
The effect of the COVID-19 Pandemic on anxiety, depression, and musculoskeletal system complaints in healthcare workers
Abstract
BACKGROUND:
COVID-19 increased psychological and physical complaints, including anxiety, depression, and pain.
OBJECTIVE:
We aimed to examine anxiety, depression, and musculoskeletal complaints that may occur in healthcare workers during the COVID-19 pandemic.
METHODS:
Data were cross-sectional, collected by the online questionnaire method consisted of demographic questions, Generalized Anxiety Disorder (GAD-7), Patient Health Questionnaire (PHQ-9), Nordic Musculoskeletal System Query (NMQ), and Visual Analogue Scale (VAS).
RESULTS:
Among the groups, the number of doctors in the frontline group, the fear of being infected, the number of tests performed, and personal protective equipment were higher than the second-line group (p < 0.05). It was found that 73.4% of the participants had anxiety, 83.5% had depression, and 94.9% had musculoskeletal pain. It was observed that there was no statistically significant difference between the applied scale scores between the groups (p > 0.05). About musculoskeletal system complaints of the participants, neck pain presence was determined as 73.4% in the last 12 months, and upper back pain was the highest with 61.4% in the last week. Neck (p < 0.005) and upper back pain (p = 0.04) parameters in the last seven days of the NMQ scale applied to the participants were found to be statistically significantly higher in the contact group.
CONCLUSIONS:
Anxiety, depression, and musculoskeletal pain of healthcare workers were found to be high. While neck and back pain was the most common in musculoskeletal complaints, it was found that these pains were higher in the frontline group. In this regard, healthcare professionals can be given psychological support and exercise training.
1Introduction
COVID-19 (Coronavirus disease 2019) is a new infectious disease that spread rapidly worldwide, causes severe effects, and became a pandemic in a short time. COVID-19 is transmitted through droplets emitted by sick individuals through coughing and sneezing. While the most common clinical symptoms are fever (87.9%), and cough (67.7%), fatigue (38.1%), diarrhea (3.7%), and vomiting (5.0%) are seen as less common symptoms [1]. As of 13 August 2020, the latest WHO numbers have been reported as 20,439,814 diagnosed cases and 744,385 deaths [2].
Healthcare professionals are the most basic and most effective workforce who risk their lives and fight at the frontline against the COVID-19 pandemic. The risk of COVID-19 is higher in healthcare workers than in other work areas due to their close contact with patients [3]. Apart from long working hours, physical and psychological stress, burnout, and fatigue for healthcare professionals, this type of infectious disease is an additional danger. Therefore, fear, anxiety, and uncertainty caused by COVID-19 in healthcare workers may cause their bodies to react differently [4].
It is stated that being healthcare workers in pandemics creates a high level of biopsychosocial stress, even if it is not traumatic [5]. COVID-19 increased psychological complaints and disorders, including anxiety, depression, and stress [6]. Physical and psychosocial factors at work play an important role in musculoskeletal diseases of the low back, neck, and shoulders. Slow developing chronic disorders of tendons, muscles, joints, nerves, and intervertebral discs due to repetitive microtraumas occur when the person’s physical capacity and the workload in extraordinary situations do not coincide. Pain, discomfort, loss of muscle strength, and endurance may be observed [7].
In addition to anxiety and depression, which are the psychosocial factors of healthcare workers exposed to COVID-19, it was aimed to examine the effects of physical factors on the musculoskeletal system.
2Materials and methods
University of Health Sciences, Diyarbakır Gazi Yaşargil Education and Research Hospital staff constituted the universe of this descriptive and cross-sectional study. For this research, 158 people were reached, including 81 healthcare workers (frontline/contact) working in the COVID-19 clinic and 77 healthcare workers (second-line/non-contact) working outside the COVID-19 clinic. The research fieldwork was conducted with the online survey method after obtaining the ethics committee (Diyarbakır Gazi Yaşargil Education and Research Hospital Non-invasive Clinical Research Ethics Committee, Number:533, Date:24/07/2020) approval and the institution’s permission. Volunteering was taken into account in participating in this study. Participants who were unwilling to participate in this study were asked not to fill in the questionnaire forms and ignore the incoming message.
