
The mediating role of religiosity and hope for the effect of self-stigma on psychological well-being among COVID-19 patients
Abstract
BACKGROUND:
Over the past few months, there has been a significant increase in mortality and morbidity due to Coronavirus disease (COVID-19). Less attention has been paid to stigmatism, psychological well-being, hope, and religiosity, and how these may impact a patient’s recovery.
OBJECTIVES:
This study aimed to detect the difference in religiosity, hope, self-stigma, and psychological well-being (PWB) due to demographic variables (age, education level, social status, and level of income). Additionally, the research sought to test the mediation role of religiosity and hope in the relationship between self-stigma and psychological well-being among COVID-19 patients.
METHOD:
A random sample of 426 COVID-19 patients answered an online questionnaire that contained four scales (Religiosity, Hope, stigma, and PWB). The data collected from the study participants were analyzed quantitatively by using One-way ANOVA, Exploratory Factor Analysis EFA, Confirmatory Factor Analysis CFA, and Structural Equation Model (IBM SPSS statistics 21, and Amos v.25).
RESULTS:
The current results showed statistically significant differences due to age in hope and well-being, in favor of the sample members belonging to the age group from 30 years old and over old, while there were no differences in religiosity and stigma due to age. There were no differences due to education level in religiosity, hope, stigma, and well-being. Results showed statistically significant differences in well-being in favor of the married group, while there were no differences in religiosity, hope, and stigma due to social status. Regarding the effect of income level in the study variables, the results showed no differences due to religiosity, hope, stigma, and well-being. Moreover, the findings found that both religiosity and hope play a mediating role.
CONCLUSION:
Religiosity and hope play a mediating role in the relationship between stigma associated with COVID-19 and psychological well-being. These results indicate several strategies to reduce the adverse effects of the stigma associated with COVID-19 and increase well-being among COVID-19 patients.
1Introduction
The Coronavirus disease (COVID-19) was discovered in 2019 and had not been previously identified in humans. On 11 March 2020, the Director-General of WHO declared a pandemic [1, 2]. Some nurses refused to care for their COVID-19 patients and preferred to stay away from them for fear of contracting the virus [3]. Other health workers had an ethical commitment to their patients and continued to their patients and continued to work with patients, resulted in feelings of fear for personal safety and psychological well-being of themselves, other medical staff, and family. Positive attitudes in the workplace, the actual improvement of injured health workers, and the interruption of the Middle East Respiratory Syndrome virus among health care workers after adopting strict preventive measures alleviated their fear and prompted them to face the epidemic [4].
Because COVID-19 spread worldwide, religiosity for many individuals is an essential aspect of their health status and psychological immunity. Spirituality plays a vital role in all the steps of health care, especially its management, treatment, and healing [5]. Hope is critical for those who suffer from chronic diseases regardless of their proximity to death. It has a positive impact on encouraging patients to plan, make decisions, and take responsibility for a better future. Without hope, life is difficult and even impossible [6, 7]. Therefore, hope is a crucial factor in individuals’ mental health, especially COVID-19 patients who suffer from stresses that have severe consequences for the patients’ psychological well-being.
Regarding stigma, self-stigma is a form of delinquency that leads others to judge an individual as ineligible to participate in social interaction.
1.1Religiosity and psychological well-being
Major life crises affect people psychologically, socially, and physically, as well as religiously and spiritually. There is no doubt that religiosity affects the psychological well-being and mental health, which affects the physical health of individuals and their ability to cope with epidemic infectious diseases, such as COVID-19 [8].
Despite the many writings on the importance of evaluation and intervention related to the patient’s religious needs, there is as yet little understanding of religiosity’s effect on the care provided by health personnel to patients [9]. The number of papers studying the relationship between religion and health in psychosocial and behavioral sciences has increased significantly [10].
The previous studies in this area showed the role of religion in health consequences. Religiosity correlates with health-related physiological processes such as cardiovascular, neuroendocrine, and immune function [11]. Regular religious attendance is related to a wide range of healthy behaviors, such as preventive care use, vitamin use, infrequent bar attendance, seat belt use, walking, strenuous exercise, sound sleep quality, never smoking, and moderate drinking [12]. Daily spiritual experiences were related to more significant health behaviors, while religion was less related to this [13]. Religiosity as a predictor of breast cancers’ psychological well-being [14].
1.2Hope and psychological well-being
The current century is considered the era of positive psychology and the study of positive features in an individual’s personality [15]. Hope is one of the essential concepts in this field; it can promote individuals’ psychological health. Hope an individual’s performance future or an individual’s competencies to achieve aims [16]. Instead, hope is the components for future expectations, and these components are based mainly on how an individual understands the world, instead of assessing their competencies [16–18].
By reviewing the theoretical literature on hope, we found that Seligman mentioned that hope is a critical component of a person’s everyday life. He stressed the importance of the relationship between hope and psychological well-being. He also saw that hope belongs to the positive emotions that have a relationship with the individual’s future, and these emotions are one of the necessary components of happiness and psychological well-being. Therefore, hope is a living experience that means a person who enjoys this experience moves towards the future. His efforts mobilized to transcend the present and contribute effectively to making a better future. That is why the theory of hope assumes that those with high hope can form new paths to their desired aims when facing obstacles and stress in their lives.
From the above, we noted that hope is significant for all individuals who face stresses, such as patients, to adapt to their disease. Several studies have found that hope has strong positive relations with various psychological outcomes, such as emotional adjustment and quality of life [19]. Foote et al. [20] indicated a relationship was found between hope, social support, and self-esteem in patients. In the same context, patients with high hope showed high acceptance of the disease and psychological pain [15]. Change [21] found a relationship was found between hope and quality of life for university students. Also, the cancer patients’ hope was a predictor of adapting and accepting the disease [22]. About the relation between hope and quality of life, Brooks et al. [23] found between hope and quality of life in elderly cancer patients. The previous studies detected the mediating role of hope in alleviating the impact of HIV stress on the quality of their lives [24, 25]. Hope is a statistical predictor of the concept of self and quality of life among patients with kidney failure [6].
Recently, study about the role of hope in shaping psychological health and psychological well-being during COVID-19, recommended to pay more attention to hope for improving psychological health during crisis time [26]. Another study indicates that the intense level of hope correlates with a lower level of anxiety and lower COVID-19 stress. Hope acts as a buffer on the face of the anxiety and the stress reactions on the virus pandemic [18]. Sheretta et al. [24] outlined the potent role of the psychological risk that could arise from the lockdown or physical distancing of COVID-19. Providing psychological skills increases hopefulness during this challenging time, Bloch-Atefi et al. [27] reported that give the clients with positive expectation and help them construct hope that makes sense for them. That could be enormously helpful in making this difficult time more manageable.
1.3Self-stigma and psychological well-being
Self-stigma is a subjective process characterized by negative feelings towards the self, non-adaptive behavior, a shift in identity, and results from an indi-vidual’s experiences or perceptions or anticipating negative social reactions [28]. Self-stigma is a concept that refers to a set of countermeasures, stereo-types, discriminatory behaviors, and biased social groupings endorsed by a large group towards ano-ther subgroup. The COVID-19 patients’ self-stigma occurs when members of a stigmatized group incorporate negative views of themselves due to their sense of humiliation and isolation from others. Stigma is a mark of disgrace that distinguishes a person from others [29]. It has many negative effects that prevent healing the disease, such as feeling shame and embarrassment [30, 31].
There are three types of stigma: Public stigma: It is the most well-known species, and some call it t group’s stigma. The focus is on the general attitudes and the attitudes of society towards persons subject to stigma. Self-stigma: The focus on this type is about assimilating and integrating individuals with negative societal views. Family stigma: This type refers to the stigma experienced by the individual due to his association with relatives who suffer stigma [30]. Brohan [7] divided stigma into three types: Extreme hatred of the body: as in the case of physical disability or apparent deformity, for example. Defects of an individual nature: such as mental illness or criminal conviction. Tribe stigma: includes race, gender, and age.
Self-stigma is associated with an increased rate of mental problems, anxiety, depression, and poor health in general [30]. Self-stigma hurts individuals, as it leads to a decrease in self-esteem, self-efficacy, life satisfaction, social adjustment, overall psychological well-being, and social contact [32]. Stigma is associated with fear of social discrimination and often chases certain people or groups because of its association with the diseases’ place and time. Stigma is a reason for isolating stigmatized persons and their fear of exposure to past or racial discrimination. Studies have shown that stigma and a sense of shame negatively affect the progress of treatment and medical intervention with patients, including COVID-19 patients, as happened previously with other patients such as HIV [33]. According to UNICEF [34], “Social stigma in the context of health is the negative association between a person or group of people who share certain characteristics and a specific disease. In an outbreak, this may mean people are label typed, discriminated against, treated separately, and experience loss of status because of a perceived link with a disease”. The COVID-19 outbreak resulted in social stigma and discriminatory behaviors against certain races and anyone infected with the virus.
Thus, we can define COVID-19 patients’ self-stigma as a perceived negative trait of COVID-19 patients to negative views and beliefs that would adversely affect their behaviors include: awareness of social discrimination, the incorporation of stigma, and avoiding situations capable of provoking him. Breast cancer self-stigma results in a lack of self-efficacy and social skills, with a loss of the original identity and its replacement with a new socially unacceptable identity that isolates them from society and strengthens the idea of social rejection, as well as a feeling of psychological insufficiency.
The degree of stigma associated with COVID-19 disease depends on some factors:(1) It is a new disease, and there is still a lot of new information; (2) We are often afraid of the unknown; (3) It is easy to link this fear to others.” Understandably, there is confusion, anxiety, and fear among the audience. Unfortunately, these factors fuel harmful stereotypes [34–36]. Also, studies found that the quarantine and strict tracking of infected cases by health authorities may cause society to reject these measures, and the spread of discrimination and social stigma among people [24]. Studies have shown that during an outbreak of epidemic diseases, which put severe stress on public health services, some people who are more likely to be at risk of stigma and discrimination will need special medical concerns [13, 37]. During the SARS virus, some people became fearful and suspicious of all individuals who seemed Asian, regardless of their nationality or the real risk factors for the disease [13].
