
Sociodemographic factors, health behavior, parental or workplace smoking, and adult asthma risk in the United States
Abstract
BACKGROUND:
Although several studies have found a link between parental or workplace smoking and asthma risk, particularly in children and adolescents, only a few studies have found this link in adults.
OBJECTIVE:
This study aimed to investigate the associations of sociodemographic factors, health behavior, and parental or workplace smoking with adult asthma risk in the United States (US).
METHODS:
A secondary data analysis on 874 participants aged 25–45 was performed using data from the 2011–2014 National Survey of Midlife Development in the United States Refresher. Participants were divided into smokers and nonsmokers. Participants were further divided into groups A (a father or mother with a smoking history) and B (others in the house or colleagues in the workplace who had a smoking history).
RESULTS:
Findings from the FREQ procedure revealed that sociodemographic (female, black, school or college education, unmarried/divorced, and employed) and lifestyle (no alcohol intake, physically inactive, and obese) and clinical (diabetes and joint disease) factors were significantly associated with one- or more-fold odds of asthma among adult smokers than nonsmokers. Adult smokers in group A, particularly females, those with a high school or college education, physically inactive, and overweight or obese, had a higher risk of asthma than those in group B.
CONCLUSION:
Adult smokers’ risk of developing asthma is increased in the US by having smoked with their parents, being a woman, being black, having a school or college education, being single or divorced, working, not drinking alcohol, being physically inactive, being obese, having diabetes, and having a joint disease.
1Introduction
Asthma has been recognized as a significant public health problem since the 1970 s [1]. The prevalence of asthma worldwide has increased by 12.6% since the 1990 s [2]. The global prevalence of self-reported, doctor-diagnosed, and treated clinical asthma in adults was estimated to be 4.3% and 4.5%, respectively, with a 21-fold variation among 70 countries (0.2% in China and 21.5% in Australia) [3]. The five countries with the highest prevalence of clinical asthma were Australia (21.5%), Sweden (20.2%), the United Kingdom (UK) (18.2%), the Netherlands (15.3%), and Brazil (13.0%) [3]. Approximately 9% of the population of the United States (US) [4] and 6.5% of those in the UK have asthma [5]. From 2000–2010, the average cost per asthma-related hospital stay in the US for adults increased from $5,200 to $6,600.
Smoking leads to acute bronchoconstriction and lung damage [6], which reduces lung function [7]. Additionally, smoking reduces responsiveness to glucocorticoids [8], which leads to an increase of T-lymphocytes (mainly CD8 cells [9] and macrophages) within the airway walls. Thus, in smokers, the peripheral airways are infiltrated by mononuclear cells and macrophages [10]. Previous studies have shown that the rate of decline in lung function is more accelerated in smokers with asthma than in nonsmokers without asthma [11]. Moreover, an accelerated decline in lung function over time has been found in asthmatic individuals [12] due to their lower forced expiratory volume in one second.
Numerous studies have explored the risk factors for asthma among children [13, 14], especially those living in the US [15, 16]. These studies identified older age, obesity, low socioeconomic status, smoking, and physical inactivity as asthma risk factors. One study also found that a group of US children, tweens, and adults had poor asthma outcomes because of ongoing exposure to modifiable factors, such as tobacco smoke, being overweight, modest physical activity, and limited family incomes [16]. One risk factor, as well as a common asthma trigger, is cigarette smoking, mainly passive (secondhand) [17]. A widespread and avoidable risk factor, passive smoking exposes individuals to more than 7,000 chemicals, including toxic hundreds, that may cause cancer [18]. Parental smoking is a common source of passive smoking.
Several studies have shown that parental smoking history is associated significantly with asthma risk, especially among children and adolescents [19, 20]. Limited studies have shown this association in adults [21]. However, these studies differ methodically (e.g., setting, population, self-reported smoking, history). Thus, the current research investigates the associations of sociodemographic (sex, race, education, marital status, and employment status), lifestyle (alcohol intake, physical inactivity, obesity, and central obesity), clinical (diabetes, joint, and cardiovascular diseases) factors, and parental or workplace smoking with adult asthma risk in the US. This research hypothesized that those who grew up living with smokers, especially with a father or mother, could be at risk for triggering asthma.
2Methods
For this secondary analysis, data was used from the National Survey of Midlife Development in the United States (MIDUS) refresher conducted between 2011 and 2014, as previously explained [22]. The 2011–2014 MIDUS refresher study data was selected because the new national probability sample was intended to expand and refresh the MIDUS study overall by recruiting a new sample with demographics similar to those of MIDUS 1 participants. The MIDUS refresher was an interdisciplinary study investigating psychosocial factors and health in adults by collecting demographic and biomarker data through an initial structured telephone interview and clinic visit. The combined response rate for the telephone interview and clinic visit was weighted to all eligible respondents across sample types to obtain unbiased estimates by including them in the analyses. The recruitment and assessment procedures utilized for the MIDUS refresher are available elsewhere [23].
The collected data in the MIDUS refresher has complied with the data protection and privacy regulations of the National Archive of Computerized Data on Aging (NACDA). The institutional review board (IRB) of Harvard University, Georgetown University, the University of California at Los Angeles, and the University of Wisconsin approved the MIDUS refresher. All participants in the MIDUS refresher provided written informed consent. The current study does not require IRB approval due to a secondary analysis performed using the original data from the MIDUS refresher. This can be explained by the lack of personal information in the data and the inability to obtain the codes due to proper coding, both of which prevent retrieval of the data. Since there were no human participants in this study, no consent was needed from the participants.
In this study, 874 adults aged between 25 and 45 years with smoking status data were included excluding those who answered “don’t know” or “refused” (n = 588). Individuals older than 45 years (n = 2,115) were also excluded. The inclusion was limited to 24–45 years of age due to an overlap in the diagnosis of adult-onset asthma in the older age group, which was particularly apparent in the survey-collected data. All participants were categorized as smokers or nonsmokers based on self-reporting to the following questions: “Have you ever smoked cigarettes regularly—that is, at least a few cigarettes every day?” If a person answered “no,” they were considered nonsmokers, whereas they were determined as smokers if they responded to the question “yes.” This question was broadly similar to a question asked in a previous study [24].
Parental smoking was determined based on the following self-reported question. “When you were growing up–that is, during your first 16 years—did you live with anyone in your household who smoked cigarettes or other tobacco products (other than yourself)—FATHER or MOTHER?” Workplace smoking was defined by asking, “While at your job in the past, did anyone regularly smoke cigarettes or other tobacco products in your immediate work area (other than yourself)?” Group A included participants who answered “yes” to the first question and defined it as parental smoking, while Group B included those who answered “yes” to the second question.
The outcome of asthma was assessed based on self-reporting: “In the past twelve months, have you experienced or been treated for asthma?” If a person answered “no,” they were considered to have no asthma, whereas those who answered “yes” were believed to have asthma. This question was similar to a question in a previous study [3].
This research included a series of sociodemographic, lifestyle, and clinical factors such as sex, race, education, marital status, employment status, alcohol intake, physical inactivity, obesity, diabetes, and joint and cardiovascular diseases. The following variables were dichotomized: male (used as a reference) and female, white (used as a reference) and Black/Asian, school/college and graduates (used as a reference), married (used as a reference) and unmarried/divorced/widow, employed and unemployed (used as a reference), and alcohol consumption (yes and no). An alcohol intake was used as a reference.
The physical inactivity was assessed based on the self-reported question: “How often do you engage in vigorous physical activity?” [25] Physical inactivity was determined if the participants answered: “once a month,” “less than once a month,” or “never” [26]. Obesity was assessed using body mass index (BMI), which is calculated by dividing individuals’ weight in kilograms (kg) by height in meters (m) squared. The participants’ height (in inches) was multiplied by 0.0254 to obtain the height in meters. The weight (in pounds) was multiplied by 0.4536 to acquire the mass in kilograms. The height was set at 84 inches to restrict extremes if it was greater than 84 inches.
