
Invisible work of using and monitoring knowledge by parents (end-users) of children with chronic conditions
Abstract
BACKGROUND: Parents who care for young children with chronic conditions are knowledge users. Their efforts, time, and energy to source, consider and monitor information add to the ‘invisible’ work of parents in making decisions about care, school transitions, and interventions. Little is known or understood about the work of parents as knowledge users.
OBJECTIVE: To understand the knowledge use patterns and how these patterns may be monitored in parents caring for their young children with cerebral palsy (CP).
METHODS: An embedded case study methodology was used. In-depth qualitative interviews and visual mapping were employed to collect and analyze data based on the experiences of three mothers of young children with CP.
RESULTS: Knowledge use in parents caring for their young children with CP is multi-factorial, complex and temporal. Findings resulted in a provisional model elaborating on the ways knowledge is used by parents and how it may be monitored.
CONCLUSIONS: The visual mapping of pathways and actions of parents as end users makes the processes of knowledge use more visible and open to be valued as well as appreciated by others. The provisional model has implications for knowledge mobilization as a strategy in childhood rehabilitation and the facilitation of knowledge use in the lives of families with children with chronic health conditions.
1Introduction
In recent years, the uptake of knowledge translation (KT) activities around the world has increased substantially. However, for KT to have its desired effect, it is important to know if people use and monitor knowledge that is disseminated [1]. Monitoring knowledge use is one way of capturing to what extent knowledge has resonated with end users, and whether the efforts to translate the knowledge to users is worthwhile. The knowledge-to-action framework was created to describe the process of KT and what steps are typically taken prior to actually monitoring the value and benefit of information to end-users [2]. For example, knowledge must be selected and tailored, and barriers and facilitators to its use must be addressed to create an effective dissemination strategy [2]. To understand how to enact any step of the knowledge-to-action framework, a specific population’s knowledge use patterns may reveal information to enhance processes from generation of knowledge to how end-users take up information and act on it to improve their lives or decisions. Knowledge translation strategies and end users vary in different settings as they relate to knowledge about health and wellbeing of children. There is a paucity of published information on end users such as teachers or parents.
Knowledge users can include teachers and parents and children in relationship to school health [3]. In rehabilitation and health care knowledge translation involves the entire family and providers especially when parents are caring for children with chronic conditions. For instance, young children with cerebral palsy (CP) rely on their caregivers (parents) to make decisions regarding their daily and intervention management. Parents of children with CP have different and greater demands as a result of their children’s condition than parents of children developing typically or with an acute condition [4, 5]. The uniqueness of a condition such as CP may have implications on how parents of children presenting with CP use knowledge across the life course of parenting [6].
The primary author of this paper conducted a review of the KT literature and noted that there is a gap in the knowledge use patterns of parents of children with chronic conditions. The majority of research focused on how to best produce research-based information incorporating feedback from parents. For example, parents of children with chronic conditions prefer evidence-based information related to their children’s specific condition, matched on age and developmental status, developed by individuals who are familiar with the health condition [7–10]. Examination of parents’ health information sources reveal that parents use a large number and wide variety of sources such as newsletters, conferences, meetings, magazines and television [8, 11]. Parents’ information seeking patterns have been found to change over time and relate to their children’s immediate needs and concerns [8, 12, 13] Lastly, parents gauge the quality of the information that is given to them and desire guidance when seeking health information independently [7, 11, 12, 14]. These studies suggest that parents engage in many activities related to accessing information however how parents actually use health information in caring for their children or in working with health providers or teachers is unknown. Further, there is no research specific to the knowledge use patterns of parents of children with CP. Thus, this study aimed to understand 1) the knowledge use processes of parents of children with CP, 2) how their use patterns could inform the “monitoring knowledge use” step of the knowledge-to-action framework and, 3) to make the invisible work of parents more apparent.
2Methods
2.1Study design and research orientation
An embedded single case study design was used involving three critical cases (parents of young children with CP) to examine in depth how the processes in a well-formulated theory are enacted [13]. In embedded cases, the units of analysis (each parent participant) are analyzed separately and then holistically.
This research was approached from a post-positivist paradigm. An objective relationship between the interviewer and the parents helped to ensure that the parents’ views and perceptions were the parents’ realities and not those of the researchers [16].
2.2Sample
A convenience sample of three parents of young children with CP was recruited from a large regional rehabilitation centre. All of the parents met the inclusion criteria for this study (i.e. parents could read and understand English and had a child with CP under the age of 5). All study participants were mothers, hereafter referred to as parents. The parents’ pseudonyms are Jessica, Monica and Bridget.
