
College students’ compliance with government measures for social isolation and quarantine during the COVID-19 outbreak: A focus on psychological predictors
Abstract
BACKGROUND:
To contain the COVID-19 pandemic, government adopted several measures to restrict social contacts including isolation, quarantine, and limitations on movement from location to location around the country.
OBJECTIVE:
To analyze the degree to which Italian college students agreed and complied with these measures and to determine if psychological variables have influenced compliance.
METHODS:
We evaluated 6075 students concerning their agreement with the government’s restrictions, as well as their health anxiety, trait positive and negative affect, and current symptoms of anxiety, depression, and stress. We performed MANOVAs, ANOVAs, path analysis, and binary logistic regressions.
RESULTS:
We found some differences in compliance with government restrictions concerning gender, geographic location, and major of study. Psychological variables did not play a significant role in predicting compliance with restriction measures and making a call for medical help. However, health anxiety predicted higher levels of worries about having contracted the virus.
CONCLUSIONS:
Based on our results, university-based interventions should primarily focus on males to foster compliance with government restriction during a pandemic, or health crisis. College students –Social Sciences students in particular –could benefit from counseling interventions to avoid the development of psychological disorders fueled by pandemic worries.
1Introduction
At the end of 2019, a novel coronavirus (COVID-19) arising in China, Hubei, rapidly demanded interest in countries worldwide. It became a public health emergency because COVID-19 has proven to be a virus characterized by high mortality and rapid transmission [1–5]. Italy became one of the most affected European countries with many cases and a large number of deaths [6]. The first case of COVID-19 was diagnosed in February 2020, in a little city in northern Italy [7]. The Italian government adopted several restrictive measures, mainly focused on limiting individuals’ movements and social contacts to help contain the pandemic. Restrictive measures included limitations such as the closure of schools, universities, and workplaces. People who tested positive for COVID-19 were told to avoid social contacts, even if they were not having symptoms. National telephone numbers were made available to get help with safely maintaining quarantine or isolation. When the virus continued to be increasingly unmanageable, the Italian government imposed a lockdown throughout the country, with disciplinary consequences for those who did not respect the quarantine guidelines.
The importance of strictly following government-imposed rigid rules to contain the pandemic has created interest in the impact that the COVID-19 outbreak (and the subsequent control measures) had on the well-being of people who faced many changes in their lifestyles, especially health care workers and university students [8–14]. It is critical to know which variables might have fostered compliance with the government’s instructions. The establishment of government restrictions is not enough to face the spread of a virus, people must be willing to strictly adhere to the required limitations. Implementation of organization-based interventions should aim to encourage the observance of the health crisis requirements. More specifically, university-based prevention activities and interventions might be easier to implement (and reach much more people) than interventions initiated in smaller organizations. In line with this assumption, a recent study (with a preventive aim) evaluated the COVID-19 associated knowledge and health behaviors of college students [15]. Therefore, it is crucial to analyze if psychological variables could predict adherence to social limitations during a major health crisis among college students.
This study aims to shed light on the degree to which a wide sample of college students complied with the government COVID-19 control measures and if psychological variables (i.e., trait positive and negative affect, health anxiety, and current symptoms of anxiety, depression, and stress) influenced compliance.
2Methods
2.1Participants
We recruited a sample of 6075 Italian college students aged between 18 and 68 years (M age = 23.60±5.02, 74.6% females) during the COVID-19 lockdown. The sample comprises 80.3% of people living in Tuscany; however, all Italian regions are represented. The participants are heterogeneous concerning both their major and year of study. For more details about the participants’ characteristics, please see [16]. For this study, we used the sample previously analyzed by other studies [16–18]; though we used this sample for different analyses.
2.2Materials
2.2.1Ad hoc questions about the quarantine measures and COVID-19
We designed a questionnaire including ad hoc questions aiming at evaluating: i) the characteristics of the home (e.g., number and relationship of people living with the student, number of rooms, presence of a pet); ii) the agreement with and the respect for the quarantine measures established by the Italian government; iii) COVID-19 symptoms (e.g., having experienced symptoms), having called the emergency assistance numbers for requesting help, and beliefs about the virus (e.g., if it is a real emergency); iv) impact of the quarantine on the didactics (e.g., satisfaction with the online didactic); v) impact on study routines and habits (e.g., traineeship interrupted, hours of studying per day). For this paper, we only used the responses gathered from sections ii and iii of these questions.
2.2.2Positive and Negative Affect Schedule (PANAS) [19]
We administered the Italian version [20] of the PANAS. It is a 20-item self-report with a response format of a 5-point Likert scale ranging from 1 (Very slightly or not at all) to 5 (Extremely). It allows for evaluation of both Positive and Negative Affect. The PANAS is available in both the trait and state versions. For this study, we used the trait version.
2.2.3Depression Anxiety Stress Scales-21 (DASS-21) [21]
We administered the Italian validation [22] of the DASS-21, which is the 21-item version derived from the 42-item DASS version by Lovibond and Lovibond [23]. It measures three scales: Depression, Anxiety, and Stress. The participants answer using a 4-point Likert scale ranging between 0 (Did not apply to me at all - Never) and 3 (Applied to me very much, or most of the time –Almost always). The time reference is “the last 7 days.”
