
New patient access via telehealth in neuromuscular medicine during COVID-19
Abstract
BACKGROUND:
The coronavirus disease 2019 (COVID-19) pandemic has changed the face of health care delivery. Health care institutions rapidly transitioned to telehealth to provide care to patients. Prior to the pandemic, telehealth services extended mostly to patients with established diagnoses. Driven by a necessity to provide care to all patients during the pandemic, neurologists started evaluating new patients also via telehealth.
OBJECTIVE:
To explore opportunities, challenges, and feasibility of telehealth for new patients with neuromuscular disorders.
METHODS:
New patient visits performed in our neuromuscular clinic were analyzed from March 18, 2020 - July 31, 2020. Data collected included visit volume, demographics, geographic distance of patient’s residence from our institution, and no-show and cancellation rates.
RESULTS:
Total number of patients seen was 1,471; 472 (32%) were new patients. No-show and cancellation rates for telehealth visits were lower than historical in-person visits. There was a wide range of ages (35–74 years) with representation of new patients from a large geographical territory.
CONCLUSION:
This study advances our understanding regarding the adoption and implementation of telehealth for new patients. Our clinic was able to provide timely access and care to a significant number of patients who could not travel to our institution during COVID-19.
1Introduction
The coronavirus disease 2019 (COVID-19) pandemic created unprecedented challenges in health care, requiring the rapid adoption of telehealth not only for established patients, but also for new patients across all medical practices and various subspecialties. The silver lining in this pandemic is the future opportunity to continue supporting virtual care to patients even beyond the pandemic. This is especially important in an era where access to neurology is a growing problem [1] with an anticipated 19%shortfall of neurologists by 2025 [2]. The benefits of telehealth have been clearly demonstrated in several neurological disorders, including multiple sclerosis, Parkinson disease, dementia, migraine, and epilepsy [3–8]. Neuromuscular disorders, such as amyotrophic lateral sclerosis and muscular dystrophy, have also been found to be suitable for telehealth [9–14].
As the stay-at-home order in Dallas County started on March 15, 2020, our institution rapidly expanded virtual care with the number of virtual visits jumping from 190 in the early part of March 2020 to 25,197 by the end of April 2020. This included access for new and established patients. In this paper, we present data on new patients seen via telehealth in our neuromuscular clinic, review challenges, and explore feasibility of delivering virtual care to new patients even beyond the pandemic. Personal patient identifiers were not used for this study; the study was thereby waived by the institutional review board.
2Impact of COVID-19 on new patient access
As the prevalence of COVID-19 increased nationally, our institution implemented an urgent expansion of telehealth capabilities for new and established patients. While we extended telehealth access initially to only established patients, we had numerous requests for new patient evaluations, some urgent and many others that had been waiting to be seen in our clinic for a long time. At first, our neurologists were reluctant to use the virtual platform for new patients; however, given the uncertain length of the pandemic, virtual care was adopted for new patients as well. With the temporary lifting of restrictive regulations, this care also extended to new patients across state boundaries.
In this study, we review data on new patient visits performed in our neuromuscular clinic from March 18, 2020 through July 31, 2020. The data used throughout the paper is sourced from appointment data in Epic, our institution’s electronic medical record. Total visit volume, visit type, age, gender, geographic distance of the patients’ residence from our institution, and no-show and cancellation rates were collected and analyzed. Our analysis is limited, with the primary focus being on evaluating new patient virtual visit data, including access, challenges, and feasibility of telehealth for new patients.
