
Perceived health and productivity when working from home during the COVID-19 pandemic
Abstract
BACKGROUND:
During the COVID-19 pandemic, office workers were obliged to work from home (WFH). Alongside known positive aspects of home-based telework, it is associated with reduced health and productivity impacts. Its success depends on employee and environmental characteristics.
OBJECTIVE:
This paper fills the gap in knowledge on the mediating role of health between personal and environmental factors and employee productivity, when obliged to work from home full-time. It covers health in full (physical, mental, and social) unlike other WFH studies.
METHODS:
Two large survey-based datasets (gathered April 27th - November 20th, 2020) were analysed resp. with a path model and descriptive analyses. The data provide experiences on health and productivity of resp. 25,058 and 18,859 Dutch office workers from different public organisations, who were obliged to work from home during the COVID-19 lockdowns.
RESULTS:
In general, the workers in the sample perceived their health to be quite good. Path analysis revealed that gender, age, education, the at-home workspace, the presence of children in the household, and perceived organisational support were significantly related to self-perceived productivity. However, most of these effects were found to be mediated by physical, mental, and/or social health indicators. Possible explanations for health issues from the descriptive analyses were sedentary behaviour, unsuitable furniture, having to be at home, social isolation and changed content and frequency of contact with colleagues.
CONCLUSION:
Findings imply that specifically engagement and organisational support of teleworkers are most relevant to steer on to ensure productivity while WFH.
1Introduction
Working from home (WFH) had not yet seen such a rise as in 2020, when it peaked all over the world as a result of the COVID-19 pandemic [1]. At first, WFH during the COVID-19 pandemic was well-received by most workers. However, as time went on, debates about not needing an office anymore shifted to expectations for a more ‘hybrid’ future working mode for office workers [e.g. 2]. A hybrid working mode expects employees to work partly in the office and partly at home or third places. Pre-Covid research on teleworking (a term used for WFH since first attempts to do so in the seventies increased during the nineties) revealed advantages and disadvantages for both the individual worker and for the company as a whole [1], such as positive effects on productivity [3], job satisfaction and morale [4], organisational commitment [5], and flexibility [6]. Also downfalls were identified, such as reduced career progression [7], increased social isolation [8], reduced organisational support [9], increased presenteeism [10], a blurring of work-life boundary [8], and several other health effects [e.g. 3, 10–12].
The occupational health of employees is very important as it relates to absenteeism, presenteeism, quality of life, job satisfaction, employee morale, and staff retention [e.g. 13–15]. At the turn of the century, it already became clear that WFH is particularly beneficial for employee health and performance when one can self-select whether you want to WFH, based on your personal preferences and circumstances [11]. Voluntary teleworkers can return to the office when dissatisfied with WFH conditions. Moreover, other instances of self-selection were found around that time, such as that family-orientated employees were more drawn to WFH for the ability to spend more time with family and take care of them [16, 17]. Also, workers with suitable at-home workspaces and sufficient social support were more likely to choose WFH, compared to those who did not [18, 19]. Unfortunately, during the COVID-19 pandemic employees did not have such luxury to return to the office when dissatisfied with WFH. Without this concept of self-selection, (some of) these employees might be ill-equipped for WFH through having no suitable workspace at home or other poor work conditions. As put forward by Bouziri et al. [20], this might make findings from pre-COVID research on health effects of WFH less applicable to the COVID-19 situation, and thus perhaps also for future hybrid working if WFH becomes the new norm instead of a voluntary option. In addition, during the pandemic people had to work fully from home, while studies have shown that especially people with a high intensity of WFH (=number of office hours versus WFH) have higher predicted health risks [21, 22] and less health benefits [23] than those WFH incidentally or only 1-2 days a week. In fact, Henke et al. [21] identified a U-shaped relationship between WFH intensity and health. So, both the high intensity and the non-voluntary nature of WFH in relation to health and productivity outcomes are research gaps addressed with his study, to prepare better for future hybrid workingmodes.
Furthermore, the World Health Organisation’s [24] definion of ‘health’ is “... a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”. However, a recent systematic review of existing WFH-health studies during COVID-19 by [25] identified only 11 studies of office workers WFH full-time (and 2 studies of teachers). These existing studies focussed only on physical health [e.g. 26–29], only on mental health [30–35], or on both [36–39], but none included social health as well, which is thus a second contribution of this study.
A third novelty is the identification of a mediating role of health issues in the relationships between personal and environmental characteristics and productivity. Several studies have identified the significance of both personal and environmental characteristics for positive health outcomes of WFH [e.g. 3, 5, 8, 11, 12, 19]. However, so far only Seva et al. [39] considered a mediating role of health in the effect of environmental characteristics on health while WFH. Their sample was small (n = 352), mental health was measured with stress only, and no personal characteristics were included in their structural equation modelling approach. So, the broader approach of this paper adds value to existing research, by studying all three types of health, productivity, and WFH effects from environmental and personal characteristics in a holistic conceptual model (see Fig. 1) in a full-time non-voluntary WFH context.
Fig. 1
Preliminary conceptual model.
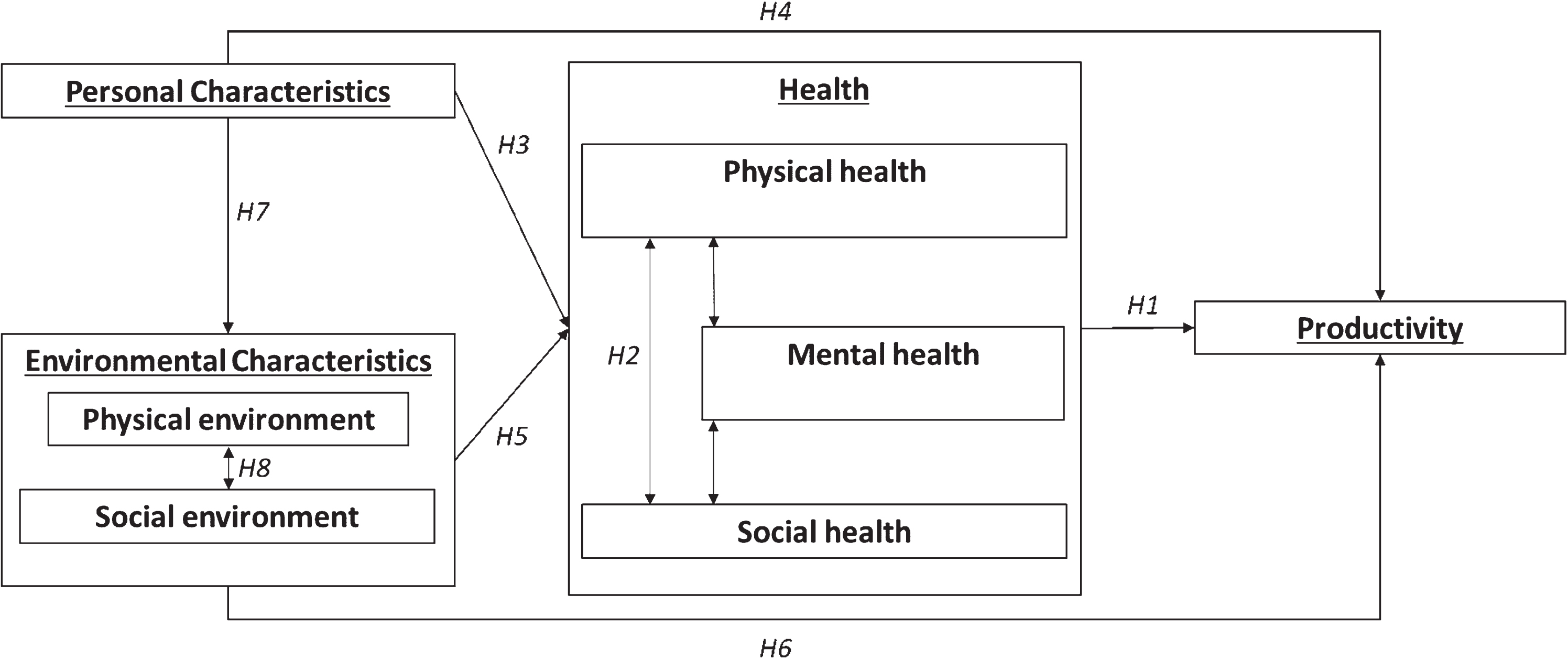
The next section explains why it is hypothesized that personal characteristics (i.e. gender and age) and environmental characteristics (i.e. the physical home environment) affect the perceived physical, mental and social health of those WFH. And why, consequently it is expected that the productivity of those WFH is affected by health, but also directly and indirectly by personal and environmentalcharacteristics.
2Occupational health and the home work environment
Taking the World Health Organisation’s health definition as a framework, this section reviews literature to pose the underlying hypotheses of Fig. 1 between productivity, physical, mental, and social health, and personal and environmental characteristics.
