
Musculoskeletal complaints and associated factors in school children aged between 6 and 13 years in Istanbul during the COVID-19 pandemic: A cross-sectional study
Abstract
BACKGROUND:
Following the first COVID-19 cases in Turkey, face-to-face education was ceased after March 16, 2020 until the end of the educational year (i.e. June 19, 2020) and education was substituted remotely due to confinement.
OBJECTIVE:
This study aims to investigate the frequency of musculoskeletal complaints in school-age children and associated risk factors including reduced physical activity, increased screen time and poor ergonomics conditions in school-age children during the pandemic.
METHODS:
This cross-sectional study included parents or guardians of 960 students aged between 6–13 years old with a non-randomized sampling. A survey was administered consisting of 65 items related with sociodemographic characteristics of the children and family, online education hours, technological device(s) used, screen time, type of physical activity, presence of musculoskeletal problems and poor ergonomics conditions such as incorrect sitting posture.
RESULTS:
Logistic regression results demonstrated that age, excess weight gain, total daily screen time, smartphone use, incorrect sitting posture were associated with musculoskeletal complaints.
CONCLUSION:
The long-term closure of schools due to the pandemic may have led to an increase in musculoskeletal complaints in 6–13 years old children, based on the factors identified in this study, which were excess weight gain, increased screen time and incorrect sitting posture. These findings might help education and health authorities to develop strategies to improve musculoskeletal health of children especially in emergencies such as the pandemic.
1Introduction
Turkey has a young growing population. According to 2020 statistics the ratio of children was 27.2% in 83.5 million people [1]. In Turkey, National Education System begins with first 4 years of primary school followed by a second block of 4 years termed as lower secondary school. At the end of the lower secondary school which is 8th grade, there is a high school entrance examination for the allocation of the students to secondary schools according to their performance in the exam.
Following the first COVID-19 cases in Turkey, face-to-face education was ceased after March 16, 2020 until the end of the educational year (i.e. June 19, 2020) and education was substituted remotely, due to confinement. Turkey has kept primary schools closed for the longest time among OECD countries in the northern hemisphere [2].
For the educational year 2020/2021, children returned to school for face-to-face education, which was scheduled for different weekdays due to pandemic precautions. Face-to-face education was arranged as two days a week for most of the classes except for 8th grades, which could come full schedule depending on the consent of the family. This arrangement lasted for approximately 6.5 months (between September 28, 2020 and April 15, 2021). Afterwards, education was switched to online until the end of the academic year (between April 15 and July 2, 2021). In this second academic year of the pandemic, infrastructure for distance education was improved; teachers and students gained experience from the previous year. Educational platforms differed from school to school. Public schools continued distance education via an official platform of Ministry of National Education, called EBA TV (EIN Education Information Network) broadcast as a TV channel and some of them also performed live lectures on different online platforms. Most of the private schools performed live lectures using online platforms such as Teams and Zoom. Therefore, there was heterogeneity of the platforms and technological resources of children. National Ministry of Education cancelled school exams of this year, except for the high school entrance examination.
Besides, for children and young people under the age of 20, a temporary lockdown was implemented in our country between April 3 and June 5 2020. During the first months of the lockdown, 72% of the parents with children aged 6–13 years stated that screen time of their children had increased to a mean of 6.4 hours per day [3]. Engaging in less physical and social activity together with increased screen time has changed sleeping and eating habits leading to an increase in sedentary lifestyle, obesity, and anxiety in children similar to adults [4]. During the pandemic, psychological stress was shown to increase neck pain [5].
Classrooms have shifted from school to home. Suitability of home environments for learning such as lighting, ventilation, noise insulation, temperature and size of the rooms would be expected to be different from that of school environment [6]. Availability and appropriateness of home furniture and digital resources has become important from an ergonomic point of view [7], as well as the awareness of the parents. Poor ergonomics is an important risk factor for musculoskeletal complaints including ache, pain or discomfort in the affected body site.
This study aims to investigate the frequency of musculoskeletal complaints in school-age children and associated factors such as lack of physical activity and prolonged screen time during the pandemic.
2Methods
2.1Ethical considerations
The study was approved by the Research Ethics Board of the University of Health Sciences and registered on the Clinical Trials Registry under number NCT04954612.
2.2Methodological design
This quantitative study with an analytical cross-sectional design was conducted in Istanbul, Turkey’s most populous mega-city with a population of over 15 million, between May 4, 2021 and July 2, 2021.
2.3Study population
In this study, we included parents/guardians of the children aged 6–13 who attend primary or secondary school in Istanbul. Information about the children was obtained from the literate, internet-enabled parents/guardians of the children who agreed to participate the study.
2.4Inclusion criteria
Inclusion criteria were being a parent or guardian of a child aged between 6 to 13 years who was attending to primary or secondary school in Istanbul and being able to access the internet and fulfill the online questionnaire.
2.5Exclusion criteria
Parents or guardians of disabled children who were attending to the special education school were not included in the study. Children attending to schools out of Istanbul were excluded.
2.6Data collection techniques
A survey assessing musculoskeletal complaints in children and associated factors during online education was structured by two physiatrists and a public health specialist after the review of the relevant literature.
Questions regarding the musculoskeletal complaints were constructed based on The Nordic musculoskeletal questionnaire extended version (NMQ-E) which was translated and validated into Turkish [8]. Presence of complaints (ache, pain or discomfort) in anatomical regions based on the body map of musculoskeletal regions in NMQ-E including neck, shoulder, upper back, elbow, wrist/hands, low back, hips/thighs, ankles, feet in the last one month and seeking treatment due to ache, pain or discomfort in those body regions were questioned with binary choices (yes or no) asking the following two questions:
• Has your child ever had any complaint (ache, pain or discomfort) in his/her neck, shoulder, upper back, elbow, wrist/hands, low back, hips/thighs, ankles, feet?