Jessica is a married mother of two children: a 5-year-old and a 3-year-old who has CP. Jessica is 29 years old, holds a university degree and works part-time. Her child was diagnosed with CP shortly after birth and is classified by Jessica to be in Gross Motor Function Classification System (GMFCS) level III [17]. Jessica rated her use of research information to be a 3 out of 7, meaning she sometimes uses research information.
Monica is a common-law mother of one child: a 3-year-old who has CP. Monica is 32 years old, holds a college degree and works full-time. Her child was diagnosed with CP shortly after birth and is classified by Monica to be in GMFCS level III. Monica rated her use of research information to be a 1 out of 7, meaning she rarely, if ever, uses research information.
Bridget is a married mother of three children: a 10-year-old, an 8-year-old and a 3-year-old who has CP. Bridget is 38 years old, holds college degree and works full-time. Her child was diagnosed with CP prenatally and is classified by Bridget to be in GMFCS level I. Bridget rated her use of research information to be 5 out of 7, meaning she often uses research information.
2.3Data collection and analysis
Demographic and descriptive data were collected to describe the sample. The primary data collection method for this research was in-depth interviews. The format of the interviews for the parents was semi-structured so that it could be guided, but still allowed for elaboration and direction change by the interviewee. Table 1 outlines the interview guide that was used.
The interviews explored parents’ information sources, information management (including gauging relevance and quality of information), and the outcomes of their information use. The knowledge-to-action framework influenced the questions in the interview guide so that results could be organized within an established theoretical framework. Jessica was interviewed at the university and Monica and Bridget were interviewed at their homes. All interview data were recorded and transcribed verbatim.
A qualitative and iterative process was used to analyze the data. Lincoln and Guba’s naturalistic criteria for determining rigour [18] and Morrow’s paradigmatic transcendent criteria for quality [19] were used to guide the analysis process. Narrative descriptions for each case were created to understand the general characteristics and relations of each unit [20]. To create these narrative descriptions, the primary author first engaged in a manual open coding process for each interview transcript. After these initial codes were made, the primary researcher engaged in axial coding which created more defined themes that described what was being said in the data. Themes were presented and discussed as a group through a series of reflexive meetings, where transcripts were re-visited and re-coded. The end result was a thick, rich description of each parent’s case, agreed upon by each researcher, supported by direct quotes from the parents themselves, and mindful of the unique parental context of each participant, derived from demographic information that was collected at the outset of the research. Visual mapping methods were used as part of the analysis [21].
Two versions of visual maps were used. The first set of visual maps helped organize the information from parents’ interviews describing their knowledge use processes, so that these processes could be visualized. The three sections in the visual maps (sources of information, information management and uses and outcomes of information) were modeled after the components of the interview guide and complement the knowledge-to-action framework. The map items themselves represent the codes that emerged in each narrative description, and the links that exist between themes are made visible. The research team read the narrative description of each parent’s experiences and reviewed the visual maps. These maps were sent back to each parent participant for review before proceeding further with the analysis process. An example of the first level of visual mapping can be seen in Fig. 1.
The second version of the visual maps helped researchers extract themes within and between parents’ narratives and understand the complex relationships of how parents use knowledge. A dialogic review process was used to inform the interpretation of each narrative, theme development, and analysis of the overarching case of all three parents. This involved several meetings among the researchers in which the data and recorded interpretations were discussed and visual maps were revised and refined until consensus was attained on the social processes and approaches to use of knowledge that each parent used. As prescribed by Yin, the researchers made sure these interpretations relied on all relevant evidence and that the most significant issue of the study was addressed [20].
Because the knowledge-to-action framework was instrumental in the study design, the framework was used to organize the analysis of the overarching case. Additional theoretical information from the literature was also sought during the analysis to make sense of the knowledge use patterns of parents to inform the overall case.
3Results
3.1Narratives of parents’ knowledge use: A spectrum
The three parents in this study used knowledge differently from one another. Table 2 summarizes each parent’s narrative on how they use knowledge to care for their young children with CP.
As demonstrated in Table 2, parents’ information sources can vary from very few to a large number. Parents retain these information sources consistently; as they tend to be satisfied by the information they are receiving from them at this point in their children’s lives. Parents who are less involved may not feel compelled to use numerous information sources. Jessica “does not know what [information] is out there so [she] trusts [the therapists] to find it”. However, parents advocating for their children’s care may feel it necessary to obtain as much information as possible, from a variety of sources, on their children’s care. Monica welcomes new information saying that she “can’t get enough! The more I know, the better I feel and the more competent I feel in being able to help her. So I try to absorb everything I can”. Bridget shares similar views to Monica, sharing that “with all three [of my children] it’s the same… just give me information!”