2.1Employee productivity and health when WFH
The general consensus of WFH is that those workers tend to show higher productivity than in traditional offices due to fewer interruptions and distractions, longer working hours, better use of high productivity moments, and increased enjoyment due to flexibility [10]. A large-scale experiment by Bloom et al. [3] even revealed a 13% increase in employee productivity from WFH compared to office workers. However, about 9% of this increase in productivity was from employees working more minutes of their shift period, including fewer breaks and sick days, and only about 4% from a higher performance per minute. Nakrošiene et al. [12] support this finding, discussing how the increase in (self-reported) productivity could be explained by a decreased time in communicating with co-workers. In addition, Hoornweg et al. [22] revealed that low WFH intensity was associated with slightly higher levels of individual productivity, while higher levels of WFH (8 or more hours per week) showed significantly lower productivity levels. Therefore, an (inverted) U-shaped relationship between WFH intensity and productivity has been suggested, suggesting that full-time working from home during lockdowns could harm productivity. But so far, studies on WFH and productivity are still in its infancy [40]. When looking at health effects on productivity, participants with more health-risk factors reported greater productivity loss than those with fewer health risks [41]. Also, the quality and quantity of work were affected when working while sick [42], which is less clear for team managers when people are WFH. In addition, research [e.g. 43, 44] has shown that physical and mental health are related in several ways, although this is not known to its full extent yet. Therefore, we pose:
H1: Employee productivity is related to their health when WFH
H2: Physical, mental, and social health indicators are interrelated
2.2Personal characteristics and health and productivity when WFH
As mentioned in the introduction, previous research has also revealed a direct significance of personal and environmental characteristics concerning WFH outcomes. For example, older workers were found to have fewer advantages of WFH [12]. In addition, education and job role are relevant. Pre-COVID, those WFH mostly consisted of either mid-level or highly educated professionals [45, 46]. Education level is also related to health [47]. Regarding job role, suitable jobs for WFH are those that involve a certain degree of autonomy, intrinsic motivation, and long periods of quiet concentration, as well as communication needs that can be met through existing technologies [48]; the latter having increased a lot since 1998. Findings on gender differences are ambiguous so far [12]. Besides demographics and job related aspects, worker behaviour at home is important. Those WFH take fewer health breaks (e.g. informal socializing with colleagues) which are important for musculoskeletal relaxation [10]. Therefore, physical activity and sedentary behaviour are important indicators of musculoskeletal health. Personal characteristics, such as gender and age, are also indicative in the way individuals perform [e.g. 5, 8, 11, 18, 19]. We pose:
H3: Personal characteristics are related to employee health when WFH
H4: Personal characteristics are related to employee productivity when WFH
2.3Environmental characteristics and health and productivity when WFH
An extensive literature review of WFH and its effects on health by Tavares [10] identified that physical health issues resulting from WFH are often related to working long hours behind a computer with poor ergonomics. For example, an unsuitable chair or desk can cause poor posture, which could prove harmful in the long run [10, 49, 50]. In addition, working in common areas in the house is shown to make work activities too permeable to interruptions, and makes it difficult to set a clear boundary between work-time and personal-time [11]. Other physical health problems resulting from the workspace are often classified as Sick Building Syndrome (SBS)-related health problems [51]. Feelings of ill-health caused by SBS include dizziness, nausea, headaches, irritation of the eyes, nose and/or throat, concentration problems, and fatigue, among others [51]. Despite being called an ‘office illness’ [52], it is also possible to suffer from SBS symptoms at home. The European Foundation for the Improvement of Living and Working Conditions [53] analysed the differences in health problems per work arrangement and found that 60% of individuals WFH parttime reported headaches and eyestrain. In comparison, only 30–40% of workers in the traditional office reported the same physical health problems. Furthermore, the share of workers reporting headaches and eyestrain decreased when the WFH intensity decreased.
A recent literature review on physical and mental health effects of working at home by [54] found that effects of WFH depend on various aspects, such as the demands of the home environment and the level of organisational support. They identified that stress, quality of life, well-being, and depression are affected by this. WFH might also be associated with reduced stress, due to the physical separation of office politics and the elimination of transport to the office - as travelling to work significantly increases stress levels of employees [8]. However, other studies claim the opposite [e.g. 10, 55, 56]. WFH might also create stress [10, 56], decrease work-life balance [55], cause higher rates of depression [57], and lower engagement [58]. So far, there is little research on home workspace design in relation to mental health. Amerio et al. [59] showed a strong association between poor housing design (outside view and apartment size) and depressive symptoms. In addition, distractions at home from noise levels have been suggested to impair employees’ mental health [60]. Also, Boegheim [61] identified the indoor environmental quality of the home (e.g. air quality, thermal comfort, lighting, noise) as a determinant of workplace mental health and productivity when WFH. Other COVID-19 studies [62] showed that perceived overall mental health decreased while WFH home as well.
Regarding social health, isolation is found to be one of the biggest disadvantages of WFH [e.g. 3, 7, 8, 11, 18]. In many studies, respondents cite isolation as the primary reason why they do not want to WFH full-time [3]. It is therefore important that the relationships between colleagues are maintained when WFH [6]. A lack of support between the organisation (colleagues/manager) and the employee has a direct effect on productivity [9, 18] plus an indirect effect through satisfaction with WFH [12]. Also, WFH intensity regulates how much one suffers from professional isolation [63]. So, we pose that:
H5: The physical and social environment at home are related to employee health when WFH
Regarding productivity and the physical environment, WFH in a separate room with a door allows to work more productively, as one can focus on work and finish tasks without being interrupted [18]. But it appears that, when choosing their at-home workplace, most people choose to take the smallest or least-contested space available in the house, over inconveniencing family members [11]. Regarding the social environment, workers with children rated the benefits of WFH to be higher, compared to those with no children at home [16]. However, Nakrošiene et al. [12] revealed that the number of children in the household negatively influences one’s satisfaction with WFH. According to Golden et al. [64], one’s household size negatively affects the work-life balance of those WFH. This means that when the household size is large, there is an increased probability of work-family conflicts (such as the intrusion of family members during work) – therefore resulting in reduced satisfaction with WFH and reduced productivity.
H6: The physical and social environment at home are related to employee productivity when WFH
2.4Mediating relationships
Obviously, personal characteristics also determine what the physical and social home work environment looks like. For example, age correlates to both (still) having children living at your home and the age of those children. Also, education and job role relate to salary and this determines house sizes and thus also the likelihood of having a dedicated and furnished workplace at home. So we first pose:
H7: Personal characteristics are related to environmental characteristics of the home workplace
In addition, the physical and social environment at home are likely to be related to each other. For example, employees with more children living at home are less likely to have a dedicated room to work in [65]. So we also pose:
H8: The physical and social environment at home are related to each other
Last, we pose a hypothesis on health as a mediator between such characteristics and productivity, as suggested by Seva et al. [39]. As this is one of the novelties of this study, no futher existing proof has been found. We pose:
H9: Relationships of the physical and social environment at home with productivity are mediated by employee health indicators
3Methods
3.1Data collection
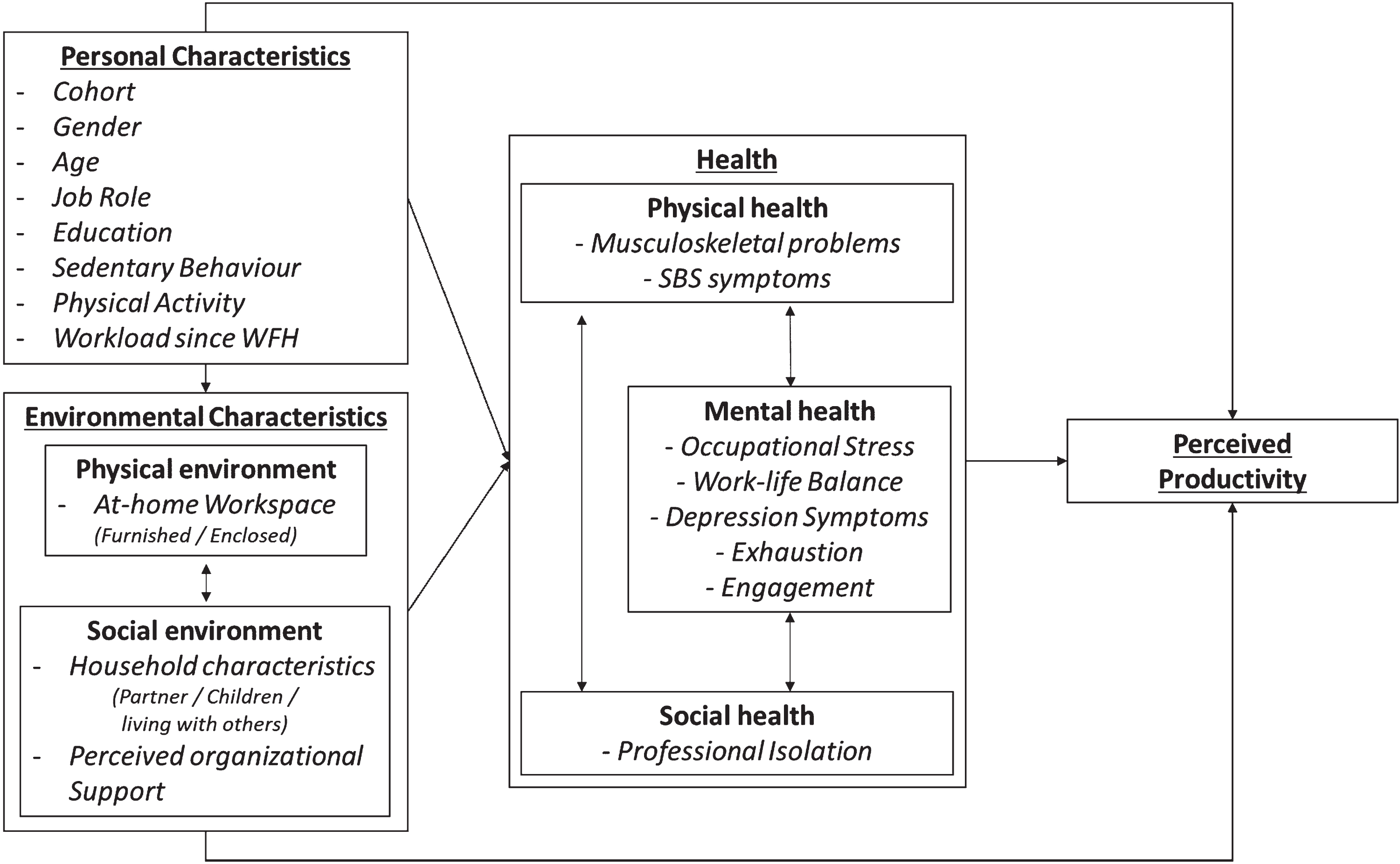
To test the conceptual model, an existing dataset was used; provided by the “We Work from Home” (WWFH) research project (a collaboration between the author institutions mentioned at the top of this paper). WWFH collected data among Dutch office workers of different public organisations, such as several Dutch ministries, the Dutch Tax Authority, the police, and other mostly public large office organisations. Employees received short weekly questionnaires for nine consecutive weeks on their WFH experiences in different topical areas. The data from questionnaire week 3 (n = 25,058; average response rate = 33%) focussed on worker health and productivity and covered the relevant variables in the conceptual model. This data was collected by WWFH throughout 2020 when the pandemic hit the Netherlands in 3 cohorts of different organisations (April 27th-June 14th, n = 5,138; July 20th-August 9th, n = 10,204; September 15th-October 23rd, n = 9,716). The cohort to which a respondent belongs has thus been added as a variable, to check for relevant time effects as the pandemic continued. The dataset also included a question whether the workload since Covid had increased, stayed the same or increased, which was added to the conceptual model because it was used by the WWFH team to structure follow-up questions in the survey. Depending on whether the workload increased, decreased or stayed the same, people would sometimes get slightly differently formulated items to measure occupational stress. Figure 2 shows the final conceptual model with the variables in the dataset.
