
The effectiveness of a 6-month intervention with sit-stand workstation in office workers: Results from the SUFHA cluster randomized controlled trial
Abstract
BACKGROUND:
Prolonged periods of sitting have been linked to negative health outcomes. Implementation of sit-stand desks in the workplace has been one strategy to reduce prolonged sitting.
OBJECTIVE:
To assess the effectiveness of sit-stand workstations on reducing sitting time and improving other health outcomes of office-based workers.
METHODS:
39 Portuguese office workers were randomized into a 6-month parallel-group cluster RCT consisting by the implementation of sit-stand desks in the workplace. The primary outcome of sitting time was assessed using ActivPAL. Secondary outcomes included biometric, psychological, and diet-related variables. All outcomes were assessed at baseline and 6 months for the whole sample and at 3 months for a sub-sample of the intervention group (n = 11).
RESULTS:
No significant time*group interaction was found for the primary or secondary outcomes, apart from waist circumference favoring the control group (Δ–1.81 cm, pinteraction = 0.04). There were significant changes within the intervention group for sitting time (–44.0 min/day), prolonged sitting (>30 min) (–45.3 min/day) and standing time (51.7 min/day) at 3 months in the sub-sample and in prolonged sitting (>30 min) (–26 min/day) in the full intervention group (p < 0.05). Changes were also observed within the intervention group for percent body fat (Δ–3.7%) and ratings of quality of life (Δ2.2), musculoskeletal discomfort (Δ–4.9), overall fatigue (Δ–2.2), and the need for recovery after work (Δ–1.7) at 6-month follow-up (p < 0.05).
CONCLUSION:
Although not being effective for reducing sitting time, the implementation of sit-stand desks in the Portuguese workspace was shown to be feasible over the long term, received well by users, and may offer other health benefits.
TRIAL REGISTRATION:
OSF Registration, OSF.IO/JHGPW. Registered 15 November 2022. https://doi.org/10.17605/OSF.IO/JHGPW.
1Introduction
Despite the recognized health benefits associated with attaining physical activity (PA) recommendations, most of the population is still inactive [1, 2]. In addition to being inactive, it is estimated that adults spend approximately 50–60% of their waking day sedentary in a sitting, reclining, or lying position [3]. This is of concern given that high sedentary behavior (SB) is associated with increased risk of cardiovascular disease (CVD) [4, 5], diabetes [6, 7], cancer [8], cognitive decline [9, 10], overall lower quality of life [11] and all-cause mortality [4], with these deleterious effects of too much SB being not just limited to high-income countries, but also a reality in middle and low-income countries [4]. In opposition, breaking up SB more often seems to protect against the harm of prolonged SB [12].
Desk-based office work is responsible for most of the SB accumulated during the day for many job occupations and, thus a strategic setting for interventions to reduce prolonged SB [13, 14]. Higher SB in the office has been related to lower job satisfaction and greater fatigue, and previous findings suggest that less SB was associated with positive health outcomes that do not seem to come at the expense of productivity [15].
A height adjustable sit-stand desk is a device that allows the worker to easily shift from a sitting to a standing posture and vice-versa (i.e., break in SB), without the need to interrupt working tasks. In the last decade, several sit-stand desk-based interventions have been performed around the world showing modest to large reductions in workers’ sitting time (i.e., –22.2 to –128.4 minutes/day) [16–34], but most of these studies were performed in English-speaking countries (i.e., 14 out of 23) [16–34]. In Europe, there is a lack of interventions using sit-stand desks, with only one performed in Finland [35], one in Austria [36], and one in Switzerland [37]. Thus, there is a clear need for more evidence on the implementation, acceptance, and effectiveness of these approaches in the work environment across countries with different cultural backgrounds and work habits.
In Portugal, recent representative accelerometer-based data suggest that, despite all efforts, PA has remained fairly stable in the last years [38], with SB still representing around 60% of a person average waking day [3, 38]. To the authors best knowledge, no sit-stand desk-based intervention has been performed in this country or any other Portuguese-speaking country. Thus, we aim to present the effectiveness of a 6-month intervention to reduce sitting time in office-based workers using a sit-stand workstation prompted by an initial educational session and ongoing motivational prompts.
2Methods
2.1Study design
This study was a two arm (1 : 1), superiority parallel-group cluster randomized controlled trial, with measurements at baseline and 6 months follow-up. The trial was prospectively registered (details at: https://doi.org/10.17605/OSF.IO/JHGPW; Registered 15 November 2022. OSF Preregistration) and has been previously described [39]. After baseline measurements, cluster randomization was performed by a researcher not involved in recruitment or data collection using a list randomizer (www.random.org). The randomization considered that control and intervention groups were matched for daily sitting time, the number of transitions from sit to stand, BMI, and age. To reduce the risk of contamination, participants who observed each other from their workstations were constituted as a cluster and were randomized as such.
2.2Setting and participants
Inclusion criteria for the intervention consisted of the suitability to install the sit-stand desk; working at least 0.6 full-time; being more than 20 years-old; and spending at least 70% of a working week performing desk-related activities. Exclusion criteria consisted of workers already using a sit-stand desk; workers without a personal workspace where a sit-stand desk could be assembled; or workers with musculoskeletal disorders/health conditions inhibiting their ability to work in a standing position. Recruitment took place between December 2022 and January 2023 via university advertisements (e.g., banners, posters, invitation institutional emails, and face-to-face word of mouth), with baseline data collection in February 2023 and follow-up data collection in August 2023. All participants provided written informed consent and the project was approved by the ethics commission of the Faculty of Physical Education and Sport at the University of Lusófona in Lisbon (Approval number D0522).
2.3Intervention group
The intervention group received a sit-stand desk (Vinsetto, Model 923-043), which was installed on top of a conventional workplace desk by means of a clamping arm. To enhance desk use, an initial psychoeducational session regarding the independent benefits of reducing and interrupting sitting time with standing was given. Participants were also given the following verbally and in written form: (i) a demonstration of how their sit-stand desk works; (ii) tailored information on the correct ergonomic posture to use; (iii) and individualized guidance on gradually building up standing time. Moreover, motivational nudges were delivered via email and on the SUFHA’s website (https://sufha.ulusofona.pt) during the intervention period to support relatedness, perceived competence, and autonomy to use the desk. These nudges varied from 4 times in the first month, to 2 times in the second and third months, and monthly until the end of the intervention.
2.4Control group
We included a waiting-list control group who only attended the initial psychoeducational session regarding the independent benefits of reducing and interrupting sitting time with standing, with no contextual change during the 6-month intervention (i.e., no access to the sit/stand desk or any other prompt). After the intervention period, the waiting-list control group had access to the sit-stand desks.
