
Telehealth in school-based practice: Perceived viability to bridge global OT practitioner shortages prior to COVID-19 global health emergency
Abstract
BACKGROUND:
Prior to the COVID-19 global health emergency, telehealth was an emerging occupational therapy (OT) service delivery model possessing many positive attributes. These include the potential to offset well-documented global occupational therapy practitioner (OTP) shortages. However, wide-spread adoption of telehealth as a delivery model in school-based practice is lacking in the OT evidence literature. While the COVID-19 global health emergency propelled many OTPs into the use of telehealth technologies, in some cases with minimal preparation, an investigation was conducted into the likelihood of telehealth adoption when comprehensive training was provided so that appropriateness of student fit for telehealth could be determined and essential planning could take place.
OBJECTIVE:
Prior to the COVID-19 global health emergency, a comprehensive training program was developed incorporating detailed perceptions of OTPs experienced in and new to telehealth in school-based practice as measured via surveys with the goal of increasing adoption of telehealth technologies for the delivery of OT services. Following the completion of the online New to Telehealth Pre-training Survey, OTPs new to telehealth were invited to complete the OT Telehealth Primer: School-based Practice training program. Analysis of pre- and post-training surveys yielded information about attitudinal changes experienced post-training.
METHODS:
Prior to the COVID-19 global health emergency, school-based occupational therapy practitioners (OTP) experienced in telehealth were invited to complete a survey exploring benefits and barriers encountered in the delivery of OT services using telehealth. OTPs new-to-telehealth were invited to complete a different survey intended to explore attitudes about the potential use of telehealth. Data collected from both surveys were used to develop a comprehensive training program, The OT Telehealth Primer for School-based Practice. OTPs new-to-telehealth were invited to complete the training program and a post-training survey. A descriptive data analysis was completed on responses from pre- to post-training surveys and the chi-square test of independence was used to evaluate difference in reported likelihood of adopting telehealth into practice before and after training.
RESULTS:
Prior to the COVID-19 global health emergency, the top benefits identified by the OTP Experienced Telehealth-User Survey included: 1) service access, 2) collaboration and carry-over with team members, 3) efficiency themes, and
4) student engagement and comfort. Top benefits identified by the OTP New to Telehealth Survey identified the same top benefits after participating in the training program. A significant decrease in perceived barriers was noted in scores from pre- to post-training by OTPs new to telehealth. The perceived barriers that did not significantly decrease post-training suggest the need for future education and future protocol development. These included: unreliable internet, lack of hands-on opportunity and e-helpers’ (parent, caregiver or support system available to assist the student in person during a telehealth session) decreased comfort with technology. Of the participants who completed the OT Telehealth Primer: School-based Practice, 80% reported being likely to add telehealth as a delivery model for future OT practice.
CONCLUSIONS:
Prior to the COVID-19 global health emergency, completion of the comprehensive training program OT Telehealth Primer: School-based Practice program yielded improved perceived benefits and an increased likelihood of telehealth adoption into practice by OTPs. However, both OTPs and school administrators require ongoing education for successful widespread adoption to be achieved thus offsetting the global shortage of OTPs and increasing service access. Future research, particularly related to available training and support for the rapid adoption of telehealth technologies during the COVID-19 global health emergency, will yield helpful information about the likelihood of continued use of telehealth in practice.
1Introduction
Occupational therapy practitioners (OTP) are considered related service providers in school-based practice, thus providing support to students with special education needs so that they can access the curriculum [1]. An Individualized Education Plan (IEP) developed by the educational team includes specific mandates for services that will be delivered. However, given the current shortage of OTPs globally [2, 3], difficulty meeting students’ education-related occupational therapy (OT) needs have occurred [4]. This is further problematic as the demand for OT services is anticipated to outpace the OTP availability by 2030 [5]. Telehealth as an OT delivery model offers promise for counterbalancing some of these shortages [6].