3Results
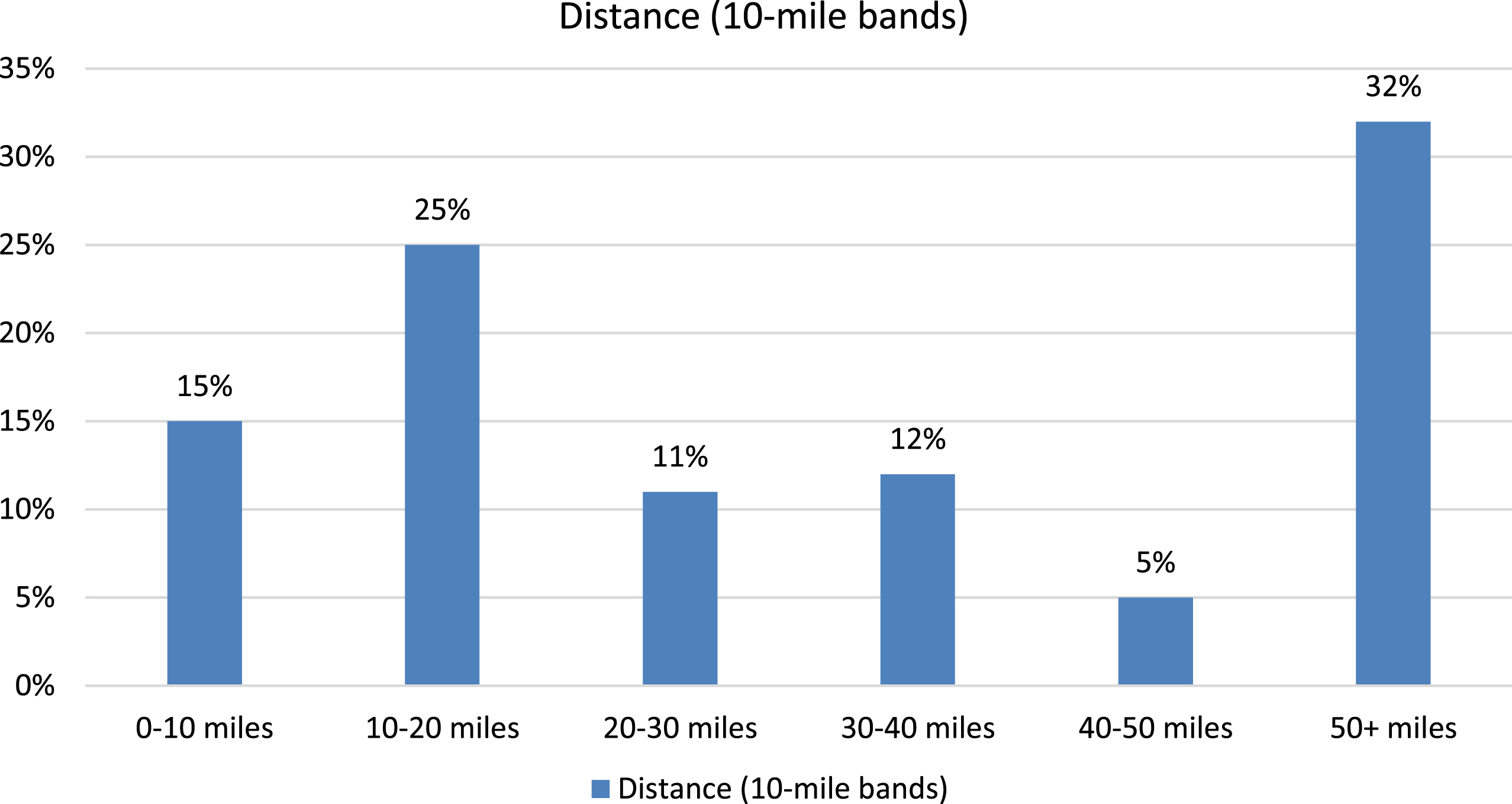
The total number of patients seen in the neuromuscular clinic via virtual care from March 18, 2020 to July 31, 2020 was 1,471 (Table 1). Of these, 472 (32%) were new to clinic and 999 (68%) were established patients. The percentages of appointment completion (76.4%vs. 72.4%), no-show rate (4.5%vs. 5.4%), and cancellations (18.4%vs. 21.2%) did not differ greatly between the new and established visits (Table 1). The no-show rate and cancellation rate for telehealth visits was lower than historical values, which were predominately for in-person visits. There was a wide range of ages, with most patients being between 35–74 years age (Fig. 1). Patients were from 13 states, including Texas. Figure 2 illustrates the volume of completed visits by the distance between patients’ residence and our institution, with about a third of the patients (32%) living 50 + miles away. Of the 472 new patient virtual visits, 161 patients (34%) were seen subsequently in clinic for electrophysiologic testing. During this visit, the patients underwent a complete neurological examination and laboratory testing as indicated. Other patients were seen in follow-up, either in-person or via telehealth. This data was not available at the time of this study.
