
Sensorimotor Impairment in Aging and Neurocognitive Disorders: Beat Synchronization and Adaptation to Tempo Changes
Abstract
Background:
Understanding the nature and extent of sensorimotor decline in aging individuals and those with neurocognitive disorders (NCD), such as Alzheimer’s disease, is essential for designing effective music-based interventions. Our understanding of rhythmic functions remains incomplete, particularly in how aging and NCD affect sensorimotor synchronization and adaptation to tempo changes.
Objective:
This study aimed to investigate how aging and NCD severity impact tapping to metronomes and music, with and without tempo changes.
Methods:
Patients from a memory clinic participated in a tapping task, synchronizing with metronomic and musical sequences, some of which contained sudden tempo changes. After exclusions, 51 patients were included in the final analysis.
Results:
Participants’ Mini-Mental State Examination scores were associated with tapping consistency. Additionally, age negatively influenced consistency when synchronizing with a musical beat, whereas consistency remained stable across age when tapping with a metronome.
Conclusions:
The results indicate that the initial decline of attention and working memory with age may impact perception and synchronization to a musical beat, whereas progressive NCD-related cognitive decline results in more widespread sensorimotor decline, affecting tapping irrespective of audio type. These findings underline the importance of customizing rhythm-based interventions to the needs of older adults and individuals with NCD, taking into consideration their cognitive as well as their rhythmic aptitudes.
INTRODUCTION
Neurocognitive disorders and music-based interventions
Neurocognitive disorders (NCD) are acquired disorders marked by a progressive decline in cognitive functioning, particularly with regards to memory, but also including domains like attention, language, learning, and social cognition, challenging the patients’ capacity to live autonomously [1]. Before the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), major NCD was referred to as dementia, but we will use the term NCD in this article. Different forms exist, such as Alzheimer’s disease (AD), vascular NCD, NCD with Lewy bodies, and others. In the same vein, minor NCD is a DSM-5 diagnosis corresponding to a milder or prodromal form of the disease, which generally does not impede autonomy, and which was referred to as mild cognitive impairment before. In the absence of a cure for NCD, there is promise in improving the quality of life of those affected by enhancing various aspects of their well-being through non-pharmacological interventions. Among these interventions, music-based approaches have shown considerable potential in this regard. It has been suggested [2–4] that they may be particularly effective if they stimulate rhythmic movement. This may be related to temporal expectations elicited by a musical beat, which may stimulate the reward network and induce pleasure [5]. Besides directly eliciting reward and pleasure, stimulating rhythmic abilities may have positive effects on the way people with NCD interact with and adapt to their environment. Improving temporal prediction abilities might help people synchronize and interact with others [6], improve communication, and reduce isolation.
Sensorimotor synchronization
Sensorimotor synchronization (SMS) is defined as the temporal coordination of rhythmic movement with an external rhythm [7]. In a typical SMS paradigm, individuals coordinate their movements with an auditory sequence, typically involving a simple metronome or music. Synchronization performance is typically assessed in terms of consistency and asynchrony. Consistency refers to the degree of variability in the time differences between taps and beats, whereas asynchrony refers to whether participants tapped before (negative asynchrony) or after (positive asynchrony) the pacing event [8]. Paced tapping to a metronome and paced tapping to music, while ostensibly the same task, may in fact engage different mechanisms. In a metronomic sequence, the beat is indicated as simple regular tones, whereas in music, the beat is embedded within a complex auditory pattern. In this context, it is useful to think of beat perception as being comprised of two subprocesses; beat induction (beat finding), where an underlying beat is inferred even when auditory events are unequally spaced [9, 10]; and beat maintenance (beat continuation), which is a more automatic and mechanical process that implies continual, sustained measurement of predictable intervals and is less dependent on attention [10, 11]. Likely, both processes are employed simultaneously, the relative dependence of each depending on the saliency of the beat. Tapping to a metronome, then, might employ primarily beat maintenance processes, whereas tapping to music may be more dependent on beat induction. As a result, tapping to music is often associated with higher difficulty, expressed in lower tapping consistency [12–14], but not all studies have confirmed this [8, 15]. Indeed, the difficulty of performing synchronous movement to music presumably depends primarily on the clarity of its beat. In terms of asynchrony, people tend to tap ahead of the beat (referred to as mean negative asynchrony) when synchronizing with a metronome but not with music [8, 12–14, 16]. The mechanisms underlying this phenomenon are still not fully understood.
A key process in SMS is error correction. While error correction is an ever-present mechanism without which one would gradually become out of sync [17], it can directly be tested by introducing tempo changes. Adapting to tempo changes requires attention, awareness and some memory for at least the preceding events [18], and is likely related to cognitive flexibility, the ability to shift between mental sets and strategies [19].
How do age and neurocognitive disorders impact sensorimotor synchronization?
The ability to perceive a beat and synchronize to it emerges early in life, remains relatively stable in adulthood [20, 21], and may be preserved in old age, at least when synchronizing with an evenly spaced beat at a comfortable tempo [22–25]. Yet, certain studies have indicated a decline of sensorimotor abilities associated with age, which seems to appear above the age of 75 [20, 21, 26] (however, see [27] for a study demonstrating a reduction in tapping performance even in relatively young older adults). Nonetheless, there remains a lack of research studying SMS in the latest decades of life. Importantly, another study [28] did not find age-related differences in simple SMS, but older participants’ performance was diminished when participants had to simultaneously perform a cognitively challenging task while tapping to a metronome. This suggests that older people may employ more attention and working memory resources when tapping at a comfortable tempo.
The aforementioned studies examined the effect of age on SMS using metronomes. To our knowledge, the influence of old age on SMS with music has not yet been tested. However, considering the typical decline in attentional capacities associated with aging [29, 30], it is reasonable to speculate that beat induction may be more vulnerable to age-related decline than beat maintenance, which would result in age-related declines in SMS performance particularly with music.
Several studies have indicated that SMS abilities tend to be relatively preserved in individuals with NCD when instructed to tap along with a metronome set to a comfortable tempo [31]. However, differences were observed when participants had to continue tapping after an external sequence had ended [22, 32] or when the target rate deviated substantially from their comfortable tempo [22, 33, 34], manipulations likely to engage working memory and attention. However, a recent study by Hobeika et al. [35] revealed a decline in performance among individuals with major NCD in tapping even at a comfortable rate with a metronome and with music, and a positive relationship between consistency during metronome tapping and participants’ score on the Mini-Mental State Examination (MMSE), a brief screening tool for assessing NCD [36]. These different results may be explained by the severity of NCD in Hobeika et al.’s study (their NCD group had a mean MMSE of 15.5, which was lower than in the other studies). However, definite conclusions cannot be drawn from Hobeika et al.’s study because they pooled together participants who were tested under different conditions, which emphasizes the need for the current study, investigating the impact of NCD severity under homogeneous testing conditions.
As previously mentioned, synchronization with music requires extracting a beat from a complex and abstract auditory signal, with musical events occurring on nested timescales, requiring efficient allocation of attention over time for successful beat extraction [37]. It may be that in healthy aging people, or mild forms of NCD, tapping with a metronome may be a largely automatic process, and only when tapping with music, or in cognitively challenging paradigms are attention and working memory processes recruited, leading to a decline in performance. However, for people at more severe stages of NCD, attention and working memory are needed even to synchronize at a comfortable pace with a metronome. Indeed, some research has demonstrated increased use of non-motor regions during simple motor tasks in NCD, at least in AD [38, 39], indicating that with increasing severity of the disease, individuals employ other domain-general brain networks during SMS, reflecting a shift to more effortful and less automatic processing of rhythm, and potentially lower performance due to increasing competition for limited cognitive resources. It is possible that individuals in moderate to severe stages of NCD may require more attention and working memory even for tapping with simple metronomic sequences, and may be more impaired in these cognitive abilities, resulting in a general sensorimotor impairment manifested by reduced consistency when tapping to any regular stimulus, be it a metronome or music.
Similar to synchronization-continuation tapping and tapping at tempi far from one’s comfortable rate, tapping with a sequence containing tempo changes may particularly involve attention and working memory [18]. A particular impairment in SMS with tempo changes has already been demonstrated in other clinical populations, namely, people with traumatic brain injury [40], autism spectrum disorder [41], basal ganglia pathology [42], and cerebellar lesions [43], and has been explained in terms of attention-dependent temporal processing. Since attention is greatly impaired in people with NCD [44], the ability of people with NCD to adapt their tempo when encountering tempo changes may be compromised, due to an imprecise representation of temporal structure and inefficient allocation of attention over time [42]. Finally, a decline in cognitive flexibility found in people with NCD [45, 46] may present another contributing factor to their potential disadvantage in adaptation to tempo changes. To our knowledge, there does not exist any research examining the effect of NCD on tempo adaptation in SMS. It is important to investigate this aspect, as adaptation to tempo changes can serve as a model for understanding how individuals interact with a dynamically changing environment in general.