2.2.4Health Anxiety Questionnaire (HAQ) [24]
We administered the Italian version [25] of the HAQ. It is a 21-item self-report scale with a response format of a 4-point Likert scale ranging between 1 (Never or rarely) and 4 (Almost ever). It evaluates, through the use of four scales: the fear of diseases and death, interference with daily life, concern about one’s own health, seeking reassurance. Also, it is possible to calculate a total score.
2.3Procedure
First, we asked for approval from the Ethical Committee of the University of Florence. Next, we created an online questionnaire, including the ad-hoc questions and the scales described in the previous section, and other scales not used for the present paper. We included a first page with demographic data (e.g., gender, age). On the first page of the questionnaire, we wrote the information required for obtaining the Informed Consent, and the participants were asked to check a box saying that they agreed to take part in the research by filling out the questionnaire on the following pages.
Our University Office contacted Florentine students by an invite sent to their institutional email addresses, including the link to the questionnaire. Moreover, to have participation of students from other Italian cities, we spread the link on Facebook University groups.
2.4Data analysis
We performed analyses using SPPS.26 (Chicago, IL, USA). First, we calculated descriptive statistics and frequencies concerning the quarantine and COVID-19 variables evaluated through ad-hoc questions. We analyzed if there are differences in the (seven) quantitative ad-hoc questions with regards to gender, location (i.e., northern, central, southern Italy), and major of study through some MANOVAs –for highly correlated variables (i.e., r values ranging between 0.56 and 0.74) –and ANOVAs. Given the high number of multiple comparisons (21 ANOVAs), we adjusted the alpha level at 0.002 through the Bonferroni correction for multiple comparisons [26].
Next, to analyze if trait positive and negative affect, health anxiety, and current symptoms of anxiety, depression, and stress predict the agreement with quarantine and social isolation measures and the worry about having contracted the virus, we tested a path analysis model (Maximum Likelihood estimate method). To evaluate its fit, we referred to the values provided in the literature [27–29]. Finally, to analyze if the previous psychological variables (and gender and age) predict making the call for help during the COVID-19 pandemic, we performed four binary logistic regressions.
3Results
3.1Agreement with the quarantine measures and COVID-19 symptoms
First, we analyzed the descriptive statistics and the frequencies for the ad-hoc questions concerning agreement with the Italian government’s measures for limiting the spread of the pandemic, the respect for these rules, and the rates of COVID-19 occurrence for Italian students (see Table 1). The results highlighted that Italian college students had a high level of agreement with the measures of social isolation despite lack of presence of symptoms. More generally, college students had a high level of agreement with the Italian government’s quarantine measures. Although the scores range between one and seven for these two questions, the average score is around six for both questions. In line with this finding, even though some students reported having left home 30 times per week, the average student left home less than twice a week. These results indicate that they generally respected the recommendation to stay home and go out only when strictly necessary. A minority of students (10.7%) moved from their home to another city/region after the government declared that people should not move across Italy. The average participant perceived the COVID-19 outbreak as a real emergency. Only a few students reported having experienced flu-like symptoms or knowing someone affected or hospitalized due to COVID-19.
Table 1
Agreement with quarantine’s measures and experience of COVID-19 symptoms among Italian college students (n = 6075)
| Question | Option | % | Range | M(DS) |
| How much do you agree with the measure of social isolation, regardless of the presence of flu symptoms? | 1– 7 | 6.14(1.28) | ||
| How much do you agree with the quarantine measures established to manage this health emergency? | 1– 7 | 5.96(1.29) | ||
