
Returning to work and the impact of post COVID-19 condition: A systematic review
Abstract
BACKGROUND:
The COVID-19 pandemic is still ongoing, with rapidly increasing cases all over the world, and the emerging issue of post COVID-19 (or Long COVID-19) condition is impacting the occupational world.
OBJECTIVE:
The aim of this systematic review was to evaluate the impact of lasting COVID-19 symptoms or disability on the working population upon their return to employment.
METHODS:
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statements we performed a systematic review in December 2021, screening three databases (PubMed, ISI Web of Knowledge, Scopus), for articles investigating return to work in patients that were previously hospitalized due to COVID-19. A hand-searched was then performed through the references of the included systematic review. A quality assessment was performed on the included studies.
RESULTS:
Out of the 263 articles found through the initial search, 11 studies were included in this systematic review. The selected studies were divided based on follow-up time, in two months follow-up, follow-up between two and six months, and six months follow-up. All the studies highlighted an important impact of post COVID-19 condition in returning to work after being hospitalized, with differences based on follow-up time, home Country and mean/median age of the sample considered.
CONCLUSIONS:
This review highlighted post COVID-19 condition as a rising problem in occupational medicine, with consequences on workers’ quality of life and productivity. The role of occupational physicians could be essential in applying limitations to work duties or hours and facilitating the return to employment in workers with a post COVID-19 condition.
1Introduction
In 2020, the Sars-CoV-2 virus (COVID-19) started spreading on a global scale, leading to a COVID-19 pandemic that has been burdening the world for the last two years, from a healthcare, social, and economic perspective.
From an occupational medicine standpoint, the impact COVID-19 had on the workplace has been enormous ever since the start of the pandemic. Since the beginning of the COVID-19 emergency, workers’ susceptibility to anxiety has been very high [1], because a shift occurred to the occupational risks workers were exposed to, as Sars-CoV-2, a biological agent, became a threat to employees worldwide [2]. Furthermore, various workplaces have been affected by the shift from presence to remote working, with a change in work dynamics, duties, and hours, in order to reduce transmission of the virus in the workplace and grant the workers the possibility to continue to work safely from their homes [3]. Working from home was not a viable option for all professions, and many essential workers had to keep working in presence despite the COVID-19 pandemic. Many essential workers, and particularly healthcare workers, have been overloaded with work since the start of the COVID-19 emergency, causing an increase in work-related stress and a decrease in general wellbeing, with an important impact on essential workers’ quality of life [4].
This far, the impact of COVID-19 on workers has been evident where working from home and essential workers were concerned, but it is not limited to this. An emerging occupational impact of the pandemic is the post COVID-19 (or Long COVID-19) condition, defined by the World Health Organization (WHO) as a condition that: “occurs in individuals with a history of probable or confirmed SARS CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms and that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include fatigue, shortness of breath, cognitive dysfunction but also others and generally have an impact on everyday functioning. Symptoms may be new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms may also fluctuate or relapse over time” [5].
According to new estimates by the American Academy of Physical Medicine and Rehabilitation dashboard [6], 23,689,349 million Americans live with Long COVID-19 condition, about 30% of the surviving cases. This alarming data highlights a secondary public health emergency, due to the medical costs that these patients must incur in, but especially due to the influence that these persistent symptoms may have on their productivity or ability to work, as highlighted by the research of Tabacof et al. [7] where the sample of the population taken into consideration has a median age of 44 years.
Furthermore, the impact of COVID-19 has been evaluated mostly in terms of the number of cases, deaths, and admissions to intensive care unit; however, the long-term effects, especially in relation to public health and occupational costs, must also be considered. As reported in the Swedish study by Palstam et al. [8], 11,955 people were subject to recurring sick-leave due to COVID-19 and the physical and psychological functions of the surviving workers were significantly worse than the healthy population, as highlighted in Liao et al.’s [9] study on the long-term effects of COVID-19 on hospitalized healthcare workers, one year after discharge, in Wuhan.
With a rapidly increasing in COVID-19 cases, the postcritical illness management is gaining more and more importance; patients recovering from COVID-19 often have residual impairments, both on laboratory exams and in functional scales, indicating that recovery from this illness, particularly for patients that had to undergo hospitalization or Intensive Care Unit (ICU) stay, might not be without complications and lasting symptoms [10]. Furthermore, according to Pèrez-Gonzàlez et al. [11], Long COVID-19 symptoms are more common in hospitalized than non-hospitalized patients (52.3% vs 38.2%) and Bellan et al. [12] reported that long-term sequelae in patients hospitalized for SARS-CoV-2 pneumonia may persist in about 40% of patients one year after discharge. For this reason, the aim of this systematic review was to investigate return to work in patients after undergoing a hospital stay due to COVID-19.
