
Inclusion of family members without ME/CFS in research studies promotes discovery of biomarkers specific for ME/CFS
Abstract
BACKGROUND:
The search for a biomarker specific for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) has been long, arduous and, to date, unsuccessful. Researchers need to consider their expenditures on each new candidate biomarker. In a previous study of antibody-dependent cell-mediated cytotoxicity (ADCC) by natural killer lymphocytes, we found lower ADCC for ME/CFS patients vs. unrelated donors but ruled against low ADCC as a biomarker because of similar ADCC for patients vs. their family members without ME/CFS.
OBJECTIVE:
We applied inclusion of family members without ME/CFS, from families with multiple CFS patients, as a second non-ME/CFS control group in order to re-examine inflammation in ME/CFS.
METHOD:
Total and CD16A-positive ‘non-classical’ anti-inflammatory monocytes were monitored.
RESULTS:
Non-classical monocytes were elevated for patients vs. unrelated healthy donors but these differences were insignificant between patients vs. unaffected family members.
CONCLUSIONS:
Inclusion of family members ruled against biomarker considerations for the monocytes characterized. These pilot findings for the non-classical monocytes are novel in the field of ME/CFS. We recommend that occupational therapists advocate and explain to family members without ME/CFS the need for the family members’ participation as a second set of controls in pilot studies to rapidly eliminate false biomarkers, optimize patient participation, and save researchers’ labor.
Abbreviations
ADCC | antibody-dependent cell-mediated cytotoxicity |
CD16A | cluster of differentiation protein 16A, the IgG Fc-receptor of monocytes and NK cells |
CFS | Chronic Fatigue Syndrome |
ME | Myalgic Encephalomyelitis |
NK | natural killer lymphocyte |
PBMC | peripheral blood mononuclear cells |
UHC | unrelated healthy control subject |
1Introduction
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a disease that still lacks unique diagnostic biomarkers or characterization of its underlying mechanisms of pathology. ME/CFS is distinguished by debilitating symptoms that are commonly shared among the patients and affects as many as 2.5 million adults in the USA [1]. The symptoms include: severe fatigue lasting more than 6 months; long-lasting post-exertional malaise; un-refreshing sleep; ‘brain fog’ in the form of lapsed memory or lessened ability to think; chronic muscle pain; and enlarged lymph nodes [2], with exclusion of patients with other conditions associated with fatigue such as anemia, cancer or severe depression. In Canada, a 2010 survey using broader criteria indicated that 1.3% of the adult population reported fatigue of over 6 months duration with 0.3% reporting positive for combined CFS and fibromyalgia [3]. There are no known causes in most cases of ME/CFS; however, long-term ME/CFS-like pathology may follow severe viral or bacterial infections [4]. ME/CFS has major costs to society [5]. Afflicted individuals would benefit from the discovery of definitive disease-specific biomarkers and these biomarkers are likely to support greater understanding of disease-promoting mechanisms.
To the best of our knowledge, this report is the first to extend the study of ME/CFS to families with multiple ME/CFS patients since the landmark study of natural killer (NK) cells in CFS by Dr. Paul Levine et al. in 1998 [6]. The Levine study compared CFS patients vs. multiple first degree family members to investigate the potential role for low NK cell activity in CFS. Several studies have compared twins, monozygotic vs. dizygotic twins, with one or both twins afflicted with ME/CFS [22—25], with the focus on etiology and genetic risk factors rather than biomarkers. Here we underscore the value of family members without ME/CFS as a separate group of controls (in addition to unrelated healthy controls). Family members have close genetic backgrounds and often similar lifestyles to the patients, and can optimize discovery of specific biomarkers by serving as maximally matched controls. In this report, we searched for a biomarker using 3 families each with 2 ME/CFS patients. The idea was to screen for a new biomarker of infection and/or inflammation that would be worthy of additional research.
