
Blood endocan as a biomarker for breast cancer recurrence
Abstract
BACKGROUND:
Endocan was reported to affect breast cancer patients negatively and was able to be detected from patients’ blood.
OBJECTIVE:
This study aimed to investigate if the measurement of blood endocan in breast cancer patients with high ESM1 expression could be an effective tool to detect postoperative recurrence compared with existing tumor markers.
METHODS:
Blood was collected before and after the tumor resection from the mouse models of breast cancer, and endocan levels were measured while visualizing metastatic recurrence with noninvasive luminescence imaging. In clinical settings, blood was withdrawn from 16 breast cancer patients before and after the tumor resection, and the effect of lumpectomy on blood endocan level was evaluated. Additionally, the blood endocan from 20 patients diagnosed with postoperative recurrence was measured, and their positivity rate for endocan was compared with that for serum carcinoembryonic antigen (CEA) or cancer antigen 15-3 (CA15-3).
RESULTS:
Our preclinical and clinical experiments revealed that blood endocan levels reflected tumor burden. Furthermore, over 60% of patients suffering from postoperative recurrence who tested negative for CEA or CA15-3 were positive for endocan.
CONCLUSIONS:
Our results support the clinical significance of endocan in breast cancer patients for detecting breast cancer recurrence.
1.Introduction
Breast cancer is now the leading cause of cancer incidence in women worldwide, accounting for one in four cancer cases and one in six cancer deaths [1]. Although the overall prognosis for breast cancer patients is relatively good when detected early, relative to other cancers, it has a high recurrence rate after surgery [2]. Cancer recurrence affects the patient’s prognosis and quality of life, posing a critical clinical problem in later years as they often resist chemotherapy. The potential for recurrence and metastasis of breast cancer varies by subtypes, proliferative potential, and dormancy [3, 4]. Even in the same subtype, recurrence-free survival varies from patient to patient; some patients experience recurrence within one year, while others do not see any recurrence over five years. Therefore, it is beneficial to predict whether each breast cancer patient is prone to relapse individually so that the frequency of follow-up tests would be personalized. For those who experience breast cancer recurrence, it is also helpful if recurrence can be diagnosed as early as possible by sensitive tests in a patient-friendly manner. Follow-up management after the initial treatment of breast cancer, such as adjuvant or neoadjuvant therapy, has generally involved physical examination and diagnostic imaging [5].
Simple and minimally invasive measurement of blood-based tumor markers is used for early detection of cancer and monitoring treatment response. Carcinoembryonic antigen (CEA) and cancer antigen 15-3 (CA15-3) are, in particular, often used as tumor markers for several cancers in clinical settings [6, 7]. CEA is a glycoprotein involved in cell adhesion and is known to be elevated in many cancers [8]. CA15-3 is a glycan-containing protein antigen of the transmembrane glycoprotein MUC-1 and has been reported to be associated with breast cancer stage and survival [9]. These two markers have been validated in several studies to measure changes in patients’ blood to evaluate their application for early detection of cancer recurrence and monitoring treatment response [10, 11]; however, there is little data available about the utility of these markers in asymptomatic or early-stage cancers. Although the frequent measurements of tumor markers in the blood have not been strongly recommended by several guidelines [12, 13], developing effective biomarkers to detect breast cancer recurrence is critical since liquid biopsy is generally more sensitive and cost-effective than diagnostic imaging.
Recently, endocan has received increasing attention as one of the blood-based biomarkers to detect various cancers. Endocan, encoded by the ESM1 gene, is a human endothelial cell-specific molecule soluble dermatan sulfate proteoglycan known to circulate in the bloodstream [14, 15]. Endocan expression is reportedly associated with clinicopathological parameters and poor prognosis in several cancers, including gastric cancer [16], hepatocellular carcinoma [17], prostate cancer [18], bladder cancer [19], and breast cancer [20]. Our previous study demonstrated that an elevated expression of ESM1 in MDA-MB-231 cells, a human triple-negative breast cancer (TNBC) cell line, increased cell proliferation, and tumor formation and that TNBC patients with high ESM1 expression in primary breast cancer had significantly shorter relapse-free survival [21]. In addition, blood endocan levels in luminal-type breast cancer patients were associated with cancer staging [20]. Therefore, since ESM1 negatively impacts breast cancer patients and endocan, the gene product of ESM1, can be detected from the peripheral blood samples, the association between the status of breast cancer and blood endocan levels is clinically worth pursuing.
To bridge the gap between endocan’s preclinical and clinical value as a blood-based biomarker, we sought to measure and assess the blood endocan levels in murine models of breast cancer and breast cancer patients. To the best of our knowledge, this is the first study to investigate the extent to which blood endocan levels in mice and patients with breast cancer are affected by the surgical removal of primary tumors and postoperative recurrence.
2.Materials and methods
2.1Cell culture
This study used the MDA-MB-231BR cell line, a metastatic variant of human-derived triple-negative breast cancer cell line MDA-MB-231 [22]. Our previous study reported that MDA-MB-231BR cells overexpressed ESM1 and secreted measurable amounts of endocan, which was detected from the supernatant of the conditioned medium as well as the blood of mouse models bearing MDA-MB-231BR tumor, which was not the case with MDA-MB-231 [21]. To our knowledge, the MDA-MB-231BR cell line is the only human breast cancer cell line overexpressing ESM1 thus far, which is why we used MDA-MB-231BR in this study.
