
The use of the Model of Occupational Self Efficacy in improving the cognitive functioning of individuals with brain injury: A pre- and post-intervention study
Abstract
BACKGROUND:
Individuals diagnosed with a Traumatic Brain Injury (TBI) often experience major limitations in returning to work despite participating in rehabilitation programmes.
OBJECTIVE:
The aim of the study was to determine whether individuals who sustained a traumatic brain injury experienced improved cognitive functioning after participating in an intervention programme that utilizes the Model of Occupational Self-Efficacy (MOOSE).
PARTICIPANTS:
Ten (10) individuals who were diagnosed with a mild to moderate brain injury participated in the study.
METHOD:
The research study was positioned within the quantitative paradigm specifically utilizing a pre and post intervention research design. In order to gather data from the participants, the Montreal Cognitive Assessment (MOCA) was used to determine whether the individual with brain injury’s cognitive functioning improved after participating in a vocational rehabilitation model called the Model of Occupational Self Efficacy (MOOSE).
RESULTS:
All the participants in this study presented with an improvement in MOCA test scores. The results of the study revealed a statistically significant effect of the intervention (i.e. MOOSE) on cognitive functioning measured using the Montreal Cognitive Assessment, F(4, 6) = 15.95, p = 0.002.
CONCLUSION:
The findings of this study indicated that MOOSE is a useful model to facilitate the return of individuals living with a TBI back to work. It is also suggested that cognitive rehabilitative activities be included as part of the vocational rehabilitation programme.
1Introduction
Traumatic brain injury is described as an unexpected, damaging blow to the head, or a sharp object penetrating the head that results in the disruption of the functioning of the brain [1]. The brain is launched into a collision with the cranium, resulting in bruising of the brain as well as the severing of nerve fibers and hemorrhaging inside the skull. Archiniegas, Held and Wagner [2] describe TBI as a sudden trauma to the head, which causes injury to the head and the brain; such injuries could result in impaired physical, cognitive, emotional, and behavioral functioning. According to the Kwazulu Natal Department of Health there are an estimate of 89 000 new cases of traumatic brain injuries that are reported annually in South Africa [3]. Fifty percent of all head injuries were due to motor vehicle and motor- pedestrian accidents, 25% have been due to falls, 20% have been due to violence and another 5% due to other injuries [3].
In the medical model, the individual with an injury or disability is regarded as having problems that require mainly medical-biological intervention, with little or no attention given to the difficult process of reintegrating the individual with disability back into society [4]. The medical approach may result in feelings of disempowerment on behalf of the individual with disability regarding the rehabilitation process [4, 5]. The lack of success of current rehabilitation interventions could be seen as a result of an inability to generalize outcomes of rehabilitation in a clinical setting to the skills needed to return to work or re-integrate into the community. This study explored whether the Model of Occupational Self Efficacy could be used practically by an occupational therapist with regard to their time and resources in order to reintegrate individuals with TBI to their worker roles.
2Literature review
Mild, moderate and severe TBI’s are classified using the Glasgow Coma Scale. The Glasgow Coma Scale is described by Gill, Reiley, and Green [6] as the most commonly used scoring system to measure an individual’s consciousness following a traumatic brain injury. The classification of mild, moderate and severe is scored and relates to the time it takes the individual with brain injury to regain consciousness following an assault to the brain. According to Norman [7] the main causes of head injuries in South Africa are road traffic collisions, violence and assaults. Road traffic accidents are amongst the top 3 leading causes of mortality in South Africa.
Holistically, there is evidence that traumatic brain injury negatively affects post injury employment status [8]. Post injury, survivors of brain injury experience a variety of physical, psychological, emotional, cognitive limitations and behavioral problems, which limit their ability to adapt to their worker role [9]. Shames and Giaquinto [10] indicated that individuals with brain injury (IBI) experience limitations with executive functions i.e. problems with goal setting, self-monitoring, and planning that usually impair the individual’s ability to return to work successfully. According to Tyreman [11] these difficulties include a limited work performance and difficulties in applying the coping skills learnt during the vocational rehabilitation (VR) process. Individuals experience difficulty in planning, prioritizing and organizing work to achieve objectives and meet deadlines. Inflexibility to changes in their work role, poor judgment and poor social control are all factors that reduce an individual’s ability to adapt to their worker role. Lefebvre [12] indicated that due to the age and stage that individuals sustain a brain injury, they are often young male workers, the injury results in severe role loss within their families and social circles. Due to these losses they no longer see themselves as contributing members of society. Most often these individuals with brain injury are no longer able to fill their roles as breadwinners in their families.