Consideration of unique infections with associated biomarkers of the inflammatory etiology began when ME/CFS was first recognized in 1984 in a regional cluster of patients [7]. Several viruses have been proposed to promote chronic immune responses in ME/CFS, including persistent herpes viruses such as Epstein Barr virus [8–10], human cytomegalovirus [11], herpes zoster [12], and human herpes virus 6 [13–15]. The fatigue of ME/CFS resembles the fatigue induced during initial viral infections [16, 17]. Gamma interferon, elevated during viral infections, is also elevated in the blood of patients with severe CFS [18]. However, attempts to find unique or re-activated viral infections that are associated with ME/CFS have been unsuccessful [19, 20].
Here we focused on properties of monocytes as inflammatory biomarkers or risk factors for ME/CFS. Circulating blood monocytes can be elevated in numbers during infections [21]. Their phenotype varies extensively among human subjects [22]. They are polarized [23] towards either a pro-inflammatory ‘classical’ group defined by their CD14-positive CD16-negative phenotype or an anti-inflammatory ‘non-classical’ group of monocytes defined by their CD14negative CD16positive phenotype. The non-classical group promotes tissue repair [24–27] and includes the precursors of ‘patrolling’ tissue macrophages [28] that are found in inflamed tissues. There is recent recognition of a third group of ‘intermediate’ CD14low CD16Apositive monocytes with distinct pro- and anti-inflammatory properties [29, 30]. In this study, the intermediate group is included within the non-classical group. The potential for alterations of monocyte polarity prompted us to evaluate blood monocyte cell counts and their polarization as a potential biomarkers for ME/CFS. We postulated that higher monocyte numbers or an imbalance in classical vs. non-classical monocytes would be biomarkers or risk factors for ME/CFS, testing if any alterations from normal controls would also apply to the family members without ME/CFS.
This pilot study focused on the ‘non-classical’ group of CD16A (IgG Fc-gamma receptor)-positive monocytes. We observed elevation of the non-classical monocytes in patients vs. unrelated donors (P < 0.05) but this difference is unsuitable as a biomarker because there was little difference between patients compared to their non-ME/CFS family members. The results underscore the value of the unaffected family members to prevent false positive conclusions concerning biomarkers.
There is additional value to inclusion of family members without ME/CFS as a control group because they can help identify risks for ME/CFS. We found a modest elevation of non-classical monocytes for the family members, and these results may imply that monocytes within the non-classical subset could influence the likelihood of disease. We also found merit for inclusion of unaffected family members in a pilot study of antibody-dependent (ADCC) mediated by NK cells in ME/CFS (manuscript in preparation). The inclusion of unaffected family indicated that low ADCC is unsuitable as a biomarker for ME/CFS but could be a risk factor for ME/CFS. In summary, in this report we present data on monocytes to support inclusion of family members without ME/CFS as a means to promote discovery of biomarkers for ME/CFS. Occupational therapists have unique opportunities to advocate to the medical community and to explain to family members the need for inclusion of non-ME/CFS first degree family members as critical controls.