MDA-MB-231BR was a kind gift from Dr. Patricia Steeg (National Cancer Institute, Bethesda, MD, USA). MDA-MB-231BR was cultured in RPMI-1640 (FujiFilm Wako Pure Chemical Corp., Osaka, Japan) with 10% fetal bovine serum (Thermo Fisher Scientific Inc.) and maintained under aseptic conditions of 5% CO2 at 37∘C. Contamination with Mycoplasma or fungi was routinely checked, and only uncontaminated cells were used. Cell line authentification was outsourced to BEX Co, Ltd. (Tokyo, Japan), and MDA-MB-231BR/mVenus-Akaluc, detailed in the next section, was confirmed to be the identical cell strain to MDA-MB-231.
2.2Generation of MDA-MB-231BR/mVenus-Akaluc
Primer was designed from pcDNA3 Venus-Akaluc vector (RDB15781; Riken BioResource Research Center, Ibaraki, Japan), and Q5® High-Fidelity 2X Master Mix (New England Biolabs, MA, USA) was used to amplify the DNA. The mVenus-Akaluc primers used for PCR amplification were as follows: FW, 5’-TAG AGC TAG CGA ATT ATG GTG AGC AAG GGC GAG-3’ (33 bp); and RV, 5’-ATT TAA ATT CGA ATT CCA TAG AGC CCA CCG CAT-3’ (33 bp). PiggyBac
2.3Animals
Female athymic nu/nu mice (Balb/c background, four weeks old, 17–20 g) and NOD.Cg-PrkdcscidIl2rgtm1Wjl/SzJ (NSG) mice (4 weeks old, 16–21 g) were purchased from CLEA Japan, Inc. (Tokyo, Japan) and The Jackson Laboratory Japan, Inc. (Kanagawa, Japan), respectively. The institutional animal care committee at Hoshi University approved the study protocol (Protocol #: 19-083) before the animal experiments.
2.4Blood endocan measurements and luminescence imaging of mice bearing orthotopic breast cancer
One million MDA-MB-231BR/mVenus-Akaluc cells were orthotopically inoculated into the mammary fat pad of mice. The tumor volume was measured and calculated in a blinded manner using a caliper:
Considering the susceptibility of mouse strain to metastatic recurrence, the primary tumor was resected from each mouse once the tumor volume exceeded 500 mm3 in nude mice and 200 mm3 in NSG mice.
Local or metastatic recurrence was visually detected by luminescence imaging with IVIS Lumina Series III after intraperitoneal injection of akaLumine
In order to quantitate endocan in the peripheral blood of nude and NSG mice, blood was collected from the tail vein at predetermined time points. Plasma was isolated by centrifugation at 4∘C, 1,200
2.5Blood collection from breast cancer patients
Clinical studies were approved by the Institutional Review Board from Showa University Hospital (#2880) and Hoshi University (#2019-12, #2021-04), which preceded the participation of the patients in this study. Participation in the study was voluntary, and written informed consent was received from all subjects. Patients with diabetes, an infectious disease, or other types of cancer were excluded from this study because all of those conditions are known to affect blood endocan levels [23, 24, 25, 26, 27, 28, 29]. The patient’s blood samples were sent to a certified clinical lab for the routine measurements of tumor markers, CEA and CA15-3. CEA concentration of over 5 ng/mL and CA15-3 concentration of over 31.5 U/mL indicated positive for serum CEA and CA15-3, respectively.
Blood was collected from breast cancer patients at the Breast Center of Showa University Hospital (Tokyo, Japan) between 2020 and 2021, and the patient population is summarized in
Supplementary Tables 1 and 2. Plasma was isolated by centrifugation at 4∘C, 1,200
2.6Enzyme-linked immunosorbent assay (ELISA) for the quantification of endocan
Plasma samples were diluted twice with sample diluent, and endocan was quantitated using commercial ELISA kits (Lunginnov (Lille, France) for plasma from nude mice and CUSABIO (Wuhan, China) for plasma from NSG mice and humans) according to the manufacturer’s instructions. The detection limit for both ELISA kits was set at 0.156 ng/mL per the protocol of the ELISA kits. Based on our previous study, an endocan level of 1.68 ng/mL or higher was considered positive for endocan [20]. Endocan expression of breast cancer cells was confirmed negative by immunohistochemistry (IHC) in the patients who showed blood endocan levels below the cutoff value (Supplementary Fig. 1) and, thus, was excluded from postsurgical endocan measurements.
2.7Statistical analysis
The normality of the data distribution was estimated using StatPlus:mac software (AnalystSoft Inc., Alexandria, VA, USA). Student’s
3.Results
3.1Blood endocan levels dropped below the detection limit after the surgical removal of primary breast tumors from nude mice
Figure 1.