The current study
The aim of the current study was to test the effects of age and NCD severity on SMS to metronomes and to music with and without tempo changes. In this context, we examined SMS skills, with particular emphasis on the impact of tempo changes by introducing sudden accelerations and decelerations every 15 s in half of the trials, and computing consistency and asynchrony. The difficulty in this task should come only from the changes in tempo, rather than presenting participants with inherently difficult tempi for synchronization. To achieve this, we selected base tempi that closely aligned with the typical spontaneous motor tempo reported in the literature for older adults [21, 25] and we confirmed this by assessing individuals’ spontaneous tempo. In traditional SMS paradigms, participants typically tap their finger or hand to an auditory regular beat. However, when applying such paradigms to individuals with NCD, particularly in advanced stages, special consideration is required to avoid stressful, unpleasant or artificial laboratory situations, as they might find it difficult to cope with such conditions, and they may experience difficulties in retaining and following instructions, especially in longer experiments. For these reasons, tasks with multimodal stimuli, creating a quasi-social situation, may be conducive [47, 48]. Additionally, people, including older adults with NCD, might actually perform better when synchronizing with a video than with another person [14, 49]. We recently developed and validated an experimental setup tailored to elderly individuals [14, 49, 50] and continue its use to present stimuli bimodally (audio plus video). Using this experimental design and assessing a group of older adults exhibiting a range of ages and varying levels of cognitive impairment created an optimal setting for examining the distinct impacts of both age and NCD on sensorimotor synchronization.
Firstly, we expect a global impairment in SMS with increasing NCD severity. Specifically, we expect that MMSE score will have a negative impact on tapping consistency. Second, we hypothesize that consistency will be lower in trials with a shifting tempo compared to those with a stable tempo. Third, we predict an interaction between the presence or absence of tempo changes and MMSE score, such that the reduction in consistency in the shifting condition will be more pronounced in individuals with a lower MMSE score, probably due to declines in attention, working memory, and cognitive flexibility. Fourth, consistent with previous research, we expect lower consistency when individuals synchronize their movements with music compared to a metronome [12–14]. Fifth, due to increased reliance on beat induction with music and decreased attentional capacities with aging, we expect consistency to decrease with age when individuals tap with music, but to a lesser extent (or not at all) with a metronome. Sixth, and finally, we hypothesize that asynchrony will be lower (more negative) in the metronome conditions compared to music [7, 8, 12–14, 51].
MATERIALS AND METHODS
Participants
A total of 61 patients were recruited at the geriatric day hospital Les Bateliers (Lille University Hospital, France), during a scheduled consultation related to memory problems or falls. Inclusion criteria included age between 60 and 99, right-handedness and native or near-native fluency in French. Patients were ineligible for participation if they had Parkinson’s disease, other motor disorders or paralysis, or uncorrected hearing or vision problems. Patients’ data were excluded from analysis if they did not finish the experiment. Most patients were diagnosed with major or minor NCD, whereas a minority of patients were attested subjective memory complaints without evidence of NCD. This diagnosis was made by a geriatrician and based on DSM-5 criteria [1]. However, in this study, we assessed cognitive impairment as a continuous variable using the MMSE. After ten exclusions (seven who withdrew from the study during the experiment, one due to technical problems, one who tapped in a seemingly random fashion in all trials as indicated by Rayleigh’s test [52], and one whose MMSE score of 14 was an outlier; 3 SDs below the mean), 51 patients were included in this study. The data were collected between November 2021 and July 2022. The study was approved by the local Ethics Committee (Comité de Protection des Personnes, Sud-Est VI, France; No. 2017-A03543-50) and by the Commission Nationale de l’Informatique et des Libertés, registered at clinicaltrials.gov (NCT04146688). All patients provided written informed consent for their participation in accordance with the Declaration of Helsinki.
Materials
Experimental apparatus
The experimental set-up included a chair with a tablet attached to the right armrest on which the patient tapped using a ball-like probe they held in their right hand [47, 48]. A life-sized screen (158×92 cm) and a pair of loudspeakers were placed in front of the patient at a distance of 230 cm. A video of a musician tapping to the simultaneously presented auditory sequence was projected onto the screen during the task in front of the patient. Each patient was tested individually and was separated from the experimenter by a curtain to avoid distraction. Stimuli were presented and responses collected using a program written in MAX/MSP (https://cycling74.com).
Stimuli
Stimuli were 75 s long and consisted of either a metronome or a musical sequence and a video recording of the musician tapping to the beat of the auditory sequence. Both types of audio were preceded by 4 beats to provide the tempo.
Metronome trials consisted of regular beats. For the music trials, a custom-made rendition of an excerpt of the French popular song “Non, je ne regrette rien” by Édith Piaf was used. This particular song was chosen because it was likely well-known to our age group and its original tempo is close to older adults’ spontaneous motor tempo [14, 25]. A MIDI version of the song (without lyrics), available in an online music repository (www.midis101.com) was selected and cropped to a length of 75 s. We opted for a MIDI version of the song in order to have completely isochronous timing and the possibility to manipulate its tempo.
The musical and metronomic sequences were manipulated to conform to one of four temporal patterns (Fig. 1): A stable IOI of 674 ms (A), a stable IOI of 741 ms (B), or a sequence in which the tempo shifted every 15 seconds between the two, starting either at 674 ms (C) or starting at 741 ms (D). Ableton Live was used to render the musical stimuli from the MIDI versions using their in-house instruments, to create the metronomic stimuli and to perform the tempo manipulations. The visual part of the audio-visual stimuli was created beforehand by filming the musician who sat in the position of the participants, listened to the musical stimuli and tapped along. An analysis of the musician’s tapping consistency and asynchrony during the recording of these videos indicated very good performance and minimal error (see Supplementary Table 1).
Fig. 1
Types of audio and temporal structures used in the experimental trials. Using two types of audio (music and metronome) and tempi corresponding to four temporal patterns (A, stable tempo of 674 ms; B, stable tempo of 741 ms; C, shifting tempo starting at 674 ms; D, shifting tempo starting at 741 ms) resulted in eight different experimental trials.
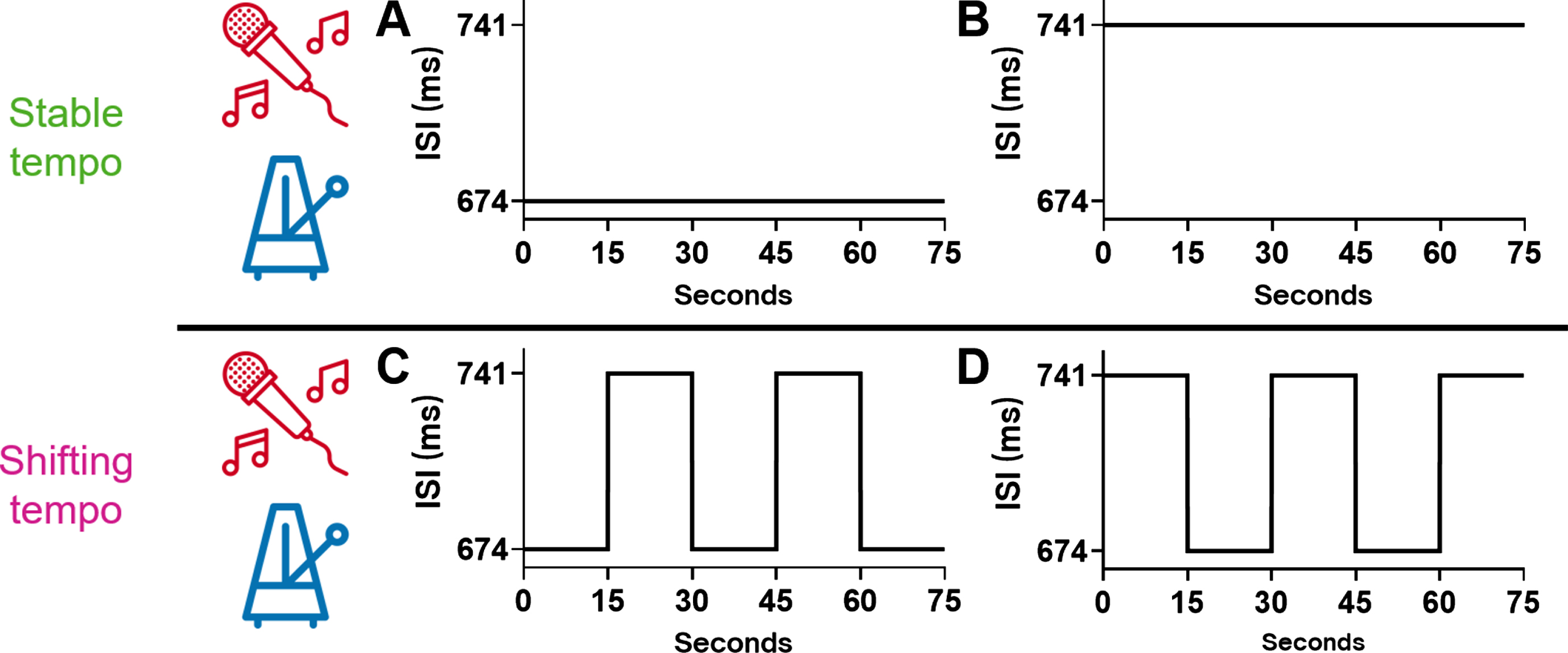
Table 1
Demographic and clinical information of patients
| N | Median [first quartile, third quartile] or frequencies (%) | Range | |
| Age | 51 | 82 [76, 86] | 61–92 |
| Gender (women) | 51 | 35 (69%) | |
| Years of education | 51 | 12 [7, 14] | 3–18 |
| Musical expertise (out of 28) | 51 | 3 [2, 4] | 0–12 |
| Diagnosis | 48 | ||
| Major NCD | 21 (44%) | ||
| Minor NCD | 24 (50%) | ||
| No NCD | 3 (6%) | ||
| MMSE (out of 30) | 51 | 25 [23, 28] | 19–30 |
| ADL (out of 6) | 50 | 5.5 [4.5, 6] | 2–6 |
| IADL (out of 4) | 50 | 2 [1, 3] | 0–4 |
| GDS (out of 15) | 50 | 5 [3, 8] | 1–12 |
| GAI (out of 5) | 50 | 2 [1, 4] | 0–5 |
NCD, neurocognitive disorder; MMSE, Mini-Mental State Examination; ADL, Activities of Daily Living; IADL, Instrumental Activities of Daily Living; GDS, Geriatric Depression Scale; GAI, Geriatric Anxiety Inventory.