• Has your child ever presented to hospital due to this complaint (ache, pain or discomfort) in his/her neck, shoulder, upper back, elbow, wrist/hands, low back, hips/thighs, ankles, feet?
Other survey questions which are related to screen time, ergonomic sitting position and posture were constructed based on the studies by Robbins et al and Majumdar et al. [9, 10].
2.7Variables
The survey consisted of 65 items, including sociodemographic characteristics of the children and family (17 items including questions related to child’s date of birth, gender, weight, height, number of siblings, chronic disease status, school type (public/private), grades of class, education level of parents, mothers’ employment status), education hours (6 items including weeks of online and face-to-face education, days of online and face-to-face education per week, number of online lectures per day, duration of online lectures) and technological device(s) used (1 item), screen time (2 items, total hours of screen time in a day, longest screen time in a day without a break) and physical activity (2 items, participation in sports/physical activity before and after pandemic), presence of musculoskeletal problems (27 items) and ergonomic conditions (10 items questioning type of the room the child used during remote education (kitchen, living room, private room etc.), table type (e.g. kitchen table, his/her own study table, coffee table), sitting position, screen viewing distance). Body mass index z score adjusted to age and gender of the children was calculated with the weight and height information obtained from the survey [11]. The questionnaire was created using the Qualtrics program.
The survey was piloted among ten participants to ensure its readability and ease of completion. After obtaining permissions from Ministry of National Education of Turkey, survey link was shared with the school principals so that they distributed the survey to the guardians of children via smart phones or email. The survey was available for one month and a reminder was sent once a week.
2.8Sample size calculation
For the educational year 2020/2021, Turkish National Education Statistics reported that Istanbul had a total of 1,825,209 students in primary and lower secondary schools with 88.4% of them in public education institutions [12]. A sample size of 784 participants was calculated by assuming a musculoskeletal problems prevalence of 15% [13] among children between the ages 6–13, with a confidence limit of 95% and with an absolute precision 2.5%. The sample size estimation analysis was performed using Open Epi program. We used a non-probability sampling strategy.
2.9Statistical analysis
Survey responses were analyzed by IBM SPSS for Windows version 28 software (IBM Corp., Armonk, NY, USA). The histogram and normality plots and Kolmogorov-Smirnov test normality test were used for data distribution analysis. Analysis of the characteristics of participants was performed using descriptive statistics. A chi-square test was used for the comparison of categorical variables while the student t test was used for the comparison of continuous variables. Bivariate analyses and then logistic regression analysis were performed for the relationship of independent variables with musculoskeletal complaints. A p value below 0.05 was considered statistically significant.
3Results
A total of 1337 parents or guardians participated in the online survey; 960 participants who completed the questionnaire completely were included in the analysis. Respondents were mainly mothers (87.1%), fathers (12.5%), or other relatives (0.4%) of the children. Proportions of parents that completed at least 8 years of education were 83.2% in mothers and 88.0% in fathers. Less than half of mothers (42.7%) and 96.4% of fathers were employed. Number of children was two in 54% and ≥ 3 in 24% of the families. Number of children aged 6 – 13 years was 1, 2 or 3 in 58%, 33% or 5% of the families, respectively. Majority of children (82.8%) were attending to a public school (n = 795).
Mean age of children was 10.1 (sd = 2.1) years and 55% of them were boys. Body mass index z-scores were 0.57 (sd = 1.19). Frequencies of overweight (z-score > 1.0), obese (z-score > 2.0), and thin (z-score < –2.0) were 32.4%, 6.6% and 2.7%, respectively. A chronic disease was reported in 68 (7%) of all children, most commonly asthma (n:17, 0.018%) or allergy (n:11, 0.011%). There were 6 children (0.006%) reported to have orthopaedic disorders. A total of 89 children had COVID-19 infection (9.3%) between the onset of the pandemic and the period during which the study was conducted (Table 1).
Table 1
Demographic variables of the children
| Variable | n (%) |
| Age, years (mean±SD) (n = 960) | 10.1±2.1 |
| Gender (n = 960) | |
| Boys | 532 (55.4) |
| Girls | 428 (44.6) |
| BMI, z score (n = 929) | 0.57±1.19 |
| School (n = 960) | |
| Public | 165 (17.2) |
| Private | 795 (82.8) |
| Grades (n = 960) | |
| 1 | 137 (14.3) |
| 2 | 155 (16.1) |
| 3 | 127 (13.2) |
| 4 | 106 (11.0) |
| 5 | 131 (13.6) |
| 6 | 102 (10.6) |
| 7 | 140 (14.6) |
| 8 | 62 (6.5) |
| History of COVID-19 infection (n = 960) | 89 (9.3) |
| Survey responder (n = 960) | |
| Mother | 836 (87.1) |
| Father | 120 (12.5) |
| Other | 4 (0.4) |
All students attended online education during the year with variable duration. More than half of the children (53.8%) had never attended to face-to-face education and completed the education year remotely, while 46.3% of them (444 children) attended to face-to-face education for different periods during the educational year 2020/2021. Among children attended to face-to-face education, 81.5% (n = 362) went to school for less than 12 weeks in total and 80.2% (n = 356) went to school for 2 days a week. Table 2 shows the number of online education days per week, number of online lectures per day and duration of online lectures. Accordingly, 83% of all children had 5 or more days of online education and 90% had 5 or more lectures per day. Duration of lectures varied between 30–39 minutes in more than half of the children.
