
Predicting Airway Invasion Using Screening Tools and Laryngeal Kinematics in People with Parkinson’s Disease: A Pilot Study
Abstract
Background:
Dysphagia in Parkinson’s disease (PD) is a common manifestation, particularly in advanced disease stages. However, the pathophysiology and time course of dysphagia progression remains unclear in non-advanced disease stages (e.g., Hoehn & Yahr stages I–III). Conflicting reports from investigations of the perception of dysphagia in people with PD further complicates our understanding of dysphagia in this population.
Objective:
The objectives of this research were to evaluate the ability of screening tools to detect swallowing impairments and how laryngeal kinematics predict the occurrence of abnormal swallowing events.
Methods:
14 individuals with non-advanced PD, no previous history of dysphagia diagnosis, and self-reported difficulty swallowing participated. The Swallow Disturbance Questionnaire (SDQ) and 3-oz water swallow test (WSST) were administered, along with a videoflouroscopic swallow study (VFSS). Laryngeal kinematics were represented by laryngeal vestibule closure reaction time (LVrt) and laryngeal vestibule closure duration (LVCd). The Penetration-Aspiration Scale (PAS) was used to quantify airway invasion.
Results:
A logistic regression indicated a significant model of predicting airway invasion from our predictors (p = 0.003). LVrt and SDQ (p < 0.05) provided the largest impact (OR = 1.11; 1.17). The WSST showed no significance in predicting swallow impairment (p > 0.05).
Conclusion:
Decreased airway safety related to laryngeal kinematic function in PD may be manifesting at non-advanced disease stages to varied degrees. Our results support expectations of dysphagia manifestation in PD although screening practices may not adequately identify impairment. Future research should target specific laryngeal characteristics within this population to better understand the physiological cause of swallowing impairment and developof targeted interventions.
INTRODUCTION
Dysphagia in people with Parkinson’s disease (PWPD) is associated with negative healthcare outcomes, decreased quality of life, and pneumonia secondary to aspiration. Aspiration pneumonia is a significant contributor to mortality rate in neurogenically impaired populations, especially in those with PD [1, 2]. Dysphagia is a public health concern, as it significantly increases costs for providers, increases the length of stay for inpatients, and decreases long-term health outcomes [3]. Studies have shown that delayed movement timing of swallow mechanics contributes to increased laryngeal penetration and aspiration in people with PWPD [4, 5]. These impairments are likely associated with the sensorimotor manifestations of PD among which include bradykinesia and akinesia [6]. It stands to reason that hypokinetic movements may impair swallow related muscular function and decrease swallowing safety in PWPD. Movements in PD can be substantially slowed, reduced in amplitude, and/or delayed. In swallowing this hypokinesia has been associated with reduced pharyngeal contraction for food bolus propulsion and delayed timing of laryngeal closure for airway protection [7].
Airway penetration and/or aspiration are often identified in PWPD, even with no or minimal complaints of swallowing difficulty [8, 9]. The pathophysiological cause of decreased swallow safety in this population is thought to be multifactorial including poor bolus control, decreased esophageal function, and somatosensory deficits [10, 11]. While laryngeal kinematics during swallowing, such as laryngeal vestibule closure reaction and duration times, are likely associated with dysphagia (specifically airway invasion) in PWPD, they have not been investigated until recently. Current evidence has shown that the timing of airway closure was the strongest predictor of airway invasion in non-advanced PD [12]. However, further knowledge of laryngeal function during swallowing in PWPD is needed to more fully inform our understanding of laryngeal impairment as the disease progresses and to inform treatment planning for rehabilitation of swallowing function.
There is evidence that the perception of swallowing impairment in PWPD is also impaired throughout the stages of disease progression. For example, while oropharyngeal dysphagia in non-advanced PD (e.g., Hoehn & Yahr stages I –III) may be present, many PWPD are unaware of their swallowing difficulties or their dysphagia symptoms may be self-perceived as “benign” [13]. This leaves the possibility of aspiration and subsequent sequelae as potential risks to health, even in non-advanced stages of the disease [14]. Dysphagia in non-advanced stages may also be present at rates higher than previously expected. A meta-analysis reported increases in dysphagia diagnosis post instrumental assessment despite there being no overt or subjectively reported dysphagia symptoms at pre-assessment [15]. Extant literature also supports the use of standardized measures for detection of swallowing impairment in PWPD in both advanced and non-advanced stages [16]. The potential lack of self-awareness in the perception of swallowing disturbances combined with increased evidence of penetration and/or aspiration in non-advanced stages supports the need to objectively determine if there are measures or means to better identify swallowing impairments in PWPD across the continuum of progression.