The central obesity was determined using a self-reported question: “What is your waist size—that is, how many inches around is your waist?” Patients were instructed to measure their waist circumference (WC) at the level of their navel at the vastest point using non-stretchable tape. Ensured participants did not measure over clothing (including thin clothing) and recorded answers to the nearest quarter (1/4) inch. The status of other diseases (e.g., cardiovascular diseases, diabetes, and joint/bone diseases) was measured using the dichotomous indicators “yes” and “no” (reference).
The Farrington-Manning test was used to estimate the required sample size for each group to prove accurate results by using the level of significance (alpha = 0.05), power (0.8), and proportion between groups (0.32, 0.21) [27]. Based on this test, the minimum sample for each group was 213. Further, the Kolmogorov-Smirnov test was used to determine the normality of the continuous variables [28]. The data was presented as the mean (standard deviation) for continuous variables and the number (percentage) for categorical variables. The chi-square test was used for the categorical variables and independent student t-tests for the continuous variables to identify statistically significant differences between smokers and nonsmokers.
The FREQ procedure was used to assess the prevalence of smokers, nonsmokers, and groups (A and B). The associations of demographic, behavioral, and clinical risk factors with the risk of asthma among adults with smokers compared to nonsmokers were examined using the FREQ procedure [29]. A multivariable regression analysis was performed to test for possible confounding interactions affecting asthma occurrence with a high degree of collinearity. To achieve this analysis, the following conditions were applied: tolerance value and eigenvalues should not be below 0.1 or close to 0, respectively. The FREQ procedure was also used to assess the prevalence and risk of asthma according to demographic, behavioral, and clinical risk factors by group (A and B) among smoking adults. A significance between asthma and exposure to smoke during childhood was determined using the Chi-square test. Furthermore, odds ratios (ORs) with associated confidence intervals (95% CI) were calculated.
The age of asthma onset in groups A and B was assessed using unadjusted and adjusted multiple linear regression models. The adjusted model includes age, sex, race, education, marital status, employment status, alcohol intake status, obesity, central obesity, joint/bone disease, diabetes, and cardiovascular disease. The Kaplan–Meier (log-rank) test was used to assess the relationship between childhood smoke exposure and the onset of asthma in groups A and B. All statistical analyses were accomplished using SAS version 9.4 (SAS Corporation Inc., Cary, NC, USA), and statistical significance was determined as a p-value <0.05.
3Results
Of 3,577 participants, 874 were included in the analysis after excluding missing data or who refused to fill in the questionnaires (16.4% of 588). Those older than 45 (59.1% of 2,115) were excluded. The study included 490 (56.1%) smokers and 384 (43.9%) nonsmokers (Fig. 1). The majority of adult smokers significantly had attained high school/college education (70.1%) (Table 1). The prevalence of asthma was higher in smokers (11%) and group B (6.2%) than in nonsmokers and group A (Fig. 2).
Fig. 1
The flow diagram of the study sample through the MIDUS refresher.
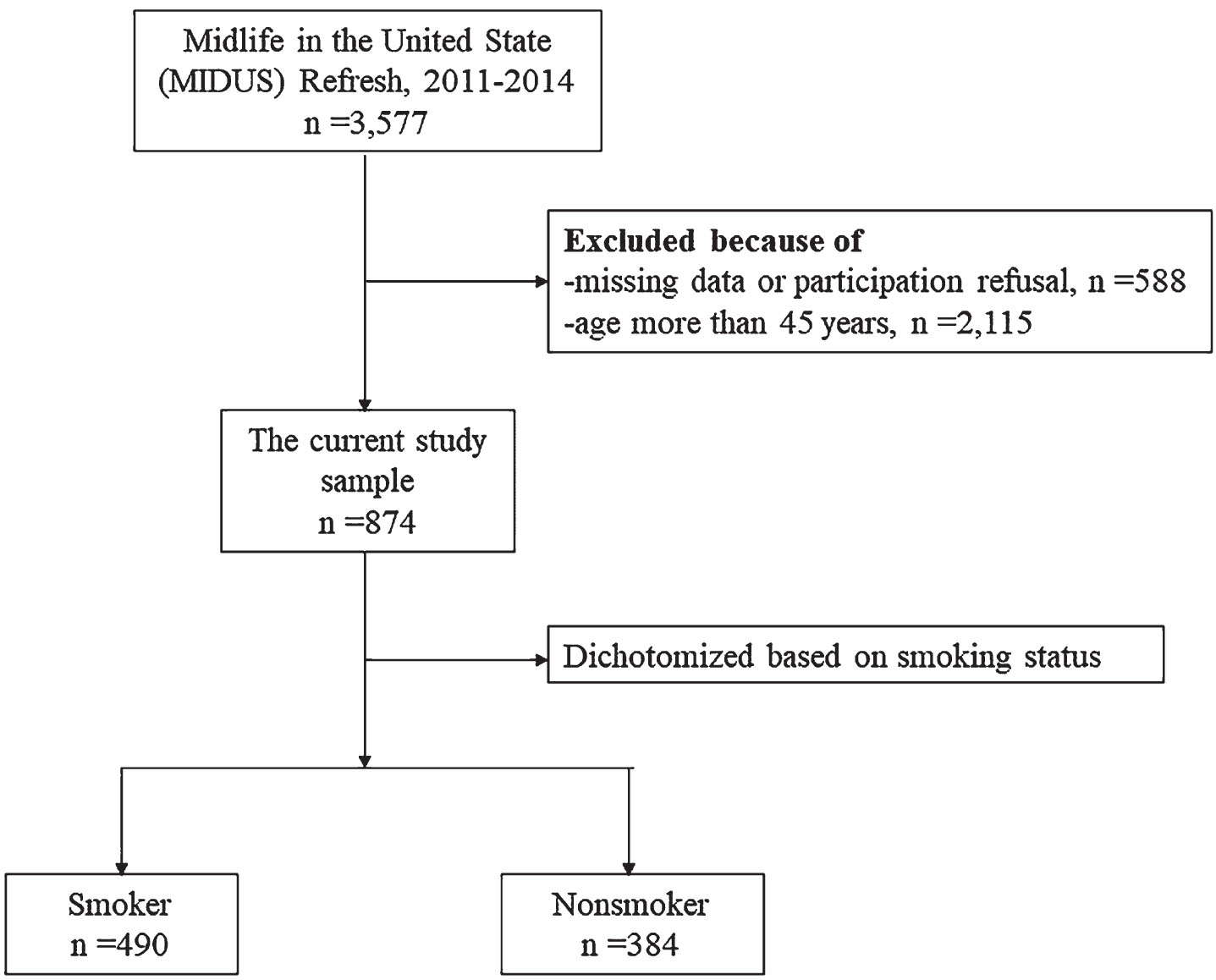
Fig. 2
Prevalence of asthma.