Volunteers between the ages of 18–80 and who do not have any mental illness (psychosis, dementia, delirium) were included in this study. Those who do not want to participate voluntarily, and those who do not comply with the mentioned conditions also established the exclusion criteria.
2.1Data collection tools
The questionnaire form consists of 5 parts: demographic questions and information questions about COVID-19, Generalized Anxiety Disorder (GAD-7), The Patient Health Questionnaire (PHQ-9), Nordic Musculoskeletal System Questionnaire (NMQ), and Visual Analogue Scale (VAS). The first part of the questionnaire includes demographic questions and information questions about COVID-19. Relevant scales were used in the second part of the questionnaire.
2.2Generalized anxiety disorder-7 (GAD-7) test
YAB-7 is a self-assessment scale with seven items. The scale was developed by Spitzer et al. [8] to evaluate generalized anxiety disorder according to DSM IV-TR criteria. Konkan et al. [9] conducted Turkish validity and reliability studies of the scale. Likert-type scale (0 = none, 1 = many days, 2 = more than half of the days, 3 = almost every day) is listed on a 4-level ordinal scale. The scores that can be obtained from the scale are between 0 and 21. The total scores obtained from the scale are 5, 10, and 15 as cut-off points for mild, moderate, and severe anxiety, respectively.
2.3The patient health questionnaire-9
The Patient Health Questionnaire-9 is a scale prepared for the screening of depression in individuals who are administered PHQ-9. It is a scale consisting of nine items questioning the diagnosis of depressive disorder. Spitzer et al. [10] and Sarı et al. [11] conducted validity and reliability studies in Turkish. Answers are scored with a minimum of 0 and a maximum of 3, namely “None,” “A few days,” “More than a week,” and “Almost every day.” Scoring 1–4 indicated no depression, 5–9 indicates mild depression, 10–14 indicates moderate depression, while 15–19 indicates partially severe depression, and 20–27 indicates severe depression.
2.4The nordic musculoskeletal questionnaire (NMQ)
NMQ anatomically shows nine regions on a figure: neck, shoulder, upper back, elbow, hand/wrist, lower back, hip/thigh, knee, foot/ankle. It is a form that questions whether there is pain, they have experienced pain complaints in the last week and one year, and the pain affects work/home life [12]. The form consists of three parts (“Have you had any complaints (pain, suffering, discomfort) in the following areas at any time during the last 12 months?”, “Have you been prevented from doing your usual work at any time during the last 12 months? and “Have you had pain at any time during the last seven days?”). Questions are answered as “Yes” and “No.” Kahraman et al. [13] conducted a Turkish validity and reliability study.
2.5Visual analog scale (VAS)
VAS is a measurement tool used for individuals to assess their pain. This tool is a scale with “0 (no pain)” at the beginning end and “10 (severe pain)” at the end. Accordingly, “0” indicates no pain, while the average VAS value of 1–4 indicates mild pain, 5-6 moderate pain, 7–10 severe pain [14].
2.6Statistical analysis
SPSS Statistics (IBM, Armonk, USA) version 22.0 was used in the analysis of the data. Descriptive values were expressed by number, percentage, mean±standard deviation. Normality analysis of the measurement data was performed using the Kolmogorov-Smirnov test. Independent-samples t-test was used to compare paired groups in data conforming to a normal distribution, and a chi-square test was used for categorical data. Pearson correlation analysis was performed for comparing quantitative data with each other, and p < 0.05 was accepted as statistical significance in all analyses.
3Results
Of the frontline group, 54.3% were women, 55.6% were unmarried, and 82.7% were university graduates. Of the second-line group, 53.2% were women, 57.1% were unmarried, and 84.4% were university graduates. In the occupational group, it was observed that the number of doctors in the frontline group was higher than the second-line group, the laboratory/physiotherapist professions in the second-line group were higher than the frontline group, and the statistical difference was due to these two occupational groups (p < 0.01). Among the groups, the fear of infection, the number of tests performed, and the use of personal protective equipment of the frontline group were statistically higher than the second-line group (p < 0.05). No statistically significant difference was found in other sociodemographic data between groups (Table 1). When asked how much they thought they knew about COVID-19, 61.2% stated that they were very knowledgeable (Fig. 1). It was found that 73.4% of the participants had anxiety, 83.5% had depression, and 94.9% had musculoskeletal Pain (Table 2). However, GAD-7, PHQ-9, and VAS scale scores applied to the participants were not found to be statistically significant between groups (p > 0.05).
