⊙dź, and Masovia [39], where we observed some of the highest PD prevalence among Polish regions. On the other hand, the Podlaskie or Lodzkie regions also had high PD prevalence rates, but these are only relatively weakly industrialized, while low prevalence rates of PD also appeared in heavily industrialized regions such as West Pomerania and the Lubuskie region [40]. Moreover, in some of the regions with the highest PD prevalence, air pollution appears not to be pronounced [41], except for pollution associated with residential heating as its distribution appears to coincide with the regions showing the highest PD prevalence [42]. In turn, inhabitants of rural areas may be exposed to high pollution despite living in relatively unindustrialized regions [42], as reflected by a study by Dorsey et al. who recently suggested a link between trichloroethylene exposure and PD. Poland has been identified as one of the countries with published groundwater TCE contamination [38], but it shows a fairly even distribution across the country. In these rural areas the exposure to pesticides, as an often-cited cause of PD, would also be expected to be higher [1, 10–13]. Finally, regional differences in smoking rates may influence PD prevalence given its well-known risk-reducing nature for the development of PD. Although it failed to the reach statistical significance, we did observe a trend for higher percentages of non-smoking amongst women to be associated with higher regional PD prevalence rates. Nonetheless, it is likely that risk factors for the development of PD are diverse, and the epidemiological data presented here reflect their simultaneous interplay.
It is important to acknowledge the strengths and limitations of the current analysis. Firstly, we were only able to study prevalence in the dataset used and were unable to comment on the incidence of PD in Poland. Secondly, we used publicly available data, capturing registered diagnoses recorded for reimbursement of medical care. As such, the PD prevalence that we calculated may have been an underestimate of the actual prevalence as not every person with PD symptoms and without a formal diagnosis might have sought medical help. Moreover, from the database, it becomes clear that some people under the age of 18 received a diagnosis of PD, which according to current criteria and guidelines would likely represent a miscoding and we feel these should have been coded as parkinsonism. Additionally, we were unable to specify types of pesticides as this information is not contained within the Food and Agriculture Organization of the United Nations database. We were also not informed about who made the diagnosis of PD. However, the way in which PD was diagnosed in the past decade has not changed in Poland, therefore regardless of who made the diagnosis, it is unlikely that this factor explains the time trends that was noted in the publication. Finally, we were not informed about the distribution of people across rural and urban places of habitation, nor about the distribution and impact of several other potential risk factors. Nonetheless, given our structured approach, we feel our data are meaningful, also given that the identified prevalence rates were in line with general prevalence rates for PD.
In summary, here we estimated the prevalence of PD in Poland and showed that this prevalence is in line with previously reported prevalence rates across Europe. However, unlike most other European countries, PD seemed more prevalent in women than in men in Poland, although in those above 70 years, this ratio changed, and PD was more prevalent in men. Further studies are needed to understand the causes specific to Poland driving these sex-specific and region-specific PD prevalence rates. International collaboration, similar to the one happening in other areas of PD research in Poland [43], are likely to be key.
ACKNOWLEDGMENTS
We thank Beata Koń for the assistance that contributed to the development of this paper. The opinions expressed in this publication are those of the authors/researchers and do not necessarily reflect the official views of the National Health Fond of Poland. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, or the Department of Health. We thank Prof. Ray Chaudhuri for his review and critique.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
KS has received honoraria from European Academy of Neurology, International Parkinson and Movement Disorder Society, AbbVie, Pfizer and Polish Brain Disease Foundation.