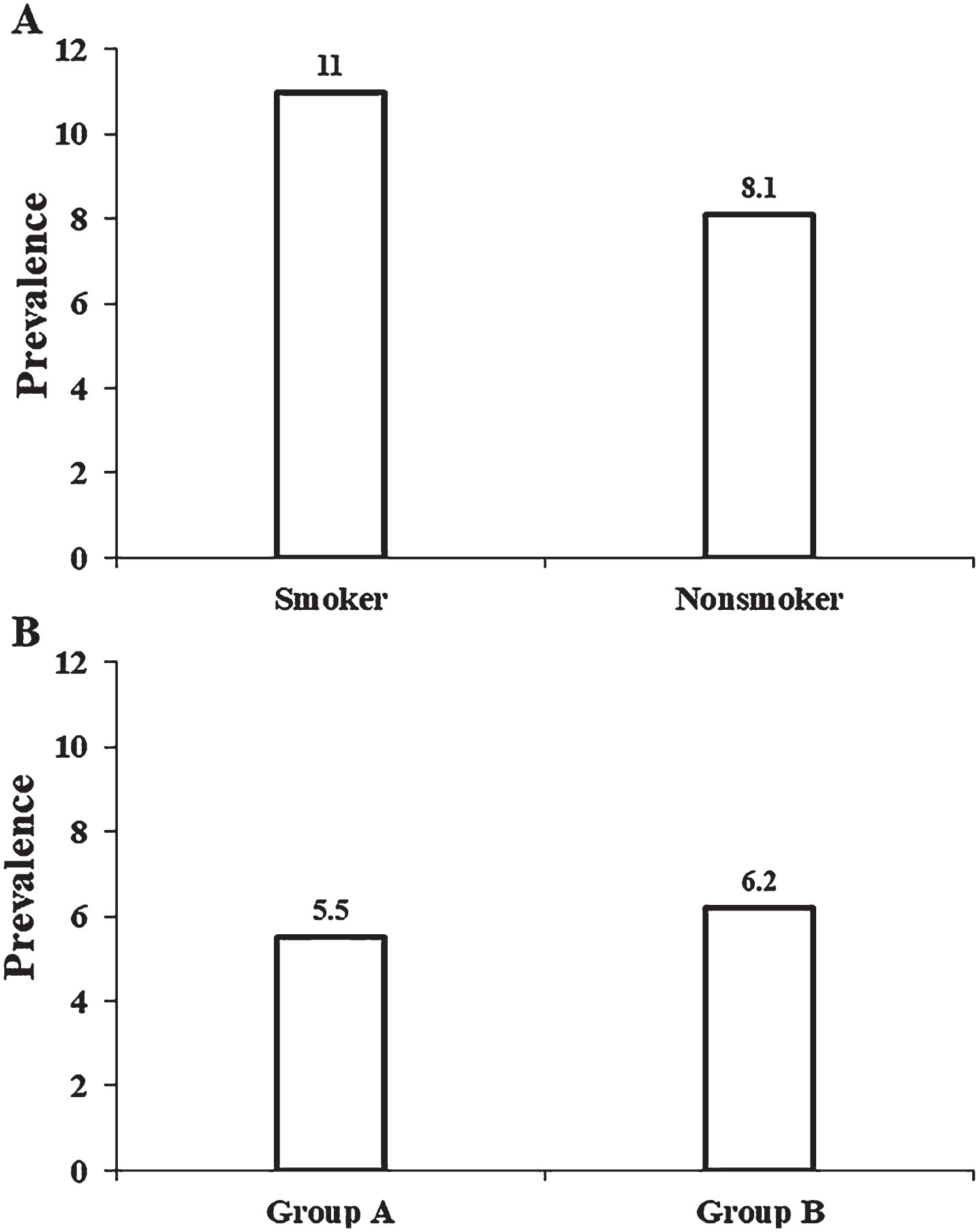
Table 1
Descriptive characteristics among adults with smoking status
| Characteristics | Smoker | Nonsmoker | P-value |
| N = 490 (56.1%) | N = 384 (43.9%) | ||
| Age in years, mean (SD) | 35.3 (5.7) | 35.9 (5.7) | .083 |
| Sex, n (%) | .814 | ||
| Male | 240 (49) | 185 (48.2) | |
| Female | 250 (51) | 199 (51.8) | |
| Race, n (%) | .511 | ||
| White | 97 (19.9) | 69 (18.1) | |
| Black/Asian | 69 (80.1) | 312 (81.9) | |
| Education, n (%) | <.0001 | ||
| High school/college | 343 (70.1) | 135 (35.2) | |
| Graduates | 146 (29.9) | 249 (64.8) | |
| Employment status, n (%) | .039 | ||
| Employed | 349 (71.4) | 297 (77.5) | |
| Unemployed | 140 (26.6) | 86 (22.5) | |
| Marital status, n (%) | <.0001 | ||
| Married | 275 (56.1) | 272 (71) | |
| Unmarried/divorced | 215 (43.9) | 111 (29) | |
| Alcohol intake, n (%) | .458 | ||
| Yes | 228 (84.8) | 234 (87) | |
| No | 41 (15.2) | 35 (13) | |
| Physical activity, n (%) | .008 | ||
| Active | 109 (40.8) | 80 (29.8) | |
| Inactive | 158 (59.2) | 188 (70.2) | |
| Body mass index, n (%) | .645 | ||
| Normal weight | 301 (61.4) | 230 (59.9) | |
| Overweight/obese | 189 (38.6) | 154 (40.1) | |
| Central obesity, n (%) | .961 | ||
| Normal | 409 (83.5) | 321 (83.6) | |
| Obese | 81 (16.5) | 63 (16.4) | |
| Joint disease, n (%) | .257 | ||
| Yes | 22 (8.4) | 15 (5.8) | |
| No | 241 (91.6) | 243 (94.2) | |
| Diabetes, n (%) | .409 | ||
| Yes | 13 (4.9) | 9 (3.5) | |
| No | 250 (95.1) | 249 (96.5) | |
| Asthma, n (%) | .263 | ||
| Yes | 29 (11) | 21 (8.1) | |
| No | 234 (89) | 237 (91.9) | |
| Cardiovascular disease, n (%) | .083 | ||
| Yes | 9 (1.8) | 2 (0.5) | |
| No | 481 (98.2) | 382 (99.5) |
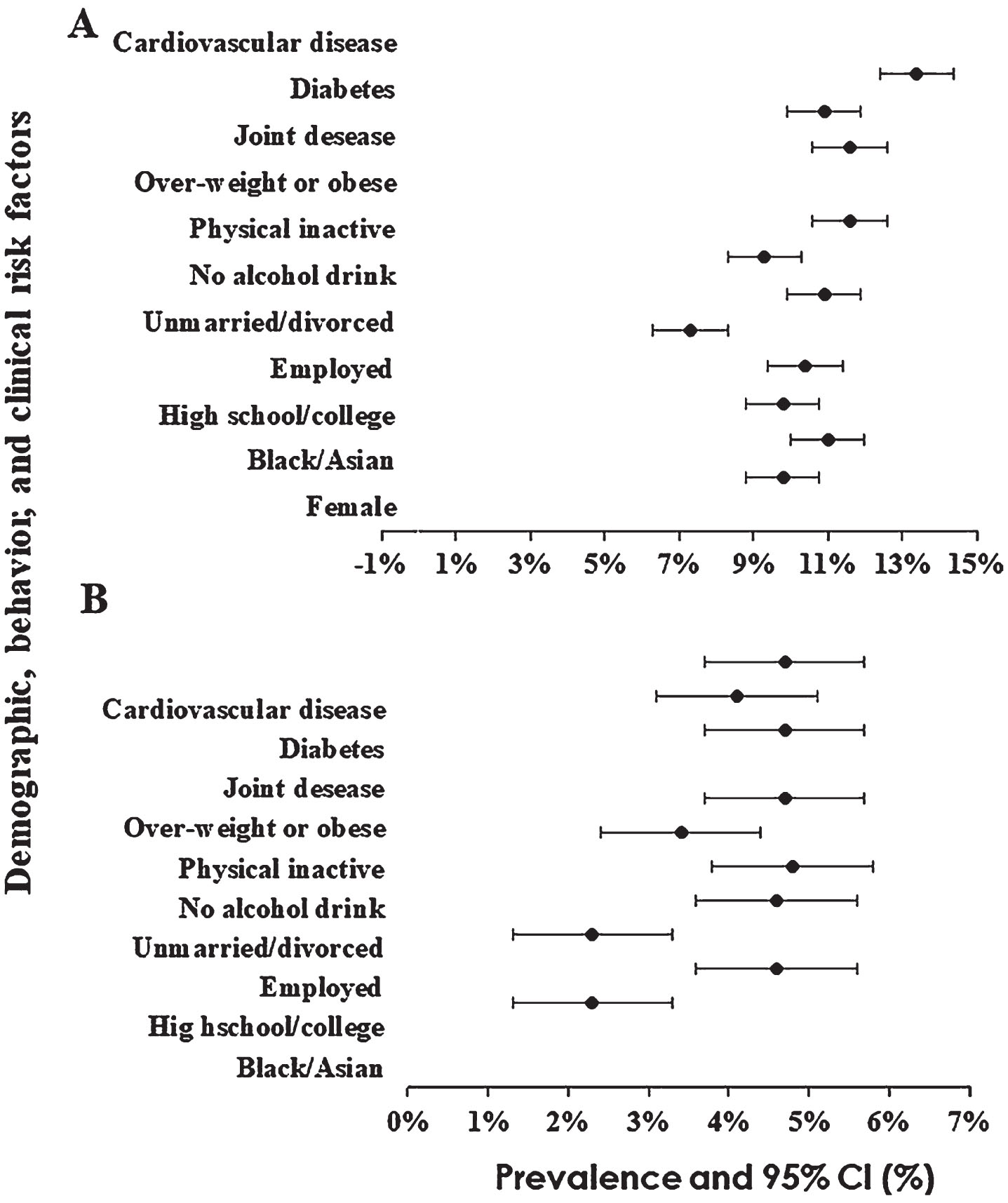
Female sex, Black race, school/college education, unmarried/divorce status, employed status, no alcohol intake, physical inactivity, obesity, diabetes, and joint diseases were significantly associated with 1- or more-fold odds of asthma. Diabetes and joint/bone diseases had two- or more-fold odds of asthma among adults who smoked (Fig. 3). The prevalence of asthma was greater (10% or more) in adult smokers who grew up living with a father or mother who had a smoking history, especially among males with a school/college education, physical inactivity, and overweight/obesity. Adult smokers -especially those with physical inactivity and overweight/obesity- were more likely to have asthma (10% or more) if they grew up living with others in the house or workplace who had a smoking history (Fig. 4).
