
Long-term employment status and quality of life after cancer: A longitudinal prospective cohort study from diagnosis up to and including 5 years post diagnosis
Abstract
BACKGROUND:
Accumulating evidence suggests that cancer survivors are able to return to work. However, little is known about their work situation 5 years after diagnosis.
OBJECTIVE:
To explore fluctuations in employment status and its association with quality of life 2, 3, and 5 years after cancer diagnosis of 65 cancer survivors employed at diagnosis.
METHODS:
In association with a randomised controlled trial (RCT), questionnaires were administrated to eligible cancer survivors at diagnosis, 2, 3, and 5 years thereafter comprising of validated questionnaires related to work (i.e. Work Ability Index (WAI), cancer, and quality of life (QOL) (i.e. SF-36, VAS QOL). The RCT studied a hospital-based work support intervention in female breast and gynaecological cancer survivors who were treated with curative intent and had paid work at diagnosis. Descriptive statistics and longitudinal multi-level analysis were employed.
RESULTS:
Sixty-five of the 102 eligible cancer survivors participated, who were primarily diagnosed with breast cancer (63%). Two and 5 years after cancer diagnosis respectively 63 (97%) and 48 (81%) participants were employed. Reasons for not being employed after 5 years included receiving unemployment benefits (7%), voluntary unemployment (3%), receiving disability benefits (3%), and early retirement (3%). Longitudinal multi-level analysis showed that employed cancer survivors reported in general statistically significant better quality of life outcomes at 5 years follow-up compared to those not being employed.
CONCLUSIONS:
We found high employment rates and few fluctuations in employment status. The steepest decline in employment rate occurs after the first two years of diagnosis. Employed participants reported better quality of life outcomes. Survivorship care should therefore focus on the population at risk possibly within the first two years after diagnosis.
1Introduction
Globally, the number of people living beyond a cancer diagnosis has increased over the past decades and is expected to continue to increase [1]. The late effects of cancer treatment will therefore become more significant. One of these problems, the impact of cancer on work, has been identified as a research gap in the scientific literature [2]. However, it is known that work is of importance to cancer survivors [3, 4]. Previously, many benefits of paid work have been reported by cancer survivors such as identity, distraction, self-esteem, return to daily activities, social support and provision of a much needed income [5].
Unfortunately, cancer survivors experience difficulties in returning to work [6] or while at work [7, 8]. Previous studies have identified various factors that can both impede or facilitate the return to work process (e.g. fatigue) [9] as well as various stakeholders that might hamper or enhance the return to work process (e.g. the employer) [10, 11].
Most research in this area has focused on the first one or two years after diagnosis [12]. As we know that 5 years after diagnosis, cancer survivors experience higher levels of fatigue compared to the general population [13] and that this may hamper the possibility to stay employed [14], it might be hypothesised that fluctuations in employment status may occur after the first two years and are therefore of added value to investigate.
The objectives of our study are therefore to explore the employment status, fluctuations in employment status, and the association between employment status and quality of life 2, 3, and 5 years after diagnosis of cancer survivors who were employed at diagnosis.
2Method
In this study we used a prospective cohort design with four measurements: baseline, 2, 3, and 5 years follow-up. Data were collected from April 2009 until January 2016. Participating in the randomised controlled trial was approved by the medical ethics committee of the Academic Medical Center [MEC 08/267]. All participants signed informed consent forms before participation.
2.1Setting
This prospective cohort study was conducted, alongside a multi-centre randomize controlled trial studying the effectiveness of a hospital-based work support intervention [15]. As we did not find any statistical significant differences between groups regarding work outcomes and quality of life outcomes [16], we decided to consider both groups as one cohort.
All data were collected by means of self-administrated questionnaires. At baseline, 2, 3, and the 5-year follow-up, participants completed validated questionnaires related to work, cancer, and quality of life.