Fig. 2
Conceptual model with available data from WWFH.
The week 7 data from the WWFH questionnaires also questioned health and productivity but in a slightly different way. These questions had a more descriptive and explanatory nature, to find out why people thought they suffered from the health issues reported in week 3. This data was collected amongst the same populations and cohorts (June 8th-July 12th, n = 3,686; August 17th-September 6th, n = 8,020; October 13th-November 20th, n = 7,156), but yielded smaller samples across all cohorts (n = 18,859; average response rate = 23%; response rates gradually decreased throughout the 9 weeks of surveys, as can be expected). This study, using existing data, is exempt from Institutional Review Board approval.
3.2Measurements
Besides the standard personal characteristics, sedentary behaviour was measured by the percentage spent daily on sitting, standing, and walking, and physical activity by the number of days one moved for at least 30 consecutive minutes. Organisational support was asked through four items (‘The organisation pays enough attention to my work-life balance’, ‘The organisation pays enough attention to health and vitality’, ‘My supervisor supports me in balancing my work-life balance’, ‘My supervisor supports me in the areas of health and vitality’). Regarding physical health, both musculoskeletal problems and symptoms of SBS were identified through questions per potential health issue: ‘have you developed ... ... in the past 4 weeks?’:
• 4 items for musculoskeletal problems (‘pain in the neck and/or shoulders’, ‘pain in hand and/or arms’, ‘pain in the lower back’, as well as ‘pain in legs and/or joints’),
• 2 items for SBS symptoms (‘irritation of the eyes, nose and/or throat’ and ‘(frequent) headaches’).
Regarding mental and social health (parts of) established scientific scales were used for most variables:
• Occupational stress: 6 of the 9 items from the work stress section by Shukla and Srivastava [56], (‘I have a lot of work and fear that very little time to do it’, ‘I feel so burdened that even a day without work seems bad’, ‘I feel that I never take a leave’, ‘My job makes me nervous’, ‘Many a times, my job becomes a big burden’, ‘I feel bad when I take a leave’).
• Work-life balance: 2 slightly rephrased of the 4 items from Brough et al. [66] (‘I am able to balance between time at work and time at other activities’, ‘I feel that the job and other activities are currently balanced’).
• Depression: 4 items of the PHQ-9 item scale [67] (‘difficulty concentrating on tasks’, ‘little interest or enjoyment in doing things’, ‘feeling gloomy, depressed or hopeless’, and ‘poor appetite or overeating’).
• Exhaustion: four items were created by the WWFH teams themselves (‘I can leave work at the end of the homework day’, ‘I can relax well after a day’s work at home’, ‘I feel mentally tired when I start work in the morning’, ‘I feel mentally exhausted by my work at the end of the day’).
• Engagement: 6 items from the 3 aspects of work engagement in the UBES scale [68] (‘I am enthusiastic about my work’, ‘My work inspires me’, ‘When I get up in the morning, I feel like going to work’, ‘When I am working very intensively, I feel happy’, ‘I am proud of the work I do’, ‘I am immersed by my work’).
• Professional isolation: 7 items from Golden et al. [69] (‘I feel left out on activities and meetings that could enhance my career’, ‘I miss out on opportunities to be mentored’, ‘I feel out of the loop’, ‘I miss face-to-face contact with co-workers’, ‘I feel isolated’, ‘I miss the emotional support of co-workers’, ‘I miss informal interaction with others’).
Productivity was rated on a scale of 1–10.
In week 7, the same personal data was asked. Next, multiple-choice questions were included such as ‘What do you think caused your physical health problems?’ and the same for mental health. Besides suggested reasons, these also included the answer option ‘Other, namely ... ’. In addition, changes in exercise and sleeping patterns were questioned. For social health, 7 statements were judged on a 5-point scale of (dis)agreement about changes in contact frequency, type, and content.
3.3Procedure for analysis
Path analysis is a special case of Structural Equation Modelling (SEM), which is generally used to examine the comparative strength of direct and indirect relationships among variables. It estimates multiple regression equations at the same time. The path diagram represents the hypothesized model in path analysis and is similar to a conceptual model in which arrows indicate a direct causal relationship between the explanatory variable to the outcome variable. A path model also controls for other variables in determining the controlled significance of each variable and can identify a mediating role of health between the personal/environmental characteristics and productivity. The amount of mediation is called the indirect effect [70], in which the total effect is the direct and indirect effect together. Furthermore, the extent of mediation can be computed by dividing the mediated effects by the total effect of the relationship [71].
Given the high number of variables, first bivariate analyses were done to determine which relationships were most likely to remain significant in the intended path analyses to test the conceptual model. As each different bivariate analysis method presents its respective indicator of strength (i.e. chi-square value, t-value, F-value, correlation coefficient), the results from the bivariate analyses were compared on the effect size estimates. Only the variables which were found to be of significant predicting power according to their effect sizes were included in the path model. The path model was estimated using the statistical package LISREL version 8.54. For LISREL to function properly, categorical variables were recoded into dummy variables. Continuous variables were kept identical to the variables used in the bivariate analyses and descriptive analyses.
Unfortunately, the datasets from the different weekly surveys did not identify respondents (for privacy reasons), so weeks 3 and 7 could not be combined for statistical analyses. Nonetheless, we used the week 7 data to get general insights into the population’s perceptions of health issue causes with a descriptive analysis next to the test of the model with the data from week 3.
4Results
First, the scales were tested on their internal validity (see Table 1) with Cronbach’s alpha and/or inter-item correlations. All scales except for ‘depression’ scored sufficiently high to be summed into a single score. Depression was recoded in a variable based on the number of symptoms, similar to the physical health variables.
Table 1
Internal validity of multi-item scale variables
| Label (N = 25,058) | # of items | Cronbach’s alpha | Mean inter-item correlation | Mean | Variance | SD |
| Perceived organisational support | 4 | 0.784 | 3.25 | 0.597 | 0.773 | |
| Physical health | ||||||
| Musculoskeletal problems | 4 | 0.507 | 0.204 | 0.98 | 1.114 | 1.055 |
| SBS symptoms | 2 | 0.230 | 0.35 | 0.356 | 0.597 | |
| Mental health | ||||||
| Job stress | 6 | 0.868 | 2.47 | 0.619 | 0.787 | |
| Work-life balance | 2 | 0.682 | 3.42 | 0.858 | 0.926 | |
| Depression symproms | 4 | 0.572 | 0.230 | 0.57 | 0.812 | 0.901 |
| Exhaustion | 4 | 0.792 | 2.49 | 0.567 | 0.753 | |
| Engagement | 6 | 0.873 | 3.76 | 0.393 | 0.627 | |
| Social health | ||||||
| Professional isolation | 7 | 0.848 | 3.15 | 0.556 | 0.746 |
4.1Personal and environmental descriptives
Tables 2 and 3 show descriptives of the personal and environmental characteristics of both samples (weeks 3 and 7). They are similar in gender, job position, and household characteristics. Statistically significant but very small differences between the samples were found for age and education distributions. Also, by week 7, some more people had (gained) the availability of an enclosed and/or furnished workspace at home. Overall, their similarities support the use of the week 7 data to help explain wellbeing outcomes from week 3.