Telehealth, which is defined as “the application of evaluative, consultative, preventative, and therapeutic services delivered through telecommunication and information technologies” [7], offers many positive qualities including improved care access, improved access to specialists, improved timing for care, reduced travel, and increased coordination of care and communication [8]. For the students receiving services via telehealth, benefits include improved planning and delivery, increased individualized instruction, and increased learning [9]. While increased adoption of telehealth as a delivery model for OT services can improve issues with OTP shortages and increase access to OT services in underserved areas, there is a gap in available information about the use of telehealth in the school setting by OTPs.
The Diffusion of Innovation (DOI) theory was employed to develop a comprehensive telehealth for school-based practice training program for OTPs. Diffusion of Innovation (DOI) is the process by which innovations are communicated through channels, over time, among members of a social system [10]. Diffusing an innovation can be more complicated than actual development of the innovation. Although change is inevitable, people avoid change primarily because of uncertainty or when clear guidelines are lacking. Therefore, implementation is often done slowly, by trial and error, resulting in resistance, incomplete implementation and failure [10]. Rogers’ theoretical work on DOI resulted in fundamental principles that guide the steps to influence adoption and diffusion. These are: 1) the social system; 2) the innovation (in this case, school-based OT Telehealth); 3) the adopter, or person who will use the innovation; 4) adoption or innovation-decision process, which is a “stage ordered model of knowledge/awareness, persuasion, decision, implementation and continuation” [10], the diffusion system or communication channel which can include mass media or interpersonal, two-way communication channels. The program’s goal was to underscore the key attributes of telehealth such as ease of use, observability, compatibility and trialability in alignment with the DOI theory [10].
1.2Research questions
1. What are the perceived benefits, barriers and needs related to telehealth use, that will positively influence OTPs who have not used telehealth to consider incorporating its use?
2. What are the experienced benefits and barriers of telehealth use according to OTPs who have successfully incorporated its use?
3. Does completion of an evidence-based training program in OT telehealth change perceived barriers, benefits and likelihood of telehealth adoption for OTPs who had not used telehealth prior to participation in the training program?
1.2Secondary research questions
1. What themes emerge regarding benefits and barriers regarding OT telehealth use in school-based practice?
2. What themes emerge regarding additional needs to increase likelihood of OT telehealth adoption?
2Methods
Prior to the onset of the COVID-19 global health emergency, exempt Internal Review Board (IRB) approval was granted by the Boston University Charles River Campus Institutional Review Board. Recruitment and data collection occurred over an eight-week period from March 15, 2019–May 15, 2019. Using surveys as a part of a systematic, mixed method, quasi-experimental, participatory action research design, quantitative and qualitative data was collected. Survey questions were both structured and open-ended. OTPs were recruited from closed OTP social media groups such as Facebook and LinkedIn using both a convenience sampling of practitioners available through those groups as well as snowball sampling when the survey link was shared with other OTPs. Practitioners who were unfamiliar with telehealth were asked to complete the OTP New to Telehealth PreTraining survey exploring perceptions about, familiarity with, and attitudes towards the use of telehealth (N = 176). Using the same recruitment methods, seasoned telehealth-using OTPs were invited to complete a different survey, OTP Experienced Telehealth-User Survey exploring the experienced OT telehealth benefits and challenges (N = 22). OTPs who were new to telehealth were later invited to complete the online educational program about telehealth developed using data from the first two surveys, then complete a post-program survey reflecting information learned. 43 participants completed all 3 components (N = 43). The online educational program, entitled the OT Telehealth Primer: School-based Practice, consisted of five audio-visual training modules and was available to participants via an online platform, Blackboard Coursesites©. Participants were provided with instructions for the creation of a free Blackboard Coursesites© account. The author granted participants access to the program through the online platform. The program modules included definitions of basic terms, licensing, reimbursement and regulatory information, evidence of telehealth’s efficacy, survey results and video interviews with OTPs experienced in the use of telehealth and video clips of actual OT telehealth sessions. All modules incorporated the guiding principles of the Diffusion of Innovation theory.