Fig. 3
Associations of demographic, behavioral, and clinical risk factors with the risk of asthma among adults who smoked. A dark dot circle represents odds ratios, and bars show a 95% confidence interval.
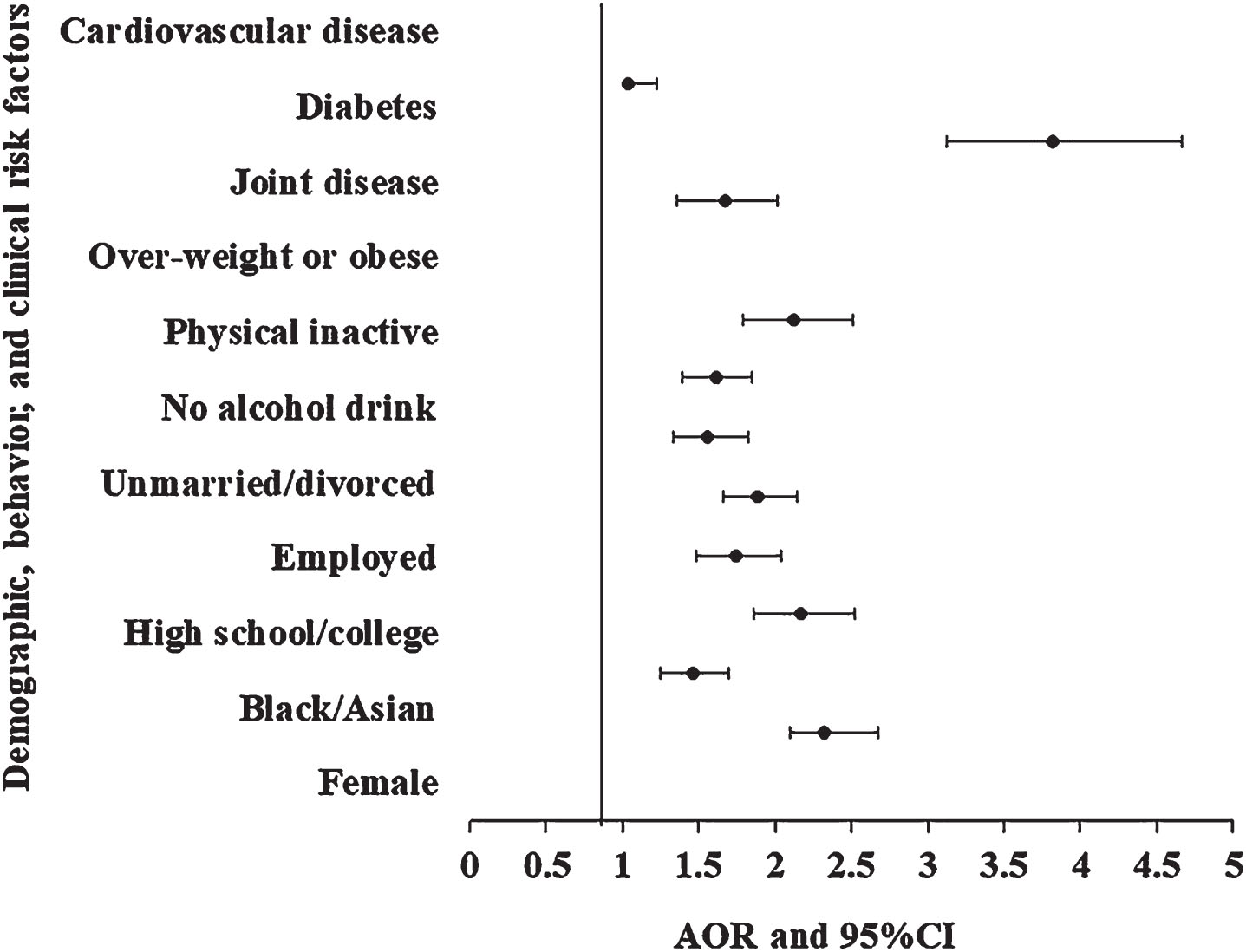
Fig. 4
Prevalence of asthma among adults who smoked according to grew up living with A) a father or mother who smoked; B) a workplace who smoked. A dark dot circle represents prevalence, and bars show a 95% confidence interval.
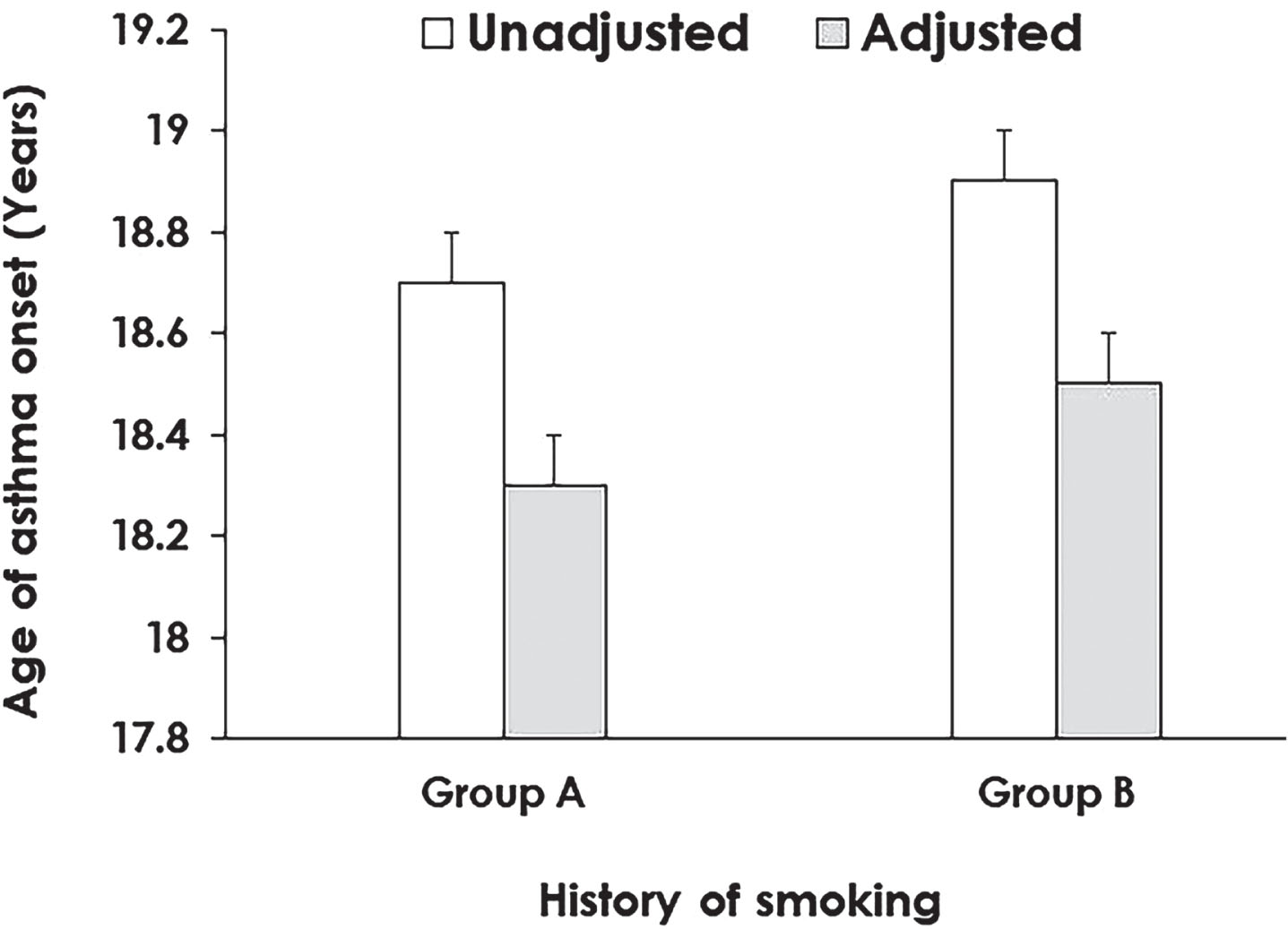
Female sex, black race, school or college education, being unmarried or divorced, being employed, having no alcohol intake, being physically inactive, being obese, having diabetes, and having joint diseases were significantly associated with 1- or more-fold odds of asthma among adults who smoked and grew up living with a father or mother who had a smoking history (Fig. 5). The mean age of asthma onset varied significantly by smoking history (18.3 years in group A and 18.5 years in group B, p = 0.021) after adjusting for covariables (Fig. 6).