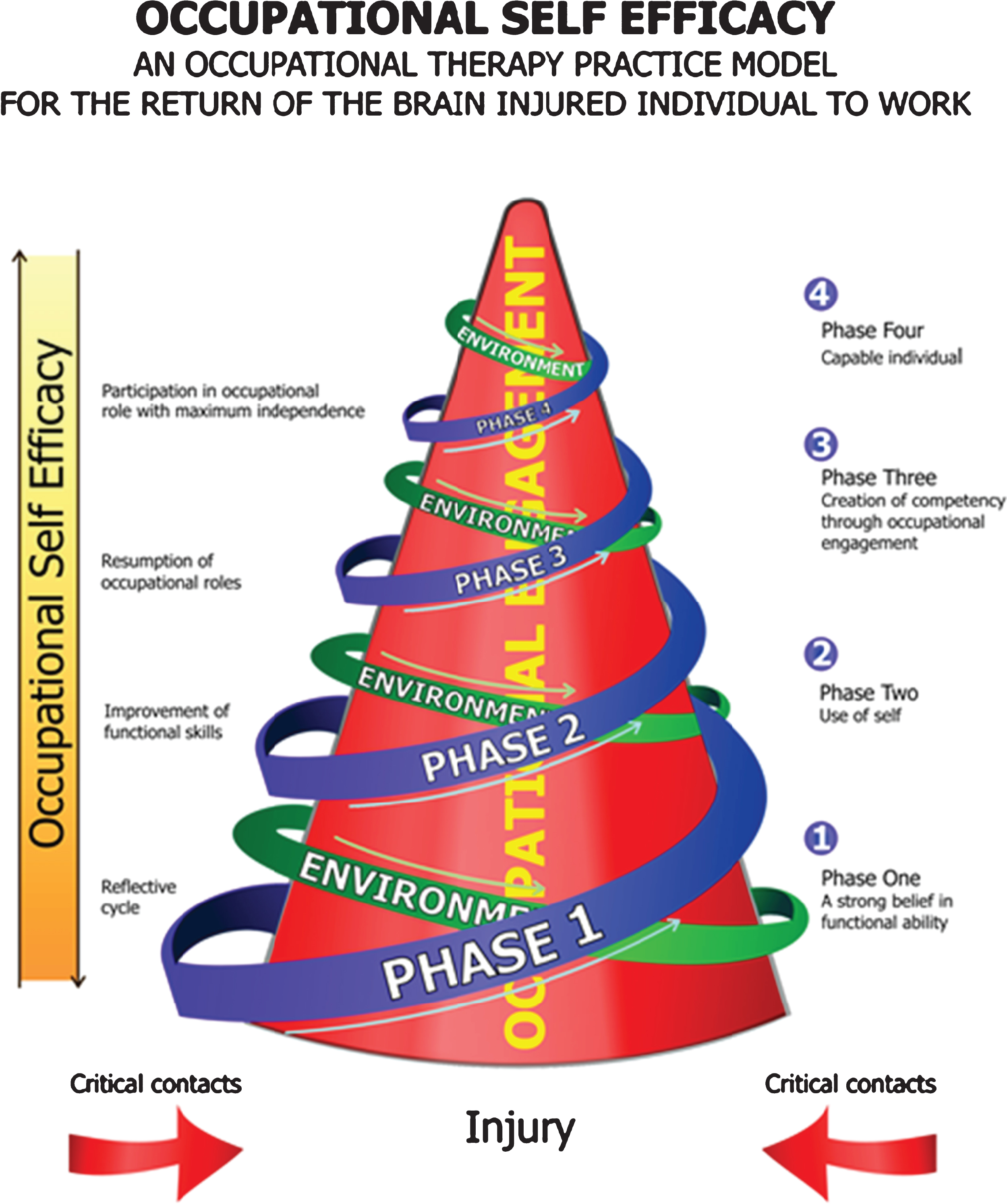
Occupational therapy is a profession that offers services that improve, maintain and restore an injured or ill individual’s ability to engage in occupations such as work related activities, leisure and self-care [13]. The Model of Occupational Self Efficacy developed by Soeker [14] is an occupational therapy practice model designed to effectively return individuals with brain injury to work. The MOOSE consists of 4 stages (see Fig. 1) namely, Stage One: “A strong personal belief in functional abilities”. During this stage the occupational therapist will facilitate a process of introspection and reflection in the client in order to develop new insights into his or her ability to cope in their work and social environment. Stage Two: “Use of Self”. During this stage the occupational therapist continues to act as a facilitator and through a process of introspection and inner strength development, the client reaches a level of autonomy which allows participation in more occupational activities such as activities of daily living, work and leisure. Stage Three: “Creation of competency through occupational engagement”. During this stage the client may be referred to vocational rehabilitation and a functional capacity assessment or screening. The client will be asked to identify a difficult workplace scenario; thereafter the occupational therapist and the client will role play the scenario in order to identify coping strategies for the client. The client will be placed in an actual work setting to practice his or her work skills. Stage Four: “Capable individual” is the final stage of the model. During this stage, the client will view him or herself as a capable worker and will be able to participate in the worker role with maximum independence and the occupational therapist will gradually withdraw as a facilitator.
Fig.1
(Permission was granted from the author to utilise the diagram of the MOOSE).