Table 1
Sociodemographic characteristics of the participants
| Frontline n (81) % | Second-line n (77) % | Total n (158) % | p | |
| Gender | ||||
| Male | 37 (45.7) | 36 (46.8) | 73 (46.2) | 0.89 |
| Female | 44 (54.3) | 41 (53.2) | 85 (53.8) | |
| Marital status | ||||
| Married | 36 (44.4) | 33 (42.9) | 69 (43.7) | 0.30 |
| Single/Divorced/Widow | 45 (55.6) | 44 (57.1) | 89 (56.3) | |
| Education | ||||
| High school | 5 (6.2) | 4 (5.2) | 9 (5.7) | 0.95 |
| College | 9 (11.1) | 8 (10.4) | 17 (10.8) | |
| University | 67 (82.7) | 65 (84.4) | 132 (83.5) | |
| Occupation | ||||
| Physician | 23 (28.4) | 6 (7.8) | 29 (18.4) | < 0.01 |
| Nurse/Midwife | 46 (56.8) | 30 (39.0) | 76 (48.1) | |
| Physiotherapist/Dietitian/Biologist/Psychologist | 5 (6.2) | 35 (45.5) | 40 (25.3) | |
| Health technician | 7 (8.6) | 6 (7.8) | 13 (8.2) | |
| Use of painkillers | ||||
| Yes | 22 (27.2) | 20 (26.0) | 42 (26.6) | 0.80 |
| No | 59 (72.8) | 57 (77.0) | 116 (73.4) | |
| Do exercise | ||||
| Yes | 18 (22.2) | 18 (23.4) | 36 (22.8) | 0.80 |
| No | 63 (77.8) | 59 (76.6) | 122 (77.2) | |
| Psychiatric treatment | ||||
| Yes | 2 (2.5) | 3 (3.9) | 5 (3.2) | 0.60 |
| No | 79 (97.5) | 74 (96.1) | 153 (96.8) | |
| Fear of getting an infection | ||||
| Yes | 67 (82.7) | 48 (62.3) | 115 (72.8) | 0.004 |
| No | 14 (17.3) | 29 (37.7) | 43 (27.2) | |
| Testing for COVID-19 | ||||
| Yes (Negative) | 43 (53.1) | 15 (19.5) | 58 (36.7) | < 0.001 |
| Yes (Positive) | 6 (7.6) | 1 (1.3) | 7 (4.4) | |
| No | 32 (39.5) | 61 (79.2) | 93 (58.9) | |
| Use of personal protective equipment | ||||
| Yes | 74 (91.4) | 49 (63.6) | 123 (77.8) | < 0.001 |
| No | 7 (8.6) | 28 (36.4) | 35 (22.2) |
Fig. 1
Levels of participants’knowledge of COVID-19.