As highlighted by a systematic review and meta-analysis conducted before the COVID-19 pandemic, return to work after postcritical illness is often delayed (33% at 3 months, 55% at 6 months, and 56% at 12 months) or does not happen at all, causing an impact in the overall quality of life among survivors [13]. As the timeline of the pandemic expands, the post COVID-19 condition is becoming ever more impactful on occupational medicine, as the number of workers affected by it is increasing steeply. The aim of this systematic review is to evaluate the impact of COVID-19 postcritical illness on workers, assessing how many patients have returned to work, after hospitalization or ICU stay, at the time of the follow-ups performed in the included studies.
2Methods
The systematic review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statements [14] in December 2021. The PRISMA Statements suggest to perform the search across multiple databases; therefore, we have chosen three databases due to their relevance in the medical and biomedical fields and due to their bibliometric characteristics: PubMed, ISI Web of Knowledge, and Scopus [15]. The query used to perform the bibliographic search, was the following:
(Covid19 OR “Covid-19” OR “Sars-CoV-2” OR Covid OR Coronavirus OR “long-Covid” OR “post-Covid”)
AND
(negativ* OR recovery OR rehab*)
AND
(“return* to work*” OR “work resum*” OR “return* work*”)
The query was developed following the PICO model, establishing the Problem (P) as COVID-19 illness, the Intervention (I) as recovering from the acute illness (negative swab, recovery or rehabilitation after post-acute illness) since our aim was to evaluate chronic sequelae, as opposed to the acute condition, and the Outcome (O) as returning to work (or failing to return to work). Comparison (C) was not applicable due to the aim of the performed review.
In order to perform a systematic search as inclusive as possible, the hospitalization or ICU stay criteria was not added to the bibliographic search, but articles that did not included hospital patients were excluded from the review by the researchers performing the screening. We have chosen to investigate return to work in patients who underwent a hospital stay because of the scientific evidence that seems to indicate higher post COVID-19 syndrome incidence and higher COVID-19 sequelae in general, in patients that underwent a hospital stay due to COVID-19 [7, 9, 11, 12].
The sample size referred to for each study includes the patients employed prior to COVID-19 accounted for at follow-up, in order to only evaluate patients that were in working age.
After retrieving the articles from all the selected databases, duplicate removal and the initial screening by title and abstract was performed through the website Rayyan [16], which allowed for articles to be screened by the researchers independently, following triple blind methodology, in order to reduce selection bias. The articles with primary data were directly included in the review, while articles that did not include primary data (review articles) were screened to assess if any possible research article included could fit into our systematic review. A quality assessment was performed for the included studies using the Newcastle-Ottawa Scale (NOS) [17].