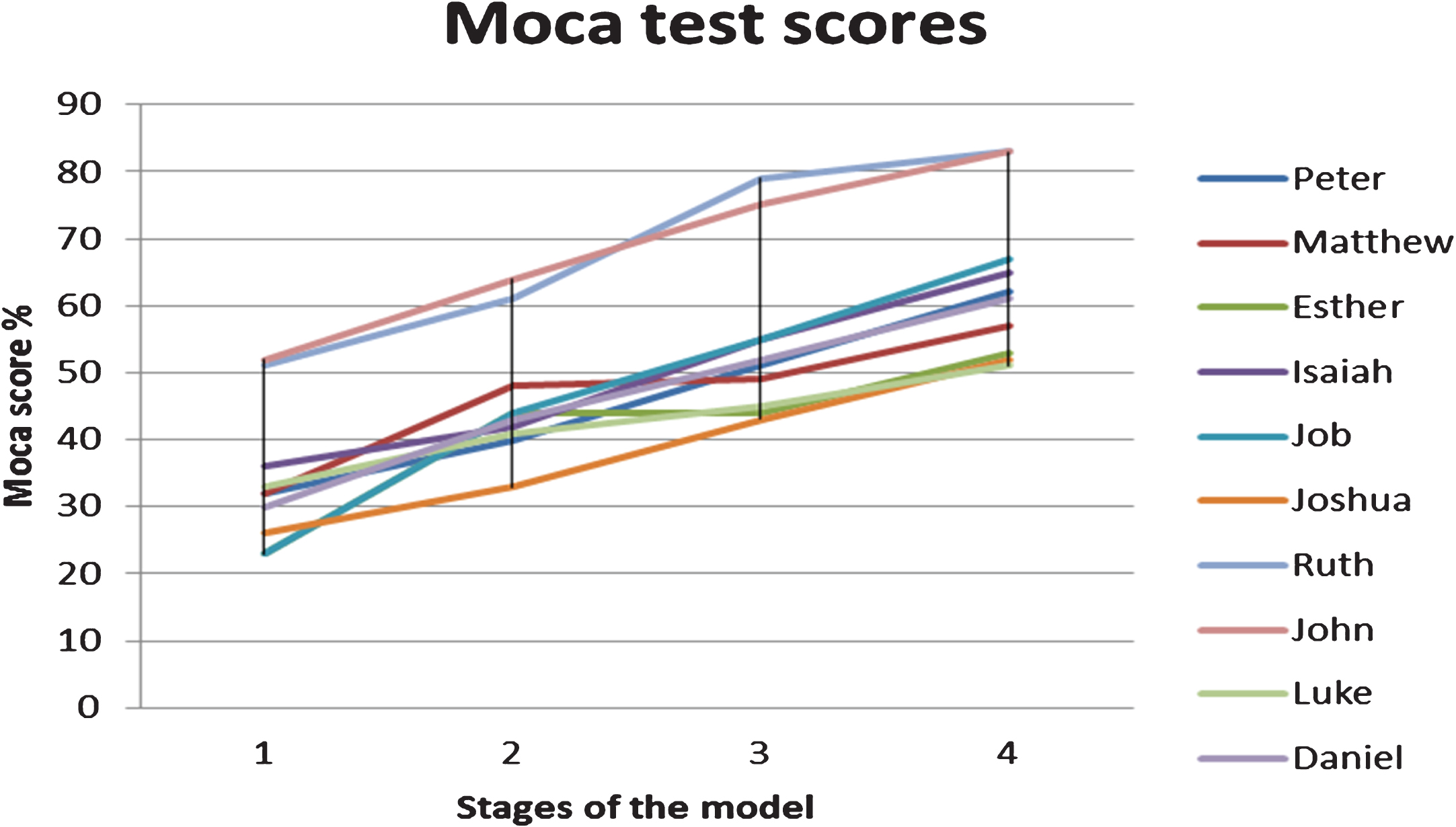
Graph 1
Graph indicating the test scores of the participants using the MOCA.
Graph 2
Results of the repeated measure ANOVA on completed cases.
2.1Aim
To determine whether MOOSE is an effective model to enhance the cognitive skills of individuals with brain injury.
2.2Objectives
∘ To determine whether the client’s memory and attention improves after participating in a vocational rehabilitation programme.
∘ To determine whether the client’s language and abstract thinking improves after participating in a vocational rehabilitation programme.
∘ To determine whether the client’s delayed recall and orientation improves after participating in a vocational rehabilitation programme.
2.3Research design
The current study was positioned in the quantitative paradigm, a pre- post non experimental research design was utilized. With pre experimental designs the researcher studies a single group and provides an intervention during the experiment. These designs do not have a control group to compare with the experimental group [15].
2.4Population and sampling
Simple random sampling was used to select ten (10) participants from the statistical records of the Occupational Therapy Departments of Tertiary Hospitals and Community Health Centers.
2.4.1Inclusion criteria
Participants were diagnosed with either a mild to moderate brain injury according to the Glasgow Coma Scale and they must have been living with a brain injury for at least one year [16]. They must have been employed for remuneration before their injury and at least for 3 months. The participant must have received rehabilitation from a multiple disciplinary team, be able to communicate effectively in English and Afrikaans and be able to understand verbal questions. They were also required to live in Cape Town and be over 18 years old.
2.4.2Exclusion criteria
Participants who had sustained severe head injuries were excluded as literature revealed that the probability of their reintegration into the open labour market as a worker would be limited [17].
Members who had active symptoms related to a psychiatric disorder according to the DSM IV, and individuals with multiple disabilities were also excluded.