2.5Outcome measures
Primary and secondary outcomes were assessed at baseline and at the end of the 6-month intervention period. The primary outcomes were also assessed at 3 months in a subsample of the intervention group.
2.5.1Primary outcomes
Sedentary and PA pattern data was collected using an ActivPAL inclinometer/accelerometer monitor (model ActivPAL4; PAL Technologies Ltd., Glasgow, UK), while using the CREA (v1.3) classification algorithm that distinguishes between non-wear time, lying, sitting, standing, cycling, seated during transport, and stepping time. Changes in the following outcomes were considered from the device in the current study: 1) sitting min/day; number of sit-to-upright transitions per day; prolonged (i.e., bouts of ≥30 min and bouts > 60 min) sitting per day; sitting while commuting min/d; lying while awake (i.e., secondary lying) min/d; lying while sleeping (i.e., primary lying) min/day; cycling min/day; standing min/day; stepping min/day; and number of steps per day.
Participants wore the device on their right thigh 24 h/day for 7 days at baseline, repeating this assessment at the end of the intervention (6 month), and on the third month of intervention (i.e., a subsample of the intervention group).
2.5.2Secondary outcomes
Body composition
Participants were weighed to the nearest 0.01 kg while wearing minimal clothes and without shoes, on an electronic scale (TANITA BC-601 scale). Height was measured to the nearest 0.1 cm with a stadiometer (Seca, Hamburg, Germany). BMI was calculated as body mass (kg)/height2 (m). Waist circumference was measured over the naked skin to the nearest 0.1 cm with the participants in a standing position. according to the World Health Organization criteria [40]. The mean of two measurements was considered. If the two measurements differed by more than 1 cm, a third measurement was performed, and the two closest measurements were averaged.
A phase-sensitive single-frequency bioimpedance analyzer (BIA) (101 Anniversary, Akern, Florence, Italy) was used to assess percent fat mass and fat free mass. The BIA analysis was performed with the participant in a fasting condition (at least 8 hours) and following the participant lying in a supine position for a minimum of 5 min, with arms and legs abducted, and all metallic accessories removed from the body. Four electrodes were placed on the right side of the participant’s body in the standardized points (two on the right hand and two on the right foot) [40]. Previously validated equations were used to estimate body fat-free mass from the BIA raw parameters [41]. Body fat mass was calculated by subtracting fat-free mass from total body mass.
Overall fatigue and musculoskeletal discomfort
Overall level of fatigue was calculated based on the sum of the answers to 8 items from the Portuguese version of the Fatigue Scale [42], which were answered on a Likert point scale ranging from 0 (“nothing”) to 4 (“extremely”). A higher score indicated more overall fatigue.
An adapted version of the Nordic Musculoskeletal Questionnaire was used to assess musculoskeletal discomfort encompassing 9 regions of the body (neck, shoulders, elbows, hands/wrists, thoracic region, lumbar region, hips/thighs, knees, and ankles/feet). A higher score indicated more overall musculoskeletal discomfort.
Work engagement and quality of life
A shorter version of the original Ultretch Work Engagement Scale (UWES-9), was used to assess work related well-being. The scale has 9 items, which were evaluated using a 7-point Likert scale ranging from 0 (“never”) to 6 (“everyday”) [43]. A total score was created by summing the answers to the 9 items, with a higher total score indicating more work engagement.
Quality of life (QoL) was assessed by EUROHIS-QOL-8 [44], which is a measure of QoL composed of 8 questions revolving around physical, psychological, social relations and environment domains that are answered on a 5-point Likert scale. The sum of the 8 responses was calculated and ranged from 0 to 32, with a higher value corresponding to a better perception of QoL.
Work difficulties and recovery from work
Work difficulties was based on the total score obtained from the sum of 8 statements from the Work Limitations Questionnaire (WLQ-8) [45] that asked the participant to indicate the percentage of output lost per hour due to health problems interfering with their performance of job tasks in the last 2 weeks.
The Need for Recovery Scale (NFR) [46] was used to assess the need to recuperate from work induced efforts. The questionnaire presents 11 items with dichotomic answers 0 (“no”) and 1 (“yes”). A higher total NFR score indicated that the worker was needing greater recovery time from their work tasks.
Eating related habits/behaviors
Eating-related habits/behaviors were assessed based on an 11-item questionnaire [47], where the participant reported their weekly consumption of 9 food groups based on the Mediterranean diet (non-refined cereals, fruits, vegetables, legumes, potatoes, fish, meat and meat products, poultry, and full fat dairy products including cheese, plus olive oil use in cooking and alcoholic beverages intake) using a scale of 0 to 5 (never, rare, frequent, very frequent, weekly, and daily consumption). A composite score summing all the responses was calculated and used in the analysis.
Participants’ barriers and facilitators to the intervention
A qualitative understanding of participant experiences with the intervention as well as barriers and facilitators was obtained from focus groups, open-ended questionnaires, and monthly email feedback. More details can be found in our previous publication [39].
Demographic data
Information on age, sex, country of birth, education, financial status, occupation, and tasks assignment/duties, working hours and years of work, current smoking status, presence of chronic disease, and total use of medication and eventual changes in medications were self-reported through an online questionnaire.
2.6Statistical analysis
2.6.1Sample size
For cluster size and number calculation, we assumed that participants within the same workplace (cluster) would be independent, and therefore, an intra-cluster correlation of 0.01 was used. Considering the main outcome of the present intervention (i.e., sitting time) and using an effect size of 0.80, the total number of participants for time*group interaction analyses (control and intervention groups) with a power of 0.80 and a significance level of 0.05 (two-tailed test) would be 34 participants. Assuming a 20% drop-out, we conservatively recruited a total sample size of 40 participants (i.e., 20 controls and 20 in the intervention group).
2.6.2Data analysis
Statistical analyses were performed using PASW Statistics for Windows version 28.0 (SPSS Inc., an IBM Company, Chicago IL, USA) and statistical significance was set at p < 0.05.
Differences between groups at baseline were examined using independent sample t-tests and differences between the baseline and 3-month follow-up within the subsample were examined using paired-sample t-tests or the non-parametric Mann-Whitney U-test and the Wilcoxon signed-rank test, respectively, for non-normally distributed variables. To evaluate the effects of the intervention on primary and secondary outcomes adjusted for age, sex, clustering, and BMI, repeated measures ANCOVA was used, where time (baseline, 6-month follow-up) was the within-subjects factor and intervention group was the between-subjects factor.