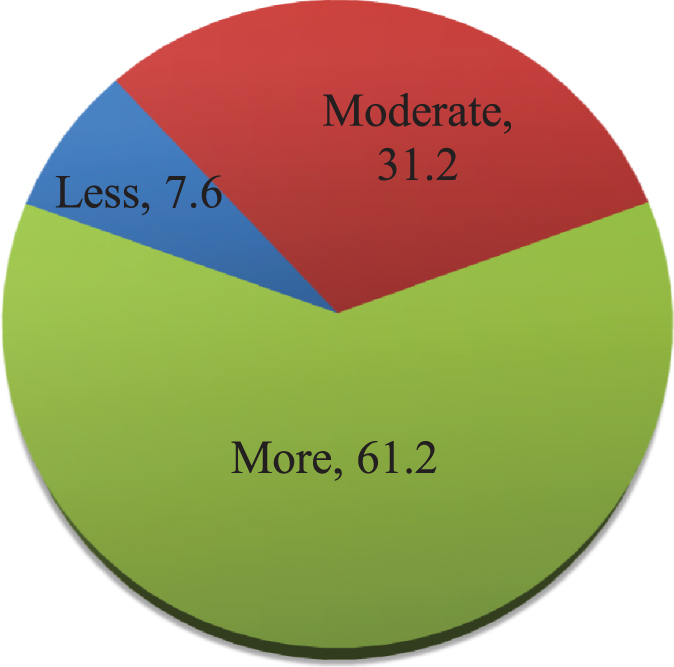
Table 2
Comparison of participants according to scale groups and scale scores
| Frontline n (81) % | Second-line n (77) % | Total n (158) % | p | |
| Anxiety group | ||||
| Normal/No | 24 (29.6) | 18 (23.4) | 42 (26.6) | 0.7* |
| Mild | 28 (34.6) | 32 (41.6) | 60 (38.0) | |
| Moderate | 15 (18.5) | 12 (15.6) | 27 (17.1) | |
| Severe | 14 (17.3) | 15 (19.5) | 29 (18.4) | |
| Depression group | ||||
| Normal/No | 14 (17.3) | 12 (15.6) | 26 (16.5) | 0.26* |
| Mild | 23 (28.4) | 31 (40.3) | 54 (34.2) | |
| Moderate | 25 (30,9) | 13 (16,9) | 38 (24,1) | |
| Moderately severe | 10 (12.3) | 10 (13.0) | 20 (12.7) | |
| Severe | 9 (11.1) | 11 (14.3) | 20 (12.7) | |
| VAS group | ||||
| No pain | 2 (2.5) | 6 (7.8) | 8 (5.1) | 0.24* |
| Mild | 25 (30.9) | 30 (39.0) | 55 (34.8) | |
| Moderate | 30 (37.0) | 22 (28.6) | 52 (32.9) | |
| Severe | 24 (29.6) | 19 (24.7) | 43 (27.2) | |
| Agea | 31.30±6.6 | 32.01±6.9 | 0.51** | |
| Anxietya | 8.04±5.6 | 8.59±5.9 | 0.55** | |
| Depressiona | 10.66±6.3 | 10.61±6.9 | 0.95** | |
| VASa | 5.32±2.1 | 4.64±2.5 | 0.73** |
*chi-square test, **independent-samples t-test, amean±standard deviation (min-max).
While neck pain came at the top of the musculoskeletal complaints of the participants in the last 12 months with 73.4%, it was observed that the neck and low back were the most critical areas affecting the everyday life activities of the people in this process with 42.4%. In the last week, upper back pain was the highest, with 61.4% (Table 3).
Table 3
Prevalence of musculoskeletal disorders
| Presence of pain, discomfort, numbness in the last 12 months | Pain preventing normal activities in the last 12 months | Musculoskeletal problems in the last 7 days | |
| n (%)* | n (%)* | n (%)* | |
| Neck | 116 (73.4) | 67 (42.4) | 89 (56.3) |
| Shoulder | 89 (56.3) | 38 (24.1) | 62 (39.2) |
| Elbow | 23 (14.6) | 15 (9.5) | 20 (12.7) |
| Wrist/Hand | 58 (36.7) | 32 (20.3) | 32 (20.3) |
| Upper back | 108 (68.4) | 59 (37.3) | 97 (61.4) |
| Lower back | 112 (70.9) | 67 (42.4) | 92 (58.2) |
| Hips/Thigh | 54 (34.2) | 29 (18.4) | 39 (24.7) |
| Knees | 75 (47.5) | 42 (26.6) | 58 (36.7) |
| Ankles/Feet | 54 (34.2) | 40 (25.3) | 46 (29.1) |
*Number and percentage of those answering the scale as “Yes”.
In the last seven days, sub-items of the NMQ scale were applied to the participants. It was determined that the neck and upper back pain parameters were statistically significantly higher in the frontline group (Table 4).