2Methods
2.1CFS patients, family members and unrelated healthy donors
Families, each with 2 ME/CFS patients at the Bateman Horne Center in Salt Lake City, UT, were selected by Dr. Lucinda Bateman and her research team from among many families afflicted with ME/CFS. Selection was for families with two (or more) patients and with multiple siblings (see pedigrees, Fig. 1), with the initial idea of finding biomarkers that would always (and even exclusively) occur in the patients. Further selection was based on the availability of the donors. The three families for which we have monocyte data had a total of 6 CFS patients and one family had two generations with CFS patients. The CFS patients met both the Fukuda CDC 1994 diagnostic criteria for CFS [2] and the international consensus criteria of 2011 for ME/CFS [31]. Seventeen family members without ME/CFS participated. Table 1 provides summary information to indicate the average age and gender balance among the 3 groups of patients, family members without ME/CFS, and the unrelated healthy controls. All participants were Caucasian and the unrelated healthy controls were age- and sex- matched with the patients. Initial selection of the families was based on family members’ willingness to participate and their availability to donate blood on the same day as the patients. Disease characterization for each of the patients participating in the study, including symptoms of the Fukuda criteria and the duration of disease, is presented in Table 2A. Table 2B provides comparative information for the non-CFS family members. The incidences for other conditions for patients vs. non-ME/CFS family members were: 3/6 vs. 0/10 for autoimmune diseases; 1/6 vs.1/10 for cancer; and 3/6 vs.4/10 for self-reported depression. Additional information concerning the patients’ characteristics may be obtained from Dr. Bateman upon request. Sixteen sex, race-, and age- matched unrelated healthy control donors, living in Salt Lake City, participated. Healthy was defined as HIV-negative, without overt infections at the time of blood donation, and without diagnosis of CFS. Blood samples were coded. The evaluations of monocytes were run with coded samples. The research with human subjects was approved by institutional review boards (IRBs) for the University of Nevada, Reno School of Medicine and for the Bateman Horne Center. Written informed consent was obtained from the donors of the blood samples.
Fig. 1
ME/CFS family pedigrees. The pedigrees of the 3 ME/CFS families are illustrated with dark gray fill for deceased parents, red fill for the ME/CFS patients and unfilled symbols for the family members without ME/CFS. Circles indicate women and squares men.
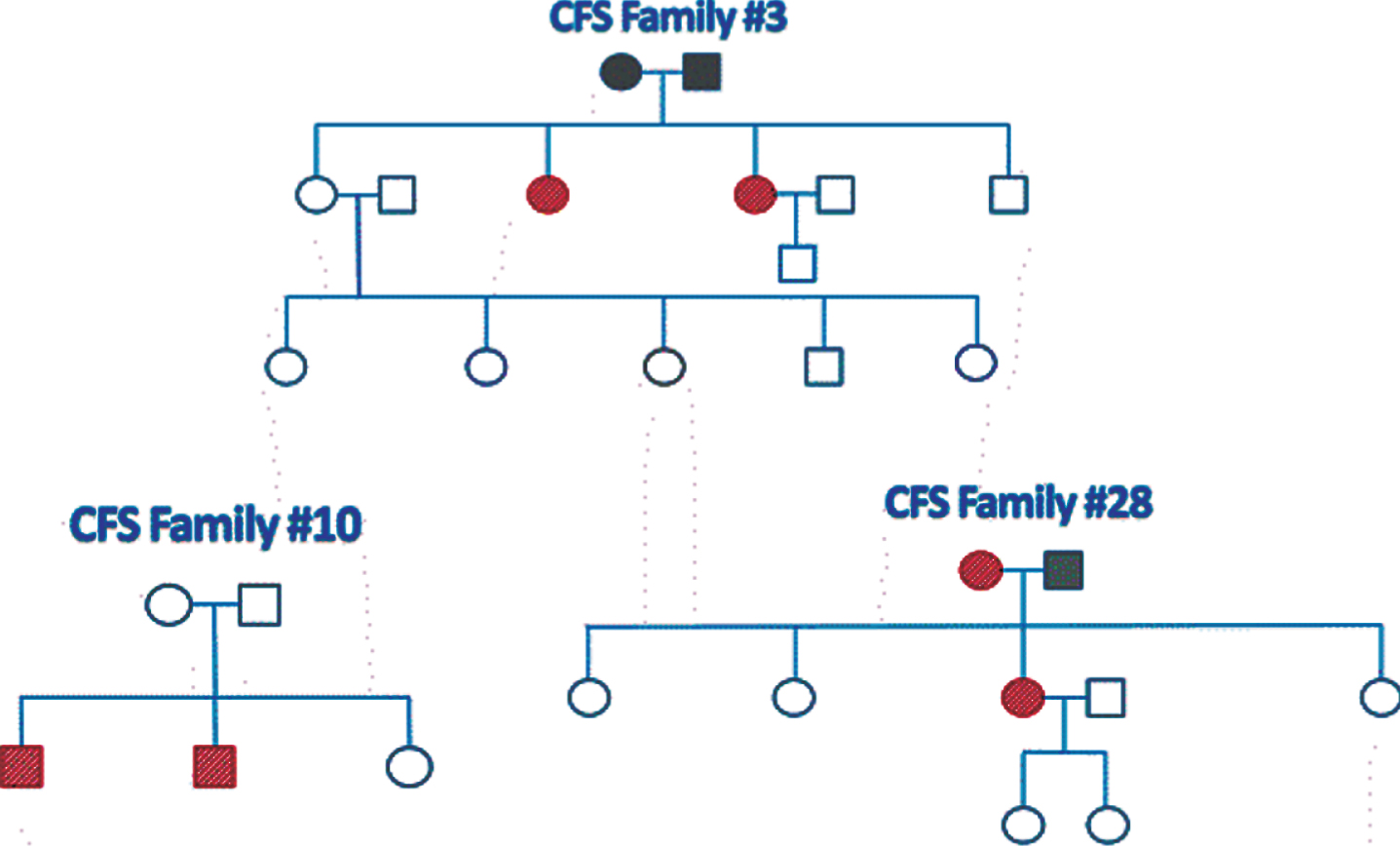
Table 1
Characteristics of the three study populations
| Characteristic | CFS cases | Family members w/o CFS | Unrelated healthy controls | ||||
| Number of participants | 6 | 17 | 16 | ||||
| Number of families | 3 | 3 | 16 | ||||
| Age, mean+/- SD | 49.0 + /- 30.1 | 48.1 + /- 14.2 | 42.8 + /- 18.6 | ||||
| Sex | Number | % | Number | % | Number | % | |