Table 1
Telehealth Visits in the Neuromuscular Clinic (March 18, 2020 - July 31, 2020)
| News (%) | Established (%) | Total | |
| Scheduled | 617 | 1,379 | 1,996 |
| Completed visits | 472 (76.4) | 999 (72.4) | 1,471 |
| No-shows | 28 (4.5) | 75 (5.4) | 103 |
| Cancellations | 114 (18.4) | 293 (21.2) | 407 |
| Left without being seen | 3 | 12 | 15 |
Fig. 1
Age distribution of new patients with completed telehealth appointments.
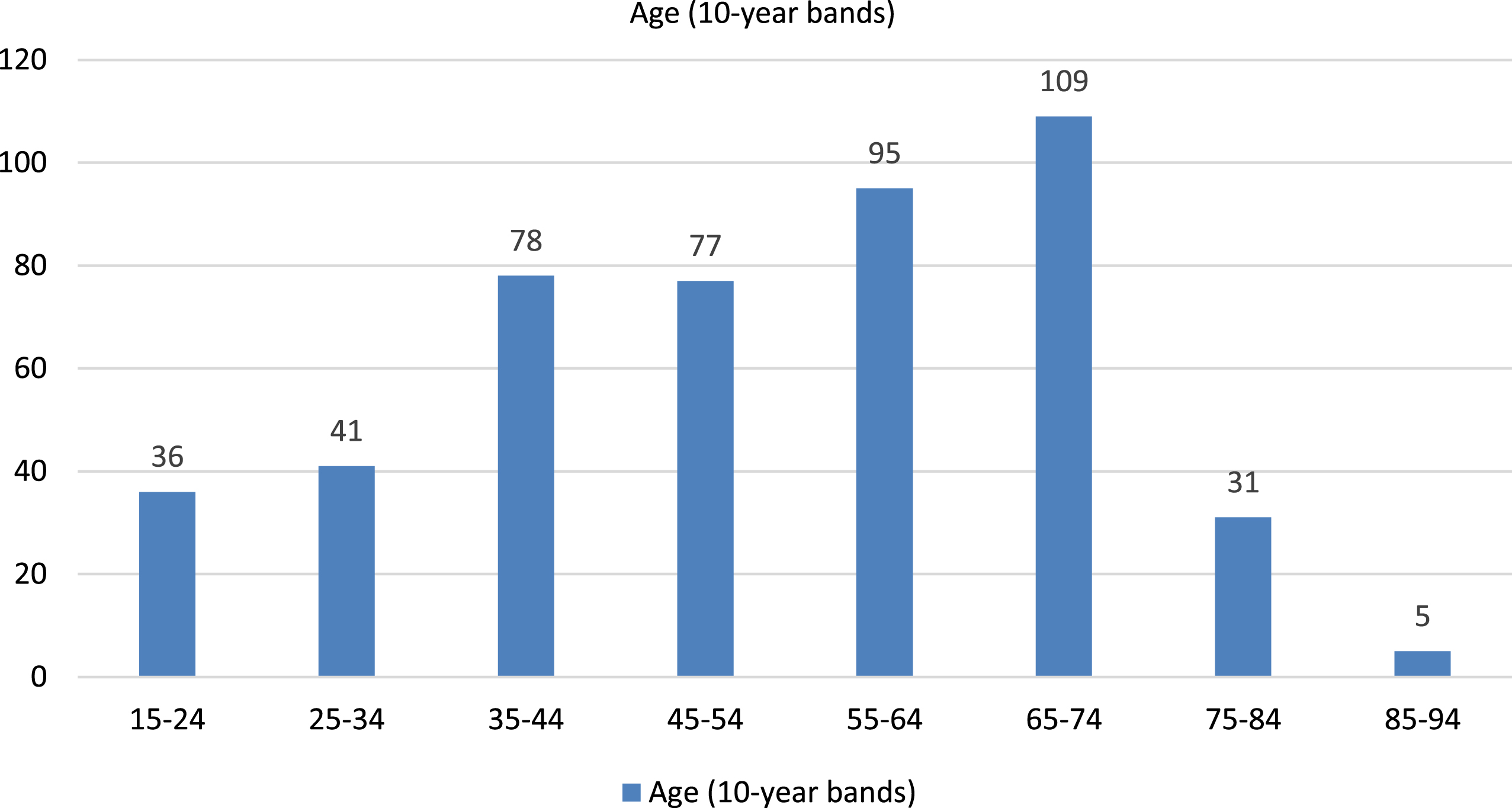
Fig. 2
Geographical distribution of completed new patient telehealth visits. Geographical data was not available in 4 patients.