ERD has received honoraria from American Neurological Association, Elsevier, International Parkinson and Movement Disorder Society, Massachusetts Medical Society, Michael J. Fox Foundation, National Institutes of Health, National Multiple Sclerosis Society, Northwestern University, Patient-Centered Outcomes Research Institute, Stanford University, Sutter Health, Texas Neurological Society. He is consulting for Abbott, AbbVie, Acadia, Acorda Therapeutics, Biogen, Biohaven Pharmaceuticals, BioSensics, Boehringer Ingelheim, Caraway Therapeutics, Cerevance, CuraSen, DConsult2, Denali Therapeutics, Eli Lilly, Genentech, Health & Wellness Partners, HMP Education, Karger, KOL groups, Life Sciences, Consultant, Mediflix, Medrhythms, Merck, MJH Holdings, NACCME, Novartis, Otsuka, Praxis Medicine, Sanofi, Seelos Therapeutics, Spark Therapeutics, Springer, Healthcare, Theravance Biopharmaceuticals, WebMD. He recived grants from Averitas, Pharma, Biogen, Burroughs Wellcome Fund, Michael J. Fox Foundation, National Institutes of Health, Pfizer, Photopharmics, Roche, Safra Foundation. Ownership interests Included Health, Mediflix, SemCap, Synapticure.
BRB serves as co-Editor-in-Chief of this journal, but was not involved in the peer-review process of this article nor had access to any information regarding its peer review. He is on the editorial board of Practical Neurology and Digital Biomarkers, has received honoraria from being on the scientific advisory board for Abbvie, Biogen, and UCB, has received fees for speaking at conferences from AbbVie, Zambon, Roche, GE Healthcare, and Bial, and has received research support from the Netherlands Organization for Scientific Research, the Michael J. Fox Foundation, UCB, Not Impossible, the Hersenstichting Nederland, the Parkinson’s Foundation, Verily Life Sciences, Horizon 2020, and the Parkinson Vereniging (all paid to the institute).
DvW has received a travel grant and speaker fees from Bial, as well as speaker fees from Britannia Pharmaceuticals, and is supported by a research grant from CHDI.
All other authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article.
REFERENCES
[1] | Wirdefeldt K , Adami HO , Cole P , Trichopoulos D , Mandel J ((2011) ) Epidemiology and etiology of Parkinson’s disease: A review of the evidence. Eur J Epidemiol 26 Suppl 1: , 1–58. |
[2] | Guehl D , Bezard E , Dovero S , Boraud T , Bioulac B , Gross C ((1999) ) Trichloroethylene and parkinsonism: A human and experimental observation. Eur J Neurol 6: , 609–611. |
[3] | Dorsey R , Sherer T , Okun MS , Bloem BR (2020) Ending Parkinson’s disease: A prescription for action, Hachette, UK. |
[4] | Rose F (2013) James Parkinson his Life and Times, Springer Science & Business Media. |
[5] | ((2017) ) Global, regional, and national burden of neurological disorders during 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol 16: , 877–897. |
[6] | ((2018) ) Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 17: , 939–953. |
[7] | Pringsheim T , Jette N , Frolkis A , Steeves TD ((2014) ) The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov Disord 29: , 1583–1590. |
[8] | Dorsey ER , Bloem BR ((2018) ) The Parkinson pandemic-a call to action. JAMA Neurol 75: , 9–10. |
[9] | Belvisi D , Pellicciari R , Fabbrini A , Costanzo M , Pietracupa S , De Lucia M , Modugno N , Magrinelli F , Dallocchio C , Ercoli T , Terravecchia C , Nicoletti A , Solla P , Fabbrini G , Tinazzi M , Berardelli A , Defazio G ((2020) ) Risk factors of Parkinson disease: Simultaneous assessment, interactions, and etiologic subtypes. Neurology 95: ,e2500–e2508. |