| Since the quarantine began, have you stayed in the house you lived in at the time of the news or have you moved (e.g., are you an off-site student and went to your parents)? | Stayed where I was Moved from where I was | 89.3 10.7 | ||
| Did you leave the house for reasons of health, work, or other needs (e.g., to go shopping, take the dog out)? | Yes No I do not want to answer | 76.0 23.4 0.6 | ||
| On average, in a week, how many times do you leave the house? | 0– 30 | 1.77(2.65) | ||
| Given the choice, do you prefer to go out to shop (or anything else) or do you want another person to go in your place? | I Another person I do not want to answer | 46.2 44.3 9.5 | ||
| If you have to do the shopping, do you prefer to use the home delivery service or go shopping yourself? | Home delivery service I go shopping I do not do the shopping I do not want to answer | 14.3 55.7 28.7 1.3 | ||
| Have you had flu symptoms (fever, cough, sore throat) since the quarantine began? | Yes No I do not want to answer | 12.0 87.2 0.8 | ||
| Since the quarantine began, how worried have you been that you may have contracted COVID-19? | 1– 7 | 3.55(1.72) | ||
| Would you like to do a swab for COVID-19 or a similar analysis that establishes whether you have had or are currently infected with COVID-19? | Yes Yes, I already did it No I do not want to answer | 58.4 0.9 38.1 2.6 | ||
| Have you personally contacted your family doctor about symptoms you thought were due to COVID-19? | Yes No I do not want to answer | 6.7 92.5 0.8 | ||
| Have you personally contacted one of the official numbers set up for the COVID-19 emergency for symptoms that you thought were due to COVID-19? | Yes No I do not want to answer | 2.5 96.8 0.7 | ||
| Have you contacted your family doctor for another person for symptoms you thought were due to COVID-19? | Yes No I do not want to answer | 4.1 95.3 0.6 | ||
| Have you contacted one of the official numbers set up for the COVID-19 emergency for another person for symptoms that you thought were due to COVID-19? | Yes No I do not want to answer | 2.3 97.2 0.5 | ||
| If you have contacted your general practitioner or one of the official numbers, have you been subjected to the precautionary isolation measure? | Yes No Not Applicable I do not want to answer | 3.7 25.9 68.4 2.0 | ||
| Do you have relatives or friends who have been hospitalized for COVID-19? | Yes No I do not want to answer | 15.9 83.5 0.6 | ||
| Have any of the people you know contracted COVID-19? | Yes No I do not want to answer | 43.9 56.1 0.0 | ||
| How much do you think COVID-19 is a real emergency? | 1– 7 | 6.35(1.02) | ||
| How much do you think COVID-19 is a laboratory-created weapon? | 1– 7 | 2.45(1.84) | ||
| How much do you think COVID-19 is a natural virus? | 1– 7 | 5.29(1.76) |
3.2Demographic differences on agreement with the quarantine measures and beliefs about COVID-19
To evaluate differences in the quantitative ad-hoc questions concerning gender, geographic area of residence, and major of study, we performed ANOVAs and MANOVAs (for the three variables highly correlated: agreement with social isolation and quarantine, and belief that COVID-19 represents a real emergency). Table 2 shows the descriptive statistics and ANOVAs results.
Table 2
Follow-up ANOVAs and ANOVAs results of the agreement with the quarantine’s measures and beliefs about COVID-19 by gender, location, and area of study
| COVID -related variable | Demographic | Group | n | M(SD) | F | df | p | Partial η2 |
| variable | ||||||||
| Agreement with social isolation | Gender | Male | 1542 | 6.02(1.37) | 21.00 | 1,6073 | < 0.001 | 0.003 |
| Female | 4533 | 6.19(1.24) | ||||||
| Total | 6075 | 6.14(1.28) | ||||||
| Area of Italy | North | 625 | 6.13(1.30) | 0.77 | 2,6038 | n.s. | 0.000 | |
| Center | 5066 | 6.14(1.28) | ||||||
| South | 350 | 6.23(1.22) | ||||||
| Total | 6041 | 6.14(1.28) | ||||||
| Area of Study | Technology | 933 | 6.08(1.33) | 4.40 | 6,5635 | < 0.001 | 0.005 | |
| Soc.Sciences | 2455 | 6.14(1.28) | ||||||
| Humanities | 935 | 6.07(1.32) | ||||||
| Medical | 395 | 6.42(.99) | ||||||
| Sciences | 558 | 6.14(1.32) | ||||||
| Help.Prof. | 154 | 6.17(1.08) | ||||||
| ParaMedical | 212 | 6.29(1.27) | ||||||
| Total | 5642 | 6.14(1.28) | ||||||
| Agreement with | Gender | Male | 1542 | 5.80(1.42) | 55.59 | 1,6073 | < 0.001 | 0.006 |
| quarantine measures | Female | 4533 | 6.02(1.23) | |||||
| Total | 6075 | 5.96(1.29) | ||||||
| Area of Italy | North | 625 | 5.92(1.28) | 0.93 | 2,6038 | n.s. | 0.000 | |
| Center | 5066 | 5.96(1.29) | ||||||
| South | 350 | 6.04(1.27) | ||||||