3.1Challenges and advantages of new patient evaluation via telehealth during COVID-19
The physical exam is paramount in the evaluation and management of neuromuscular disorders; it is the gold standard and cannot be replaced. Proximal or distal weakness can localize to the muscles, peripheral nerves, neuromuscular junction, lower motor neurons, or could be central nervous system in origin; in all these cases, the neurological examination is crucial. Critical elements of strength, sensation, and reflex examination are needed to make a diagnosis. Another concern is that of patient safety during a telehealth visit. This comes up during gait evaluation of a patient with sensory ataxia, spasticity, or weakness. At-home evaluation of such a patient via telehealth, in the absence of caregiver presence, is risky as it can lead to falls. These limitations of physical exam affected our ability to diagnose or confirm neuromuscular disorders in some of the new patients during their telehealth visit. To this end, we would schedule patients for an in-person visit in clinic often linked to their procedure visit, both performed by a neuromuscular specialist. We were able to accommodate these combined visits in a third of our new patients. Another challenge was ensuring these new patients returned for a follow up, especially when Dallas county was in lockdown and patients were hesitant to travel long distances or across state boundaries during the pandemic.
Despite the aforementioned challenges, our clinic was able to provide care to a significant number of new patients, both locally and from 12 other states. Most importantly, it allowed us to continue providing care to new patients that could not travel to our institution during this lengthy pandemic. Fortunately, most new patients had seen community neurologists and therefore neurological exams were available for review and, in many cases, the diagnoses had been well established.
3.2Feasibility of new patient evaluation via telehealth post COVID-19: is this an option in neuromuscular medicine?
Poor access harms neurology. It lowers the quality of care, lowers patient satisfaction, and slows development of research. In the past few years, the demand for a neurologist has outgrown supply and this mismatch will only get worse with an anticipated 19%shortfall of neurologists by 2025 [2]. There is a need to increase access to new patients, decrease appointment wait times, and improve clinic workflow. Telehealth opens the doors to timely access to care, access to subspecialists, and clinical trial participation [6]. Other advantages include: decrease in travel burden for patients, possible reduction in overhead for medical practices, reduced caregiver burden, improved patient satisfaction, and flexibility in work schedule for providers thereby reducing burnout [14–16]. Technological advances, widespread and reliable wireless connectivity, and more affordable electronic devices make telehealth an even more desirable platform to provide care. When patients are unable or unwilling to travel, an initial visit via telehealth may be preferred over complete lack of neurological care [17].
