
A systematic review of working conditions and occupational health in home office
Abstract
BACKGROUND:
In times of the COVID-19 pandemic, employees around the world may be practicing part-time telework at home. Little is known about the working conditions at home and its impact on the employee’s occupational health.
OBJECTIVE:
This systematic review examines the working conditions at employees’ homes, the work-related disorders associated with working from home, organizations’ perceptions of ergonomics at home and how they support their teleworkers.
METHODS:
A search of electronic databases (Cochrane Library, Embase, Medline, Google Scholar, Open Grey, Pedro, PsychInfo, PubPsych, Scopus and Web of Science) was performed. Twelve studies were included in this review.
RESULTS:
The findings highlight the lack of ergonomic working conditions for home-based teleworkers. Furthermore, the results underline organizations’ lack of awareness regarding home-based policies, ergonomics programs and the health-related consequences associated with the absence of ergonomic support.
CONCLUSION:
These findings suggest that home-based teleworkers have increased health risks. This assumption is substantiated by the fact that most of the included studies reported teleworkers who have experienced musculoskeletal issues. These results underline the necessity for implementing ergonomic design recommendations, especially for working at home. Further research is needed to understand the impact of ergonomics programs and workplace design for working at home.
1Introduction
The increasing flexibility in working hours and the delocalization of the workplace over the past 50 years have been a part of the New Ways of Working (NWW) era, better known as telework [1]. A variety of definitions exist for the term “telework” [2–4]. In the past, telework was perceived as one of several types of work that differ from traditional office work. Telework is characterized by employees’ increased use of information and communications technologies (ICTs), which allow users to work from anywhere and at any time [5–7].
Since the 20th century, both employers and employees viewed teleworking as an extended workplace [8–11]. Past research has examined the effects of part-time telework on either job-related outcomes, such as job performance or job satisfaction [12, 13], as well as absenteeism and work-life balance [6, 14] or family-work/work-family conflict [8, 15], but not much research exists regarding general working conditions at home-based telework. The systematic review on the topic of ergonomics and telework by de Macedo et al. [16] showed that the interest about ergonomics and teleworking is increasing in the economy, especially in the United States and Europe. According to de Macedo et al. [16] the growing attention is related to the increased flexibility made possible by remote working and the necessity to address the new working conditions in the home office [17]. The systematic review from de Macedo et al. [16] examined the advantages and disadvantages of telework and the growing interest worldwide. In contrast, the present review aims to investigate the research gap in more detail by examining the impact of the may existing working condition in the home office and its effect on employee’s health.
As mentioned above teleworking enjoys many advantages, such as working across geographical boundaries; communication and collaboration take place in virtual spaces or chats and is supposed to be less time-consuming and more efficient than on-site conferences [18, 19]. All these reasons are why telework has a reputation for improving work-life balance because the time flexibility it offers is highly appreciated [20–23]. However, the mentioned increased use of ICTs may lead employees to develop musculoskeletal disorders (MSDs) [22, 24–26]. Various studies have shown that teleworking is asscociated with the likelihood to experience MSDs [19, 27–29]. MSDs include injuries and disorders of the muscles, nerves, tendons, ligaments, joints, cartilage, and spinal discs [30]. MSDs include repetitive strain injuries, also known as cumulative trauma disorders. These disorders are not immediately apparent and can take days, months or years before they affect a worker [31]. Therefore, the World Health Organization (WHO) recommends that organizations implement ergonomics to promote health, prevent injuries and reduce the occurrence of MSDs in office settings. These interventions aim to change workplace behavior and improve work conditions [32].
However, while the ergonomic workplace conditions at the regular workplace are mostly well covered and researched [33], the question arises if these interventions also offered to home-based teleworkers? Therefore, the present systematic review examines the following research questions: (1) Under which conditions do home-based teleworkers perform their work? (2) Do home-based teleworkers report work-related disorders? and (3) What current policies and ergonomic training programs do organizations implement for their employees who work at home? By answering these questions, the present review makes an important contribution to the existing literature and workplace design in the home office.
2Materials and methods
2.1Search strategy
After an initial literature search in March 2020, a search strategy was developed. The search then began in April 2020 and was completed in June 2020. This review followed the systematic literature review guidelines, as presented by PRISMA [34]. To ensure that this review had a broad data set, a comprehensive cross-disciplinary search was conducted in the following electronic databases: Cochrane Library (n = 8), Embase and MedLine (n = 1,449), Google Scholar, Open Grey (n = 23), PEDro (n = 248), PsychInfo (n = 4,124), PubPsych (n = 117), Scopus (n = 1,470) and Web of Science (n = 890).
2.2Inclusion criteria
This systematic review included studies published between 1990 and 2020. The studies were peer-reviewed and available in English and German. Inclusion criteria were defined using PICo: population (P), the phenomenon of interest (I) and context (Co) [35–37]. The search terms were combined into three groups according to PICo: (1) The population consisted of people who work at home; therefore, the research team searched explicit for teleworkers who were allowed to work at home at least one day per week. The relevant population also needed to have an age-appropriate state of health. (2) The phenomena of interest included ergonomic workplace designs at home, workers’ physical activity and work-related disorders originating from home-based teleworking. (3) The context included organizations’ general perceptions of home-based teleworking, organizations’ ergonomics policies and the support organizations offer their home-based teleworkers, such as ergonomic programs or training. This review’s search terms can be found in Table 1.