Persons who are feared and stigmatized may delay seeking care and remain in the community undetected”. Person et al. [13] found that discrimination often has social and economic ramifications that intensify internalized stigmatization and feelings of fear. In the same, stigma affected most residents and took various forms of being shunned, insulted, marginalized, and rejected in work, interpersonal relationships, use of services, and schooling. Lee et al. [36] indicated that Stigma was also associated with psychosomatic distress. James et al. [38] found a high level of internalized stigma (0.92±0.77) Compared to total enacted stigma that came relatively low (0.71±0.61) among Ebola survivors in Sierra Leone. Religiosity perceived health status and region were the independent predictors of stigma. After checking the results of many studies [39–41] about stigma among patients, we can summarize these results as follows:
1. Stigma can dramatically increase the suffering of people infected with the disease caused by the virus.
2. It may lead to the failure to seek health care services by people who are sick with or at risk of infection, which increases the difficulties for health authorities to control the disease.
3. Stigmatization of health professionals and health care professionals may lead to high rates of stress and fatigue and, consequently, their inability to provide the required quality medical services.
These adverse effects that self-stigma has on COVID-19 patients’ personalities may disrupt their awareness of reality, distort their way of thinking, and attack them many psychological disorders.
1.4COVID-19 patients’ psychological well-being
The Kingdom of Saudi Arabia is considered the Arab country in which COVID-19 has spread most, with estimates that reached in May 20-2020 to approximately 154,233 cases, of which 98,917 recovered, while the total mortality of the virus reached 1230 patients [42] confirmed cases of the COVID-19 might experience fear of severe disease consequences [36, 43]. As a result, their PWB is affected because they may suffer from anxiety, insomnia, denial, loneliness, and depression, reducing their benefit from COVID’s medical treatment. Also, some of these conditions may increase the risk of suicide. Furthermore, isolated cases may suffer from anxiety due to uncertainty about their health condition and the development of Obsessive Compulsive disorder symptoms, such as temperature checks and frequent sterilization [36].
2The current study
From the above, it is worth noting that the literature has scarce information on the importance of the median role of hope for the effect of self-stigma on psychological well-being among COVID-19 patients. There is a lack of studies interested in studying the modified role of hope to relieve the impact of stigma on psychological well-being in patients with COVID-19. Thus we need to shed light on the nature of the relationship between the self-stigma among COVID-19 patients and their psychological well-being and detect the role that religiosity and hope can play in relief the negative effect of self-stigma on COVID-19 patients’ psychological well-being. Therefore, in the present study, we assumed that religiosity and hope could play a median role in the relationship between stigma related to COVID-19 and psychological well-being.
3Method
3.1Participants
A random sample of 426 COVID-19 patients who reside in the Kingdom of Saudi Arabian. The researchers choose the study sample from different ages, social statuses, education levels, and income levels. A total of 11.0%(N = 47) were less than 30 years old, 61.2%(N = 262) between 30–50 years old, and 27.5%(N = 117) were over than 50 years old. While the distribution of the sample at the level of education in three levels, a total of 28.9%(N = 123) less than university education level, 59.6%(N = 254) university graduates, and 11.5%(N = 49) were postgraduate. Out of 79.1%(N = 337) were married, 14.1%(N = 60) was unmarried, 4.9%(N = 21) were divorced, and 1.9%(N = 8) widower. This study sample was distributed over four income levels, a total of 44.6 (N = 190) less than 10 thousand SAR, 44.1%(N = 188) between 10–20 thousand SAR, 8.0%(N = 34) between 20–30 thousand SAR, and 3.3%(N = 14) more than 30 thousand SAR.
3.2Procedures
The current study applied a descriptive method to detect the differences in religiosity, hope, stigma, and psychological well-being and reveal the direct and indirect effects among religiosity, hope, stigma, and well-being. The online questionnaire (contain self-report scales of religiosity, hope, stigma, and psychological well-being) sent to the study sample.
3.3Instruments
3.3.1COVID-19 Patients’ Religiosity Scale (CPRS-9)
In this study, the researchers prepared the self- report COVID-19 Patients’ Religiosity Scale, which consisted of 9 items. The participate response with a 5-point Likert scale (full agree = 5 to not fully agree = 1). The correlations between CPRS-9 and the scale’s total score were calculated, and the correlation coefficients ranged from 0.400 to 0.813 and were statistically significant at 0.01 level (2-tailed). Also, Cronbach’s Alpha for the CPRS-9 was 0.761, Spearman-Brown Coefficient for unequal length was 0.688. These results indicated that CPRS-9 is validated and reliable.
Exploratory Factor Analysis (EFA) the Principle Components Analysis (PCA) method was used to derive CPRS-9 factors. EFA produced two factors that accounted for (62.283%) of the total variance of the scale. The results are shown in Table 1.
Table 1
Rotated Component Matrixa
| Component | ||
| 1 | 2 | |
| R1 | 0.791 | |
| R2 | 0.877 | |
| R3 | 0.733 | |
| R4 | 0.735 | |
| R5 | 0.776 | |
| R6 | 0.684 | |
| R7 | 0.598 | |
| R8 | 0.729 | |
| R9 | 0.739 | |
| Total of variance | 34.030 | 28.253 |
Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalization.
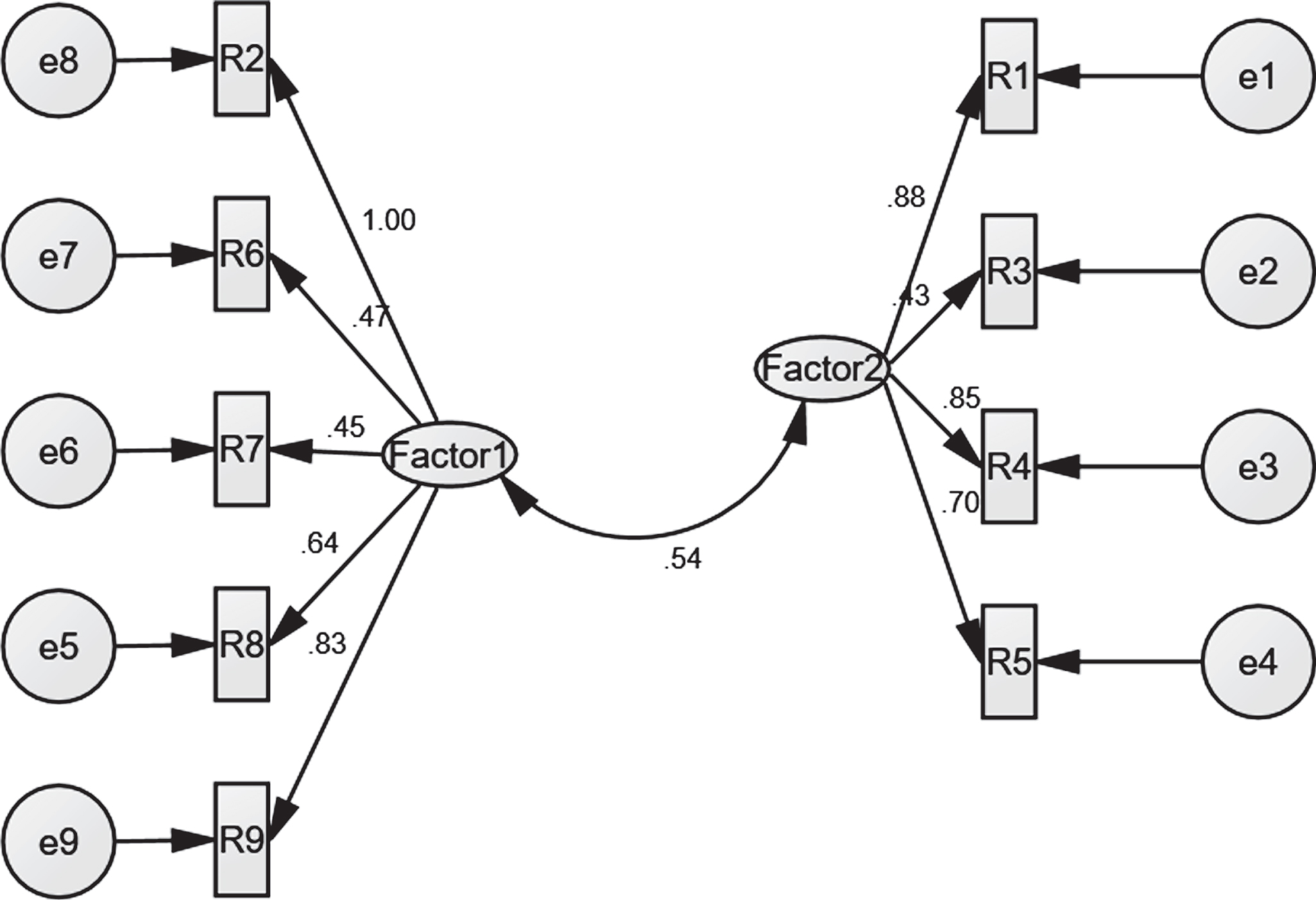
To validate the religiosity factors, Confirmatory Factor Analysis CFA was used. The results showed that there are appropriate goodness fit indexes (CMIN/DF = 3.652; NFI = 0.808; CFI = 0.849; RMSEA = 0.05), all of which indicated that the religiosity standards proposed model is acceptable. All of the religiosity observed variables had statistically significant (p < 0.001) loadings on the respective latent variables (see Fig. 1).
Fig. 1
Confirmatory factor analysis of the religiosity standards proposed model.
3.3.2COVID-19 Patients’ Hope Scale (CPHS-8)
The researchers prepared the COVID-19 Patients’ Hope Scale, which consisted of 8 items. The participate responds with a 5-point Likert scale (fully agree = 5 to not fully agree = 1). The correlations between CPHS-8 and the total scale score were calculated. The correlation coefficients ranged between 0.429 and 0.659, with significance at the 0.01 level (2-tailed). As well as, Cronbach’s Alpha for the CPHS-8 was 0.639, Spearman-Brown Coefficient for unequal length was 0.430. These results indicated that CPHS-8 is validated and reliable.
Exploratory Factor Analysis (EFA) the Principle Components Analysis (PCA) method was used to derive CSHS-8 factors. EFA produced two factors that accounted for (53.886%) of the total variance of the scale. The results are shown in Table 2.
Table 2
Rotated Component Matrixa
| Component | ||
| 1 | 2 | |
| H1 | 0.478 | |
| H2 | 0.734 | |
| H3 | 0.747 | |
| H4 | 0.549 | |
| H5 | 0.722 | |
| H6 | 0.726 | |
| H7 | 0.895 | |
| H8 | 0.874 | |
| Total of variance | 36.120 | 17.766 |
Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalization.