Table 2
Descriptives of personal characteristics
| Personal characteristics | Survey week 3 | Survey week 7 | |||
| Frequency | Sample (%) | Frequency | Sample (%) | ||
| Cohort | Cohort 1 | 5138 | 20.5% | 3683 | 19.5% |
| Cohort 2 | 10204 | 40.7% | 8020 | 42.5% | |
| Cohort 3 | 9716 | 38.8% | 7156 | 37.9% | |
| Gender | Male | 11798 | 47.1% | 8964 | 47.5% |
| Female | 13142 | 52.4% | 9819 | 52.1% | |
| Other | 118 | 0.5% | 76 | 0.4% | |
| Age | ≤30 years old | 2145 | 8.6% | 1436 | 7.6% |
| 31–40 years old | 4010 | 16.0% | 2885 | 15.3% | |
| 41–50 years old | 5764 | 23.0% | 4406 | 23.4% | |
| 51–60 years old | 9360 | 37.4% | 7157 | 38.0% | |
| >60 years old | 3779 | 15.1% | 2975 | 15.8% | |
| Job role | Management employee | 1724 | 6.9% | 1286 | 6.8% |
| Regular employee | 23334 | 93.1% | 17573 | 93.2% | |
| Level of education | Primary & secondary education | 1633 | 6.5% | 1119 | 5.9% |
| MBO | 4349 | 17.4% | 3113 | 16.5% | |
| HBO | 10115 | 40.4% | 7815 | 41.4% | |
| University | 8763 | 35.0% | 6678 | 35.4% | |
| Other | 198 | 0.8% | 134 | 0.7% | |
| Sedentary behaviour | N | 25058 | 18859 | ||
| % of time in the workday that is spent sitting | Mean | 81.11 | 81.50 | ||
| Standard deviation | 13.539 | 13.216 | |||
| Physical activity | N | 25058 | 18859 | ||
| # of days per week with a minimum of 30 minutes of exercise | Mean | 4.24 | 3.79 | ||
| Standard deviation | 2.050 | 2.018 | |||
| Workload since WFH | Increased workload | 6715 | 26.8% | 5063 | 26.8% |
| Similar workload | 15744 | 62.8% | 12104 | 64.2% | |
| Decreased workload | 2599 | 10.4% | 1692 | 9.0% | |
Table 3
Descriptives of environmental characteristics
| Environmental characteristics | Survey week 3 | Survey week 7 | ||||
| Frequency | Sample (%) | Frequency | Sample (%) | |||
| At-home workspace | Furnished workspace | No | 10088 | 40.3% | 6915 | 36.7% |
| Yes | 14970 | 59.7% | 11944 | 63.3% | ||
| Enclosed workspace | No | 8606 | 34.3% | 6265 | 33.2% | |
| Yes | 16452 | 65.7% | 12594 | 66.8% | ||
| Household characteristics | Partner | No | 6029 | 24.1% | 4525 | 24.0% |
| based on household type | Yes | 19029 | 75.9% | 14334 | 76.0% | |
| Children | No | 13746 | 54.9% | 10363 | 54.9% | |
| based on household type | Yes | 11312 | 45.1% | 8496 | 45.1% | |
| Living with others | No | 3886 | 15.5% | 2905 | 15.4% | |
| based on household type | Yes | 21172 | 84.5% | 15954 | 84.6% | |
| Perceived organisational support | N | 25058 | 18859 | |||
| on a scale from 1 (very low) to (very high) | Mean | 3.247 | 3.252 | |||
| Standard deviation | 0.773 | 0.753 | ||||
Regarding the different cohorts, cohort 2 was the largest, but the others also had many respondents due to the large sample. No significant differences were observed between the cohorts in gender or household composition, but several other statistical differences came forward. Regarding personal characteristics, cohort 3 contained relatively more people in the older age groups than cohort 1 and 2 (X2(25058;8) = 17.307, p = 0.027), although the differences were very small. Cohort 3 also more often indicated increased workloads and less often decreased workloads than the other two cohorts (X2(25058;4) = 283.010, p = 0.000). Nonetheless, in all cohorts, approximately 61–64% observed a similar workload than before the pandemic. Cohort 1 contained significantly fewer managers than the other two cohorts (X2(25058;2) = 88,923, p = 0.000) and also less low educated and more highly educated people (X2(25058;4) = 37.154, p = 0.000). Regarding active behaviour, the percentage of time sitting significantly increased from cohort 1 (80.8) to cohort 2 (81.0) to cohort 3 (81.4) (F(2;25058) = 4.570, p = 0.010). Similarly, the number of days with 30 minutes of exercise decreased significantly from cohort 1 (4.5) to cohort 2 (4.3) to cohort 3 (4.1) (F(2;25058) = 81.640, p = 0.000). Regarding environmental characteristics (see Table 3), cohort 1 had significantly less often the availability of a furnished workspace (X2(25058;2) = 8.235, p = 0.016) or an enclosed workspace (X2(25058;2) = 7.002, p = 0.030). Cohort 1 also perceived organisational support significantly lower (3.22) compared to cohort 2 (3.26) and 3 (3.26). The cohort variable was therefore included in further analyses to include potential effects.
4.2Health status and perceived productivity descriptives
Regarding physical health, only 36.7% of the respondents reported not having developed any of the questioned musculoskeletal or SBS symptoms over the previous four weeks. Most reported problems like pain in the neck and/or shoulders (40.5%) or lower back (27.8%). Also, quite a large group of respondents reported headaches (20.6%) and irritation of the eyes, nose and/or throat (14.9%). When counting the number of musculoskeletal problems, respondents suffered on average from 0.98 (out of 4) problems. For the number of SBS symptoms, the mean was lower with 0.35 (out of 2, see Table 4). All scale-based mental health variables were within normal distribution ranges. As they were all measured on 5-point scales, Table 4 makes clear that occupational stress (2.47) and exhaustion (2.48) on average were lower and in the middle of the scale, while the work-life balance (3.42) and engagement (3.76) scored on the positive side of the scale. The average number of depression symptoms was also low with 0.57 (out of 2), so in general mental health was perceived as reasonable. Social health (professional isolation) was also normally spread, with a mean of 3.15 (on a 7-point scale). Perceived productivity was high, with a mean of 7.59 (SD = 1.217) on a 10-point scale.
Table 4
Descriptives of health indicators week 3
| N = 25,058 | Mean | SD | |
| Physical health | Number of musculoskeletal problems | 0.98 | 1.055 |
| Number of SBS symptoms | 0.35 | 0.597 | |
| Mental health | Job stress | 2.47 | 0.787 |
| Work-life balance | 3.42 | 0.926 | |
| Number of depression symptoms | 0.57 | 0.901 | |
| Exhaustion | 2.49 | 0.753 | |
| Engagement | 3.76 | 0.627 | |
| Social health | Professional isolation | 3.15 | 0.746 |
4.3Path analysis hypotheses 1–8
In the bivariate analyses, almost all variables were significantly related to at least one of the other variables, which would confirm all the hypotheses that are posed. However, the effect sizes (see Table 5) revealed that many of the relationships were relatively weak. Mostly, relationships between different health indicators and between health and productivity or health and the social environment (support) were stronger. These findings suggest that health plays a larger role in the perceived productivity of those WFH, and personal and environmental factors only a relatively small role. Nonetheless, all significant bivariate relationships were included in the path analysis to find out which hypotheses remain confirmed when tested in a holistic matter with a full path model. Persons that identify as neither male nor female (118 respondents) were removed from the path analysis data-set as this category was not suitable for path analysis, due to being such a small proportion of the sample. Similarly, persons that stated having ‘other’ education (189 respondents) were also excluded from the dataset for the same reason. This resulted in a new research sample of 24,751 respondents for the path analysis. As path analysis does not allow the use of dummy variables when these variables are endogenous (i.e. having no incoming arrows in the path model [72]), potential relationships between personal characteristics and the at-home workplace and household factors could not be included in the path model. This means that H7 could only be tested partially this way.
Table 5
Effect sizes bivariate analyses
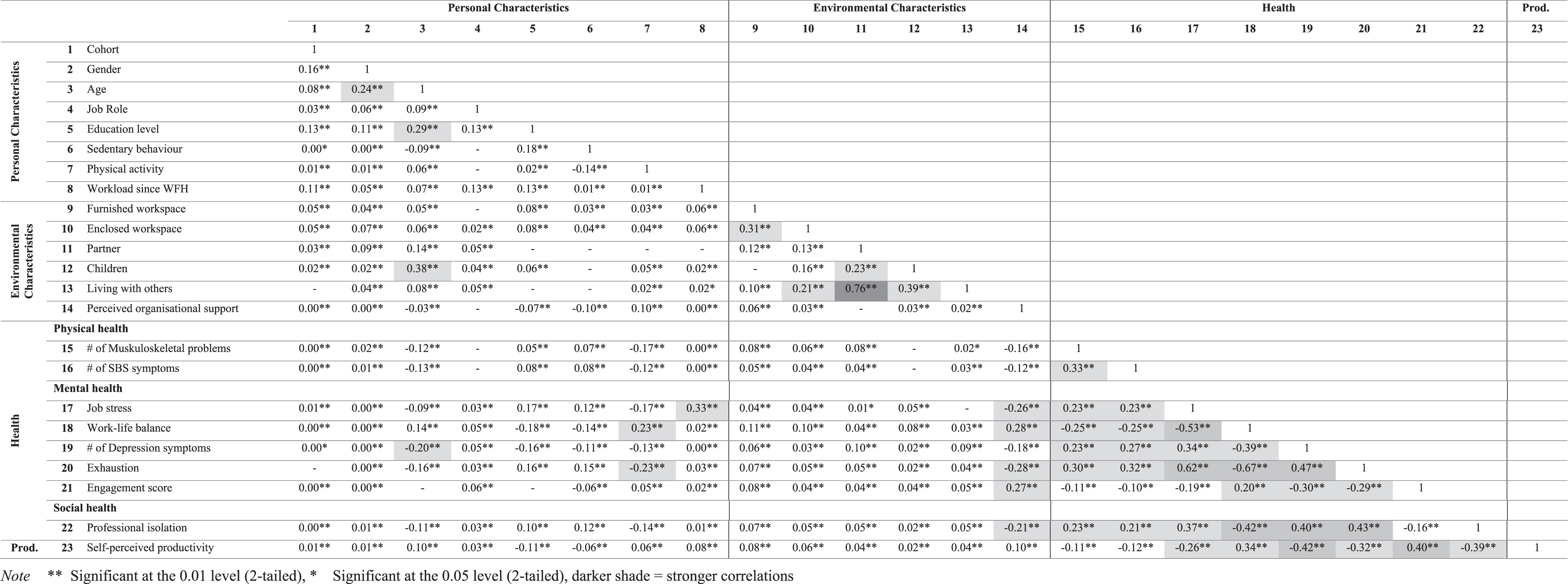 |
Note **Significant at the 0.01 level (2-tailed), *Significant at the 0.05 level (2-tailed), darker shade = stronger correlations.