2.5Data collection and analysis
A client information data capturing sheet was used to record the patient’s name, demographics, address, telephone number, age, gender, language, employment status, return to work status, leisure, date of discharge from the vocational rehabilitation program, diagnosis and the participant’s MOCA score. Using the different stages of the MOOSE the data related to the MOCA was captured five (5) times (i.e. once before the intervention and then at the completion of each of the 4 stages of theintervention).
2.5.1Application of intervention and procedure followed
The participants in this research study engaged in the vocational rehabilitation process using the MOOSE. Before the participants participated in the programme, they had to provide informed consent. They also had to meet the inclusion and exclusion criteria of the study. In the Pre intervention stage of study the participants were randomly selected to participate in the vocational rehabilitation procedures, the participants then completed the MOCA questionnaire in order to get a baseline score regarding their cognitive functioning. In Stage One: “A strong personal belief in functional abilities”, the participants engaged in a reflection process using the GIBS reflective cycle [18]. During this stage the participants focused on the challenges related to them when returning to work. The types of activities they engaged in were creative writing, using a reflection journal and group as well as individual discussions. In Stage Two: “Use of Self”, the participants participated in activities that would enhance their individual capabilities, such as improving their endurance, muscle strength and cognitive skills. They participated in activities that enhanced their memory such as Kim’s game and table top activities to improve their perceptual skills as well. The participants were often given tasks to do at home to enhance their cognitive skills and then they had to give feedback on their return to the occupational therapy department. In Stage Three: “Creation of competency through occupational engagement”, the participants participated in simulated work tasks in order to specifically improve their work skills. During this stage, the participant engaged in tasks related to a specific job to which they wanted to return (e.g. security guard, shop assistant etc.). These participants would engage in tasks such as role play activities in order to improve their coping skills, problem solving skills and communication skills. They were then placed in a specific job (work test placement) for a temporary period. Support was provided to the participant in the workplace in the form of training the participant on specific parts of the job deemed as problematic (e.g. how to operate a cash register). In Stage Four: “Capable individual” which is the final stage of the model, the participant would either return to their pre-morbid jobs in the open labour market or a new job for a period of at least four (4) months. The participants continued to get support in the workplace if required, however the intensity of support given would be gradually reduced in order to ensure that the participant works independently in their jobs.
Descriptive data was summarized in tables for analysis. Values were accepted as significant at the 5% level (p < 0.05). Data was first captured in excel and analyzed using SPSS along with the assistance of a statistician. The repeated measure ANOVA was used to analyze the data.
2.6Reliability and validity
According to Hoops et al. [22] the MOCA assessment provided good validity and reliability in detecting Mild Cognitive Impairment (MCI). MOCA assesses the following component areas i.e. visual spatial relations, naming, attention, language, abstraction, orientation and identification. The MOCA is scored out of a total of 30 points, with an additional point given if the subject has an education level of Grade 12 and below [19].
The MOCA was used as a cognitive screening tool in a study with 132 patients with Parkinson’s Disease Dementia (PDD), the results indicated that approximately one third of the sample met diagnostic criteria for a cognitive disorder (12.9% PDD and 17.4% MCI), with the mean (SD) MOCA being 25.0 (3.8). The overall discriminant validity for the detection of any cognitive disorder was [95% confidence interval]: MOCA (0.79 [0.72, 0.87]). As a screening instrument, the MOCA was seen as a good instrument for detecting MCI (optimal cut off point = 26/27, 64% correctly diagnosed, lack of ceiling effect). According to Gelb, Oliver and Gilman [20] the MOCA had good test-retest reliability, interrater reliability, and convergent validity as a neuropsychological battery in a small sample of patients with Parkinson’s Disease. It could therefore be argued that based on the latter studies the MOCA is a good cognitive screening tool in order to assess cognitive functioning over time.
In the current study, the questionnaire was piloted with four participants. The participants responded appropriately and the questionnaire proved to have good face and content validity. The results of these participants were not included in the results of the current study.
2.6.1Administration of the questionnaires
The researcher used the MOOSE as a framework to improve the work skills of the participants. The participants in the study therefore participated in all four stages of the Model (i.e. Stage one: “A strong personal belief in functional abilities”, Stage two: “Use of Self”, Stage three: “Creation of competency through occupational engagement” and Stage four: “Capable individual”). During the latter stages, the participants participated in a series of activities such as role playing, life skills training, work endurance training, and activities that promote the enhancement of an individual’s memory. Before the commencement of the participant in the intervention programme, the participants were requested to complete the MOCA questionnaire. A score was obtained and this served as the baseline assessment of their cognitive functioning (pre-intervention score). They were then requested to complete the MOCA after the completion of each stage of the MOOSE (a post-intervention score was obtained). In the current study each stage of the MOOSE was about 1.5 months in duration on average. The researcher therefore used the five scores of the participant’s responses to various sections of the MOCA for the analysis of the participant’s performance.
Demographic information and medical information were obtained from the client’s medical records at a tertiary hospital in Cape Town.