3Results
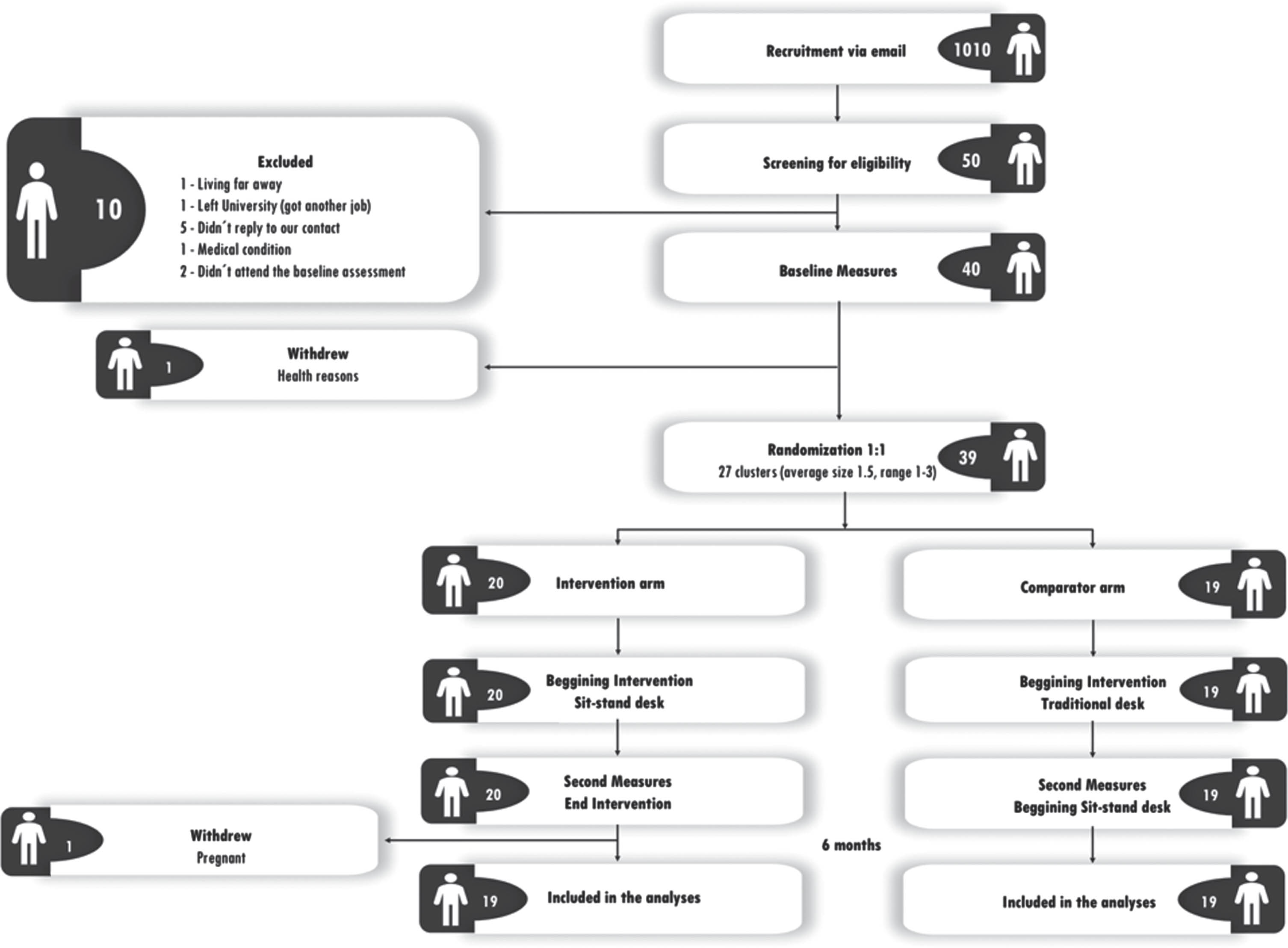
Figure 1 displays the flow of participants through the study. Between December 2022 and January 2023, 40 participants were recruited and assessed at baseline. But due to health problems one participant withdrew from the study, thus we randomized 27 office clusters, with 15 office clusters (20 participants) randomized to the intervention arm and 12 clusters (19 participants) to the control arm. After randomization, no participants withdrew from the study. However, of these 39 participants that completed the study, one participant from the intervention group was not included in the analyses due to pregnancy during the intervention period, so 38 participants (19 in each group) were considered in the final analyses. The primary outcomes were additionally assessed at 3 months (midway of the intervention) in a subsample of the intervention group (11 participants; 55% of the intervention group). There were no baseline differences found for any of the primary outcomes between this subsample and the remaining participants from the intervention group (p > 0.05) (data not shown).
Fig. 1
Flow diagram of participants through the study.
Baseline characteristics of the current sample are depicted in Table 1. No differences were found between the intervention and control groups for any of the main outcomes (p > 0.05).