After putting all significant bivariate relationships in the model, it was further optimized. The risk of overfitting the model was reduced by reducing the number of variables in the model and removing insignificant relationships (t < 1.96). This step-by-step process was repeated until an acceptable model fit was found and all insignificant relationships were removed from the model. As a result, five variables of personal characteristics were removed from the path model for being insignificantly related to aspects of health or perceived productivity (Cohort, Job role, Sedentary behaviour, Physical activity, and Workload since WFH). In addition, one variable of the social environment (the Partner at home dummy) had to be removed for the same reason.
Table 6 shows the information regarding the goodness of fit of the final path model. The Goodness of Fit Index of 1 is high, as it should be larger than 0.90 to indicate a good model [73]. Similarly, the Comparative Fit Index (CFI) shows a good fit [74]. The Root Mean Square Error of Approximation (RMSEA = 0.012) is commonly considered a good fit with values less than 0.05 [73]. Other indicators were within ranges as well. The final path model (see Fig. 3) shows a very complex picture of health and productivity in relation to each other (H1 and H2) and to the home work environment (H3-8) (see Table 7 for all standardized coefficients). The effects that were 0.20 or higher (when rounded) have been emphasized in Fig. 3 with thicker lines to show more clearly which effects are the strongest.
Table 6
Goodness of fit
| Full information ML chi-square | 140.81 (p = 0.000) |
| Degrees of freedom (df) | 29 |
| Goodness of fit index | 1 |
| Comparative fit index (CFI) | 1 |
| Root mean square error of approximations (RMSEA) | 0.012 |
| 90% confidence interval of RMSEA | 0.010; 0.015 |
| p-value for test of close fit (RMSEA <0.05) | 1 |
| Root mean square residual (RMR) | 0.0033 |
| Chi-square / df | 4.856 |
Fig. 3
Final path model.
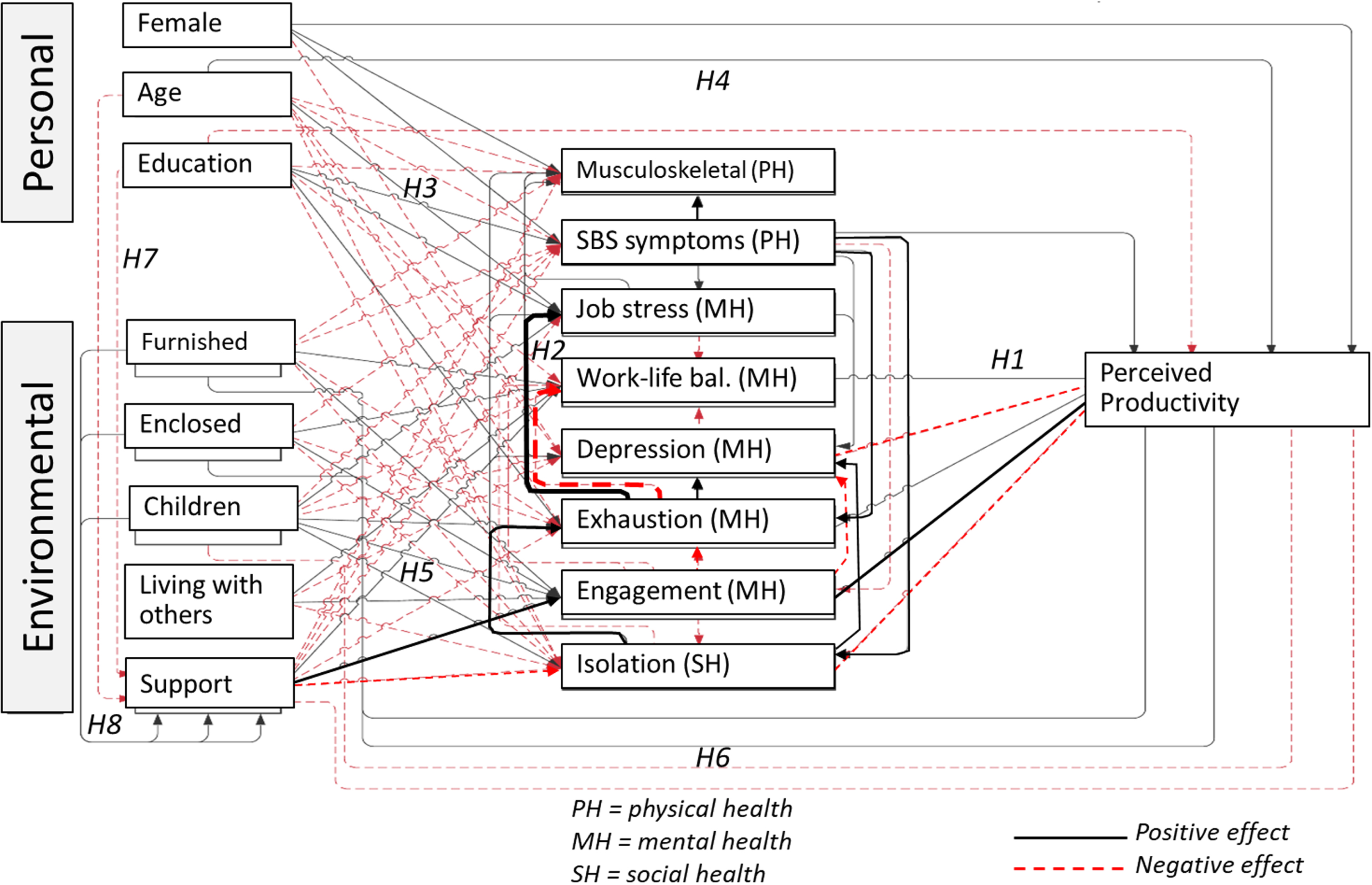
Table 7
Standardized coefficients path analysis
| Variables | Support | Musculoskeletal problems | SBS symptoms | Job stress | Work-life balance | Depression symptoms | Exhaustion | Engagement | Professional isolation | Self-perceived productivity | ||
| Standardized coefficients | ||||||||||||
| Personal characteristics | Gender | Male | - | - | - | - | - | - | - | - | - | - |
| Female | 0.09** | 0.07** | –0.03** | 0.10** | ||||||||
| Age | –0.05** | –0.03** | –0.11** | 0.03** | –0.12** | –0.08** | –0.08** | 0.03** | ||||
| Education | Low | - | - | - | - | - | - | - | - | - | - | |
| High | –0.09** | –0.03** | 0.04** | 0.06** | –0.06** | 0.08** | 0.06** | –0.02** | ||||
| Environmental characteristics | Furnished workspace | No | - | - | - | - | - | - | - | - | - | - |
| Yes | 0.05** | –0.04** | –0.03** | 0.04** | –0.02** | 0.05** | –0.03** | 0.01** | ||||
| Enclosed workspace | No | - | - | - | - | - | - | - | - | - | - | |
| Yes | 0.03** | –0.02** | 0.04** | –0.01* | 0.02** | –0.03** | 0.02** | |||||
| Children | No | - | - | - | - | - | - | - | - | - | - | |
| Yes | 0.04** | –0.02** | 0.04** | –0.07** | –0.02** | 0.02** | 0.02** | 0.03** | –0.02** | |||
| Living with others | No | - | - | - | - | - | - | - | - | - | - | |
| Yes | 0.03** | –0.05** | 0.04** | –0.05** | ||||||||
| Support | –0.07** | –0.12** | –0.08** | 0.07** | –0.14** | 0.26** | –0.16** | –0.05** | ||||
| Physical health | Musculoskeletal problems | |||||||||||
| SBS symptoms | 0.23** | 0.03** | 0.10** | 0.19** | –0.07** | 0.16** | 0.03** | |||||
| Mental health | Job stress | 0.02** | –0.13** | –0.05** | ||||||||
| Work-life balance | 0.13** | |||||||||||
| Depression symptoms | 0.04** | –0.06** | –0.21** | |||||||||
| Exhaustion | 0.14** | 0.53** | –0.48** | 0.24** | 0.03** | |||||||
| Engagement | –0.02** | –0.17** | –0.18** | –0.10** | 0.30** | |||||||
| Social health | Professional isolation | 0.07** | 0.11** | –0.12** | 0.22** | 0.31** | –0.23** | |||||
- Reference category. **Significant at the 0.01 level (2-tailed) t > 2.58. *Significant at the 0.05 level (2-tailed) t > 1.96.
This confirms again that both personal and environmental characteristics play a relatively small role, although three personal (gender, age, education) and five environmental (furnished workspace, enclosed workspace, children, living with others, organisational support) characteristics have significant relationships with indicators of health and perceived productivity. This confirms hypotheses H3-6. But only perceived organisational support at home shows relatively strong relations with mental health (engagement, β= 0.26) and social health (isolation, β= –0.16)). Thus H5 is the only hypothesis that can be confirmed with a strong relationship.
Within the different health indicators several stronger relationships are found as well, also strongly confirming H2. Regarding physical health, symptoms of Sick Building Syndrome appear to relate to experiencing musculoskeletal problems (β= 0.23), but also to mental health (exhaustion, β= 0.19) and social health (increased feelings of isolation, β= 0.16). The strongest relations within the path model, however, are between the different mental health indicators. Especially exhaustion seems to play a key role here. It relates to increased stress (β= 0.53), poorer work-life balance (β= –0.48) and more depressive symptoms (β= 0.24) and is increased in case of lower engagement (β= –0.18). A second mental health aspect that shows many relatively stronger relationships is engagement. Higher engagement does not only decrease exhaustion, but also depressive symptoms (β= –0.17). Regarding social health (professional isolation), this relates to increased exhaustion (β= 0.31) and more depressive symptoms (β= 0.22).