Table 1
Search terms and databases (using search string AND / OR)
| PICO | Search terms |
| Population (P) | Home-based teleworker; working at home, telecommuting at home; home-based telecommute; home working; employees who working at home; flexible worker; mobile worker; virtual worker |
| Phenomenon of interest (I) | Health; physical health; occupational health; ergonomics; ergonomics intervention; ergonomics program; fitness program; teleworking policies; teleworking programs; physical activity; musculoskeletal disorder; musculoskeletal pain; musculoskeletal problems; musculoskeletal complaints; physical complaints; shoulder, neck; lower back; upper extremity musculoskeletal disorder; musculoskeletal injuries; tension neck syndrome; eye symptoms |
| Context (Co) | Working at home; workplace design at home; home-based workstation; home office; home-based working environment; flexible workplaces; working conditions at home; home-based teleworking; virtual office; new ways of working; flexible work schedule; alternative work; lighting; teleworking policies, ergonomic program, organizational support, ergonomic program |
| Databases | Embase |
| (via Elsevier) including Medline | |
| Scopus | |
| PubPsych | |
| PsychInfo | |
| Web of Science | |
| Google Scholar | |
| Open Grey |
2.3Screening
Two independent researchers (MSW, LS) screened the studies’ titles and abstracts. Full text was requested if the study met the inclusion criteria or if an abstract did not provide enough information. To assess the agreement between reviewers for study selection, we used the k statistic (Cohen‘s kappa). A Kappa value > 0.6 is a substantial agreement and a Kappa value > 0.8 is an almost perfect agreement [38]. The Cohen‘s kappa was k = 0.83. If there was a disagreement about a study’s inclusion, the researchers discussed the inconsistency. If the researchers still could not agree, other team members (AE, DP, HS) were consulted.
The researchers used the software EndNote X9 and CADIMA, a free web-based systematic review tool designed to facilitate the creation of the protocol and process of parallel screening, data extraction and synthesis (https://www.cadima.info/index.php).
2.4Data extraction
For the included studies the authors extracted the following information: (1) publication details (i.e. first author and publication year); (2) study location; (3) study design; (4) population characteristics; (5) occupation; (6) aim of the study; (7) study outcomes and (8) quality assessment score. The extracted information of the included studies can be found in Table 2.
Table 2
Study characteristics of the included studies (n = 12)
| Author a, year | Study location | Study design | Population characteristic | Occupation | Aim of the study | Study outcomes | MMAT Scoreb |
| Aborg [4] | Sweden | Qualitative study | n = 28 M = NR F = NR | Private sector | Effects on part-time teleworker on office workers’ physical, well-being, psychosocial work environment, at home and the ordinary workplace. | Work conditions Technology use and technical equipment Physical exercise | High quality |
| Harrington [20] | USA | Quantitative randomized controlled trials | n = 50 M = 56% F = 44% | Private sector Public sector | Short- term effects of an ergonomics training program on the knowledge, attitudes, and practices. | Working conditions Musculoskeletal complaints Pre-experience with ergonomics training Intervention ergonomics program | Moderate quality |
| Jaakson [2] | Estonia | Qualitative study | n = NR M = NR F = NR | Industrial sectors Public sectors | Teleworkers technical equipment, cost-sharing practices and the responsibility for health and safety. | Policy for teleworking Cost responsibility for teleworking Reasons for non-compensation of costs by employees | Moderate quality |
| Janneck [42] | Germany | Mixed method design | n = 41 M = 28 F = 13 | Different industrial sectors | Evaluation of the ergonomics requirements of mobile workers and working from home. | Ergonomics awareness Personal ergonomics strategies Working condition Musculoskeletal complaints | Moderate quality |
| Montreuil [28] | Canada | Qualitative study | n = 103 M = NR F = NR | Public sector Private sector | Issues and health risks associated with telework. Examine the legal framework governing occupational health and safety of teleworkers. | Working conditions Technology use and technical equipment Musculoskeletal complaints | Moderate quality |
| Olsen [40] | Australia | Qualitative study | n = 38 M = 38% F = 62% | Private sector | Office-based employees’ perceptions of the impact of flexible work (after six months) on physical activity, sedentary behavior and preferences for associated interventions. | Health behavior Intervention preferences | High quality |
| Robelski [43] | Germany | Quantitative study | n = 112 M = 61.6% F = 38.9% | Private sectors Industrial sector | Psychosocial demands experienced by working in a coworking space in contrast to working at home. | Health behavior Working conditions Working performance | Moderate quality |
| Spinks [44] | Japan | Quantitative study | n = 672 M = 91 F = 581 | Different industrial sectors | Examination of the nature of home-based telework, work environment, work experience, health issues and policies to support this kind of work. | Musculoskeletal complaints Treatment of musculoskeletal complaints Ergonomic intervention Health behavior | Moderate quality |
| Steward [45] | England | Mixed-method design | n = 44 M = NR F = NR | Privat sector Public sector | Work and health experiences of telework. | Working conditions Health behavior | Moderate quality |
| Steward [46] | England | Mixed-method design | n = 56 M = 26 F = 18 | Private sector Public sector | Health experiences of teleworkers and exploration of their understanding and management of health and illness. | Working conditions Health behavior | Moderate quality |
| Ferreira [41] | South Africa | Quantitative study | n = 163 M = NR F = NR | Industry sector Public sector | Identification of the work-related musculoskeletal disorders, ergonomics, regulations for teleworkers | Organizational perception of telework Policy for teleworking Cost responsibility for teleworking Reasons for non-compensation of costs | Moderate quality |
| Wegner [21] | Germany | Quantitative study | n = 25 M = 09 F = 16 | NR | Working conditions at home and the comparison of strain with work in the office workplace. | Working conditions Musculoskeletal complaints Mental state Biological parameters | Moderate quality |
Note: F, female subjects; M, male subjects; MMAT, mixed methods appraisal tool; NR, not reported. aOnly the first author is named by each study, full author details can be found in the references. bKey: MMAT Score in total: 1–2 (low quality), 3–5 (moderate quality) and 6–7 (high quality).