2.2Participants
Eligible criteria for inclusion into the randomised controlled trial were: 1) being a cancer patient between 18 and 60 years of age, 2) treated with curative intent at one of the participating hospital departments, 3) having paid work, and 4) being on sick leave. Patients were excluded who were not sufficiently able to speak, read, or write Dutch, had a severe mental disorder or other severe co-morbidity, and for whom the primary diagnosis of cancer had been made more than two months previously. Additional eligible criteria for participation in this prospective cohort study were: 1) completing the randomised controlled trial, 2) giving consent to be contacted for potentially participation in further research, and 3) not receiving palliative treatment.
Eligible criteria for the randomised controlled trial were checked by the treating physician or nurse at the participating hospitals. One of the researchers checked the additional eligibility criteria for participation in this prospective cohort study after the end of the randomised controlled trial.
2.3Variables
2.3.1Descriptive variables
Demographic (e.g. age), health-related (e.g. quality of life), and work-related variables (e.g. type of employment contract, work ability index (WAI) [17] were included in the questionnaire at baseline (Tables 1 and 2). The reliability of the WAI is considered to be satisfactory [18].
Table 1
Baseline characteristics
| Patient characteristics | Responders | Non-responders |
| (N = 65) | (N = 37) | |
| Socio-demographic characteristics* | ||
| Age (years) | 46.9±7.5 | 48.0±8.6 |
| Gender (N (%) female) | 64 (99) | 37 (100) |
| Marital status (N (%) married or living with partner) | 54 (83) | 24 (65) |
| Breadwinner position (N (%) sole or shared) | 44 (69) | 27 (73) |
| Education level (N (%)) | ||
| Low | 6 (9) | 5 (14) |
| Intermediate | 37 (58) | 18 (49) |
| High | 21 (33) | 14 (38) |
| Cancer-related characteristics | ||
| Diagnosis (N (%)) | ||
| Breast cancer | 40 (62) | 24 (65) |
| Cervix cancer | 16 (25) | 7 (19) |
| Ovarian cancer | 4 (6) | 4 (11) |
| Vulva cancer | 3 (5) | 1 (3) |
| Other | 2 (3) | 1 (3) |
| Number of co-morbidities (N (%)) | ||
| 0 | 36 (55) | 20 (54) |
| ≥1 | 29 (45) | 17 (46) |
| Surgery (N (%) yes) | 54 (83) | 30 (81) |
| Chemotherapy (N (%) yes) | 35 (54) | 24 (65) |
| Radiotherapy (N (%) yes) | 45 (29) | 21 (57) |
| Hormone treatment (N (%) yes) | 22 (34) | 16 (43) |
| Work-related characteristics | ||
| Type of work (N (%) mainly physically work) | 25 (39) | 10 (27) |
| Type of contract (N (%)) | ||
| Permanent | 58 (89) | 32 (87) |
| Temporary | 5 (8) | 3 (8) |
| Self-employed | 0 | 2 (5) |
| Other | 2 (3) | 0 |
| Fatigue (MFI)** General fatigue (0–20) | 12.5±4.8 | 12.9±4.7 |
| Depression (CES-D)** Sum score (0–60) | 12.9±8.5 | 12.9±8.3 |
| Overall Quality of life (VAS-scale) (0–100) | 63.0±18.5 | 60.4±23.9 |
Table 2
Overall quality of life between those reported being employed and not being employed 5 years after cancer diagnosis
| Group at 5 year follow-up | Baseline | 1 year | 2 years | 3 years | 5 years | P -value ** | ||