Concerning data extraction, two of the researchers built a table using the Microsoft Excel software with the data evaluated as important for the aim of this systematic review, the tables were then integrated and used to build a summary of our results (Table 1).
Table 1
Studies included in the review sorted by follow-up time, and sample size (the number of patients evaluated at follow-up that were employed prior to COVID-19 illness). The table includes authors, country, sample size, follow-up time, and relevant outcomes
| Authors | Country | Sample | Hospitalized (H) | Mean age | Follow-up | Returned to | Limitation to work | Not able to return | Other outcome |
| size | or Stay in | (SD) or Median | time | same work, | duties/hours | to work due | (re-integration, | ||
| Intensive Care | age (IQR) | n (%) | due to health | to health | job-change, etc.) | ||||
| Unit (ICU) | issues, n (%) | issues, n (%) | or did not respond | ||||||
| Robinson-Lane et al. [19] | USA | 233 | H | – | 2 months | 135 (57.9%) | 24 (10.3%) | 59 (25.3%) | 15 (6.5%) |
| Chopra et al. [18] | USA | 195 | H | ME: 62 (50-72) | 2 months | 87 (44.6%) | 30 (15.4%) | 45 (23.1%) | 33 (16.9%) |
| Monti et al. [20] | Italy | 28 | ICU | M: 56 (10.5) | 2 months | 8 (28.6%) | 1 (3.6%) | 19 (67.8%) | 0 |
| Zhao et al. [21] | China | 55 | H | M: 47.74 (15.49) | 2-3 months | 55 (100%) | 0 | 0 | 0 |
| Liang et al. [22] | China | 76 | H | M: 41.3 (13.8) | 3 months | 69 (90.8%) | – | – | – |
| Garrigues et al. [23] | France | 41 | H | M: 64.1 (16.1) | 110 days | 31 (75.6%) | – | – | – |
| 15 | ICU | M: 59.6 (13.7) | 7 (46.7%) | – | – | – | |||
| Jacobson et al. [24] | USA | 22 (11) | H (ICU) | M: 50.6 (15.1) | 4 months | – | 7 (31,8%) | – | – |
| Hodgson et al. [25] | Australia | 114 | ICU | ME: 61 (51-70) | 6 months | – | – | 13 (11.4%) | – |
| Lindahl et al. [26] | Finland | 71 | H | M: 60 (11) | 6 months | 55 (77.5%) | 4 (5.6%) | 9 (12.7%) | 3 (4.2%) |
| Carenzo et al. [27] | Italy | 45 | ICU | ME: 57 (51-61) | 6 months | 27 (60.0%) | 6 (1.3%) | 10 (22.2%) | 2 (4.5%) |
| van Veenendaal et al. [28] | The Netherlands | 30 | ICU | ME: 62.5 (55.3-68.0) | 6 months | 3 (10.0%) | 4 (13.3%) | 13 (43.3%) | 10 (33.4%) |
2.1Inclusion criteria
The research was restricted to articles published during the COVID-19 Pandemic (from December 2019), up to December 2021 (when the databases search was performed) and included articles in Italian and English languages. Inclusion criteria were met if the articles investigated: ability to return to work, partial ability to return to work, with duty or hours limitations, or not being able to return to work after being hospitalized due to COVID-19 at the time of follow up.
2.2Exclusion criteria
Articles not written in English or Italian languages, or that did not mention post COVID-19 return to work, were excluded from the systematic review. Furthermore, based on the type of publication, non-research articles were excluded (i.e.: commentaries, letters, and editorials).
3Results
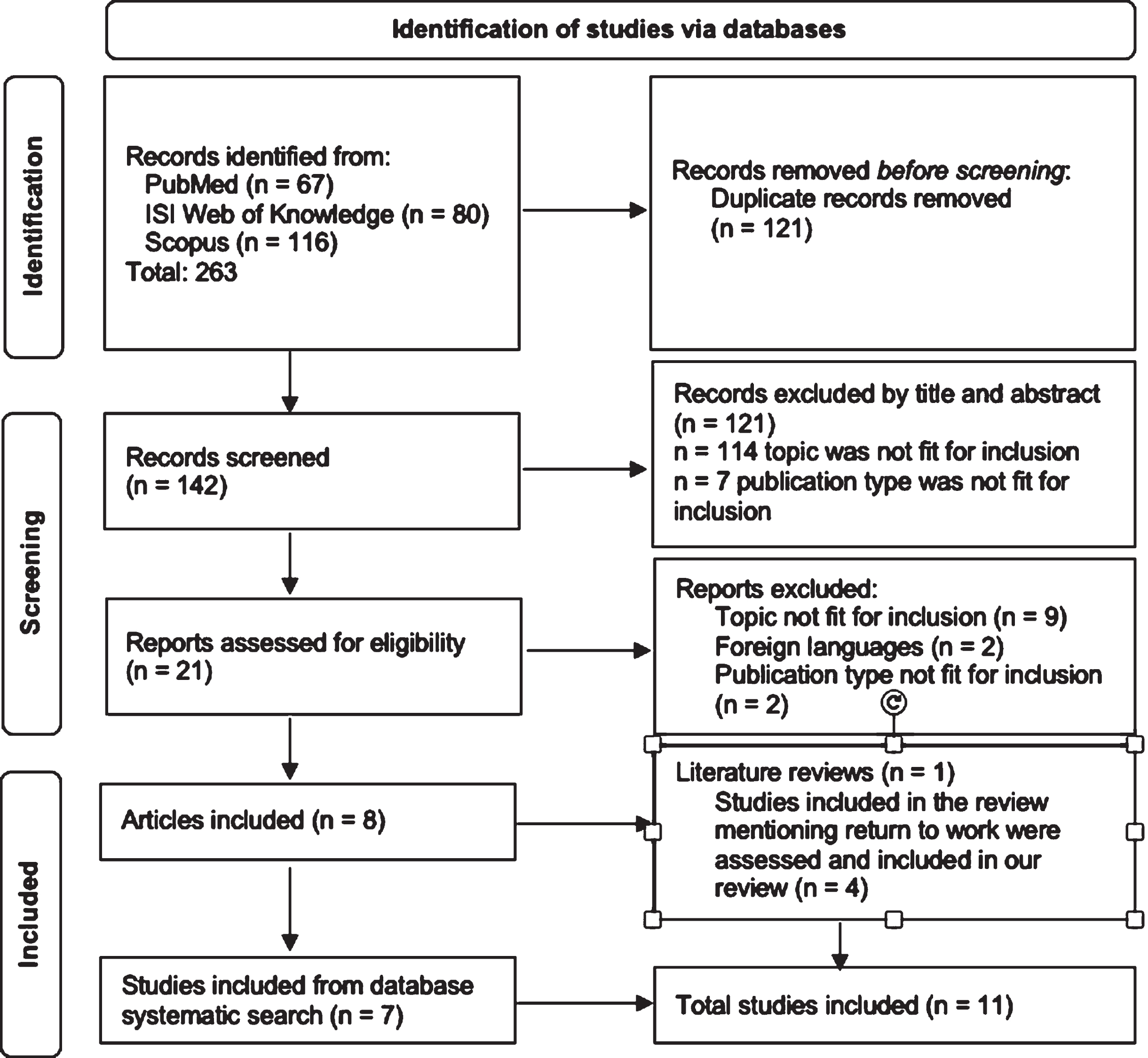
The systematic search resulted in 263 relevant articles across the three databases (PubMed, ISI Web of Knowledge, and Scopus). After removing duplicates (121 duplicate articles), the initial search resulted in 142 eligible articles. The initial screening by title and abstract resulted in a total of 121 excluded articles: 114 articles were excluded based on the addressed topics; 7 articles were excluded according to the type of publication.