Consistent across all parents was their appreciation of and satisfaction with their health care professionals. Parents like Jessica feel very comfortable having therapists find and tailor their information, and see no need to do it themselves. She has “a lot of confidence in [her] therapists that if there is something out there that [she] should know about, they will tell [her]”. However, parents like Bridget seem to have more self-efficacy to find and tailor their own information, without the aid of a therapist. Bridget likes “going everywhere for [information], printing it off and reading it. And then going ‘oh this applies’ and then highlight it or ‘this doesn’t apply’.” Bridget uses therapists as information sources and as aids in making health care decisions, but not to the extent of Jessica and Monica who rely on their therapists more heavily. In fact, Bridget uses therapists as sources to information that other parents might not have been privy too. She shares “[The speech language pathologist] just went to a seminar about different techniques. She photocopied the entire PowerPoint presentation and gave it to me so I could continue to work with her at home with the different techniques and tongue placement. And [the therapist] knows it’s because I’ve researched the information, and we’ve always done speech therapy.”
Table 2 also demonstrates differences in health information management among Jessica, Monica and Bridget. Jessica does not keep health information that is not perceived to be useful to her. Monica keeps all her information to reference in future, regardless of its current perceived usefulness. As she says, “we hold on to everything, and it’s always useful. There hasn’t been anything where we were like ‘oh, this sucks’ and then throw it aside”. Bridget also keeps all her health information, but uses it to help effectively advocate for her child’s care. Bridget said “if anything happens like surgery or something I have it here [gestures to binder] in [my child’s] binder of information. And all of her reports, like her MRI and everything, I’ll request for a copy to be sent to me so I have it on file. So if we get sent to a new specialist or whatever I’ve got it. And I can revisit it so I can understand what’s going on and what they’re saying.” For parents like Bridget, the more she gets involved in her child’s care and gathers information, the more she wishes to share what she has with others.
None of the three parents particularly seek out information that has been sourced from research. Jessica does not “like going through [research]” because “a lot of it is confusing”. Monica addressed a lack of tailoring as a deterrent against using research, saying “the only problem is that research, when it’s usually conducted, is a big group, and the age range usually varies. So you get mixed results, when I just want to know about [my child]…” Information from therapists that is tailored to their children and can be practically applied is more important to these parents than information sourced from research. The parents seemed to not associate research-based information as applicable or useful to them. When parents get information from their therapists or doctors, they do not question their sources. When asked about the sources of the information Jessica receives from her therapists, she says “I never ask where they found it, I just trust them to give me the right information”.
A spectrum that can be applied to the results of this study is Chiarello’s role of family member’s spectrum [22]. This spectrum attempts to order the extent and type of participation by family members in the care of their children. The spectrum (see Fig. 2) acts as a continuum in which a family may be placed depending on varying factors unique to each family at any time.
Figure 2 describes family involvement in care as Chiarello suggests, but can also be applied to parents’ involvement in the seeking, tailoring and use of health information for their children. Jessica, Monica and Bridget have differing opinions when it comes to their role in information seeking, tailoring and use. In Chiarello’s model above, Jessica can be placed between ‘passive involvement/ information seeking’, Monica between ‘information seeking/partnership’ and Bridget between ‘service co-ordination/advocacy’.
3.2Provisional model of knowledge use
Figure 3 is a provisional model in response to the knowledge-to-action framework that has guided this research. It is also a result of interpreting and explicating the multi-faceted way in which parents use health information. The visual mapping helped to illuminate and make apparent the investment of time and the multitude of steps and pathways that are needed to understand, interpret and decide to use or not use information.
One of the major themes of this research is that the knowledge use patterns of parents of young children with CP is temporal. That is, to effectively and accurately understand how to monitor knowledge use in these parents, it must be understood that knowledge use will be connected to whatever point that parent is in his or her life (or the child’s life). This temporality is represented by an arrow denoting the time in Fig. 3, and why the cycle describing knowledge use is not contained, but rather evolves over time. Each ‘spiral’ on Fig. 3 indicates a separate knowledge-use cycle. The initial knowledge use cycle was filled in knowing how Jessica, Monica and Bridget currently use health information at this point in their lives. Phases in a potential ‘next cycle’ have been included, however we are not able to comment on what these phases might be as they could change at that later point. The cycle represents a complete transition through the health information, from first encountering it to eventually using it (or not using it).
The initial cycle in Fig. 3 begins with a ‘trigger point’ phase. This represents a point in time characterized by an event or occurrence in the parent’s life that causes them to use health information. Such an event may be planning for a major transition such as preparing for kindergarten, needing information to provide to a health care provider or to fill out a form, or wanting information on a general aspect of CP to understand the condition better.