Fig. 5
Associations of demographic, behavioral, and clinical risk factors with the risk of asthma among adults who smoked according to grew up living with A) a father or mother who smoked; B) other people who smoked in the workplace. A dark dot circle represents odds ratios, and bars show a 95% confidence interval.
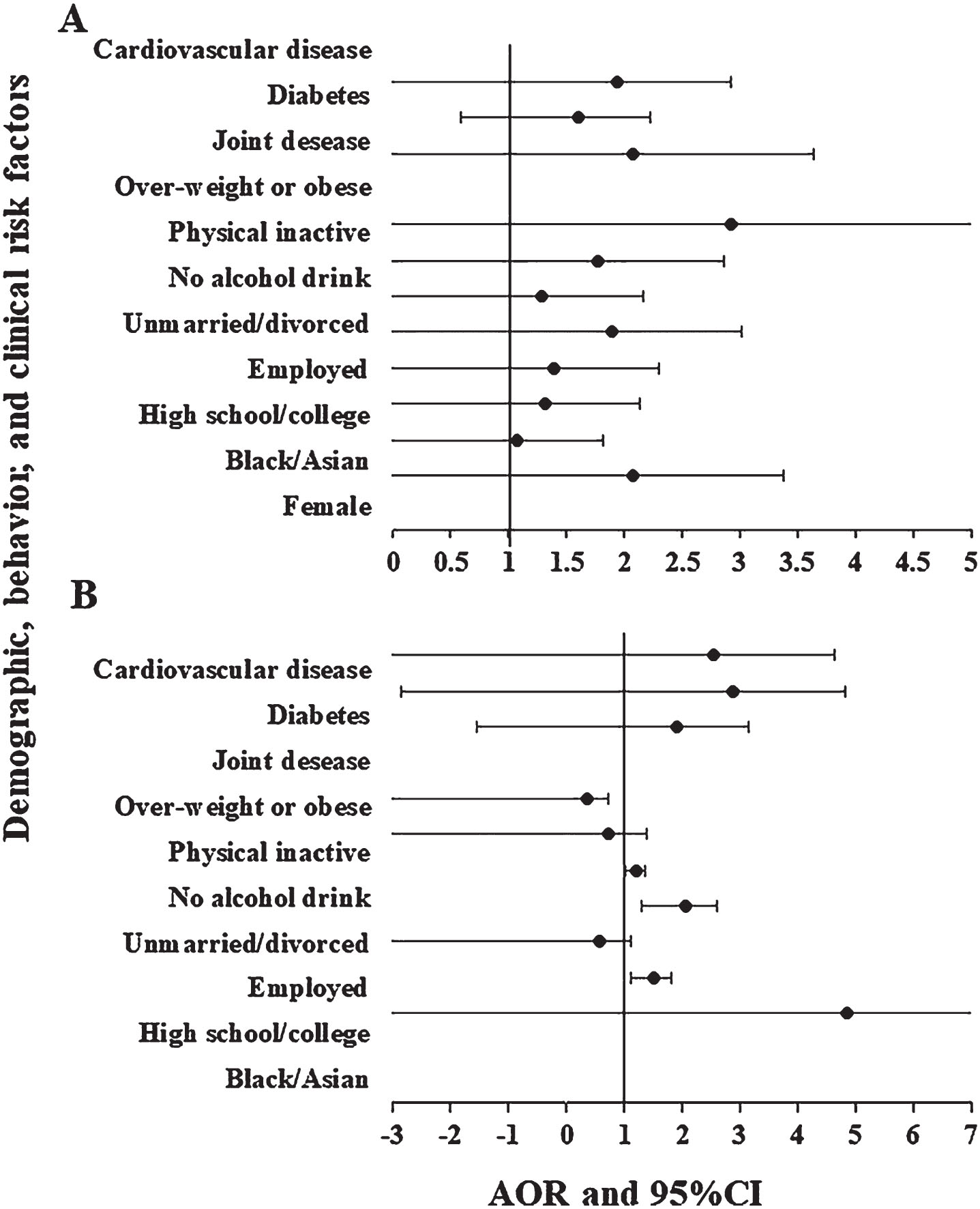
Fig. 6
The mean age of asthma onset among adults who smoked according to grew up living with A) a father or mother who smoked; B) other people who smoked in the workplace. The multiple linear regression model is adjusted for age, sex, race, educational level, employment status, marital status, alcohol intake status, physical activity status, obesity status, central obesity status, joint disease, diabetes, and cardiovascular diseases. Empty bars represent unadjusted estimates of the mean age of asthma onset; light gray bars show adjusted estimates of the mean age of asthma onset.