| Total | 6041 | 5.96(1.29) | ||||||
| Area of Study | Technology | 933 | 5.92(1.32) | 2.41 | 6,5635 | 0.025* | 0.003 | |
| Soc.Sciences | 2455 | 5.96(1.27) | ||||||
| Humanities | 935 | 5.87(1.32) | ||||||
| Medical | 395 | 6.15(1.16) | ||||||
| Sciences | 558 | 5.97(1.37) | ||||||
| Help.Prof. | 154 | 5.97(1.27) | ||||||
| ParaMedical | 212 | 6.03(1.23) | ||||||
| Total | 5642 | 5.96(1.29) | ||||||
| COVID-19 real | Gender | Male | 1542 | 6.14(1.15) | 87.51 | 1,6073 | < 0.001 | 0.014 |
| emergency | Female | 4533 | 6.42(.96) | |||||
| Total | 6075 | 6.35(1.02) | ||||||
| Area of Italy | North | 625 | 6.38(.96) | 2.16 | 2,6038 | n.s. | 0.001 | |
| Center | 5066 | 6.34(1.03) | ||||||
| South | 350 | 6.44(1.00) | ||||||
| Total | 6041 | 6.35(1.02) | ||||||
| Area of Study | Technology | 933 | 6.28(1.06) | 3.42 | 6,5635 | 0.003* | 0.004 | |
| Soc.Sciences | 2455 | 6.36(1.00) | ||||||
| Humanities | 935 | 6.36(1.05) | ||||||
| Medical | 395 | 6.46(.92) | ||||||
| Sciences | 558 | 6.25(1.10) | ||||||
| Help.Prof. | 154 | 6.32(.95) | ||||||
| ParaMedical | 212 | 6.50(.87) | ||||||
| Total | 5642 | 6.35(1.02) | ||||||
| Average number of | Gender | Male | 1541 | 2.03(2.63) | 19.66 | 1,6071 | < 0.001 | 0.003 |
| outgoes per week | Female | 4532 | 1.68(2.64) | |||||
| Total | 6073 | 1.77(2.65) | ||||||
| Area of Italy | North | 625 | 1.89(2.74) | 8.16 | 2,6037 | < 0.001 | 0.003 | |
| Center | 5065 | 1.79(2.68) | ||||||
| South | 350 | 1.23(1.81) | ||||||
| Total | 6040 | 1.77(2.65) | ||||||
| Area of Study | Technology | 933 | 1.53(2.15) | 2.91 | 6,5633 | 0.008* | 0.003 | |
| Soc.Sciences | 2453 | 1.84(2.83) | ||||||
| Humanities | 935 | 1.73(2.62) | ||||||
| Medical | 395 | 1.80(2.43) | ||||||
| Sciences | 558 | 1.64(2.56) | ||||||
| Help.Prof. | 154 | 2.27(3.47) | ||||||
| ParaMedical | 212 | 1.62(2.38) | ||||||
| Total | 5640 | 1.75(2.65) | ||||||
| Worried about having | Gender | Male | 1542 | 3.17(1.63) | 102.69 | 1,6073 | < 0.001 | 0.017 |
| contracted COVID-19 | Female | 4533 | 3.68(1.74) | |||||
| Total | 6075 | 3.55(1.72) | ||||||
| Area of Italy | North | 625 | 3.65(1.70) | 2.84 | 2,6038 | n.s. | 0.001 | |
| Center | 5066 | 3.53(1.72) | ||||||
| South | 350 | 3.70(1.77) | ||||||
| Total | 6041 | 3.55(1.72) | ||||||
| Area of Study | Technology | 933 | 3.41(1.68) | 7.75 | 6,5635 | < 0.001 | 0.008 | |
| Soc.Sciences | 2455 | 3.69(1.73) | ||||||
| Humanities | 935 | 3.60(1.76) | ||||||
| Medical | 395 | 3.33(1.64) | ||||||
| Sciences | 558 | 3.28(1.68) | ||||||
| Help.Prof. | 154 | 3.74(1.68) | ||||||
| ParaMedical | 212 | 3.56(1.82) | ||||||
| Total | 5642 | 3.56(1.72) | ||||||
| COVID-19 laboratory- | Gender | Male | 1542 | 2.07(1.62) | 92.41 | 1,6073 | < 0.001 | 0.015 |
| created weapon | Female | 4533 | 2.58(1.89) | |||||
| Total | 6075 | 2.45(1.84) | ||||||
| Area of Italy | North | 625 | 2.37(1.83) | 4.75 | 2,6038 | .009* | 0.002 | |
| Center | 5066 | 2.44(1.83) | ||||||
| South | 350 | 2.73(1.99) | ||||||
| Total | 6041 | 2.45(1.84) | ||||||
| Area of Study | Technology | 933 | 2.43(1.80) | 27.93 | 6,5635 | < 0.001 | 0.029 | |
| Soc.Sciences | 2455 | 2.68(1.91) | ||||||
| Humanities | 935 | 2.42(1.88) | ||||||
| Medical | 395 | 1.78(1.46) | ||||||
| Sciences | 558 | 1.93(1.52) | ||||||
| Help.Prof. | 154 | 3.11(2.10) | ||||||
| ParaMedical | 212 | 2.12(1.53) | ||||||
| Total | 5642 | 2.45(1.84) | ||||||
| COVID-19 natural virus | Gender | Male | 1542 | 5.69(1.58) | 107.87 | 1,6073 | < 0.001 | 0.017 |
| Female | 4533 | 5.15(1.79) | ||||||
| Total | 6075 | 5.29(1.76) | ||||||
| Area of Italy | North | 625 | 5.37(1.76) | 1.76 | 2,6038 | n.s. | 0.001 | |
| Center | 5066 | 5.29(1.75) | ||||||
| South | 350 | 5.15(1.81) | ||||||
| Total | 6041 | 5.29(1.76) | ||||||
| Area of Study | Technology | 933 | 5.27(1.77) | 35.16 | 6,5635 | < 0.001 | 0.036 | |
| Soc.Sciences | 2455 | 5.05(1.80) | ||||||
| Humanities | 935 | 5.28(1.73) | ||||||
| Medical | 395 | 6.03(1.44) | ||||||
| Sciences | 558 | 5.83(1.52) | ||||||
| Help.Prof. | 154 | 4.65(1.95) | ||||||
| ParaMedical | 212 | 5.78(1.47) | ||||||
| Total | 5642 | 5.29(1.76) |
Note. Technology = Engineering, Architecture, Design, Informatics; Soc.Sciences = Social Sciences: Psychology, Sociology, Economy, Law, Educational Studies, . . . ; Humanities: Literature, Language, Philosophy, History, . . . ; Help.Prof. = Helping Professions: Nursing; ParaMedical = Biotechnology, Pharmacy, Odontoiatry, . . . ; *p is not statistically significant using the adjusted alpha level of 0.002.