The purpose of the current pilot study was twofold. The first was to investigate the predictive ability of swallow screening tools for identifying dysphagia in PWPD in non-advanced stages. Our second purpose was to identify how specific laryngeal kinematics predict penetration and/or aspiration occurrence. We hypothesized that scores from a validated swallow questionnaire (Swallow Disturbance Questionnaire, SDQ) [16] and a conventional screening method (3 oz water swallow screening test, WSST) would be able to predict the occurrence of penetration and/or aspiration identified by instrumental assessment. We also hypothesized that participants in our sample would exhibit frequent occurrences of abnormal airway invasion as measured by the Penetration Aspiration Scale (PAS). We lastly hypothesized that laryngeal kinematics, specifically laryngeal vestibule closure reaction time (LVrt) and duration time (LVCd), would predict the occurrence of larger (abnormal) PAS scores.
MATERIALS AND METHODS
This study was approved by a university institutional review board (IRB). 14 individuals diagnosed with PD were recruited to participate. Inclusion criteria consisted of: 1) diagnosis of idiopathic PD by a neurologist, 2) current disease severity in stage I–III based on the original H & Y scale [17] which has been previously staged by the participants’ neurologist, 3) no previous diagnosis of dysphagia or treatment for dysphagia by a healthcare professional, 4) no comorbid neurological impairments not associated with PD, and 5) no history of pneumonia or other pulmonary/respiratory illness within the last two years. Participants were considered to have no prior history of dysphagia if there was no previous documentation of dysphagia evaluation or treatment contained in the patient records obtained in accordance with IRB protocols, which have been previously obtained as part of an ongoing program of research in our lab, as well as verbal confirmation by the subjects. Inclusion criteria also necessitated self-reports of dysphagia-symptoms on a swallowing symptom questionnaire and was completed by the participants during a previous visit to the research laboratory. This questionnaire consisted of several general symptoms potentially related to swallow dysfunction. The questionnaire asked participants how frequently they experienced the dysfunction presented, including items such as “Drooling” and “I cough when I eat solid foods”. If the participants identified experiencing at least one dysfunction, they were considered eligible for inclusion into the present study assuming all other inclusion criteria were met. Participants were required to complete all consenting procedures prior to enrolling in the study. All research activities took place on a university campus and a mobile radiography unit.
Participants completed a self-report questionnaire of their swallow function (SDQ), performed a 3 oz water swallow screen test, and completed a VFSS. Based on previous literature using the SDQ, the optimal score for detecting dysphagia in PD is 11 [16]. However, this number is nonspecific as individuals may only respond to important items regarding airway safety such as coughing frequently on liquids and solid foods, yet not score above the dysphagia cutoff score. The SDQ was therefore treated as a continuous measure where individuals may report their dysphagia on a continuum of symptoms, rather than needing to meet a cutoff.
For the 3 oz WSST, positive responses (suggestive of dysphagia) included (a) coughing, (b) throat clearing, and (c) wet, gurgling vocal quality were compared to baseline (e.g., prior to swallowing water). This was aligned with previous literature which utilized variations of the 3 oz WSST [3]. Participants were provided with 3 ounces of room temperature water via cup, as measured by syringe, and were cued to “drink the water as fast and as comfortably as they could on consecutive sips”. Previous research has investigated the application of swallowing speed with a water swallow protocol to detect airway invasion [18, 19, 20], but with inconsistent findings related to the measure of swallow speed during this test. Therefore, while we did not specifically measure swallow speed, the decreased synchrony of the respiratory-swallow pattern in PWPD [18, 21] may be used to identify episodes of aspiration causing an active airway response. Any positive sign of airway invasion related to throat clearing, coughing, or wet voicing after drinking were recorded as a “1”, while no signs exhibited were recorded as “0”.
For the VFSS, all participants were asked to consume three thin liquid bolus trials at increasing volumes (10, 15, and 20 mL), three trials of 1 tablespoon (tbsp) of pudding, and three trials of a regular food texture (for which a cookie was used) that were mixed and/or coated with barium (E-Z Paque). For the thin liquid bolus swallows, participants were instructed to place the whole bolus into their mouth, hold, and then swallow when ready. Pudding and regular texture boluses were administered to the participant but swallow timing was not cued, allowing patients to orally prepare the bolus that is typical for their everyday swallow performance.
All VFSS were conducted via a mobile swallowing/dysphagia assessment unit (Diagnostex, LLC, Hurst, TX) on the university campus in order to reduce additional travel burden for the participants. All studies were recorded at 30 frames per second (fps) in agreement with current literature [22]. All swallow studies were conducted by a trained Speech-Language Pathologist (SLP) who was blind to the conditions and purposes of this particular study. The principle investigator (PI) was present for all VFSS studies to maintain fidelity of the methodology. All swallow studies were recorded on de-identified digital recordings and analyzed at a later date.