The phases in Fig. 3 after the trigger point occur in a particular order for these parents, but may be repeated or skipped as well, depending on their personal context and the particular trigger that has made them enter the cycle. The first step is to acquire information. Next, parents have to understand the information they are receiving or they will not be able to progress further. The third step is to gauge the relevance of the information to their child’s current condition, their family context, and their child’s personal developmental trajectory. The fourth step is to gauge the quality of the information, including whether it is too negative or goes against their personal beliefs and values. The fifth step is to decide what to do with this information. There are three options mentioned by Jessica, Monica and Bridget. These are to discard the information due to its inability to be used right away, to keep it for later use or reference, or to immediately apply and use. These initial five steps in this cycle will either happen independently (for parents such as Bridget), with the aid of a therapist (for parents like Monica) or mostly done by the therapists themselves (for parents like Jessica).
The ‘outcome’ phase is what occurs as a result from the decision of their previous phase. If it is to use the information, then the outcome is a treatment or management decision that parents have made as a result of the information (instrumental use), or the change in understanding as a result of the information (conceptual use). This could also include the strategic use of knowledge, if that was the initial goal. If parents choose to not immediately use the information, but catalogue it for later, this includes the placement of such tangible information into a binder. If the parent decides not to use or keep the information, then the information is discarded and the parent may go back to the first phase to find other information instead. The subsequent phase, sharing outcomes, indicates that parents will discuss their decision or the result of their decision with therapists, their family or other individuals invested in their children’s care. After this phase, a new cycle may begin, or parents may remain on the straight path before a cycle for a longer period of time (or until they are presented with another trigger point).
The stars in Fig. 3 indicate places in the cycle where knowledge use could be monitored. Unlike the knowledge-to-action framework which only indicates this after information has progressed through the initial phases of the cycle can it be effectively monitored, Fig. 3 indicates that monitoring can occur at multiple stages. The primary difference is that classification of monitoring knowledge use is more than just a quantitative technique to see if knowledge was ultimately used or not. In contrast, knowledge ‘use’ appears to be a process, not an outcome.
Depending on where one monitors knowledge use, different results will emerge. For example, monitoring knowledge use when parents are gauging the quality of information will look different than monitoring knowledge use when parents are sharing the results of their information use or lack of use. Not only will monitoring knowledge use be different depending on where the parent is in their cycle, it will be different depending on who the parent is in the cycle and what their context and background is. With these two conditions in mind, it becomes clear how complex monitoring knowledge use is, especially among parents of children with complex and wide-spectrum of involvement health conditions (such as CP) who change over time as they grow and develop. Therefore, the entire cycle displayed in Fig. 3 is considered to be ‘the use of knowledge’ in that it is not restricted to one phase of a cycle.
4Discussion
The major finding of this study is that knowledge use in parents living with and caring for their young children with CP is multi-factorial, complex and temporal. Parents’ health information sources, management and outcomes differ across a wide spectrum depending on the parent, family, and child. This finding supports the role of family members’ spectrum which describes family involvement in care, while adding a unique lens to the spectrum regarding parents’ information use [22].
One consistent observation among all parents in this study is that therapists are instrumental in their use of health information. Some parents prefer to use their therapists as knowledge mediators over an individual who is not involved in the care of their child. Furthermore, some parents adopt the knowledge mediator role themselves for both their children and others with a similar condition. This has implications for how therapists deliver health information to parents who exist on various points on the knowledge use spectrum. Furthermore, these findings may have implications for the training and support that therapists should receive in acting as the primary knowledge mediators. In all knowledge mediating endeavours, research-based information is not necessarily preferred by parents over other sources, primarily due to the perceived lack of tailored results to individual children and families. This gap could be addressed if therapists tailored the research-based information they have to a child’s or family’s current state.
A limitation of this research is that the provisional model could be more well-rounded and representative if it was based on the experiences of more parents. Recruiting more parents might yield a wider spectrum of results, potentially leading to broader implications for practice and research. However, a wide spectrum of knowledge use was uncovered in this research study by solely focusing on the three parent participants. This study also highlighted the complexity of knowledge use and revealed the breadth of actions, tasks, reflection and demands of being a knowledge user as a parent that may not be detected in a larger study.
This research adds to the knowledge use patterns of parents of children with a chronic health condition. By acknowledging that knowledge use by parents is complex, service providers, researchers and KT professionals may become more aware of and consider multiple and individual factors in each family that might support parents as optimal end-users. The provisional model is a description of what knowledge use looks like among the end-users and tapped into the ways that parents were engaged in monitoring knowledge use in the context of parents of young children with CP. Graham and Tetroe state that ‘the [knowledge-to-action] framework does not prescribe specifically what needs to be done at each phase in the process, nor populate each phase with theory that might direct action at each phase’ [23]. More attention is needed on understanding how to monitor knowledge use more broadly in this population, to further support parents’ tireless work and efforts to effectively parent and manage the chronic health conditions of their children.