Procedure
The experiment started by orally administering a musical expertise questionnaire, which inquired about participants’ musical training, listening habits, and engagement with music (only the total score is reported here). Then, short forms of the Geriatric Depression Scale [53] and the Geriatric Anxiety Inventory [54] were orally administered. Next, each patient performed a brief spontaneous motor task by tapping as regularly as possible for 31 taps (30 inter-tap intervals; ITIs), at their preferred, comfortable tempo.
Afterwards, each patient underwent the paced tapping task, in which they were exposed to audio-visual stimuli (described in the preceding section) and tapped along with every beat, just like they watched the musician do in the video. A practice trial was followed by eight experimental trials, counterbalanced across participants, in a randomized order. The participant was not informed that tempo changes might occur. The patient was given the possibility to take a break after half of the experimental trials.
Data analysis
Calculation of SMS variables
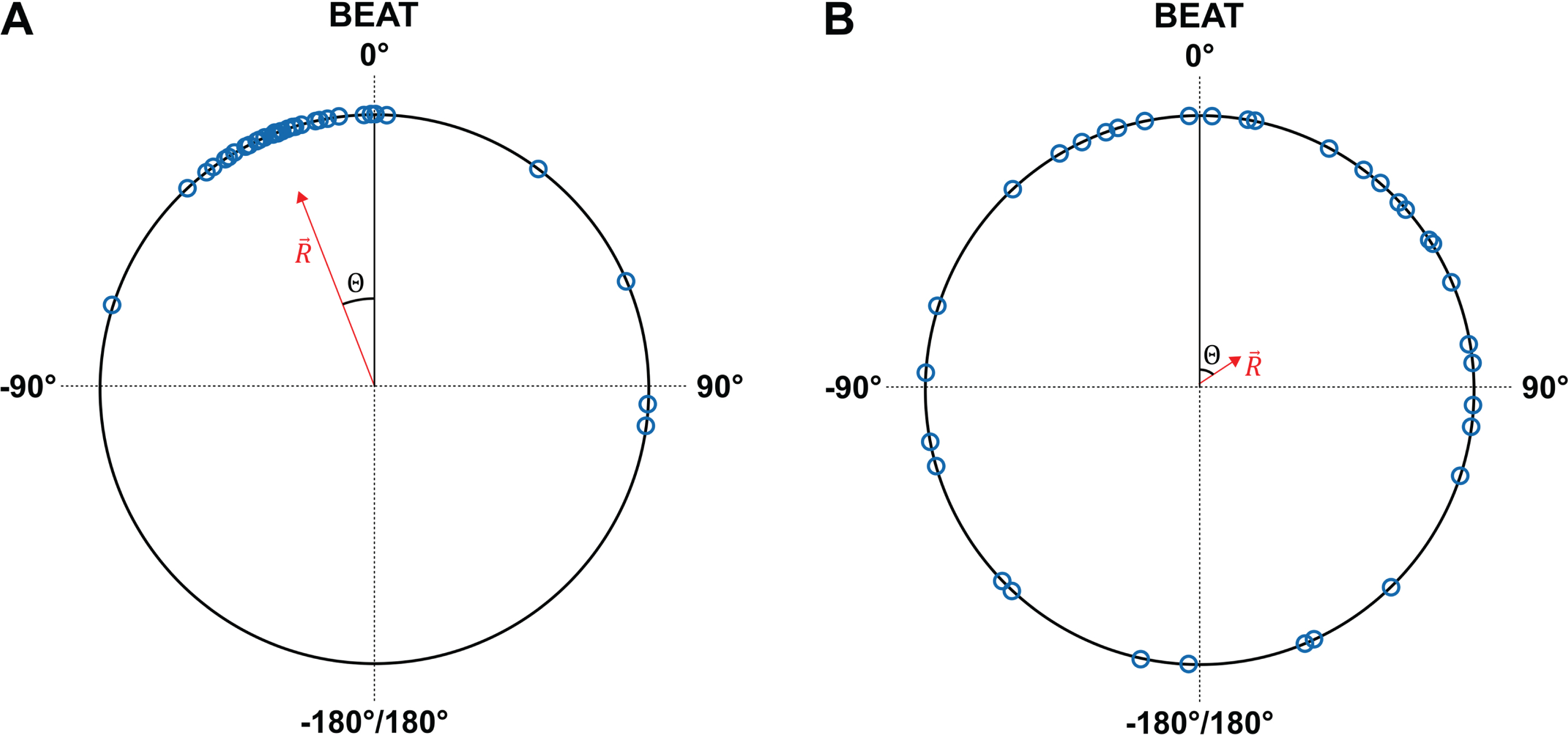
For the 30 intervals produced during the spontaneous motor task, we calculated mean ITI and CV (standard deviation divided by mean) of ITI. In the paced tapping task, as we mentioned above, the tempo either remained stable or shifted every 15 s. We therefore computed consistency and asynchrony per 15-s segment using circular statistics [55] with the CircStat toolbox [56] in MATLAB [57]. We opted for circular analysis of synchronization data as this allowed for a robust analysis even in the case of missing or superfluous taps, as asynchronies and their variability can be computed without necessarily attributing each response event to a particular beat [58]. In a given trial, ms in an inter-onset interval (IOI) are converted into degrees on a circular scale going from ?180° to +180°. The beat’s onset is at 0°, the time a participant would be expected to tap. An angle of 180° would indicate a participant tapping in antiphase. Vectors were averaged to obtain a mean resultant vector
Fig. 2
Two examples of circular synchronization analysis in a given trial. Each inter-onset interval is converted to degrees on a circular scale. The time at which each tap occurs, relative to the beat (= 0 degrees) is then represented by a specific angle on the circle (blue minicircles). The mean vector R summarizes the performance during a 15-second segment. The mean direction (Θ) represents asynchrony, whereas the length
Statistical analyses
All statistical analyses were performed in R 4.2.2 using RStudio [59, 60]. We analyzed SMS consistency and asynchrony by conducting mixed-effects models. In the analysis of consistency, fixed effects included the variables audio, tempo stability, age, MMSE, as well as the interactions between audio and age, audio and MMSE, tempo stability and age, and tempo stability and MMSE. The analysis of asynchrony only included audio as a variable of interest since the only hypothesis regarding asynchrony pertained to this variable. In both analyses, we controlled for the effects of gender, years of education, and musical expertise by entering them as additional fixed effects in the model. Finally, participant was entered as a random effect in both models. In the analysis with consistency as a dependent variable, a generalized linear mixed model with a beta distribution and a logit link was performed using the glmmTMB package [61] in R. For both analyses, we removed segments where asynchrony was lower than –135° or higher than 135°, indicating tapping in antiphase. In the analysis with asynchrony as a dependent variable, we first removed from the analysis segments with insufficient taps (i.e., where the percentage of taps relative to the number of beats was more than 2 standard deviations below the mean). Then, we transformed the variable asynchrony by taking the cubic root of its absolute value and multiplying it with its original sign. This was done to fulfil the assumption of normality of residuals, as asynchrony was right-skewed. Then, we performed a linear mixed-effects model analysis using the lme4 package [62]. Type II Wald chi-square tests were used to test the main effects and interactions. We present effect size by computing f2, which is considered an appropriate metric of effect size in mixed-effects regression models [63].
RESULTS
Participants
Demographic data, including age, gender, education and musical expertise, and clinical data, encompassing diagnosis, MMSE, Activities of Daily Living [64], Instrumental Activities of Daily Living [65], Geriatric Depression Scale, and Geriatric Anxiety Inventory, can be found in Table 1. Of the 21 participants diagnosed with major NCD, nine were diagnosed with AD, two with vascular NCD, 11 with NCD of mixed etiology, and one with NCD of an unknown origin. A distribution of MMSE scores is shown in Supplementary Figure 2. An analysis of variance revealed significant differences in MMSE between groups of people with different diagnoses, F(2, 1510) = 847.2, p < 0.001. Post hoc tests using Bonferroni correction confirmed that the group of people without NCD had the highest average MMSE (M = 29.00, SD = 0.82), followed by the group with minor NCD (M = 25.22, SD = 2.83), and finally, the group with major NCD had the lowest average MMSE (M = 24.51, SD = 3.42). These differences in MMSE scores were statistically significant across all groups (all ps < 0.001). Demographic and clinical data of the seven participants who withdrew from participation during the study can be found in Supplementary Table 2. The participants who did not finish the study were on average older (U = 66.0, p < 0.01, Mann-Whitney U test) and had a lower MMSE score (U = 265.5, p < 0.05, Mann-Whitney U test) than those who did, whereas the two groups did not differ in terms of gender, diagnosis, education, musical expertise, ADL, IADL, depression, or anxiety (all ps > 0.05). Moreover, all participants who finished the study prematurely were diagnosed with major NCD.