Video analysis software Avidemux v. 2.7 was used to gather the kinematic measures of laryngeal movements. Two kinematic timing measures were obtained from the VFSS recordings: laryngeal vestibule closure reaction time (LVrt) and laryngeal vestibule closure duration (LVCd). These measurements have been utilized in previous studies to assess physiological timing events related to airway closure and protection during swallowing [23]. LVrt was operationally defined as beginning with (a) the initial and consistent anterior-superior burst of the hyoid and ending when (b) the arytenoids contacted the underside of the epiglottis and the maximum extent of laryngeal vestibule obstruction was observed. LVcD was defined as beginning at (a) the moment of maximum obstruction of the laryngeal vestibule was observed and ending when (b) the descent of the arytenoids from the underside of the epiglottis began, as seen by the reemergence of the vestibule. Both kinematic measurements, based on timing of movement, were treated as continuous variables for our analysis. The PAS [24] was applied to every swallow recording of each participant. The PAS measured the degree of laryngeal penetration and/or aspiration as judged by the depth of bolus material entering the airway. It has been used in previous literature to measure swallow safety in people with PD [4, 25]. All timing measurements were performed independently by the 1st author and a second trained assistant so that measures of inter- and intra-measurement reliability could be obtained (Table 1). 30% of swallows were chosen at random and remeasured by the second rater for all kinematic measures.
Table 1
Interrater and intrarater reliability for LVrt and LVcD
| Measurement (type) | ICC | 95% CI | Sig. (p-value) |
| LVrt (Inter) | 0.93 | 0.88 –0.97 | <0.001 |
| LVCd (Inter) | 0.94 | 0.91 –0.97 | <0.001 |
| LVrt (Intra) | 0.97 | 0.94 –0.99 | <0.001 |
| LVCd (Intra) | 0.98 | 0.97 –0.99 | <0.001 |
All statistical analyses were performed in SPSS (v. 24). Descriptive statistics were computed to identify demographic information including H&Y stage, age, LVrt, LVcD, and PAS scores. A standard entry logistic regression was performed to predict the probability of identifying laryngeal impairment as a function of the PAS from a preselected set of predictor variables including: the SDQ, the 3 oz WSST, LVrt, and LVcD. These predictor variables were specifically chosen a priori to be included into the analysis based on the projects aims and hypotheses. In order to conduct this analysis, PAS scores were coded to reflect either a “normal” and safe swallow (PAS score of 1 or 2), or “abnormal” (PAS score > 3). This method has been suggested as one of several appropriate approaches with a logistic regression [26] and used in recent work [12] to quantify the PAS. Receiver operating characteristics (ROC) analysis was then performed to produce an area under the curve (AUC) for sensitivity and specificity of screening methods (SDQ and 3 oz WSST) for predicting those who are at risk of dysphagia.
Reliability
A 30% randomly assigned remeasure of all kinematic timing measurements (LVrt and LVCd) was performed by a second, trained, independent rater for reliability measurement. A 30% remeasure was also performed by the 1st author to obtain intrarater reliability. Both inter- and intra-rater reliability for all timing measures were classified as excellent based on intraclass correlation coefficients (ICC) obtained. Reliability values are presented in Table 1.
RESULTS
A total of 135 swallows across the 14 participants were included in the analysis and no swallows were excluded. Descriptive statistics of the participant pool are shown in Table 2. A total of 7 males and 7 females with PD participated. Participants had a mean age of 66 years (SD±9.8), and a median H&Y stage of 2 (IQR = 1) (Table 2). 40% of swallows were considered abnormal (PAS score ≥3) and bolus material in 27% of these swallows either reached the level of the vocal folds or entered the trachea (PAS scores 4–8) [26]. Mean LVrt & LVCd were 0.42 seconds (SD±0.22) and 0.46 seconds (SD±0.22), respectively. There were no occurrences of incomplete laryngeal vestibule closure.
Table 2
Descriptive and demographic information
| Descriptive categories | Mean(±SD)/# of cases |
| Age | 66 (9.8) |
| Hoehn and Yahr Stage* | 2 (1) |
| Years post onset | 4.77 (1.9) |
| LVrt | 0.42 (0.22) |
| LVCd | 0.46 (0.22) |
| 3 oz Water Swallow Screen** | Positive response: n = 1 |
| Absent response: n = 13 | |
| SDQ scores | 6.2 (3.9) |
| PAS scores | 1–2: n = 81 |
| 3–8: n = 54 |
*Expressed as Median (Inter-Quartile Range); **Expressed in a positive response or absent response.
Table 3
Logistic regression model predicting swallow function
| Predictors | β | Wald | Sig. (p-value) | Odds ratio |
| LVrt | 2.18 | 4.12 | 0.042 | 1.11 |
| SDQ | 0.156 | 8.7 | 0.003 | 1.17 |
| LVCd | –0.53 | 0.37 | 0.55 | 0.11 |
| 3 oz WSST | –1.12 | 2.27 | 0.13 | 0.33 |
The regression model produced a significant result above the constant model, χ2 (4) = 15.99, p = 0.003, and Hosmer-Lemeshow Test of fit (χ2 = 6.5, p = 0.592) indicated that our predictive model accurately fit our data. Inspection of our correlation matrix to assess multicollinearity between our predictor variables indicated no R greater than 0.28. This indicated there were high correlations between predictor variables in the model, and we were able to move forward with interpretation of our analysis. Both LVrt (β= 2.18, p = 0.042, OR = 1.11) and the SDQ (β= 0.156, p = 0.003. OR = 1.17) contributed significantly to predicting abnormal swallow function in the sample. This indicated that in terms of screening tools, the SDQ showed a significant ability to predict airway invasion, while the 3 oz WSST (p > 0.05) did not. For kinematic measurements, these results indicated that LVrt was able to significantly contribute to predicting the occurrence of airway invasion while LVCd (p > 0.05) was not. A full model summary is provided in Table 2.