Table 1
Baseline characteristics at both cluster and individual levels according to randomized groups: usual practice (control) and SUFHA intervention. Values are means (standard deviations) unless stated otherwise
| Characteristics | Control | Intervention | Total |
| Cluster level | (n = 12) | (n = 15) | (n = 27) |
| Mean No (range) of participants | 1.6 (1–3) | 1.3 (1–3) | 1.5 (1–3) |
| No of participants: | |||
| ≤2 | 9 | 14 | 23 |
| >2 | 3 | 1 | 4 |
| Individual level | (n = 19) | (n = 19) | (n = 38) |
| Age (years) | 42.3 (9.5) | 45.3 (6.0) | 43.8 (8.0) |
| Nationality (%): | |||
| Portuguese | 84.2% | 95.0% | 89.6% |
| Brazilian | 0.0% | 5.0% | 2.5% |
| Dual nationality (including portuguese) | 15.8% | 0.0% | 7.9% |
| No (%) women | 14 (73.3%) | 15 (78.9%) | 29 (76.3%) |
| No (%) men | 5 (26.7%) | 4 (21.1%) | 9 (23.7%) |
| Smoking status (%): | |||
| Current | 21.1% | 5.0% | 13.0% |
| Former | 15.8% | 45.0% | 30.4% |
| Occasionally | 5.3% | 10.0% | 7.6% |
| Never | 57.9% | 40.0% | 49.0% |
| Worker status (No): | |||
| Full time | 19 | 19 | 38 |
| Part time | 0 | 0 | 0 |
| Years of Service | 14.6 (11.5) | 15.2 (10.1) | 14.9 (10.7) |
| Daily Working (min/day) | 467.4 (79.0) | 480.0 (80.3) | 474.0 (78.8) |
| Salary band (%): | |||
| Very difficult | 5.3% | 15.0% | 10.1% |
| Sufficient for requirements | 42.1% | 60.0% | 51.1% |
| Comfortable | 52.6% | 25.0% | 38.8% |
| Education (%): | |||
| Ph.D. Degree | 15.8% | 10.0% | 12.9% |
| Master’s Degree | 15.8% | 10.0% | 12.9% |
| Bachelor’s Degree | 31.6% | 60.0% | 45.8% |
| High School | 36.8% | 20.0% | 28.4% |
| Occupation (%): | |||
| Academic/Administrative Services | 26.3% | 50.0% | 38.2% |
| Management/Administrative Services | 15.8% | 20.0% | 17.9% |
| Financial Services | 15.8% | 0.0% | 7.9% |
| Other | 42.1% | 30.0% | 36.0% |
| Chronic Disease | |||
| Yes | 21.1% | 20.0% | 20.6% |
| No | 78.9% | 80.0% | 79.4% |
| Medication | |||
| Yes | 57.9% | 20.0% | 39.0% |
| No | 42.1% | 80.0% | 61.0% |
| Biometric measurements | |||
| Body mass index (kg/m2) | 30.5 (7.4) | 27.2 (6.1) | 28.8 (6.9) |
| Body fat (%) | 38.3 (8.6) | 36.5 (6.9) | 37.4 (7.8) |
| Body weight (kg) | 82.3 (21.1) | 72.0 (16.5) | 77.0 (19.4) |
| Height (m) | 1.64 (0.1) | 1.63 (0.1) | 1.63 (0.1) |
| Waist circumference (cm) | 90.2 | 82.8 | 86.4 |
| ActivPAL outcomes | |||
| Sitting time (min/day) | 475.9 (130.4) | 469.0 (70.5) | 472.4 (102.7) |
| Prolonged (≥30 min) sitting (min/day) | 266.7 (118.7) | 276.1 (93.8) | 271.5 (105.4) |
| Prolonged (≥60 min) sitting (min/day) | 125.6 (104.9) | 145.0 (86.7) | 135.5 (95.2) |
| Seated Transport Time (min/day) | 69.9 (47.9) | 63.8 (26.1) | 66.8 (37.9) |
| Standing time (min/day) | 248.4 (82.2) | 274.2 (92.5) | 261.6 (87.5) |
| Stepping time (min/day) | 81.5 (23.3) | 99.9 (27.3) | 91.0 (26.8) |
| No sit to stand transitions | 45.1 (12.2) | 44.9 (11.2) | 45.0 (11.6) |
| Total no Steps per day | 6519.2 (2239.7) | 8235.3 (2664.7) | 7399.3 (2584.8) |
| Cycling time (min/day) | 0.02 (0.1) | 0.43 (1.7) | 0.23 (1.2) |
| Wear time (min/day) | 1440 (0.0) | 1440 (0.0) | 1440 (0.0) |
| No of valid days | 6.0 (0.0) | 6.0 (0.0) | 6.0 (0.0) |
Comparisons between baseline and 3 months follow-up for the primary outcomes of the subsample of the intervention group are presented in Table 2. As shown, there were significant reductions in sitting time and prolonged sitting time (> 30 min) and a concomitant increase in the time spent standing (p < 0.05) during this period.
Table 2
Differences in ActivPAL outcomes between baseline and 3-month follow-up in a subsample of the SUFHA intervention group (n = 11)
| Mean (SD) | Paired-sample T-test | |||
| Baseline | 3 Months | Difference | P value | |
| Sitting time (min/day) | 456.6 (81.9) | 412.6 (106.5) | –44.0 (72.4) | 0.036* |
| Prolonged (≥30 min) sitting (min/day) | 270.9 (105.7) | 225.6 (96.1) | –45.3 (68.6) | 0.027* |
| Prolonged (≥60 min) sitting (min/day) | 150.6 (84.9) | 122.9 (74.8) | –27.7 (76.5) | 0.129 |
| Seated Transport (min/day) | 66.9 (21.3) | 64.6 (28.7) | –2.3 (32.0) | 0.407 |
| Standing time (min/day) | 307.3 (111.6) | 359.0 (125.1) | 51.7 (53.3) | 0.005* |
| Stepping time (min/day) | 106.5 (30.3) | 111.3 (31.5) | 4.8 (14.1) | 0.144 |
| No sit to stand transitions | 44.0 (9.3) | 44.2 (8.4) | 0.18 (10.2) | 0.477 |
| Total Steps per day | 8750 (2927) | 8933 (2855) | 183.6 (1474) | 0.344 |
| Cycling time (min/day) | 0.71 (2.3) | 0.77 (2.5) | 0.6 (0.3) | 0.264 |
| Wear time (min/day) | 1440 (0.0) | 1440 (0.0) | 0.0 (0.0) | N/A |
| No of valid days | 6.0 (0.0) | 5.9 (0.3) | 0.09 (0.30) | 0.170 |
*Mean significant differences between moments of assessment based on the paired sample T-test analysis.
Within and between group comparisons of the intervention and control group from baseline to the 6-months are presented in Table 3 (primary outcomes) and Table 4 (secondary outcomes).
Table 3
Changes in primary outcomes at 6-month follow up between participants randomized to usual practice (control) or SUFHA intervention
| Mean change from baseline (SD) | Time*group | ||
| interaction effect | |||
| Control (n = 19) | Intervention (n = 19) | P value | |
| Sitting time (min/day) | 8.63 (75.6) | –9.91 (54.7) | 0.392 |
| Prolonged (≥30 min) sitting (min/day) | –1.26 (65.9) | –25.5 (58.2)* | 0.236 |
| Prolonged (≥60 min) sitting (min/day) | –1.62 (68.1) | –19.9 (70.6) | 0.421 |
| Seated Transport (min/day) | 0.55 (39.5) | 10.1 (20.7)* | 0.355 |
| Standing time (min/day) | –11.8 (50.3) | 5.96 (55.1) | 0.307 |
| Stepping time (min/day) | 5.27 (20.8) | 0.19 (21.5) | 0.464 |
| No sit to stand transitions | 0.79 (7.35) | 1.66 (6.11) | 0.695 |
| Total Steps per day | 613.0 (2053) | –90.1 (1916) | 0.282 |
| Cycling time (min/day) | 0.43 (1.19) | 0.73 (2.18) | 0.289 |
| Non-wear time (min/day) | 3.89 (11.6) | 1.48 (6.44) | 0.623 |
| No of valid days | 0.00 (0.46) | 0.00 (0.47) | 0.899 |
*Mean significant differences between moments of assessment based on the paired sample T-test analysis. Note: The model included clustering, age sex, and BMI as covariates in the repeated measures ANCOVA.