Survey questions were adapted and expanded with permission from a 2018 survey previously designed and administered by Rortvedt and Jacobs [11]. Participants used a 5-point Likert scale from strongly agree (1) to strongly disagree (5) to describe their likelihood of adopting telehealth into practice. Demographic information was collected including credentials, years of experience, and current practice setting. Open-ended questions exploring participant’s perceptions of benefits and barriers to telehealth use in school-based OT practice were additionally collected. Using QualtricsXM software, phase one collected data from OTP participants who had not used telehealth and from OTPs experienced in telehealth by posting a survey link to closed social media groups. OTP participants inexperienced in telehealth who later completed the online training program, additionally completed a post-training survey, the OTP New to Telehealth Post-Training Survey using QualtricsXM.
Themes described by OTPs experienced in telehealth and those new to telehealth appearing in descriptive responses were categorized to tally frequencies of identified benefits and barriers to prevent expression of too narrowly describing these perceived benefits and barriers. Thematic analysis was applied to identify OTPs’ perceptions of the benefits and barriers to telehealth use. Mention of these themes was tallied for each participant, descriptively summarized, and compared before and after the training. The chi-square test of independence was used to evaluate difference in reported likelihood of adopting telehealth into practice before and after training.
3Results
Prior to the COVID-19 global health emergency, OTP participants experienced in using telehealth technologies (N = 22) highlighted most significant benefits of OT telehealth in school-based practice as: 1) service access, 2) collaboration and carry-over with team members, 3) efficiency themes, and 4) student engagement and comfort; and reported the most significant barriers as: 1) internet instability, 2) decreased opportunity for direct hands on assistance by OTP, 3) technology challenges, 4) unreliability with e-helper, 5) lack of licensure portability (the ability to transfer ones license to another state or have a professional license accepted by another state versus seeking a separate license in each every state in which one practices), and 6) inappropriate referrals.
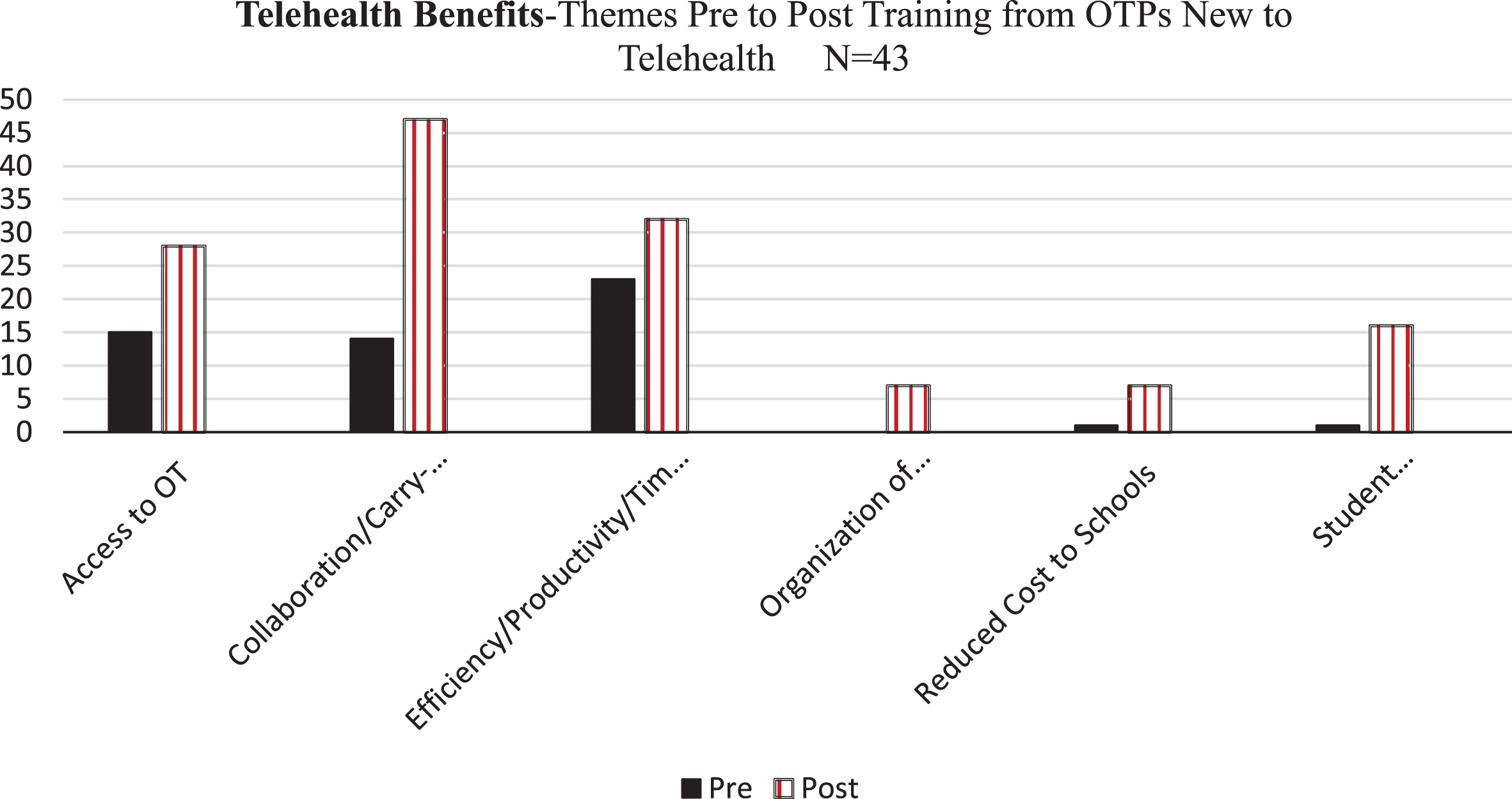
OTPs (N = 176) who were unfamiliar with telehealth completed the initial pre-training survey and collected data was used to develop the OT Telehealth Primer for School-based Practice training program. Prior to completing the training program, participants (N = 43) OTPs identified 54 potential benefits to using telehealth. Post-training, identified potential benefits climbed to 137. Pre-training, the top four benefits reported: 1) service access, 2) collaboration and carry-over with team members, 3) efficiency themes, and 4) student engagement and comfort. Post-training, OTP participants who were new to telehealth (N = 43), reported the same benefits with an increase in the number of times these benefits were mentioned, as described in Fig. 1. Additional benefits from this group were identified and included organization of evidence/documentation and reduced costs to schools. 74% of participants, pre-training, reported that they agreed or strongly agreed with the likelihood of adopting telehealth into future practice. Pre- to post-training benefits are summarized in Fig. 1.