Effect of removing primary breast tumors on blood endocan levels of nude mice. a & b, Fluorescence micrographs of MDA-MB-231BR/mVenus-Akaluc (a, phase-contrast; b, fluorescence). c & d, Optical imaging (c, fluorescence; d, luminescence) of cell pellets of MDA-MB- 231BR/mVenus-Akaluc (top) and non-transfected original cells (bottom). e, Schedule of in vivo experiments using nude mice (
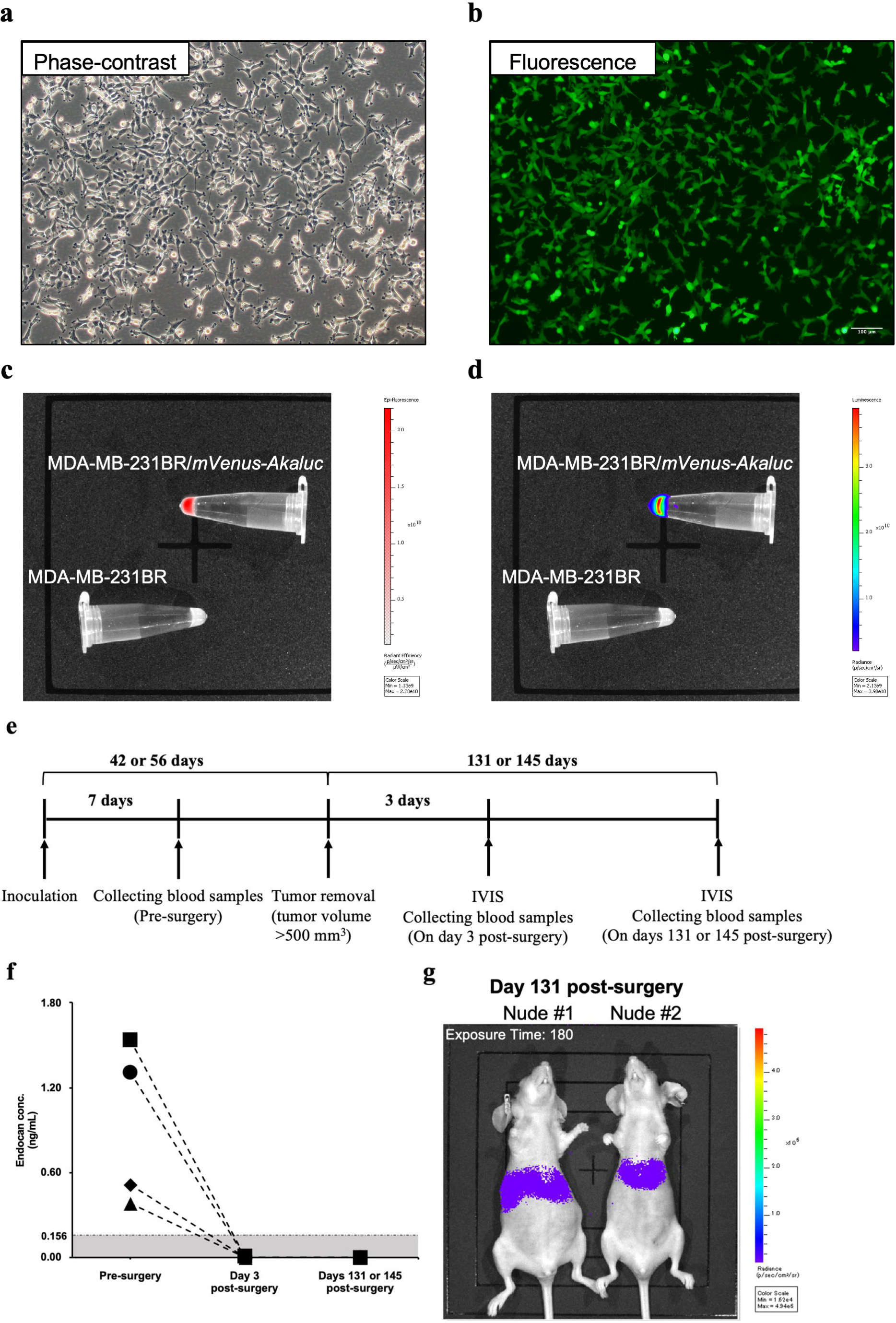
MDA-MB-231BR/mVenus-Akaluc was generated to visualize tumor recurrence and metastasis noninvasively. Fluorescence and luminescence imaging confirmed the expressions of mVenus fluorescent protein (Fig. 1b and 1c) and Akaluc enzyme (Fig. 1d) in MDA-MB-231BR/mVenus-Akaluc. The doubling time of the generated cell line was 22.7
At seven days after inoculation of the MDA-MB-231BR/mVenus-Akaluc, tumor volume reached 56–110 mm3, and blood endocan levels were 0.73 ng/mL (range; 0.38–1.54) (Fig. 1f). When the tumor was resected, plasma endocan levels were below the detection limit of the ELISA kit three days after the surgery. Although weak luminescent signals were detected 131 and 145 days after surgery (Fig. 1g), blood endocan levels remained below the detection limit (Fig. 1f).
3.2Blood endocan levels showed a similar pattern in NSG mice and breast cancer patients after the surgical removal of the primary breast tumor
Figure 2.