2.5Quality assessment
The quality assessment was evaluated using the mixed methods appraisal tool (MMAT) from Hong, Pluye [39]. The MMAT is designed to evaluate reviews that include qualitative, quantitative and mixed methods studies. The MMAT consists of five categories: (1) qualitative research, (2) randomized controlled trials, (3) non-randomized studies, (4) quantitative descriptive studies, and (5) mixed methods studies. Each category has seven criteria, which include selection samples, cofounding factors and data analysis. Each criterion requires a yes, no or unclear designation, with a yes being assigned one point and a no or unclear being assigned 0 points. Based on their total score, the studies were assigned one of the following quality categories: 1-2 (low quality), 3–5 (moderate quality) and 6–7 (high quality). Two reviewers (MSW, LS) independently evaluated the quality assessment. Any disagreement that occurred was resolved through a discussion within the research team. In present review non study hat to be excluded because of a low MMAT score. The extracted details of the quality assessment can be found in Table 3.
Table 3
Quality assessment: Mixed Methods Appraisal Tool (MMAT), version 2018 [39]
| 1. Category: Qualitative study | Quality assessment | ||||||||
| Authora, year | Are there clear research questions? | Do the collected data allow to address the research questions? | Is the qualitative approach appropriate to answer the research question? | Are the qualitative data collection methods adequate to address the research question? | Are the findings adequately derived from the data? | Is the interpretation of results sufficiently substantiated by data? | Is there coherence between qualitative data sources, collection, analysis and interpretation? | Total MMAT score | Percent agreement of authors |
| Aborg [4] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 6 | 100% |
| (p. 6) | (p. 8) | (p. 15) | (p. 8) | (p. 8) | the sample size was gradually reduced | (p. 19) | |||
| Jaakson [2] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 4 | 86% |
| (p. 198) | (p. 200, 201) | (p. 203) | (p. 202, 203) | not reported | unclear | not reported | |||
| Olsen [40] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 | 100% |
| (p. 345) | (p. 346-347) | (p. 345) | (p. 345) | (p. 345, 346) | (p. 346f.) | (p. 345) | |||
| Montreuil [28] | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 5 | 100% |
| (p. 341) | (p. 341) | (p. 341) | (p. 341) | unclear | (p. 343f.) | unclear | |||
| (p. 343) | |||||||||
| 2. Category: Quantitative randomized controlled trials | Quality assessment | ||||||||
| Authora, year | Are there clear research questions? | Do the collected data allow to address the research questions? | Is randomization appropriately performed? | Are the groups comparable at baseline? | Are there complete outcome data? | Are outcome assessors blinded to the intervention provided? | Did the participants adhere to the assigned intervention? | Total MMAT Score | Percent agreement of authors |
| Harrington [20] | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 4 | 86% |
| (p. 15) | (p. 15) | unclear | (p. 18) | (p. 17, 18) | not reported | not reported | |||
| (p. 17) | (p. 16) | ||||||||
| 3. Category: Quantitative non-randomized | Quality assessment | ||||||||
| Authora, year | Are there clear research questions? | Do the collected data allow to address the research questions? | Are the participants representative of the target population? | Are measurements appropriate regarding both the outcome/ intervention (or exposure)? | Are there complete outcome data? | Are the confounders accounted for in the design and analysis? | During the study period, is the intervention administered (or exposure occurred) as intended? | Total MMAT Score | Percent agreement of authors |
| Robelski [43] | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 4 | 86% |
| (p. 2) | (p. 6f.) | (p. 6) | (p. 7) | (p. 8) | (p. 10) | unclear | |||
| (p. 6) | information on disturbance variables, current time in HO is not collected | ||||||||
| Wegner [21] | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 5 | 86% |
| (p. 15) | (p. 15, 16) | (p. 15) | (p. 16) measurements checked for plausibility, no reliability information | not reported | (S. 15) | (S. 15) | |||
| 4. Category: Quantitative descriptive | Quality assessment | ||||||||
| Authora, year | Are there clear research questions? | Do the collected data allow to address the research questions? | Is the sampling strategy relevant to address the research question? | Is the sample representative of the target population? | Are the measurements appropriate? | Is the risk of nonresponse bias low? | Is the statistical analysis appropriate to answer the research question? | Total MMAT Score | Percent agreement of authors |
| Spinks [44] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 4 | 86% |
| (p. 249) | (p. 249) Survey: | (p. 249) | (p. 249) | not reported | not reported | not reported | |||
| Ferreira [41] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 3 | 100% |
| (p. 120) | (p. 124) | (p. 125) | unclear | not reported | not reported | not reported | |||
| (p. 125) | |||||||||
| no description of the sample | |||||||||
| 5. Category: Mixed methods | Quality assessment | ||||||||
| Authora, year | Are there clear research questions? | Do the collected data allow to address the research questions? | Is there an adequate rationale for using a mixed methods design to address the research question? | Are the different components of the study effectively integrated to answer the research question? | Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | Total MMAT Score | Percent agreement of authors |
| Janneck [42] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 5 | 86% |
| (p. 1052) | (p. 1055ff.) | (p. 1055) | unclear | not reported | (p. 1055) | ||||
| (p. 1055) | (p. 1056) | ||||||||
| Steward [45] | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 5 | 86% |
| unclear (p. 104) not clear enough | (p. 105) | (p. 105) | (p. 105) | (p. 105f.) | not reported | (p. 105) | |||
| Steward (2001) [46] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 5 | 100% |
| (p. 143) | (p. 143) | (p. 142, 143) | (p. 143) | (p. 144f.) | not reported | not reported | |||
Key: yes = 1, no/unclear = 0, NR = not reported, total = MMAT score in total: 1-2 (low quality), 3–5 (moderate quality) and 6–7 (high quality). aOnly the first author’s name for each study is shown here; full author details can be found in the references.