| Female | 4 | 66.7 | 11 | 64.7 | 12 | 75.0 | |
| Male | 2 | 33.3 | 6 | 35.3 | 4 | 25.0 | |
Table 2
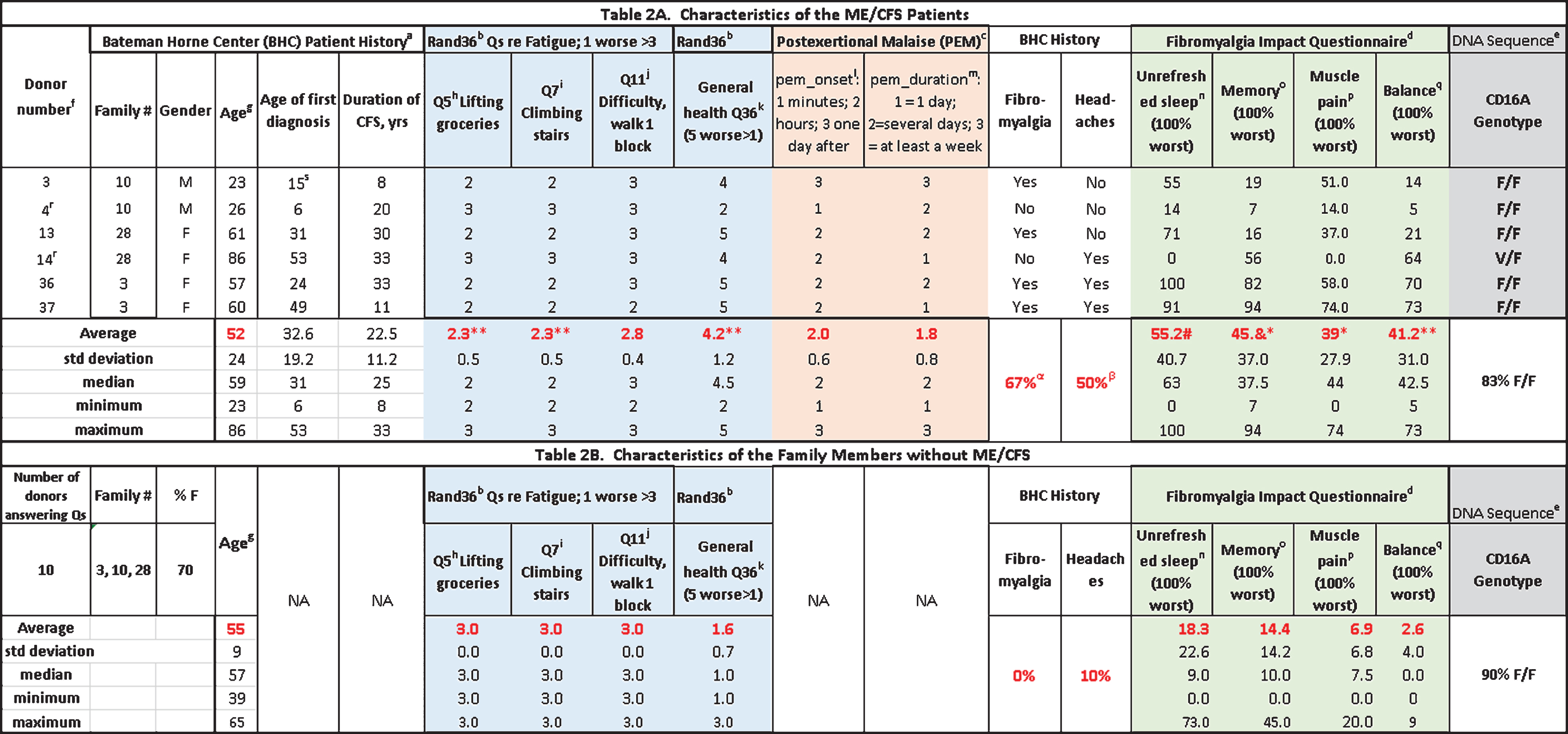 |
αP < 0.05 by Fisher exact test. βP = 0.07 by Chi square. aBHC data from patient records. bRand36 questionnaire [53]. cThe Canadian Consensus Criteria defines Post-Exertional Malaise (PEM) as an inappropriate loss of physical and mental stamina, rapid muscular and cognitive fatigability, post-exertional malaise and/or fatigue and/or pain and a tendency for other associated symptoms within the patient’s cluster of symptoms to worsen. There is a pathologically slow recovery period-usually 24 hours or longer. Please answer the following questions to describe how you experience PEM. dFibromyalgia Impact Questionnaire [54]. eAge at time of blood donation. fDifficulty lifting or carrying groceries. 1, Yes, limited a lot; 2, Yes, limited a little; 3, No, not limited at all. gClimbing one flight of stairs. 1, Yes, limited a lot; 2, Yes, limited a little; 3, No, not limited at all. hWalking one block. 1, Yes, limited a lot; 2, Yes, limited a little; 3, No, not limited at all. iDuration. How long does it take you to recover from PEM? 1, minutes after exertion; 2, hours after exertion; 3, a day or more after exertion; 4, not at all. jPlease rate the quality of your sleep. Slider scale, 0-100: Awoke well rested vs. Awoke very tired. kPlease rate your level of memory problems. Slider scale, 0 -100: Good memory vs. Very poor memory. lPlease rate your level of pain. Slider scale, 0 -100: No pain vs. Unbearable pain.