Table 4
Changes in secondary outcomes at 6-month follow up between participants randomized to usual practice (control) or SUFHA intervention
| Mean change from baseline (95% CI) | Time*group | ||
| interaction effect | |||
| Control (n = 19) | Intervention (n = 19) | P value | |
| Biometric measurements | |||
| Body mass index (kg/m2) | –0.31 (–0.94 to 0.31) | 0.01 (–0.37 to 0.38) | 0.397 |
| Body fat mass (%) | –1.61 (–2.78 to –0.43)* | –3.65 (–5.82 to –1.49)* | 0.109 |
| Waist Circumference (cm) | –1.81 (–4.02 to 0.39) | 1.48 (–0.74 to 3.69) | 0.037# |
| Psychologic measurements | |||
| Need for Recovery after work (0–11) | –1.05 (–2.44 to 0.33) | –1.68 (–2.96 to –0.41)* | 0.486 |
| Work engagement (0–63) | –2.11 (–6.03 to 1.82) | 0.63 (–2.87 to 4.13) | 0.282 |
| Work difficulties (0–40) | –2.37 (–5.56 to 0.82) | –2.68 (–6.19 to 0.82) | 0.889 |
| Overall fatigue (0–32) | –1.84 (–4.64 to 0.95) | –2.21 (0.33 to 4.09)* | 0.835 |
| Musculoskeletal discomfort (0–77) | –4.00 (–8.36 to 0.36) | –4.89 (–8.86 to –0.93)* | 0.752 |
| Quality of Life (score) | 1.53 (0.39 to 2.67)* | 2.16 (0.76 to 3.55)* | 0.466 |
| Diet-related measurements | |||
| Adherence to Mediterranean diet (score) | –3.68 (–2.06 to 1.32) | 1.00 (–0.96 to 2.96) | 0.274 |
Note: The model included clustering, age sex, and BMI as covariates in the repeated measures ANCOVA. #mean significant time*group interaction, thus a difference between groups for the changes from baseline to the 6 months. *mean significant time effect within group based on the paired-sample T-test.
As shown in Table 3, no significant time*group interaction was found for any of the primary outcomes. Although, there was a significant reduction within the intervention group for prolonged sitting (> 30 min) of about 26 min/day (p < 0.05).
There is relevant information from the monthly self-reported questionnaire regarding the usage of the sit-stand desk by the intervention group. In the first month of the intervention the participants reported an average of 4.6 days of usage, progressively reducing to an average of 3.1 days of usage per week at the 6th month. Also, they reported standing for bouts of 20–30 minutes in the first month, reducing to 10–20 minutes in the last month. Regarding the percentage of the day using the sit-stand desk while standing, it started at an average of 36% lowering to 27% in the last month of the intervention. The number of participants that reported difficulties while using the sit-stand desk changed from 4 in the first three months to 5 in the fourth month, lowering to 3 in the final two months of the intervention. Regarding the self-reported pain during the intervention, there were 9 occurrences in the first month, lowering to 4 in both the second and third months, increasing to 7 in the fourth month, and finally reducing to 5 in the last two months.
As shown in Table 4, no significant time*group interactions were found for any of the secondary outcomes, except for waist circumference, favoring the control group. Although not statistically apart from the alteration found in the control group, there were significant improvements within the intervention group for body fat mass percentage, quality of life, musculoskeletal discomfort, overall fatigue, and the need for recovery after work (p < 0.05).
4Discussion
The findings from our intervention showed significant reductions in sitting time and increases in standing time at 3 months, but no differences between the control and intervention group from baseline to 6 months, for the main outcomes (e.g., sitting, standing, sit-to-stand transitions) (p > 0.05). Despite the majority of the literature indicating a significant beneficial effect of sit-to-stand desks on reducing sitting time after 6 months [16–34], this is not the first time a sit-to-stand desk based intervention failed to reduce sitting time at 6 months [48–50]. In fact, in a previous trial, although there were reductions of about 42 min/day in the intervention group at 3 months in comparison to the control group, these reductions were not maintained at 6 months [28]. Other studies have also reported successful reductions in sitting time over the short term in the intervention group as compared to the control group (3 months: –50.6 min/workday [51] and –48 min/day [52]). Although only performed in a subsample of the intervention group, the within group reductions in sitting time at 3 months observed in our study (–44.0 min/day) were like those reported previously.
There are some reasons that may justify the lack of intervention effect in the present trial at 6 months. First, there seems to have been a decrease in the usage of the sit-stand desk throughout the intervention period (i.e., based on the self-reported results from the monthly questionnaire), which can be justified not only by the lack of novelty effect as time passes, but also by a higher work flux that participants reported in the final month of the intervention. This higher work-flux, in some cases, may have compromised the habitual use of the sit-stand desk, making the usage during the final month of the intervention to not be completely representative of the usage during the prior months. Indeed, the responses to the monthly questionnaire revealed that 9 out of 19 participants considered that during the final week of ActivPAL use (i.e., 6-month), they had more work-flux than in the baseline week. Also, when directly asked if the work-flux somehow reduced their ability to use the sit-stand desk, 13 out of 19 said yes, which again supports our hypothesis. Moreover, the results for some of the secondary outcomes support this idea, as significant improvements were found from baseline to the end of the intervention period in the intervention group that did not happen in the control group, which may be explained by changes in physical behaviors throughout the intervention period that were not detected on that final week of assessment.
Other reasons may explain the lack of results from the present intervention in comparison to the ones from previous 6-month interventions. For example, in opposition to some prior interventions, in the current study there were no mandatory goals to attain (i.e., a specific amount of daily standing), but simply the recommendation to reduce sitting time as much as possible, having in mind that shifting from sitting to a standing posture more often would be beneficial. There were some prompts to keep the participants engaged (that went from 4/monthly in the first month, progressively decreasing to 1/monthly in the last month), however, this is substantially different from several daily or hourly prompts throughout the intervention [24, 25, 34]. Interestingly, a study [53] that simply sent a monthly email to the participants from the intervention group reminding them about good practices, found a 22 min/day reduction in sitting time when compared to the control group, which is similar to our intervention within-subject reductions at 6 months (i.e., 19 min/day). This fact can also justify the lower magnitude of sitting time reduction at the end of the intervention period and suggest that a more ecological approach, in which the participants are not receiving prompts as often, may not work as well as prompting them to reduce sitting time in a more demanding way. Lastly, there was no financial incentive given to the participants, a strategy that has been used in previous sit-stand interventions to boost participants to engage deeper into this type of intervention [23, 25, 34, 51, 54].