Conflict of interest
None to declare.
References
[1] | Straus SE , Tetroe J , Graham ID . Defining knowledge translation. Can Med Assoc J (2009) ;181: (3-4):165–8. |
[2] | Graham ID , Logan J , Harrison MB , Straus SE , Tetroe J , Caswell W , Robinson N . Lost in knowledge translation: Time for a map? J Contin Educ Health (2006) ;26: (1):13–24. |
[3] | Miles-To F , Shaw L . Knowledge transfer with children and adolescents in promoting comfort, health and safety in technology use: Strategies and opportunities. Work (2012) ;43: (3):387–97. |
[4] | Morris C . Definition and classification of cerebral palsy: A historical perspective. Dev Med Child Neurol Suppl (2007) ;49: (109):3–7. |
[5] | Newton M . Family-centered care: Current realities in parent participation. J Pediatr Nurs (2000) ;26: (2):164–8. |
[6] | Johnston CE , Marder LR . Parenting the child with a chronic condition: An emotional experience. J Pediatr Nurs (1994) ;20: (6):611–4. |
[7] | Jackson R , Baird W , Davis-Reynolds L , Smith C , Blackburn S , Allsebrook J . Qualitative analysis of parents’ information needs and psychosocial experiences when supporting children with health care needs. Health Info Libr J (2008) ;25: (1):31–7. |
[8] | Huber JT , Dietrich JD , Cugini E , Burke S . F2F connection: A community health information needs assessment of Texas families who have children with chronic illnesses and/or disabilities and their care providers. J Med Libr Assoc (2005) ;93: (2):278–81. |
[9] | Mitchell W , Sloper P . Information that informs rather than alienates families with disabled children: Developing a model of good practice. Health Soc Care Comm (2002) ;10: (2):74–81. |
[10] | Fisher HR . The needs of parents with chronically sick children: A literature review. J Adv Nurs (2001) ;36: (4):600–7. |
[11] | Khoo K , Bolt P , Babl FE , Jury S , Goldman RD . Health information seeking by parents in the internet age. J Pediatr Child Health (2008) ;44: (7-8):419–23. |
[12] | Mulligan J , Steel L , Macculloch R , Nicholas D . Evaluation of an information resource for parents of children with autism spectrum disorder. Autism (2010) ;14: (2):113–26. |
[13] | Osborne LA , Reed P . Parents’ perceptions of communication with professionals during the diagnosis of autism. Autism (2008) ;12: (13):309–24. |
[14] | Bernhardt JM , Felter EM . Online pediatric information seeking among mothers of young children: Results from a qualitative study using focus groups. J Med Internet Res (2004) ;6: (1):e7. |
[15] | Yin RK . Case study research: Design and methods. 3rd ed. Thousand Oaks, CA: Sage Publications; (2003) . |
[16] | Straus A , Corbin J . Basics of qualitative research techniques and procedures for developing grounded theory. London, UK: Sage Publications; (1998) . |
[17] | Palisano RJ , Rosenbaum PL , Walter S , Russel D , Wood E , Galuppi B . Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neuro (1997) ;39: (4):214–33. |
[18] | Lincoln YS , Guba EG . Naturalistic inquiry. Thousand Oaks, CA: Sage Publications; (1985) . |
[19] | Morrow SL . Quality and trustworthiness in qualitative research in counseling psychology. J Couns Psycol (2005) ;52: (2):250–60. |
[20] | Yin RK . Case study research: Design and methods. 2nd ed. London, UK: Sage Publications; (1994) . |
[21] | Charmaz K . Grounded theory: Objectivist and constructivist methods. Strategies of qualitative inquiry. Thousand Oaks, CA: Sage Publications; (2003) . |
[22] | Chiarello LA . Serving infants, toddlers, and their families: Early intervention services under IDEA. In: Campbell SK , Palisano RJ , Orlin MN , editors. Physical Therapy for Children. St. Louis: Elsevier Saunder; (2012) . pp 944–67. |
[23] | Graham ID , Tetroe J . Chapter 10: The knowledge to action framework. In: Rycroft-Malone J , Bucknall T , editors. Models and frameworks for implementing evidence-based practice: Linking evidence to action. Wiley-Blackwell. (2010) . pp 207–21. |
Figures and Tables
Fig.1
Example of visual mapping technique.