Fig. 1
Reported Perceived Benefits with Telehealth per OTPs New to Telehealth: Pre and Post Training Completion.
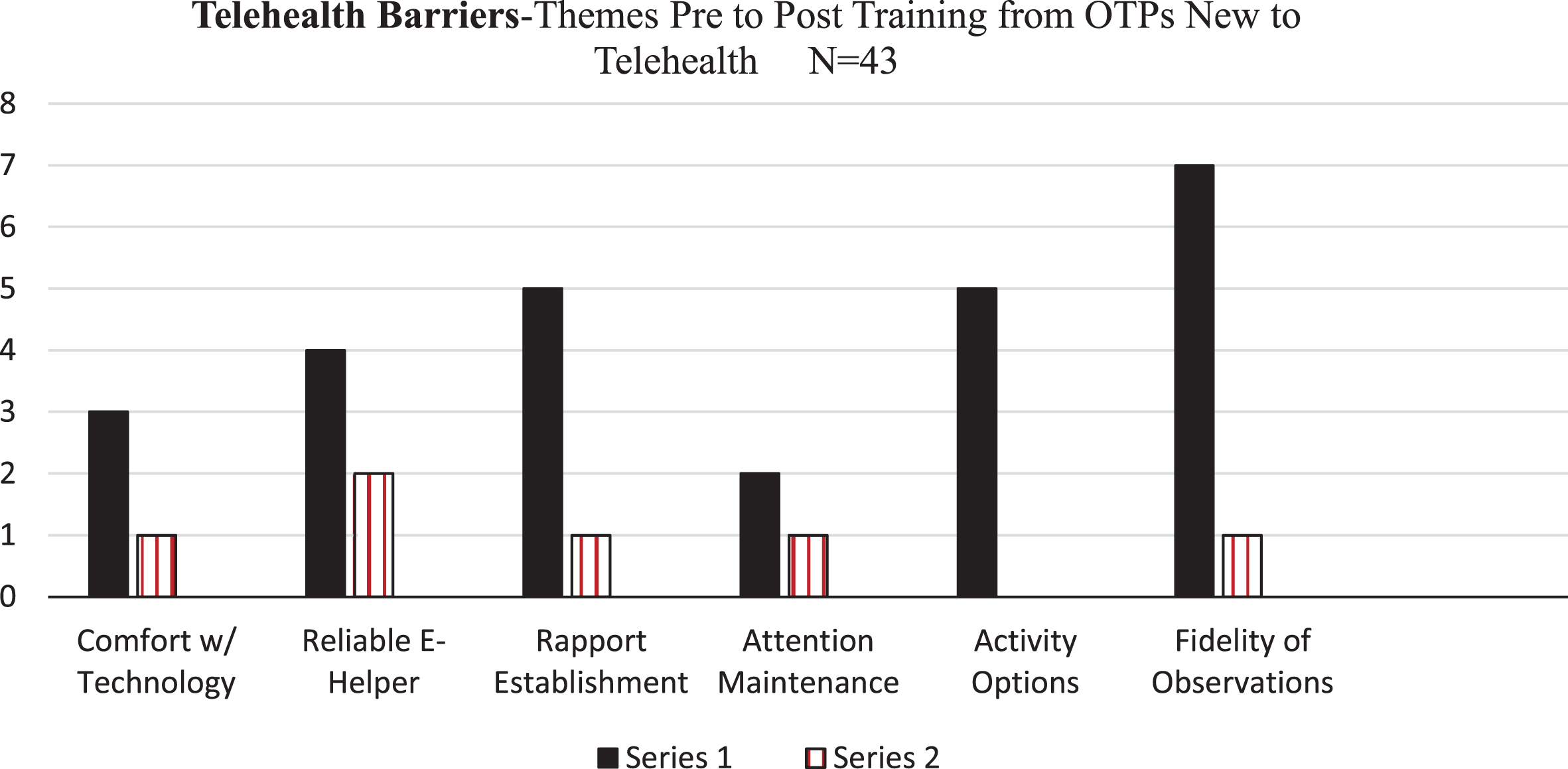
Participants narratively listed perceived barriers to telehealth use in OT in an open-ended format (N = 43). Perceived barriers reported by OTPs new to telehealth revealed two overarching themes: 1) barriers significantly reduced or alleviated by completing the OT Telehealth Primer: School-based Practice, and 2) unchanged or increased barriers after training participation (see Fig. 2). Reported barriers to telehealth use that were significantly reduced or alleviated after completing the training are listed below and summarized in Fig. 2:
• One participant listed comfort with technology as a barrier on the post training survey as compared to three participants on the pre-training survey
• Two participants listed reliability of the e-helper as a barrier on the post training survey as compared to four participants on the pre-training survey
• One participant listed rapport establishment as a barrier on the post training survey as compared to five participants on the pre-training survey
• One participant listed maintaining students’ attention as a barrier on the post-training survey as compared to two participants on the pre-training survey
• No participants listed activity options as a barrier on the post-training survey as compared to five participants on the pre-training survey
• One participant listed fidelity of observations as a barrier on the post training survey as compared to seven participants on the pre-training survey
Fig. 2
Reported Perceived Barriers with Telehealth per OTPs New to TelehealthPre and Post Training Completion: Perceived Barriers That Decreased Post Training.