Tapping tasks
Participants’ mean spontaneous motor tempo was 715 ms (SD = 468 ms). This confirms that the tempo of the experimental stimuli (674 ms and 741 ms) was within a comfortable range.
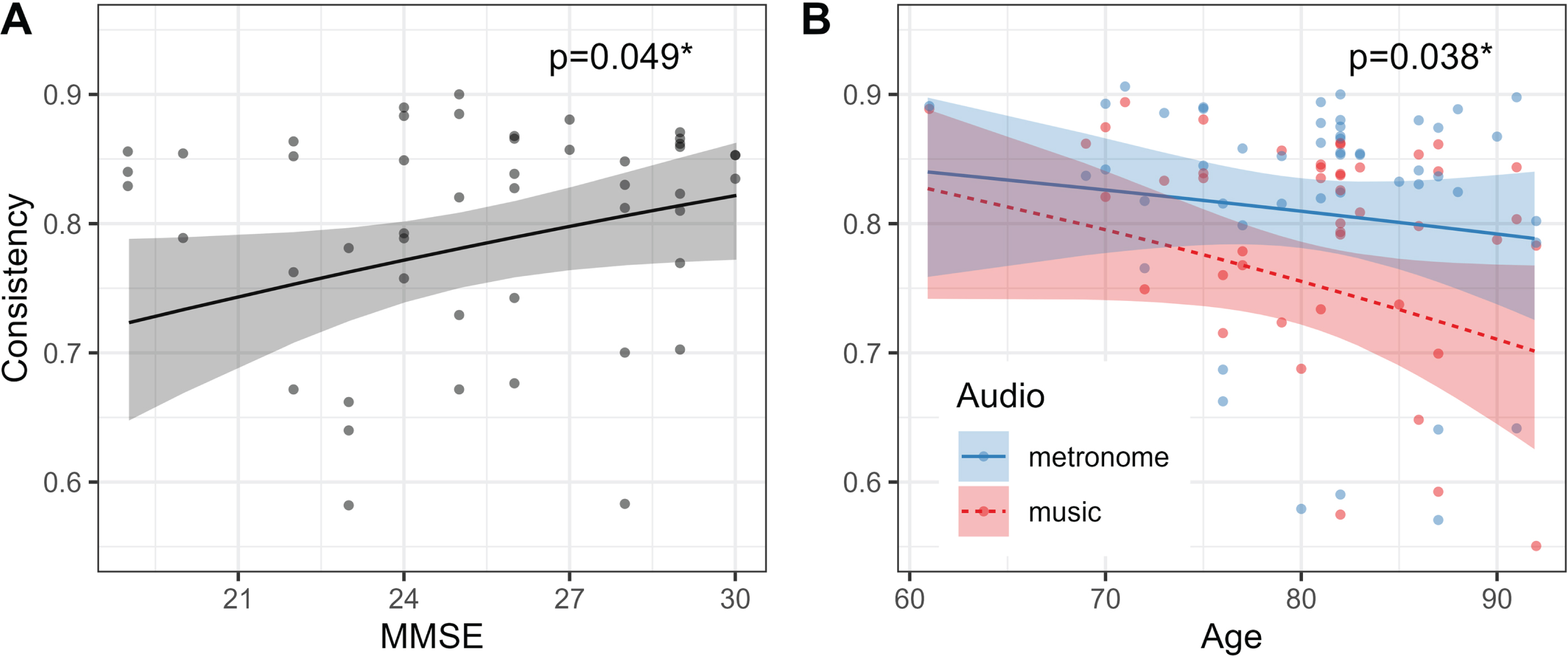
The results of the generalized linear mixed model with consistency as a dependent variable are presented in Supplementary Table 3. A main effect of MMSE (Wald χ2 = 3.86, p < 0.05, f2 = 0.03) suggests that more cognitively impaired people (i.e., with a lower MMSE score) tapped with a lower level of consistency (Fig. 3A). Unsurprisingly, a main effect of tempo stability (χ2 = 756.34, p < 0.001, f2 = 0.21) indicates that consistency was higher in trials with a stable tempo compared to those with a shifting tempo. In addition, there was a significant effect of Audio (χ2 = 76.44, p < 0.001, f2 = 0.04), with consistency being higher when participants synchronized with a metronome compared to music. Furthermore, there was a significant interaction of audio and age (Wald χ2 = 4.28, p < 0.05 f2 < 0.01; Fig. 3B). Consistency appeared to decrease with age, but only in the music conditions.
Fig. 3
Effects of MMSE, and of the interaction of audio and age on consistency. A) More cognitively impaired people (i.e., with a lower MMSE score) tapped with a lower level of consistency. B) Consistency decreased with age, but only in the music conditions. MMSE, Mini-Mental State Examination.
There was also a two-way interaction effect of tempo stability and age on consistency. However, the slopes of the two regression lines were not significantly different from zero (both ps > 0.05) and is unlikely to have practical significance. We therefore report this effect only in Supplementary Figure 3.
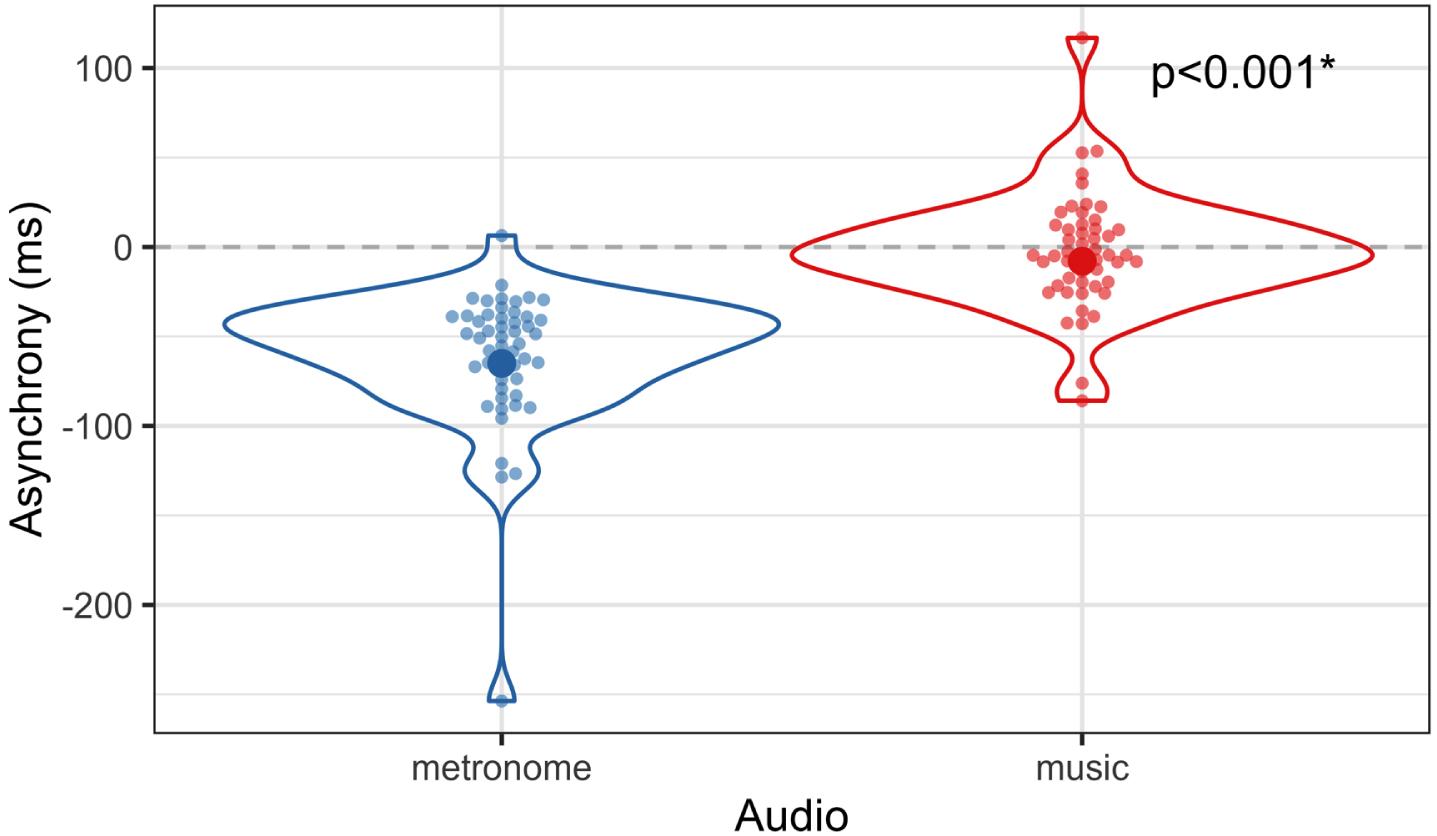
The results of the linear mixed model with asynchrony as a dependent variable are presented in Supplementary Table 4. As predicted, the main effect of audio was significant (Wald χ2 = 248.08, p < 0.001, f2 = 1.38), indicating that participants’ taps occurred close to the beat when tapping with music, whereas their taps tended to anticipate the beat when tapping with a metronome (Fig. 4).