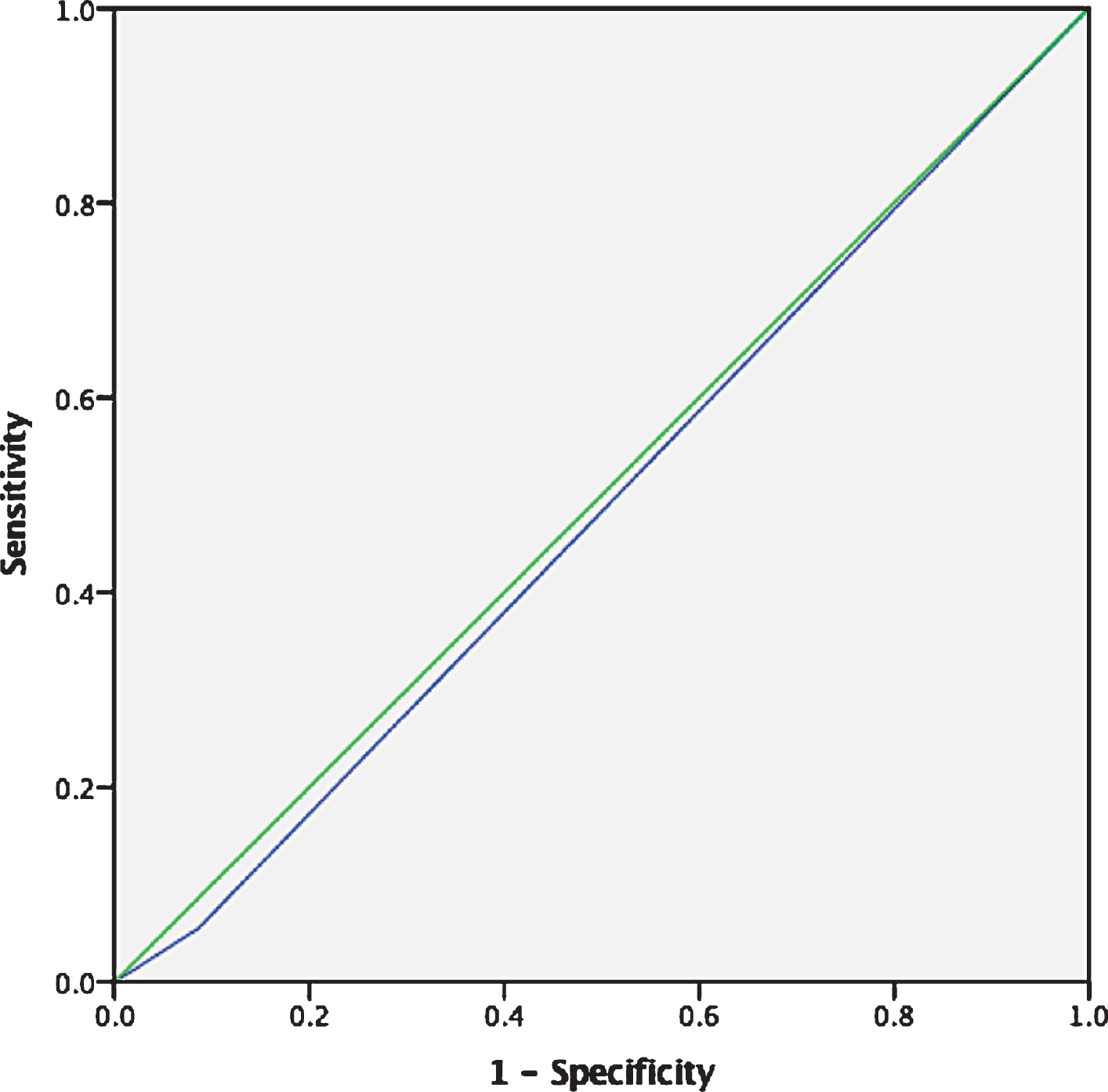
ROC (Fig. 1) analysis revealed a significant result and area under the curve for the SDQ of 0.67 (p < 0.001, 95% CI = 0.599 –0.836). This indicated that the SDQ was robust for identifying true positive states related to abnormal swallowing. Our ROC analysis for the 3 oz WSST (Fig. 2), however, indicated a nonsignificant result (A = 0.49, p > 0.05). This suggested that in this particular sample of participants, this water screen methodology was no better than chance at detecting the potential penetration and/or aspiration.
Fig. 1
AUC for SDQ detecting impaired swallow safety.