Changes in blood endocan levels before and after the surgical removal of primary breast tumors in NSG mice and breast cancer patients. a, Schedule of in vivo experiments using NSG mise (
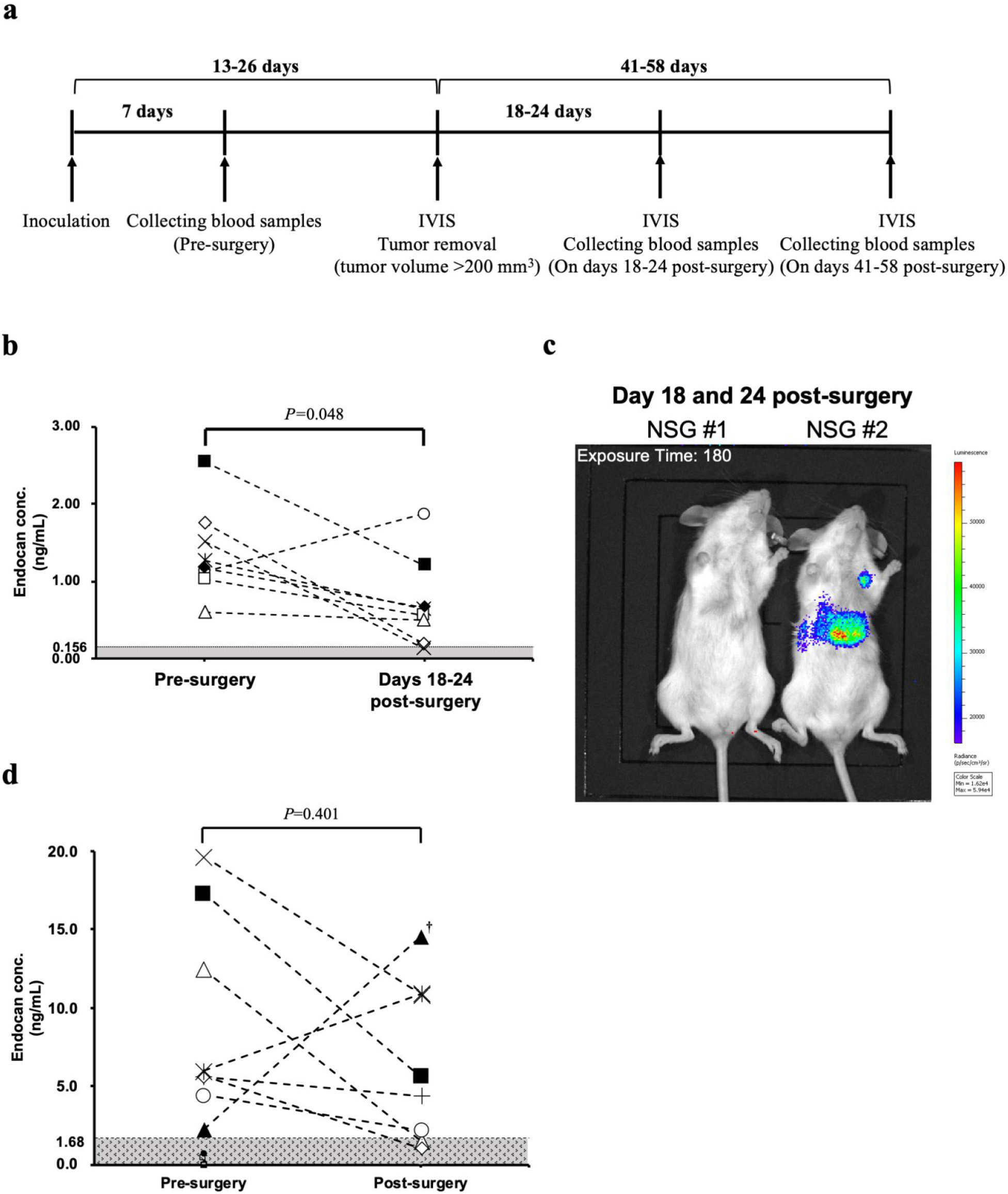
Since elevation of blood endocan levels in the status of recurrence or metastasis was not observed in nude mice, more susceptible NSG mice were used in a similar experiment (Fig. 2a). At seven days after inoculation of MDA-MB-231BR/mVenus-Akaluc, tumor size reached 77–147 mm3 and endocan was detected in all eight mice (range; 0.60–2.54). When the tumor was resected, blood endocan levels dropped in all but one mouse (Fig. 2b). Luminescence imaging displayed weak luminescence signals in distant organs in some mice (Fig. 2c).
To investigate how blood endocan levels respond to tumor resection in the clinical setting, we measured the blood endocan levels of 16 breast cancer patients pre- and post-surgery. Eight patients tested positive for endocan; the endocan level for pre-surgery ranged from 2.24 to 19.64 ng/mL. Blood endocan levels decreased after the surgery except for two patients (Fig. 2d).