3Results
In Table 1 the characteristics of the 10 participants [n = 10] reveal that [2/10] participants were female and [8/10] were male participants. Furthermore, the mean age of the participants were
Table 1
Demographics of participants
| Names | Age | Gender | Education | Marital status | Diagnosis | Employment prior to injury | Treatment prior to Rehab |
| Peter (P1) | 28 | Male | Grade 10 | Single | Mild frontal | Security guard | None |
| Matthew (P2) | 34 | Male | Grade 7 | Divorced | Moderate frontal and parietal lobe | Security guard | Hand Treatment |
| Esther (P3) | 33 | Female | Tertiary | Single | Moderate frontal | Jewelry Designer | None |
| Isaiah (P4) | 34 | Male | Grade 11 | Single | Mild frontal and temporal | Petrol attendant | Support group |
| Job (P5) | 30 | Male | Grade 10 | Single | Mild frontal | Hair salon | Support group |
| Joshua (P6) | 28 | Male | Grade 10 | Single | Moderate frontal &parietal | General worker | Hand treatment |
| Ruth (P7) | 33 | Female | Tertiary | Single | Mild frontal &occipital | Bank Teller | None |
| John (P8) | 20 | Male | Grade 12 | Single | Mild parietal | General worker | Support group |
| Luke (P9) | 36 | Male | Grade 10 | Single | Mild frontal &parietal | General worker | Support group |
| Daniel (P10) | 21 | Male | Grade 11 | Single | Mild frontal | General worker | Support group |
Table 2 describes the amount of sessions that each participant took at each stage of the research process. In stage 1 of the model, the average number of sessions was 23.20 sessions per individual. In stage 2 of the model, the average number of sessions was 18.8 sessions per individual. In stage 3 of the model, the average number of sessions was 17.8 sessions per individual. In stage 4 of the model, the average number of sessions was 14.2 sessions perindividual.
Table 2
Depicts the amount of sessions given to each participant in each stage
| Name of participant | No. of sessions in Stage 1 | No. of sessions in Stage 2 | No. of sessions in Stage 3 | No. of sessions in Stage 4 | Outcome |
| Peter | 24 | 16 | 14 | 12 | Successful to R.T.W |
| Matthew | 22 | 16 | 14 | 10 | Unsuccessful to R.T.W |
| Esther | 24 | 24 | 26 | 22 | Unsuccessful |
| Isaiah | 24 | 16 | 14 | 14 | Successful |
| Job | 22 | 14 | 12 | 10 | Successful |
| Ruth | 24 | 22 | 16 | 10 | Successful |
| Joshua | 24 | 24 | 16 | 16 | Successful |
| John | 20 | 18 | 16 | 14 | Successful |
| Luke | 24 | 16 | 24 | 12 | Unsuccessful |
| Daniel | 24 | 22 | 26 | 22 | Successful |
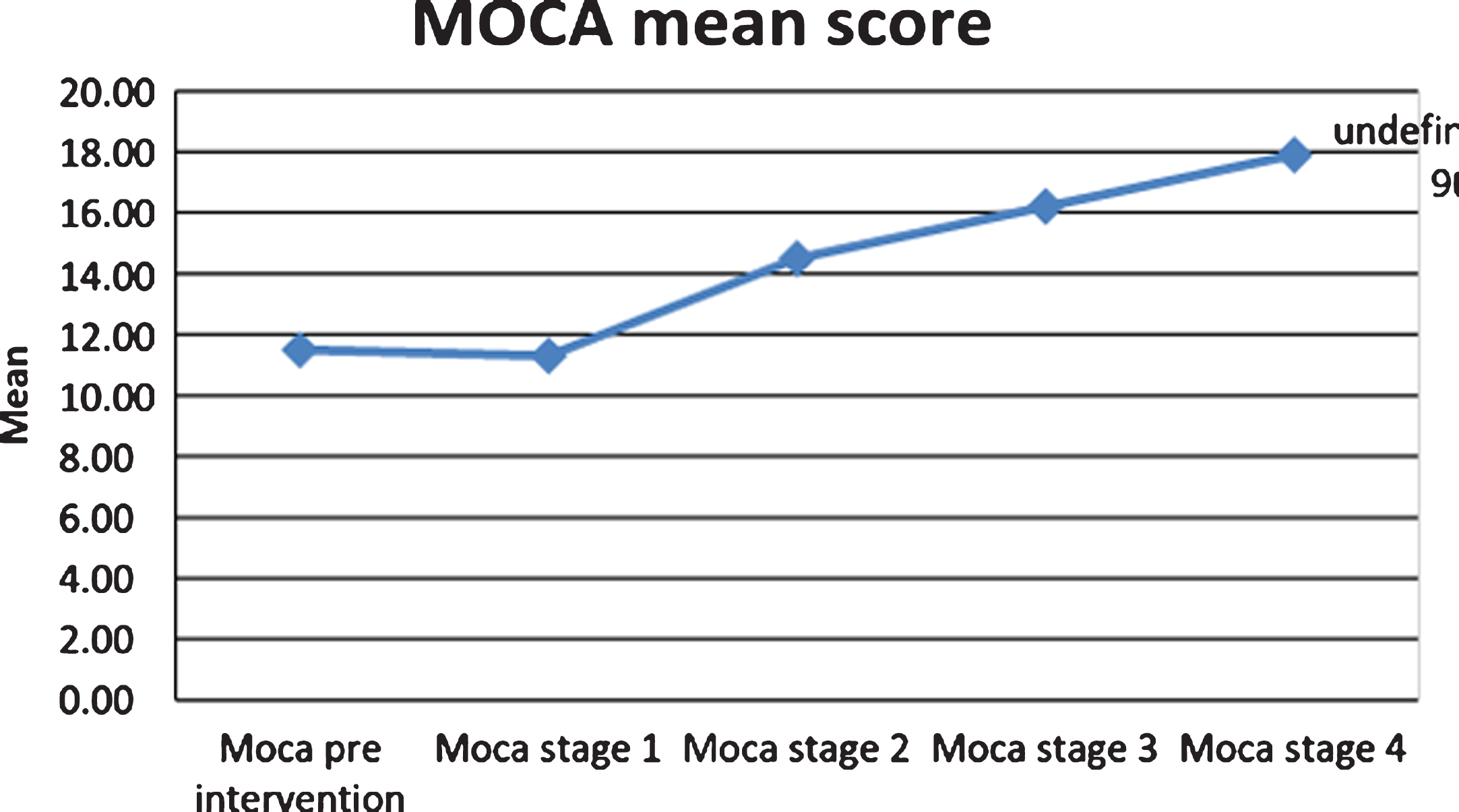
Table 3 describes the total scores of the participants after each stage of the MOOSE. The table also describes the means scores per stage, the table indicates the mean scores improved from the Pre-intervention phase to Stage 4 of the model.
Table 3
Total intervention and mean scores