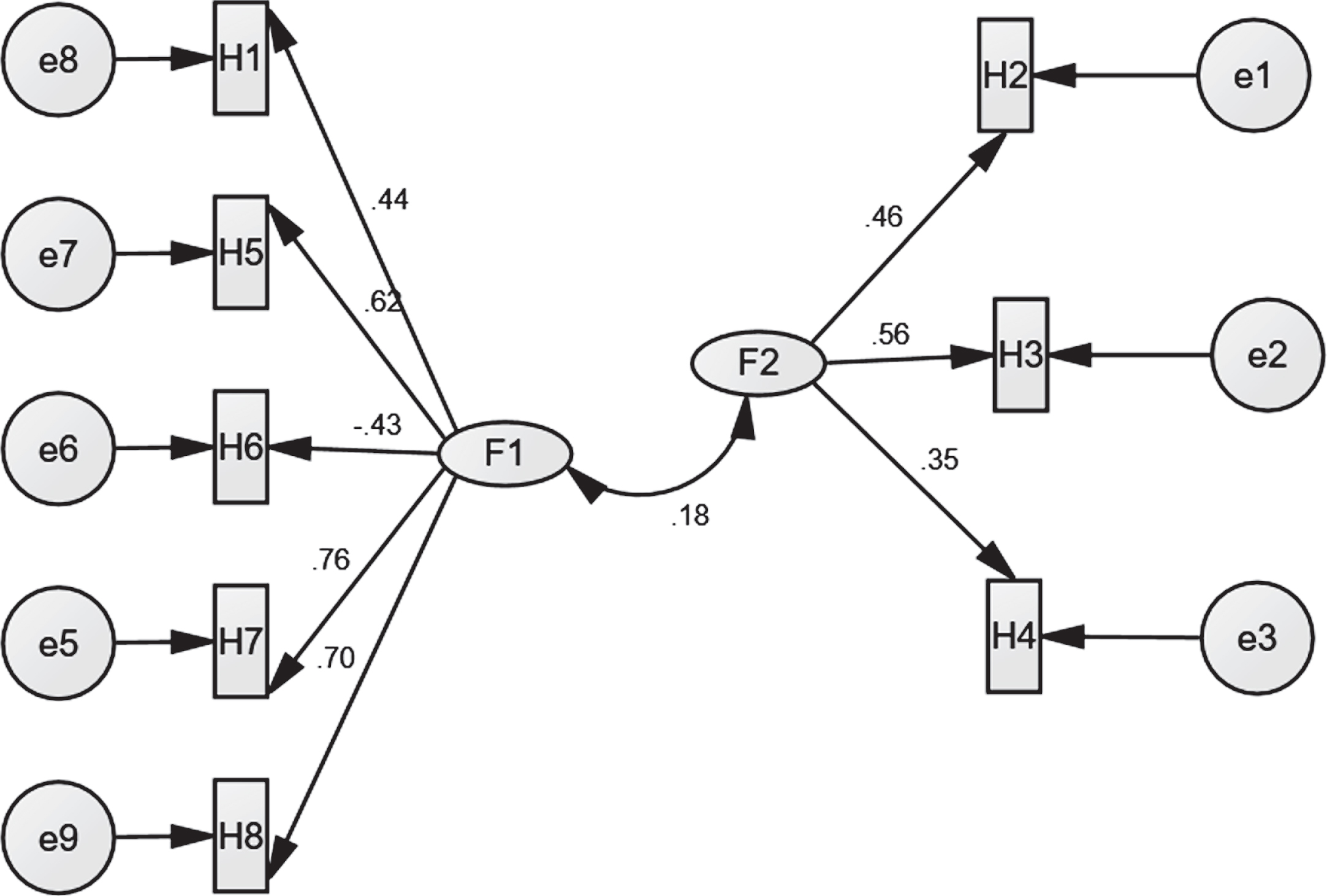
To validate the hope factors, Confirmatory Factor Analysis CFA was used. The results showed that there are appropriate goodness fit indexes (CMIN/DF = 2.360; NFI = 0.860; CFI = 0.878; RMSEA =0.053), all of which indicated that the hope standards proposed model is acceptable. All of the Hope observed variables had statistically significant (p < 0.001) loadings on the respective latent variables (see Fig. 2).
Fig. 2
Confirmatory factor analysis of the hope standards proposed model.
3.3.3COVID-19 Patients’ Stigma Scale (CPSS-10)
The self- report COVID-19 Patients’ Stigma Scale, which consisted of 10 items. The participate responds with a 5-point Likert scale (fully agree = 5 to not fully agree = 1). The correlations between CPSS-10 and the scale’s total score were calculated, and the correlation coefficients ranged from 0.526 to 0.804, with significance at 0.01 level (2-tailed). As well as, Cronbach’s Alpha for the CPSS-10 was 0.884, Spearman-Brown Coefficient for unequal length was 0.881. These results indicated that the CPSS-10 is validated and reliable.
Exploratory Factor Analysis (EFA) the Principle Components Analysis (PCA) method was used to derive CPSS-10 factors. EFA produced two factors that accounted for (65.743%) of the total variance of the scale. The results are shown in Table 3.
Table 3
Rotated Component Matrixa
| Component | ||
| 1 | 2 | |
| S1 | 0.804 | |
| S2 | 0.643 | |
| S3 | 0.776 | |
| S4 | 0.841 | |
| S5 | 0.801 | |
| S6 | 0.818 | |
| S7 | 0.806 | |
| S8 | 0.663 | |
| S9 | 0.754 | |
| S10 | 0.546 | |
| Total of variance | 42.851 | 22.892 |
Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalization.
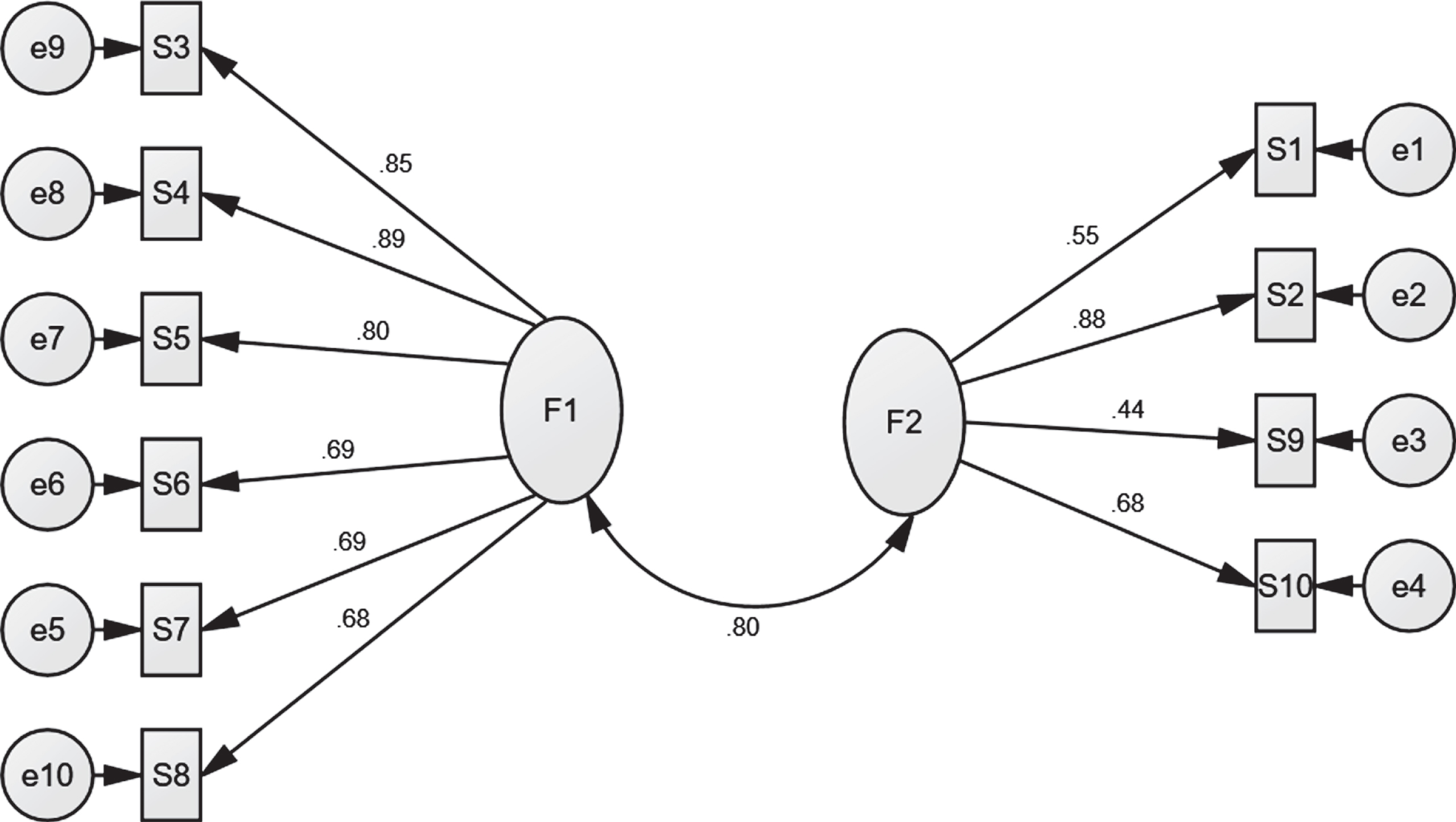
Confirmatory Factor Analysis CFA was used to validate the stigma factors. The results showed that there are appropriate goodness fit indexes (CMIN/DF = 3.281; NFI = 0.789; CFI = 0.832; RMSEA =0.049) that the stigma standards proposed model is acceptable. All of the Hope observed variables had statistically significant (p < 0.001) loadings on the respective latent variables (see Fig. 3).
Fig. 3
Confirmatory factor analysis of the stigma standards proposed model.
3.3.4COVID-19 Patients’ Psychological Well-being Scale (CPWS-10)
The researchers prepared the self-report COVID-19 Patients’ Psychological Well-being Scale, which consisted of 10 items. The participate responds with a 5-point Likert scale (fully agree = 5 to not fully agree = 1). The correlations between CPWS-10 and the scale’s total score were calculated, and the correlation coefficients ranged from 0.524 to 0.718, with significance at 0.01 level (2-tailed). As well as, Cronbach’s Alpha for the CPWS-10 was 0.809, Spearman-Brown Coefficient for unequal length was 0.790. These results indicated that CPWS-10 is validated and reliable.
Exploratory Factor Analysis (EFA) the Principle Components Analysis (PCA) method was used to derive CSWS-10 factors. EFA produced three factors that accounted for (60.386%) of the total variance of the scale. The results are shown in Table 4.