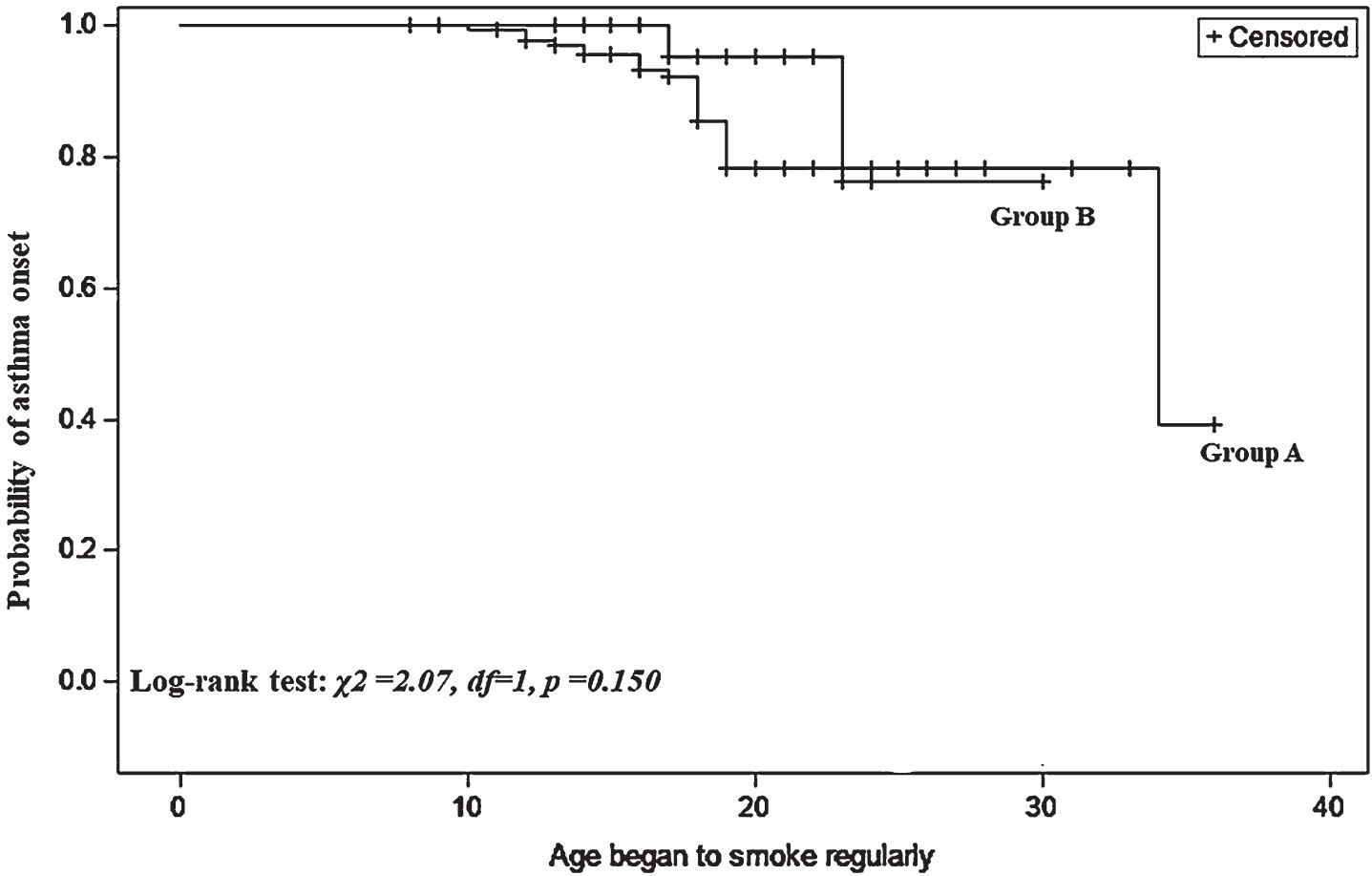
The results comparing the age at which the individual began to smoke regularly and the probability of asthma onset for groups A and B are shown in Fig. 7. The log-rank tests for homogeneity indicated no significant difference in groups regarding the age at which smoking began and asthma onset (p = 0.150). The Kaplan-Meier curve estimating the probability of asthma onset among smokers aged 30 years was about 0.8 for group B and 0.4 for group A.
Fig. 7
Kepler-Meire curve for age began to smoke regularly and probability of asthma onset among groups.
4Discussion
The results showed that female sex, black race, school or college education, unmarried or divorced status, employed status, no alcohol intake, physical inactivity, and obesity were associated with an increased risk of asthma. Moreover, adult smokers who grew up living with smokers, especially a father or mother, were at increased risk of asthma compared to workplace smoking. The mean age of asthma onset varied slightly among those living with smokers, such as a father, mother, others in the house, or colleagues at the workplace. About 60% of adult smokers who grew up with a smoking father or mother triggered asthma.
The findings of this study were broadly consistent with a previous study that showed that both parents’ smoking more than half a pack of cigarettes a day was significantly associated with a 2.9-fold risk of physician-reported asthma and a 3.3-fold risk of current asthma among participants in grade 7 [30]. Another study found that cigarette smoking was consistently associated with prevalent asthma in a sample of 57,779 adults aged 20 years or older from six geographical regions in China [21]. They also showed that a 10-year increase in age was associated with an increased risk of asthma in primary school graduates or those without formal education. A possible trigger of asthma among smokers might be the increase in T-lymphocytes, mostly CD8 cells and macrophages within the airway wall, and the infiltration of mononuclear cells and macrophages into the peripheral airways [8, 31]. A recent study revealed that children for whom both parents smoked had the highest urine 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol and cotinine concentrations [32, 33]. A review suggested an increased risk for respiratory illness-related absences from school in children with asthma who were exposed to multiple household smokers.
Similar to the present study’s findings, previous research showed that female sex, black race, an annual family income < $50,000, physical inactivity, and obesity were individually associated with increased risk of asthma development, especially in US children, adolescents, and adults [34]. One possible reason for this finding may be the failure to reach the recommended level of 15 or more minutes of moderate activity five or more days per week, as per the Centers for Disease Control [34]. However, our educational finding was somewhat contradictory to an earlier US study, which showed that higher academic degrees had been achieved by individuals with asthma than those without asthma [35].
Alcohol contains histamines and sulfites, which are known to exacerbate asthma symptoms in certain people [36]. It’s crucial to keep in mind that not everyone who consumes alcohol experiences the development or exacerbation of their asthma [37]. According to a previous study, consuming wine is related to a lower risk of developing asthma, which suggests that it may even help prevent asthma [38]. The finding of this study that there was no association between alcohol consumption and the risk of developing asthma could be explained by potential residual confounding, such as socioeconomic or lifestyle factors. Therefore, this finding from the present study can raise doubt on the idea that drinking alcohol increases asthma risk.
Although the relationship between diabetes and asthma in adults has not been thoroughly investigated, one study found that type 1 diabetes was associated with a significantly higher incidence of asthma in patients aged < 8 years than in the general population [39]. That study provided a possible explanation for the association between diabetes and asthma onset at the pathophysiological level. Another study found that asthma onset was higher among adults with either type 1 or 2 diabetes than those without diabetes [40]. This risk of asthma onset in those with type 2 diabetes might be due to obesity, insulin resistance, or metabolic syndrome [41, 42]. Some studies found that arthritis was associated with a higher risk of asthma [43].
It’s interesting to note that a recent study [44] contradicts the current study’s finding that adult smokers who are single or divorced are much more likely to develop asthma. Asthma sufferers were shown to have higher rates of alcohol usage as they aged, according to another conclusion from the prior study [45]. The results of this investigation contradict this finding. Geographical variation and various populations may be a factor in this finding’s explanation.
The primary strength of this study was the larger sample size, with more than 80% power, which showed a statistically significant relationship. However, this study also had some limitations. The first limitation was self-reported questionnaires. The results may have been biased by self-reported asthma, leading to recall bias and misclassification. Second, the cross-sectional design of this study somewhat limited the associations between sociodemographic, behavioral, and clinical factors with asthma risk in adult smokers [46]. Third, the history of the smoking measure was valid to use with parents, others in the house, and colleagues at the workplace. Fourth, the method used for participants’ smoking status categorization could be misleading, as it neglects any effect of the degree of smoke exposure in ex-smokers and current smokers. Finally, data on the quantity of smoking, medication for asthma, type and quantity of alcohol intake, severity, and family history of asthma were not available, which would have been useful in our study.
While asthma is not yet curable, symptoms can typically be improved by identifying triggers. Adjustable triggers, such as cigarette smoking and exposure to parental smoking, are significant for asthma prevention [47, 48]. Additionally, the effectiveness of medications may be reduced by cigarette smoking or passive smoking [49]. Therefore, the harmful effects of passive smoking show the need for maintaining a smoke-free environment [50]. Comprehensive national anti-smoking policies are needed to achieve this favored environment; laws that limit smoking decrease the number of people hospitalized for asthma [51]. In addition, a prior study showed that a long-term, multi-component program for workplace health promotion could alter smoking behavior, attitudes about smoking, and preparedness to stop smoking [52].