| Name | Pre Intervention Phase (Total Score) | Stage 1 (Total Score) | Stage 2 (Total Score) | Stage 3 (Total Score) | Stage 4 (Total Score) |
| Peter (P1) | 4 | 11 | 14 | 16 | 19 |
| Matthew (P2) | 8 | 11 | 15 | 16 | 18 |
| Esther (P3) | 4 | 7 | 13 | 13 | 13 |
| Isaiah (P4) | 11 | 12 | 14 | 14 | 21 |
| Job (P5) | 7 | 10 | 14 | 18 | 22 |
| Joshua (P6) | 17 | 11 | 11 | 14 | 17 |
| Ruth (P7) | 18 | 15 | 18 | 18 | 18 |
| John (P8) | 14 | 16 | 19 | 23 | 19 |
| Luke (P9) | 13 | 10 | 13 | 13 | 13 |
| Daniel (P10) | 19 | 10 | 14 | 17 | 19 |
| Pre Intervention Phase | Phase 1 | Phase 2 | Phase 3 | Phase 4 | |
| Stage mean | 11.5 | 11.3 | 14.5 | 16.2 | 17.9 |
As seen in the graph below, there is a gradual increase in the participants’ test scores from stage 1 to stage 4. This indicated that the program may have been successful and that the therapy given was beneficial and purposeful for the participants to regain their worker role.
3.1The results of the repeated measure ANOVA revealed the following:
The results of the participants after participating in the intervention programme revealed a statistically significant effect of the intervention on cognitive functioning measured using the Montreal Cognitive Assessment, F(4, 6) = 15.95, p = 0.002. In the latter result, the multivariate test called the Wilks’ Lambda was used.
Pairwise comparisons revealed a statistical significant result when comparing the results of Stage 1 (
Pairwise comparisons also revealed a non-statistical significant result when comparing the results of Stage 2 with Stage 3 and Stage 4 of the MOOSE, i.e. Stage 3: F(4, 6) = 5.95, p = 0.116 and Stage 4: F(4, 6) = 15.95, p = 0.084
Pairwise comparisons also revealed a non-statistical significant result when comparing the results of Stage 3 with Stage 4 of the MOOSE, i.e. Stage 4: F(4, 6) = 5.95, p = 1.00
When analysing the mean scores from Stage 1 to Stage 4 with a sample of 10 (n) participants, there was a gradual improvement in means scores with Pre intervention = 11.5 and Stage 4 = 17.9. According to the MOCA scoring criteria, 10–17 indicates moderate cognitive impairment, 18–26 indicates mild cognitive impairment, and a score of less than 10 indicates severe impairment [21].
4Discussion
The component areas on the MOCA that were assessed included visual spatial/executive function, naming, attention, language, abstraction, delayed recall and orientation. In the pre intervention there was a considerable limitation in the total scores (in all the component areas above) in particular participant 2, 4, 6 and 8 had a score that was regarded as “very poor” as they obtained scores below 10. According to the scoring criteria of the MOCA, a score of below 10 is indicative of severe impairment [21]. The component areas that the participant’s functioned poorly in were attention, language, abstraction and orientation. The participants in the study performed well in the component areas of visual spatial, naming and delayed recall.