The MANOVA multivariate test showed a statistically significant effect for gender: F(3, 6071) = 29.922, p < 0.001, partial η= 2.02. Follow-up ANOVAs highlighted that women, compared to men, have a higher level of agreement with both social isolation and quarantine measures. Women believe at a higher level that the virus is a real emergency.
The multivariate test did not show a statistically significant effect for the area of living: F(6, 12072) = 1.22, p = 0.291, partial η2 = 0.001.
Major of study has a multivariate statistically significant effect: F(18, 15933.015) = 0.99, p < 0.001, partial η2 = 0.003. Using our adjusted alpha level (0.002), follow-up ANOVAs highlighted a statistically significant difference for the level of agreement with social isolation regardless of the presence of flu symptoms. Bonferroni post-hoc analyses showed that Medical students had a higher level of agreement with social isolation compared to most of the other majors: Technology students (p < 0.001), Social Sciences students (p = 0.001), Humanities students (p < 0.001), and Sciences students (p = 0.023).
Gender has a statistically significant effect on all four variables analyzed. More specifically, males as compared to females, reported going out of the home a higher number of times per week and males had lower worries about having contracted COVID-19. Males are less likely to believe that COVID-19 is a laboratory-created weapon. Males are more likely than females to believe that it is a natural virus.
Regarding the geographic area of residence, we found a statistically significant effect only on the number of reports of going out of the home per week: students living in the south of Italy reported a lower average number than students living in the north of Italy (p = 0.001) and central Italy (p < 0.001).
The area of study does not have an effect on the average number of reported times of going out of the home per week. However, there is an influence on the preoccupation of having contracted the virus: Social Sciences students have a higher level of preoccupation than Technology students (p < 0.001), Medical students (p = 0.002), and Sciences students (p < 0.001). Humanistic students have a higher score for experiencing worry than Sciences students (p = 0.011). The belief that COVID-19 is a laboratory-created weapon is influenced by the area of study: Medical students and Sciences students have a lower level of belief than Technology students, Social Sciences students, Humanities students, and Helping Professions students (p < 0.001). Helping Professions students have a higher level of belief that COVID-19 is a laboratory-crated weapon than Technology students, Humanities students, or Paramedical students (p < 0.001). Social Sciences students have a higher level of belief than Technology students (p < 0.005) and Humanities students (p = 0.003), while Paramedical students (p < 0.001) have a lower level of belief than Social Sciences students (p < 0.001).