[10] | Richardson JR , Shalat SL , Buckley B , Winnik B , O’Suilleabhain P , Diaz-Arrastia R , Reisch J , German DC ((2009) ) Elevated serum pesticide levels and risk of Parkinson disease. Arch Neurol 66: , 870–875. |
[11] | Dick FD ((2006) ) Parkinson’s disease and pesticide exposures. Br Med Bull 79: , 219–231. |
[12] | Van Der Mark M , Brouwer M , Kromhout H , Nijssen P , Huss A , Vermeulen R ((2012) ) Is pesticide use related to Parkinson disease? Some clues to heterogeneity in study results. Environ Health Perspect 120: , 340–347. |
[13] | Elbaz A , Clavel J , Rathouz PJ , Moisan F , Galanaud JP , Delemotte B , Alpéerovitch A , Tzourio C ((2009) ) Professional exposure to pesticides and Parkinson disease. Ann Neurol 66: , 494–504. |
[14] | Barbeau A , Roy M , Bernier G , Campanella G , Paris S ((1987) ) Ecogenetics of Parkinson’s disease: Prevalence and environmental aspects in rural areas. Can J Neurol Sci 14: , 36–41. |
[15] | Hugh-Jones ME , Peele RH , Wilson VL ((2020) ) Parkinson’s disease in Louisiana, 1999–2012: Based on hospital primary discharge diagnoses, incidence, and risk in relation to local agricultural crops, pesticides, and aquifer recharge. Int J Environ Res Public Health 17: , 1584. |
[16] | Polakowska M , Piotrowski W , Tykarski A , Drygas W , Wyrzykowski B , Pająk A , Kozakiewicz K , Rywik S ((2005) ) Nałóg palenia tytoniu w populacji polskiej. Wyniki programu WOBASZ. Kardiol Pol 63: (Suppl 4), S1–S6. |
[17] | von Campenhausen S , Bornschein B , Wick R , Bötzel K , Sampaio C , Poewe W , Oertel W , Siebert U , Berger K , Dodel R ((2005) ) Prevalence and incidence of Parkinson’s disease in Europe. Eur Neuropsychopharmacol 15: , 473–490. |
[18] | de Lau LM , Breteler MM ((2006) ) Epidemiology of Parkinson’s disease. Lancet Neurol 5: , 525–535. |
[19] | Nussbaum RL , Ellis CE ((2003) ) Alzheimer’s disease and Parkinson’s disease. N Engl J Med 348: , 1356–1364. |
[20] | Post B , Van Den Heuvel L , Van Prooije T , Van Ruissen X , Van De Warrenburg B , Nonnekes J ((2020) ) Young onset Parkinson’s disease: A modern and tailored approach. , S29-S. J Parkinsons Dis 10: , S29–S36. |
[21] | Koziorowski D , Hoffman-Zacharska D , Sławek J , Jamrozik Z , Janik P , Potulska-Chromik A , Roszmann A , Tataj R , Bal J , Friedman A ((2013) ) Incidence of mutations in the PARK2, PINK1, PARK7 genes in Polish early-onset Parkinson disease patients. Neurol Neurochir Pol 47: , 319–324. |
[22] | Turski P , Chaberska I , Szukało P , Pyska P , Milanowski Ł , Szlufik S , Figura M , Hoffman-Zacharska D , Siuda J , Koziorowski D ((2022) ) Review of the epidemiology and variability of LRRK2 non-p.Gly2019Ser pathogenic mutations in Parkinson’s disease. Front Neurosci 16: , 971270. |
[23] | Bogers JS , Bloem BR , Den Heijer JM ((2023) ) The etiology of Parkinson’s disease: New perspectives from gene-environment interactions. J Parkinsons Dis 13: , 1281–1288. |
[24] | Huber F ((1969) ) [Clinical aspects and neuropathology of trichloroethylene poisoning]. Z Unfallmed Berufskr 62: , 226–267. |
[25] | Food and Agriculture Organization of the United Nations. FAOSTAT: Pesticides Use.https://www.fao.org/faostat/en/#data/RP . Last updated July 14. |
[26] | Parkinson J (1817) An Essay on the Shaking Palsy, Whittingham & Rowland. |
[27] | Hernán MA , Clayton D , Keiding N ((2011) ) The Simpson’s paradox unraveled. Int J Epidemiol 40: , 780–785. |
[28] | Muangpaisan W , Hori H , Brayne C ((2009) ) Systematic review of the prevalence and incidence of Parkinson’s disease in Asia.. J Epidemiol 19: , 281–293. |