MOCA was administered after the completion of each stage of intervention. After Stage 1 was completed, the participants struggled in the following areas: visual spatial relations, naming, attention, language, abstraction, orientation and identification. The participants performed well in the delayed recall sections of the test. However the results also indicate that participant 6, 7, 9 and 10 had a decline in their total scores when comparing their pre-intervention total score with their total score in Stage 1 of the MOOSE. This is in contrast to other participants who had an improvement in their scores. A possible reason for this could be that these participants who participated in Stage 1 of MOOSE could have experienced deficits in cognitive functioning or struggled with concentration at the time when the test was completed. The latter could have affected their ability to complete the MOCA questionnaire accurately, therefore resulting in a decline in their total scores on the MOCA questionnaire. After Stage 2 was completed the participants struggled in the following areas: visual spatial relations, naming, attention, abstraction and orientation. The participants’ performance improved in the following areas: delayed recall and identification sections of the test. During Stage 1 and 2 of the test there was an indication that the clients were still struggling with visual spatial relations, naming, attention, abstraction and orientation. However, the mean scores on the tests improved from Stage 1 to Stage 2. During Stages 3 and 4 of the test, the mean scores gradually improved. This could be attributed to the fact that the participants were exposed to more tasks in the intervention programme that helped them enhance their cognitive skills. Example, participants were required to do simulated tasks where they had to read and remember instructions in order to do work tasks. Based on a study conducted by Olver, Ponsford and Curran [22], the participants in their study also struggled with attention, language, abstraction, delayed recall and orientation. It could be argued that the nature of a brain injury could affect an individual’s ability to do tasks that require executive functioning. Despite the focus of intervention being mainly on improving the client’s cognitive functions, communication skills and physical endurance, these clients continued to struggle. Although it was difficult to predict an exact period of time when each stage of the model was completed, it was clear that more intervention may be required after the completion of Stage 4 of the intervention. The test results indicate that younger individuals and individuals with a higher education level performed better over the course of the programme. Furthermore, many individuals had good performance in the visual spatial and naming components particularly during Stage 3 and Stage 4 of the intervention programme. One possible explanation for this was the fact that the participants were exposed to activities that were work related such as doing filing, data capturing and performing certain work tasks according to the sequence required to do the tasks (simulated tasks). During Stage 3 of the study, the participants were involved in doing simulated tasks (i.e. practicing the actual work that they wanted to return to or perform in the Open Labour Market). In Stage 4, the participants were placed in a job in the open labour market (work test placement) in order to obtain a real life work experience (i.e. working an 8 hour work shift, working with the tools of the particular job and interacting with work colleagues and customers if required). A study conducted by Law, Polatajko, Baptiste and Townsend [23] indicated that most interventions by occupational therapists utilized functional activities such as activities of daily living (ADL) whereby their approach was either remedial and/or compensatory. In the remedial approach, the occupational therapist would focus on table top activities such as memory games to improve the client’s cognitive function. Whereby compensatory approaches would focus mainly on modifying the client’s environment (e.g. adapting the tools the client uses) or adapting the manner in which the client does a work task (e.g. changing the client’s work routine). The therapists using the MOOSE mainly used the remedial approach during Stages 1 and 2, where the focus was on improving the client’s cognition, communication and physical functioning. Whereby in Stages 3 and 4, the therapists focused on the functional skills in preparation for the placement of the participant in work-related tasks. It was quite interesting to note that of the ten participants who completed the programme, seven participants returned to work.
During the study, it was noticed that activity choices were crucial to the participants’ responsiveness to the treatment given. Activities that were seen as not meaningful or unfamiliar to the participants tended to be paper based. This was mostly due to the participant’s lack of exposure to paper based activities as most of the participants were manual labourers prior to their injury (worked practically with their hands, did not engage in clerical related tasks). Chamberlain, Mosser, Ekholm, O’Connor, Herceg and Ekholm [24] described work to be the most important aspect of the human life span. Work is an important aspect of how people define themselves. The negative consequences of unemployment include depression, impaired social functioning, and various physical ailments. Considering the negative psychosocial and physical health consequences associated with TBI/ABI, which includes loss of self-awareness, depression, and inappropriate social behaviors, people with TBI/ABI may be more deeply impacted by unemployment than the general population [25].
The findings from the current study revealed that most participants were the recipients of disability grants despite the fact that tests revealed that they cognitively and physically did not meet the criteria for a disability grant, yet were receiving this financial assistance due to their impoverished social circumstances. A limitation to the MOOSE was that despite all efforts of going through the model, it did not guarantee a positive outcome (not all of the participants were successfully placed in working environments due to shortage of employment opportunities) which leads to demotivation and a reduction in self-efficacy.
4.1Limitations of the study
One major limitation that was identified in this study was the inability to generalise the findings of this study to the larger population due to the small sample size. Another limitation was the fact that mainly male participants participated in the study. The last limitation related to the fact that the participants may have been familiar with the MOCA questionnaire, despite there being on average a 4 week gap between the repeat of the questionnaires.
5Conclusion
This study revealed that MOOSE was an effective model in returning clients to work in that 70% of the participants returned to work after participating in the return to work programme. Of the 30% that did not return to work, the causes of them not returning to work were mainly related to the shortage of available jobs in their communities and not due to their inability to be productive in the open labour market. The results of the study revealed a statistically significant effect of the intervention (i.e. MOOSE) on cognitive functioning measured using the Montreal Cognitive Assessment, F(4, 6) = 15.95, p = 0.002. The participants in this study could maintain employment in the open labour market for a period of at least 12 months, these individuals were formally followed up. In conclusion, the MOOSE proved to be a useful model in enhancing the clients’ cognitive skills, as well as adapt to their worker roles.