Table 2
Number of online education days per week, number of online lectures per day and duration of online lectures (N = 960)
| Variable | n (%) |
| Days of online education per week | |
| ≤ 4 | 160 (16.7) |
| 5 | 656 (68.3) |
| ≥6 | 144 (15.0) |
| Number of online lectures per day | |
| ≤ 4 | 101 (10.5) |
| 5 | 147 (15.3) |
| 6 | 432 (45.0) |
| 7 | 164 (17.1) |
| ≥8 | 116 (12.1) |
| Duration of an online lecture, min | |
| <20 | 10 (1.0) |
| 20–29 | 222 (23.1) |
| 30–39 | 553 (57.6) |
| 40–49 | 112 (11.7) |
| >50 | 63 (6.5) |
Digital devices used for remote education were tablet (38%), laptop (44%), desktop (17%), smartphone (29%), and television (5%). These were also the most common devices used for leisure time activities. Average total screen time in a day was 6.6 (sd = 2.8) hours (min – max: 0.5 – 13) and longest screen time at a time without a break estimated by parents was 56.1 minutes (sd = 41.6); (min – max: 20 – 190). 38% of children spent ≥8 hours on the screen in a day and % 41 of children had ≥50 minutes of screen time at a time without a break
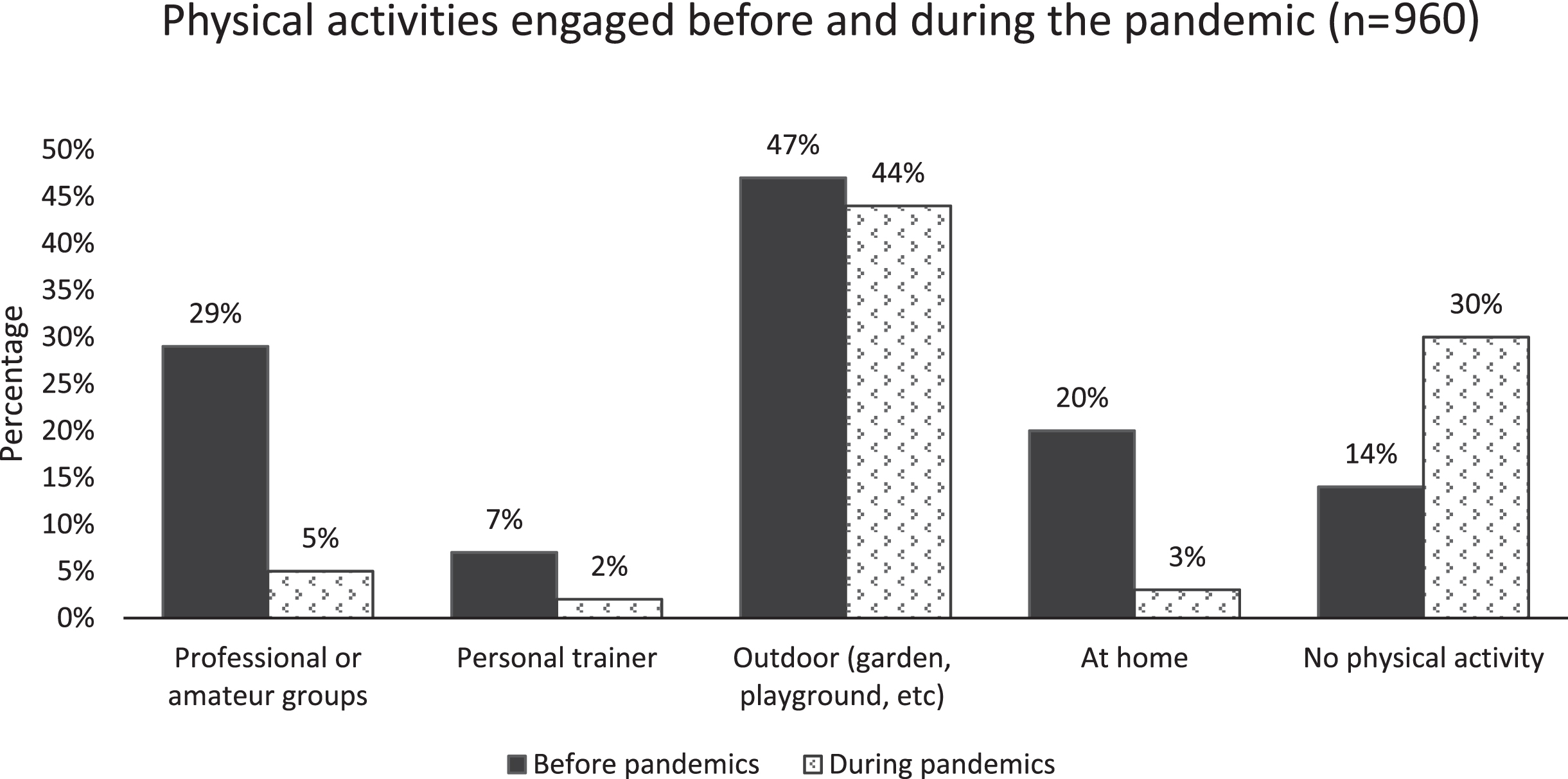
Of 960 participants, 35.1% thought that their children gained weight more than normal, 44.1% thought their children gained appropriate weight according to their development; 18.3% reported no change and 2.5% reported weight lost during the pandemic. Physical activities engaged before and during the pandemic are given in Fig. 1. Accordingly, the frequency of physical activity in all of the kinds decreased during the pandemic; however, activities at home and sedentary behavior increased (p < 0.001 for each comparison).
Fig. 1
Physical activities engaged before and during the pandemic (n = 960). (Differences between all activities before and during the pandemic were statistically significant, p < 0.001 for each).
Regarding study environment at home during online education, 46% of the respondents thought that it was ergonomic for their children, whereas 23% thought their environment was not ergonomic and 31% were uncertain or not able to evaluate. Places which children continued online education were their own room (76%), living room (41%), kitchen (5%) or another location (4%). Study tables used were their own desk (78%), dining table (23%) or different surfaces (coffee table (9%), sofa (6%), bed (6%), or some other places (2%).