Table 4
Rotated Component Matrixa
| Component | |||
| 1 | 2 | 3 | |
| W1 | 0.313 | ||
| W2 | 0.813 | ||
| W3 | 0.783 | ||
| W4 | 0.757 | ||
| W5 | 0.431 | ||
| W6 | 0.839 | ||
| W7 | 0.719 | ||
| W8 | 0.471 | ||
| W9 | 0.745 | ||
| W10 | 0.813 | ||
| Total of variance | 22.236 | 19.269 | 18.858 |
Extraction Method: Principal Component Analysis. Rotation Method: Varimax with Kaiser Normalization.
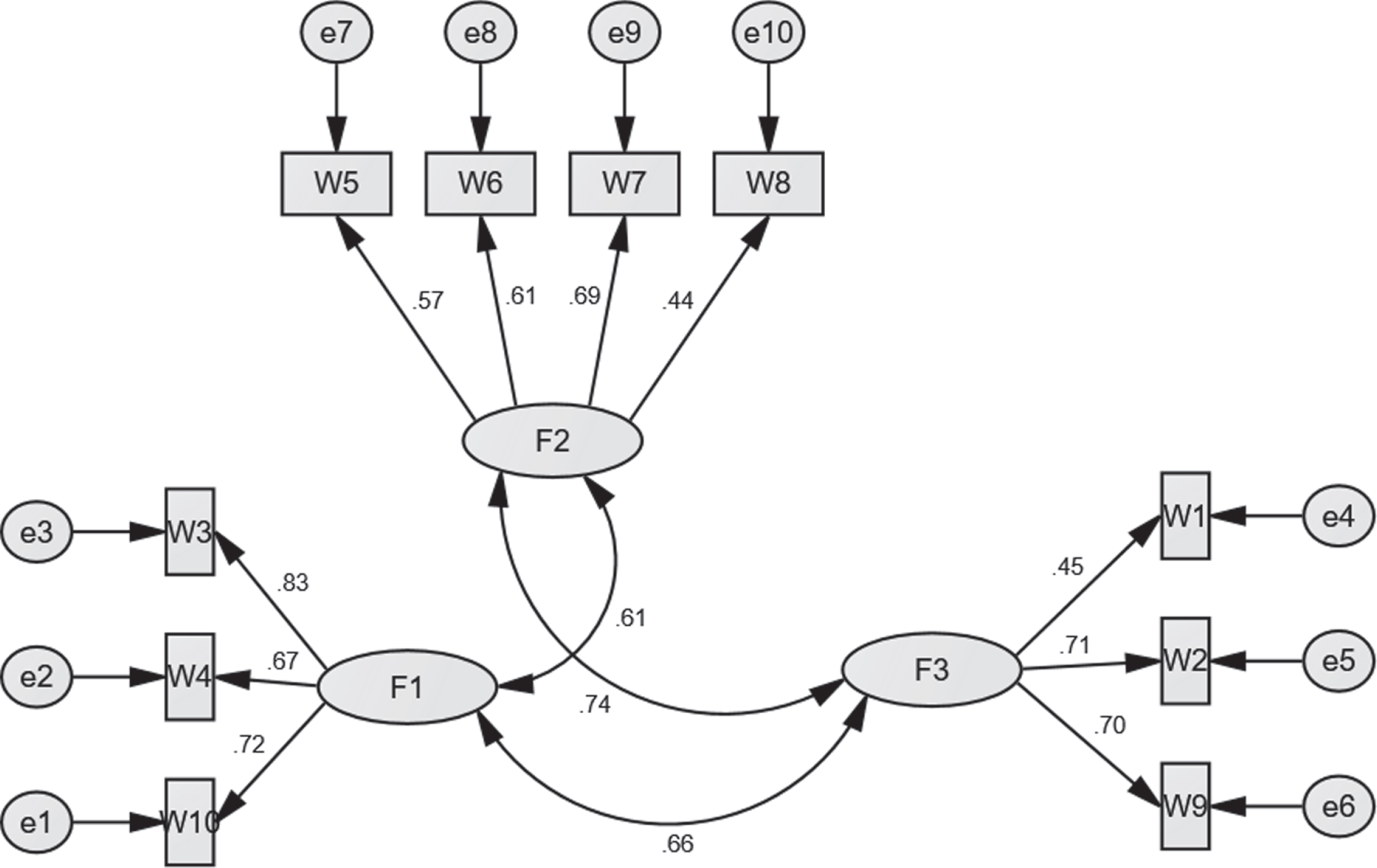
Confirmatory Factor Analysis CFA was used to validate the PWB factors. The results showed that there are appropriate goodness fit indexes (CMIN/DF = 1.671; NFI = 0.822; CFI = 0.920; RMSEA =0.054), all of which indicated that the PWB standards proposed model is acceptable. All of the Hope observed variables had statistically significant (p < 0.001) loadings on the respective latent variables (see Fig. 4).
Fig. 4
Confirmatory factor analysis of the hope standards proposed model.
3.4Data analysis
The data collected from the study participants were analyzed quantitatively. One-way ANOVA was calculated to reveal the study variables’ differences due to age, level of education, marital status, and income level variables (IBM SPSS statistics version 21). Exploratory Factor Analysis EFA using to extract the factors of each scales prepared in this study, and then using Confirmatory Factor Analysis CFA to validate this factor (IBM SPSS Amos 25). The Structural Equation Model was used to test the direct and indirect effects between study variables and validate the mediating role of religiosity and hope in the relationship between the stigma associated with COVID-19 and psychological well-being.
4Results
4.1The results about the differences in religiosity, hope, stigma, and psychological well-being due to age: one-way ANOVA calculated to detect the differences in religiosity, hope, stigma, and PWB. The findings are shown in Tables 5, 6, 7
The results shown in Table 6 indicated significant differences due to age in Hope and psychological well-being, while there are no differences in religiosity and stigma due to age. A Scheffe test was used to determine the direction of the differences (see results in Table 7). The results indicate the differences in hope and psychological well-being were in favor of members belonging to the age group from 30 years old and over.
Table 5
The results about the differences in religiosity, hope, stigma, and psychological well-being due to age
| N | Mean | Std. deviation | Std. error | ||
| Religiosity | 1 | 47 | 43.5319 | 2.26362 | 0.33018 |
| 2 | 262 | 43.8550 | 1.76870 | 0.10927 | |
| 3 | 117 | 43.8462 | 1.77926 | 0.16449 | |
| Total | 426 | 43.8169 | 1.83028 | 0.08868 | |
| Hope | 1 | 47 | 22.4894 | 2.74157 | 0.39990 |
| 2 | 262 | 23.7557 | 2.90486 | 0.17946 | |
| 3 | 117 | 23.3162 | 2.57190 | 0.23777 | |
| Total | 426 | 23.4953 | 2.82197 | 0.13672 | |
| Stigma | 1 | 47 | 19.8511 | 8.44928 | 1.23245 |
| 2 | 262 | 18.6336 | 5.83648 | 0.36058 | |
| 3 | 117 | 18.0171 | 5.67205 | 0.52438 | |
| Total | 426 | 18.5986 | 6.13962 | 0.29747 | |
| PWB | 1 | 46 | 40.7391 | 5.91208 | 0.87169 |
| 2 | 261 | 44.3448 | 4.81543 | 0.29807 | |
| 3 | 117 | 44.2393 | 4.10351 | 0.37937 | |
| Total | 424 | 43.9245 | 4.88148 | 0.23707 |
Table 6
The results about the differences in religiosity, hope, stigma, and psychological well-being due to age (ANOVA)
| Sum of squares | df | Mean square | F | Sig. | ||
| Religiosity | Between groups | 4.297 | 2 | 2.148 | 0.640 | 0.528 |
| Within groups | 1419.421 | 423 | 3.356 | |||
| Total | 1423.718 | 425 | ||||
| Hope | Between groups | 69.080 | 2 | 34.540 | 4.407 | 0.013 |
| Within groups | 3315.410 | 423 | 7.838 | |||
| Total | 3384.491 | 425 | ||||
| Stigma | Between groups | 113.611 | 2 | 56.806 | 1.511 | 0.222 |
| Within groups | 15906.748 | 423 | 37.605 | |||
| Total | 16020.359 | 425 | ||||
| PWB | Between groups | 524.451 | 2 | 262.225 | 11.554 | 0.000 |
| Within groups | 9555.134 | 421 | 22.696 | |||
| Total | 10079.585 | 423 |
Table 7
The results of the Scheffe test for the differences in religiosity, hope, stigma, and psychological well-being due to age
| Dependent variable | (I) Age | (J) Age | Mean difference (I-J) | Std. error | Sig. |
| Religiosity | 1 | 2 | –0.32305- | 0.29018 | 0.539 |
| 3 | –0.31424- | 0.31635 | 0.611 | ||
| 2 | 1 | 0.32305 | 0.29018 | 0.539 | |
| 3 | 0.00881 | 0.20369 | 0.999 | ||
| 3 | 1 | 0.31424 | 0.31635 | 0.611 | |
| 2 | –0.00881- | 0.20369 | 0.999 | ||
| Hope | 1 | 2 | –1.26636- * | 0.44348 | 0.018 |
| 3 | –0.82688- | 0.48348 | 0.233 | ||
| 2 | 1 | 1.26636 * | 0.44348 | 0.018 | |
| 3 | 0.43949 | 0.31130 | 0.370 | ||
| 3 | 1 | 0.82688 | 0.48348 | 0.233 | |
| 2 | –0.43949- | 0.31130 | 0.370 | ||
| Stigma | 1 | 2 | 1.21748 | 0.97140 | 0.457 |
| 3 | 1.83397 | 1.05901 | 0.224 | ||
| 2 | 1 | –0.1.21748- | 0.97140 | 0.457 | |
| 3 | 0.61649 | 0.68186 | 0.665 | ||
| 3 | 1 | –1.83397- | 1.05901 | 0.224 | |
| 2 | –0.61649- | 0.68186 | 0.665 | ||
| PWB | 1 | 2 | –3.60570- * | 0.76181 | 0.000 |
| 3 | –3.50019- * | 0.82909 | 0.000 | ||
| 2 | 1 | 3.60570 * | 0.76181 | 0.000 | |
| 3 | 0.10551 | 0.53004 | 0.980 | ||
| 3 | 1 | 3.50019 * | 0.82909 | 0.000 | |
| 2 | –0.10551- | 0.53004 | 0.980 |
4.2The results about the differences in religiosity, hope, stigma, and psychological well-being due to education level: one-way ANOVA calculated to detect the differences in religiosity, hope, stigma, and psychological well-being. The findings are shown in Tables 8, 9
The results shown in Table 9 indicated that there are no statistically significant differences due to education status in religiosity, hope, stigma, and psychological well-being among COVID-19 patients.