3.3Changes in blood endocan level in response to breast cancer recurrence
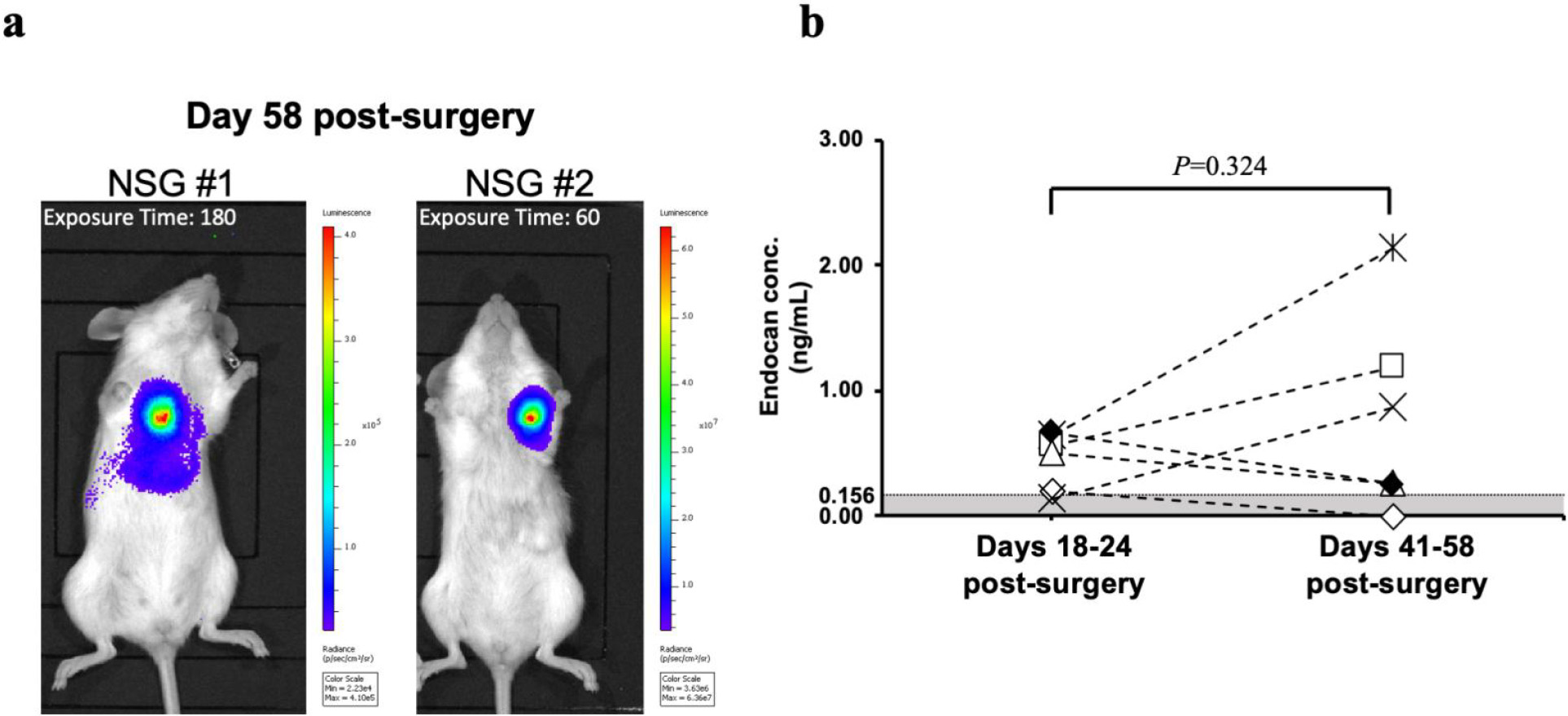
In order to examine the changes in blood endocan levels with the growth of metastatic recurrence, the animals were monitored until recurrent tumor burdens were evident. On days 41–58, metastatic recurrence was observed with strong luminescent signals in all mice tested (Fig. 3a). Relative to 18–24 days post-surgery, blood endocan levels increased on days 41–58 post-surgery in three out of six mice (Fig. 3b). There was no correlation between the luminescence intensity of the metastases and blood endocan levels.
We next assessed the clinical benefit of blood endocan as a blood-based biomarker for breast cancer recurrence. Endocan in the blood of the patients diagnosed with postoperative recurrence (
4.Discussion
For successful clinical translation of endocan as a blood-based breast cancer biomarker, it is critical to be accurately reflected by the status of tumors. Surgical resection of primary breast tumors is expected to reduce blood endocan levels, while recurrence potentially increases blood endocan levels. As expected, removing primary tumors decreased blood endocan levels of the majority of tumor-bearing mice and breast cancer patients. However, most of them did not reach an undetectable level, except for nude mice. Luminescence signals from athymic nude mice were much weaker than the ones from NSG mice, judging from both in vivo and ex vivo bioluminescence imaging (Fig. 1g, Fig. 3a, and Supplementary Fig. 2). NSG mice are more susceptible to engraftment, growth, metastasis, and recurrence of xenogeneic cancer cells than conventional immunodeficient mice, including nude mice [30, 31], which may explain why the number of MDA-MB-231BR/mVenus-Akaluc cells that remained in the body of nude mice was small and did not produce enough endocan detectable in the peripheral blood. Although we do not know how many cells are the detection threshold for blood endocan levels, the number of cells that remained in the body reflected the outcome of blood endocan levels.
Table 1
Comparison of endocan with CEA or CA15-3 in the blood samples of patients with postoperative breast cancer recurrence as a blood-based biomarker
| CEA-negative patients ( | CEA-positive patients ( | CA15-3-negative patients ( | CA15-3-positive patients ( | |
|---|---|---|---|---|
| Endocan-negative patients ( | 5/13 (38.5%) | 2/7 (28.6%) | 5/15 (33.3%) | 2/5 (40%) |
| Endocan-positive patients ( | 8/13 (61.5%) | 5/7 (71.4%) | 10/15 (66.7%) | 3/5 (60%) |
Figure 3.