2.6Study characteristics
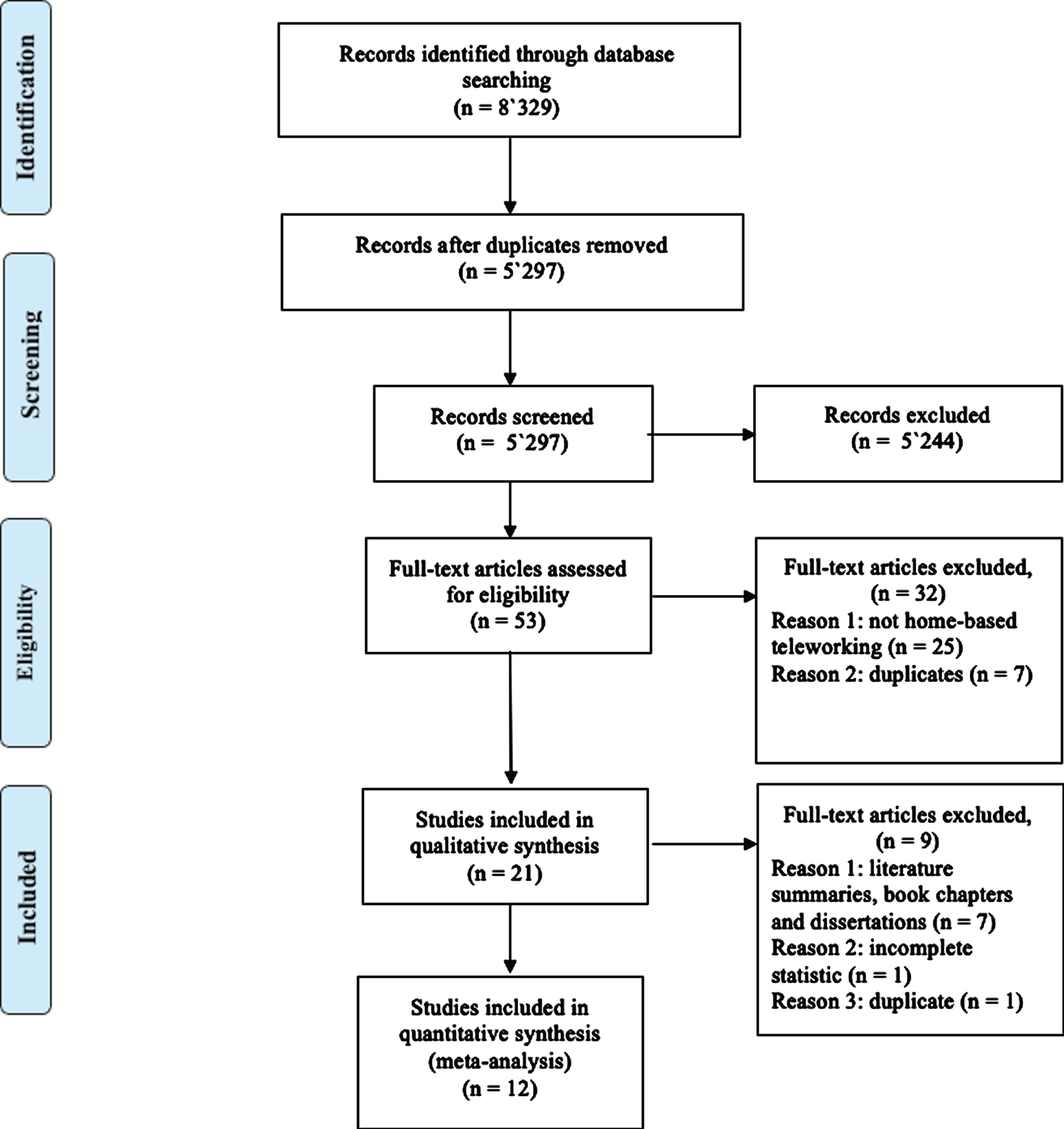
The search identified 8,329 references (including duplicates) and 5,297 references after removing duplicates. A total of 5,244 references were excluded based on the studies’ titles and abstracts, which resulted in a subtotal of 53 articles to be assessed for eligibility. After a full-text analysis, 32 studies were excluded. This amounted to a total of 21 articles that fulfilled the inclusion criteria. Of the remaining 21 articles, seven articles were excluded based on their literature summaries, book chapters and dissertations. These seven studies were proofed for further studies that could have been included in the present systematic review. No further studies were found.
Furthermore, one article was excluded because it was not clear whether the sample included home-based teleworkers, and its statistical data were missing. Another article was a duplicate. These exclusions led to the total of 12 studies to be examined in the present systematic review. Figure 1 shows a flow diagram of the study selection.
Fig. 1
Flow diagram of the study selection.
2.7Types of included studies
The systematic review method was chosen because this growing topic of home-based teleworking and its potential ergonomics issues does not currently have a large amount of evidence. This systematic review, therefore, contains a synthesis of qualitative studies (n = 4), quantitative randomized controlled trials (n = 1), quantitative non-randomized (n = 2), quantitative descriptive (n = 2), mixed methods (n = 3).
2.8Study quality
As shown in Tables 2 and 3, there were two studies of high quality [4, 40]. Ten studies had a moderate quality [2, 20, 21, 28, 41–46]. The percentage of agreement was between 86% and 100%.
3Results
3.1Working conditions for home-based telework
Seven studies collected data on ergonomics-related outcomes regarding workplace design and furniture [4, 20, 21, 28, 42, 43, 45]. Four studies have shown that most home-based teleworkers do computer-based work [4, 20, 44, 46]. Six studies evaluated the current space condition which home-based teleworker experienced [20, 21, 28, 42, 43, 46] and three studies examined the changed working conditions after a longer period in the home office [4, 42, 44].
3.1.1Workplace design in the home office
Most home-based teleworkers did not have well-designed home workstations. Home-based teleworkers complained about uncomfortable furniture, lack of storage for devices and office supplies, and poor lighting conditions [4, 21, 42]. Regarding furniture, Wegner et al. [21] reported the following complaints: no foot contact with the ground or missing footrests on chairs; weak screen positioning and small desktop areas; unsuitable arrangements of telecommunications equipment and insufficient backrest support for the spine.