Table 8
The results about the differences in religiosity, hope, stigma, and psychological well-being due to education level
| N | Mean | Std. deviation | Std. error | ||
| Religiosity | 1 | 123 | 43.8780 | 1.77221 | 0.15980 |
| 2 | 254 | 43.8780 | 1.78843 | 0.11222 | |
| 3 | 49 | 43.3469 | 2.13650 | 0.30521 | |
| Total | 426 | 43.8169 | 1.83028 | 0.08868 | |
| Hope | 1 | 123 | 23.7317 | 2.61482 | 0.23577 |
| 2 | 254 | 23.4370 | 2.90052 | 0.18199 | |
| 3 | 49 | 23.2041 | 2.92247 | 0.41750 | |
| Total | 426 | 23.4953 | 2.82197 | 0.13672 | |
| Stigma | 1 | 123 | 18.2520 | 4.89160 | 0.44106 |
| 2 | 254 | 18.6732 | 5.98809 | 0.37573 | |
| 3 | 49 | 19.0816 | 9.13062 | 1.30437 | |
| Total | 426 | 18.5986 | 6.13962 | 0.29747 | |
| PWB | 1 | 123 | 44.3984 | 4.62484 | 0.41701 |
| 2 | 253 | 43.8933 | 4.62057 | 0.29049 | |
| 3 | 48 | 42.8750 | 6.53835 | 0.94373 | |
| Total | 424 | 43.9245 | 4.88148 | 0.23707 |
Table 9
The results about the differences in religiosity, hope, stigma, and psychological well-being due to education level (ANOVA)
| Sum of squares | df | Mean square | F | Sig. | ||
| Religiosity | Between groups | 12.229 | 2 | 6.115 | 1.832 | 0.161 |
| Within groups | 1411.489 | 423 | 3.337 | |||
| Total | 1423.718 | 425 | ||||
| Hope | Between groups | 11.893 | 2 | 5.946 | 0.746 | 0.475 |
| Within groups | 3372.598 | 423 | 7.973 | |||
| Total | 3384.491 | 425 | ||||
| Stigma | Between groups | 27.621 | 2 | 13.810 | 0.365 | 0.694 |
| Within groups | 15992.738 | 423 | 37.808 | |||
| Total | 16020.359 | 425 | ||||
| PWB | Between groups | 80.737 | 2 | 40.368 | 1.700 | 0.184 |
| Within groups | 9998.848 | 421 | 23.750 | |||
| Total | 10079.585 | 423 |
4.3The results about differences in religiosity, hope, stigma, and psychological well-being due to social status: one-way ANOVA calculated to detect the differences in religiosity, hope, stigma, and psychological well-being. The findings are shown in Tables 10, 11, 12
The results shown in Table 11 indicated statistically significant differences due to social status in psychological well-being while there are no differences in religiosity, hope, and stigma among COVID-19 patients. A Scheffe test was used to determine the direction of the differences (see results in Table 12). The results indicate that the differences in psychological well-being were in favor of the sample members belonging to the married group of COVID-19 patients.
Table 10
The results about differences in religiosity, hope, stigma, and psychological well-being due to social status
| N | Mean | Std. deviation | Std. error | ||
| Religiosity | 1 | 60 | 43.6333 | 2.01660 | 0.26034 |
| 2 | 337 | 43.8309 | 1.81213 | 0.09871 | |
| 3 | 21 | 44.0952 | 1.78619 | 0.38978 | |
| 4 | 8 | 43.8750 | 1.35620 | 0.47949 | |
| Total | 426 | 43.8169 | 1.83028 | 0.08868 | |
| Hope | 1 | 60 | 22.7500 | 2.34792 | 0.30311 |
| 2 | 337 | 23.6409 | 2.91627 | 0.15886 | |
| 3 | 21 | 22.9048 | 2.30010 | 0.50192 | |
| 4 | 8 | 24.5000 | 2.39046 | 0.84515 | |
| Total | 426 | 23.4953 | 2.82197 | 0.13672 | |
| Stigma | 1 | 60 | 19.4500 | 8.10404 | 1.04623 |
| 2 | 337 | 18.3976 | 5.71827 | 0.31149 | |
| 3 | 21 | 17.8571 | 6.31099 | 1.37717 | |
| 4 | 8 | 22.6250 | 4.83846 | 1.71065 | |
| Total | 426 | 18.5986 | 6.13962 | 0.29747 | |
| PWB | 1 | 59 | 41.4068 | 6.15915 | 0.80185 |
| 2 | 336 | 44.3690 | 4.50878 | 0.24597 | |
| 3 | 21 | 44.0476 | 4.95456 | 1.08117 | |
| 4 | 8 | 43.5000 | 4.40779 | 1.55839 | |
| Total | 424 | 43.9245 | 4.88148 | 0.23707 |
Table 11
The results about differences in religiosity, hope, stigma, and psychological well-being due to social status (ANOVA)
| Sum of squares | df | Mean square | F | Sig. | ||
| Religiosity | Between groups | 3.741 | 3 | 1.247 | 0.371 | 0.774 |
| Within groups | 1419.977 | 422 | 3.365 | |||
| Total | 1423.718 | 425 | ||||
| Hope | Between groups | 55.876 | 3 | 18.625 | 2.361 | 0.071 |
| Within groups | 3328.614 | 422 | 7.888 | |||
| Total | 3384.491 | 425 | ||||
| Stigma | Between groups | 198.345 | 3 | 66.115 | 1.763 | 0.153 |
| Within groups | 15822.015 | 422 | 37.493 | |||
| Total | 16020.359 | 425 | ||||
| PWB | Between groups | 442.157 | 3 | 147.386 | 6.423 | 0.000 |
| Within groups | 9637.428 | 420 | 22.946 | |||
| Total | 10079.585 | 423 |
Table 12
The results of the Scheffe test for the differences in religiosity, hope, stigma, and PWB due to social status
| Dependent variable | (I) Social status | (J) Social status | Mean difference (I-J) | Std. error | Sig. |
| Religiosity | 1 | 2 | –0.19753- | 0.25703 | 0.899 |
| 3 | –0.46190- | 0.46509 | 0.805 | ||
| 4 | –0.24167- | 0.69043 | 0.989 | ||
| 2 | 1 | 0.19753 | 0.25703 | 0.899 | |
| 3 | –0.26438- | 0.41257 | 0.938 | ||
| 4 | –0.04414- | 0.65620 | 1.000 | ||
| 3 | 1 | 0.46190 | 0.46509 | 0.805 | |
| 2 | 0.26438 | 0.41257 | 0.938 | ||
| 4 | 0.22024 | 0.76213 | 0.994 | ||
| 4 | 1 | 0.24167 | 0.69043 | 0.989 | |
| 2 | 0.04414 | 0.65620 | 1.000 | ||
| 3 | –0.22024- | 0.76213 | 0.994 | ||
| Hope | 1 | 2 | –0.89095- | 0.39353 | 0.165 |
| 3 | –0.15476- | 0.71209 | 0.997 | ||
| 4 | –1.75000- | 1.05708 | 0.434 | ||
| 2 | 1 | 0.89095 | 0.39353 | 0.165 | |
| 3 | 0.73619 | 0.63167 | 0.715 | ||
| 4 | –0.85905- | 1.00467 | 0.866 | ||
| 3 | 1 | 0.15476 | 0.71209 | 0.997 | |
| 2 | –0.73619- | 0.63167 | 0.715 | ||
| 4 | –1.59524- | 1.16686 | 0.600 | ||
| 4 | 1 | 1.75000 | 1.05708 | 0.434 | |
| 2 | 0.85905 | 1.00467 | 0.866 | ||
| 3 | 1.59524 | 1.16686 | 0.600 | ||
| Stigma | 1 | 2 | 1.05237 | 0.85798 | 0.681 |
| 3 | 1.59286 | 1.55250 | 0.789 | ||
| 4 | –3.17500- | 2.30467 | 0.594 | ||
| 2 | 1 | –1.05237- | 0.85798 | 0.681 | |
| 3 | 0.54048 | 1.37718 | 0.985 | ||
| 4 | –4.22737- | 2.19040 | 0.294 | ||
| 3 | 1 | –1.59286- | 1.55250 | 0.789 | |
| 2 | –0.54048- | 1.37718 | 0.985 | ||
| 4 | –4.76786- | 2.54401 | 0.320 | ||
| 4 | 1 | 3.17500 | 2.30467 | 0.594 | |
| 2 | 4.22737 | 2.19040 | 0.294 | ||
| 3 | 4.76786 | 2.54401 | 0.320 | ||
| PWB | 1 | 2 | –2.96227- * | 0.67617 | 0.000 |
| 3 | –2.64084- | 1.21721 | 0.196 | ||
| 4 | –2.09322- | 1.80477 | 0.719 | ||
| 2 | 1 | 2.96227 * | 0.67617 | 0.000 | |
| 3 | 0.32143 | 1.07748 | 0.993 | ||
| 4 | 0.86905 | 1.71364 | 0.968 | ||
| 3 | 1 | 2.64084 | 1.21721 | 0.196 | |
| 2 | –0.32143- | 1.07748 | 0.993 | ||
| 4 | 0.54762 | 1.99022 | 0.995 | ||
| 4 | 1 | 2.09322 | 1.80477 | 0.719 | |
| 2 | –0.86905- | 1.71364 | 0.968 | ||
| 3 | –0.54762- | 1.99022 | 0.995 |
4.4The results about the differences in religiosity, hope, stigma, and psychological well-being due to income level: one-way ANOVA calculated to detect religiosity, hope, stigma, and psychological well-being among COVID-19 patients. The findings are shown in Tables 13, 14
The results shown in Table 14 indicated no statistically significant differences due to income level in religiosity, hope, stigma, and psychological well-being among COVID-19 patients.