Table 4
Association between study area and musculoskeletal disorders
| Frontline n (81) % | Second-line n (77) % | Overall n (158) % | p value | |
| Neck | ||||
| Pain | 54 (66.7) | 35 (45.5) | 89 (56.3) | < 0.005 |
| No pain | 27 (33.3) | 42 (54.5) | 69 (43.7) | |
| Shoulder | ||||
| Pain | 33 (40.7) | 29 (37.7) | 62 (39.2) | 0.69 |
| No pain | 48 (59.3) | 48 (62.3) | 96 (60.8) | |
| Elbow | ||||
| Pain | 12 (14.8) | 8 (10.4) | 20 (12.7) | 0.40 |
| No pain | 69 (85.2) | 69 (89.6) | 138 (87.3) | |
| Wrist/Hand | ||||
| Pain | 21 (25.9) | 11 (14.3) | 32 (20.3) | 0.06 |
| No pain | 60 (74.1) | 66 (85.7) | 126 (79.7) | |
| Upper back pain | ||||
| Pain | 56 (69.1) | 41 (53.2) | 97 (61.4) | 0.04 |
| No pain | 25 (30.9) | 36 (46.8) | 61 (38.6) | |
| Lower back pain | ||||
| Pain | 45 (55.6) | 47 (61.0) | 92 (58.2) | 0.48 |
| No pain | 36 (44.4) | 30 (39.0) | 66 (41.8) | |
| Hips/Thigh | ||||
| Pain | 20 (24.7) | 19 (24.7) | 39 (24.7) | 0.99 |
| No pain | 61 (75.3) | 58 (75.3) | 119 (75.3) | |
| Knees | ||||
| Pain | 28 (34,6) | 30 (39.0) | 58 (36.7) | 0.56 |
| No pain | 53 (65,4) | 47 (61.0) | 100 (63.3) | |
| Ankles/Feet | ||||
| Pain | 24 (29,6) | 22 (28.6) | 46 (29.1) | 0.88 |
| No pain | 57 (70,4) | 55 (71.4) | 112 (70.9) |
†Pain in the last 7 days has been included from the table.
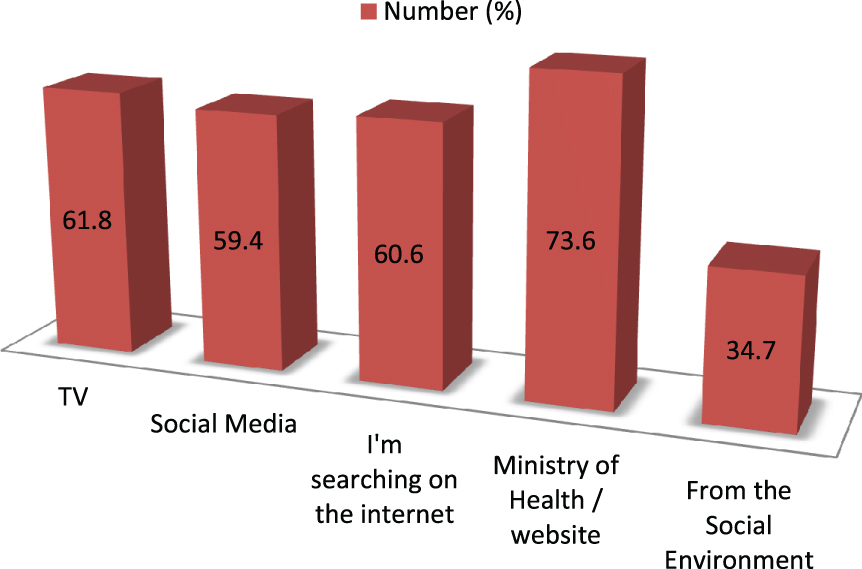
Participants received most information about COVID-19 from the Ministry of Health website as a source of information. Then they were getting information from television, the internet, social media, and their environment, respectively (Fig. 2).
Fig. 2
Source of knowledge about COVID-19.
A strong, positive, and significant relationship was found between the PHQ-9 scale and the GAD-7 scale. A positive, moderate, significant correlation was found between the VAS total score and the GAD-7 scale and PHQ scale (Table 5).
Table 5
Correlation of age and scale scores
| Age score | GAD-7 score | PHQ-9 score | VAS | ||
| Age | |||||
| GAD-7 | r | –0.084 | |||
| score | p | 0.296 | |||
| PHQ-9 | r | – 0.179 | 0.823 | ||
| score | p | 0.025 | 0.000 | ||
| VAS | r | –0.035 | 0.293 | 0.435 | |
| score | p | 0.664 | 0.000 | 0.000 |
4Discussion
While the COVID-19 outbreak has been one of the biggest public health problems seen on a global scale in recent years, it has also had a severe impact on healthy communities. Healthcare workers being at risk of infectious disease, fear, stress, and a heavy workload can reduce their concentration and negatively affect their work. Therefore, it is essential to evaluate healthcare workers’ preventive behaviors, psychological conditions, and musculoskeletal system effects against the virus.