Fig. 4
Effect of audio on asynchrony. In order to fulfil the assumption of multivariate normality, the dependent variable asynchrony was transformed by taking the cubic root of its absolute value and multiplying it with its original sign. However, this figure was created by taking estimated marginal means and standard deviations of a linear mixed model with non-transformed data.
Finally, we checked for the potential confounding effects (such as tempo and segment) in a supplementary analysis presented in Supplementary Tables 5 and 6. The results revealed that the effects of interest showed no difference with the simplified models presented above.
DISCUSSION
The purpose of this study was to investigate the influence of age and NCD severity on SMS performance, quantified as tapping consistency and asynchrony. We were particularly interested in whether different subprocesses of SMS, including beat induction, beat maintenance, and error correction, might be differentially impacted by age and NCD. This differential impact could manifest in age and NCD unequally influencing SMS performance when synchronizing with music versus metronomes, and with tempo-changing sequences compared to sequences with a stable tempo. We demonstrated that tapping consistency decreased with MMSE, providing evidence of the impact of neurocognitive disorders on sensorimotor abilities and thereby confirming our first hypothesis. Not surprisingly, our second hypothesis of a detrimental effect of tempo changes on tapping consistency was also confirmed. Contrary to our third hypothesis, however, the effect of MMSE did not depend on tempo stability. People in general tapped with a lower level of consistency to music than to a metronome, confirming our fourth hypothesis and the results of previous studies [12–14]. Additionally, and as predicted by our fifth hypothesis, we observed a decrease in consistency with age, but only when individuals tapped with musical sequences and not with a metronome. Supporting our sixth and final hypothesis, asynchrony was lower (more negative) in the metronome condition compared to the music condition. Before discussing these results in depth, it is worth noting that participants’ mean spontaneous motor tempo of 715 ms is close to what has previously been found in older adults [21, 25]. More importantly, it was squarely in between the two stimulus tempi in the paced tapping task (674 ms and 741 ms). It is therefore reasonable to assume that both tempi were in the range of comfortable rates for our participants.
Effect of NCD severity on consistency
The observed association between MMSE score and tapping consistency is in line with previous findings. A recent study by Hobeika et al [35] also found reduced consistency in people with major NCD compared to those with mild or no NCD, as well as a positive linear relationship between MMSE and consistency during an audio-visual tapping task. However, the latter result was limited to the metronome condition, whereas participants were not impaired with music. Interestingly, in our study, cognitive impairment had a global impact on consistency, affecting tapping with both metronome and music. Perhaps these differences stem from the fact that our study, which included trials with tempo changes, was more sensitive to uncovering NCD-related effects. On the other hand, the effect of NCD severity on tapping to music present here but absent in Hobeika et al.’s study might be attributed to music-induced reward. The motivating and rewarding qualities of music may boost synchronization, resulting in more consistent tapping [66]. Perhaps Hobeika et al.’s stimuli, with original music recordings and sung lyrics, were more rewarding than our MIDI-based stimuli which did not contain lyrics and which were also repeated more often within the same experiment. Perhaps a difficulty in synchronizing to music was offset by enhanced synchronicity related to reward in Hobeika et al.’s study, underscoring the relevance of selecting music for its motivating and rewarding qualities.
The finding of an NCD-related deficit in SMS at a comfortable rate is novel: Some studies have previously shown lower tapping consistency in people with NCD, but only when they had to continue tapping after an external sequence had ended [22, 32] and/or when the tempo they synchronized with was far from their comfortable tempo (i.e., slower [22, 34] or faster [33]). We hypothesized that the tempo-changing manipulation would be particularly difficult for more cognitively impaired people and that MMSE and tempo stability would therefore interact, but this effect was not observed in this study. It may be that the current task and its analysis pipeline, examining consistency by 15-s segments, and comparing these segments across conditions, may have been too crude, given that people only take a few taps to adapt to a new tempo [18, 67, 68], at least healthy participants. Additionally, it is possible that the bimodal nature of the task (audio and video) made the task easier, offsetting the difficulty introduced by the tempo changes. Finally, while MMSE was chosen as a predictor variable to capture the full spectrum of cognitive impairment, this may have resulted in reduced statistical power to detect effects, especially interaction effects, than sampling two extreme groups [69]. Additional research on rhythmic synchronization with tempo changes is warranted, as it may provide insights into how individuals generally entrain to regularities and adapt to changes in their sensory environment.
This study, along with another recent study [35], highlights a global deficit in SMS abilities among individuals with NCD. Given the established connection between rhythmic and cognitive abilities, it can be speculated that rhythmic training may confer cognitive benefits. However, the direct transfer of benefits from musical to non-musical domains requires further investigation. There exist other neurological conditions like Parkinson’s disease, Huntington’s disease, autism spectrum disorder, attention deficit hyperactivity disorder, and dyslexia, where rhythmic deficits are prominent and rhythm-based training may offer advantages beyond the motor realm, such as on communication and executive functions [70–76]. By continuing to study SMS and its links with cognitive abilities, we may get a clearer picture of what processes may inadvertently be stimulated through rhythm-based interventions, to slow down symptoms in NCD, but also as a preventive strategy in healthy older adults [77–80]. Finally, the current results also suggest that sensorimotor problems could serve as a potential diagnostic marker of NCD, warranting inclusion in the neuropsychological evaluation process, but only as complementary tests among measures of working memory and attention, for which the link with NCD is more established.
Interaction between audio and age on consistency
Another noteworthy result was an interaction effect of audio and age on consistency. Age negatively affected tapping consistency when people synchronized their taps with music, but not with a metronome. This observation offers a more nuanced perspective on past research that found higher consistency when tapping with metronomes compared to music [12–14] and research on the effect of age on SMS which often found null results at least with a comfortable tempo, but which rarely used music material as a stimulus, but rather metronomes [20–22, 24–26, 33, 81] (but see [27, 82]). The current findings, revealing distinct effects of age on tapping to metronomes versus tapping to music, suggest that beat maintenance and beat induction may be affected differently. Perhaps older adults experience greater impairment in beat induction processes, which are crucial for tapping with music, whereas they retain their ability in the automatic and mechanical aspects of beat maintenance, resulting in comparable performance to younger individuals when tapping with a metronome.
Previous research indicates that during movement performance in older adults, additional brain regions, specifically prefrontal areas, become active [83–85], even in situations where there are no age-related differences in performance outcomes. This suggests increased cognitive control in executing movements in older individuals. Thus, there might be a beginning decline in motor control associated with aging, which people compensate for by employing extra neural and cognitive resources, leading them to achieve performance levels comparable to those of younger individuals when the task is simple, such as metronome tapping in this study. However, in tasks that demand higher-level representations and/or executive control such as bimanual [86–89] and sequential [90] tapping, or having to rapidly extract the beat from a musical sequence such as in this study, these compensatory mechanisms might not be sufficient, leading to age-related differences in performance in these more complex tasks. The global effect of MMSE on consistency discussed in the previous section may also imply that people with NCD do not engage in compensatory mechanisms as efficiently as healthy older adults, or that this compensation is not sufficient to mask differences in performance even on simpler tasks like tapping with a metronome. For future research, it is crucial to use stimuli with varying levels of complexity, as in this study, to discern the factors that yield observable performance differences.
Implications for music-based interventions
The results highlight that motor and cognitive skills may be tightly linked, indicating the potential of rhythm-based interventions to stimulate non-motor domains, such as working memory, executive functions, language, and socio-emotional functioning, presenting a promising avenue for improving the quality of life in individuals with NCDs. The current findings are relevant to how interventions may be tailored to a person’s cognitive status. Considering that individuals with lower cognitive functioning may have difficulties in synchronizing movements to auditory stimuli, particularly those that are not intrinsically motivating or rewarding, it is essential to adapt music-based interventions based on cognitive ability and carefully select appropriate stimuli. One may consider using stable and predictable beats, potentially including metronomes or music with high beat clarity when working with older adults, given the age-related decline in beat induction demonstrated here. Indeed, previous studies have used music with beats sonically enhanced or reinforced by a superimposed metronome to facilitate synchronization in a rehabilitative setting [72, 91, 92] The observed reduction in consistency when introducing tempo changes could serve as an argument for adaptive programs, starting with simpler, stable tempi and gradually introducing more complex rhythms to ensure task engagement and build rhythmic skills progressively. While our research and its implications for rhythm-based interventions are focused on simple, unimanual tapping, it is essential to note that music-based interventions requiring finer motor control may specifically engender cognitive benefits [93]. While this study did not compare audio-visual stimuli with purely auditory stimuli, the high levels of performance observed here suggest that visual cues of any kind may enhance synchronization. Finally, non-musical cognitive training could be intertwined with musical exercises, mutually enhancing each other’s effectiveness.