The rapid expansion of telehealth in medicine during COVID-19 has led to immense opportunities to further extend this platform of care to neurology patients even beyond the pandemic. Barring legislations, reimbursement policies, technological limitations, medico-legal concerns and other barriers, new patients will likely be seeking care via telehealth even beyond the pandemic. In neuromuscular medicine, patients often have chronic disabling conditions with mobility issues that limit the ability to make the trips to their physician’s offices, especially those living in assisted living facilities [18]. Additionally, some patients live in rural areas where there is a shortage of neurologists while others have rare disorders and are seeking subspecialty neuromuscular care at tertiary care centers. While nothing replaces the traditional in-person physical exam, telehealth is perhaps feasible in these patients as well as those with select diagnoses such as diabetic polyneuropathy, radiculopathy, well-established diagnosis of myasthenia gravis, or genetically confirmed hereditary neuromuscular disorders. The telehealth new visit could be applied as a triage or an intake visit for patients that need an urgent evaluation; this would be followed by an in-person exam. This triaging method addresses limitations in the physical examination and is of value in managing chronic disorders [19]. Some patients might prefer this option over waiting for an appointment for many months or not getting care at all [17]. Additionally, expanding the use of telehealth services goes beyond direct neurological care by a neuromuscular specialist. Other allied health services such as physical therapy (PT), occupational therapy (OT), and speech therapy (ST) serve a vital role in the care of our patients, and telehealth offers an opportunity to expand access to these services. Telehealth has been show to produce similar outcomes to in-person rehabilitation services [21]; in one survey of occupational therapy practitioners (OTP) new to telehealth completing a school-based training program, 80%indicated they are likely to add telehealth to their future OT practice [22]. The demand for OT services is also growing and outpacing the supply, with an anticipated shortage of OTPs occurring by 2030 [21]; so simultaneous access to neurological care and its allied services via telehealth is crucial.
Provision of care to new patients via telehealth is a large cultural shift in neuromuscular disorders. There is data to support patient satisfaction, cost savings, and improved outcomes in select neuromuscular disorders [14]. However, further studies are needed to validate outcomes, patient-physician satisfaction, access to care, diagnostic accuracy, and cost savings comparing these quality measures between telehealth and in-person evaluations. Determining which disorders would be feasible and viable for virtual care and developing standards of care for telehealth will be important. From an administrative standpoint, there will be a need to evaluate workflow processes and staffing models given that the infrastructure for telehealth visit is much different from in-person visits. Practices will need to be cognizant of patients with cognitive, visual, and hearing impairment for whom telehealth may not be an optimal platform and for those individuals with socioeconomic limitations [19, 20]. Telehealth has changed the face of health care delivery; hopefully, federal and state regulations will allow continuation of this endeavor beyond the pandemic.
4Conclusion
In conclusion, despite the drawn-out pandemic, telehealth has continued to provide an opportunity to provide care to new patients that cannot travel to medical practices. While traditional in-clinic care is valuable, telehealth provides an advantageous leap forward to improve timely access to new patients in an era where demand exceeds capacity. Further studies will broaden our understanding about feasibility of providing access to new patients in neuromuscular disorders via telehealth, beyond the pandemic.
Conflict of interest
None to report.
References
[1] | Freeman WD , Vatz KA , Griggs RC , Pedley T . The Workforce Task Force report: clinical implications for neurology. Neurology. (2013) ;81: (5):479–86. |
[2] | Dall TM , Storm MV , Chakrabarti R , Drogan O , Keran CM , Donofrio PD , Henderson VW , Kaminski HJ , Stevens JC , Vidic TR . Supply and demand analysis of the current and future US neurology workforce. Neurology. (2013) ;81: (5):470–8. |