The remining 21 articles were screened by full text; all the articles were successfully retrieved. A total of 13 articles were excluded based on full text, leaving 8 articles to be included based on full text: one was a literature review, while the other 7 studies were included in our systematic review (Fig. 1). The systematic review that was included in our screening [10] had a different aim than our own, but results were screened to see if any of the included articles mentioned return to work after COVID-19 hospitalization and could fit into our aim as well. Four articles were retrieved and included in this systematic review, for a total of 11 included articles. Any conflict about the inclusion or exclusion of the articles was resolved by internal discussion between the researchers.
Fig. 1
PRISMA flowchart of the article selection process.
A quality evaluation was performed on the included studies, using the NOS [17]; all the included studies were at least at a good quality level on the scale (7 points or higher) (Table 2).
Table 2
Quality assessment of included studies through the Newcastle-Ottawa Scale
| Authors | Study design | Newcastle Ottawa scale | Overall quality | ||
| Selection | Comparability | Outcome | assessment | ||
| Robinson-Lane et al. [19] | Cross sectional | 5 | 1 | 2 | 8 |
| Chopra et al. [18] | Observational cohort | 5 | 1 | 2 | 8 |
| Monti et al. [20] | Prospective observational | 5 | 1 | 2 | 8 |
| Zhao et al. [21] | Prospective observational | 4 | 1 | 2 | 7 |
| Liang et al. [22] | Prospective observational | 4 | 1 | 2 | 7 |
| Garrigues et al. [23] | Prospective case series | 4 | 1 | 2 | 7 |
| Jacobson et al. [24] | Prospective cohort | 5 | 1 | 2 | 8 |
| Hodgson et al. [25] | Prospective cohort | 5 | 1 | 2 | 8 |
| Lindahl et al. [26] | Prospective observational | 4 | 1 | 2 | 7 |
| Carenzo et al. [27] | Prospective case series | 4 | 1 | 2 | 7 |
| van Veenendaal et al. [28] | Prospective cohort | 5 | 1 | 2 | 8 |
Out of the 11 studies included in the review (Table 1), 4 (36.4%) had a follow-up interval of six months, 4 (36.4%) studies had a follow-up interval between 2 and six months, while 3 (27.2% %) had a follow-up period of two months. Three studies were performed in the USA (27.2% %), two in Italy (18.2%), two in China (18.2%), one in Australia (9.1%), one in France (9.1%), one in Finland (9.1% %), and one in the Netherlands (9.1% %). Four studies (36.4%) had a sample of less than 50 people who were employed before suffering from COVID-19, 4 studies (36.4% %) had a sample size between 50 and 100 patients, whilst 3 (27.2% %) had a sample larger than 100 workers.
3.1Two months follow-up
Three studies had a follow-up time set at two months [18–20]. Chopra et al.’s [18] and Robinson-Lane et al.’s [19] studies were conducted in the USA and had a larger sample of patients that were employed before being hospitalized due to COVID-19; these studies highlighted that 44.6% and 57.9% respectively of patients had returned to work. The study by Monti et al. [20] was conducted in Italy and had a smaller sample, less than 30 people, of patients that underwent an ICU stay and at least one day of invasive ventilation, and reported that only 28.6% of the previously employed patients had returned to work at the follow-up mark. Return to work at two-months post illness was not without limitations to work duties: Chopra et al. [18] highlighted that 15.4% of people had resumed work but had limitations or adjustments made in their work duties or hours in order to go back to employment, Robinson-Lane et al. [19] reported 10.3% of participants needing the same adjustments, while this percentage was just 3.6% in the study by Monti et al. [20]. The two USA studies reported 23.1% and 25.3 respectively of the sample not being able to return to work at the two months mark due to health problems [18, 19], while this number was much higher in the Italian study (67.8%) [20].