| Quality of life* (SF-36) (0–100) | Physical functioning | Employed | 80.0±3.3 | 82.2±2.3 | 86.1±2.1 | 83.1±2.7 | 85.3±3.0 | <0.001 |
| Not employed | 81.4±6.8 | 73.6±4.7 | 74.2±4.2 | 69.5±5.7 | 65.9±6.2 | |||
| (N = 59) | Role-physical | Employed | 54.2±6.3 | 55.3±5.9 | 79.2±5.8 | 70.3±6.1 | 77.1±5.8 | 0.002 |
| Not employed | 59.1±13.1 | 36.4±12.2 | 52.3±11.3 | 52.3±12.8 | 40.9±11.9 | |||
| Vitality | Employed | 59.1±2.8 | 57.2±2.6 | 61.9±2.7 | 60.7±2.9 | 61.7±2.8 | 0.257 | |
| Not employed | 65.5±5.9 | 53.2±5.3 | 55.9±5.3 | 56.8±6.0 | 53.2±5.9 | |||
| General health | Employed | 63.2±2.3 | 66.5±2.5 | 70.1±2.8 | 66.7±2.7 | 66.6±3.1 | 0.025 | |
| Not employed | 65.5±4.8 | 69.5±5.2 | 55.9±5.5 | 54.5±5.7 | 56.3±6.5 | |||
| Social functioning | Employed | 71.1±3.3 | 80.3±2.6 | 84.5±2.9 | 78.4±3.1 | 80.3±3.2 | 0.028 | |
| Not employed | 79.5±6.9 | 67.0±5.5 | 79.5±5.7 | 64.8±6.6 | 69.3±6.6 | |||
| Role-emotional | Employed | 47.2±6.3 | 70.3±5.7 | 77.0±5.8 | 77.8±5.8 | 80.1±5.7 | 0.749 | |
| Not employed | 72.7±13.1 | 75.8±11.7 | 69.7±11.4 | 66.7±12.8 | 77.3±11.7 | |||
| Mental health | Employed | 63.8±2.3 | 74.4±2.2 | 78.1±2.3 | 76.4±2.5 | 77.3±2.4 | 0.061 | |
| Not employed | 66.2±4.8 | 71.3±4.6 | 66.2±4.6 | 71.6±5.2 | 72.0±4.9 | |||
| Pain | Employed | 71.1±4.1 | 77.2±2.8 | 81.6±3.1 | 77.0±3.4 | 76.2±3.7 | 0.003 | |
| Not employed | 67.2±8.6 | 69.4±5.7 | 667.0±6.0 | 64.0±7.1 | 62.5±7.7 | |||
| Quality of life* | Employed | 63.5±2.7 | 70.4±2.5 | 73.7±2.9 | 73.3±2.5 | 76.1±2.3 | 0.003 | |
| VAS (0–100) (N = 59) | Not employed | 66.3±5.6 | 69.5±5.0 | 56.5±5.7 | 65.9±5.2 | 59.6±4.9 | ||
| Work Ability Index (WAI) (0–10) (N = 59) | Employed | 6.0±0.4 | 6.9±0.3 | 7.9±0.3 | 7.6±0.3 | 7.6±0.2 | <0.001 | |
| Not employed | 6.1±0.9 | 5.9±0.5 | 6.2±0.5 | 5.9±0.6 | 6.2±0.5 | |||
| Physical subscale (0–5) | Employed | 3.7±0.1 | 3.7±0.1 | 4.0±0.1 | 3.8±0.1 | 3.8±0.1 | <0.001 | |
| Not employed | 3.5±0.3 | 3.2±0.2 | 3.2±0.2 | 3.2±0.3 | 3.2±0.3 | |||
| Mental subscale (0–5) | Employed | 3.2±0.1 | 3.6±0.1 | 3.9±0.1 | 3.9±0.1 | 3.9±0.1 | 0.301 | |
| Not employed | 3.9±0.3 | 3.5±0.2 | 3.5±0.2 | 3.4±0.3 | 3.4±0.3 |
Mean±standard error; *Higher scores represent a higher level of functioning/well-being/quality of life and less pain. **P-value represents the effect of group.
2.3.2Employment outcomes
Employment status was measured with an extensive question indicating whether someone was employed or not employed. We considered someone employed for cases in which someone was: employed, employed but on sick-leave, or self-employed. We considered someone not employed for cases in which someone: received disability pension, received unemployment benefits, was voluntarily unemployed, did volunteer work, was retired, or received training.
We considered a fluctuation in employment status when a participant went from being employed to not being employed, or vice versa, or when a participant went from one reason for not being employed to another (e.g. from unemployment benefits to disability pension).