[3] | Robb JF , Hyland MH , Goodman AD . Comparison of telemedicine versus in-person visits for persons with multiple sclerosis: A randomized crossover study of feasibility, cost, and satisfaction. Mult Scler Relat Disord. (2019) ;36: :101258. |
[4] | Achey M , Aldred JL , Aljehani N , Bloem BR , Biglan KM , Chan P , Cubo E , Dorsey ER , Goetz CG , Guttman M , Hassan A , Khandhar SM , Mari Z , Spindler M , Tanner CM , Van den Haak P , Walker R , Wilkinson JR . The past, present, and future of telemedicine for Parkinson’s disease. Mov Disord. (2014) ;29: (7):871–83. |
[5] | Ben-Pazi H , Browne P , Chan P , Cubo E , Guttman M , Hassan A , Hatcher-Martin J , Mari Z , Moukheiber E , Okubadejo NU , Shalash A . The Promise of Telemedicine for Movement Disorders: an Interdisciplinary Approach. Curr Neurol Neurosci Rep. (2018) ;18: (5):26. |
[6] | Friedman DI , Rajan B , Seidmann A . A randomized trial of telemedicine for migraine management. Cephalalgia. (2019) ;39: (12):1577–85. |
[7] | Powers JS , Buckner J . Reaching Out to Rural Caregivers and Veterans with Dementia Utilizing Clinical Video-Telehealth. Geriatrics (Basel). (2018) ;3: (2). |
[8] | Haddad N , Grant I , Eswaran H . Telemedicine for patients with epilepsy: a pilot experience. Epilepsy Behav. (2015) ;44: :1–4. |
[9] | Garibaldi M , Siciliano G , Antonini G . Telemedicine for neuromuscular disorders during the COVID-19 outbreak. J Neurol. 2020. |
[10] | Portaro S , Calabro RS , Bramanti P , Silvestri G , Torrisi M , Conti-Nibali V , Caliri S , Lunetta C , Alagna B , Naro A , Bramanti A . Telemedicine for Facio-Scapulo-Humeral Muscular Dystrophy: A multidisciplinary approach to improve quality of life and reduce hospitalization rate? Disabil Health J. (2018) ;11: (2):306–9. |
[11] | Andrews JA , Berry JD , Baloh RH , Carberry N , Cudkowicz ME , Dedi B , Glass J , Maragakis NJ , Miller TM , Paganoni S , Rothstein JD , Shefner JM , Simmons Z , Weiss MD , Bedlack RS . Amyotrophic lateral sclerosis care and research in the United States during the COVID-19 pandemic: Challenges and opportunities. Muscle Nerve. (2020) ;62: (2):182–6. |
[12] | Haulman A , Geronimo A , Chahwala A , Simmons Z . The Use of Telehealth to Enhance Care in ALS and other Neuromuscular Disorders. Muscle Nerve. (2020) ;61: (6):682–91. |
[13] | Paganoni S , Simmons Z . Telemedicine to innovate amyotrophic lateral sclerosis multidisciplinary care: The time has come. Muscle Nerve. (2019) ;59: (1):3–5. |
[14] | Hatcher-Martin JM , Adams JL , Anderson ER , Bove R , Burrus TM , Chehrenama M , O’Brien MD , Eliashiv DS , Erten-Lyons D , Giesser BS , Mpp LR , Narayanaswami P , Rossi MA , Soni M , Tariq N , Tsao JW , Vargas BB , Vota SA , Wessels SR , Planalp H , Govindarajan R . Telemedicine in neurology: Telemedicine Work Group of the American Academy of Neurology update. Neurology. (2020) ;94: (1):30–8. |
[15] | Ray KN , Chari AV , Engberg J , Bertolet M , Mehrotra A . Disparities in Time Spent Seeking Medical Care in the United States. JAMA Intern Med. (2015) ;175: (12):1983–6. |
[16] | Howard IM , Kaufman MS . Telehealth applications for outpatients with neuromuscular or musculoskeletal disorders. Muscle Nerve. (2018) ;58: (4):475–85. |
[17] | Wechsler LR . Advantages and limitations of teleneurology. JAMA Neurol. (2015) ;72: (3):349–54. |
[18] | Chirra M , Marsili L , Wattley L , Sokol LL , Keeling E , Maule S , Sobrero G , Artusi CA , Romagnolo A , Zibetti M , Lopiano L , Espay AJ , Obeidat AZ , Merola A . Telemedicine in Neurological Disorders: Opportunities and Challenges. Telemed J E Health. (2019) ;25: (7):541–50. |
[19] | Dorsey ER , Topol EJ . State of Telehealth. N Engl J Med. (2016) ;375: (14):1400. |
[20] | Grossman SN , Han SC , Balcer LJ , Kurzweil A , Weinberg H , Galetta SL , Busis NA . Rapid implementation of virtual neurology in response to the COVID-19 pandemic. Neurology. (2020) ;94: (24):1077–87. |
[21] | Hoel V , von Zweck C , Ledgerd R ; World Federation of Occcupational Therapists. Was a global pandemic needed to adopt the use of telehealth in occupational therapy? Work. (2021) ;68: (1):13–20. |
[22] | Abbott-Gaffney C , Jacobs K . Telehealth in school-based practice: Perceived viability to bridge global OT practitioner shortages prior to COVID-19 global health emergency. Work. (2020) ;67: (1):29–35. |