Effect of breast cancer recurrence on blood endocan levels of NSG mice (
The case is more complicated for breast cancer patients, however, because various diseases, including inflammatory diseases [27], diabetes [28], and sepsis [29], are known to increase blood endocan levels. Although such patients were excluded from this study, unnoticeable inflammation or undeclared events might have occurred during the study, which might be why the blood endocan levels were not entirely down below the cutoff value. As endocan was originally known to express on endothelial cells, active endothelial cells produce and secrete endocan, which might increase blood endocan levels by inflammation. However, the IHC of breast cancer patients revealed that blood endocan levels were below the cutoff value even for patients whose endothelial cells expressed endocan, which was in stark contrast to patients whose cancer cells expressed endocan (Supplementary Fig. 1). With current knowledge, it is difficult to distinguish breast cancer from other diseases from the perspective of blood endocan levels. However, rather than a single-point measurement, multiple blood withdrawal to see the kinetics of endocan in the circulation may help differentiate at least the inflammatory states and breast cancer recurrence. Blood endocan possibly reduces as inflammation heals because most inflammatory states are temporary events. In contrast, blood endocan is constantly high if breast cancer recurrence occurs. Nevertheless, further studies are needed in case breast cancer patients occur with other diseases.
Blood endocan levels of a few individuals were increased even after the surgery, both in NSG mice and breast cancer patients. Although the blood endocan level in one patient whose blood was collected on day 29 post-surgery was increased, that in other two patients whose blood was collected on day 32 post-surgery was decreased (Supplementary Table 3), implying that surgical inflammation was not considered to affect the postsurgical blood endocan levels. Therefore, other than one patient who ran a marathon, which might cause an increase in the blood endocan level, the day before the postsurgical blood collection, it is difficult to identify the reasons for the discrepancy with limited information and sample size.
CEA and CA15-3 have been used in clinical practice for years but are not well supported by clinical evidence [12, 32]. Despite a limited number of patients participating in this study, endocan seems more responsive to breast cancer recurrence than CEA and CA15-3. Due to technical issues, CEA and CA15-3 in mouse models were not measured in this study, as it is necessary to obtain sufficient amounts of mouse plasma to quantify all three markers in each ELISA kit. More importantly, the main objective of this study is not just to compare blood endocan with the existing biomarkers, but eventually to show the “clinical” benefit of blood endocan measurement. Since CEA and CA15-3 are routinely measured in clinical settings, we can compare blood endocan with the existing biomarkers of the same patient, which is more valuable information than preclinical comparisons for future clinical use. Still, one-fourth of the patients with breast cancer recurrence were negative for all three markers (Supplementary Table 4). Not all breast cancer patients have primary tumors expressing endocan, and the patients with postoperative recurrence participating in this study were not prescreened by de novo endocan expression. A longitudinal study tracking endocan-positive breast cancer patients is necessary to corroborate the clinical benefit of blood endocan measurements.
In order to achieve the clinical use of blood endocan measurement for breast cancer recurrence, several possible limitations need to be addressed. First, as described above, blood endocan rises in patients with inflammatory disease, diabetes, and sepsis. Therefore, it is important to include patients without breast cancer recurrence and compare with patients with breast cancer recurrence in order to determine if blood endocan levels are specifically elevated when breast cancer recurrence occurs. However, providing conclusive evidence of “non-recurrence” in patients is challenging as physicians typically do not perform diagnostic imaging if patients do not show any abnormalities during routine follow-up, leaving the recurrence status undetermined. Since performing additional diagnostic tests to confirm “non-recurrence” may impose medical costs, potential radiation exposure from mammography, and unnecessary tissue diagnosis, this study primarily focused on the sensitivity of the blood endocan measurement and left the specificity for future studies. Generally speaking, sensitivity is more important when the consequence of missing a positive case is serious, such as in screening for a life-threatening disease, like cancer, which is the case for this study. In addition, some ELISA kits from other suppliers did not work well with measuring blood endocan in our study. Epitopes that anti-endocan antibodies recognize may vary depending on each ELISA kit supplied by manufacturers, which might be responsible for inconsistent results when ELISA kits from different suppliers were used. We have worked on developing a new alternative to ELISA for future clinical use of blood endocan measurement.
5.Conclusion
This study is the first report on the effect of the surgical resection of primary breast tumors and recurrence on blood endocan levels, and our findings are consistent with the earlier reports for low-grade glioma [33] and renal cell carcinoma [23]. More importantly, the current study demonstrated that blood endocan measurement could detect breast cancer recurrence with a higher probability than conventional tumor markers, CEA and CA15-3, in a limited number of patients (
Author contributions
Conception: SN and YKato.
Interpretation or analysis of data: KD, YKanada, AN, KT, KI, TY, HO, FS, SN, and YKato.
Preparation of the manuscript: KD, FS, SN, and YKato.
Revision for important intellectual content: KD, YKanada, AN, KT, FS, SN, and YKato.
Supervision: KI, FS, SN and YKato.
All authors read and approved the final manuscript.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/CBM-240034.