We found the major of study has a statistically significant effect on the belief that COVID-19 is a natural virus: Medical students and Sciences students are more likely to believe that it is natural than Technology students, Social Sciences students, Humanities students, and Helping Professions students (p < 0.001). Helping Professions students have a lower level of belief than Technology students (p = 0.001), Humanities students (p = 0.001), and Paramedical students (p < 0.001). Paramedical students have a higher level of belief that COVID-19 is a natural virus than Technology students (p = 0.002), Social Sciences students (p < 0.001), and Humanities students (p = 0.003). Social Sciences students have a lower level of belief than Technology students (p = 0.024) and Humanities students (p = 0.012).
3.3Predictors of agreement with government measures, worries about having contracted the virus, and calling for medical help
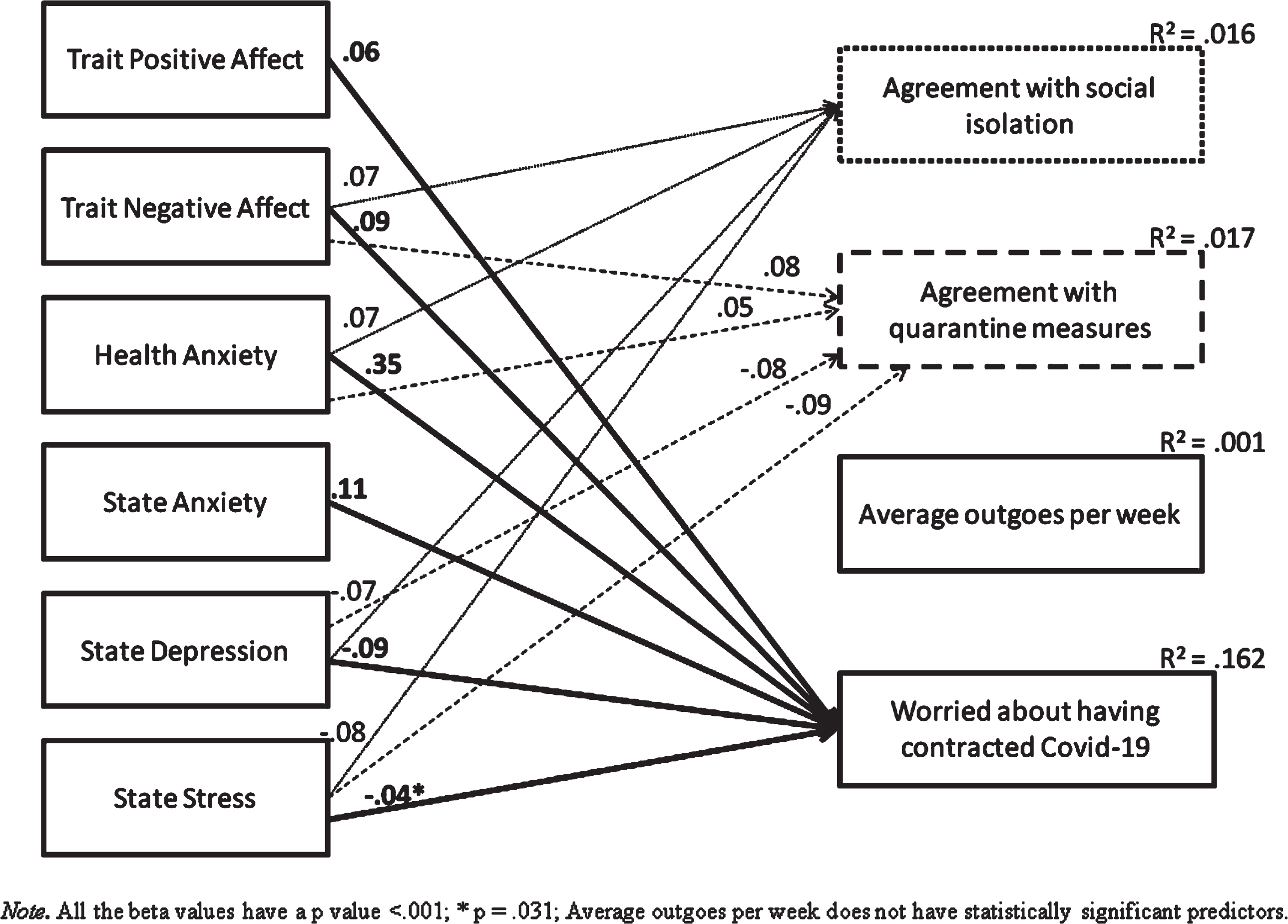
We performed a path analysis to evaluate if psychological variables (i.e., trait negative and positive affect, health anxiety, and current symptoms of anxiety, depression, and stress) predict level of agreement with the government measures or the amount of worry about having contracted the virus. The model showed an excellent fit to the data: χ2/df = 18.63, p < 0.001; GFI = 0.998; CFI = 0.997; RMSEA = 0.054, 90% CI = [0.042–0.067]. Other than the positive predictive value of health anxiety on the level of worry of having contracted the virus, no other psychological variables make a substantial contribution to the prediction of this and the other dependent variables (Fig. 1).
Fig. 1
Structural model with standardized path estimates (n = 6075).
To analyze if these psychological variables predict making the call for help during the COVID-19 pandemic, we performed four binary logistic regressions that included gender and age among the independent variables. All the models are statistically significant; however, just a few predictors reach statistical significance, and their OR values are barely higher than 1 (Table 3).
Table 3
Binary Logistic Regressions with age, gender, health anxiety, state anxiety, state depression, state stress, trait positive affect, and trait negative affect as predictors (n = 6075)
| Dependent variable | Predictors * | OR[95% CI] | p |
| Calling family doctor for oneselfa | Age | 1.03[1.01– 1.04] | 0.004 |
| Health Anxiety | 1.02[1.01– 1.02] | < 0.001 | |
| State Anxiety | 1.06[1.03– 1.09] | < 0.001 | |
| Trait Positive Affect | 1.02[1.00– 1.03] | 0.023 | |
| Calling the family doctor for othersb | Health Anxiety | 1.01[1.00– 1.03] | 0.017 |
| Trait Positive Affect | 1.02[1.00– 1.04] | 0.048 | |
| Calling a national official number for oneselfc | Age | 1.03[1.00– 1.06] | 0.04 |
| State Anxiety | 1.08[1.03– 1.13] | 0.001 | |
| Trait Positive Affect | 1.03[1.01– 1.06] | 0.011 | |
| Calling a national official number for othersd | Health Anxiety | 1.02[1.00– 1.03] | 0.019 |
Note. Only statistically significant predictors are reported. aLR Test =χ2(9) = 66.53, p < 0.001; Nagelkerke’s R = 0.028; bLR Test =χ2(9) = 23.81, p = 0.005; Nagelkerke’s R = 0.013; c χ2(9) = 33.96, p < 0.001, Nagelkerke R2 = 0.027; dχ2(9) = 21.32, p = 0.011, Nagelkerke R2 = 0.018.
4Discussion
The COVID-19 pandemic challenged all countries worldwide with a need to contain the spread of this new harmful virus. This study proves Italian college students perceived the COVID-19 outbreak as a real emergency and most agreed with the government’s measures. Most students complied with the requirement to only leave home if strictly necessary, and just a minority of students traveled across Italy when it was forbidden.