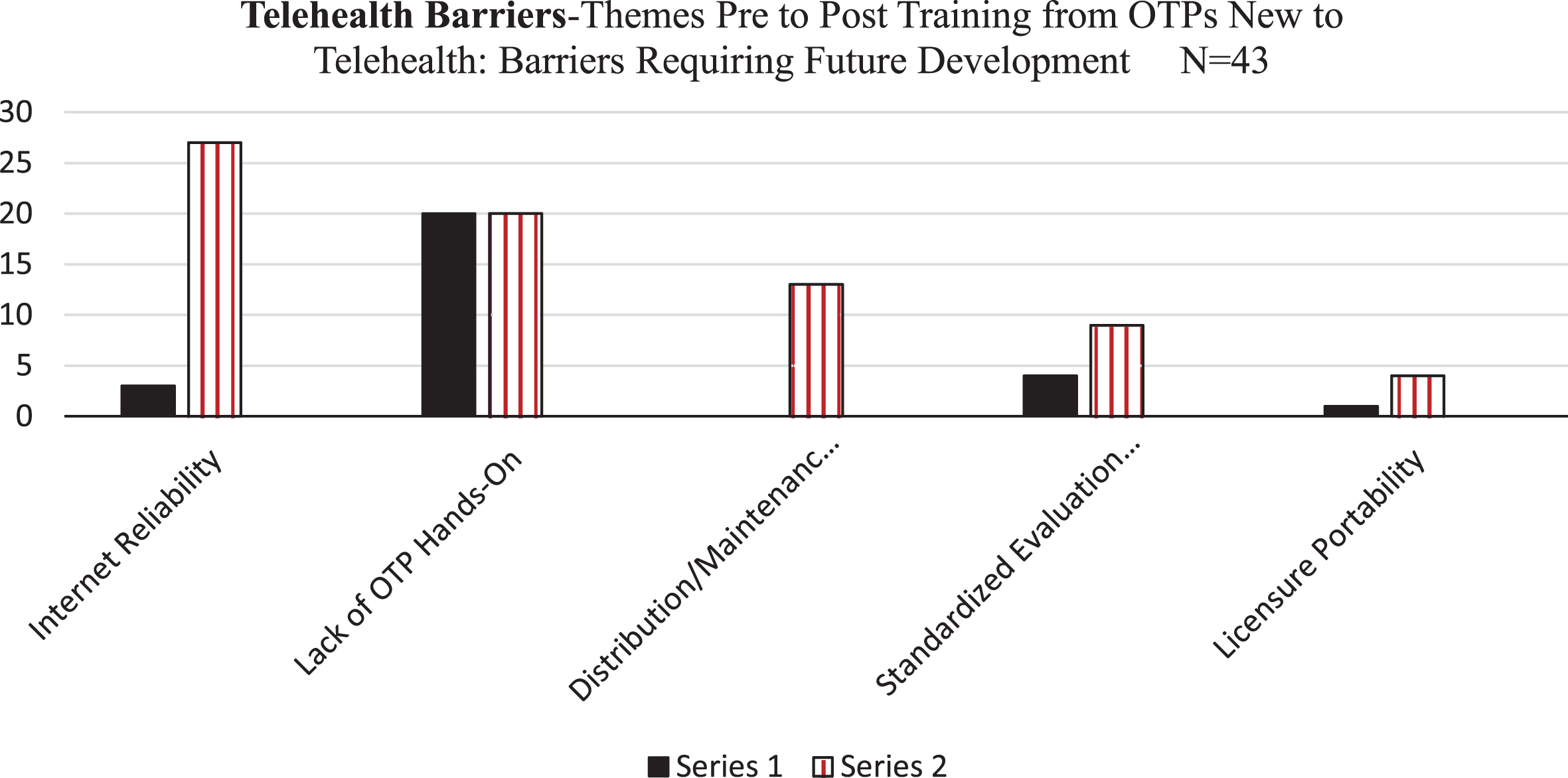
Reported barriers to telehealth use that were not significantly reduced, or increased following training are listed and summarized in Fig. 3:
• Unreliable internet
• OTP inability to use hands-on techniques in intervention
• Decreased familiarity or comfort with technology (family or e-helpers)
Fig. 3
Reported Perceived Barriers with Telehealth per OTPs New to Telehealth: Pre and Post Training Completion: Perceived Barriers Requiring Future Development.
In response to the statement: “I can see myself adding telehealth into practice in the future,” 74% of OTPs New to Telehealth reported they agreed or strongly agreed on the pre-training survey whereas 80% of the 43 participants reported they agreed or strongly agreed with seeing the addition of telehealth into future practice. The proportion of OTPs who reported a strong or very strong intention to use telehealth did not differ between pre-test and post-test, χ2 = 2.54, p = 0.53.