3.1.2Technological use in the home office
In the study by Aborg et al. [4], most home-based teleworkers reported that they worked for longer periods at home without taking a break from the computer. Participants also reported that they work on the weekends and in the evenings. Aborg et al. [4] showed that, after working from home for two years, workers’ time spent on a computer and the length of continuous computer usage did not change. In addition, both the periods of time spent on a computer without breaks and the time spent on breaks were shorter at home than at the office. The time spent on the telephone per day was also twice as long at home (mean 38 minutes) than at the office (mean 19 minutes) [4]. These results are supported by further studies in present review [20, 44, 46].
3.1.3Space conditions in the home office
Montreuil and Lippel [28] studied whether teleworkers had rooms dedicated for work in their homes. The results were mixed. Some teleworkers had one room dedicated for work [20, 28] and others studies reported from well-equipped home offices, but observation revealed that over 70% of teleworkers used dual-purpose living rooms or bedrooms to perform their work [46]. Home-based teleworkers may use dual-purpose spaces because they consider what room in their home is available before they consider its ergonomic aspects. Steward [46] emphasized that most teleworkers choose the smallest or least-contested space available in their house, rather than inconvenience family members. Wegner et al. [21] showed that 23 out of 25 participants had a separate room for work, and 15 of those 23 shared that room with other family members. Steward [46] underlined the importance of having a separate working room: home-based teleworker perceived it as difficult to defend their work boundaries against family members who often do not respect home office spaces. Steward [46] reported that the mentioned situation could lead to work wherever they have space in their house, such as at the kitchen table or on a sofa in the living room. Home-based teleworkers can also be confronted with various other disruption factors, such as background noise [42] which could then lead them to prefer working in coworking spaces [43].
3.1.4Improving working conditions in the home office after implementation
Aborg et al. [4] found that, after two years of working from home, only half of their participants had improved their working conditions. The study also reported that, despite the experience gained from the longitudinal study, participating teleworkers’ ergonomic conditions at home still varied considerably from very good to very poor quality [4].
Teleworkers tried to address the ergonomic aspects of their work environments and acknowledge the potential for improvement [42]. Some workers develop their own ergonomic strategies, such as moving as much as possible; using special chairs, sitting balls and seat cushions; working in a standing position and using height-adjustable tables [42]. Spinks [44] found that teleworkers also take regular breaks, improve their lighting, ergonomics workstation design and safety (e.g., stumbling blocks).
3.2Experienced health-related outcomes in the home office
Six studies discussed physical exercise, activity or general health behaviors related to home-based telework [4, 21, 40, 43–45]. Work-related complaints, disorders and workdays lost were reported in eight studies [20, 21, 28, 41, 42, 44–46].
3.2.1Positive health-related outcomes
Steward [45] found that teleworkers perceived themselves to be more fit to work at home than when they worked in a conventional office. Even those with chronic illnesses reported feeling healthier [45]. Wegner et al. [21] found that teleworkers scored mood, vigilance and distinct inner calm higher than when they worked in an office. Workers’ blood pressures also often had higher values at company offices than in home offices [21]. Robelski et al. [43] evaluated that home-based teleworker had better eating behaviors, achieved more physical activity and took more breaks at home than in coworking spaces.
3.2.2Negative health-related outcomes
Olsen et al. [40] found that physical activity was neither positively nor negatively impacted by working at home; however, they also found that workers’ sedentary behavior increased while working at home. Additionally, home-based teleworkers complained of pain in their upper limbs, back and neck, which they attributed to inadequate furnishings [28]. Teleworkers who only had access to a laptop while working at home reported problems regarding eye strain and wrist pain [42]. The most common reported work-related disorders in the home office were migraines, eye strain, shoulder tendinitis, sore back, neck pains, and wrist pain [20]. Home-based teleworkers stated that they experienced discomfort while teleworking, and if they worked for a long time in their home office, a higher incidence of work-related discomfort was reported [20, 41]. Home-based teleworkers anticipated that they would experience computer-related health problems in the next five years [46], and the study by Wegner et al. [21] reported that 43% of teleworkers complained of musculoskeletal issues. For 12% of those who reported musculoskeletal issues, medical examinations revealed that the complications, such as cervical spine symptoms with hard muscular tension, were work related [21].
Spinks [44] evaluated work-related disorders which impacted job performance. The most common complaints were stiff shoulders, eye strain and lower back pain; these disorders also led to ongoing treatment. Montreuil and Lippel [28] reported that three employees had developed musculoskeletal injuries that resulted in a total of 80 days of work absence in the preceding year.
Ferreira and Strydom [41] found that workers suffering from shoulder tendinitis lost 45.2 workdays, and workers who suffered from tension neck syndrome lost 4.6 workdays.
It is also worth noting how teleworkers perceive illness when working at home. Steward [45] evaluated whether home-based teleworkers ignored symptoms of illness, and over half of the respondents reported that they had continued to work when they felt sick. Participants said that feeling unwell was not a reason to stop home-based work. In other words, some teleworkers believe that symptoms which would have prevented an employee from going in to work at an office should not prevent work from being done at home [45]. In contrast, participants also said that the health risks and adverse experiences of telework were trivial compared to the stress they experienced in their offices [37]. Various studies have also shown that teleworkers do not prioritize their health because home-based teleworking has many other advantages, such as higher personal efficiency, no travel time, better work-life balance (including opportunities to provide childcare) and elimination of emotional stress [4, 20, 21, 46].
Furthermore, Aborg et al. [4] noted a tendency of longer working hours while working from home. Steward [46] showed that some home-based teleworkers deducted breaks, short periods of socialization, and thinking and waiting periods when calculating their work hours. In addition, teleworkers tended to not report overtime, which would generally be compensated for [46].
3.3Organizational responsibilities and support
Ergonomic interventions, teleworking training and employee policies were reported in eight studies [4, 20, 28, 40–42, 44, 46]. Two studies discussed the responsibility for covering the cost of telework and the reasons why employees prefer not to compensate this cost [2, 41].