There are some demographic-related differences. Women, as compared to men, reported a higher level of agreement with measures for social isolation (despite the lack of flu-like symptoms) and quarantine. Accordingly, females left home at a lower rate than males. Females had more worries about having contracted COVID-19. Females are more likely to believe that the virus is a real emergency and they are more likely to believe that it is a laboratory-created weapon, while males are more likely to believe that it is a natural virus. Students living in the south of Italy reported a lower average number of times of going out from the home per week than students living in the north and central parts of Italy. Among students of different academic majors, our main findings showed that Medical students have a higher likelihood to agree with social isolation measures as compared to most of the other majors (Technology, Social Sciences, Humanities, and Sciences). Additionally, we found Social Sciences students reported the highest preoccupation levels about having contracted the virus, especially when compared to Technology students, Medical students, and Sciences students. Medical students and Sciences students are less likely to believe that COVID-19 is a laboratory-created weapon and they are more likely to believe that it is a natural virus as compared to most of other majors (Technology, Social Sciences, Humanities, and Helping Professions).
The psychological variables we analyzed as potential predictors of compliance with the government’s requirement do not predict (or predict with very low beta values) the likelihood of agreement with social isolation and quarantine measures. Though, it is interesting to note that the agreement with social isolation and quarantine measures is positively predicted by trait negative affect and health anxiety, while it is negatively predicted by current symptoms of depression and stress. We conjecture that depression and stress are negative predictors since people experiencing high levels of these symptoms due to home confinement might be moved to actions by the desire to get out from home, despite the increased risk to health. This speculation should be tested through future qualitative and quantitative studies.
We analyzed if psychological variables, gender, and age predict the likelihood of calling for help during the COVID-19 pandemic. Again, the psychological variables did not play a strong role, as highlighted by the scant amount of variance explained on the dependent variables. They do not seem to be valuable for planning intervention for increasing compliance with the government requirements or the development of a more suitable approach to making the call for help.
5Conclusions
Based on our demographic-related findings, we speculate that interventions to foster compliance with government restrictions to contain a pandemic might primarily address males. We found that most non-Medical students believed that social isolation is not as crucial for those who have no symptoms and that students of majors other than Medical and Sciences areas have a higher likelihood of accepting the belief that the virus is a laboratory-created weapon. Hence, we suggest implementing university-based interventions aimed towards increasing students’ compliance with restrictions and rules during a pandemic. College students, especially Social Sciences students as those more likely to be worried about having contracted the virus, might benefit from counseling interventions to manage anxieties and to avoid the development of psychological disorders fueled by the pandemic. We found that the worry of having contracted the virus is positively predicted by health anxiety. We believe that it is imperative to reduce anxiety, for example, through interventions aimed at increasing awareness of real health risks.
Among the main limitations of this study, there is an unequal geographic distribution with a higher presence of students from central Italy. Gender distribution has a high proportion of females. As another limitation, it would be interesting to replicate the study with adolescents and to compare the results with students of different ages. We recruited university students and we did not recruit from the workforce. Workers might have showed different degrees of agreement with the government measures, beliefs concerning the nature of the virus, and relationships with the analyzed psychological variables. However, this study has the merit of having a wide sample of Italian college students, and our sample is heterogeneous for year and major. We encourage future researchers to examine factors such as availability and type of media communications, socioeconomic status, and family structure.
Our study sheds light on the responsible behavior taken by Italian college students during the COVID-19 pandemic. Generally, they respected the measures established to contain the spread of the virus. In addition, we believe there is a need for prevention interventions to decrease anxiety and avoid the development of psychological disorders, especially in Social Sciences students. We suggest that the psychological variables we analyzed are not valuable for studying compliance with government rules. We postulate that other variables might be more critical for understanding potential for compliance with restrictive measures such as social isolation and quarantine.
Conflict of interest
None to report.