2.2Collection of blood and preparation of peripheral blood mononuclear cells (PBMCs) for overnight culture before characterization of CD16A-positive cells
Entire families, or groups of members of the larger families, with inclusion of 1 or 2 unrelated healthy controls were drawn on the same day. Blood was drawn from the subjects in Salt Lake City between 8-10 AM; 8 ml into tubes for DNA isolation and 24 ml into heparinized tubes for cell preparation. For each family, two ME/CFS patients, and one (or two) family members and one (or two) unrelated healthy controls were included within a shipment of samples that was assessed as one experiment. Samples from additional family members and unrelated controls were sent in shipments representing 3-6 donors per shipment. Researchers at UNR were unaware which shipments had ME/CFS donors. The samples were coded and shipped overnight to Reno, NV, and the samples remained coded until the cellular analyses were completed. Plasma was collected at UNR from centrifuged whole blood and phosphate-buffered saline was added to the cells to replace the plasma volume. Then the PBMCs were isolated by their ficoll-hypaque density [32]. The PBMCs were cultured overnight at 1-2 x 106 cells/ml in assay media containing 90% Dulbecco’ s complete media containing high (4.5 g/L) glucose and L-glutamine (Corning), 10% fetal calf serum (Atlanta Biologicals), 10 mM hepes, and 1% penicillin-streptomycin (Sigma-Aldrich, St. Louis, MO). Culture conditions were standardized with one lot of (frozen) fetal calf serum and one lot of 75 mm tissue culture flasks (Biolite, Thermo Scientific) throughout the experiments.
2.3TruCounts® of monocytes/μl blood
Fifty μl aliquots of whole blood were labeled on the days of arrival with the following panel of antibodies designed for no-wash TruCount® analyses that included: PacBlue anti-CD45 for identification of all cells (clone HI30); PE-Cy7-anti-CD3e for T cells (clone UCHT1); PE-Cy7-anti-CD33 for monocytes (P67.6). Antibodies were purchased from BioLegend (San Diego, CA). Cells were labeled for 30 minutes in tubes with TruCount® beads (Becton Dickenson no. 340334 [33]), fixed, and analyzed by flow cytometry the same day. The flow cytometer was a BD LSR II analytical flow cytometer (a modified Biosciences Special Order Research Product) with a high throughput sampler unit. Analyses were made with FlowJo software (FlowJo, LLC, Ashland, OR) to determine the numbers of CD33pos cells and TruCount® beads used calculate the number of CD33pos monocytes per μl blood [34].
2.4Assessment of non-classical monocytes by analytical flow cytometry
After overnight culture, PBMCs were stained with a panel that included Pac-Blue anti-CD45 (clone HI30) to detect all the leukocytes, FITC-anti-CD3 (UCHT1) to detect T cells & FITC anti-CD91 (2MR-alpha; BD Biosciences) to detect monocytes, and AF647-anti-CD16A (clone 3G8) to detect the non-classical CD16Apos monocytes. Cells were fixed and washed twice to remove unbound antibodies before analysis. Total monocytes were defined by their CD91-positive, high side scatter area (SSC-A) status.
2.5Efforts to limit intra-experimental variation
These experiments were conducted between November 19, 2015 and January 26, 2017. Inclusion of family members, ME/CFS patients and unrelated healthy controls in a single experiments with 4–6 donors reduced the total number of experiments and helped to limit inter-experimental variations. We also used only single lots of fluor-tagged antibodies to promote consistency.
2.6Statistical analyses
Student’s t-tests assuming equal variances that were included in the Microsoft Excel data analysis tool pack were used to compare the different groups of subjects when the variables were quantitative. When the variables were yes/no as for clinically diagnosed headaches or fibromyalgia (Table 2), chi-square with Yates correction and Fisher’s exact tests were applied, using software at www.socscistatistics.com. Excel and GraphPad Prism 7 (San Diego, CA) were used for illustrations.