3.2Follow-up more than two and less than six months
Two of the studies were performed in China [21, 22]. Zhao et al. [21] conducted a study in China with a follow-up between two and three months after acute illness; the sample consisted in 55 hospitalized patients; all of them had returned to their previous work at follow-up. Liang et al. [22] performed a study in China on 76 hospitalized patients, with a follow-up at 3 months: 90.8% of patients (69) had returned to work.
Garrigues et al. [23] performed a study on a total of 56 patients, 41 hospitalized and 15 ICU patients, and had a follow-up period of 110 days; 75.6% (31) of hospitalized patients had return to work at the time of follow-up, while only 46.7% (15) of ICU patients had returned to work.
Jacobson et al. [24] performed a study in the USA on 22 hospitalized patients, 11 of whom underwent an ICU stay; the follow-up at 4 months highlighted that 31.8% of patients (7) had limitations to their work tasks due to health issues, but no other outcome concerning work was evaluated.
3.3Six months follow-up
Four studies had a follow-up period of six months; the study performed by Hodgson et al. [25] had a sample of more than 100 patients that stayed in ICU for at least 24 hours, was carried out in Australia, and reported that only 11.4% of workers were not back to work at the six months mark, although the percentage of workers requiring adjustments to their work duties or hours was not investigated; the study also highlighted that 34% of participants had new problems with mobility, 34% with pain and 43% with usual activities. The other studies had smaller samples, two of these studies, the one by Lindahl et al. [26] conducted in Finland on hospitalized patients, and the one by Carenzo et al. [27] conducted in Italy on patients with a ICU stay of at least 72 hours, respectively reported that 77.5% and 60.0% of employees were back to work after six months; Carenzo et al. also stratified patients not able to return to work based on age, but found a similar rate for patients under and over 57 years of age (76% and 74% respectively). Van Veenendaal et al. [28] carried out a study in the Netherlands, on 30 patients discharged from ICU, and highlighted that only 10.0% of patients were back to work at time of follow-up. Limitations to work duties or hours upon returning to work after suffering from COVID-19 were various in these studies (Table 1). The percentage of patients not able to resume working at all at six months follow-up in the study Lindahl et al. [26] it was 12.7%, in Carenzo et al.’s [27] it was 22.2%, and in van Veenendaal et al.’s [28] it was 43.3%.
4Discussion
The COVID-19 pandemic had a large impact on workers’ quality of life, and on occupational medicine in general. As the post COVID-19 or Long COVID-19 becomes progressively more common, the impact of this postcritical illness on occupational health should be considered and assessed. In this systematic review, we investigated the impact of post COVID-19 on previously hospitalized patients, highlighting as outcomes the number of workers returning to work, with or without limitations to work duties or hours, or not returning to work, at the time of follow-up.
The included articles had a follow-up period ranging from two to six months, and a highly variable return to work rate, ranging from 10.0% to 100.0% (Table 1).
Time of follow-up seems to be an important factor in resuming work post COVID-19 hospitalization; two of the included studies both investigated return to work in Italian workers after undergoing an ICU stay, with vastly different results: the study with a 2 months follow-up highlighted 28.6% of workers were back at their job without duty or hours limitations [20], while the same was true for 60.0% of patients of the study with a 6 months follow-up [27], leading to believe that a recovery, even if partial, is achievable over time.
The difference in the percentages of workers resuming their job at follow-up might be because of the sample included in these studies: both Monti et al.’s study [20], with 28.6% of patients resuming work at two months, and van Veenendaal et al.’s study [28], with 10% of patients going back to their job at six months, had a sample made up of only patients from the ICU. As supported by scientific literature, the post COVID-19 condition can cause fatigue or dyspnea 7 months after hospitalization in about 70% of COVID-19 patients, residual impaired cognition in almost 70% of patients, and residual disability in over 50% [29, 30]; psychiatric symptoms were even higher, affecting over 90% of patients at six months after discharge [31]. Residual impairments lasting months after the acute COVID-19 illness would also explain why some of the people returning to work needed adjustments in their work duties or hours, although the ability to return to work with limitations could also be due to confounding factors (such as age or comorbidity) that were not assessed in the studies.