Beyond our main outcomes, we also did not observe a significant time*group effect for any of the secondary outcomes. Nevertheless, the intervention group significantly improved several aspects from baseline to the end of the intervention, that are worth noting. For example, there was a significant reduction of 3.65% in body fat mass that can entail a clinical meaning, as well as an improvement in overall fatigue, need for recovery after work, musculoskeletal discomfort, and quality of life of these workers. Also, despite the non-significant reduction in overall sitting time, the time spent in this behavior in a prolonged manner (>30 min) was significantly reduced in the intervention group by 26 min/day. This is of significance given that breaking up 30 minutes of sitting every 5 min has been shown to help regulate blood pressure and control blood glucose levels [55]. Beyond the intervention group, we also observed improvements in the control group from baseline to the end of the 6 months for body fat mass and quality of life. Even though the clustered nature of the present RCT was to protect against the contamination of the control group by the intervention group, the improvements in the control group during the intervention period may be associated with some alteration in their normal routines in response to the initial psychoeducational session. Control group improvement in PA intervention trials is not uncommon. A systematic review on this topic found that 28% of all included studies reported significant improvements in control group PA, most of which were similar to the improvements observed in the intervention group [56].
There is evidence suggesting that using a sit-stand desk had no negative effect on performance or perception, and it can even lead to increased brain activity in the alpha band for the parietal region [57], thus concluding that users of sit-stand desks can freely stand for any level of task difficulty for work that involves working memory. However, not all standing desks are the same, and one must be careful with the space for working that these desks allow. For example, some of our participants reported that this specific standing desk (i.e., 80 cm per 63.5 cm) did not have enough space to perform work that relies on a lot of paperwork, which can limit the adoption of a standing posture during this type of work. Also, another limitation reported by some participants was the fact that the space for the keyboard and mouse was not deep enough to completely support the forearm on that platform. This may have led to muscular discomfort, although the intervention group reported having decreased muscular discomfort during the 6 months. It is likely that the potential discomfort from a standing desk is minor compared to the many discomforts that can result from working in a prolonged seated position at a desk [58]. Nevertheless, for workers to maximally benefit from using a sit-stand desk in terms of reduced risk of musculoskeletal disorders, while also not compromising work productivity, it is important that the ergonomic set up and allottable functional working space of the desk are fully taken into consideration.
Besides the impact of the intervention itself, there is evidence supporting changes and fluctuations of device-measured movement behaviors according to seasons and weather [59]. In fact, PA volume and moderate-to-vigorous PA have been found to be greater in summer than winter [59]. Sedentary behavior seems to be greater in winter than either spring or summer, and inversely associated with photoperiod and positively associated with precipitation [59]. Our data somehow contradicts this trend, as although non-significant, we found higher standing and lower sitting in the winter (March) and higher sitting and lower standing in the summer (August), in the control group. Once again, we believe that the higher work-flux during the second moment of assessment may have contradicted some of the natural changes that could occur.
This study has many strengths, including its robust randomized controlled cluster design, objectively measured data for standing and sitting time, use of validated questionnaires and focus groups to gain in-depth understanding of reasons for the results observed, and our excellent retention of participants (0% drop-out) with no missing measures at the 6-month follow-up. Despite strengths, there are some limitations worth noting. First, our intervention consisted of office workers at a university and mostly women. Thus, our results may not apply to office workers in other types of industry jobs with different work schedules and office space layouts. Secondly, although our sample size was powered to detect significant differences in our primary outcomes, we may have been underpowered for some of our secondary outcomes.
5Conclusion
The implementation of sit-stand desks in Portugal with full-time university office workers using a more ecological approach was not effective at reducing sitting time after 6 months of usage when compared to workers without sit-stand desks. Nevertheless, there were within group reductions in prolonged sitting (≥30 min), need for recovery after work, and overall fatigue in workers using the sit-stand desk that were not observed in the control group. Thus, SUFHA demonstrated for the first time that the implementation of sit-stand desks in the Portuguese workspace is feasible over the medium term, received well by users, and, although not being effective for reducing sitting time, may offer other health benefits. Future studies in Portugal are needed using different office work settings to collaborate on our findings.
Ethical approval
The project was approved by the ethics commission of the Faculty of Physical Education and Sport at the University of Lusófona in Lisbon (Approval number D0522).
Informed consent
All participants provided written informed consent.
Conflicts of interest
The authors declare that they have no conflict of interest.
Acknowledgments
We appreciate all the time and effort from the participants.
Funding
This study was funded by the ILIND “Fazer+” scientific program (FAZER+/ILIND/CIDEFES/1/2022).
References
[1] | Guthold R , Stevens GA , Riley LM , Bull FC . Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. (2020) ;41: :23–35. |
[2] | Guthold R , Stevens GA , Riley LM , Bull FC . Worldwide trends in insufficient physical activity from to A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health ((2016) ). (2018) ;610: :e1077–e86. |
[3] | Santos DA , Júdice PB , Magalhães JP , Correia IR , Silva AM , Baptista F , et al. Patterns of accelerometer-derived sedentary timeacross the lifespan. Journal of Sports Sciences. (2018) ;3624: :2809–17. |