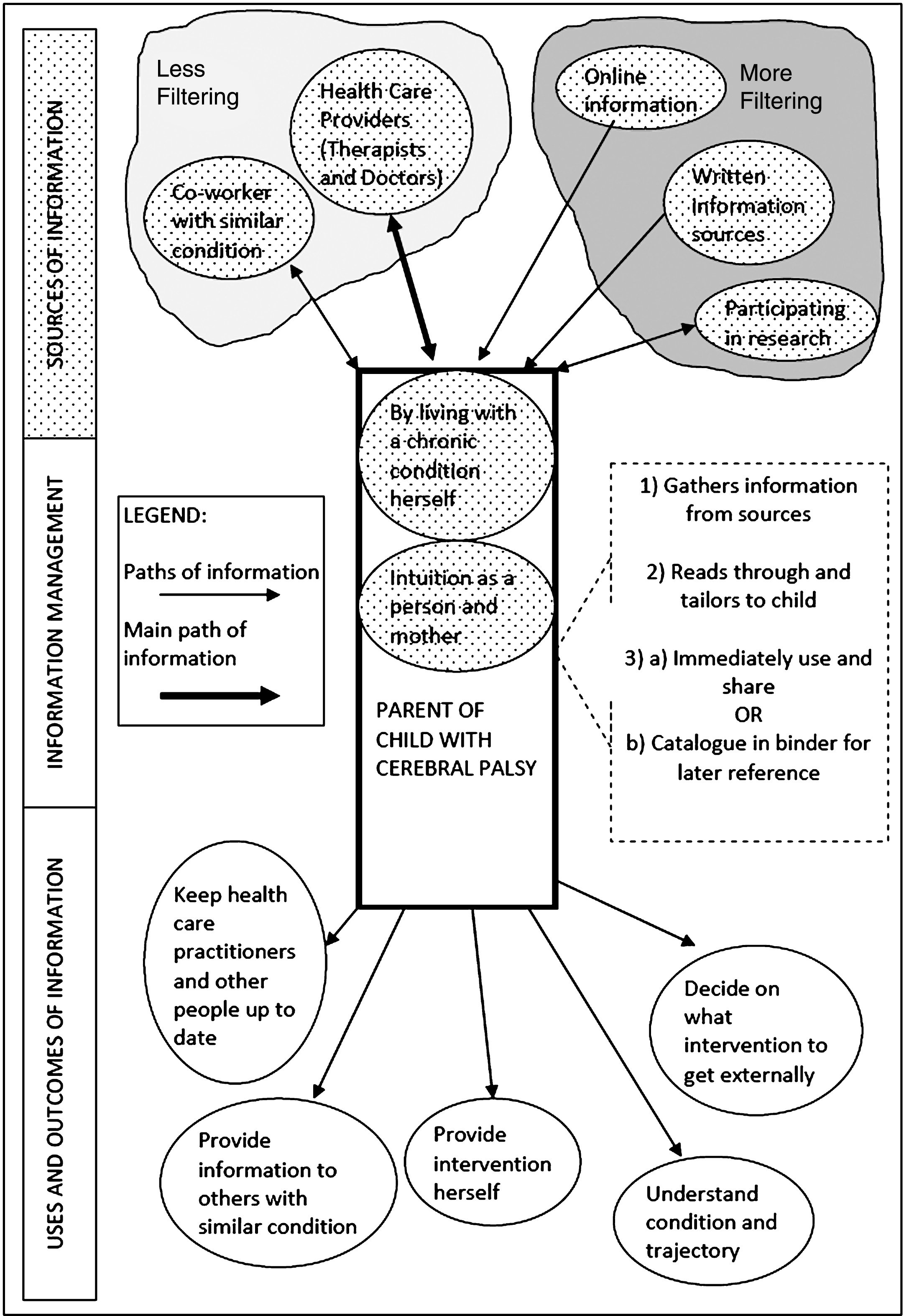
Fig.2
Chiarello’s role of family members spectrum demonstrates the extent and type of participation by family members in the care of their children.
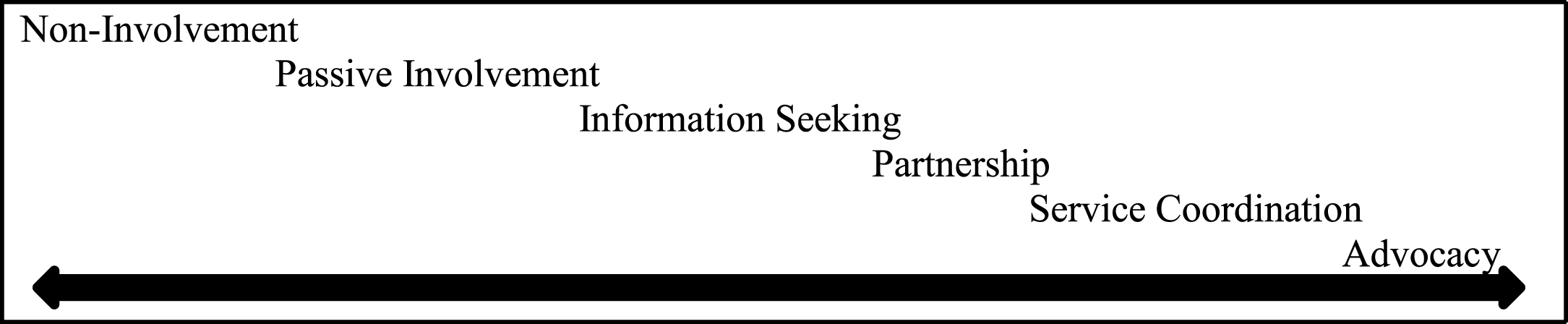
Fig.3
A provisional model for conceptualizing the monitoring of knowledge use in parents with young children with cerebral palsy.