Due to their close contact with patients, getting COVID-19 is higher in frontline healthcare workers than other healthcare workers. In this study, it was observed that among the groups, the frontline group had a statistically higher fear of being infected about themselves than the second-line group. Nemati et al. [15] identified the nurses’ concerns for themselves and family ailments with COVID-19 working in the front line. Under these circumstances, it may be natural for healthcare professionals to develop a fear of being infected by their patients.
In this study, no statistically significant difference was found between healthcare workers’ anxiety scale scores. However, 73.4% of all participants had anxiety (38.0% mild, 17.1% moderate, and 18.4% severe anxiety). In a similar study conducted on healthcare workers in the COVID-19 pandemic in Italy [16], no difference was found between healthcare professionals working in the front line and anxiety. In this study conducted during the pandemic period in China, Haung and Zhao [17] stated that healthcare workers have higher anxiety levels than other professions. Turkey has in society in 5–10% of any kind of anxiety disorder [18]. Possible reasons for all healthcare professionals to have higher anxiety than the general population may be the anxiety of becoming infected, the uncertainty of a new disease, and the difficulty in controlling the pandemic.
In this study, no statistically significant difference was found between the depression scale scores of healthcare workers. However, it was found that 83.5% of all participants had depression (34.2% mild, 24.1% moderate, and 25.4% severe depression). A similar study stated that 24.7% of healthcare workers had severe depression in the COVID-19 pandemic, but working in the front line did not differ [16]. Lai et al. [19] reported that a significant portion of healthcare workers experienced anxiety and depression symptoms, and consequently, more than 70% of them experienced psychological problems. According to the WHO 2017 report, the prevalence of depressive disorders in Turkey is 4.4% [20]. The frequency of depression found in this study is much higher than the general population. Sources of distress, feelings of loss of control, the spread of the virus, the health of the family, and others, changes in work can lead to health workers’ psychological effects in the infectious disease pandemic.
It was determined that 94.9% of all health workers had musculoskeletal pain (34.8% mild, 32.9% moderate, and 27.2% severe pain). The most common musculoskeletal complaints in the last 12 months were neck pain with 73.4% and lower back pain, with 70.9%. It was observed that the neck and low back, with 42.4%, were the most critical regions affecting people’s everyday life activities in this process. In the last seven days, upper back pain was the highest, with 61.4% and lower back pain with 58.2%. It was found that neck and upper back pain parameters in the last seven days sub-items were statistically significantly higher in the frontline group. Gül et al. [21] stated that 92.6% of the nurses stated that they had musculoskeletal pain in at least one body region. Abu Tariah et al. [22] reported that nurses felt discomfort in the lower back (63.8%) and upper back (48.9%) in the last twelve months and that this discomfort decreased work activities and leisure activities. Alwabli et al. [23] stated that doctors experienced most neck and lower back pain in the last seven days. In conclusion, in this study, following the literature, it was observed that healthcare workers had a high rate of experiencing work-related musculoskeletal pain, and especially the neck, low back, and upper back areas were affected. During pandemic periods such as COVID-19, musculoskeletal complaints may increase due to the increased workload of healthcare workers, irregular shifts, inadequate rest, and psychosocial stress.
Healthcare professionals need to access up-to-date information on COVID-19 from reliable sources. Huynh et al. reported in their study that healthcare workers gathered their information on COVID-19 through various media, such as the Internet/social media (91.1%), hospital/Ministry of Health (82.6%), and television (79.2%) [24]. A study conducted in Iran showed that nurses received their information from various media such as reliable websites, the internet, and TV [15]. In Saudi Arabia, awareness messages about COVID-19 were sent in 24 languages to residents on their personal mobile phones [25]. In this study, it was concluded that the Ministry of Health website, television, and the internet were the most used sources of information about the disease. In Turkey, The Ministry of Health’s provision of appropriate information to people about the coronavirus on television and the internet through scientists may have been effective in this regard.