Conflict of interest
The author certifies that there was no conflict of interest during the completion of the research project.
Acknowledgment
The author would like to thank the National Research Fund (South Africa) for funding the project.
References
[1] | Gill M. , Reiley D. , Green S. . Intra-reliability of Glascow coma scale scores in the emergency department. Journal of Emergency Medicine (2004) ;43: (2):215–23. |
[2] | Archiniegas D. , Held K. , Wagner P. . Cognitive impairment following Traumatic brain injury. Current Treatment options. Journal of Neurology (2002) ;4: (1):43–57. |
[3] | KwaZulu-Natal Department of Health. World Head Injury Awareness Day: 20 March Retrieved 23 April (2013) , from http://www.kznhealth.gov.za/headinjury.htm. |
[4] | Raskin S. , Mateer C. . Neuropsychological Management of Mild traumatic Brain Injury England: Oxford University press (2000) . |
[5] | Khan F. , Baguley I.J. , Cameron I.D. . Rehabilitation after traumatic brain injury. Medical Journal of Australia (2003) ;178: :290–5. |
[6] | Gill M. , Reiley D. , Green S. . Intra-reliability of Glascow coma scale scores in the emergency department. Journal of Emergency Medicine (2004) ;43: (2):215–23. |
[7] | Norman R . Estimates of Injury Mortality and disability based on the Cape Metropole study. Technical report. Burden of disease research unit. South African Medical Research Council (2002) 1–75. |
[8] | Bruns J. , Hauser W. . The epidemiology of Traumatic brain injury: A review. Journal of Neurology and Sengievsky Centre (2003) ;44: (10):2–10. |
[9] | Bounds T.A. , Schopp L. , Johnstone B. , Unger C. , Goldman H. . Gender differences in a sample of vocational rehabilitation clients with TBI. Neurorehabilitation (2003) ;18: (3):189–96. |
[10] | Shames J. , Giaquinto S. . Return to work following traumatic brain injury: Trends and challenges. Journal of Disability and Rehabilitation (2007) ;29: (17):1387–95. |
[11] | Tyreman A. . Vocational rehabilitation specific needs and interventions England: Aylesbury Bucks (2006) . |
[12] | Lefebvre H. , Cloutier G. , Josee Levert M. . Perspectives of survivors of traumatic brain injury and their caregivers on long term social integration. Brain Injury (2008) ;22: (7-8):535–43. |
[13] | Moyers P. , Introduction to occupation based practise. In Occupational therapy: Performance, participation & well-being 3rd edition. Christiansen C.H. , Baum C.M. , Bass- Haugen J. , Thorofare New Jersey: Slack incorporated; (2005) . |
[14] | Soeker M.S. . The development of the model of occupational self-efficacy. Work (2012) ;3: (03):313–22. |
[15] | Creswell J.W. . Research Design: Qualitative, Quantitative, and Mixed Methods Approaches Washington: Sage (2014) . |
[16] | Jennette B. , Teasdale G. . Management of head injuries Philadelphia: F.A. Davis Company (1981) . |
[17] | Vuadens P. , Arnold P. , Bellmann A. . Return to work after a traumatic brain injury- Vocational Rehabilitation Paris: Springer; (2006) . |
[18] | Gibbs G. . Learning by doing: A Guide to Teaching and Learning. London: Further Educational Unit; (1998) . |
[19] | Hoops S. , Nazem S. , Siderowf A.D. , Duda J.E. , Xie S.X. , Stern M.B. , Weintraub D. . Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology (2009) ;73: (21):1738–45. |
[20] | Gelb D.J. , Oliver E. , Gilman S. . Diagnostic criteria for Parkinson’s disease. Arch Neurol (1999) ;56: :33–9. |
[21] | Montreal Cognitive Assessment. (2015) –http://www.mocatest.org/wp-content/uploads/2015/tests-instructions/MoCA-Test-English_7_1.pdf. |
[22] | Olver J. , Ponsford J. , Curran C. . A profile of an outcome: 2 years after traumatic brain injury. Brain Injury (1996) ;10: (11):841–8. |
[23] | Law M. , Polatajko H. , Baptiste S. , Townsend E. . Core concepts ofoccupational therapy. In Townsend E. editor. Enabling occupation:An occupational therapy perspective Halifax: CAOT Publications; (1997) . |
[24] | Chamberlain M. , Mosser V. , Ekholm K. , O’Connor R. , Herceg M. , Ekholm J. . Vocational Rehabilitation: Aneducational review. Journal of Rehabilitation Medicine (2009) ;41: (11):856–69. |
[25] | Bombardier C. , Fann J. , Temkin N. , Esselman P. , Barber J. , Dickmen S. . Rates of Major depressive disorder and clinical outcomes following traumatic brain injury. Journal of the American Model Association (2010) ;303: (19):1938–45. |