[29] | Lee JE , Choi J-k , Lim HS , Kim JH , Cho JH , Kim GS , Lee PH , Sohn YH , Lee JH ((2017) ) The prevalence and incidence of Parkinson’s disease in South Korea: A 10-year nationwide population–based study. J Korean Neurol Assoc 35: , 191–198. |
[30] | Kaiyrzhanov R , Zharkinbekova N , Shashkin C , Khaibullin T , Kaishibayeva G , Akhmetzhanov V , Sadykova DZ , Seidinova Z , Taskinbayeva A , Karimova A , Rizig M , Houlden H ((2020) ) Parkinson’s disease in Kazakhstan: Clinico-demographic description of a large cohort. J Parkinsons Dis 10: , 707–709. |
[31] | Kimura H , Kurimura M , Wada M , Kawanami T , Kurita K , Suzuki Y , Katagiri T , Daimon M , Kayama T , Kato T ((2002) ) Female preponderance of Parkinson’s disease in Japan. Neuroepidemiology 21: , 292–296. |
[32] | Eurostat. Women in total working population and in agriculture, 2016 (LFS).https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Women_in_total_working_population_and_in_agriculture,_2016_(LFS).png. |
[33] | Statistics Poland (2022) Rural areas in Poland 2020.https://stat.gov.pl/en/topics/agriculture-forestry/agriculture/rural-areas-in-poland-2020,3,5.html. |
[34] | Zintegrowana Platforma Edukacyjna Ministerstwa Edukacji i Nauki. Biologiczna struktura ludności Polski.https://zpe.gov.pl/a/biologiczna-struktura-ludnosci-polski/DoyDpyCa6. |
[35] | World Bank Group (2019) Air Quality in Poland, what are the issues and what can be done?https://documents1.worldbank.org/curated/en/426051575639438457/pdf/Air-Quality-in-Poland-What-are-the-Issues-and-What-can-be-Done.pdf . |
[36] | Khomenko S , Cirach M , Pereira-Barboza E , Mueller N , Barrera-Gómez J , Rojas-Rueda D , de Hoogh K , Hoek G , Nieuwenhuijsen M ((2021) ) Premature mortality due to air pollution in European cities: A health impact assessment. Lancet Planet Health 5: , e121–e134. |
[37] | Murata H , Barnhill LM , Bronstein JM ((2022) ) Air pollution and the risk of Parkinson’s disease: A review. Mov Disord 37: , 894–904. |
[38] | Dorsey ER , Zafar M , Lettenberger SE , Pawlik ME , Kinel D , Frissen M , Schneider RB , Kieburtz K , Tanner CM , De Miranda BR , Goldman SM , Bloem BR ((2023) ) Trichloroethylene: An invisible cause of Parkinson’s disease? . J Parkinsons Dis 13: , 203–218. |
[39] | Główny inspektorat ochrony środowiska. Bank danych pomiarowych. ,https://powietrze.gios.gov.pl/pjp/archives. |
[40] | Eurostat. Regions in Europe 2022 interactive edition. https://ec.europa.eu/eurostat/cache/digpub/regions/. |
[41] | Kaleta D ((2014) ) State of air pollution in Silesia province including low emission sources. Architecture Civil Eng Environ J7: , 79–87. |
[42] | Pokorná P , Schwarz J , Krejci R , Swietlicki E , Havránek V , Zdímal V ((2018) ) Comparison of PM(2.5) chemical composition and sources at a rural background site in Central Europe between 1993/1994/1995 and 2009/2010: Effect of legislative regulations and economic transformation on the air quality. Environ Pollut 241: , 841–851. |
[43] | Siuda J , Boczarska-Jedynak M , Budrewicz S , Figura M , Fiszer U , Gajos A , Gorzkowska A , Koziorowska-Gawron E , Koziorowski D , Krygowska-Wajs A , Rudzińska-Bar M , Sławek J , Ren X , Luo S , Martinez-Martin P , Stebbins G , Goetz CG , Opala G , Bogucki A , Dulski J , Janik P , Koszewicz M , Leńska-Mieciek M , Michałowska M , Piaścik-Gromada M , Potasz-Kulikowska K , Śmiłowski M , Wasielewska A , Wójcik-Pędziwiatr M ((2020) ) Validation of the Polish version of the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS). Neurol Neurochir Pol 54: , 416–425. |