A significant positive correlation was found between the PHQ scale and GAD-7 scale, VAS total score, and GAD-7 scale and PHQ scale in this study. In terms of psychological influence, anxiety can increase depression, and depression may increase anxiety [26]. Davison et al. [27] stated that they found a significant relationship between work-related musculoskeletal complaints and psychosocial risk factors in cases. There are factors such as work-related anxiety, psychosocial stress, and tension, and there may be a significant relationship between work stress and musculoskeletal complaints.
4.1Limitations
During the study period, the rate of answering the questionnaire may have been low in the busy pace of work due to the increased intervention of healthcare professionals to COVID-19 patients. No studies related to the musculoskeletal system for healthcare workers in the COVID-19 pandemic have been found in the literature. Therefore, musculoskeletal complaints have been discussed with studies conducted outside the pandemic period.
5Conclusions
More doctors and nurses in the front line were the occupational groups that could provide emergency intervention. While working in this field, it has been observed that it increases the fear of infection. It did not make a difference in terms of anxiety, depression, and musculoskeletal system effects. However, anxiety, depression, and musculoskeletal pain were found to be high in total healthcare workers. In musculoskeletal system complaints, neck and back pains are the most common, while those who work in the front line had more pain.
In line with these results, psychological support programs can be created for healthcare workers during an infectious disease epidemic. In this challenging process, healthcare workers can manage their psychological processes by doing activities such as appropriate exercise, reading, listening to music at home, and communicating well with their friends and families. Healthcare workers need to be aware of the risk of experiencing musculoskeletal pain and receive training to avoid or deal with their pain. Workloads of healthcare professionals should be reduced, and they should be provided to work in an ergonomically appropriate environment.
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
References
[1] | Guan WJ , Ni ZY , Hu Y , Liang WH , Ou CQ , He JX , et al. Clinical characteristics of 2019 novel coronavirus infection in China. NEJM 2020. doi: 10.1056/NEJMoa2002032. |
[2] | World Health Organization (WHO). Coronavirus Disease (COVID-19) Dashboard [Internet]. 2020. Available at: https://covid19.who.int/ |
[3] | Sim MR . The COVID-19 pandemic: major risks to healthcare and other workers on the front line. BMJ Occupational & Enviromental Medicine. 2020;281-2. doi: 10.1136/oemed-2020-106567. |
[4] | Langade D , Modi PD , Sidhwa YF , Hishikar NA , Gharpure AS , Wankhade K , et al. Burnout syndrome among medical practitioners across India: a questionnaire-based survey. Cureus. (2016) ;8: (9). doi: 10.7759/cureus.771. |
[5] | Suwantarat N , Apisarnthanarak A . Risks to healthcare workers with emerging diseases: lessons from MERS-CoV, Ebola, SARS, and avian flu. Curr Opin Infect Dis. (2015) ;28: (4):349–61. doi: 10.1097/QCO.0000000000000183. |
[6] | Duan L , Zhu G . Psychological interventions for people affected by the COVID-19 epidemic. The Lancet Psychiatry. (2020) ;7: (4):300–2. doi: 10.1016/S2215-0366(20)30073-0. |
[7] | Hengel KM , Visser B , Sluiter JK . The prevalence and incidence of musculoskeletal symptoms among hospital physicians: a systematic review. Int Arch Occup Environ. Health. (2011) ;84: :115–9. doi: 10.1007/s00420-010-0565-8. |
[8] | Spitzer RL , Kroenke K , Williams JB , Löwe B . A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) ;166: :1092–7. doi: 10.1001/archinte.166.10.1092. |