4Discussion
Prior to the onset of the COVID-19 global health emergency, participants completing the OTP Experienced Telehealth-User identified the top four benefits of telehealth use as 1) service access, particularly in instances when services would not otherwise be available (reported by 25% of participants), 2) themes related to improved communication, collaboration, consultation and carry-over of treatment interventions with team members including educators, parents and para-professionals (reported by 25% of participants), 3) themes related to productivity, efficiency, schedule flexibility and reduced travel (reported by 20% of participants), and 4) themes related to increased student engagement, motivation, comfort and privacy (reported by 15% of participants). These new-to-telehealth OTPs identified the same top four benefits after participating in the training program suggesting they possibly accepted the benefits described by experienced OTPs in the OT Telehealth Primer for School-based Practice and/or were convinced of those benefits by seeing actual video clips of real telehealth sessions with students.
OTPs experienced in the use of telehealth, reported the top three barriers to success with telehealth use as 1) internet reliability (reported by 17%), 2) familiarity with and dependability of technology (reported by 17.3%), 3) inability to use hands-on intervention during a telehealth session (reported by 13% of participants). OTPs new to telehealth echoed concern related to internet reliability and technology-familiarity as the top two perceived barriers, but reported time and effort related to distribution and coordination of needed materials as the third top barrier. The absence of specific data on actual time required to do this or experience in doing so likely elevated this concern for inexperienced telehealth users and is a potential area of future research.
OTPs new-to-telehealth responses on the pre- and post-training surveys shed light on the importance of education and addressing gaps in knowledge. These may positively influence the likelihood of adopting telehealth use, with 54 telehealth benefits identified pre-training and 137 benefits described post-training. This idea is further supported by the number of reported barriers described prior to training and the decrease in these reported post-training, which surrounded comfort with technology, establishing a rapport with students, maintaining students’ attention, activity options and fidelity of observations.
Both OTPs experienced in and new to telehealth (on both pre- and post-training surveys) described concerns related to internet reliability both for practitioners and service consumers as a potential barrier suggesting further investigation is needed into whether participants are experienced in back-up options (like mobile hot spots and planning for power outages). Similarly, absence of hands-on intervention during telehealth sessions was a reported barrier at the same frequency by OTPs new to telehealth (n = 20) on the pre-and post-training survey, and by 13% of OTPs experienced in telehealth use. This suggests value in further exploration of use of a coaching model [12] and e-helper, development of succinct cueing methods, and use of modeling or instruction protocols to guide students or e-helpers in supporting interventions during OT telehealth sessions. These surveys did not explicitly explore percentages of time requiring hands-on support, nor the characteristics of a student who would most likely require hands-on cueing or support suggesting that further investigation into these themes is warranted. With a high opening percentage (74%) increasing to a post-training percentage of 80% of OTPs new-to-telehealth participants reporting likelihood of adopting telehealth in the future, there is indication that OTP participants entered the study with an interest and openness to telehealth use. Because this study was completed prior to the rapid adoption of telehealth technologies for OT service delivery during the COVID-19 global health emergency, different results would likely be received after that experience. Additionally, having recruited participants from closed social media sites, suggesting an existing familiarity with current technology, may have contributed to these high percentages. Results from pre-to post-training may be very different if completed with a random sampling of participants recruited in a different way that did not involve technology.
5Limitations
The evaluation of the OT Telehealth Primer: School-based Practice was limited as the pilot time period was eight-weeks. Additionally, a small sample size was achieved of participants (N = 43) who completed all three components: the pre- and post-training survey and the full training program. Results may have varied if calculated for a larger number of participants. However, notable themes in the evaluation outcome indicate areas for future research. Additionally, all participants were recruited using technology and social media platforms. The results may be different if participants are recruited in different ways that do not involve technology.