[4] | Li S , Lear SA , Rangarajan S , Hu B , Yin L , Bangdiwala SI , et al. Association of Sitting Time With Mortality and Cardiovascular Events in High-Income, Middle-Income, and Low-Income Countries. JAMA Cardiol. (2022) ;78: :796–807. |
[5] | Paudel S , Ahmadi M , Phongsavan P , Hamer M , Stamatakis E Do associations of physical activity and sedentary behaviour with cardiovascular disease and mortality differ across socioeconomic groups? A prospective analysis of device-measured and self-reported UK Biobank data. British Journal of Sports Medicine. 2023. |
[6] | Dempsey PC , Owen N , Yates TE , Kingwell BA , Dunstan DW . Sitting Less and Moving More: Improved Glycaemic Control for Type 2 Diabetes Prevention and Management. Current Diabetes Reports. (2016) ;1611: :114. |
[7] | Zou H , Huang L , Zhao Z , Meng X , Li D , Chen X , et al. Dose-response association between sedentary time and incident of diabetes in Chinese middle-aged and older adults: The 4C study. Diabetes Res Clin Pract. (2022) ;191: :110044. |
[8] | Lin Y , Liu Q , Liu F , Huang K , Li J , Yang X , et al. Adverse associations of sedentary behavior with cancer incidence and all-cause mortality: A prospective cohort study. J Sport Health Sci. (2021) ;105: :560–9. |
[9] | Wheeler MJ , Dempsey PC , Grace MS , Ellis KA , Gardiner PA , Green DJ , et al. Sedentary behavior as a risk factor for cognitive decline? A focus on the influence of glycemic control in brain health. Alzheimers Dement (N Y). (2017) ;33: :291–300. |
[10] | Webster KE , Zhou W , Gallagher NA , Smith EML , Gothe NP , Ploutz-Snyder R , et al. Device-measured sedentary behavior in oldest old adults: A systematic review and meta-analysis. Prev Med Rep. (2021) ;23: :101405. |
[11] | Dempsey PC , Friedenreich CM , Leitzmann MF , Buman MP , Lambert E , Willumsen J , et al. Global Public Health Guidelines on PhysicalActivity and Sedentary Behavior for People Living With ChronicConditions: A Call to Action. Journal of Physical Activity &Health. (2021) ;181: :76–85. |
[12] | Whipple MO , Masters KS , Huebschmann AG , Scalzo RL , Reusch JE , Bergouignan A , et al. Acute effects of sedentary breaks on vascular health in adults at risk for type 2 diabetes: A systematic review. Vasc Med. (2021) ;264: :448–58. |
[13] | Wong JY , Gilson ND , van Uffelen JG , Brown WJ . The effects of workplace physical activity interventions in men: A systematic review. Am J Mens Health. (2012) ;64: :303–13. |
[14] | van Uffelen JG , Wong J , Chau JY , van der Ploeg HP , Riphagen I , Gilson ND , et al. Occupational sitting and health risks: A systematic review. American Journal of Preventive Medicine. (2010) ;394: :379–88. |
[15] | Rosenkranz SK , Mailey EL , Umansky E , Rosenkranz RR , Ablah E . Workplace Sedentary Behavior and Productivity: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. (2020) ;1718. |
[16] | Stephens SK , Eakin EG , Clark BK , Winkler EAH , Owen N , LaMontagne AD , et al. What strategies do desk-based workers choose to reduce sitting time and how well do they work? Findings from a cluster randomised controlled trial. Int J Behav Nutr Phys Act. (2018) ;151: :98. |
[17] | Healy GN , Eakin EG , Owen N , Lamontagne AD , Moodie M , Winkler EA , et al. A Cluster Randomized Controlled Trial to Reduce Office Workers’ Sitting Time: Effect on Activity Outcomes. Med Sci Sports Exerc. (2016) ;489: :1787–97. |
[18] | Brakenridge CL , Healy GN , Winkler EAH , Fjeldsoe BS . What Do Workers Do to Reduce Their Sitting Time? The Relationships of Strategy Use and Workplace Support With Desk-Based Workers’ Behavior Changes in a Workplace-Delivered Sitting-Reduction and Activity-Promoting Intervention. J Occup Environ Med. (2018) ;6011: :1026–33. |
[19] | Chau JY , Daley M , Dunn S , Srinivasan A , Do A , Bauman AE , et al. The effectiveness of sit-stand workstations for changing office workers’ sitting time: results from the Stand@Work randomized controlled trial pilot. Int J Behav Nutr Phys Act. (2014) ;11: :127. |
[20] | Peterman JE , Healy GN , Winkler EA , Moodie M , Eakin EG , Lawler SP , et al. A cluster randomized controlled trial to reduce office workers’ sitting time: effect on productivity outcomes. Scand J Work Environ Health. (2019) ;455: :483–92. |
[21] | Winkler EAH , Chastin S , Eakin EG , Owen N , Lamontagne AD , Moodie M , et al. Cardiometabolic Impact of Changing Sitting, Standing, and Stepping in the Workplace. Med Sci Sports Exerc. (2018) ;503: :516–24. |
[22] | Pierce J , Legg S , Godfrey JR , Kawabata E . The effects of introducing electric adjustable height desks in an office setting on workplace physical activity levels: A randomised control field trial. Work. (2019) ;621: :139–50. |
[23] | Edwardson CL , Biddle SJH , Clemes SA , Davies MJ , Dunstan DW , Eborall H , et al. Effectiveness of an intervention for reducing sitting time and improving health in office workers: three arm cluster randomised controlled trial. BMJ. (2022) ;378: :e069288. |
[24] | Edwardson CL , Yates T , Biddle SJH , Davies MJ , Dunstan DW , Esliger DW , et al. Effectiveness of the Stand More AT (SMArT) Work intervention: cluster randomised controlled trial. BMJ. (2018) ;363: :k3870. |
[25] | Barone Gibbs B , Hergenroeder AL , Perdomo SJ , Kowalsky RJ , Delitto A , Jakicic JM . Reducing sedentary behaviour to decrease chronic low back pain: the stand back randomised trial. Occupational and Environmental Medicine. (2018) ;755: :321–7. |
[26] | Graves EFL , Murphy CR , Shepherd SO , Cabot J , Hopkins ND . Evaluation of sit-stand workstations in an office setting: A randomised controlled trial. BMC Public Health. (2015) ;15: :1145. |
[27] | Dewitt S , Hall J , Smith L , Buckley JP , Biddle SJH , Mansfield L , et al. Office workers’ experiences of attempts to reduce sitting-time: An exploratory, mixed-methods uncontrolled intervention pilot study. BMC Public Health. (2019) ;191: :819. |
[28] | Weatherson KA , Wunderlich KB , Faulkner GE . Impact of a low-cost standing desk on reducing workplace sitting (StandUP UBC): A randomised controlled trial. Appl Ergon. (2020) ;82: :102951. |
[29] | MacEwen BT , Saunders TJ , MacDonald DJ , Burr JF . Sit-Stand Desks To Reduce Workplace Sitting Time In Office Workers With Abdominal Obesity: A Randomized Controlled Trial. J Phys Act Health. (2017) ;149: :710–5. |
[30] | Arguello D , Thorndike AN , Cloutier G , Morton A , Castaneda-Sceppa C , John D . Effects of an “Active-Workstation” Cluster RCT on Daily Waking Physical Behaviors. Med Sci Sports Exerc. (2021) ;537: :1434–45. |
[31] | Resendiz M , Lustik MB , Conkright WR , West GF . Standing desks for sedentary occupations: Assessing changes in satisfaction and health outcomes after six months of use. Work. (2019) ;633: :347–53. |