References
[1] | Guan W-J , Ni Z-Y , Hu Y , et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020) ;328: (18):1708–20. |
[2] | Liu Y , Gayle AA , Wilder-Smith A , Rocklöv J . The reproductive number of COVID-19 is higher compared to SARS coronavirus. J Travel Med. (2020) ;27: (2):taaa021. |
[3] | Rocklöv J , Sjödin H , Wilder-Smith A . COVID-19 outbreak on the Diamond Princess cruise ship: Estimating the epidemic potential and effectiveness of public health countermeasures. J Travel Med. (2020) ;27: (3):taaa030. |
[4] | Ryu S , Chun BC . Epidemiological characteristics of novel coronavirus: An interim review. Epidemiol Health. (2020) ;42: :e2020–2026. |
[5] | Wang C , Horby PW , Hayden FG , et al. A novel coronavirus outbreak of global health concern. Lancet. (2020) ;395: (10223):470–3. |
[6] | World Health Organization (2020). Coronavirus disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2020083-1weekly-epi-update-3.pdf?sfvrsn=d7032a2a_4. Accessed September 1, 2020. |
[7] | Gagliano A , Villani PG , Cò FM , et al. 2019-nCov’s epidemic in middle province of northern Italy: Impact, logistic & strategy in the first line hospital. [published online March 24, 2020]. Disaster Med Public Health Prep. (2020) ;24: . |
[8] | Afshari D , Nourollahi-darabad M , Chinisaz N . Demographic Predictors of Resilience Among Nurses During the COVID-19 Pandemic. Work. (2021) ;68: (2):297–303. |
[9] | De Sio S , Buomprisco G , La Torre G , Lapteva E , Perri R , Greco E , Mucci N , Cedrone F . The impact of COVID-19 on doctors’ well-being: results of a web survey during the lockdown in Italy. Eur Rev Med Pharmacol Sci. (2020) ;24: (14):7869–79. |
[10] | Loscalzo Y , Marucci S , Garofalo P , Attanasio R , Lisco G , De Geronimo V , Guastamacchia E , Giannini M , Triggiani V . Assessment of Burnout Levels before and duringCOVID-19 Pandemic: A Web-Based Survey by the (Italian) Association of Medical Endocrinologists (AME). Endocr Metab Immune Disord Drug Targets; in press. |
[11] | Maduke T , Dorroh J , Bhat A , Krvavac A , Regunath H . Are We Coping Well with COVID-19? A Study on Its Psycho-Social Impact on Front-line Healthcare Workers. Mo Med. (2021) ;118: (1):55–62. |
[12] | Pniak B , Leszczak J , Marzena A , Wojciech R , Matlosz P , Guzik A . Occupational Burnout Among Active Physiotherapists Working in Clinical Hospitals During the COVID-19 Pandemic in South-eastern Poland. Work. (2021) ;68: (2):285–95. |
[13] | Yang Q , Huo j , li J , Jiang Y . Research on the Influence of the COVID-19 Epidemic on Work Stress of Returning Workers in China: A Study Based on Empirical Analyses of Industrial Enterprises. Work. (2020) ;67: (1):67–79. |
[14] | Memari A , Shariat A , Anastasio AT . Rising Incidence of Musculoskeletal Discomfort in the Wake of the COVID-19 Crisis. Work. (2020) ;66: (4):751–3. |
[15] | Zandian H , et al. Evaluation of Knowledge and Health Behavior of University of Medical Sciences Students About the Prevention of COVID-19. Work. 2021: :543–9. |
[16] | Loscalzo Y , Giannini M . Covid-19 outbreak and Italian College Students’ well-being: Evidence for both negative and positive consequences. Psychology Hub. Manuscript accepted for publication. 2022. |
[17] | Loscalzo Y , Ramazzotti C , Giannini M . Studyholism e Study Engagement in relazione alle conseguenze sullo studio dovute alla pandemia da Covid- Uno studio pilota quali-quantitativo su studenti universitari [Studyholism and Study Engagement in relation to the consequences on study due to the Covid-19 pandemic: A qualitative quantitative pilot study on university students]. Counseling. (2021) ;14: (2):79–91. DOI:10.14605/CS1422106 |
[18] | Loscalzo Y , Giannini M . Covid-19 outbreak: What impact of the lockdown on college students’ academic path and attitudes toward studying? Applied Psychological Bulletin. (2021) ;291: (2):63–74. DOI: 10.26387/bpa.291.5 |
[19] | Watson D , Clark LA , Tellegen A . Development and validation of brief measure of positive and negative affect: the PANAS scales. J Pers Soc Psychol. (1998) ;54: (6):1063–70. |
[20] | Terracciano A , McCrae RR , Costa PT Jr . Factorial and construct validity of the Italian positive and negative affect schedule (PANAS). Eur J Psychol Assess. (2003) ;19: (2):131–41. |
[21] | Lovibond PF , Lovibond SH . The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. (1995) ;33: (3):335–43. |
[22] | Bottesi G , Ghisi M , Altoè G , Conforti E , Melli G , Sica C . The Italian version of the Depression Anxiety Stress Scales- Factor structure and psychometric properties on community and clinical sample. Compr Psychiatry. (2015) ;60: :170–81. |
[23] | Lovibond SH , Lovibond PF . Manual for the Depression Anxiety Stress Scales. 2nd edition. (1995) ; Sydney: Psychology Foundation. |
[24] | Lucock MP , Morley S . The Health Anxiety Questionnaire. Br J Health Psychol. (1996) ;1: (2):137–50. |
[25] | Melli G , Coradeschi D , Smurra . La versione italiana dell’Health Anxiety Questionnaire: attendibilitá e struttura fattoriale [The Italian version of the Health Anxiety Questionnaire: Internal reliablity and factorial structure]. Psicoterapia Cognitiva e Comportamentale. (2007) ;13: (1). |
[26] | Chen SY , Feng Z , Yi X . A general introduction to adjustment for multiple comparisons. J Thorac Dis. (2017) ;9: (6):1725–9. |
[27] | Byrne BM . Structural equation modeling with AMOS: Basic concepts, applications, and programming. (2001) ; Mahwah, NJ: Lawrence Erlbaum Associates. |
[28] | Hu L , Bentler PM . Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct Equ Modeling. (1999) ;6: (1):1–55. |
[29] | Reeve BB , Hays RD , Bjorner JK , et al. Psychometric Evaluation and Calibration of Health Related Quality of Life Item Banks: Plans for the Patient-Reported Outcomes Measurement Information System (PROMIS). Med Care. (2007) ;45: (5):S22–S31. |