Seven of the included studies reported residual difficulties upon returning to work [18–20,24,26–28], both at the two and six months follow-ups, highlighting how residual impairment is present in some of the workers even upon returning to work, for at least a few months after suffering from COVID-19, influencing their ability to perform the same duties as before or causing a limitation in working hours. These results highlight an impact of post COVID-19 not only in returning to work, but also in the ability to perform the same job as before, for months after the primary illness.
While a difference between patients undergoing a hospital or ICU stay seems present, with a higher return to work in hospitalized patients compared with those who underwent an ICU stay when populations with similar characteristics were considered [23], a definite conclusion cannot be drawn from the presented data, as a meta-analysis was not performed.
Some relevant differences in returning to work were also observed based on the country the study was performed in: the two studies with the highest return to work rate were conducted in China on hospitalized patients, with 100% [21] and 90.8% [22] of patients returning to work at 3 months. In the two studies conducted in the USA, return to work was 57.9% [19] and 44.6% [18] at a 2 months follow-up. As for Europe, return to work was higher in France (75.6% for hospitalized patients and 46.7% for ICU patients) [23] and Finland (77.5%) [26], it was lower in Italy (28.6% [20] at 2 months and 60.0% [27] at 6 months), and the lowest return to work rate was found in the Netherlands’ study (10.0% of workers were back after 6 months) [28].
A difference between countries seems clear, as almost all of the Chinese workers were back at work at the follow-up mark, and the percentage was also high in the USA, considering the follow-up was only 2 months, compared with European countries, where return to work was lower, or similar but with longer follow-up periods. This is consistent with scientific literature, seeing as many studies have underlined that presenteeism (i.e.: working while sick) is common in Chinese workers [32–34]. The high rate in the USA, on the other hand, might be influenced by the healthcare system [35], as well as the fact that not all employees are entitled to paid sick leave [36, 37].
However, is it important to note that the differences observed between countries might at least partially be due to the different mean age of the patients included in the studies: the two Chinese studies, with the highest return to work percentage of patients, also had the lowest mean age (47.74 for Zhao et al. and 41.3 for Liang et al.). In all the other studies included in the review, mean or median age was between 50 and 65 years of age, so the age gap, however small, may have played a difference in return to work, leading to assume both the cultural and social aspect as well as the age aspect might have played an important role.
The number of workers not being able to resume their job due to being hospitalized because of COVID-19, is going to have a massive impact on the world’s working population. Post COVID-19 condition is a rising problem in occupational medicine and should be thoroughly assessed in further studies.
This systematic review has some strengths and limitations. A systematic approach was used to search the three chosen databases following the PRISMA Statements, and selection of the articles was performed by three researchers following triple blind methodology. However, only articles in English or Italian languages were included in the review, and articles not focusing on return to work might have been left out, for this reason a hand-search was performed on the systematic review included that, albeit with a different aim than our own, also included articles that briefly mentioned return to work. Furthermore, the included studies did not consider which COVID-19 variant the patients were infected by, therefore we could not take into account the different effect of different variants on returning to work after COVID-19 disease. The Newcastle-Ottawa Scale used for Quality Assessment of the included studies has shown some consistency problems and is a tool highly dependent on operator [38, 39], therefore, quality assessment may have shown different results if performed by a different research group.
5Conclusions
Post COVID-19 condition is a rising problem in occupational medicine, and the impact it has on the workforce is rapidly increasing. This review highlights how ability to return to work seem to increase over time, as it was higher in studies performed in the same Country but with a longer follow-up; it depends on the Country the patients are from, as notable differences were present; return to work was also higher for younger workers.
This review highlighted the impact of this condition on a global scale, underlining that many workers are not able to resume prior employment, due to health conditions, with an impact on the workforce that cannot be overlooked. Further studies are needed to assess this upcoming issue. From an occupational medicine perspective, occupational physicians could facilitate the process of returning to work, by accommodating the work situation, in order to facilitate the transition back to employment in workers with a post COVID-19 condition.
Ethical considerations
This study, as a literature review, did not require Institutional Review Board approval.
Informed consent
This study, as a literature review, did not require informed consent.
Conflict of interest
The authors have no conflict of interest to declare.
Acknowledgments
None to report.
Funding
This research received no funding.