[32] | Bodker A , Visotcky A , Gutterman D , Widlansky ME , Kulinski J . The impact of standing desks on cardiometabolic and vascular health. Vasc Med. (2021) ;264: :374–82. |
[33] | Nelson-Wong E , Gallagher K , Johnson E , Antonioli C , Ferguson A , Harris S , et al. Increasing standing tolerance in office workers with standing-induced back pain. Ergonomics. (2020) ;637: :804–17. |
[34] | Hergenroeder A , Quinn TD , Perdomo SJ , Kline CE , Gibbs BB . Effect of a 6-month sedentary behavior reduction intervention on well-being and workplace health in desk workers with low back pain. Work (Reading, Mass). (2022) ;714: :1145–55. |
[35] | Gao L , Flego A , Dunstan DW , Winkler EA , Healy GN , Eakin EG , et al. Economic evaluation of a randomized controlled trial of an intervention to reduce office workers’ sitting time: the “Stand Up Victoria” trial. Scand J Work Environ Health. (2018) ;445: :503–11. |
[36] | Schwartz B , Kapellusch JM , Baca A , Wessner B . Medium-term effects of a two-desk sit/stand workstation on cognitive performance and workload for healthy people performing sedentary work: A secondary analysis of a randomised controlled trial. Ergonomics. (2019) ;626: :794–810. |
[37] | Donath L , Faude O , Schefer Y , Roth R , Zahner L . Repetitive daily point of choice prompts and occupational sit-stand transfers, concentration and neuromuscular performance in office workers: An RCT. Int J Environ Res Public Health. (2015) ;124: :4340–53. |
[38] | Magalhães JP , Hetherington-Rauth M , Rosa GB , Correia IR , Pinto GM , Ferreira JP , et al. Physical Activity and Sedentary Behavior in the Portuguese Population: What Has Changed from 2008 to 2018? Medicine and Science in Sports and Exercise. 2023. |
[39] | Júdice PB , Silva H , Teno SC , Monteiro P , Silva MN , Carraça EV , et al. Providing office workers with height-adjustable workstation to reduce and interrupt workplace sitting time: protocol for the Stand Up for Healthy Aging (SUFHA) cluster randomized controlled trial. Trials. (2023) ;241: :381. |
[40] | Use WHOECoPSt, Interpretation of A, World Health O. Physical status : the use of and interpretation of anthropometry, report of a WHO expert committee. Geneva: World Health Organization; 1995. |
[41] | Segal KR , Van Loan M , Fitzgerald PI , Hodgdon JA , Van Itallie TB . Lean body mass estimation by bioelectrical impedance analysis: A four-site cross-validation study. The American Journal of Clinical Nutrition. (1988) ;471: :7–14. |
[42] | Pichot P , Brun JP . Questionnaire bref d’auto-évaluation des dimensions dépressive, asthénique et anxieuse [Short self-assessment questionnaire on depressive, asthenic, and anxiety dimensions]. Annales Médico-Psychologiques. (1984) ;1426: :862–5. |
[43] | Schaufeli WB , Bakker AB , Salanova M . The Measurement of Work Engagement With a Short Questionnaire: A Cross-National Study. Educational and Psychological Measurement. (2006) ;664: :701–16. |
[44] | Schmidt S , Mühlan H , Power M . The EUROHIS-QOL 8-item index: Psychometric results of a cross-cultural field study. European Journal of Public Health. (2005) ;164: :420–8. |
[45] | Ozminkowski RJ , Goetzel RZ , Chang S , Long S . The application of two health and productivity instruments at a large employer. Journal of Occupational and Environmental Medicine/American College of Occupational and Environmental Medicine. (2004) ;467: :635–48. |
[46] | van Veldhoven M , Broersen S . Measurement quality and validity of the “need for recovery scale. Occupational and Environmental Medicine. (2003) ;60: (Suppl 1):i3–9. |
[47] | Panagiotakos DB , Pitsavos C , Arvaniti F , Stefanadis C . Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietScore. Preventive Medicine. (2007) ;444: :335–40. |
[48] | Renaud LR , Jelsma JGM , Huysmans MA , van Nassau F , Lakerveld J , Speklé EM , et al. Effectiveness of the multi-component dynamic work intervention to reduce sitting time in office workers –Results from a pragmatic cluster randomised controlled trial. Applied Ergonomics. (2020) ;84: :103027. |
[49] | Nooijen CFJ , Blom V , Ekblom Ö , Heiland EG , Larisch L-M , Bojsen-Møller E , et al. The effectiveness of multi-componentinterventions targeting physical activity or sedentary behaviouramongst office workers: A three-arm cluster randomised controlledtrial. BMC Public Health. (2020) ;201: :1329. |
[50] | Akksilp K , Koh JJE , Tan V , Tong EH , Budtarad N , Xueying G , et al. The physical activity at work (PAW) study: A cluster randomised trial of a multicomponent short-break intervention to reduce sitting time and increase physical activity among office workers in Thailand. The Lancet Regional Health - Southeast Asia. (2023) ;8: :100086. |
[51] | Edwardson CL , Yates T , Biddle SJH , Davies MJ , Dunstan DW , Esliger DW , et al. Effectiveness of the Stand More AT (SMArT) Work intervention: Cluster randomised controlled trial. BMJ. (2018) ;363: :k3870. |
[52] | Danquah I , Kloster S , Holtermann A , Aadahl M , Bauman A , Ersbøll A , et al. Take a Stand!–a multi-component intervention aimed at reducing sitting time among office workers–a cluster randomized trial. International Journal of Epidemiology. (2016) ;461: :128–40. |
[53] | Ma J , Ma D , Li Z , Kim H Effects of aWorkplace Sit-Stand Desk Intervention on Health and Productivity. Int J Environ Res Public Health. 2021;1821. |
[54] | Dutta N , Koepp GA , Stovitz SD , Levine JA , Pereira MA . Using sit-stand workstations to decrease sedentary time in office workers: A randomized crossover trial. International Journal of Environmental Research and Public Health. (2014) ;117: :6653–65. |
[55] | Duran AT , Friel CP , Serafini MA , Ensari I , Cheung YK , Diaz KM . Breaking Up Prolonged Sitting to Improve Cardiometabolic Risk: Dose-Response Analysis of a Randomized Crossover Trial. Med Sci Sports Exerc. (2023) ;555: :847–55. |
[56] | Waters L , Reeves M , Fjeldsoe B , Eakin E . Control group improvementsin physical activity intervention trials and possible explanatoryfactors: A systematic review. Journal of Physical Activity &Health. (2012) ;96: :884–95. |
[57] | Labonté-LeMoyne E , Jutras MA , Léger PM , Sénécal S , Fredette M , Begon M , et al. Does Reducing Sedentarity With StandingDesks Hinder Cognitive Performance? Hum Factors. (2020) ;624: :603–12. |
[58] | Putsa B , Jalayondeja W , Mekhora K , Bhuanantanondh P , Jalayondeja C . Factors associated with reduced risk of musculoskeletal disorders among office workers: A cross-sectional study 2017 to 2020. BMC Public Health. (2022) ;221: :1503. |
[59] | Turrisi TB , Bittel KM , West AB , Hojjatinia S , Hojjatinia S , Mama SK , et al. Seasons, weather, and device-measured movement behaviors: A scoping review from 2006 to 2020. International Journal of Behavioral Nutrition and Physical Activity. (2021) ;181: :24. |