Acknowledgments
The authors would like to thank Dr. Yosuke Sasaki for his technical assistance. We pay special tribute to Dr. Katsuhide Igarashi, who passed away before publishing this study. This research was supported by JSPS KAKENHI, grant number JP19K07760.
References
[1] | H. Sung, J. Ferlay, R.L. Siegel, M. Laversanne, I. Soerjomataram, A. Jemal and F. Bray, Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries, CA Cancer J Clin 71: ((2021) ), 209–249. |
[2] | G. Disibio and S.W. French, Metastatic patterns of cancers: results from a large autopsy study, Arch Pathol Lab Med 132: ((2008) ), 931–9. |
[3] | M. Moossdorff, M.L.G. Vane, T.J.A. van Nijnatten, M.C. van Maaren, B. Goorts, E.M. Heuts, L.J.A. Strobbe and M.L. Smidt, Conditional local recurrence risk: the effect of event-free years in different subtypes of breast cancer, Breast Cancer Res Treat 186: ((2021) ), 863–870. |
[4] | J. Dittmer, Mechanisms governing metastatic dormancy in breast cancer, Semin Cancer Biol 44: ((2017) ), 72–82. |
[5] | H.J. Burstein and E.P. Winer, Primary care for survivors of breast cancer, N Engl J Med 343: ((2000) ), 1086–94. |
[6] | L. Harris, H. Fritsche, R. Mennel, L. Norton, P. Ravdin, S. Taube, M.R. Somerfield, D.F. Hayes, R.C. Bast Jr. and O. American Society of Clinical, American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer, J Clin Oncol 25: ((2007) ), 5287–312. |
[7] | F. Safi, I. Kohler, E. Rottinger, P. Suhr and H.G. Beger, Comparison of CA 15-3 and CEA in diagnosis and monitoring of breast cancer, Int J Biol Markers 4: ((1989) ), 207–14. |
[8] | M. Grunnet and J.B. Sorensen, Carcinoembryonic antigen (CEA) as tumor marker in lung cancer, Lung Cancer 76: ((2012) ), 138–43. |
[9] | F.G. Ebeling, P. Stieber, M. Untch, D. Nagel, G.E. Konecny, U.M. Schmitt, A. Fateh-Moghadam and D. Seidel, Serum CEA and CA 15-3 as prognostic factors in primary breast cancer, Br J Cancer 86: ((2002) ), 1217–22. |
[10] | A. Nicolini, G. Tartarelli, A. Carpi, M.R. Metelli, P. Ferrari, L. Anselmi, M. Conte, P. Berti and P. Miccoli, Intensive post-operative follow-up of breast cancer patients with tumour markers: CEA, TPA or CA15.3 vs MCA and MCA-CA15.3 vs CEA-TPA-CA15.3 panel in the early detection of distant metastases, BMC Cancer 6: ((2006) ), 269. |
[11] | Y. Fu and H. Li, Assessing clinical significance of serum CA15-3 and carcinoembryonic antigen (cea) levels in breast cancer patients: A meta-analysis, Med Sci Monit 22: ((2016) ), 3154–62. |
[12] | J.L. Khatcheressian, P. Hurley, E. Bantug, L.J. Esserman, E. Grunfeld, F. Halberg, A. Hantel, N.L. Henry, H.B. Muss, T.J. Smith, V.G. Vogel, A.C. Wolff, M.R. Somerfield, N.E. Davidson and O. American Society of Clinical, Breast cancer follow-up and management after primary treatment: American Society of Clinical Oncology clinical practice guideline update, J Clin Oncol 31: ((2013) ), 961–5. |
[13] | F. Cardoso, S. Kyriakides, S. Ohno, F. Penault-Llorca, P. Poortmans, I.T. Rubio, S. Zackrisson and E. Senkus, Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up, Ann Oncol 30: ((2019) ), 1194–1220. |
[14] | P. Lassalle, S. Molet, A. Janin, J.V. Heyden, J. Tavernier, W. Fiers, R. Devos and A.B. Tonnel, ESM-1 is a novel human endothelial cell-specific molecule expressed in lung and regulated by cytokines, J Biol Chem 271: ((1996) ), 20458–64. |
[15] | D. Bechard, T. Gentina, M. Delehedde, A. Scherpereel, M. Lyon, M. Aumercier, R. Vazeux, C. Richet, P. Degand, B. Jude, A. Janin, D.G. Fernig, A.B. Tonnel and P. Lassalle, Endocan is a novel chondroitin sulfate/dermatan sulfate proteoglycan that promotes hepatocyte growth factor/scatter factor mitogenic activity, J Biol Chem 276: ((2001) ), 48341–9. |
[16] | W. Zhao, M. Sun, S. Li, Y. Wang and J. Liu, Biological and clinical implications of endocan in gastric cancer, Tumour Biol 35: ((2014) ), 10043–9. |
[17] | K. Ozaki, N. Toshikuni, J. George, T. Minato, Y. Matsue, T. Arisawa and M. Tsutsumi, Serum endocan as a novel prognostic biomarker in patients with hepatocellular carcinoma, J Cancer 5: ((2014) ), 221–30. |