Our findings could help provide patient education, one of the four essential components of asthma management, including monitoring symptoms and lung function, controlling triggering factors and comorbid conditions, and providing pharmacologic therapy [53]. Since asthma severity varies among people depending on socioeconomic, behavioral, and clinical characteristics, patient education and physical exercise are essential for decreasing asthma exacerbations and improving the control [54, 55]. Thus, expert panel reports three and Global Initiative for Asthma has described a stepwise treatment approach and strategy to prevent future risks of asthma onset [56]. Since most workplaces have anti-smoking regulations, they might be applicable to the likelihood that secondhand smoke exposure occurs within prohibited smoking areas. However, despite the implementation of the smoking prohibition policy at work, evidence from a recent evaluation suggests that a number of employees are still suffering from the effects of secondhand smoke [57]. This shows that there is still a knowledge, attitude, and practice gap among non-smokers when it comes to enhancing the smoke-free workplace policy.
5Conclusions
Being female, black, having a school/college education, unmarried or divorced, employed, having no alcohol intake, physically inactive, obese, having diabetes, and having a joint disease was associated with asthma risk among adults who smoked. Moreover, smoking adults who grew up living with smokers, especially a father or mother, were at increased risk of asthma compared to workplace smoking. These results suggest that parental smoking history is one of several critical modifiable triggers for populations at risk for asthma. However, more empirical evidence is needed to use familial smoking history as a tool for the early diagnosis and management of asthma. Further evidence is also required to determine whether the use of parental smoking history for identifying patients at high risk for asthma will lead to an overall reduction in the rates of asthma-related morbidity and mortality.
Ethical approval
Since a secondary analysis was conducted utilizing the initial data from the MIDUS refresher, the current study does not need institutional review board approval. No personal information is included in the data and appropriate coding makes it impossible to obtain the codes, both of which preclude retrieval of the data.
Informed consent
This study did not require informed consent because it did not involve any human subjects.
Conflict of interest
None to report.
Acknowledgments
The author extends his appreciation to the Deputyship for Research and Innovation, “Ministry of Education” in Saudi Arabia for funding this research.
Funding
The Deputyship for Research and Innovation, “Ministry of Education” in Saudi Arabia funded this research work through project no. IFKSUOR3-394-1.
References
[1] | Broaddus VC , Ernst JD , King TE Jr , Lazarus SC , Sarmiento KF , Schnapp LM , , et al. Murray & Nadel’s textbook of respiratory medicine e-book: Elsevier Health Sciences; 2021. |
[2] | Joao C , Jacome C , Brito D , Teixeira P , Quelhas-Santos J , Amorim L , et al. Prevalence and Characterisation of Patients with Asthma According to Disease Severity in Portugal: Findings from the EPI-ASTHMA Pilot Study. J Asthma Allergy. (2022) ;15: :1441–53. |
[3] | To T , Stanojevic S , Moores G , Gershon AS , Bateman ED , Cruz AA , et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. (2012) ;12: :1–8. |
[4] | Guo Z , Qin X , Pate CA , Zahran HS , Malilay J . Asthma Among Adults and Children by Urban-Rural Classification Scheme, United States, 2016-2018. Public Health Rep. (2022) ;137: (6):1100–6. |
[5] | Bloom CI , Saglani S , Feary J , Jarvis D , Quint JK . Changing prevalence of current asthma and inhaled corticosteroid treatment in the UK: population-based cohort 2006-2016. Eur Respir J. (2019) ;53: (4). |
[6] | Li Y , Dai Y , Guo Y . The pulmonary damage caused by smoking: A longitudinal study. Technol Health Care. (2018) ;26: (S1):501–7. |
[7] | Lorensia A , Muntu CM , Suryadinata RV , Septiani R . Effect of lung function disorders and physical activity on smoking and non-smoking students. J Prev Med Hyg.. (2021) ;62: (1):E89–E96. |
[8] | Castillo JR , Peters SP , Busse WW . Asthma Exacerbations: Pathogenesis, Prevention, and Treatment. J Allergy Clin Immunol Pract. (2017) ;5: (4):918–27. |
[9] | Corleis B , Cho JL , Gates SJ , Linder AH , Dickey A , Lisanti-Park AC , et al. Smoking and Human Immunodeficiency Virus 1 Infection Promote Retention of CD8(+) T Cells in the Airway Mucosa.. Am J Respir Cell Mol Biol. (2021) ;65: (5):513–20. |
[10] | Masunaga A , Takemura T , Ichiyasu H , Migiyama E , Horio Y , Saeki S , et al. Pathological and clinical relevance of selective recruitment of Langerhans cells in the respiratory bronchioles of smokers. Respir Investig. (2021) ;59: (4):513–21. |
[11] | Kamga A , Rochefort-Morel C , Guen YL , Ouksel H , Pipet A , Leroyer C . Asthma and smoking: A review. Respir Med Res. (2022) ;82: :100916. |
[12] | Khan AH , Gray C , Eckert L , Amand C , Maroni J , Wang Z , et al. Impact of Baseline Lung Function on Future Exacerbations in Patients with Moderate-to-Severe Asthma. J Asthma Allergy. (2022) ;15: :1639–44. |
[13] | Bao Y , Chen Z , Liu E , Xiang L , Zhao D , Hong J . Risk Factors in Preschool Children for Predicting Asthma During the Preschool Age and the Early School Age: a Systematic Review and Meta-Analysis. Curr Allergy Asthma Rep. (2017) ;17: (12):85. |
[14] | Deng X , Thurston G , Zhang W , Ryan I , Jiang C , Khwaja H , et al. Application of data science methods to identify school and home risk factors for asthma and allergy-related symptoms among children in New York. Sci Total Environ. (2021) ;770: :144746. |
[15] | Adzrago D , Nyarko SH , Ananaba N , Asare M , Odame E , Jones A , et al. Between and Within Sexual Identity-Group Differences in Asthma Prevalence in the United States. Respir Care. (2022) ;67: (3):331–8. |
[16] | Yawn BP , Rank MA , Bertram SL , Wollan PC . Obesity, low levels of physical activity and smoking present opportunities for primary care asthma interventions: an analysis of baseline data from The Asthma Tools Study. NPJ Prim Care Respir Med. (2015) ;25: (1):1–7. |
[17] | He Z , Wu H , Zhang S , Lin Y , Li R , Xie L , et al. The association between secondhand smoke and childhood asthma: A systematic review and meta-analysis. Pediatr Pulmonol. (2020) ;55: (10):2518–31. |
[18] | Soleimani F , Dobaradaran S , De-la-Torre GE , Schmidt TC , Saeedi R . Content of toxic components of cigarette, cigarette smoke vs cigarette butts: A comprehensive systematic review. Sci Total Environ. (2022) ;813: :152667. |
[19] | Harju M , Keski-Nisula L , Georgiadis L , Heinonen S . Parental smoking and cessation during pregnancy and the riskof childhood asthma. BMC Public Health. (2016) ;16: :428. |
[20] | Urrutia-Pereira M , Chong-Neto H , Mocellin LP , Ellwood P , Garcia-Marcos L , Simon L , et al. Prevalence of asthma symptoms and associated factors in adolescents and adults in southern Brazil: A Global Asthma Network Phase I study. World Allergy Organ J. (2021) ;14: (3):100529. |
[21] | Huang K , Yang T , Xu J , Yang L , Zhao J , Zhang X , et al. Prevalence, risk factors, and management of asthma in China: a national cross-sectional study. Lancet. (2019) ;394: (10196):407–18. |