Table 13
The results about the differences in religiosity, hope, stigma, and psychological well-being due to income level
| N | Mean | Std. deviation | Std. error | ||
| Religiosity | 1 | 190 | 43.7263 | 1.93788 | 0.14059 |
| 2 | 188 | 43.9681 | 1.69272 | 0.12345 | |
| 3 | 34 | 43.6176 | 1.84251 | 0.31599 | |
| 4 | 14 | 43.5000 | 2.10311 | 0.56208 | |
| Total | 426 | 43.8169 | 1.83028 | 0.08868 | |
| Hope | 1 | 190 | 23.1947 | 2.65851 | 0.19287 |
| 2 | 188 | 23.8723 | 2.71944 | 0.19834 | |
| 3 | 34 | 23.4706 | 3.61173 | 0.61941 | |
| 4 | 14 | 22.5714 | 3.71513 | 0.99291 | |
| Total | 426 | 23.4953 | 2.82197 | 0.13672 | |
| Stigma | 1 | 190 | 18.9421 | 6.34308 | 0.46018 |
| 2 | 188 | 18.5479 | 5.92311 | 0.43199 | |
| 3 | 34 | 17.5000 | 6.03148 | 1.03439 | |
| 4 | 14 | 17.2857 | 6.60336 | 1.76482 | |
| Total | 426 | 18.5986 | 6.13962 | 0.29747 | |
| PWB | 1 | 188 | 43.4096 | 5.26996 | 0.38435 |
| 2 | 188 | 44.1277 | 4.62089 | 0.33701 | |
| 3 | 34 | 44.7941 | 4.14714 | 0.71123 | |
| 4 | 14 | 46.0000 | 3.74166 | 1.00000 | |
| Total | 424 | 43.9245 | 4.88148 | 0.23707 |
Table 14
The results about the differences in religiosity, hope, stigma, and psychological well-being due to income level (ANOVA)
| Variables | Sum of squares | df | Mean square | F | Sig. | |
| Religiosity | Between groups | 8.612 | 3 | 2.871 | 0.856 | 0.464 |
| Within groups | 1415.106 | 422 | 3.353 | |||
| Total | 1423.718 | 425 | ||||
| Hope | Between groups | 55.861 | 3 | 18.620 | 2.361 | 0.071 |
| Within groups | 3328.630 | 422 | 7.888 | |||
| Total | 3384.491 | 425 | ||||
| Stigma | Between groups | 88.070 | 3 | 29.357 | 0.778 | 0.507 |
| Within groups | 15932.289 | 422 | 37.754 | |||
| Total | 16020.359 | 425 | ||||
| PWB | Between groups | 143.627 | 3 | 47.876 | 2.024 | 0.110 |
| Within groups | 9935.958 | 420 | 23.657 | |||
| Total | 10079.585 | 423 |
4.5The results about the intermediate role of religiosity and hope variables between stigma and psychological well-being among patients of COVID-19. The researchers drew a diagram model of the relationships between the study variables (see Fig. 5). To test this proposed model, structural equation modeling was used by the Maximum Likelihood Estimation method to find out the effects of religiosity and hope on stigma and psychological well-being as intermediate variables
To verify the fitness of the proposed model, the researchers used several indicators (Table 15) such as Chi-square divided in Degree of Freedom CMIN/DF (2.645), which is not insignificant value, and a Goodness Fit Index GFI (.96), the Root Mean Square Error of Approximation RAMSE (.062), which indicates that the proposed model is good. The results shown in Fig. 6 told that all paths of the model are statistically significant.
Table 15
Fit indices of the hypothesized model
| Indicators | Values in this study | |
| CMIN/DF | 2.645 | |
| GFI | 0.96 | |
| RAMSEA | 0.062 | |
| NFI | 0.964 | |
| RFI | 0.893 | |
| IFI | 0.965 | |
| CFI | 0.965 | |
| AIC | Model | Value |
| Default | 122.844 | |
| Independence | 1134.839 | |
| BBC | Model | Value |
| Default | 124.338 | |
| Independence | 1135.275 | |
Fig. 5
The structural equation model for the relation between religiosity, hope, stigma, and PWB.
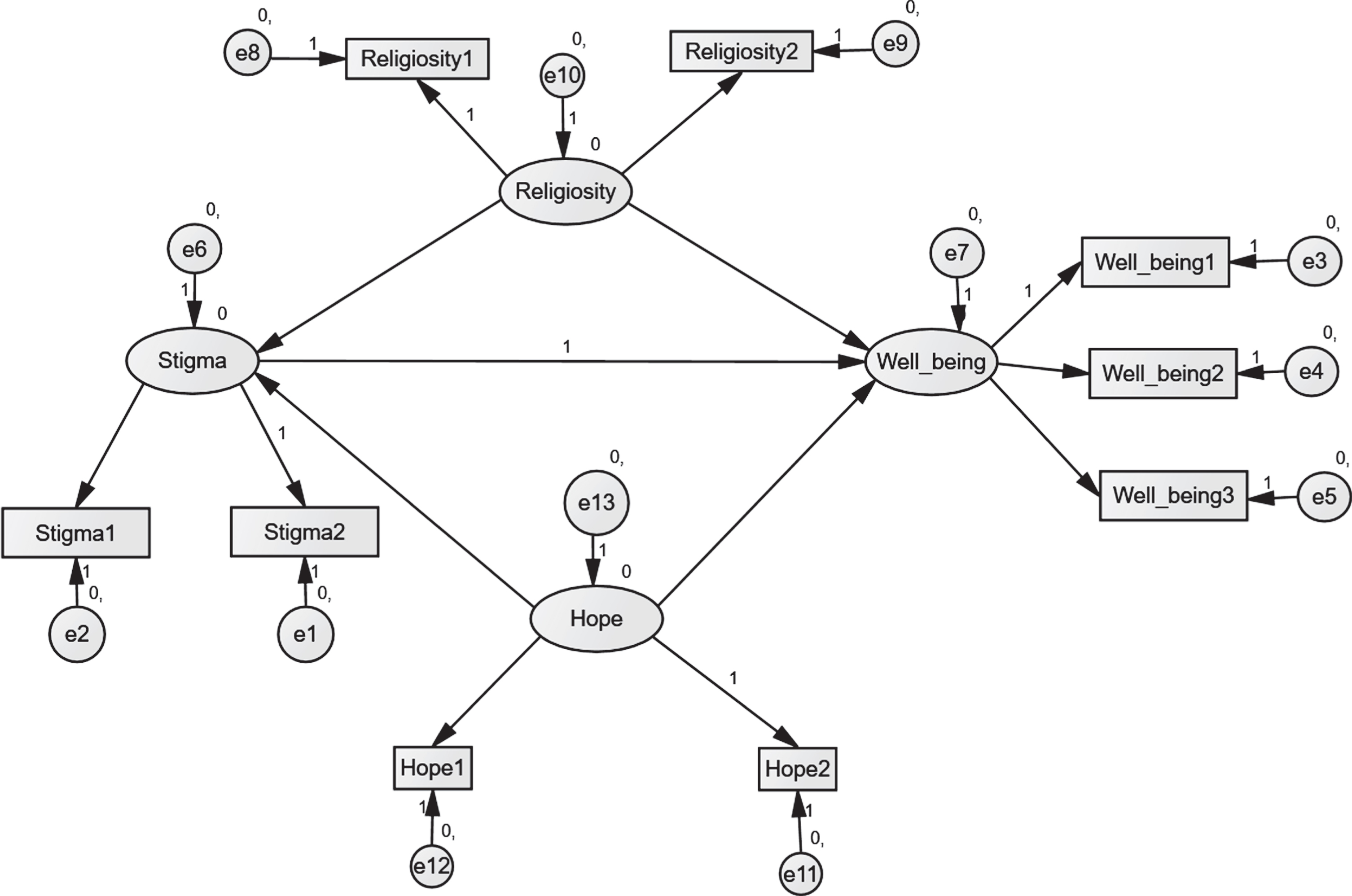
Fig. 6
The structural equation model for the relation between religiosity, hope, stigma, and psychological well-being.
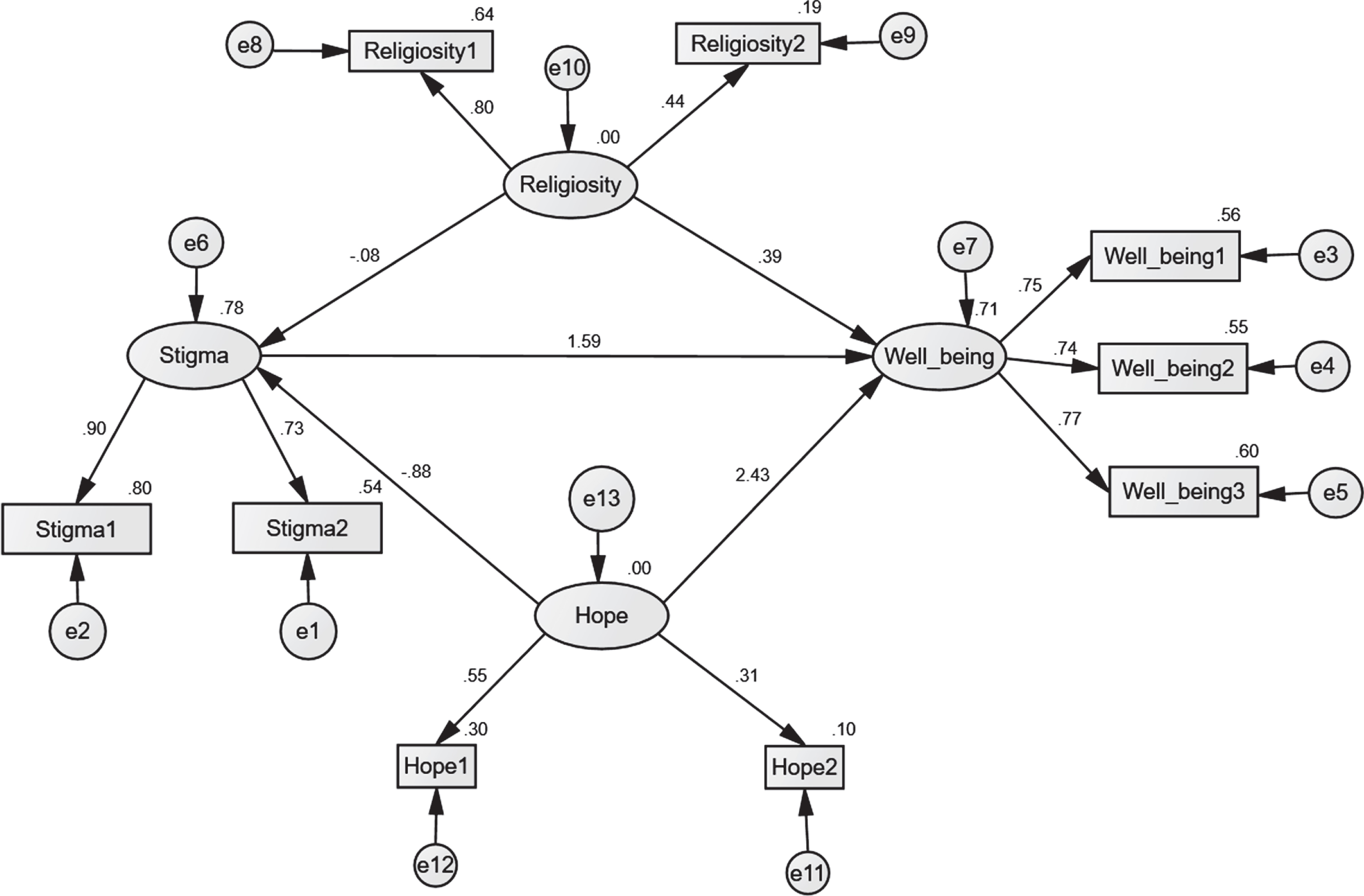
The results shown in Table 16 indicated that the direct (unmediated) effect of hope on psychological well-being is 7.236, which means when hope goes up by 1, psychological well-being (PWS) goes up by 7.236. As well as, the direct (unmediated) effect of religiosity on psychological well-being is.807. When religiosity goes up by 1, psychological well-being goes up by 0.807. Also, the direct (unmediated) effect of stigma on PWB is 1.000. When stigma goes up by 1, psychological well-being goes up by 1.