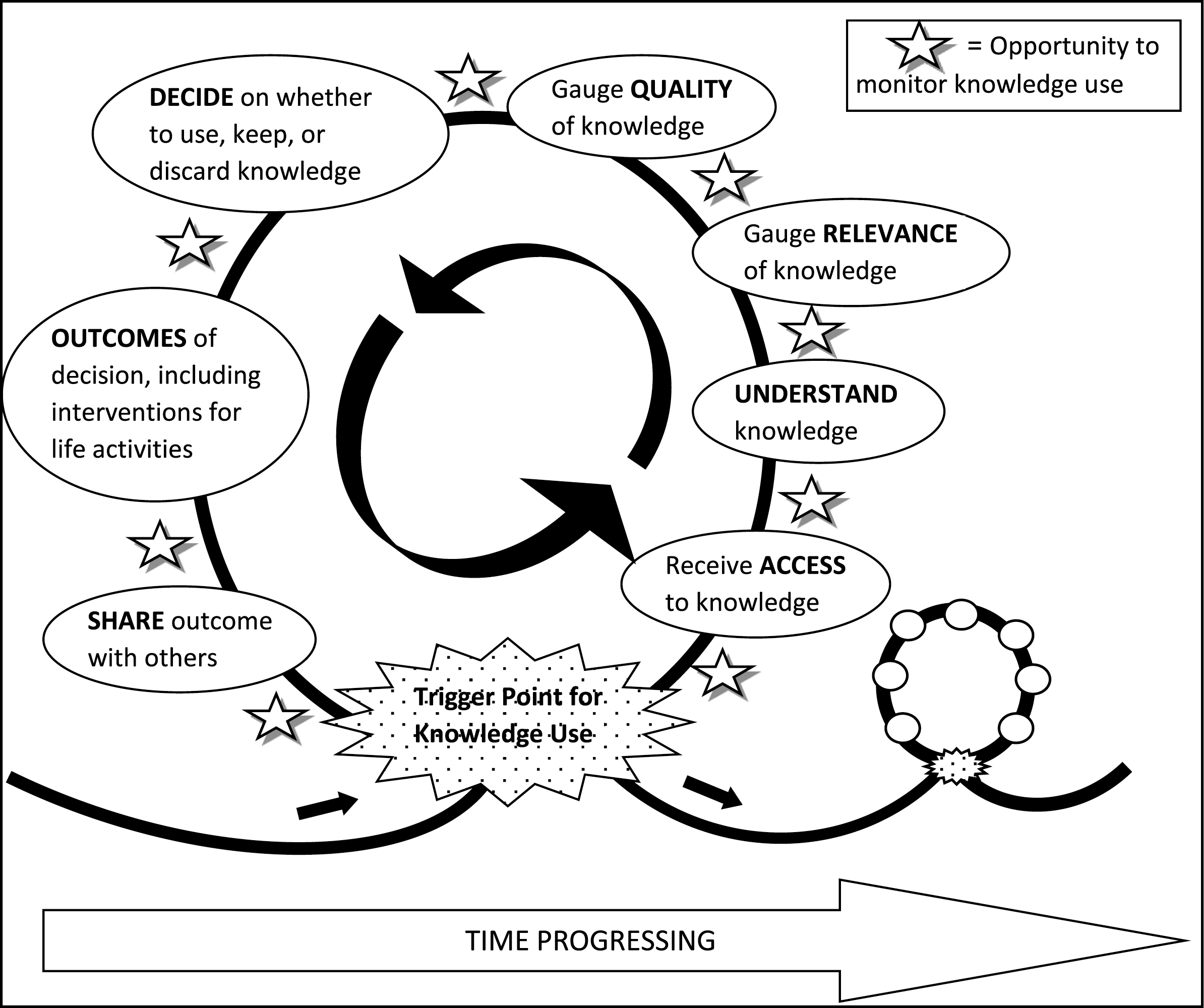
Table 1
Interview guide
| Preamble | Over the past one to two months, you have had access to both a series of research summaries and a knowledge broker to help you find and use health information. I am interested in knowing a bit about how you used information before this whole research experience. |
| Question 1 | What information did you use before this experience? How did you become aware of this information? What were the things that made it easy or difficult for you to use information prior to this experience? [Prompt: what information did you value, where did you access the information, what kind (oral or written) etc.] |
| Preamble | Now I would like you to help me understand how you currently use health information (specifically). In particular, I would like to understand how you use health information in regards to your child. |
| Question 2 | Think of a situation where you had to make a decision that would change the direction of care you provided at home, at school, or within the social life of your child. What health information was helpful to you in making a decision or considering options about the direction of care? [Prompt: Did this information change how you interacted with your child? What was the nature of this health information re: written brochure, article, information on web, shared from another source? How (if at all) did the health information combine with other sources of information to help you make a new direction in how you cared for your child/client at home at school or in the community or in the health care or rehabilitation system?] |
| DEPENDING ON ABOVE ANSWER (SATISFIED OR UNSATISFIED), ASK THE OPPOSITE: | a. Can you tell me about an example of a certain experience that helped you choose or make a decision you were satisfied with? b. Can you tell me about a situation where information you used did not lead to the outcome you wanted in the care of your child? [Prompt: What was it that happened or led to you needing the information, who was involved and why you felt that the information did not help you achieve the outcome you were looking for? What would you do differently in considering the way you used information in this later situation?] |
| Question 3 | Can you give me an example of a situation where you were unsure or uncomfortable with the health information you were considering, that was a situation where you did not necessarily believe the information would be helpful? What did you do along the way to sort out how to use it, and what steps (if at all) did you actually take to use the information? |
| Question 4 | How (if at all) does the way that others use health information influence the way you think about or use information in caring for your child? [Prompt: Can you give me an example of situation where you considered how others viewed information? Does anyone else involved in your child’s care (i.e. family, friends OR other health service providers) use health information? In what ways does this influence the way you made decisions about your child’s care?] |
| Question 5 | How do you decide what information is relevant to use when you need to make a challenging decision about the care of your child? How (if at all) do you use this information in context with what you already know? What if anything helps you sort out what information you use and what information you do not use? Can you give an example? [Prompt: do you discuss it with others, or think about it for a period of time, what do you consider valuable about the information you use]? |