3.3.1Training for home-based teleworking
Most teleworkers receive no training [20, 41]. Montreuil and Lippel [28] showed that less than 50% of teleworkers received training for specific teleworking tasks, and only a few workers received teleworking training that related to potential personal and professional lifestyle changes. Over 50% of teleworkers did not receive training, which was seen as a disadvantage by most teleworkers, while those who were offered support appreciated it [4, 28].
3.3.2Ergonomic programs in the home office
Janneck et al. [42] studied ergonomic intervention programs. They showed that, in all cases, workers preferred video and audio information over text-based information. Video and audio information helped workers understand ergonomic exercises more easily [42]. In addition, Harrington and Walker [20] showed that ergonomic intervention programs had a significant positive impact on workers’ knowledge, attitudes and practices. Teleworkers who improved the ergonomics of their home offices based on training reduced or eliminated back, eye, finger and shoulder pain [20].
Regarding ergonomics programs and interventions, most home-based teleworkers did not want their employers to intrude on their homes, such as via health and safety inspections, and employers did not wish to intrude either [41, 46]. In the study by Olsen et al. [40], even managers felt that home-based telework had negatively impacted teleworkers’ sedentary behavior. However, managers agreed that employees should choose how they combat sedentary behavior and that they would support the employees’ decisions [40]. However, Spinks [44] has shown that certain occupational groups (such as desktop publishers and graphic designers) who do not take ergonomic interventions into account, have increased instances of work-related injuries. In addition, few teleworkers report doctor’s visits once they begin working at home [44].
3.3.3Policies for home-based telework
Evidence suggests that organizations lack awareness of their home-based teleworkers [2, 41]. For example, teleworking policies were regulated to the teleworkers themselves in some larger companies [2]. Some smaller companies also felt that they did not need and were reluctant to deal with regulations [2]. It was also found that employers did not feel responsible for creating their teleworkers’ home working environments, and organization usually did not offer any compensation for home office preparations [2]. In the study by Ferreira and Strydom [41], managers rated the priority which organizational policies, procedures and government acts applied to their organizations; they rated ergonomics policies as the lowest. Furthermore, managers indicated what they thought should be included in their company’s training programs; ergonomics policies and guidelines were the third last to be included [41].
3.3.4Technical equipment and organizational support for providing
Aborg et al. [4] and Montreuil and Lippel [28] evaluated the general technical situations at workers’ homes and whether organizations provided technical equipment for their workers. Harrington and Walker [20] as well as Jaakson and Kallaste [2] reported that most teleworkers purchased their own home office equipment. In addition, higher-status workers and those who work the longest hours did not have better working environments [37]. Montreuil and Lippel [28] reported in their study that employers supplied computer equipment for 60 of the 63 participating teleworkers. However, in some cases, the equipment that the employers supplied only consisted of a laptop computer without a conventional screen. Aborg et al. [4] evaluated that after beginning home-based telework, employees found technical support to be unacceptable; however, after two years, technical support was generally improved with help from the employees’ organizations.
Jaakson and Kallaste [2] evaluated the internet connections, furniture and home office facilities. Most companies did not offer compensation, and the teleworkers did not ask for it. Only two out of eight companies paid for internet connection or electricity used at employees’ homes. Jaakson and Kallaste [2] and Ferreira and Strydom [41] as well as Spinks [44] asked home-based teleworkers why they do not compensate the cost of home offices; the reasons were that it was difficult to assess which portions of electricity were used for work and that some teleworkers have more than one employer [41]. When asked why no compensation was provided for health issues, home-based teleworkers stated the following reasons: lack of knowledge, unwillingness to provide compensation, belief that treatment would not be successful, belief that the disorders were minor and belief that the problem was already covered by the employee’s medical aid funds [44]. The main opinion of management was that ergonomic programs and equipment existed at their company’s office and that employees were free to access them at the office [2].
4Conclusion and practical implications
This review highlights home-based teleworkers’ lack of ergonomic working conditions. Although employees try to implement ergonomic approaches while working at home, they do not receive enough support from the organizations they work for. A further complicating factor is that, if home-based teleworkers ask for help with ergonomic guidance, their companies often do not offer support because the companies do not have a support system in place or because they do not consider such support to be critically important. Management seems to lack knowledge and awareness about ergonomics and the consequences of its non-application to workers’ health. The situation is further complicated by the fact that, in many companies and countries, the regulations for working at home are different or only roughly outlined. To date, in some countries, it is still not clear which requirements that are present in an employment contract apply to home-based teleworkers [2, 47].
Nevertheless, the confusion surrounding this issue is also partly due to teleworkers who do not report their health complications or their medical expenses. The main reasons for this are complex. On the one hand, teleworkers lack knowledge about their rights to claim medical costs. On the other hand, a teleworker’s main motivation for working at home may not be to prevent health risks. It can also be assumed that employees must be made aware of ergonomics. The development of work-related MSDs is related to the duration and intensity of exposure to risk factors. It must also be mentioned that when teleworkers work from home one or two days per week, the long-term health consequences are more difficult to see, which could lead to postponing urgent care [30, 31].
Several studies reported that teleworkers spend long hours in front of computers [4, 28]. Aborg et al. [4] showed that, even after two years of teleworking, workers’ hours spent on the computer did not decrease. Olsen et al. [40] also showed that employees who work at home stay sedentary for longer periods of time than office workers. Working long hours on a computer combined with sedentary behavior and low ergonomic conditions lead to health complications. These findings lead to the assumption that health risks are increased for home-based teleworkers [28, 48]. This is substantiated by the fact that most of the included studies reported that their participants had musculoskeletal issues. These results underline the necessity of implementing ergonomic design recommendations, especially for those working at home.