2.4Statistical analysis
To describe the population, their employment status, and fluctuations in employment status, we used descriptive statistics.
When comparing responders with non-responders on baseline characteristics, a chi-square test was used in the case of a categorical variable and Student’s t-test in the case of continuous variables. The significance level for these tests was ≤0.01. Differences in quality of life outcomes were assessed at all measurement points between those being employed and not being employed 5 years after cancer diagnosis using longitudinal multi-level analysis. All statistical analyses were performed with IBM SPSS Statistics version 20 [22].
3Results
3.1Participants
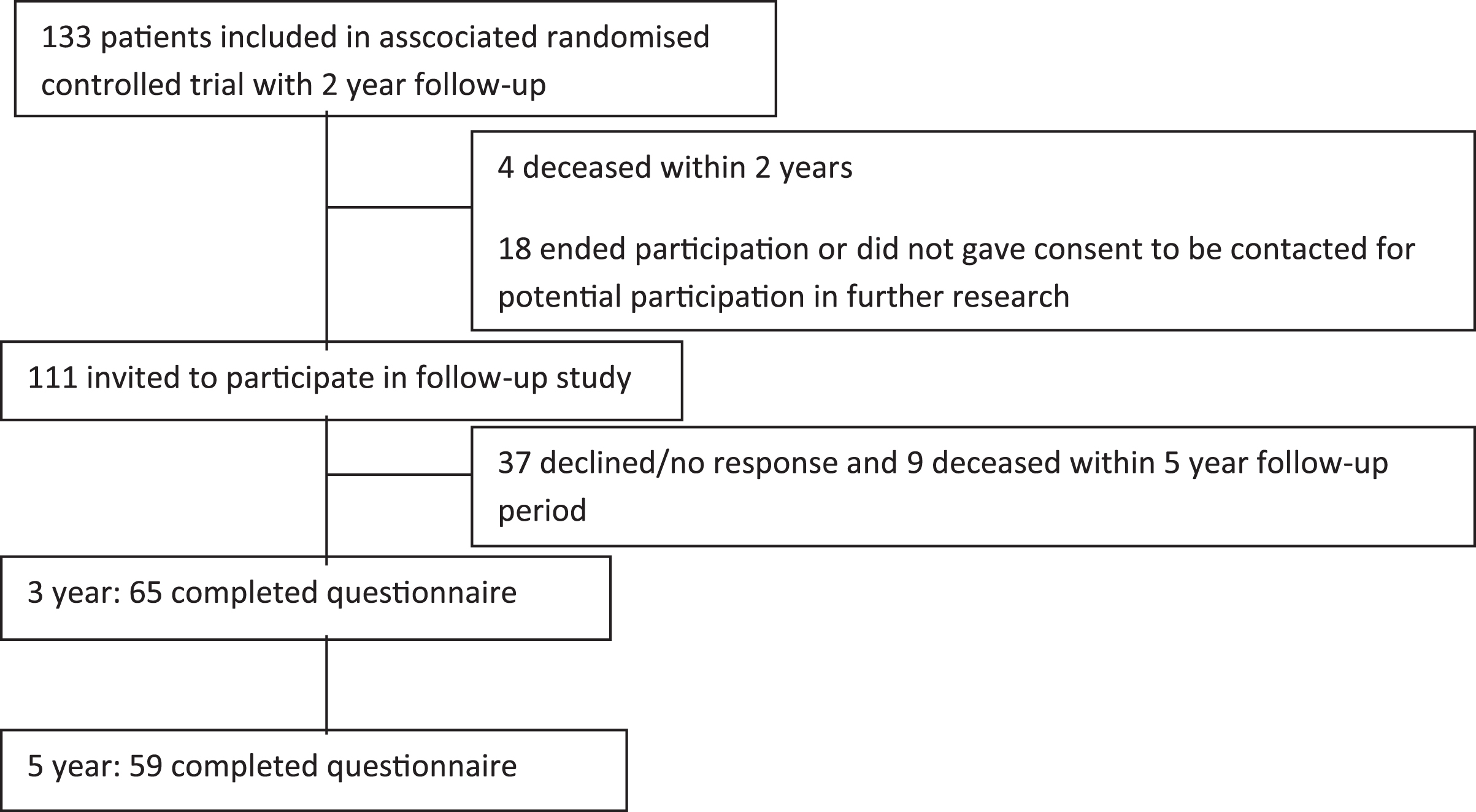
Of the 133 participants who were included in the associated randomised controlled trial [15], 65 were included in this prospective cohort study, excluding those who deceased during the follow-up period or were not able to invite to participate (Fig. 1). Reasons for not participating were: 13 deceased within 5 years of follow-up, 18 ended participation during the first two years of the randomised controlled trial or did not gave consent to be contacted for potentially participation in further research, and 37 declined or gave no response to the invitation to participate in this prospective cohort study.