Table 16
The direct effects (n = 426 - default model)
| Hope | Religiosity | Stigma | PWB | |
| Stigma | –4.147 | –0.267 | 0.000 | 0.000 |
| PWB | 7.236 | 0.807 | 1.000 | 0.000 |
The results shown in Table 17 indicated that the indirect (mediated) effect of hope on stigma is 0.000. Also, the indirect (mediated) effect of hope on psychological well-being is –4.147. As well as the in-direct (mediated) effect of religiosity on stigma is 0.000. Results about the indirect (mediated) effect of religiosity on psychological well-being are –.267. That is, due to the indirect (mediated) effect of religiosity on psychological well-being. As well as the indirect (mediated) effect of stigma on well-being is 0.000.
Table 17
The indirect effects (n = 426 - default model)
| Hope | Religiosity | Stigma | PWB | |
| Stigma | 0.000 | 0.000 | 0.000 | 0.000 |
| PWB | –4.147 | –0.267 | 0.000 | 0.000 |
The results on regression in Table 18 indicated that the regression weight for religiosity in the prediction of stigma is not significantly at the 0.05 level (two-tailed). Simultaneously, the regression weight for hope in the prediction of stigma is significantly at the 0.001 level (two-tailed). Also, the regression weight for hope in predicting psychological well-being is significantly at the 0.001 level (two-tailed). The regression weight for religiosity in the prediction of psychological well-being is significantly at the 0.05 level (two-tailed). Findings also revealed that the regression weight for stigma in predicting psychological well-being is significantly at the 0.001 level (two-tailed).
Table 18
The regression weights (n = 426 - default model)
| Estimate | S.E. | C.R. | P | Label | |||
| Stigma | < — | Religiosity | –0.267 | 0.210 | –1.269 | 0.204 | par_7 |
| Stigma | < — | Hope | –4.147 | 0.668 | –6.207 | *** | par_8 |
| Psychological well-being | < — | Hope | 7.236 | 1.136 | 6.370 | *** | par_6 |
| Psychological well-being | < — | Religiosity | 0.807 | 0.368 | 2.191 | 0.028 | par_9 |
| Psychological well-being | < — | Stigma | –0.447 | 0.057 | –7.804 | *** | par_8 |
5Discussion
The current study addresses many significant re-sults about the effect of demographic variables on study variables: religiosity, hope, stigma, psychological well-being. The results showed that there are statistically significant differences due to age in hope and psychological well-being. These differences favor the sample members belonging to the age group from 30 years old and over. In contrast, there are no differences in religiosity and stigma due to age. The findings also indicated that there are no differences due to education level in religiosity, hope, stigma, and psychological well-being. The results also showed statistically significant differences due to social status in psychological well-being in favor of the sample members belonging to the married group. At the same time, there are no differences in religiosity, hope, and stigma. Regarding the effect of income level in the study variables, the current study results showed no differences due to income level in religiosity, hope, stigma, and psychological well-being.
The high level of religiosity of the study sample members increased the level of their hope and psychological well-being, as well as the nature of Saudi religious society, and the preservation of religious rituals such as prayers to God in times of crises or illness. The nature of the community members supporting each other, from providing material support to the needy persons, and psychological support to patients, reduced the negative impact of COVID-19 infection and reduced the stigma related to it.
Moreover, we cannot deny the Kingdom’s efforts in providing patients with health care and financial support to COVID-19 patients and their families to achieve the 2030 vision that aims to the quality of life for the Saudi citizen. Since most of the sample is over 30 years old (n = 379, 89%of the total sample), this higher age group has a higher level of psychological well-being than the individuals less than 30 years old. Married people the highest group in psychological well-being (n = 337, 79.1%of the total sample). Married people have a positive attitude toward life and a high level of psychological well-being. This result can be interpreted by the fact that marital life provides them with social support in crises and distresses, including illness. Also, marriage makes the individual feel psychological stability and social appreciation. It is satisfied with life and providing support to Saudi families from governmental and voluntary institutions, especially in times of crisis and disaster, such as the COVID-19 pandemic.
On the other hand, this study tried to reveal the mediating role that religiosity and hope play in the relationship between the stigma related to COVID-19 and psychological well-being. Structural Equation Modeling was used to investigate, at the same time, the direct and indirect effects between the variables of this study. The final structural model (see Fig. 6) allows for many interpretations. The previous reviews were found that religiosity and hope are strong predictors of the latent psychological well-being. In light of these results, the current study results indicate that religiosity has a direct positive effect on the psychological well-being of patients of COVID-19, which suggests that the greater the individual’s religiosity, the greater his psychological well-being. The results by Yildirim et al. [26] indicated that religiosity was related to higher authoritarianism levels, parental religious attendance, religious orthodoxy, self-righteousness, and intrinsic religiousness.
The results also found that hope also has a direct positive effect on psychological well-being, given that the more a person feels hope, the greater his level of psychological well-being. These findings indicate that religiosity and hope have a positive role in improving the psychological well-being level of individuals who survived the COVID-19 infection. The current study results also revealed that religiosity and hope played an intermediate role between the stigma and psychological well-being among those who survived from COVID-19. Pollner [44] found a high level of stigma among Ebola survivors; stigma increases people’s suffering from the virus.
As Pollner [44] argued, infection and disease are stigmatizing, which may have adverse effects that prevent healing the illness because the stigma is related to fear of social discrimination and shame, which negatively affects the progress of treatment and interventions. Therefore, this resulted in a decrease in patients’ psychological well-being, including COVID-19 patients. There are many studies [23, 24, 28, 34] that emphasized that affection with COVID-19 resulted in social stigma and discriminatory behaviors against COVID-19 patients.
Religiosity is considered as shelters that support individuals in their cope with life stresses. Thus religiosity can decrease negative feelings and increase psychological well-being [10]. Pollner [44] reported that religiosity related positively to psychological well-being. In the same context, Chang et al. [21] indicated that religiosity plays an essential role in psychological well-being through many mechanisms such as specific coping resources, healthy lifestyle, behavior regulation, positive self-perception, and emotions. Levin [28] argued that when the individual feels loved by God, this feeling increases his health and psychological well-being. Quintana [45] found that religion plays a mediator role in the relationship between the stigma of mental illness and mental health. Also, Wagner et al.’s [46] findings revealed that religiosity affects psychological well-being by increasing hope and meaning because religiosity makes personal feelings with happiness, well-being, and satisfaction. Sheretta et al. [22] showed that relationship with God correlated to PWB and found a relationship with God to play a moderator role in racial stigma. Thus a relationship with God is considered a coping mechanism that promotes psychological well-being. Recently, AlEid et al. [14] found that religiosity a statistically significant predictor for breast cancer patients’ psychological well-being.
A review of existing literature found that religiosity related to higher physical and psychological well-being. Studies conducted by [11, 12, 14, 47] found that religiosity plays an important in determining mental health among patients with chronic diseases and the relation between religiosity and health-related outcomes. As well as, [6, 19–21, 25, 27, 32, 48] showed the role that hope play as a predictor of quality of life and positive personality traits of chronic disease patients (such as HIV, cancer).
Also, Yildirim et al. [26] showed the role of hope play to improve mental health during crisis times. [18, 27, 49] found that hope plays a role in buffering anxiety and stress among COVID-19 patients. According to Seligman, hope is one of the components of happiness and psychological well-being; thus, hope is essential for individuals’ psychological well-being. Hope to help them, especially those with chronic diseases (such as COVID-19), moving them toward the future and mobilizing them to cope with stresses related to their illnesses and adapt to life.
6Conclusion
The current study provides another evidence for the relationship between religiosity, the stigma associated with COVID-19, and COVID-19 patients’ psychological well-being. And revealed the mediating role of religiosity and hope with psychological well-being, which indicates several potential strategies to reduce the adverse effects of the stigma associated with COVID-19 and increase the level of psychological well-being among COVID-19 patients.
7Limitations and future directions
This study presents several significant findings that clarify the role of religiousness and hope to alleviate the adverse effects of the stigma associated with COVID-19 on psychological well-being. Although these critical results, the current study has many limitations; one is the participants’ heterogeneity. Most of them were more than 30 years year, and most of them were married. These limitations affected the results of the current study, as the differences in hope and psychological well-being favored these two groups of study sample individuals. Another limitation that our recent study relied on the descriptive design, and therefore it provides a real limited insight into the causal relationships between the variables of the present study. We still need experimental studies. We may also need longitudinal studies to explore changes in religion and hope among COVID-19 patients and investigate the development in their level of psychological well-being during the years following their affection with COVID-19. We also need for intervention studies to detect the causal relationship and to reveal the effect of interventions based on religiosity and hope to reduce the harmful effects of the stigma, and to increase psychological well-being among those COVID-19 patients, according to World Health Organization reports, as an attempt to preserve the mental health of community members and sustainable human development. Therefore, we hope that the current study results will stimulate more future studies in this field, especially intervention studies and longitudinal studies, to better understand the nature of the causal relationships between religiosity, hope, stigma, and psychological well-being.
Author contributions
BA, MA, FF and AA participated in the supervision, guidance of the study, and revision of the paper. BA and MA were responsible for the design, data presentation, manuscript writing, and revision. MA and FF contributed to the study’s conceptualization, oversaw the study design and data collection, and revised the manuscript. NE arranged the funding only. All authors read and approved the final version of the manuscript.
Conflict of interest
None to report.
Acknowledgments
This research was funded by the Deanship of Scientific Research at Princess Nourah bint Abdulrahman University through the Fast-track Research Funding Program.