Regarding posture and sitting position during online education, 24% of the participants thought that their children had correct posture, whereas 47% thought their posture were not appropriate and 29% were uncertain or did not know. Percentage of parents reporting that their children’s feet touch the floor was 58%, back rest at the chair support 33%, upper part of the screen was at the eye level 73%, and the screen was at arm length distance 71%.
Prevalence of musculoskeletal problems, healthcare seeking behaviour and treatment needed are provided in Fig. 2. Accordingly, 47.5% of the children experienced some kind of musculoskeletal problems. Children with musculoskeletal problems were older and in higher grades than those without complaints (p < 0.001) (Table 3). Prevalence of chronic diseases and weight gain during the pandemic was higher in children with complaints (p = 0.004 and p = 0.005, respectively). Total screen time in a day and longest duration of screen time at a time without break was higher among children with musculoskeletal complaints (p < 0.001 and p = 0.002, respectively). Number of parents reporting inappropriate study environment was higher in children with musculoskeletal complaints (p = 0.001) (Table 4).
Fig. 2
Prevalence of musculoskeletal problems in the last month.
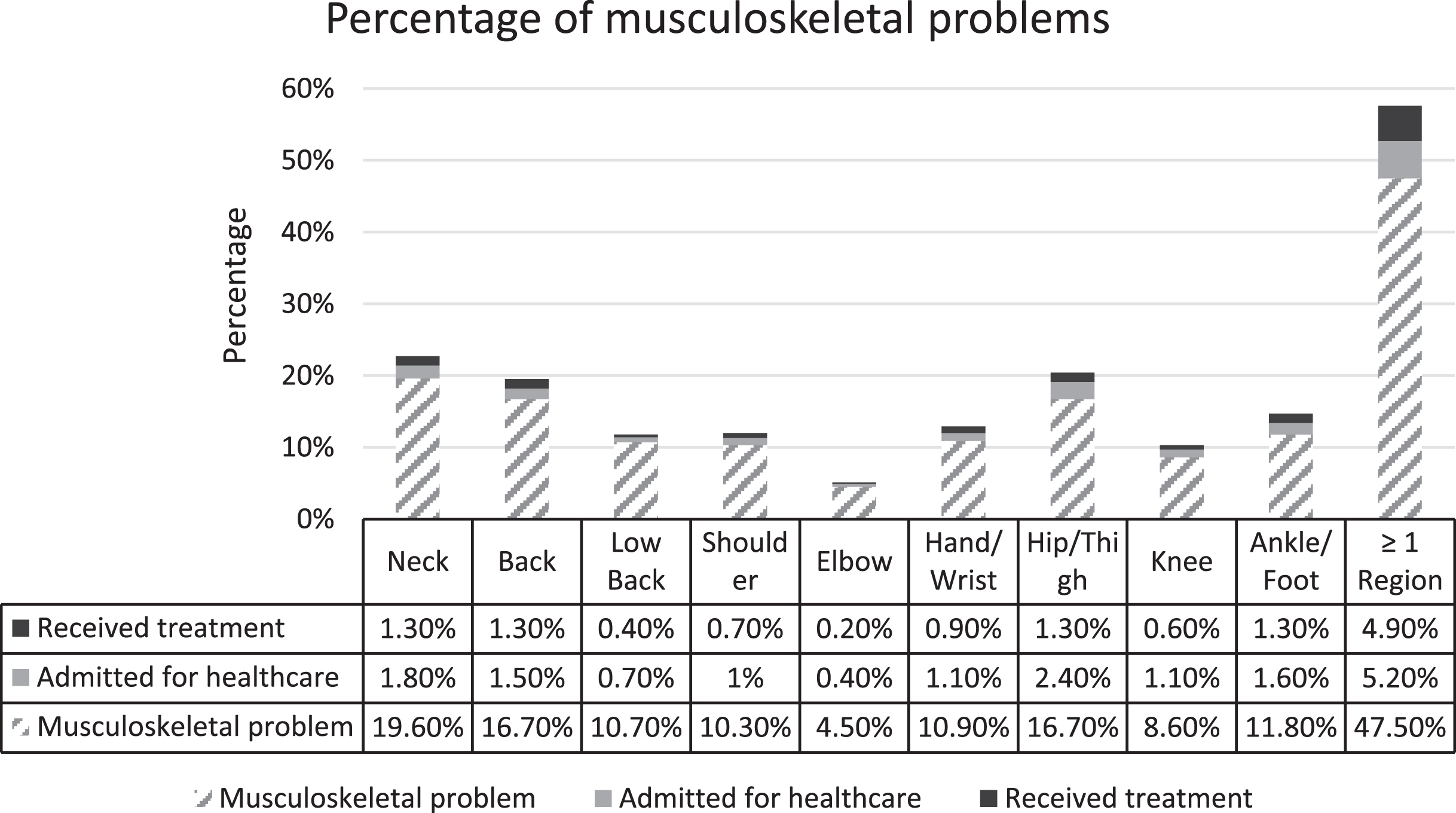
Table 3
Demographic and educational parameters in children with and without musculoskeletal complaints
| Variable | Children with a musculoskeletal complaint (n = 456) | Children without a musculoskeletal complaint (n = 504) | p |
| Age, years | 10.4±2.1 | 9.8±2.1 | <0.001a |
| Gender, boys, % | 55.5 | 55.4 | 1.000 |
| BMI z-score | 0.61±1.16 | 0.54±1.23 | 0.394 |
| Presence of chronic disease, % | 9.6 | 4.8 | 0.004b |
| History of COVID-19 infection, % | 9.9 | 8.7 | 0.578 |
| Type of school, % | |||
| Public | 80.0 | 85.0 | 0.049 |
| Private | 20.0 | 15.0 | |
| Grade | 4.5±2.2 | 3.9±2.2 | <0.001c |
| Face-to-face education | |||
| Total weeks in a year | 3.0±4.5 | 3.2±4.6 | 0.567 |
| Days in a week | 1.1±1.4 | 1.0±1.3 | 0.374 |
| Online education | |||
| Days in a week | 4.8±1.2 | 4.7±1.3 | 0.105 |
| Number of lectures in a day | 6.1±1.5 | 6.0±1.4 | 0.127 |
| Duration of a lecture, min | 37.3±14.5 | 36.4±13.9 | 0.371 |
aStudent’s t test; bChi square test; cMann-Whitney U test.