Despite its key role within the health relationships, exhaustion does not have a strong direct relationship with perceived productivity (β= 0.03). The relationship of engagement with perceived productivity is much stronger (β= 0.30). Furthermore, depressive symptoms relate to decreased perceived productivity (β= –0.21). Social health also relatively strongly relates to decreased perceived productivity (β= –0.23). So, H1 is confirmed with strong relationships too.
4.4Mediation analysis hypothesis 9
In total, 78.8% of the total effects on perceived productivity in the model originated from aspects of health (e.g. 25% of effects from engagement and 19% from professional isolation), which confirms H9. Table 8 presents an analysis of the mediation found in the path model, showing direct, indirect, and total effects of the different significant relationships. It shows that health mediated more than half of the total effects from most personal and environmental characteristics on perceived productivity. Only gender had no mediation in its effect on perceived productivity. On the other end of the mediation spectrum, living with others only showed an indirect effect through mediators such as work-life balance, depression, engagement and professional isolation. The negative effect of living with children on productivity was higher direct than the indirect effect, but in all other cases the indirect effect was higher than the direct effect. Age relates to increased perceived productivity indirectly for 78%, mediated through support, SBS, job stress, depression, exhaustion, and professional isolation. Similarly, education is found to decrease perceived productivity directly only to a small extent, as 72% of the total effects were indirect through support, SBS symptoms, job stress, work-life balance, exhaustion, and professional isolation.
Table 8
Mediation analysis
| Relationships with perceived productivity (PP)* | Direct effect | Indirect effect | Total effect | Proportion of mediation |
| Personal characteristics | ||||
| Gender | 0.24 | 0.24 | 0.00 | |
| Age ⟶ (Support, MSK, SBS, stress, depression, exhaustion, ISO) | 0.02 | 0.07 | 0.09 | 0.78 |
| Education ⟶ (Support, MSK, SBS, stress, WLB, exhaustion, ISO) | –0.05 | –0.13 | –0.18 | 0.72 |
| Environmental characteristics | ||||
| Furnished workspace ⟶ (Support, MSK, SBS, WLB, exhaustion, ENG, ISO) | 0.03 | 0.12 | 0.15 | 0.80 |
| Enclosed workspace ⟶ (Support, SBS, WLB, exhaustion, ENG, ISO) | 0.05 | 0.08 | 0.13 | 0.62 |
| Children ⟶ (Support, SBS, stress, WLB, depression, exhaustion, ENG, ISO) | –0.05 | –0.01 | –0.06 | 0.17 |
| Living with others ⟶ WLB, depression, ENG, ISO | 0.14 | 0.14 | 1.00 | |
| Support ⟶ (MSK, SBS, stress, WLB, exhaustion, ENG, ISO) | –0.09 | 0.30 | 0.21 | 1.43 |
*MSK = Musculoskeletal problems, WLB = Work-life balance, ENG = Engagement, ISO = Professional Isolation.
The effects from working from a furnished at-home workspace on perceived productivity were found to consist for 80% out of indirect effects. Support, SBS, work-life balance, exhaustion, engagement, and professional isolation mediated to a large extent the effects of working from a furnished at-home workspace on perceived productivity. A slightly smaller proportion of the effects from working from an enclosed at-home workspace on perceived productivity consisted out of indirect effects from almost the same mediator variables (62%). The effects of perceived organisational support on perceived productivity are largely mediated again by SBS, job stress, work-life balance, exhaustion, engagement, and professional isolation.
5Discussion and conclusions
The current research has expanded upon the growing body of literature on WFH and employee outcomes on health and productivity in several ways. First of all, it has shed light on the persistence of proven relations between employees, their work environment, and health outcomes during the exceptional circumstances of obliged, high-intensity WFH during Covid-19. Some older studies discuss that, in general, non-work-related factors, such as family orientation and amount of household distractions, are most predictive of an individual’s choice to work remotely [5]. In normal circumstances, some sort of self-selection process takes place in which employees with a suitable home situation choose to WFH (when also allowed to by the organisation). Conversely, in this study, also employees with unsuitable home environments were obliged to WFH, resulting in an exceptional opportunity to study relationships between the at-home environment and perceived health and productivity in that situation. Findings support the assumption in studies in voluntary WFH contexts [e.g. 3, 8, 10, 12] that the suitability of the home workplace indeed plays a role for employee health and productivity.
However, through the novelties of investigating a holistic model of relationships between personal and environmental characteristics, health and productivity, and by including a potential mediating role of employee health, novel findings came forward. Results suggest that the significance of personal and environmental characteristics for productivity outcomes of WFH might be limited. This is in contrast to previous studies that stress the importance of both categories of characteristics [e.g. 5, 8, 11, 18 –19]. But because those studies did not include a mediating approach, they were unable to identify the large mediating role of health that came forward in this study. Although most personal and environmental characteristics remained significant in the path analysis, their effects on productivitity were largely mediated by the health indicators. Only gender and having children at home, showed more direct effects on perceived productivity while WFH. So, health indicators might be the most important aspect for organisations to measure and keep in mind when implementing future hybrid working modes, particularly engagement and exhaustion.
During Covid-19, most attention of employers went to providing ICT connectivity and ergonomic support (chairs, screens, etc.) to ensure employee wellbeing and productivity. However, the current study seems to suggest that while physical health might have suffered from forced full-time WFH too, particularly mental and social health determined productivity outcomes during Covid-19. In addition, media particularly covered sedentary behaviour and lack of physical activity as reasons for poorer health during the pandemic, but both variables were not significant in this study. From all the personal and environmental characteristics that were included, particularly perceived organizational support showed to improve both mental and social health (by decreased feelings of isolation and increased engagement). Previous studies [e.g. 75] have also shown that supervisor and co-worker support relates to many employee outcomes, including stress and work-life balance. This is clearly an important point of attention for future hybrid working modes as well.
In addition, the path analysis shows a strong network of relationships between the social and mental health indicators, where exhaustion appears to play a central mediating role. So, despite the limited impact of exhaustion on perceived productivity, it mediates relations with many health indicators that do play a role. Particularly feelings of depression, isolation and engagement were stronger predictors of perceived productivity than exhaustion. As this study shows, mental health while WFH is a complex network of interacting variables and needs further research.
As mentioned, a brief descriptive analysis of data from the week 7 survey of WWFH is now used to interpret the findings further. It showed that the majority of home workers with physical health problems (74.7%) think these problems are caused by their sedentary behaviour, in which there is too little alteration between sitting and standing or walking. On the other hand, most of the respondents with mental health problems attributed these problems to being obliged to work from home (66.6%) and feeling socially isolated (57%). Contact with colleagues was found to have become less personal as a result of the obliged WFH. As there is a lack of research on obliged WFH, this is an interesting new finding too. It suggests that future research should include the voluntariness of WFH to study new hybrid working modes. And, in practice, managers have to discuss with invidual employees how to best fill in the choice of working home and/or in the office to ensure their mental health. Of course, there are both positive and negative aspects to social isolation when WFH: positive aspects of social isolation are related to having a quiet private space to work with no interruptions [6], while negative aspects are related to feelings of loneliness [3, 8]. Other Covid-19 studies have shown that loneliness increases depression and decreases helping behaviours between colleagues [e.g. 76]. So, it is important to strike a balance between the ability to do focussed work and feeling forced to do this type of work from home. Not all home workplaces are evenly likely to even provide this ability to focus.
What the week 7 data also showed, is that despite the high prevalence of reported health problems, only 6.2% reported calling in sick. Two decades ago, Mann & Holdsworth [8] already suggested that improved policies are necessary for sick leave while WFH. The current results suggest that this advice has not yet been implemented by the managers in this sample. Especially young adults appeared vulnerable to mental health issues, which supports similar findings by Pieh et al. [77] and Weitzer et al. [78]. Pieh et al. suggested that this could potentially be explained by their higher (occupational) uncertainty and larger restrictions in their daily lives due to COVID-19 induced lockdowns. They might thus be even less inclined to call in sick, while they have more likeliness of health problems when WFH. This is not only true for mental health, but most likely also for physical health as they generally have smaller housing then those in more advanced careers. This has longer term consequences, because through this form of presenteeism an employee’s self-regulation is demanded, which depletes their resources and reduces their work effectiveness on the following day [79].
5.1Limitations and future research
The WWFH dataset included perceived productivity measurements only, as it is easier to measure productivity through questionnaires than objectively on site. Leaman & Bordass [80] found that perceived productivity scales may not be the same as actual productivity due to a lack of reference. Nevertheless, the use of perceived productivity is commonly accepted as an indicator of individual productivity [81]. For this sample, productivity increased slightly but significantly between each consecutive cohort from 7.53 (cohort 1) to 7.59 (cohort 2) to 7.62 (cohort 3) (F(2;24748) = 10.403, p = 0.000). This suggests that people felt that they learned to work from home even better over time. It remains to be seen whether perceived productivity at home correlates strongly with actual productivity, as this has not been studied yet. It could well be that the workers considered themselves really productive because of the individual concentrated work that they were able to do, while they might have neglected potential negative influences of the lack of joint collocated activities on productivity (e.g. serendipitous knowledge sharing) and health effects.
This study was conducted during the COVID-pandemic lockdowns in the Netherlands. Therefore, some of the findings regarding health may contain biases or exaggerations, hence limiting the generalizability of the results. Once hybrid working has been embraced by more workers, future research can repeat this study with workers in a non-pandemic context. This would also allow more diversification in the intensity of WFH, to find an ‘ideal’ split in WFH and at the office. In addition, more longitudinal research is necessary. While this sample included 3 cohorts, it did not follow the same people over the course of time. It could be that decreasing health did not immediately affect productivity, but has more impact on the longer term. For example, Guler et al. [82] found a decline in health during Covid-19 while perceived productivity increased.