[18] | B. Arslan, O. Onuk, I. Hazar, M. Aydin, N.C. Cilesiz, A. Eroglu and B. Nuhoglu, Prognostic value of endocan in prostate cancer: clinicopathologic association between serum endocan levels and biochemical recurrence after radical prostatectomy, Tumori 103: ((2017) ), 204–208. |
[19] | E. Laloglu, H. Aksoy, Y. Aksoy, F. Ozkaya and F. Akcay, The determination of serum and urinary endocan concentrations in patients with bladder cancer, Ann Clin Biochem 53: ((2016) ), 647–653. |
[20] | Y. Kanada, K. Daiki, A. Nagata, K. Taruno, T. Kuwayama, R. Hashimoto, H. Masuda, S. Akashi-Tanaka, S. Nakamura and Y. Kato, Clinical significance of blood endocan level in breast cancer patients, Showa Univ J Med Sci 35: ((2023) ), 98–102. |
[21] | A. Sagara, K. Igarashi, M. Otsuka, A. Kodama, M. Yamashita, R. Sugiura, T. Karasawa, K. Arakawa, M. Narita, N. Kuzumaki, M. Narita and Y. Kato, Endocan as a prognostic biomarker of triple-negative breast cancer, Breast Cancer Res Treat 161: ((2017) ), 269–278. |
[22] | T. Yoneda, P.J. Williams, T. Hiraga, M. Niewolna and R. Nishimura, A bone-seeking clone exhibits different biological properties from the MDA-MB-231 parental human breast cancer cells and a brain-seeking clone in vivo and in vitro, J Bone Miner Res 16: ((2001) ), 1486–95. |
[23] | K.H. Kim, H.H. Lee, Y.E. Yoon, J.C. Na, S.Y. Kim, Y.I. Cho, S.J. Hong and W.K. Han, Clinical validation of serum endocan (ESM-1) as a potential biomarker in patients with renal cell carcinoma, Oncotarget 9: ((2018) ), 662–667. |
[24] | Y.C. Yang, K.F. Pan, W.J. Lee, J.H. Chang, P. Tan, C.C. Gu, W.M. Chang, S.F. Yang, M. Hsiao, K.T. Hua and M.H. Chien, Circulating proteoglycan endocan mediates EGFR-driven progression of non-small cell lung cancer, Cancer Res 80: ((2020) ), 3292–3304. |
[25] | Y. Zhu, X. Zhang, L. Qi, Y. Cai, P. Yang, G. Xuan and Y. Jiang, HULC long noncoding RNA silencing suppresses angiogenesis by regulating ESM-1 via the PI3K/Akt/mTOR signaling pathway in human gliomas, Oncotarget 7: ((2016) ), 14429–40. |
[26] | K.F. Pan, Y.C. Yang, W.J. Lee, K.T. Hua and M.H. Chien, Proteoglycan endocan: A multifaceted therapeutic target in Cancer, Biochim Biophys Acta Rev Cancer 1877: ((2022) ), 188672. |
[27] | S.F. Rocha, M. Schiller, D. Jing, H. Li, S. Butz, D. Vestweber, D. Biljes, H.C. Drexler, M. Nieminen-Kelha, P. Vajkoczy, S. Adams, R. Benedito and R.H. Adams, ESM1 modulates endothelial tip cell behavior and vascular permeability by enhancing VEGF bioavailability, Circ Res 115: ((2014) ), 581–90. |
[28] | A. Klisic, N. Kavaric, V. Stanisic, S. Vujcic, V. Spasojevic-Kalimanovska, A. Ninic and J. Kotur-Stevuljevic, Endocan and a novel score for dyslipidemia, oxidative stress and inflammation (DOI score) are independently correlated with glycated hemoglobin (HbA(1c)) in patients with prediabetes and type 2 diabetes, Arch Med Sci 16: ((2020) ), 42–50. |
[29] | A. Scherpereel, F. Depontieu, B. Grigoriu, B. Cavestri, A. Tsicopoulos, T. Gentina, M. Jourdain, J. Pugin, A.B. Tonnel and P. Lassalle, Endocan, a new endothelial marker in human sepsis, Crit Care Med 34: ((2006) ), 532–7. |
[30] | C.C. Milsom, C.R. Lee, C. Hackl, S. Man and R.S. Kerbel, Differential post-surgical metastasis and survival in SCID, NOD-SCID and NOD-SCID-IL-2Rgamma(null) mice with parental and subline variants of human breast cancer: implications for host defense mechanisms regulating metastasis, PLoS One 8: ((2013) ), e71270. |
[31] | E. Iorns, K. Drews-Elger, T.M. Ward, S. Dean, J. Clarke, D. Berry, D. El Ashry and M. Lippman, A new mouse model for the study of human breast cancer metastasis, PLoS One 7: ((2012) ), e47995. |
[32] | T. Naruse, A. Koike, K. Suzumura, K. Matsumoto, Y. Ooiwa, M. Miwa, T. Kojima, T. Kanemitsu and S. Yamamoto, Studies of carcinoembryonic antigen and glucoprotein antigen in sera of patients with breast cancer, J Jpn Prac Surg Soc 49: ((1988) ), 774–778. |
[33] | T. Tanriverdi, R. Kemerdere, B.B. Inal, O. Yuksel, H.O. Emre, M. Ahmedov, O. Baran and S. Ates, Serum endocan levels before and after surgery on low-grade gliomas, Surg Neurol Int 8: ((2017) ), 32. |