6Conclusion
This investigation of OTPs’ perceptions of telehealth as a delivery model was completed one year prior to the COVID-19 global pandemic which resulted in rapid adoption of telehealth use out of emergent necessity. Future research will further explore the impact of the rapid adoption of telehealth and its impact on continued use of telehealth. However, well-documented national shortages of OTPs and decreased service access continue to exist in the U.S. and around the globe [13–15]. Telehealth has the potential to offset some service delivery shortages and service access issues. While there is clear evidence on the benefits for OT services delivered via telehealth [16], there is a gap in the evidence literature on this delivery model for school-based OT services. Widespread adoption may be limited by existing perceived barriers. The development of the OT Telehealth Primer: School-based Practice, and completion of the course by OTPs yielded outcomes that suggest a comprehensive training program can influence the likelihood of telehealth being successfully adopted into practice. Adoption of telehealth as a welcomed service delivery option will likely be increased by the dissemination of the post-training program findings on the perceived attributes of this innovative delivery method as well as the ongoing dissemination of information on successful ways to implement telehealth technologies. Increased adoption of telehealth as a supplemental delivery model, has the potential to contribute towards improved availability of OT services and offset OTP shortage issues.
Conflict of interest
None to report.
Acknowledgments
This study was completed as a component of a post-professional doctorate in occupational therapy program at Boston University, Sargent College of Health & Rehabilitation Sciences.
References
[1] | United States Department of Education. (n.d.-b). Sec. 300.34 Related services. Retrieved July 25, 2018, from https://sites.ed.gov/idea/regs/b/a/300.34 |
[2] | Bureau of Labor Statistics. Occupational Outlook Handbook. 2018. Retrieved from https://www.bls.gov/ooh/healthcare/Occupationaltherapists.html |
[3] | World Federation of Occupational Therapy. WFOT Human Resources Project. 2018. Retrieved from: http://www.wfot.org/ResourceCentre.aspx |
[4] | Lehrer B . Follow up: Occupational therapy shortage [Audio podcast]. 2016. Retrieved from: https://www.wnyc.org/story/followingoccupational-therapist-shortage/ |
[5] | Lin V , Zhang X , Dixon P . Occupational therapy workforce in the United States: Forecasting nationwide shortages. PM&R. (2015) ;7: (9):946–54. |
[6] | Hersch G , Kao B , Melton L , Pancheri K . Telehealth usage by occupational therapy practitioners. Am J Occup Ther. (2015) ;69: :6911510038p. 1. doi: 10.5014/ajot.2015.69s1-po1095 |
[7] | American Occupational Therapy Association. Telehealth in occupational therapy. Am J Occup Ther. (2018) ;72: :1–18. Doi: 10.5014/ajot.2018.72S219 |
[8] | Cason J . Telehealth and occupational therapy: Integral to the triple aim of health care reform. Am J Occup Ther. (2015) ;69: (2):1–8. doi: 10.5014/ajot.2015.692003 |
[9] | Tucker J . Perspectives of speech-language pathologists on the use of tele-practice in schools: The Qualitative view. International Journal of Tele-rehabilitation.. (2012) ;4: (2):47–60. |
[10] | Rogers E . Diffusion of innovations, 3rd ed. New York, London: Free Press; Collier Macmillan, (1983) . |
[11] | Rortvedt D , JacobsK. Perspectives on the use of a telehealth service-delivery model as a component of school-based occupational therapy practice: Designing a user-experience. Work. (2019) ;62: :125–31. doi: 10.3233/WOR-182847 |
[12] | Little L , Pope E , Wallisch A , Dunn W . Occupation-based coaching by means of telehealth for families of young children with Autism Spectrum Disorder. Am J Occup Ther. (2018) ;72: (2):7202205020p1–7202205020p7. doi:10.5014/ajot.2018.024786. |
[13] | American Association for Employment in Education. Educator supply and demand report 2016–2017: Executive summary. 2016. Retrieved from: https://www.aaee.org/resources/ |
[14] | Bureau of Labor Statistics. Occupational Outlook Handbook. 2018. Retrieved from https://www.bls.gov/ooh/healthcare/Occupationaltherapists.html |
[15] | World Federation of Occupational Therapy. WFOT Human Resources Project. 2018. Retrieved from: http://www.wfot.org/ResourceCentre.aspx |
[16] | Cason J . Telehealth and occupational therapy: Integral to the triple aim of health care reform. Am J Occup Ther. (2015) ;69: (2):1–8. doi: 10.5014/ajot.2015.692003. |