The results and interpretations are also limited by not having insights in the WWFH dataset in some other potentially influential aspects of the physical and social working environment (e.g. objective indoor temperature, lighting and noise), as well as other indicators of mental and social health (e.g. job satisfaction and happiness). Last, the results of this research are limited by the methodological and practical limitations of path analysis regarding the use of exogenous dichotomous variables.
Future research should first try to overcome the limitations of the current study, for example by also assessing the unidentified influential aspects of the physical and social working environment (e.g. satisfaction with lighting, temperature and noise, as well as the age of the youngest child in the household) and important aspects of physical, mental and social health (e.g. quality of life, happiness and strain). By including these characteristics and health aspects, an even more comprehensive understanding of the influences of WFH on health and productivity, and the role of personal and environmental characteristics can be produced. Furthermore, future research could study samples in other countries and cultures, where at-home conditions could be very different and thus perhaps impacting employee outcomes differently.
5.2Practical implications
The knowledge gained from the current study can also assist in the design and implementation of policies for improving, protecting and promoting occupational health practices, both in the office and at home. It seems important that significant investments are made in protecting and promoting occupational health among hybrid workers. As the cohort variable was not significant, this suggests that workers do not find a more healthy balance themselves after WFH for a longer time.
Even though health was identified as having the largest effect on perceived productivity, the authors emphasise the importance of a suitable physical and social homeworking environment for successful WFH as well. It is recommended that the employer plays a facilitating and supporting role in fulfilling the individual needs of their employees regarding WFH intensity, flexibility and the physical home workplace.
Disclaimer
This article is based on the master thesis of Thijs Voulon at Eindhoven University of Technology.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
The authors report no funding.
Ethics statement
The data were gathered by the Centre for People & Buildings through informed consent of the anonymous individual participants, funded partially by the participating organisations in the We Work from Home project. No ethical reviews were necessary at the time of data gathering within the involved universities, but of course all ethical considerations have been taken to merit such approval.
References
[1] | Buomprisco G , Ricci S , Perri R , De Sio S . Health and telework: New challenges after COVID-19 pandemic. Eur J Environ Public Health. (2021) ;5: (2):em0073. |
[2] | Fayard A-L , Weeks J , Khan M . Designing the Hybrid Office. Harvard business review [Internet]. 2021[cited 2022 Oct 4]. Available from: https://hbr.org/2021/03/designing-the-hybrid-office |
[3] | Bloom N , Liang J , Roberts J , Ying ZJ . Does working from home work? Evidence from a Chinese experiment. Q J Econ. (2015) ;130: (1):165–218. |
[4] | Felstead A , Henseke G . Assessing the growth of remote working and its consequences for effort, well-being and work-life balance. New Technol Work Employ. (2017) ;32: (3):195–212. |
[5] | Bailey DE , Kurland NB . A review of telework research: Findings, new directions, and lessons for the study of modern work. J Organ Behav. (2002) ;23: (4):383–400. |
[6] | Grant CA , Wallace LM , Spurgeon PC . An exploration of the psychological factors affecting remote e-worker’s job effectiveness, well-being and work-life balance. Empl Relat. (2013) ;35: (5):527–46. |
[7] | Mann S , Varey R , Button W . An exploration of the emotional impact of tele-working via computer-mediated communication. J Manag Psychol. (2000) ;15: (7):668–90. |
[8] | Mann S , Holdsworth L . The psychological impact of teleworking: Stress, emotions and health. New Technol Work Employ. (2003) ;18: (3):196–211. |
[9] | Golden TD , Gajendran RS . Unpacking the role of a telecommuter’s job in their performance: Examining job complexity, problem solving, interdependence, and social support. J Bus Psychol. (2019) ;34: (1):55–69. |
[10] | Tavares AI . Telework and health effects review. Int J Healthc. (2017) ;3: (2):30. |
[11] | Ammons SK , Markham WT . Working at hdome: Experiences of skilled white collar workers. Sociol Spectr. (2004) ;24: (2):191–238. |
[12] | Nakrošiene A , Buciuniene I , Goštautaitė B . TELEWORK OUTCOMES Preprint Research Gate [Internet]. Unpublished; 2020. Available from: http://dx.doi.org/10.13140/RG.2.2.11064.08961 |
[13] | Horst* DJ , Broday EE , Bondarick R , Serpe LF , Pilatti LA . Quality of working life and productivity: An overview of the conceptual framework. Int J Managerial Studies Research. (2014) ;2: (5):87–98. |
[14] | Merrill RM , Aldana SG , Pope JE , Anderson DR , Coberley CR , Whitmer RW , et al. Presenteeism according to healthy behaviors, physical health, and work environment. Popul Health Manag. (2012) ;15: (5):293–301. |
[15] | Vittersø J , Akselsen S , Evjemo B , Julsrud TE , Yttri B , Bergvik S . Impacts of home-based telework on quality of life for employees and their partners. Quantitative and qualitative results from a european survey. J Happiness Studies. (2003) ;42: (2):201–33. |
[16] | Mokhtarian PL , Bagley MN , Salomon I . The impact of gender, occupation, and presence of children on telecommuting motivations and constraints. J Am Soc Inf Sci. (1998) ;49: (12):1115–34. |
[17] | Standen P , Daniels K , Lamond D . The home as a workplace: Work-family interaction and psychological well-being in telework. J Occup Health Psychol. (1999) ;4: (4):368–81. |
[18] | Thorstensson E . The Influence of Working from Home on Employees’ Productivity: Comparative document analysis between the years. Karlstad: Karlstad University; (2000) . |
[19] | Troup C , Rose J . Working from home: Do formal or informal telework arrangements provide better work–family outcomes? Community Work Fam. (2012) ;15: (4):471–86. |
[20] | Bouziri H , Smith DRM , Descatha A , Dab W , Jean K . Working from home in the time of COVID-19: How to best preserve occupational health? Occup Environ Med. (2020) ;77: (7):509–10. |
[21] | Henke RM , Benevent R , Schulte P , Rinehart C , Crighton KA , Corcoran M . The effects of telecommuting intensity on employee health. Am J Health Promot. (2016) ;30: (8):604–12. |
[22] | Hoornweg N , Peters P , van der Heijden B . Finding the optimal mix between telework and office hours to enhance employee productivity: A study into the relationship between telework intensity and individual productivity, with mediation of intrinsic motivation and moderation of office hours. In: De LeedeJ; editor. New ways of working practices. Antecedents and outcomes. Bingley, U.K.: Emerald Group Publishing Limited. (2016) , pp. 1–28. |
[23] | Gajendran RS , Harrison DA . The good, the bad, and the unknown about telecommuting: Meta-analysis of psychological mediators and individual consequences. J Appl Psychol. (2007) ;92: (6):1524–41. |
[24] | WHO. What is The WHO Definition of Health? [Internet]. Who.int. [cited 2022 Nov 11. Available from: https://www.who.int/about/governance/constitution |
[25] | Chirico F , Zaffina S , Di Prinzio RR , Giorgi G , Ferrari G , Capitanelli I , et al. Working from home in the context of COVID-19: A systematic review of physical and. (2021) ;6: (3):319–32. |
[26] | Argus M , Pääsuke M . Effects of the COVID-19 lockdown on musculoskeletal pain, physical activity, and work environment in Estonian office workers transitioning to working from home. Work. (2021) ;69: (3):741–9. |
[27] | Houle M , Lessard A , Marineau-Bélanger É , Lardon A , Marchand A-A , Descarreaux M , et al. Factors associated with headache and neck pain among telecommuters - a five days follow-up. BMC Public Health. (2021) ;21: (1):1086. |
[28] | Larrea-Araujo C , Ayala-Granja J , Vinueza-Cabezas A , Acosta-Vargas P . Ergonomic risk factors of teleworking in Ecuador during the COVID-19 pandemic: A cross-sectional study. Int J Environ Res Public Health. (2021) ;18: (10):5063. |
[29] | Rodríguez-Nogueira Ó , Leirós-Rodríguez R , Benítez-Andrades JA , Álvarez-Álvarez MJ , Marqués-Sánchez P , Pinto-Carral A . Musculoskeletal pain and teleworking in times of the COVID-19: Analysis of the impact on the workers at two Spanish universities. Int J Environ Res Public Health. (2021) ;18: (1):31. |
[30] | Afonso P , Fonseca M , Teodoro T . Evaluation of anxiety, depression, and sleep quality in full-time teleworkers. Journal of Public Health. (2021) ;1–8. |
[31] | De Sio S , Cedrone F , Nieto HA , Lapteva E , Perri R , Greco E , et al. Telework and its effects on mental health during the COVID-19 lockdown. Eur Rev Med Pharmacol Sci. (2021) ;25: (10):3914–22. |
[32] | Escudero-Castillo I , Mato-Díaz FJ , Rodriguez-Alvarez A . Furloughs, teleworking and other work situations during the COVID-19 lockdown: Impact on mental well-being. Int J Environ Res Public Health. (2021) ;18: (6):2898. |
[33] | Galanti T , Guidetti G , Mazzei E , Zappalà S , Toscano F . Work from home during the COVID-19 outbreak: The impact on employees’ remote work productivity, engagement, and stress: The impact on employees’ remote work productivity, engagement and stress. J Occup Environ Med. (2021) ;63: (7):e426–32. |