Table 4
Ergonomic and postural parameters in children with and without musculoskeletal complaints
| Variable | Children with a musculoskeletal complaint (n = 456) | Children without a musculoskeletal complaint (n = 504) | p |
| Screen time | |||
| Total time in a day, hours | 7.0±2.9 | 6.2±2.6 | <0.001a |
| Longest time without a break, min | 60.4±45.3 | 52.2±37.6 | 0.002b |
| Digital device users, % * | |||
| Television | 47.8 | 48.4 | 0.897c |
| Desktop computer | 22.4 | 16.9 | 0.034c |
| Laptop computer | 45.6 | 48.4 | 0.212c |
| Tablet | 54.8 | 52.6 | 0.517c |
| Smartphone | 64.5 | 53.2 | <0.001c |
| Ergonomic study environment, % | |||
| Appropriate | 39.9 | 51.6 | 0.001c |
| Inappropriate | 26.3 | 19.6 | |
| Not known | 33.8 | 28.8 | |
| Sitting posture, % | |||
| Correct | 17.8 | 30.4 | <0.001c |
| Incorrect | 55.7 | 39.5 | |
| Not known | 26.5 | 30.1 | |
| Feet touch the floor % | 56.8 | 59.9 | 0.359c |
| Back rest at the chair support % | 28.1 | 38.1 | 0.001c |
| Upper part of the screen at eye level % | 68.1 | 77.2 | 0.002c |
| Screen at arm length distance % | 63.6 | 77.2 | <0.001c |
| Physical inactivity during the pandemic, % | 49.6 | 48.4 | 0.747c |
| Abnormal weight change, % | |||
| Excess weight gain | 40.4 | 30.3 | 0.005c |
| Weight loss | 2.4 | 2.6 | |
| Unchanged | 17.5 | 19.0 | |
| Age-appropriate weight gain | 39.7 | 48.0 |
*This item was prepared as respondents could choice more than one alternative. aMann-Whitney U test; bStudent’s t test. cChi square test.
Number of children admitted to healthcare due to musculoskeletal problems was 74 (16.2%) and they were older (10.7±2.0 vs 10.1±2.1 years, p = 0.019), had longer duration of online lectures (40.7±27.3 vs 36.5±13.9 min, p = 0.044) when compared to the rest of the children. Fifty-one children (68.9%) were treated for their musculoskeletal problems. These children had higher prevalence of chronic diseases (15.7%, 6.6%, p = 0.023) and attended to less weeks of face-to-face education (1.86±3.10 vs 3.21±4.60 weeks, p = 0.005) when compared to the rest of the children.
Logistic regression analysis results demonstrated that age (OR: 1.11, 95% : 1.04–1.19), excess weight gain (OR: 1.38, 95% : 1.01–1.87), total daily screen time (OR: 1.06, 95% : 1.01–1.12), smartphone use (OR: 1.49, 95% : 1.12–1.99), and incorrect sitting posture (OR: 1.89, 95% : 1.31–2.72) were associated with musculoskeletal problems (Table 5).
Table 5
Logistic regression analysis of predictors of musculoskeletal problems
| Variable | B | OR (95% CI) | p |
| Age, years | 0.108 | 1.11 (1.04–1.19) | 0.002 |
| Total daily screen time, hours | 0.060 | 1.06 (1.01–1.12) | 0.029 |
| Weight change, % | |||
| Age-appropriate weight gain | 1 | ||
| Excess weight gain | 0.322 | 1.38 (1.01–1.87) | 0.041 |
| Weight loss/unchanged | 0.087 | 1.09 (0.76–1.56) | 0.633 |
| Smartphone, % | |||
| Not user | 1 | ||
| User | 0.401 | 1.49 (1.12–1.99) | 0.006 |
| Sitting posture, % | |||
| Correct | 1 | ||
| Incorrect | 0.637 | 1.89 (1.31–2.72) | <0.001 |
| Not known | 0.210 | 1.23 (0.83–1.81) | 0.286 |
OR: Odds ratio, CI: Confidence interval. Variables entered into the analysis; age, gender, change of weight during the pandemic, physical activity during the pandemic, type of school, total daily screen time, desktop computer use, smartphone use, tablet use, ergonomic environment, sitting posture. Only the variables found statistically significant are included in this table.
When associations of musculoskeletal problems were analysed separately according to the nine body regions; age was higher in neck, shoulder, back, and low back pain (p < 0.001 for each) but not in elbow, hand/wrist, hip/leg, knee, or ankle/foot. Excess weight gain during the pandemic was significantly higher in neck (p = 0.002), shoulder (p = 0.047), back (p = 0.011), hand/wrist (p = 0.001), low back (p = 0.004), and ankle/foot (p = 0.011), but not in elbow, hip/leg or knee complaint. Total screen time was longer in neck (p = 0.021), shoulder (p = 0.020), back (p < 0.001), low back (p = 0.021), knee (p = 0.029), ankle/foot (p = 0.001) but not in elbow, hand/wrist or hip/leg complaints.