[9] | Konkan R , Şenormancı Ö , Güçlü O , Aydın E , Sungur MZ . Validity and reliability study for the Turkish adaptation of the Generalized Anxiety Disorder-7 (GAD-7) scale. Archives of Neuropsychiatry. (2013) ;50: :53–8. doi: 10.4274/npa.y6308. |
[10] | Spitzer RL , Kroenke K , Williams JB , Patient Health Questionnaire Primary Care Study Group. Validation and Utility of A Self-Report Version Of PRIME-MD: The PHQ Primary Care Study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. (1999) ;282: :1737–44. doi: 10.1001/jama.282.18.1737. |
[11] | Sarı YE , Kokoglu B , Balcioglu H , Bilge U , Colak E , Unluoglu I . Turkish reliability of the patient health questionnaire-9. Biomedical Research. 2016;460-2. |
[12] | Kurinka I , Jonsson B , Kilbom A , Vinter berg H , Biering-sorensen F , Anderon G , et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. (1987) ;18: :233–7. doi: 10.1016/0003-6870(87)90010-X. |
[13] | Kahraman T , Genç cA , Göz E . The Nordic Musculoskeletal Questionnaire: Cross-Cultural Adaptation Into Turkish Assessing Its Psychometric Properties. Disability and Rehabilitation (2016) ;38: (21):2153–60. doi: 10.3109/09638288.2015.1114034. |
[14] | Albersnagel FA . Velten and Music Mood Induction Procedures: A Comparision With Accessibility of Thought Associations. Behavioral Research and Theory. (1988) ;26: (1):79–96. doi: 10.1016/0005-7967(88)90035-6. |
[15] | Nemati M , Ebrahimi B , Nemati F . Assessment of İranian nurses’ knowledge and anxiety toward COVID-19 during the current outbreak in Iran. Archives of Clinical Infectious Diseases. (2020) ;15: . doi: 10.5812/archcid.102848. |
[16] | Rossi R , Socci V , Pacitti F , Di Lorenzo G , Di Marco A , Siracusano A , et al. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Network Open. (2010) ;3: (5):e185–e185. doi: 10.1001/jamanetworkopen.2020.10185. |
[17] | Huang Y , Zhao N . Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China:Aweb-based cross-sectional survey. medRxiv. 2020. doi: 10.1101/2020.02.19.20025395. |
[18] | JOHN WG . Depression and Anxiety. MJA Open. (2012) ;1: (Suppl 4):28–31. |
[19] | Lai J , Ma S , Wang Y , Cai Z , Hu J , Wei N , et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA network open. (2020) ;3: (3):e203976–e203976. doi: 10.1001/jamanetworkopen.2020.3976. |
[20] | Vos T , Allen C , Arora M , Barber RM , Bhutta ZA , Brown A , et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. The lancet. (2016) ;388: (10053):1545–602. doi: 10.1016/S0140-6736(16)31678-6. |
[21] | Gül A , Üstündağ H , Kahraman B , Purisa S . Hemşirelerde Kas. İskelet Ağrılarının Değerlendirilmesi [Assessment of Musculoskeletal Pain in Nurses]. HSP. (2014) ;1: (1):1–10. |
[22] | Abu Tariah H , Nafaic S , Alajmia M , Almutairi F , Alanazi B . Work-related musculoskeletal disorders in nurses working in the Kingdom of Saudi Arabia. Work Preprint. 2020;1-8. doi: 10.3233/WOR-203094. |
[23] | Alwabli Y , Almatroudi MA , Alharbi MA , Alharbi MY , Alreshood S , Althwiny FA . Work-Related Musculoskeletal Disorders Among Medical Practitioners in the Hospitals of Al’Qassim Region, Saudi Arabia. Cureus. (2020) ;12: (5). doi: 10.7759/cureus.8382. |
[24] | Huynh G , Nguyen TNH , Vo KN , Pham LA . Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pacific Journal of Tropical Medicine. (2020) ;13: (6):260. doi: 10.4103/1995-7645.280396. |
[25] | Siddiqui AA , Alshammary F , Amin J , Rathore HA , Hassan I , Ilyas M , et al. Knowledge and practice regarding prevention of COVID-19 among the Saudi Arabian population. Work. 2020; (Preprint): 1-9. |
[26] | Kolahkaj B , Zargar F . Effect of mindfulness-based stress reduction on anxiety, depression and stress in women with multiple sclerosis. Nurs Midwifery Stud. (2015) ;4: :e29655. doi: 10.17795/nmsjournal29655. |
[27] | Davıson C , Cotrim TP , Gonçalves S . Perception of Musculoskeletal Symptoms and Psychosocial Risk Factors Among a Sample of Portuguese Emergency Medical Technicians. In: International Conference on Healthcare Ergonomics and Patient Safety. Springer, Cham. (2019) ;46–55. |