[34] | Ghislieri C , Molino M , Dolce V , Sanseverino D , Presutti M . Work-family conflict during the Covid-19 pandemic: Teleworking of administrative and technical staff in healthcare. An Italian study. Med Lav. (2021) ;112: (3):229–40. |
[35] | Hallman DM , Januario LB , Mathiassen SE , Heiden M , Svensson S , Bergström G . Working from home during the COVID-19 outbreak in Sweden: Effects on 24-h time-use in office workers. BMC Public Health. (2021) ;21: (1):528. |
[36] | Ekpanyaskul C , Padungtod C . Occupational health problems and lifestyle changes among novice working-from-home workers amid the COVID-19 pandemic. Saf Health Work. (2021) ;12: (3):384–9. |
[37] | Moretti A , Menna F , Aulicino M , Paoletta M , Liguori S , Iolascon G . Characterization of home working population during COVID-19 emergency: A cross-sectional analysis. Int J Environ Res Public Health. (2020) ;17: (17):6284. |
[38] | Niu Q , Nagata T , Fukutani N , Tezuka M , Shimoura K , Nagai-Tanima M , et al. Health effects of immediate telework introduction during the COVID-19 era in Japan: A cross-sectional study. PLoS One. (2021) ;16: (10):e0256530. |
[39] | Seva RR , Tejero LMS , Fadrilan-Camacho VFF . Barriers and facilitators of productivity while working from home during pandemic. J Occup Health. (2021) ;63: (1):e12242. |
[40] | Farooq R , Sultana A . The potential impact of the COVID-19 pandemic on work from home and employee productivity. Meas Bus Excel. (2022) ;26: (3):308–25. |
[41] | Boles M , Pelletier B , Lynch W . The relationship between health risks and work productivity. J Occup Environ Med. (2004) ;46: (7):737–45. |
[42] | Mitchell RJ , Bates P . Measuring health-related productivity loss. Popul Health Manag. (2011) ;14: (2):93–8. |
[43] | Kemp AH , Quintana DS . The relationship between mental and physical health: Insights from the study of heart rate variability. Int J Psychophysiol. (2013) ;89: (3):288–96. |
[44] | Ohrnberger J , Fichera E , Sutton M . The relationship between physical and mental health: A mediation analysis. Soc Sci Med. (2017) ;195: :42–9. |
[45] | Sardeshmukh SR , Sharma D , Golden TD . Impact of telework on exhaustion and job engagement: A job demands and job resources model: Impact of telework on exhaustion and job engagement. New Technol Work Employ. (2012) ;27: (3):193–207. |
[46] | López-Igual P , Rodríguez-Modroño P . Who is teleworking and where from? Exploring the main determinants of telework in Europe. Sustainability. (2020) ;12: (21):8797. |
[47] | Zajacova A , Lawrence EM . The relationship between education and health: Reducing disparities through a contextual approach. Annu Rev Public Health. (2018) ;39: :273–89. |
[48] | Hobbs D , Armstrong J . An experimental study of social and psychological aspects of teleworking. Facilities Facilities. (1998) ;16: (12–13):366–71. |
[49] | Beauregard TA , Basile KA , Canonico E . Telework: Outcomes and Facilitators for Employees. In: LandersRN, editor. The Cambridge Handbook of Technology and Employee Behavior. Cambridge, TAS, Australia: Cambridge University Press; (2019) . |
[50] | Crawford JO , MacCalman L , Jackson CA . The health and well-being of remote and mobile workers. Occup Med (Lond). (2011) ;61: (6):385–94. |
[51] | Joshi SM . The sick building syndrome. Indian J Occup Environ Med. (2008) ;12: (2):61–4. |
[52] | Wang J , Li B , Yang Q , Wang H , Norback D , Sundell J . Sick building syndrome among parents of preschool children in relation to home environment in Chongqing, China. Chin Sci Bull. (2013) ;58: (34):4267–76. |
[53] | Vargas Llave O , Mandl I , Weber T , Wilkens M . Telework and ICT-based mobile work: Flexible working in the digital [Internet, cited 2022 Oct 4]]. Eurofound; 2020. Available from: http://eurofound.link/efs009 |
[54] | Oakman J , Kinsman N , Stuckey R , Graham M , Weale V . A rapid review of mental and physical health effects of working at home: How do we optimise health? BMC. BMC Publi. (2020) ;20: (1):1–13. |
[55] | Palumbo R . Let me go to the office! An investigation into the side effects of working from home on work-life balance. Int J Publ Sect Manag. (2020) ;33: (6/7):771–90. |
[56] | Shukla A , Srivastava R . Development of short questionnaire to measure an extended set of role expectation conflict, coworker support and work-life balance: The new job stress scale. Cogent Bus Manag. (2016) ;3: (1):1. |
[57] | Kossek EE , Lautsch BA , Eaton SC . Telecommuting, control, and boundary management: Correlates of policy use and practice, job control, and work–family effectiveness. J Vocat Behav. (2006) ;68: (2):347–67. |
[58] | Wiesenfeld BM , Raghuram S , Garud R . Communication patterns as determinants of organizational identification in a virtual organization. Organ Sci. (1999) ;10: (6):777–90. |
[59] | Amerio A , Brambilla A , Morganti A , Aguglia A , Bianchi D , Santi F , et al. COVID-19 lockdown: Housing built environment’s effects on mental health. Int J Environ Res Public Health. (2020) ;17: (16):5973. |
[60] | Blasio D , Shtrepi S , Puglisi L , Astolfi GE . A cross-sectional survey on the impact of irrelevant speech noise on annoyance, mental health and well-being. Int J Environ Res Public Health. (2019) ;16: (2):280. |
[61] | Boegheim B . Relationships between mental health and indoor environmental quality (IEQ) in the workplace at home; An explorative case study using both subjective IEQ experience and objective IEQ sensor data during the COVID-19 pandemic. Eindhoven: Eindhoven University of Technology; (2020) . |
[62] | Xiao Y , Becerik-Gerber B , Lucas G , Roll SC . Impacts of working from home during COVID-19 pandemic on physical and mental well-being of office workstation users. J Occup Environ Med. (2021) ;63: (3):181–90. |
[63] | Kurkland NB , Bailey DE . The advantages and challenges of working here, there anywhere, and anytime. Organ Dyn. (1999) ;28: (2):53–68. |
[64] | Golden TD , Veiga JF , Simsek Z . Telecommuting’s differential impact on work-family conflict: Is there no place like home? J Appl Psychol. (2006) ;91: (6):1340–50. |
[65] | Bergefurt L , Appel-Meulenbroek R , Maris C , Arentze T , Weijs-Perrée M , de Kort Y . The influence of distractions of the home-work environment on mental health during the COVID-19 pandemic. Ergonomics. (2022) ;1-18. ahead of print. |
[66] | Brough P , Timms C , O’Driscoll MP , Kalliath T , Siu O-L , Sit C , et al. Work–life balance: A longitudinal evaluation of a new measure across Australia and New Zealand workers. Int J Hum Resour Manag. (2014) ;25: (19):2724–44. |
[67] | Kroenke K , Spitzer RL . The PHQ- A new depression diagnostic and severity measure. Psychiatr Ann. (2002) ;32: (9):509–15. |
[68] | Schaufeli WB , Bakker AB . Utrecht work engagement scale Preliminary Manual Version 1.1. Occupational Health Psychology Unit. (2004) . |
[69] | Golden TD , Veiga JF , Dino RN . The impact of professional isolation on teleworker job performance and turnover intentions: Does time spent teleworking, interacting face-to-face, or having access to communication-enhancing technology matter? Journal of Applied Psychology. (2008) ;93: (6):1412–21. |
[70] | James LR , Brett JM . Mediators, moderators, and tests for mediation. J Appl Psychol. (1984) ;69: (2):307–21. |
[71] | Kenny DA , Kashy D , Bolger N . Data analysis in social psychology. In: GilbertD, FiskeS, LindzeyG, editors. Handbook of Social Psychology. McGraw-Hill College; (1998) , pp. 233–65. |
[72] | Finney SJ , Distefano C . Non-normal and categorical data in structural equation modeling. In: HancockGR, MuellerRO, editors. Structural equation modeling: A second course. Greenwich, CT: Information Age Publishing; (2006) , pp. 269–314. |
[73] | Byrne BM . Structural equation modeling with lisrel, prelis, and simplis: Basic concepts, applications, and programming. Psychology Press; (2013) . |
[74] | Schumacker RE , Lomax RG . A beginner’s guide to structural equation modeling: Fourth edition. 4th ed. London, England: Routledge; (2015) . |
[75] | Thompson CA , Prottas DJ . Relationships among organizational family support, job autonomy, perceived control, and employee well-being. J Occup Health Psychol. (2006) ;11: (1):100–18. |
[76] | Andel SA , Shen W , Arvan ML . Depending on your own kindness: The moderating role of self-compassion on the within-person consequences of work loneliness during the COVID-19 pandemic. J Occup Health Psychol. (2021) ;26: (4):276–90. |
[77] | Pieh C , Budimir S , Probst T . The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J Psychosom Res. .(2020) ;136(110186):110186. |
[78] | Weitzer J , Papantoniou K , Seidel S , Klösch G , Caniglia G , Laubichler M , et al. Working from home, quality of life, and perceived productivity during the first 50-day COVID-19 mitigation measures in Austria: A cross-sectional study. Int Arch Occup Environ Health. (2021) ;94: (8):1823–37. |
[79] | Rivkin W , Diestel S , Gerpott FH , Unger D . Should I stay or should I go? The role of daily presenteeism as an adaptive response to perform at work despite somatic complaints for employee effectiveness. J Occup Health Psychol. (2022) ;27: (4):411–25. |
[80] | Leaman A , Bordass B . Productivity in buildings: The ‘killer’ variables. Build Res Inf. (1999) ;27: (1):4–19. |
[81] | Jensen PA , Voordt T . Productivity as a value parameter for FM and CREM. Facilities. (2020) ;39: (5–6):305–20. |
[82] | Guler MA , Guler K , Guneser Gulec M , Ozdoglar E . Working from home during a pandemic: Investigation of the impact of COVID-19 on employee health and productivity: Investigation of the impact of COVID-19 on employee health and productivity. J Occup Environ Med. (2021) ;63: (9):731–41. |