Regarding the associations between the sitting posture and musculoskeletal problems in different body regions; percentage of feet not touching the floor was only higher in children with elbow problems (58.1% vs 40.8%, p = 0.027). Back not resting at chair support was higher in children with neck (p = 0.002), back (p < 0.001), and low back problems (p = 0.003) but not in children with shoulder, elbow, hand/wrist, hip/leg, knee or ankle/foot problems. Children who did not use screen right in front or upper part of the screen at the eye level had higher back problems (p = 0.007), but not neck, shoulder, elbow, hand/wrist, low back, hip/leg, knee or ankle/foot problems. Children who did not have screen distance at an arm length reported neck (p < 0.001), shoulder (p = 0.014), back (p = 0.004), low back (p = 0.001), hip/leg problems (p < 0.001) but not elbow, hand/wrist, knee or ankle/foot problems.
Regarding digital devices used, smartphone users had higher rate of musculoskeletal complaints, especially in the neck (p = 0.019), back (p = 0.003), low back (p = 0.008) and hip/leg regions (p = 0.018). Desktop computers users had higher rate of neck (p = 0.023), shoulder (p = 0.016), hand/wrist (p = 0.021), hip/leg (p = 0.023) complaints. TV or laptop users did not have any increased rate for complaints in any of the nine regions.
4Discussion
The present study has investigated musculoskeletal complaints and associated factors such as screen time, physical activity, weight change and ergonomic conditions in school children aged between 6 and 13 years in Turkey during the COVID-19 pandemic. Our study showed that almost half of the children (47.5%) experienced some kind of musculoskeletal complaint during the pandemic. This frequency is greater than the previously reported numbers of 8% [14], 15% [13] and 4–40% [15] among children aged between 6 and 13 years. There can be several possible explanations for this higher prevalence. The frequency of musculoskeletal complaints may have been overreported due to non-random sampling. On the other hand, this may be a real increase as schools have been closed for a long time due to the pandemic and children are more exposed to factors that increase musculoskeletal problems. Even in such case, it is important to note that only 16% of them sought help for their complaints.
There was no difference between boys and girls in contrast to the previous studies with higher frequency in boys [14, 16]. However, children who were older, who had a higher prevalence of chronic disease, gained excess weight during the pandemic, and whose parents reported higher estimated screen time and inappropriate sitting posture were more likely to have musculoskeletal complaints. Although having a chronic disease was statistically significant in bivariate analysis, we did not include it in the logistic regression analysis because parents of children with chronic disease may be more likely to report musculoskeletal complaints.
Schoolchildren are exposed to ergonomic risk factors such as sitting posture for long hours and inadequate furniture because they spend most of their times related to school activities such as listening to lessons, writing and reading while seated [17]. Prolonged screen time also causes impaired posture and reduced physical activity in children [18]. During listening lessons, children often sit with poor posture for long periods, forcing their spine into an awkward position by having their trunk, back, and neck flexed or rotated. Awkward position and prolonged sitting with a lack of exercise contribute to musculoskeletal pain in school-aged children [19]. Musculoskeletal problems seen in school-aged children are frequently related to bad posture and infrequent breaks while using technologic devices such as computers, tablets and smartphones [10]. During the COVID-19 pandemic, a transition from face-to-face to a distance education process occurred at schools via digital devices due to COVID-19 precautions. In school-aged-children continuing their education with computers, tablets, smart phones or TV staying at a static position by repeated movements such as using a keyboard, clicking on a mouse or TV remote, usage of the body in incorrect positions and the inadequate ergonomic conditions in the learning environment led to musculoskeletal pain [18].
Children with musculoskeletal pain had higher rates of total screen time in a day and the longest screen time without a break. As the total screen time increased, we found increased risk of musculoskeletal pain similar to previous studies [20–23].
The use of digital devices has increased widely among students during the COVID-19 pandemic due to shifting to e-learning and led to several musculoskeletal complaints. In present study musculoskeletal pain was more common in children using smartphone. Due to growing use of computer and mobile device in young population musculoskeletal problems especially neck and shoulder pain has increased [24]. Many studies represented that mobile phone texting is significantly associated with neck pain [24–26]. In present study smartphone users had higher rate of musculoskeletal complaints, especially in the neck, back, low back and hip/leg regions. A study that analyse the spinal segment kinematics during smartphone and computer typing in sitting position reported that smartphone using causes larger degrees of cervical and thoracic flexion compared to desktop typing and in contrast lumbar flexion was greater in desktop typing. Thoracic flexion could be a compensatory mechanism to avoid further cervical flexion in smartphone users. This altered kinematics may be associated with pain [24]. Prolonged neck flexion is linked to neck, shoulder, and upper extremity pain [26]. Considering the kinematics of adjacent spinal segments which affect each other [24], it could be understood that head and neck posture and thoracolumbar posture interact each other and cause discomfort or pain. The best position using smartphone is recommended as sitting position with a straight neck and supporting the forearms while holding the phone with both hands and using both thumbs [26].
In our study, we found that smartphone use was 1.3 times higher among children in 10–14 age group compared to 6–9 age group. Similarly total daily screen time was 1 hour longer among older children. This may explain the association between increased age and musculoskeletal complaints.
The size and usage manner are different between digital devices, so it could be expected that it could cause different symptom patterns as present study. In another study overall pain location were similar to this study and most frequent region was neck. However, lower back, wrist, hand and thumb were more common sites in smartphone users and arms and shoulders were more prominent pain locations among tablet users [27]. In present study, there was increased rate of complaints in neck, shoulder, hand/wrist, hip/leg in desktop users. TV or laptop users did not have any increased rate for complaints in any regions. Similarly, in 50% of university students, using electronic devices was associated with neck and shoulder pain followed by wrist/hand, lower and upper back pain [28]. According to a systematic review, large amount of mobile device users experiences musculoskeletal problems with the highest prevalence in neck (17–86%). Sustained neck flexion could be the key factor which cause compressive loading on the cervical spine [25]. Using laptop computer causes both neck and shoulder flexion. Neck flexion and pain are greater when using the computer in sofa and bed than in table, but shoulder flexion and shoulder muscle activity is greater in working at table [29]. Likewise, desktop using in sitting position cause increased shoulder muscle activity and less neutral shoulder posture and, sitting without back support leads either supporting upper body weight with their spine or placing forearm on the desk with leaning forward [30]. Also, wrist deviation from neutral with these positions could lead to median nerve deformation [31]. Similar to our results, university students using desktop, laptop or tablet during e-learning due to pandemic reported neck (32%), shoulder (25%) and back pain 15% [26]. It is important to guide the students and the caregivers about the best body position during e-learning and teach the appropriate exercises for trunk and extremity muscles.