References
[1] | Çelikkalp Ü , Irmak AY , Ekuklu G . Working conditions and anxiety levels of employees who have to work during the COVID-19 pandemic. Work. (2021) ;70: (4):1047–55. |
[2] | Carvalhais C , Querido M , Pereira CC , Santos J . Biological risk assessment: A challenge for occupational safety and health practitioners during the COVID-19 (SARS-CoV-2) pandemic. Work. (2021) ;69: (1):3–13. |
[3] | Kramer A , Kramer KZ . The potential impact of the Covid-19 pandemic on occupational status, work from home, and occupational mobility. J Vocat Behav. (2020) ;119: :103442. |
[4] | Bond AE , Wagler K , Anestis MD . Essential workers: Past month suicidal ideation and COVID-19 stress. J Clin Psychol. (2021) ;77: (12):2849–59. |
[5] | A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October (2021) [Internet]. [citato 6 aprile 2022]. Disponibile su: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1. |
[6] | PASC Dashboard [Internet]. [citato 10 aprile (2022) ]. Disponibile su: https://pascdashboard.aapmr.org/. |
[7] | Tabacof L , Tosto-Mancuso J , Wood J , Cortes M , Kontorovich A , McCarthy D , et al. Post-acute COVID-19 Syndrome Negatively Impacts Physical Function, Cognitive Function, Health-Related Quality of Life, and Participation. Am J Phys Med Rehabil. (2022) ;101: (1):48–52. |
[8] | Palstam A , Westerlind E , Sunnerhagen KS , Persson HC . Recurrent sick leave after COVID- investigating the first wave of the pandemic in a comprehensive Swedish registry-based study. BMC Public Health. (2021) ;21: (1):1914. |
[9] | Liao T , Meng D , Xiong L , Wu S , Yang L , Wang S , et al. Long-Term Effects of COVID-19 on Health Care Workers 1-Year Post-Discharge in Wuhan. Infect Dis Ther. (2022) ;11: (1):145–63. |
[10] | Sanchez-Ramirez DC , Normand K , Zhaoyun Y , Torres-Castro R . Long-Term Impact of COVID-19: A Systematic Review of the Literature and Meta-Analysis. Biomedicines. (2021) ;9: (8):900. |
[11] | Pérez-González A , Araújo-Ameijeiras A , Fernández-Villar A , Crespo M , Poveda E . Long COVID in hospitalized and non-hospitalized patients in a large cohort in Northwest Spain, a prospective cohort study. Sci Rep. (2022) ;12: (1):3369. |
[12] | Bellan M , Baricich A , Patrucco F , Zeppegno P , Gramaglia C , Balbo PE , et al. Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19. Sci Rep. (2021) ;11: (1):22666. |
[13] | McPeake J , Mikkelsen ME , Quasim T , Hibbert E , Cannon P , Shaw M , et al. Return to Employment after Critical Illness and Its Association with Psychosocial Outcomes. A Systematic Review and Meta-Analysis. Ann Am Thorac Soc. (2019) ;16: (10):1304–11. |
[14] | Page MJ , McKenzie JE , Bossuyt PM , Boutron I , Hoffmann TC , Mulrow CD , et al. The PRISMA statement: an updated guideline for reporting systematic reviews. BMJ. (2021) ;372: :71. |
[15] | Falagas ME , Pitsouni EI , Malietzis GA , Pappas G . Comparison of PubMed, Scopus, Web of Science, and Google Scholar: strengths and weaknesses. The FASEB Journal. (2008) ;22: (2):338–42. |
[16] | Rayyan – Intelligent Systematic Review [Internet]. [citato 6 aprile (2022) ]. Disponibile su: https://www.rayyan.ai/. |
[17] | Wells GA , Shea B , O’Connell D , Peterson J , Welch V , Losos M , Tugwell P . The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. The Ottawa Hospital Research Institute. |
[18] | Chopra V , Flanders SA , O’Malley M , Malani AN , Prescott HC . Sixty-Day Outcomes Among Patients Hospitalized With COVID-19. Ann Intern Med. (2021) ;174: (4):576–8. |
[19] | Robinson-Lane SG , Sutton NR , Chubb H , Yeow RY , Mazzara N , DeMarco K , et al. Race, Ethnicity, and 60-Day Outcomes After Hospitalization With COVID-19. J Am Med Dir Assoc. (2021) ;22: (11):2245–50. |
[20] | Monti G , Leggieri C , Fominskiy E , Scandroglio AM , Colombo S , Tozzi M , et al. Two-months quality of life of COVID-19 invasively ventilated survivors; an Italian single-center study. Acta Anaesthesiol Scand. (2021) ;65: (7):912–20. |
[21] | Zhao YM , Shang YM , Song WB , Li QQ , Xie H , Xu QF , et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine. (2020) ;25: :100463. |