Therefore, the practical recommendations can be summarized as follows: (1) the lack of awareness regarding home-based policies, ergonomics programs and the health-related consequences associated with the absence of ergonomic support must be addressed by educational work in an organization with employees and leaders combined with a willingness to change [4, 40]. (2) A convincing argument for many companies could be that employees who must take sick days due to the lack of ergonomic conditions represent a significant financial factor [2, 44]. (3) Another beneficial aspect could also be that such an organization’s approach can be promoted under sustainability, making them more attractive to future employees [47]. Furthermore, (4) Employees must be provided with specific education, online training sessions or advice on establishing a home office [4]. Harrington and Walker [20] underlines the importance of ergonomic intervention programs. Teleworkers who improved the ergonomics of their home offices, based on training, reduced or eliminated back, eye, finger and shoulder pain [20]. Therefore, improving employee ergonomic awareness and providing programs can be a worthwhile benefit for organization. (5) In principle, employees’ financial compensation should also be considered because organizations can save rental space by increasing home office [2, 4]. (6) For example, an organization’s furniture could be made available to employees for use at home. All these practical implications are related to the awareness or the knowledge of sustainable health in the home office. Therefore, it is essential to educate first. Until now, home office has led a shadowy existence, running alongside the regular working world. Now it is time to recognize the home office as an extended, accepted workplace and deal with the associated responsibilities under sustainable health.
4.1Limitations
First, this review’s quality assessment was used to increase transparency and to distinguish between studies of moderate and high quality. As shown in Tables 2 and 3, there were two studies of high quality [4, 28]. Ten studies had a moderate quality [2, 20, 21, 28, 41–46]. Second, the included studies presented in this review should be interpreted with caution because of the small sample size and the methodological diversity of the studies. Third, the present review focuses only on home-based teleworking and excluded other types of remote work. Fourth, to assure adequate scientific quality, only articles published in peer-reviewed journals were included, not theses, dissertations, or unpublished material. Fifth, for comparing the studies, this review included only employees with an age-appropriate health and excluded therefore, workers with disabilities.
Nevertheless, this review provides an overview of the available studies that pertain to current home-based teleworkers and the associated ergonomic conditions they have at home, the extent of work-related disorders and organizations’ awareness of this issue.
Well-designed studies are needed to further research in this topic. In general, more research must be conducted that focuses on the use of ergonomics, ergonomic interventions, and work-related disorders regarding home-based teleworking. There is also a need to understand the impact of virtual ergonomics interventions programs and how to integrate interventions successfully in the daily life of home-based teleworkers. Future research could also evaluate the potential of teleworking for employees with disabilities. People with disabilities’ current situation and their associated ergonomic conditions should also be examined.
Conflict of interest
The authors reported no potential conflict of interest.
References
[1] | Allen TD , Golden TD , Shockley KM . How effective is telecommuting? Assessing the status of our scientific findings. Psychol Sci Public Interest. (2015) ;16: (2):40–68. |
[2] | Jaakson K , Kallaste E . Beyond flexibility: Reallocation of responsibilities in the case of telework. New Technol Work Employ. (2010) ;25: (3):196–209. |
[3] | Felstead A , Jewson N . In work, at home: Towards an understanding of homeworking. London: Routledge; (2002) . |
[4] | Aborg C , Fernström E , Ericson MATS . Telework–work environment and well being. A longitudinal study. Uppsala University. Department of Information Technology. (2002) :2002–031. |
[5] | Messenger JC , Gschwind L . Three generations of Telework: New ICT s and the (R) evolution from Home Office to Virtual Office. New Technol Work Employ. (2016) ;31: (3):195–208. |
[6] | Bailey DE , Kurland NB . A review of telework research: Findings, new directions, and lessons for the study of modern work. J Organ Behav. (2002) ;23: (4):383–400. |
[7] | Charalampous M , Grant CA , Tramontano C , Michailidis E . Systematically reviewing remote e-workers’ well-being at work: A multidimensional approach. Eur J Work Organ Psychol. (2019) ;28: (1):51–73. |
[8] | Allen TD , Merlo K , Lawrence RC , Slutsky J , Gray CE . Boundary management and work-nonwork balance while working from home. Appl Psychol. (2021) ;70: (1):60–84. |
[9] | Rudolph CW , Allan B , Clark M , Hertel G , Hirschi A , Kunze F , et al. Pandemics: Implications for research and practice in industrial and organizational psychology. Industrial and Organizational Psychology: Perspectives on Science and Practice. (2020) . |
[10] | Sinclair RR , Allen T , Barber L , Bergman M , Britt T , Butler A , et al. Occupational health science in the time of COVID- Now more than ever. Occup Health Sci. (2020) ;19: :1–22. |
[11] | Blount Y . Pondering the fault lines of anywhere working (telework, telecommuting): A literature review. Foundations and Trends® in Information Systems. (2015) ;1: (3):163–276. |
[12] | Kröll C , Nüesch S . The effects of flexible work practices on employee attitudes: Evidence from a large-scale panel study in Germany. Int J Hum Resour Manag. (2019) ;30: (9):1505–25. |
[13] | De Menezes LM , Kelliher C . Flexible working and performance: A systematic review of the evidence for a business case. Int J Manag Rev. (2011) ;13: (4):452–74. |