Fig. 1
Flowchart of the study.
3.2Descriptive data
No statistically significant differences between responders and non-responders were found on any of the descriptive variables (Table 1). Cancer diagnoses included breast cancer (62.7%), cervical cancer (22.5%), cancer of the ovaries (7.8%) or vulva (3.9%), and other (2.9%).
3.3Employment status and fluctuations in employment status
During the first two years after diagnosis, 63 (97%) participants were employed, this percentage declined to 59 (92%) and 48 (81%) after 3 and 5 years respectively. Reasons for not being employed included disability pension 2 (3%), unemployment 2 (3%), and voluntarily unemployed 1 (2%) at 3 years follow-up and unemployment 4 (7%), disability 2 (3 %), voluntarily unemployed 2 (3%) and retirement 2 (3 %) at 5 years follow-up.
Fifty-eight participants provided complete work-status information during all follow-up measurements. For this group 3 patterns of employment over time were observed. A total of 81% of the participants were employed at all-time points, while 12% and 5% moved from employed to unemployed after 5 and 3 years respectively, and 2% stayed unemployed during 2 to 5 years.
3.4Quality of life
When comparing participants being employed at 5 years follow-up with participants not being employed we found that those being employed reported better quality of life on: overall quality of life, physical functioning, role-physical, and pain (Table 2). We found no interaction effect of being employed and time, or on improvement over time.
4Discussion and conclusion
Our finding that employed cancer survivors 5 years after diagnosis had better quality of life outcomes compared to those not being employed support the importance of work for cancer survivors. The finding that employed cancer survivors have better quality of life outcomes 5 years after diagnosis, is in line with Timperi et al. (2013) [23] who employed a 2–8 months follow-up period, Mehnert and Koch, 2013 [24] who employed a 1 year follow-up period after rehabilitation, and Duijts et al. (2017) [12], who employed a 4 year follow-up period after cancer diagnosis. Although we employed a prospective cohort study, the direction of the relationship between quality of life and employment might be many-sided as being employed may enhance quality of life but a certain level of quality of life (e.g. physical functioning) may be needed to be able to work. The first side is supported by Duijts et al. (2017) [12] who found that those experiencing a negative change in employment had worst quality of life outcomes compared to the continuously working cancer survivors. They furthermore found in their final model that quality of life measured at baseline was not statistically significant associated with employment one year later [12]. Additionally, this side is supported by the finding of Mehnert and Koch who found an association between quality of life and job satisfaction [24]. In contrast, our finding that the largest differences between employed and not employed cancer survivors were found for the SF-36 subscales physical functioning, role-physical and pain may suggest that a decline in health may have triggered changes in employment status. To be able to disentangle the relationship between quality of life and employment we therefore recommend for further research to collect data on quality of life and employment status on a very regular basis with a long follow-up period.
Our finding that the overall work ability and physical work ability of the WAI differs between employed and not employed cancer survivors but that these groups did not differ in mental work ability is in line with previous research [12]. This finding may support the need of a certain level of (self-assessed) physical functioning to be able to remain employed.