Limitations
Our sample included individuals with NCD of diverse origins, predominantly AD, vascular NCD, and NCD of mixed etiology. While this sample is likely representative of the general population of individuals with NCD, the limited numbers within each subgroup did not allow us to explore differences between various etiologies, which presents an interesting avenue for future research. In fact, we are aware of only one study [34] that compared sensorimotor synchronization abilities across different NCD groups and identified differences between AD and frontotemporal NCD.
We recognized the importance of good hearing and vision for our experiment, screening out potential participants with impairments or those who did not have the necessary aids with them. However, we did not conduct formal audiometry or visual acuity tests, leaving the possibility that performance variations could be attributed in part to differences in hearing and visual abilities, considering the common prevalence of hearing loss [94] and visual impairment [95, 96] in older adults.
It is worth repeating that we deliberately chose to use audio-visual stimuli to synchronize to, a manipulation deemed necessary to maintain participants’ engagement and motivation throughout the task. Nevertheless, this prevented us from assessing the degree to which participants relied on auditory versus visual information. Especially in terms of beat induction and beat maintenance, it is conceivable that the presentation of sensory information through different modalities could impact them in different ways. An interesting path for future investigation is to compare how these processes are influenced when information is presented solely through auditory, solely through visual, or through both modalities.
Concluding remarks
This study highlights two primary findings. The first is an influence of MMSE score on tapping consistency, irrespective of audio stimulus type and of the presence or absence of tempo changes, suggesting an effect of NCD severity on the ability to maintain a steady rhythm. Two possible mechanisms could explain this, which are not mutually exclusive. Firstly, neural reorganizing over the course of the disorder may increasingly engage non-motor areas to sustain performance during a simple motor task, indicating a shift towards more cognitive and effortful processing of rhythm. Secondly, even simple metronome tapping may require some degree of attention and working memory, albeit less than tapping with music. Healthy aging individuals may therefore maintain a consistent level of performance when tapping with a metronome, whereas in more cognitively impaired individuals with a lower MMSE, the impairment of attention and working memory is severe enough to significantly hinder performance, even in tapping with a simple metronome, arguably the simplest form of SMS. However, it is important to acknowledge the importance of tempo changes in half of the trials. While the statistical analysis indicates that the impact of cognitive impairment held for both conditions (with and without tempo changes), it may still be that the primary difficulty in this study might have arisen from the presence of tempo changes in half of the trials, even though the difference in decline of consistency as a function of MMSE across the two levels of tempo stability was not large enough to yield statistical significance. Although we did not observe an interaction between tempo stability and MMSE in this study, the current results do not eliminate the possibility that individuals with NCD might experience specific difficulties in adapting to tempo changes. The involvement of working memory, attention, and cognitive flexibility in error correction could still play a role, warranting further investigation. The second result shows an age-related decline in consistency during SMS but only when tapping with music, whereas consistency remains stable when tapping with a metronome. This observation implies that beat induction, a process especially relevant for perceiving the underlying beat in musical sequences, is affected in healthy aging, potentially indicating a beginning decline of attention and working memory. Beat maintenance, on the other hand, may be relatively spared.
In conclusion, this research emphasizes the importance of sensorimotor impairment as a symptom in NCD. The findings suggest that motor and cognitive skills may be tightly linked, implying that deficits in one domain may potentially impact the other. This interplay underlines the potential for rhythm-based training to inadvertently stimulate non-motor domains, such as working memory, executive functions, language, and socio-emotional functioning, presenting a promising avenue for enhancing the quality of life in individuals living with NCDs. These insights provide a foundation for continued research and therapeutic interventions aimed at enhancing well-being in healthy and pathological aging by targeting the sensorimotor domain. The possibility for therapeutic approaches are vast, ranging from group drumming [97] to remote interventions using mobile devices [98].
AUTHOR CONTRIBUTIONS
Andres von Schnehen (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Software; Visualization; Writing – original draft); Lise Hobeika (Conceptualization; Formal analysis; Methodology; Software; Supervision; Writing – review & editing); Marion Houot (Formal analysis; Software; Writing – review & editing); Arnaud Recher (Resources; Software); François Puisieux (Resources; Supervision); Dominique Huvent-Grelle (Resources; Writing – review & editing); Séverine Samson (Conceptualization; Funding acquisition; Supervision; Validation; Writing – review & editing).
ACKNOWLEDGMENTS
The authors thank Ivan Schepers of Ghent University for help in the material’s development, and the musician Sotirios Sideris with whom the stimuli were developed. The authors are grateful to Nicholas Foster for invaluable advice regarding data analysis and visualization. We furthermore thank the geriatrician Jean Roche, the neuropsychologists Anita Clercx, Sylvie Schoenenburg, and Laurence Grymonprez, and the entire dedicated staff at the day hospital Les Bateliers in Lille. Finally, we thank all participants involved in this study.
During the preparation of this work the authors used the large language model ChatGPT [99] in order to improve the flow and readability of the writing. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
FUNDING
This project has received funding from the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement No 847568. Moreover, this study was supported by the French government through the Programme Investissement d’Avenir (I-SITE ULNE/ANR-16-IDEX-0004 ULNE) managed by the Agence Nationale de la Recherche.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings and a script to analyze them are openly available at https://osf.io/78k46/?view_only=9e15fa4ac33d49e1aff47bd609c305ab.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-231433.
REFERENCES
[1] | American Psychiatric Association ((2013) ) Diagnostic and statistical manual of mental disorders (5th ed.), American Psychiatric Association, Arlington, VA. |
[2] | Cason N , Schiaratura L , Samson S ((2017) ) Synchronization to music as a tool for enhancing non-verbal communication in people with neurological diseases. Routledge Companion Embodied Music Interact, pp. 304–312. |
[3] | Hobeika L , Samson S ((2020) ) Why do music-based interventions benefit persons with neurodegenerative disease? In Music and the Aging Brain, Cuddy LL, Belleville S, Moussard A, eds. Academic Press, pp. 333–349. |
[4] | Ghilain M , Schiaratura L , Singh A , Lesaffre M , Samson S ((2019) ) Is music special for people with dementia? In Music and dementia: From cognition to therapy, Baird A, Garrido S, Tamplin J, eds. Oxford University Press, pp. 24–40. |
[5] | Salimpoor VN , Benovoy M , Larcher K , Dagher A , Zatorre RJ ((2011) ) Anatomically distinct dopamine release during anticipation and experience of peak emotion to music. Nat Neurosci 14: , 257–264. |
[6] | Pecenka N , Keller PE ((2011) ) The role of temporal prediction abilities in interpersonal sensorimotor synchronization. Exp Brain Res 211: , 505–515. |
[7] | Repp BH ((2005) ) Sensorimotor synchronization: A review of the tapping literature. Psychon Bull Rev 12: , 969–992. |
[8] | Sowiński J , Dalla Bella S ((2013) ) Poor synchronization to the beat may result from deficient auditory-motor mapping. Neuropsychologia 51: , 1952–1963. |
[9] | Honing H ((2012) ) Without it no music: beat induction as a fundamental musical trait. Ann N Y Acad Sci 1252: , 85–91. |