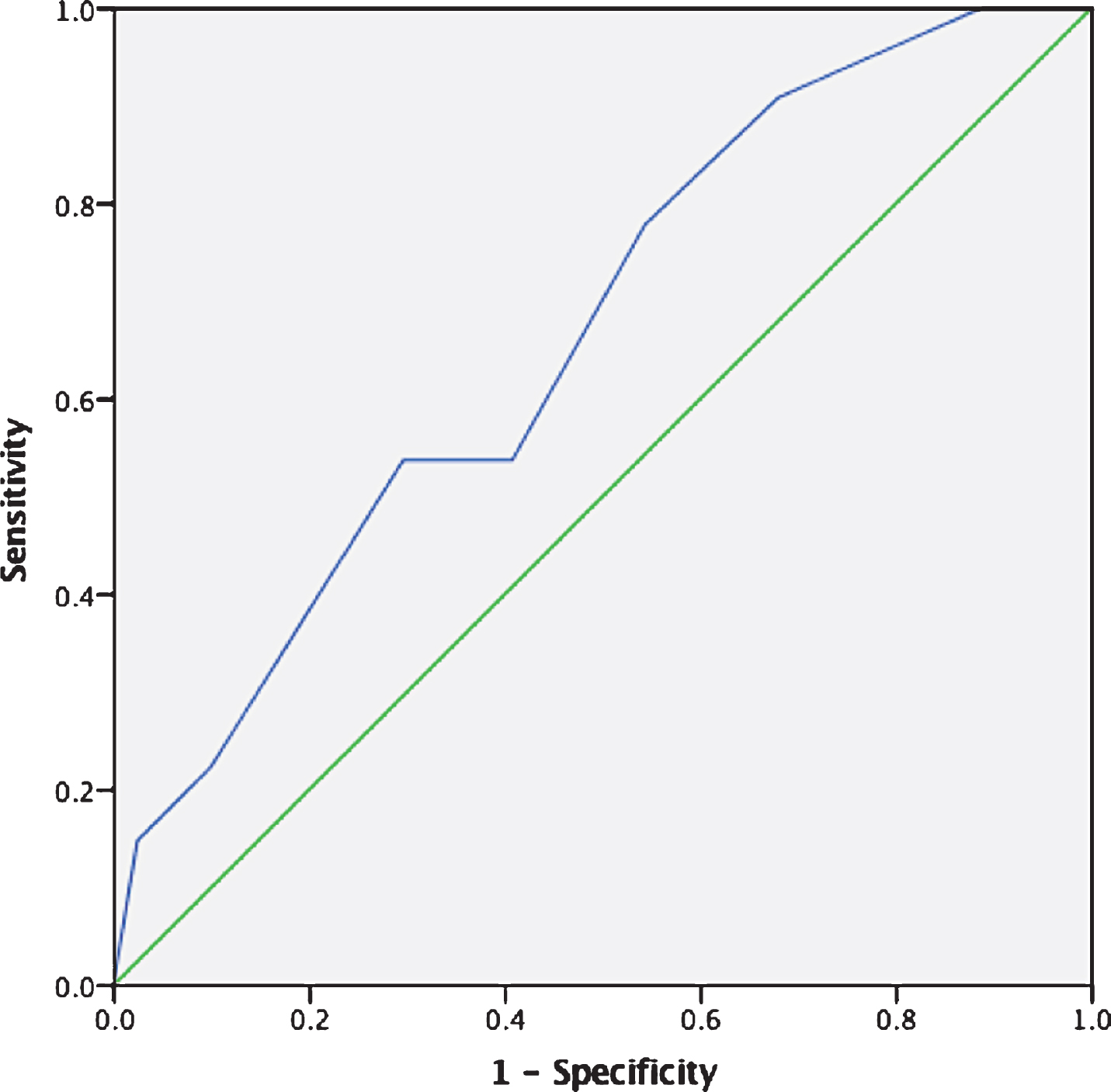
Fig. 2
AUC for 3 oz WSST detection of impaired swallow safety.
DISCUSSION
Questionnaire responses and VFSS findings
Dysphagia in non-advanced stages of PD can occurs without any subjective signs or reports of penetration or aspiration [27]. Evidence has shown that many individuals with PD, regardless of stage, are poor and inconsistent self-reporters of dysphagia symptoms unless sufficiently prompted to intentionally focus on the symptoms [28, 29]. Our study sought to investigate how specific, non-invasive screening methodologies (questionnaire and water screen) detected swallow safety related to laryngeal kinematics and penetration/aspiration in a population of PWPD at non-advanced disease stages.