As we found a high percentage of the cancer survivors being employed, interventions supporting work outcomes should only be targeted at the population at risk. The timing of such an intervention based on our results might possible be during the first 2 years after cancer diagnosis as the major part of those having employment after two years stayed employed. The setting of such an intervention may be best as part of survivorship care as most patients have regular follow-up meetings with their specialised nurse or doctor at the hospital and work-related advice by health care professionals is associated with work outcomes [25]. Additionally, such an intervention should take into account cancer survivors who voluntarily wish to stop working.
Most likely, a selective population of cancer survivors able and willing to participate participated in our study. This assumption is supported by our finding of a comparatively high percentage of cancer survivors being employed 5 years after cancer diagnosis as compared to rates reported more often in the literature [26]. It is furthermore supported by our finding of three employment patterns while Duijts et al. [12] reported a fourth pattern consisting of cancer survivors who went from unemployment to employment. This selective population can be considered a major limitation of our study hampering the generalisability of our results to all cancer survivors 5 years after cancer diagnosis. Additionally, our small sample size limited the statistical strength of our analysis leading to more uncertainty in the results. For further research either using register-based data or specifically involving the population at risk in research could tackle this problem.
We found high employment rates and few fluctuations in employment status. Employed participants reported better quality of life outcomes. Survivorship care should therefore focus on the population at risk possibly within the first two years after diagnosis.
Conflict of interest
None to report.
Ethics approval and consent to participate
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. This work was supported by COST Action IS1211 CANWON (A.G.E.M. de Boer & S.J. Tamminga).
References
[1] | Ferlay J , Soerjomataram I , Dikshit R , Eser S , Mathers C , Rebelo M , et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer. (2015) ;136: (5):E359–86. |
[2] | Brearley SG , Stamataki Z , Addington-Hall J , Foster C , Hodges L , Jarrett N , et al. The physical and practical problems experienced by cancer survivors: a rapid review and synthesis of the literature. Eur J Oncol Nurs. (2011) ;15: (3):204–12. |
[3] | Amir Z , Neary D , Luker K . Cancer survivors’ views of work 3 years post diagnosis: a UK perspective. Eur J Oncol Nurs. (2008) ;12: (3):190–7. |
[4] | Sun W , Chen K , Terhaar A , Wiegmann DA , Heidrich SM , Tevaarwerk AJ , et al. Work-related barriers, facilitators, and strategies of breast cancer survivors working during curative treatment. Work. (2016) ;55: (4):783–95. |
[5] | Wells M , Williams B , Firnigl D , Lang H , Coyle J , Kroll T , et al. Supporting ‘work-related goals’ rather than ‘return to work’ after cancer? A systematic review and meta-synthesis of 25 qualitative studies. Psycho-oncology. (2013) ;22: (6):1208–19. |
[6] | Wells M , Amir Z , Cox T , Eva G , Greenfield D , Hubbard G , et al. Time to act: the challenges of working during and after cancer, initiatives in research and practice. Eur J Oncol Nurs. (2014) ;18: (1):1–2. |
[7] | Bartolo A , Andrade A , Silva D , Monteiro S . Psychosocial risks at the workplace and quality of life in cancer survivors in employment. Psycho-oncology. (2018) ;27: (4):1347–9. |
[8] | Dorland HF , Abma FI , Van Zon SKR , Stewart RE , Amick BC , Ranchor AV , et al. Fatigue and depressive symptoms improve but remain negatively related to work functioning over 18 months after return to work in cancer patients. J Cancer Surviv. (2018) ;12: (3):371–8. |