References
[1] | Arnout B, Al-Dabbagh Z, Al Eid N, Al Eid M, Al-Musaibeh S, Al-Miqtiq M, Al-Zeyad G. The Effects of Corona Virus (COVID-19) Outbreak on the individuals’ Mental Health and the Decision-Makers: A Comparative Epidemiological Study. International Journal of Medical Research & Health Sciences. (2020) ;9: (3):26–47. |
[2] | ArnoutB. COVID-19 Pandemic Crisis: And The New Face Of The World. (2020) . Scholars Press, Germany. |
[3] | Algarni SM, Almalki HA, Al-Raddadi RM. Epidemic and pandemic events preparedness in Ministry of Health hospitals, Jeddah, 2017, A Cross-sectional study. Int J Adv Res. (2017) ;5: (11)590–98. DOI: 10.21474/IJAR01/5806 |
[4] | Khalid I, Khalid TJ, Qabajah MR, Barnard AG, Qushmaq IA. Healthcare Workers Emotions, Perceived Stressors, and Coping Strategies During MERS-CoV Outbreak. Published online ahead of print February 4, 2016, DOI:10.3121/cmr.2016.1303 Rapid Release CM&R: Marshfield Clinic Health System. |
[5] | King B. Rethinking claims of spiritual intelligence: A definition, model, & measure. 2007, Unpublished master’s thesis, Trent University, Peterborough, Ontario, Canada. |
[6] | Arnout B. Hope and self-concept as a predictor of the quality of life of renal failure patients. Journal of the Faculty of Arts, Banha University. (2012) ;30: :567–626. |
[7] | Brohan E, Slade M, Clement S, Thornicroft G. Experiences of mental illness stigma, prejudice, and discrimination: A review of measures. BMC Health Services Research. (2010) ;10: (80):1–12. DOI:10.1186/1472-6963-10-80 |
[8] | Dein D, Loewenthal K, Lewis CA, Pargament KI. COVID-19, mental health, and religion: an agenda for future research. Mental Health, Religion & Culture. (2020) ;23: :1: ,1–9, DOI: 10.1080/13674676.2020.1768725 |
[9] | BjarnasonD. Concept Analysis of Religiosity. Home Health Care Management & Practice. (2007) ;19: (5):350–5. https://doi.org/10.1177/1084822307300883 |
[10] | Chatters LM. Religion and health: public health research and practice. Annu. Rev. Public Health. (2020) ;21: :335–67. |
[11] | Seeman TE, Dubin LF, Seeman M. Religiosity/spirituality and health. A critical review of the evidence for biological pathways. The American Psychologist. (2003) ;58: (1):53–63. |
[12] | Hill TD, Burdette AM, Ellison CG, Musick MA. Religious attendance and the health behaviors of Texas adults. Preventive Medicine. (2006) ;42: (2):309–12. DOI: 10.1016/j |
[13] | Person B, Sy F, Holton K, Govert B, Liang A. the NCID/SARS Community Outreach Team. Fear and Stigma: The Epidemic within the SARS Outbreak. 2004; Emerging Infectious Diseases • www.cdc.gov/eid • 10, 2. |
[14] | Al Eid N, Alqahtani M, Marwa K, Arnout B, Alswailem H, Al Toaimi A. Religiosity, Psychological Resilience, and Mental Health among Breast Cancer Survivors in the Kingdom of Saudi Arabia. Breast Cancer: Basic and Clinical Research. (2020) ;17: :1–13. |
[15] | Arslan G. Psychological maltreatment, emotional and behavioral problems in adolescents: The mediating role of resilience and self-esteem. Child Abuse & Neglect.. (2016) ;52: :200–9. |
[16] | Snyder CR, Harris C, Anderson JR, Holleran SA, Irving LM, Sigmon ST, Harney P. The will and the ways: development and validation of an individual differences measure of hope. Journal of personality and social psychology. (1991) ;60: (4):570. |
[17] | Long KN, Kim ES, Chen Y, Wilson MF, WorthingtonJr, VanderWeele TJ. The role of Hope in subsequent health and PWB for older adults: An outcome-wide longitudinal approach. Global Epidemiology. 2020;100018. |
[18] | Trzebiński J, Cabański M, Czarnecka JZ. Reaction to the COVID-19 pandemic: the influence of meaning in life, life satisfaction, and assumptions on world orderliness and positivity. Journal of Loss and Trauma. (2020) ;1–14. DOI:10.1080/15325024.2020.1765098. |
[19] | Stoyles G, Chadwick A, Caputi P. Purpose in life and PWB: The relationship between purpose in life, hope, coping, and inward sensitivity among first-year university students. Journal of Spirituality in Mental Health. (2015) ;17: (2):119–34. |
[20] | Foote A, Piazza A, Holcomb J, Paul P, Daffin P. Hope, self-esteem, and social support in persons with multiple sclerosis. Journal of Neurosci Nurs. (1990) ;22: (3):155–9. |
[21] | Chang EC. Hope, problem-solving ability, and coping in a college student population: Some implications for theory and practice. Journal of Clinical Psychology.. (1998) ;54: (7):953–62. |
[22] | Sheretta T, Pamela P, Elan C, Nikeea C. Marquisha L. Religiosity and Coping: Racial Stigma and PWB among African American Girls. J Relig Health. (2018) ;57: :1980–95. |
[23] | Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, Rubin GJ. The psychological impact of quarantine and how to reduce it: a rapid review of the evidence. Lancet. (2020) ;395: :912–20. https://doi.org/10.1016/S0140-6736(20)30460-8. |
[24] | Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM. Public responses to the novel coronavirus (2019-nCoV) in Japan: mental health consequences and target populations. Psychiatry and Clinical Neurosciences. (2020) ;74: (4):281–2. 10.1111/pcn.12988 |
[25] | Yadav S. Perceived social support, hope, and quality of life of persons living with HIV/AIDS: a case study from Nepal. Springer Science+Business Media B.V. (2010) . |
[26] | Yildirim M, Arslan G. Exploring the associations between resilience, dispositional hope, subjective PWB, and psychological health among adults during the early stage of COVID-19. 2020; DOI: 10.31234/osf.io/vpu5q |
[27] | Bloch-Atefi A, Day E, O’Neill G, Price-Robertson R, Snell T. (2020). Reflections on psychotherapy and counseling from COVID-19 lockdown. 2020. https://pdf.printfriendly.com/downloads/pdf_1592891227_74a0aeA4.pdf |
[28] | Levin J. God, love, and health: Findings from a clinical study. Review of Religious Research. (2001) ;42: (3):277–93. |
[29] | Pescosolido BA. The public stigma of mental illness: What do we think; what do we know; what can we prove? J Health Soc Behav. (2013) ;54: :1–21. |
[30] | Corrigan PW, Bink AB, Schmidt A, Jones N, Rüsch N. What is the impact of self-stigma? Loss of self-respect and the “why try” effect. J Ment Health. (2016) ;25: :10–5. |
[31] | Giorgi G, Arcangeli G, Ariza-Montes A, Rapisarda V, Mucci N. Work-related stress in the Italian banking population and its association with recovery experience. IJOMEH. (2019) ;32: :255–65. |
[32] | Koenig HG. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry. 2012;1-33. |
[33] | International Labour Organization. Addressing stigma and discrimination in the COVID-19 response: Key lessons from the response to HIV and AIDS. ILO Brief, May. 2020. https://www.ilo.org/wcmsp5/groups/public/—dgreports/-gender/documents/publication/wcms_744799.pdf |
[34] | UNICEF. The social stigma associated with the coronavirus disease (COVID-19): A guide to preventing and addressing social stigma. 2020; UNICEF Geneva. |
[35] | Crandall CS. Multiple stigma and AIDS: Illness stigma and attitudes toward homosexuals and IV drug users in AIDS-related stigmatization. Journal of Community & Applied Social Psychology. (1991) ;1: :165–72. |
[36] | Lee S, Chan LY, Chau AM, Kwok KP, Kleinman A. The experience of SARS-related stigma at Amoy Gardens. Soc Sci Med. (2005) ;61: :2038–46. DOI: 10.1016/j.socscimed.2005.04.010 |
[37] | Markel H. Quarantine!: East European Jewish immigrants and the NewYork City epidemics of 1892. Baltimore: Johns Hopkins University Press, (1977) . |
[38] | James PB, Wardle J, Steel A, Adams J. An assessment of Ebola-related stigma and its association with informal healthcare utilization among Ebola survivors in Sierra Leone: a cross-sectional study. BMC Public Health. (2020) ;20: :182 https://doi.org/10.1186/s12889-020-8279-7 |
[39] | Ramaci T, Barattucci M, Ledda C, Rapisarda V. Social Stigma during COVID-19 and its Impact on HCWs Outcomes. Sustainability. (2020) ;12: :3834. |
[40] | Ramaci T, Pellerone M, Iacolino C. Stress-related diseases: significant influence on the quality of life at workplaces. Eur Proc Soc Behav Sci. (2016) ;8: :29–38. |
[41] | Santarelli L, Rapisarda V, Fago L, Vella F, Ramaci T, Ledda C, Bracci M. The relation between psychosomatic disturbances and job stress in video display unit operators. Work. (2019) ;64: :303–10. |
[42] | Ministry of Health. Daily report, 20-June 2020.KSA. |
[43] | Xiang YT, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, Ng CH. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. (2020) ;4: :30046–8. |
[44] | Pollner M. Divine relations, social relations, and PWB. Journal of Health and Social Behavior. (1989) ;30: (2):92–104. |
[45] | Quintana FJ. The Influence of Religiosity and Stigma on Mental Health Outcomes for an African American and Latino Clinical Sample. 2013; Doctoral Dissertations. 224. https://opencommons.uconn.edu/dissertations/224 |
[46] | Wagner AC, Hart TA, Mc Shane KE, Margoles S, Girard TA. Health care provider attitudes and beliefs about people living with HIV: Initial validation of the health care provider HIV/AIDS Stigma Scale (HPASS). AIDS Behav. (2014) ;18: :2397–408. |
[47] | Phelan J, Link BG, Dovidio JF. Stigma and Prejudice: One Animal or Two? Soc Sci Med. (2008) ;67: :358–67. |
[48] | Tsaousis I, Karademas E, Kalatzi D. The role of core self-evaluations in the relationship between religious involvement and subjective PWB: A moderated mediation model. Mental Health, Religion, & Culture.. (2013) ;16: (2):138–54. |
[49] | Overholt L, Wohl DA, Fischer WAII, Westreich D, Tozay S, Reeves E, et al. Stigma and Ebola survivorship in Liberia: Results from a longitudinal cohort study. PLoS ONE. (2018) ; 13: (11):e0206595. https://doi.org/10.1371/journal.pone.0206595 |