Our findings showed that for every unit increase in perceptual SDQ scores there is a 17% increase in the odds of experiencing swallow impairment as confirmed with instrumental assessment. A mean SDQ score of 6 in our sample may indicate that while PWPD in non-advanced disease stages do not report a critical cutoff score of 11, swallow impairment characterized by impaired airway safety may be present. Nienstedt et al. [29] recently reported that when PWPD are provided with questions related to swallow function from typical assessments, they are unreliably and inconsistently reporting their symptoms. Questions utilized in published research have provided limited specificity of dysphagia symptomology. Questions that only include “difficulty with pills” and “voluntary diet alterations” [30] or broad queries of experience choking while swallowing [31] may not be sensitive to the range of swallowing symptoms experienced by PWPD. Despite different outcome measures, Andres et al. [32] reported that when PWPD indicated even a minimal degree of dysphagia when given the SDQ, 94% were measured as exhibiting swallow impairment. Results from our current study indicate a similar trend, that when PWPD are provided with more specific sets of symptoms within a questionnaire such as the SDQ, those who are experiencing dysphagia (as confirmed with instrumental assessment) are more likely to perceive and report the symptoms. This supports the need to include comprehensive methods of dysphagia assessments for PWPD in early disease stages.
Water swallow screen and VFSS results
The 3-ounce water swallow test has shown high sensitivity for detecting aspiration events in various neurodegenerative populations, including PWPD [33], and is recommended for inclusion in clinical swallow assessments related to PD such as the SCAS-PD [34]. A broad clinical swallow assessment such as the SCAS-PD is recommended to detect those at risk of aspiration. However, a precursor to a clinical swallow assessment in many settings is the use of a simple water screening, which can be administered by various healthcare professionals including SLP’s and nurses [35]. There are several variations of the water swallow screen test that may be used, which differ by either volume, consecutive or single sips, or other metrics [3]. Our results indicated that in non-advanced PD, the 3-ounce water swallow screen protocol implemented was not effective at identifying participants with impaired swallow safety. This supported the supposition that despite the water screen’s low-cost and easy administration, the use of a speed-based water swallow screen may not be effective for identifying PWPD in non-advanced stages who are experiencing dysphagia but have not yet been referred for formal diagnostic assessment. Our findings agree with Pflug et al. [19] that swallow speed ability in a water screen test does not accurately reflect dysphagia or aspiration risk. Different methodologies exploring volume may be more sensitive to detecting aspiration risk in PD [10]. Further studies with substantially larger participant samples are needed to further investigate this phenomenon in PWPD at non-advanced stages.
Airway invasion and laryngeal kinematics
Our findings indicated that a large proportion (40%) of swallows in this study were abnormal (PAS score ≥3) and of those abnormal swallows, 27% either reached the level of the vocal folds or entered the trachea (PAS scores 4–8). Literature has indicated that PAS scores of 1 and 2 are within normal limits, and in healthy older adults PAS scores >2 occur rarely [36]. A much higher rate of abnormal swallows even in a smaller sample suggested that changes in laryngeal and airway responses are present in non-advanced stages of PD. An important observation in this study was that penetration and aspiration events occurred multiple times across different swallows in multiple participants. Considering this and the large proportion of swallows that received “abnormal” PAS categorization, these results were likely not due to a single poor performer or isolated events.
Continuing research is needed to more fully understand the contribution of LVrt and LVCd to airway safety during swallowing in PWPD. Our findings showed that LVrt was a significant predictor for more severe penetration and aspiration events (e.g., higher PAS scores). Our OR (1.11) for LVrt indicated a small increase in the odds of an abnormal penetration or aspiration event (11%) with slower LVrt times. It is possible that the low OR is due to sample size as our findings agree with recent work by Curtis et al. [12]. Predictive models have also shown that other kinematic factors including hyolaryngeal movement are useful predictors for decreased airway safety in PWPD [37] and warrant further investigation.
The detection of abnormal swallowing and increased airway invasion in the non-advanced stages of PD contributes to the body of knowledge about dysphagia manifestation in this population. The identification of penetration and aspiration of material into the airway during swallowing could have a significant impact on screening approaches, assessment methods, and directions for future therapeutic research in PWPD at non-advanced stages. If dysphagia in PWPD results from a combination of impaired somatosensory responses coupled with slowed kinematic timing, results from our study suggest that these impairments are occurring at a substantial rate in PWPD at non-advanced stages, and across multiple swallows and bolus textures. Moreover, the current level of screening methodologies (i.e., 3 oz WSST) may not be sensitive enough to detect swallowing changes in this subgroup of PWPD. From a translational perspective, clinically relevant recommendations could include the use of a detailed questionnaire to gather patient perceptions of swallow function as part of a comprehensive swallow assessment. Future directions for research should include investigating other aspects of laryngeal kinematics in non-advanced PD as well as considering volume and consistencies of trials. Replication of this study in healthy, older individuals is also needed to determine if kinematic changes seen in PWPD are due to disease process or aging.
Limitations of the study
Generalizations of the results from this pilot study should be guarded for a number of reasons. As an initial pilot study, the sample size for this particular project was small. Therefore, translation related to non-significant findings such as the water screening should be interpreted with caution. This small sample only included PWPD at non-advanced stages of the disease (H & Y I–III) which will limit the generalization of the current results to the larger population of PWPD. However, data obtained from this study can be used for future a priori power analyses to determine appropriate sample sizes for subsequent investigations.