In present study, 32.4% of children was overweight and, 6.6% of them obese; in addition, 35% of parents reported that their children gained weight more than normal in pandemic. School provides a structured routine in meals, physical activity and sleep that implicated in obesity risk. With lock-down due to pandemic, children in different parts of the world gained weight, this could be related to increased food intake, physical inactivity, increased screen time or increased in snacking [4]. Presence of musculoskeletal complaints was higher in children with weight gain (40%) than those with no weight gain (30%) in present study. A systematic review reported that there is positive association between overweight in childhood and musculoskeletal pain, the prevalence is 26% higher in overweight children than in normal weight children. Also, there is small positive association with low back pain. Various mechanisms underlie these relationships like reduced physical activity [32]. The causes of higher pain prevalence in present study could be longer inappropriate posture and sitting position, decreased physical activity levels and increase in sedentary behavior. Weight gain during the pandemic was significantly higher in neck, shoulder, back, hand/wrist, low back, and ankle/foot, but not in elbow, hip/leg or knee complaint in this study. Obesity could be associated with increased pain in more body locations and increased pain intensity when compared with normal weight. Physical inactivity could play role in pain intensity and lower limb pain. Due to increased loading and biomechanical alterations, weight gain is a possible contributor to musculoskeletal pain and total body mass is related musculoskeletal pain rather than adiposity [33].
4.1Strengths
To the best of our knowledge, this is the first study that examines musculoskeletal problems in children during the COVID-19 pandemic in a country like Turkey where schools were closed for the longest time (among OECD countries).
4.2Limitations
Information relied on the observation and report of the parents. There may be some recall bias if the child has told some symptoms, parents might pay more attention to their children’s posture and study environment, realizing the mismatches. Similarly, parents of children who spend a long time in front of a screen or are physically inactive may be more inclined to report children’s musculoskeletal complaints. This problem also arises from the cross-sectional nature of the study. The non-random sampling method of the study can also be considered as another limitation.
5Conclusion
We found that about half of children aged 6–13 years experienced musculoskeletal complaints during the COVID-19 pandemic. The long-term closure of schools due to the pandemic may have led to this increase in musculoskeletal complaints, based on the factors determined in this study. These findings might help education and health authorities to develop strategies to improve musculoskeletal health of children especially in emergencies such as the pandemic. The reporting of some parents that they could not evaluate whether their children’s sitting position or ergonomics is appropriate demonstrates the importance of training the children and their families regarding the safe and rational use of digital devices, appropriate sitting posture and ergonomics.
Ethics statement
The study was approved by the Research Ethics Board of the University of Health Sciences and registered on the Clinical Trials Registry under number NCT04954612.
Informed consent
The ‘Informed Volunteer Participation Form’ was included in the questionnaire and the parents who agreed to participate in the study were included in the study.
Conflict of interest
The authors declare that they have no conflict of interest.
Acknowledgments
The authors have no acknowledgments.
Funding
The authors report no funding.
References
[1] | Institute TS. Statistics of Children, 2020. https://data.tuik.gov.tr/Bulten/Index?p=Istatistiklerle-Cocuk-2020-37228: Turkish Statistical Institute; 2021 April 20, 2021. Contract No.: 37228. |
[2] | The State of School Education: One Year into the COVID Pandemic, OECD Publishing, Paris. 2021. |
[3] | Ozturk Eyimaya A , Yalcin Irmak A . Relationship Between Parenting Practices and Children’s Screen Time During the COVID-19 Pandemic in Turkey. J Pediatr Nurs. (2021) ;56: :24–9. |
[4] | Cena H , Fiechtner L , Vincenti A , Magenes VC , De Giuseppe R , Manuelli M , et al. COVID-19 Pandemic as Risk Factors for Excessive Weight Gain in Pediatrics: The Role of Changes in Nutrition Behavior. A Narrative Review. Nutrients. (2021) ;13(12). |
[5] | Daher A , Halperin O . Association between Psychological Stress and Neck Pain among College Students during the Coronavirus Disease of 2019 Pandemic: A Questionnaire-Based Cross-Sectional Study. Healthcare (Basel). (2021) ;9(11). |
[6] | Soltaninejad M , Babaei-Pouya A , Poursadeqiyan M , Feiz Arefi M . Ergonomics factors influencing school education during the COVID-19 pandemic: A literature review. Work. (2021) ;68: (1):69–75. |
[7] | Ayyildiz E , Taskin Gumus A . A novel distance learning ergonomics checklist and risk evaluation methodology: A case of Covid-19 pandemic. Hum Factors Ergon Manuf. (2021) ;31: (4):397–411. |
[8] | Alaca N , Safran EE , Karamanlargil A , Timucin E . Translation and cross-cultural adaptation of the extended version of the Nordic musculoskeletal questionnaire into Turkish. Journal of musculoskeletal & neuronal interactions. (2019) ;19: (4):472–81. |