[10] | Toiviainen P , Burunat I , Brattico E , Vuust P , Alluri V ((2020) ) The chronnectome of musical beat. Neuroimage 216: , 116191. |
[11] | Cannon JJ , Patel AD ((2021) ) How beat perception co-opts motor neurophysiology. Trends Cogn Sci 25: , 137–150. |
[12] | Aschersleben G ((2002) ) Temporal control of movements in sensorimotor synchronization. Brain Cogn 48: , 66–79. |
[13] | Dalla Bella S , Farrugia N , Benoit CE , Begel V , Verga L , Harding E , Kotz SA ((2017) ) BAASTA: Battery for the assessment of auditory sensorimotor and timing abilities. Behav Res Methods 49: , 1128–1145. |
[14] | Ghilain M , Hobeika L , Lesaffre M , Schiaratura L , Singh A , Six J , Huvent-Grelle D , Puisieux F , Samson S ((2020) ) Does a live performance impact synchronization to musical rhythm in cognitively impaired elderly? J Alzheimers Dis 78: , 939–949. |
[15] | Repp BH ((2010) ) Sensorimotor synchronization and perception of timing: Effects of music training and task experience. Hum Mov Sci 29: , 200–213. |
[16] | Rose D , Delevoye-Turrell Y , Ott L , Annett LE , Lovatt PJ ((2019) ) Music and metronomes differentially impact motor timing in people with and without Parkinson’s disease: Effects of slow, medium, and fast tempi on entrainment and synchronization performances in finger tapping, toe tapping, and stepping on the spot tasks. Parkinsons Dis 2019: , 6530838. |
[17] | Vorberg D , Wing A ((1996) ) Modeling variability and dependence in timing. In Handbook of perception and action, Heuer H, Keele SW, eds. Elsevier, pp. 181–262. . |
[18] | Repp BH ((2001) ) Processes underlying adaptation to tempo changes in sensorimotor synchronization. Hum Mov Sci 20: , 277–312. |
[19] | Friedman NP , Miyake A , Corley RP , Young SE , DeFries JC , Hewitt JK ((2006) ) Not all executive functions are related to intelligence. Psychol Sci 17: , 172–179. |
[20] | Drewing K , Aschersleben G , Li SC ((2006) ) Sensorimotor synchronization across the life span. Int J Behav Dev 30: , 280–287. |
[21] | McAuley JD , Jones MR , Holub S , Johnston HM , Miller NS ((2006) ) The time of our lives: Life span development of timing and event tracking. J Exp Psychol Gen 135: , 348. |
[22] | Bangert AS , Balota DA ((2012) ) Keep up the pace: Declines in simple repetitive timing differentiate healthy aging from the earliest stages of Alzheimer’s disease. J Int Neuropsychol Soc 18: , 1052–1063. |
[23] | Krampe RT , Engbert R , Kliegl R ((2001) ) Age-specific problems in rhythmic timing. Psychol Aging 16: , 12–30. |
[24] | Krampe RT , Kliegl R , Mayr U ((2005) ) Timing, sequencing, and executive control in repetitive movement production. J Exp Psychol Hum Percept Perform 31: , 379–397. |
[25] | Vanneste S , Pouthas V , Wearden JH ((2001) ) Temporal control of rhythmic performance: A comparison between young and old adults. Exp Aging Res 27: , 83–102. |
[26] | Duchek JM , Balota DA , Ferraro FR ((1994) ) Component analysis of a rhythmic finger tapping task in individuals with senile dementia of the Alzheimer type and in individuals with Parkinson’s disease. Neuropsychology 8: , 218–226. |
[27] | Thompson EC , White-Schwoch T , Tierney A , Kraus N ((2015) ) Beat synchronization across the lifespan: Intersection of development and musical experience. PLoS One 10: , 1–13. |
[28] | Krampe RT , Doumas M , Lavrysen A , Rapp M ((2010) ) The costs of taking it slowly: fast and slow movement timing in older age. Psychol Aging 25: , 980–990. |
[29] | Grady C ((2012) ) The cognitive neuroscience of ageing. Nat Rev Neurosci 13: , 491–505. |
[30] | Harada CN , Natelson Love MC , Triebel KL ((2013) ) Normal cognitive aging. Clin Geriatr Med 29: , 737–752. |
[31] | von Schnehen A , Hobeika L , Huvent-Grelle D , Samson S ((2022) ) Sensorimotor synchronization in healthy aging and neurocognitive disorders. Front Psychol 13: , 838511. |
[32] | Martin E , Blais M , Albaret JM , Pariente J , Tallet J ((2017) ) Alteration of rhythmic unimanual tapping and anti-phase bimanual coordination in Alzheimer’s disease: A sign of inter-hemispheric disconnection? Hum Mov Sci 55: , 43–53. |
[33] | Carment L , Abdellatif A , Lafuente-Lafuente C , Pariel S , Maier MA , Belmin J , Lindberg PG ((2018) ) Manual dexterity and aging: A pilot study disentangling sensorimotor from cognitive decline. Front Neurol 9: , 910. |
[34] | Henley SMD , Downey LE , Nicholas JM , Kinnunen KM , Golden HL , Buckley A , Mahoney CJ , Crutch SJ ((2014) ) Degradation of cognitive timing mechanisms in behavioural variant frontotemporal dementia. Neuropsychologia 65: , 88–101. |
[35] | Hobeika L , Ghilain M , Schiaratura L , Lesaffre M , Puisieux F , Huvent-Grelle D , Samson S ((2022) ) The effect of the severity of neurocognitive disorders on emotional and motor responses to music. Ann N Y Acad Sci 1518: , 231–238. |
[36] | Folstein MF , Robins LN , Helzer JE ((1983) ) The mini-mental state examination. Arch Gen Psychiatry 40: , 812. |
[37] | Large EW , Herrera JA , Velasco MJ ((2015) ) Neural networks for beat perception in musical rhythm. Front Syst Neurosci 9: , 159. |
[38] | Agosta F , Rocca MA , Pagani E , Absinta M , Magnani G , Marcone A , Falautano M , Comi G , Gorno-Tempini ML , Filippi M ((2010) ) Sensorimotor network rewiring in mild cognitive impairment and Alzheimer’s disease. Hum Brain Mapp 31: , 515–525. |
[39] | Ferreri F , Vecchio F , Vollero L , Guerra A , Petrichella S , Ponzo D , Määtta S , Mervaala E , Könönen M , Ursini F , Pasqualetti P , Iannello G , Rossini PM , Di Lazzaro V ((2016) ) Sensorimotor cortex excitability and connectivity in Alzheimer’s disease: A TMS-EEG Co-registration study. Hum Brain Mapp 37: , 2083–2096. |
[40] | Verga L , Schwartze M , Stapert S , Winkens I , Kotz SA ((2021) ) Dysfunctional timing in traumatic brain injury patients: co-occurrence of cognitive, motor, and perceptual deficits. Front Psychol 12: , 731898. |
[41] | Vishne G , Jacoby N , Malinovitch T , Epstein T , Frenkel O , Ahissar M ((2021) ) Slow update of internal representations impedes synchronization in autism. Nat Commun 12: , 5439. |
[42] | Schwartze M , Keller PE , Patel AD , Kotz SA ((2011) ) The impact of basal ganglia lesions on sensorimotor synchronization, spontaneous motor tempo, and the detection of tempo changes. Behav Brain Res 216: , 685–691. |
[43] | Schwartze M , Keller PE , Kotz SA ((2016) ) Spontaneous, synchronized, and corrective timing behavior in cerebellar lesion patients. Behav Brain Res 312: , 285–293. |
[44] | Stopford CL , Thompson JC , Neary D , Richardson AMT , Snowden JS ((2012) ) Working memory, attention, and executive function in Alzheimer’s disease and frontotemporal dementia. Cortex 48: , 429–446. |
[45] | Garrett KD , Browndyke JN , Whelihan W , Paul RH , DiCarlo M , Moser DJ , Cohen RA , Ott BR ((2004) ) The neuropsychological profile of vascular cognitive impairment—no dementia: comparisons to patients at risk for cerebrovascular disease and vascular dementia. Arch Clin Neuropsychol 19: , 745–757. |
[46] | Kowalczyk A , McDonald S , Cranney J , McMahon M ((2001) ) Cognitive flexibility in the normal elderly and in persons with dementia as measured by the written and oral Trail Making Tests. Brain Impair 2: , 11–21. |
[47] | Desmet F , Lesaffre M , Six J , Ehrlé N , Samson S ((2017) ) Multimodal analysis of synchronization data from patients with dementia. Proc 25th Anniv Conf Eur Soc Cogn Sci Music 31: , 53–58. |
[48] | Lesaffre M , Moens B , Desmet F ((2017) ) Monitoring music and movement interaction in people with dementia. In The Routledge Companion to embodied music interaction, Lesaffre M, Maes P-J, Leman M, eds. Routledge, pp. 294–303. |
[49] | Ghilain M , Hobeika L , Schiaratura L , Lesaffre M , Six J , Desmet F , Clément S , Samson S ((2020) ) Sensorimotor synchronization and non-verbal behaviors in Alzheimer’s disease: The influence of social and musical context. Geriatr Psychol Neuropsychiatr Vieil 18: , 213–222. |
[50] | Hobeika L , Ghilain M , Schiaratura L , Lesaffre M , Huvent-Grelle D , Puisieux F , Samson S ((2021) ) Socio-emotional and motor engagement during musical activities in older adults with major neurocognitive impairment. Sci Rep 11: , 15291. |
[51] | Fiveash A , Bella SD , Bigand E , Gordon RL , Tillmann B ((2022) ) You got rhythm, or more: The multidimensionality of rhythmic abilities. Atten Percept Psychophys 84: , 1370–1392. |
[52] | Pewsey A , Neuhäuser M , Ruxton GD ((2013) ) Circular statistics in R,Oxford University Press, Oxford. |
[53] | Yesavage JA , Brink TL , Rose TL , Lum O , Huang V , Adey M , Leirer VO ((1982) ) Development and validation of a geriatric depression screening scale: A preliminary report. J Psychiatr Res 17: , 37–49. |