This study only targeted two kinematic measures of interest (LVrt and LVCd). Future studies in this sample should investigate other kinematic measures to determine spatial and temporal factors which might also be contributing to decreased airway safety. Although normal values related to LVrt and LVCd are available, there were no healthy control participants for comparison of timing measures or PAS scores to examine changes in swallow safety.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
ACKNOWLEDGMENTS
We would like to acknowledge Diagnostex, LLC for their assistance in scheduling and conducting the videofluoroscopic studies used in this project.
REFERENCES
[1] | Attrill S , White S , Murray J , Hammond S , Doeltgen S ((2018) ) Impact of oropharyngeal dysphagia on healthcare cost and length of stay in hospital: A systematic review. BMC Health Serv Res 18: , 594. |
[2] | Lim S , Kim J , Hong B , Sul B ((2018) ) The findings of dysphagia in patients with Parkinson’s disease, using videofluoroscopic study. Parkinsonism Relat Disord 46: , 8–12. |
[3] | Brodsky MB , Suiter DM , González-Fernández M , Michtalik HJ , Frymark TB , Venediktov R , Schooling T ((2016) ) Screening accuracy for aspiration using bedside water swallow tests: a systematic review and meta-analysis. Chest 150: , 148–163. |
[4] | Argolo N , Sampaio M , Pinho P , Melo A , Nobrega AC ((2015) ) Videofluoroscopic predictors of penetration/aspiration in Parkinson’s disease patients. Dysphagia 30: , 751–758. |
[5] | Schiffer BL , Kendall K ((2018) ) Changes in timing of swallow events in Parkinson’s disease. Ann Otol Rhinol Laryngol 128: , 22–27. |
[6] | Berardelli A ((2001) ) Pathophysiology of bradykinesia in Parkinsons disease. Brain 124: , 2131–2146. |
[7] | Ellerston JK , Heller AC , Houtz DR , Kendall KA ((2016) ) Quantitative measures of swallowing deficits in patients with Parkinson s disease. Ann Otol Rhinol Laryngol 125: , 385–392. |
[8] | Tjaden K ((2008) ) Speech and swallowing in Parkinson’s disease. Top Geriatr Rehabil 24: , 115–126. |
[9] | Pflug C , Bihler M , Emich K , Niessen A , Nienstedt JC , Flügel T , Koseki JC , Plaetke R , Hidding U , Gerloff C , Buhmann C ((2018) ) Critical dysphagia is common in Parkinson disease and occurs even in non-advanced: a prospective cohort study. Dysphagia 33: , 41–50. |
[10] | Suttrup I , Warnecke T ((2016) ) Dysphagia in Parkinson’s disease. Dysphagia 31: , 24–32. |
[11] | Kwon M , Lee JH ((2019) ) Oro-pharyngeal dysphagia in Parkinson’s disease and related movement disorders. J Mov Disord 12: , 152–160. |
[12] | Curtis JA , Molfenter S , Troche MS ((2020) ) Predictors of residue and airway invasion in Parkinson’s disease. Dysphagia 35: , 220–230. |
[13] | Ertekin C , Tarlaci S , Aydogdu I , Kiylioglu N , Yuceyar N , Turman AB , Secil Y , Esmeli F ((2002) ) Electrophysiological evaluation of pharyngeal phase of swallowing in patients with Parkinson’s disease. Mov Disord 17: , 942–949. |
[14] | Michou E , Baijens L , Rofes L , Cartgena PS , Clave P ((2013) ) Oropharyngeal swallowing disorders in Parkinson’s disease: revisited. Int J Speech Lang Pathol Audiol 1: , 76–88. |
[15] | Kalf JG , de Swart BJM , Ensink RJH , Bloem BR ((2008) ) Dysphagia in Parkinson’s disease. B-Ent 4: (Suppl. 10), 57–59. |
[16] | Manor Y , Giladi N , Cohen A , Fliss DM , Cohen JT ((2007) ) Validation of a swallowing disturbance questionnaire for detecting dysphagia in patients with Parkinson’s disease. Mov Disord 22: , 1917–1921. |
[17] | Goetz CG , Poewe W , Rascol O , Sampaio C , Stebbins GT , Counsell C , Giladi N , Holloway RG , Moore CG , Wenning GK , Yahr MD , Seidl L ((2004) ) Movement Disorder Society Task Force on Rating Scales for Parkinson’s Disease. Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord 19: , 1020–1028. |
[18] | Miller N , Allcock L , Hildreth AJ , Jones D , Noble E , Burn DJ ((2008) ) Swallowing problems in Parkinson disease: frequency and clinical correlates. J Neurol Neurosurg Psychiatry 80: , 1047–1049. |
[19] | Pflug C , Niessen A , Buhmann C , Bihler M ((2019) ) Swallowing speed is no adequate predictor of aspiration in Parkinsons disease. Neurogastroenterol Motil 31: , e13713. |