[9] | Wolvers MDJ , Leensen MCJ , Groeneveld IF , Frings-Dresen MHW , De Boer A . Predictors for earlier return to work of cancer patients. J Cancer Surviv. (2018) ;12: (2):169–77. |
[10] | Greidanus MA , de Boer A , de Rijk AE , Tiedtke CM , Dierckx de Casterle B , Frings-Dresen MHW , et al. Perceived employer-related barriers and facilitators for work participation of cancer survivors: A systematic review of employers’ and survivors’ perspectives. Psychooncology. (2018) ;27: (3):725–733. d |
[11] | Yagil D , Goldblatt H , Cohen M . Dyadic resources in the return to work of cancer survivors: exploring supervisor-employee perspectives. Disability and Rehabilitation. 2018:1-8. |
[12] | Duijts SF , Kieffer JM , van Muijen P , van der Beek AJ . Sustained employability and health-related quality of life in cancer survivors up to four years after diagnosis. Acta oncologica. (2017) ;56: (2):174–82. |
[13] | Oerlemans S , Mols F , Issa DE , Pruijt JH , Peters WG , Lybeert M , et al. A high level of fatigue among long-term survivors of non-Hodgkin’s lymphoma: results from the longitudinal population-based PROFILES registry in the south of the Netherlands. Haematologica. (2013) ;98: (3):479–86. |
[14] | van Muijen P , Weevers NL , Snels IA , Duijts SF , Bruinvels DJ , Schellart AJ , et al. Predictors of return to work and employment in cancer survivors: a systematic review. Eur J Cancer Care (Engl). (2013) ;22: (2):144–60. |
[15] | Tamminga SJ , de Boer AG , Verbeek JH , Taskila T , Frings-Dresen MH . Enhancing return-to-work in cancer patients, development of an intervention and design of a randomised controlled trial. BMC Cancer. (2010) ;10: :345. |
[16] | Tamminga SJ , Verbeek JH , Bos MM , Fons G , Kitzen JJ , Plaisier PW , et al. Effectiveness of a hospital-based work support intervention for female cancer patients - a multi-centre randomised controlled trial. PloS One. (2013) ;8: (5):e63271. |
[17] | Ilmarinen J , Tuomi K . Work ability of aging workers. Scand J Work Environ Health. (1992) ;18: (Suppl 2):8–10. |
[18] | de Zwart BC , Frings-Dresen MH , van Duivenbooden JC . Test-retest reliability of the Work Ability Index questionnaire. Occup Med. (2002) ;52: (4):177–81. |
[19] | Aaronson NK , Muller M , Cohen PD , Essink-Bot ML , Fekkes M , Sanderman R , et al. Translation, validation, and norming of the Dutch language version of the SF-36 Health Survey in community and chronic disease populations. J Clin Epidemiol. (1998) ;51: (11):1055–68. |
[20] | de Boer AG , van Lanschot JJ , Stalmeier PF , van Sandick JW , Hulscher JB , de Haes JC , et al. Is a single-item visual analogue scale as valid, reliable and responsive as multi-item scales in measuring quality of life? QualLife Res. (2004) ;13: (2):311–20. |
[21] | Treanor C , Donnelly M . A methodological review of the Short Form Health Survey 36 (SF-36) and its derivatives among breast cancer survivors. Quality of life research: an international journal of quality of life aspects of treatment, care and rehabilitation. (2015) ;24: (2):339–62. |
[22] | SPSS software. IBM, USA. 2016. |
[23] | Timperi AW , Ergas IJ , Rehkopf DH , Roh JM , Kwan ML , Kushi LH . Employment status and quality of life in recently diagnosed breast cancer survivors. Psycho-oncology. (2013) ;22: (6):1411–20. |
[24] | Mehnert A , Koch U . Work satisfaction and quality of life in cancer survivors in the first year after oncological rehabilitation. Work. (2013) ;46: (4):407–15. |
[25] | Pryce J , Munir F , Haslam C . Cancer survivorship and work: symptoms, supervisor response, co-worker disclosure and work adjustment. J Occup Rehabil. (2007) ;17: (1):83–92. |
[26] | Roelen CA , Koopmans PC , Groothoff JW , van der Klink JJ , Bultmann U . Return to work after cancer diagnosed in 2002, 2005 and 2008. J Occup Rehabil. (2011) ;21: (3):335–41. |
[27] | Smets EM , Garssen B , Bonke B , de Haes JC . The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. (1995) ;39: (3):315–25. |
[28] | Radloff LS . The CES-D Scale, a self-report depression scale for research in the general population. Appl Psych Meas. (1977) ;3: :385–401. |