[54] | Pachana NA , Byrne GJ , Siddle H , Koloski N , Harley E , Arnold E ((2007) ) Development and validation of the Geriatric Anxiety Inventory. Int Psychogeriatr 19: , 103. |
[55] | Fisher NI ((1995) ), Statistical analysis of circular data, Cambridge University Press. |
[56] | Berens P ((2009) ) CircStat: A MATLAB Toolbox for Circular Statistics. J Stat Softw 31: , 1–21. |
[57] | The MathWorks Inc ((2022) ) MATLAB, version 9.12.0. Natick, MA. |
[58] | Kirschner S , Tomasello M ((2009) ) Joint drumming: Social context facilitates synchronization in preschool children. J Exp Child Psychol 102: , 299–314. |
[59] | R Core Team ((2023) ) R: A language and environment for statistical computing. |
[60] | RStudio Team ((2023) ) RStudio: Integrated Development Environment for R. |
[61] | Brooks ME , Kristensen K , Benthem KJ , van , Magnusson A , Berg CW , Nielsen A , Skaug HJ , Mächler M , Bolker BM ((2017) ) glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. R J 9: , 378. |
[62] | Bates D , Mächler M , Bolker B , Walker S ((2014) ) Fitting linear mixed-effects models using lme4. |
[63] | Selya AS , Rose JS , Dierker LC , Hedeker D , Mermelstein RJ ((2012) ) A practical guide to calculating Cohen’s f2, a measure of local effect size, from PROC MIXED. Front Psychol 3: , 111. |
[64] | Galasko D , Bennett D , Sano M , Ernesto C , Thomas R , Grundman M , Ferris S ((1997) ) An inventory to assess activities of daily living for clinical trials in Alzheimer’s disease. Alzheimer Dis Assoc Disord 11: , S33–S39. |
[65] | Lawton MP , Brody EM ((1969) ) Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 9: , 179–186. |
[66] | Fiveash A , Ferreri L , Bouwer FL , Kösem A , Moghimi S , Ravignani A , Keller PE , Tillmann B ((2023) ) Can rhythm-mediated reward boost learning, memory, and social connection? Perspectives for future research. Neurosci Biobehav Rev 149: , 105153. |
[67] | Repp BH , Keller PE ((2004) ) Adaptation to tempo changes in sensorimotor synchronization: Effects of intention, attention, and awareness. Q J Exp Psychol Sect Hum Exp Psychol 57: , 499–521. |
[68] | Thaut MH , Miller RA , Schauer LM ((1998) ) Multiple synchronization strategies in rhythmic sensorimotor tasks: Phase vs period correction. Biol Cybern 79: , 241–250. |
[69] | McClelland GH , Judd CM ((1993) ) Statistical difficulties of detecting interactions and moderator effects. Psychol Bull 114: , 376. |
[70] | Allman MJ , Pelphrey KA , Meck WH ((2012) ) Developmental neuroscience of time and number: implications for autism and other neurodevelopmental disabilities. Front Integr Neurosci 6: , 7. |
[71] | Bégel V , Dalla Bella S , Devignes Q , Vandenbergue M , Lemaître M-P , Dellacherie D ((2022) ) Rhythm as an independent determinant of developmental dyslexia. Dev Psychol 58: , 339–358. |
[72] | Dalla Bella S , Benoit CE , Farrugia N , Keller PE , Obrig H , Mainka S , Kotz SA ((2017) ) Gait improvement via rhythmic stimulation in Parkinson’s disease is linked to rhythmic skills. Sci Rep 7: , 42005. |
[73] | Metzler-Baddeley C , Cantera J , Coulthard E , Rosser A , Jones DK , Baddeley RJ ((2014) ) Improved executive function and callosal white matter microstructure after rhythm exercise in Huntington’s disease. J Huntingtons Dis 3: , 273–283. |
[74] | Noreika V , Falter CM , Rubia K ((2013) ) Timing deficits in attention-deficit/hyperactivity disorder (ADHD): Evidence from neurocognitive and neuroimaging studies. Neuropsychologia 51: , 235–266. |
[75] | Puyjarinet F , Bégel V , Lopez R , Dellacherie D , Dalla Bella S ((2017) ) Children and adults with attention-deficit/hyperactivity disorder cannot move to the beat. Sci Rep 7: , 11550. |
[76] | Thomson JM , Leong V , Goswami U ((2013) ) Auditory processing interventions and developmental dyslexia: a comparison of phonemic and rhythmic approaches. Read Writ 26: , 139–161. |
[77] | Degé F , Kerkovius K ((2018) ) The effects of drumming on working memory in older adults. Ann N Y Acad Sci 1423: , 242–250. |
[78] | Jünemann K , Marie D , Worschech F , Scholz DS , Grouiller F , Kliegel M , Van De Ville D , James CE , Krüger THC , Altenmüller E , Sinke C ((2022) ) Six months of piano training in healthy elderly stabilizes white matter microstructure in the fornix, compared to an active control group. Front Aging Neurosci 14: , 817889. |
[79] | Marie D , Müller CAH , Altenmüller E , Van De Ville D , Jünemann K , Scholz DS , Krüger THC , Worschech F , Kliegel M , Sinke C , James CE ((2023) ) Music interventions in 132 healthy older adults enhance cerebellar grey matter and auditory working memory, despite general brain atrophy. Neuroimage Rep 3: , 100166. |
[80] | Worschech F , Marie D , Jünemann K , Sinke C , Krüger THC , Grossbach M , Scholz DS , Abdili L , Kliegel M , James CE , Altenmüller E ((2021) ) Improved speech in noise perception in the elderly after 6 months of musical instruction. Front Neurosci 15: , 696240. |
[81] | Turgeon M , Wing AM , Taylor LW ((2011) ) Timing and aging: slowing of fastest regular tapping rate with preserved timing error detection and correction. Psychol Aging 26: , 150–161. |
[82] | Nagasaki H , Itoh H , Maruyama H , Hashizume K ((1988) ) Characteristic difficulty in rhythmic movement with aging and its relation to Parkinson’s disease. Exp Aging Res 14: , 171–176. |
[83] | Heuninckx S , Wenderoth N , Debaere F , Peeters R , Swinnen SP ((2005) ) Neural basis of aging: The penetration of cognition into action control. J Neurosci 25: , 6787–6796. |
[84] | Heuninckx S , Wenderoth N , Swinnen SP ((2008) ) Systems neuroplasticity in the aging brain: Recruiting additional neural resources for successful motor performance in elderly persons. J Neurosci 28: , 91–99. |
[85] | Seidler RD , Bernard JA , Burutolu TB , Fling BW , Gordon MT , Gwin JT , Kwak Y , Lipps DB ((2010) ) Motor control and aging: Links to age-related brain structural, functional, and biochemical effects. Neurosci Biobehav Rev 34: , 721–733. |
[86] | Bangert AS , Reuter-Lorenz PA , Walsh CM , Schachter AB , Seidler RD ((2010) ) Bimanual coordination and aging: Neurobehavioral implications. Neuropsychologia 48: , 1165–1170. |
[87] | Serbruyns L , Gooijers J , Caeyenberghs K , Meesen RL , Cuypers K , Sisti HM , Leemans A , Swinnen SP ((2015) ) Bimanual motor deficits in older adults predicted by diffusion tensor imaging metrics of corpus callosum subregions. Brain Struct Funct 220: , 273–290. |
[88] | Solesio-Jofre E , Serbruyns L , Woolley DG , Mantini D , Beets IA , Swinnen SP ((2014) ) Aging effects on the resting state motor network and interlimb coordination. Hum Brain Mapp 35: , 3945–3961. |
[89] | Summers JJ , Lewis J , Fujiyama H ((2010) ) Aging effects on event and emergent timing in bimanual coordination. Hum Mov Sci 29: , 820–830. |
[90] | Shea CH , Park J-H , Wilde Braden H ((2006) ) Age-related effects in sequential motor learning. Phys Ther 86: , 478–488. |
[91] | Park KS , Buseth L , Hong J , Etnier JL ((2023) ) Music-based multicomponent exercise training for community-dwelling older adults with mild-to-moderate cognitive decline: a feasibility study. Front Med 10: , 1224728. |
[92] | Alter DA , O’Sullivan M , Oh PI , Redelmeier DA , Marzolini S , Liu R , Forhan M , Silver M , Goodman JM , Bartel LR ((2015) ) Synchronized personalized music audio-playlists to improve adherence to physical activity among patients participating in a structured exercise program: a proof-of-principle feasibility study. Sports Med Open 1: , 23. |
[93] | Bugos JA ((2019) ) The effects of bimanual coordination in music interventions on executive functions in aging adults. Front Integr Neurosci 13: , 68. |
[94] | Lin FR , Niparko JK , Ferrucci L ((2011) ) Hearing loss prevalence in the United States. Arch Intern Med 171: , 1851–1853. |
[95] | Evans JR , Fletcher AE , Wormald RPL , Ng ES-W , Stirling S , Smeeth L , Breeze E , Bulpitt CJ , Nunes M , Jones D , Tulloch A ((2002) ) Prevalence of visual impairment in people aged 75 years and older in Britain: results from the MRC trial of assessment and management of older people in the community. Br J Ophthalmol 86: , 795–800. |
[96] | Michon JJ ((2002) ) Prevalence of visual impairment, blindness, and cataract surgery in the Hong Kong elderly. Br J Ophthalmol 86: , 133–139. |
[97] | Miyazaki A , Ito Y , Okuyama T , Mori H , Sato K , Ichiki M , Hiyama A , Dinet J , Nouchi R ((2023) ) Association between upper limb movements during drumming and cognition in older adults with cognitive impairment and dementia at a nursing home: a pilot study. Front Rehabil Sci 4: , 1079781. |
[98] | Dalla Bella S ((2022) ) Rhythmic serious games as an inclusive tool for music-based interventions. Ann N Y Acad Sci 1517: , 15–24. |
[99] | OpenAI ((2023) ) ChatGPT. version 3.5. |