| Question 6 | Can you give me an example of a situation where you have become more confident in making plans and making a decision about using information over time, to point that you do not think about it, you just know? |
| Question 7 | Given that in some instances a change in one thing may affect others, how do you go about sorting out what to do and how go about making changes in the care of your child? What do you do? How are decisions made? |
| Question 8 | In this study, we provided access to a KB, but I understand that you did not interact with this person. |
| a. Is there anything that we could have done to facilitate this interaction? | |
| b. What else could we have provided that would have been of use to you in accessing and understanding information? | |
| Question 9 | How if at all do you feel your approach to make decisions and considering health information has changed due to this experience? |
| a. In what way do you feel that using research materials, such as those materials from the Move and Play study, impacted the way you view various rehabilitation and health options? [Prompt: What is it about these materials that have helped you consider options? How do you use these materials to add to or compliment other things that you know?] | |
| b. In what way do you think your usage of research materials will increase or stay the same? | |
| c. In what way do you think your approach to sharing information with your health service provider has changed? [Prompt: For instance if you found new information from a different source such as the internet or a friend would you bring it forward?] | |
| d. In what way do you think the health information you have learned will have other benefits in the daily care of your child (i.e. just increase of knowledge)? | |
| Question 10 | Knowing that new parents will face new information and may struggle with how to use it, what advice would you give them about how to consider and think about health information before they make plans to use it? |
| Question 11 | Knowing that you were going to do this interview today, was there anything you were thinking of discussing regarding the use of information that we haven’t talked about yet? |
| Wrap Up | Thank you for sharing your experiences with us. |
Table 2
Spectrum of parents’ knowledge use
| Jessica | Monica | Bridget | ||
| Sources of health | •health care providers | •health care providers | •health care providers | |
| information | •family members | •family members | •family members | |
| •the internet | •the internet | •others with similar condition | ||
| •conferences and workshops | •participating in research | |||
| •written and online information | ||||
| Information searching and tailoring | Therapists find and tailor information to parents’ needs | Therapists mostly find and tailor information to parents’ needs, but parent also attempts this alone | Parent finds and tailors information to her own needs, with occasional help from therapists | |
| Managing health information | Does not keep or catalogue health information | Keeps all health information to personally reference at a later date | Keeps all health information to reference at a later date and to inform others | |
| Use of research-based information | Dislikes research-based information | Skeptical of research-based information | Impartial to research-based information |