[22] | Stokes JE . Social Integration, Daily Discrimination, and Biological Markers of Health in Mid- and Later Life: Does Self-Esteem Play an Intermediary Role? Innov Aging. (2020) ;4: (4):igaa026. |
[23] | Dienberg Love G , Seeman TE , Weinstein M , Ryff CD . Bioindicators in the MIDUS national study: protocol, measures, sample, and comparative context. J Aging Health. (2010) ;22: (8):1059–80. |
[24] | Wang M , Wang JW , Cao SS , Wang HQ , Hu RY . Cigarette Smoking and Electronic Cigarettes Use: A Meta-Analysis. Int J Environ Res Public Health. (2016) ;13: (1):120. |
[25] | de Souto Barreto P , Cesari M , Andrieu S , Vellas B , Rolland Y . Physical Activity and Incident Chronic Diseases: A Longitudinal Observational Study in 16 European Countries. Am J Prev Med. (2017) ;52: (3):373–8. |
[26] | Gomes M , Figueiredo D , Teixeira L , Poveda V , Paul C , Santos-Silva A , et al. Physical inactivity among older adults across Europe based on the SHARE database. Age Ageing. (2017) ;46: (1):71–7. |
[27] | Farrington CP , Manning G . Test statistics and sample size formulae for comparative binomial trials with null hypothesis of non-zero risk difference or non-unity relative risk. Stat Med. (1990) ;9: (12):1447–54. |
[28] | Hanusz Z , Tarasińska J . Normalization of theKolmogorov–Smirnov and Shapiro–Wilk tests ofnormality. Biometrical Letters. (2015) ;52: (2):85–93. |
[29] | De Rooij M , Anderson CJ . Visualizing, summarizing, and comparing odds ratio structures. Methodology: European Journal of Research Methods for the Behavioral and Social Sciences. (2007) ;3: (4):139. |
[30] | Hu FB , Persky V , Flay BR , Richardson J . An epidemiological study of asthma prevalence and related factors among young adults. J Asthma. (1997) ;34: (1):67–76. |
[31] | Dey S , Eapen MS , Chia C , Gaikwad AV , Wark PAB , Sohal SS . Pathogenesis, clinical features of asthma COPD overlap, and therapeutic modalities. Am J Physiol Lung Cell Mol Physiol. (2022) ;322: (1):L64–L83. |
[32] | Jeong SH , Jang BN , Kang SH , Joo JH , Park EC . Association between parents’ smoking status and tobacco exposure in school-age children: assessment using major urine biomarkers. Sci Rep. (2021) ;11: (1):4536. |
[33] | Baos S , Cremades-Jimeno L , Lopez-Ramos M , de Pedro MA , Uriarte SA , Sastre J , et al. Expression of Macrophage Scavenger Receptor (MSR1) in Peripheral Blood Cells from Patients with Different Respiratory Diseases: Beyond Monocytes. J Clin Med. (2022) ;11: (5). |
[34] | Yawn BP , Rank MA , Bertram SL , Wollan PC . Obesity, low levels of physical activity and smoking present opportunities for primary care asthma interventions: an analysis of baseline data from The Asthma Tools Study. NPJ Prim Care Respir Med. (2015) ;25: :15058. |
[35] | Mazurek JM , Schleiff PL , Henneberger PK . Is childhood asthma associated with educational level and longest-held occupation? Am J Epidemiol. (2012) ;175: (4):279–88. |
[36] | Vally H , de Klerk N , Thompson PJ . Alcoholic drinks: important triggers for asthma. J Allergy Clin Immunol. (2000) ;105: (3):462–7. |
[37] | Skaaby T , Kilpelainen TO , Taylor AE , Mahendran Y , Wong A , Ahluwalia TS , et al. Association of alcohol consumption with allergic disease and asthma: a multi-centre Mendelian randomization analysis. Addiction. (2019) ;114: (2):216–25. |
[38] | Lieberoth S , Backer V , Kyvik KO , Skadhauge LR , Tolstrup JS , Gronbaek M , et al. Intake of alcohol and risk of adult-onset asthma. Respir Med. (2012) ;106: (2):184–8. |
[39] | Hsiao YT , Cheng WC , Liao WC , Lin CL , Shen TC , Chen WC , et al. Type 1 Diabetes and Increased Risk of Subsequent Asthma: A Nationwide Population-Based Cohort Study. Medicine (Baltimore). (2015) ;94: (36):e1466. |
[40] | Ehrlich SF , Quesenberry CP Jr , Van Den Eeden SK , Shan J , Ferrara A . Patients diagnosed with diabetes are at increased risk for asthma, chronic obstructive pulmonary disease, pulmonary fibrosis, and pneumonia but not lung cancer. Diabetes Care. (2010) ;33: (1):55–60. |
[41] | Serafino-Agrusa L , Spatafora M , Scichilone N . Asthma and metabolic syndrome: Current knowledge and future perspectives. World J Clin Cases. (2015) ;3: (3):285–92. |
[42] | Rayner L , McGovern A , Creagh-Brown B , Woodmansey C , de Lusignan S . Type 2 Diabetes and Asthma: Systematic Reviewof the Bidirectional Relationship. Curr Diabetes. (2019) ;15: (2):118–26. |
[43] | Kim SY , Min C , Oh DJ , Choi HG . Increased risk of asthma in patients with rheumatoid arthritis: A longitudinal follow-up study using a national sample cohort. Sci Rep. (2019) ;9: (1):6957. |
[44] | Chen Z , Wasti B , Shang Y , Ouyang R , Yuan Y , He Y , et al. Different clinical characteristics of current smokers and former smokers with asthma: a cross-sectional study of adult asthma patients in China. Sci Rep. (2023) ;13: (1):1035. |
[45] | Dowdell EB , Posner MA , Hutchinson MK . Cigarette Smoking and Alcohol Use among Adolescents and Young Adults with Asthma. Nurs Res Pract. (2011) ;2011: 503201. |
[46] | Spector PE . Do not cross me: Optimizing the use of cross-sectional designs. Bus Psychol. (2019) ;34: (2):125–37. |
[47] | Henneberger PK . Work-exacerbated asthma. Curr Opin Allergy Clin Immunol. (2007) ;7: (2):146–51. |
[48] | Thomson NC , Spears M . The influence of smoking on the treatment response in patients with asthma. Curr Opin Allergy Clin Immunol. (2005) ;5: (1):57–63. |
[49] | Stapleton M , Howard-Thompson A , George C , Hoover RM , Self TH . Smoking and asthma. J Am Board Fam Med. (2011) ;24: (3):313–22. |
[50] | Landers G . The impact of smoke-free laws on asthma discharges: a multistate analysis. Am J Public Health. (2014) ;104: (2):e74–9. |
[51] | Been JV , Nurmatov UB , Cox B , Nawrot TS , van Schayck CP , Sheikh A . Effect of smoke-free legislation on perinatal and child health: a systematic review and meta-analysis. Lancet. (2014) ;383: (9928)1549–60. |
[52] | Mache S , Vitzthum K , Groneberg DA , Harth V . Effects of a multi-behavioral health promotion program at worksite on smoking patterns and quit behavior. Work. (2019) ;62: (4):543–51. |
[53] | Janson SL , McGrath KW , Covington JK , Cheng SC , Boushey HA . Individualized asthma self-management improves medication adherence and markers of asthma control. J Allergy Clin Immunol. (2009) ;123: (4):840–6. |
[54] | Zhu Q , Zhu J , Wang X , Xu Q . A Meta Analysis of Physical Exercise on Improving Lung Function and Quality of Life Among Asthma Patients. J Asthma Allergy. (2022) ;15: :939–55. |
[55] | Rumrill PD , Romeo JM , Wickert K , Sheppard-Jones K , Park S , Souders J . Providing quality employment services to people living with asthma in the vocational rehabilitation program: A model for meeting the needs of an emerging clientele. Work. (2023) ;75: (2):367–74. |
[56] | Haselkorn T , Fish JE , Zeiger RS , Szefler SJ , Miller DP , Chipps BE , et al. Consistently very poorly controlled asthma, as defined by the impairment domain of the Expert Panel Report 3 guidelines, increases risk for future severe asthma exacerbations in The Epidemiology and Natural History of Asthma: Outcomes and Treatment Regimens (TENOR) study. J Allergy Clin Immunol.. (2009) ;124: (5):895–902. e4. |
[57] | Rashiden I , Ahmad Tajuddin N , Yee A , Zhen STE , Bin Amir Nordin AS . The efficacy of smoking ban policy at the workplace on secondhand smoking: systematic review and meta-analysis. Environ Sci Pollut Res Int. (2020) ;27: (24):29856–66. |