[14] | Joyce K , Pabayo R , Critchley JA , Bambra C . Flexible working conditions and their effects on employee health and wellbeing. Cochrane Database Syst Rev. (2010) ;2: :CD008009. |
[15] | Jostell D , Hemlin S . After hours teleworking and boundary management: Effects on work-family conflict. Work. (2018) ;60: (3):475–83. |
[16] | de Macedo TAM , Cabral E , Silva Castro WR , de Souza Junior CC , da Costa Junior JF , Pedrosa FM , et al. Ergonomics and telework: A systematic review. Work. (2020) ;66: (4):777–88. |
[17] | Garnadt N , Schnitzer M , Viete S . Räumliche Flexibilisierung durch zunehmende Homeoffice-Nutzung. Wirtschaftsdienst. (2020) ;100: (9):661–6. |
[18] | Manger T , Wicklund RA , Eikeland O-J . Speed communication and solving social problems. Int J Commun. (2003) ;28: (3). |
[19] | Demerouti E , Derks D , Lieke L , Bakker AB . New ways of working: Impact on working conditions, work–family balance, and well-being. Dordrecht: Springer; (2014) . |
[20] | Harrington SS , Walker BL . The effects of ergonomics training on the knowledge, attitudes, and practices of teleworkers. J Safety Res. (2004) ;35: (1):13–22. |
[21] | Wegner R , Schröder M , Poschadel B , Baur X . Belastung und Beanspruchung durch alternierende Telearbeit. Zentralblatt für Arbeitsmedizin, Arbeitsschutz und Ergonomie. (2011) ;61: (1):14–20. |
[22] | Buomprisco G , Ricci S , Perri R , De Sio S . Health and Telework: New Challenges after COVID-19 Pandemic. Eur J Public Health. (2021) ;5: (2). |
[23] | Making Telework Work: The upsides, downsides and the way forward – Blog Expertisecentrum [https://www.rug.nl/hrm-ob/bloggen/]. Groningen: University of groningen; 2021 [updated 2021 May 12; cited 2021 May 20]. Available from: https://www.rug.nl/hrm-ob/bloggen/making-telework-work-the-upsides-downsides-and-the-way-forward-part-1. |
[24] | Hush JM , Michaleff Z , Maher CG , Refshauge K . Individual, physical and psychological risk factors for neck pain in Australian office workers: A 1-year longitudinal study. Eur Spine J. (2009) ;18: (10):1532–40. |
[25] | Choobineh A , Motamedzade M , Kazemi M , Moghimbeigi A , Pahlavian AH . The impact of ergonomics intervention on psychosocial factors and musculoskeletal symptoms among office workers. Int J Ind Ergon. (2011) ;41: (6):671–6. |
[26] | Aegerter AM , Deforth M , Johnston V , Sjogaard G , Volken T , Luomajoki H , et al. No evidence for an effect of working from home on neck pain and neck disability among Swiss office workers: Short-term impact of COVID-19. Eur Spine J. (2021) . |
[27] | Tavares AI . Telework and health effects review. Int J Health Serv. (2017) ;3: (2). |
[28] | Montreuil S , Lippel K . Telework and occupational health: A Quebec empirical study and regulatory implications. Saf Sci. (2003) ;41: (4):339–58. |
[29] | Crawford JO , MacCalman L , Jackson CA . The health and well-being of remote and mobile workers. Occup Med (Lond). (2011) ;61: (6):385–94. |
[30] | Occupational Injury and Illness Recording and Reporting Requirements United States: Occupational Safety and Health Administration (OSHA) [https://www.osha.gov]. United States: Occupational Safety and Health Administration Department of Labor; 2001 [updated 2001 January 19; cited 2021 May 20]. Available from: https://www.osha.gov/laws-regs/federalregister/2001-01-19. |
[31] | Burton J , Worl Health Organization WHO. WHO Healthy workplace framework and model: Background and supporting literature and practices: World Health Organization; (2010) . |
[32] | Koma BS , Bergh AM , Costa-Black KM . Barriers to and facilitators for implementing an office ergonomics programme in a South African research organisation. Appl Ergon. (2019) ;75: :83–90. |
[33] | Heidarimoghadam R , Mohammadfam I , Babamiri M , Soltanian AR , Khotanlou H , Sohrabi MS . What do the different ergonomic interventions accomplish in the workplace? A systematic review. Int J Occup Saf Ergon. (2020) )1–25. |
[34] | Moher D , Shamseer L , Clarke C , Ghersi D , Liberati A , Petticrew M , et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) statement. Systematic Reviews. (2015) ;4: (1):1–9. |
[35] | Aromataris E , Pearson A . The systematic review: An overview. Am J Nurs. (2014) ;114: (3):53–8. |
[36] | Cooke A , Smith D , Booth A . Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual Health Res. (2012) ;22: (10):1435–43. |
[37] | Methley AM , Campbell S , Chew-Graham C , McNally R , Cheraghi-Sohi S . PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res. (2014) ;14: (1):1–10. |
[38] | Cohen J . A power primer: Psychological bulletin; (1992) . |
[39] | Hong Q , Pluye P , Fàbregues S , Bartlett G , F B , Cargo M , et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Education for Information. (2018) ;34: (4):285–91. |
[40] | Olsen HM , Brown WJ , Kolbe-Alexander T , Burton NW . Physical activity and sedentary behaviour in a flexible office-based workplace: Employee perceptions and priorities for change. Health Promot J Austr. (2018) ;29: (3):344–52. |
[41] | Ferreira EJ , Strydom EA . Managing work-related musculoskeletal disorders in the virtual office. J Contemp Manag. (2016) ;13: (1):117–43. |
[42] | Janneck M , Jent S , Weber P , Nissen H . Ergonomics to go: Designing the mobile workspace. Int J Hum-Comput Interact. (2018) ;34: (11):1052–62. |
[43] | Robelski S , Keller H , Harth V , Mache S . Coworking spaces: The better home office? A psychosocial and health-related perspective on an emerging work environment. Int J Environ Res Public Health (2019) ;16: (13). |
[44] | Spinks WA . A survey of home-based workers in Japan: Emerging health issues. J Occup Health. (2002) ;44: (4):248–53. |
[45] | Steward B . Fit to telework-The changing meaning of fitness in new forms of employment. Advances in Physiotherapy. (2000) ;2: (3):103–11. |
[46] | Steward B . Health trade-offs in teleworking: An exploratory study of work and health in computer homebased working. Indexer. (2001) ;22: (3):142–6. |
[47] | Mergener A . Berufliche zugänge zum homeoffice. Kölner Zeitschrift für Soziologie und Sozialpsychologie. (2020) ;72: (S1):511–34. |
[48] | Barron J . Making the virtual leap: Ten issues to consider about telecommuting. Ind Commer Train. (2007) ;39: (7):396–9. |