[9] | Majumdar P , Biswas A , Sahu S . COVID-19 pandemic and lockdown: cause of sleep disruption, depression, somatic pain, and increased screen exposure of office workers and students of India. Chronobiology international. (2020) ;37: (8):1191–200. |
[10] | Robbins M , Johnson I , Cunliffe CJCC . Encouraging good posture in school children using computers. (2009) ;12: (1):35–44. |
[11] | Gunoz H , Bundak R , Furman A , Darendeliler F , Saka N , Bas F , et al. Z-score reference values for height in Turkish children aged 6 to 18 years. J Clin Res Pediatr Endocrinol. (2014) ;6: (1):28–33. |
[12] | Presidency MoNESD. National Education Statistics - Formal Education 2020/’21. September 10, 2021 ed2021. pp. 284. |
[13] | Kamper SJ , Williams CM . Musculoskeletal Pain in Children and Adolescents: A Way Forward. J Orthop Sports Phys Ther. (2017) ;47: (10):702–4. |
[14] | Jordan KP , Kadam UT , Hayward R , Porcheret M , Young C , Croft P . Annual consultation prevalence of regional musculoskeletal problems in primary care: an observational study. BMC Musculoskelet Disord. (2010) ;11: :144. |
[15] | King S , Chambers CT , Huguet A , MacNevin RC , McGrath PJ , Parker L , et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain. (2011) ;152: (12):2729–38. |
[16] | Tan A , Strauss VY , Protheroe J , Dunn KM . Epidemiology of paediatric presentations with musculoskeletal problems in primary care. BMC Musculoskelet Disord. (2018) ;19: (1):40. |
[17] | Foltran FA , Moreira RF , Komatsu MO , Falconi MF , Sato TO . Effects of an educational back care program on Brazilian schoolchildren’s knowledge regarding back pain prevention. Revista brasileira de fisioterapia (Sao Carlos (Sao Paulo, Brazil)). (2012) ;16: (2):128–33. |
[18] | Tİgİ A , AltintaşA AjjoetAytar. Rehabilitation. Effects of posture and ergonomics training for students receiving distance education during the covid-19 pandemic on musculoskeletal pain, exercise behavior decision-making balance, and physical activity level. (2020) ;7: (2):137–44. |
[19] | Syazwan A , Azhar MM , Anita A , Azizan H , Shaharuddin M , Hanafiah JM , et al. Poor sitting posture and a heavy schoolbag as contributors to musculoskeletal pain in children: an ergonomic school education intervention program. Journal of Pain Research. (2011) ;4: :287–96. |
[20] | Hakala PT , Saarni LA , Punamäki R-L , Wallenius MA , Nygård C-H , Rimpelä AH . Musculoskeletal symptoms and computer use among Finnish adolescents - pain intensity and inconvenience to everyday life: a cross-sectional study. BMC Musculoskeletal Disorders. (2012) ;13: (1):41. |
[21] | Silva GRR , Pitangui ACR , Xavier MKA , Correia-Júnior MAV , De Araújo RC . Prevalence of musculoskeletal pain in adolescents and association with computer and videogame use. Jornal de Pediatria. (2016) ;92: (2):188–96. |
[22] | Torsheim T , Eriksson L , Schnohr CW , Hansen F , Bjarnason T , Välimaa R . Screen-based activities and physical complaints among adolescents from the Nordic countries. BMC Public Health. (2010) ;10: (1):324. |
[23] | Joergensen AC , Strandberg-Larsen K , Andersen PK , Hestbaek L , Andersen AN . Spinal pain in pre-adolescence and the relation with screen time and physical activity behavior. BMC Musculoskelet Disord. (2021) ;22: (1):393. |
[24] | Xie YF , Szeto G , Madeleine P , Tsang S . Spinal kinematics during smartphone texting - A comparison between young adults with and without chronic neck-shoulder pain. Appl Ergon. (2018) ;68: :160–8. |
[25] | Xie Y , Szeto G , Dai J . Prevalence and risk factors associated with musculoskeletal complaints among users of mobile handheld devices: A systematic review. Appl Ergon. (2017) ;59: (Pt A):132–42. |
[26] | Yaseen QB , Salah H . The impact of e-learning during COVID-19 pandemic on students’ body aches in Palestine. Sci Rep. (2021) ;11: (1):22379. |
[27] | Thorburn E , Pope R , Wang S . Musculoskeletal symptoms among adult smartphone and tablet device users: a retrospective study. Arch Physiother. (2021) ;11: (1):1. |
[28] | Woo EHC , White P , Lai CWK . Musculoskeletal impact of the use of various types of electronic devices on university students in Hong Kong: An evaluation by means of self-reported questionnaire. Man Ther. (2016) ;26: :47–53. |
[29] | Intolo P , Shalokhon B , Wongwech G , Wisiasut P , Nanthavanij S , Baxter DG . Analysis of neck and shoulder postures, and muscle activities relative to perceived pain during laptop computer use at a low-height table, sofa and bed. Work. (2019) ;63: (3):361–7. |
[30] | Lin MY , Barbir A , Dennerlein JT . Evaluating biomechanics of user-selected sitting and standing computer workstation. Appl Ergon. (2017) ;65: :382–8. |
[31] | Woo EHC , White P , Lai CWK . Morphological Changes of the Median Nerve Within the Carpal Tunnel During Various Finger and Wrist Positions: An Analysis of Intensive and Nonintensive Electronic Device Users. J Hand Surg Am. (2019) ;44: (7):610. e1–e15. |
[32] | Paulis WD , Silva S , Koes BW , van Middelkoop M . Overweight and obesity are associated with musculoskeletal complaints as early as childhood: a systematic review. Obes Rev. (2014) ;15: (1):52–67. |
[33] | Tsiros MD , Buckley JD , Howe PR , Walkley J , Hills AP , Coates AM . Musculoskeletal pain in obese compared with healthy-weight children. Clin J Pain. (2014) ;30: (7):583–8. |