[20] | Sulena Gupta D , Sharma AK , Singh B ((2017) ) Clinical profile of dysphagia in patients with Parkinson’s disease, progressive supranuclear palsy and multiple system atrophy. J Assoc Physicians India 65: , 32–37. |
[21] | Wang CM , Shieh WY , Weng YH , Hsu YH , Wu YR ((2017) ) Non-invasive assessment determine the swallowing and respiration dysfunction in early Parkinson’s disease. Parkinsonism Relat Disord 42: , 22–27. |
[22] | Mulheren RW , Azola A , González-Fernández M ((2019) ) Do ratings of swallowing function differ by videofluoroscopic rate? An exploratory analysis in patients after acute stroke. Arch Arch Phys Med Rehabil 100: , 1085–1090. |
[23] | Vose A , Humbert I ((2019) ) “Hidden in plain sight”: A descriptive review of laryngeal vestibule closure. Dysphagia 34: , 281–289. |
[24] | Rosenbek JC , Robbins JA , Roecker EB , Coyle JL , Wood JL ((1996) ) A penetration-aspiration scale. Dysphagia 11: , 93–98. |
[25] | Baijens LW , Speyer R , Passos VL , Pilz W , Roodenburg N , Clave P ((2011) ) Swallowing in Parkinson patients versus healthy controls: reliability of measurements in videofluoroscopy. Gastroenterol Res Pract 2011: , 1–9. |
[26] | Steele CM , Grace-Martin K ((2017) ) Reflections on clinical and statistical use of the penetration-aspiration scale. Dysphagia 32: , 601–616. |
[27] | Walker RW , Dunn JR , Gray WK ((2011) ) Self-reported dysphagia and its correlates within a prevalent population of people with Parkinson’s disease. Dysphagia 26: , 92–96. |
[28] | Kalf JG , de Swart BJ , Bloem BR , Munneke M ((2012) ) Prevalence of oropharyngeal dysphagia in Parkinson’s disease: a meta-analysis. Parkinsonism Relat Disord 18: , 311–315. |
[29] | Nienstedt JC , Bihler M , Niessen A , Plaetke R , Pötter-Nerger M , Gerloff C , Buhmann C , Pflug C ((2018) ) Predictive clinical factors for penetration and aspiration in Parkinson’s disease. Neurogastroenterol Motil 31: , e13524. |
[30] | Goetz CG , Tilley BC , Shaftman SR , Stebbins GT , Fahn S , Martinez-Martin P , Poewe W , Sampaio C , Stern M , Dodel R , Dubois B , Holloway R , Jankovic J , Kulisevsky J , Lang A , Lees A , Leurgans S , LeWitt PA , Nyenhuis D , Olanow CW , Rascol O , Schrag A , Teresi JA , van Hilten JJ , Lapelle N ((2008) ) Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov Disord 23: , 2129–2170. |
[31] | Chaudhuri KR , Martinez-Martin P , Schapira AH , Stocchi F , Sethi K , Odin P , Brown RG , Koller W , Barone P , MacPhee G , Kelly L , Rabey M , MacMahon D , Thomas S , Ondo W , Rye D , Forbes A , Tluk S , Dhawan V , Bowron A , Williams AJ , Olanow CW ((2006) ) International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: The NMSQuest study. Mov Disord 21: , 916–923. |
[32] | Mamolar Andrés S , Santamarina Rabanal ML , Granda Membiela CM , Fernández Gutiérrez MJ , Sirgo Rodríguez P , Álvarez Marcos C ((2017) ) Swallowing disorders in Parkinson’s disease. Trastornos de la deglución en la enfermedad de Parkinson. Acta Otorrinolaringol Esp 68: , 15–22. |
[33] | Suiter DM , Leder SB ((2007) ) Clinical utility of the 3-ounce Water Swallow Test. Dysphagia 23: , 244–250. |
[34] | Branco LL , Trentin S , Schwanke CH , Gomes I , Loureiro F ((2019) ) The Swallowing Clinical Assessment Score in Parkinson’s Disease (SCAS-PD) is a valid and low-cost tool for evaluation of dysphagia: a gold-standard comparison study. J Aging Res 2019: , 7984635. |
[35] | Warner HL , Suiter DM , Nystrom KV , Poskus K , Leder SB ((2014) ) Comparing accuracy of the Yale swallow protocol when administered by registered nurses and speech-language pathologists. J Clin Nurs 23: , 1908–1915. |
[36] | Humbert IA , Sunday KL , Karagiorgos E , Vose AK , Gould F , Greene L , Azola A , Tolar A , Rivet A ((2018) ) Swallowing kinematic differences across frozen, mixed, and ultrathin liquid boluses in healthy adults: age, sex, and normal variability. J Speech Lang Hear Res 61: , 1544–1559. |
[37] | Gaeckle M , Domahs F , Kartmann A , Tomandl B , Frank U ((2019) ) Predictors of penetration-aspiration in Parkinson’s disease patients with dysphagia: a retrospective analysis. Ann Otol Rhinol Laryngol 128: , 728–735. |