[22] | Liang L , Yang B , Jiang N , Fu W , He X , Zhou Y , et al. Three-month Follow-up Study of Survivors of Coronavirus Disease after Discharge. J Korean Med Sci. (2020) ;35: (47):e418. |
[23] | Garrigues E , Janvier P , Kherabi Y , Le Bot A , Hamon A , Gouze H , et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect. (2020) ;81: (6):e4–6. |
[24] | Jacobson KB , Rao M , Bonilla H , Subramanian A , Hack I , Madrigal M , et al. Patients With Uncomplicated Coronavirus Disease (COVID-19) Have Long-Term Persistent Symptoms and Functional Impairment Similar to Patients with Severe COVID- A Cautionary Tale During a Global Pandemic. Clin Infect Dis. (2021) ;73: (3):e826–9. |
[25] | Hodgson CL , Higgins AM , Bailey MJ , Mather AM , Beach L , Bellomo R , et al. The impact of COVID-19 critical illness on new disability, functional outcomes and return to work at 6 months: a prospective cohort study. Crit Care. (2021) ;25: (1):382. |
[26] | Lindahl A , Aro M , Reijula J , Mäkelä MJ , Ollgren J , Puolanne M , et al. Women report more symptoms and impaired quality of life: a survey of Finnish COVID-19 survivors. Infect Dis (Lond). (2022) ;54: (1):53–62. |
[27] | Carenzo L , Dalla Corte F , Haines RW , Palandri C , Milani A , Aghemo A , et al. Return to Work After Coronavirus Disease Acute Respiratory Distress Syndrome and Intensive Care Admission: Prospective, Case Series at 6 Months From Hospital Discharge*. Crit Care Med. (2021) ;49: (11):e1157–62. |
[28] | van Veenendaal N , van der Meulen IC , Onrust M , Paans W , Dieperink W , van der Voort PHJ . Six-Month Outcomes in COVID-19 ICU Patients and Their Family Members: A Prospective Cohort Study. Healthcare (Basel). (2021) ;9: (7):865. |
[29] | Fernández-de-Las-Peñas C , Palacios-Ceña D , Gómez-Mayordomo V , Palacios-Ceña M , Rodríguez-Jiménez J , de-la-Llave-Rincón AI , et al. Fatigue and Dyspnoea as Main Persistent Post-COVID-19 Symptoms in Previously Hospitalized Patients: Related Functional Limitations and Disability. Respiration. (2022) ;101: (2):132–41. |
[30] | Chaumont H , Meppiel E , Roze E , Tressières B , de Broucker T , Lannuzel A , et al. Long-term outcomes after NeuroCOVID: A 6-month follow-up study on 60 patients. Rev Neurol (Paris). (2022) ;178: (1-2):137–43. |
[31] | Ahmed GK , Khedr EM , Hamad DA , Meshref TS , Hashem MM , Aly MM . Long term impact of Covid-19 infection on sleep and mental health: A cross-sectional study. Psychiatry Res. (2021) ;305: :114243. |
[32] | Lu L , Cooper C , Lin H . A cross-cultural examination of presenteeism and supervisory support. (2013) . |
[33] | Li W , Moriyama M , Cui Y , Kazawa K , Nakaya T , Susanto T . Presenteeism among Chinese workers in Japan and its relationship with mental health and health-promoting lifestyles. Ind Health. (2020) ;58: (1):35–45. |
[34] | Wang Yanxia , Chen Chih-Chieh , Fosh Patricia . Presenteeism in the Chinese Work Context. In: Presenteeism at Work. Cambridge University Press. (2018) ;286–311. |
[35] | The U.S. Health Care System: An International Perspective [Internet]. Department for Professional Employees, AFL-CIO. [citato 3 giugno (2022) ]. Disponibile su: https://www.dpeaflcio.org/factsheets/the-us-health-care-system-an-international-perspective |
[36] | Heymann J , Raub A , Waisath W , McCormack M , Weistroffer R , Moreno G , et al. Protecting health during COVID-19 and beyond: A global examination of paid sick leave design in 193 countries. Glob Public Health. (2020) ;15: (7):925–34. |
[37] | Sick Leave | U.S. Department of Labor [Internet]. [citato 3 giugno (2022) ]. Disponibile su: https://www.dol.gov/general/topic/workhours/sickleave |
[38] | Lo CKL , Mertz D , Loeb M . Newcastle-Ottawa Scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol. (2014) ;14: :45. |
[39] | Hartling L , Milne A , Hamm MP , Vandermeer B , Ansari M , Tsertsvadze A , et al. Testing the Newcastle Ottawa Scale showed low reliability between individual reviewers. J Clin Epidemiol. (2013) ;66: (9):982–93. |