3Results
3.1 Figure 2 indicates how inclusion of family members without ME/CFS can promote detection of a valid diagnostic biomarker vs. a risk factor for disease
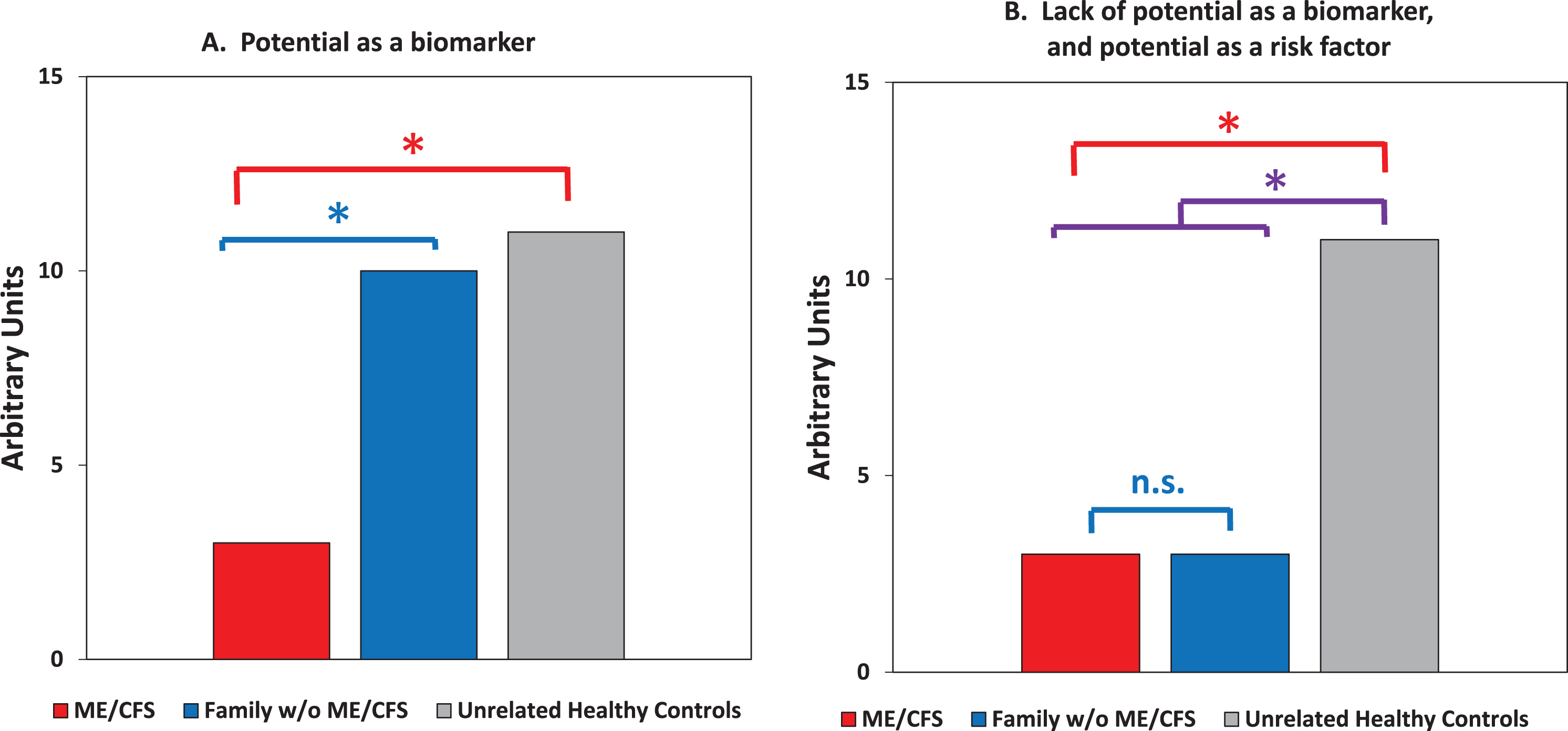
Figure 2A illustrates expected results that would qualify a diagnostic biomarker for further consideration. A definitive diagnostic biomarker must be positive for patients and negative for all unaffected persons, including family members. Differences between only the patients and the unrelated healthy controls are necessary (but insufficient) to indicate a definitive biomarker. Figure 2B illustrates differences between patients vs. unrelated healthy controls that would lead to erroneous conclusions if the data also showed little difference between patients vs. family members but were excluded from consideration. If only the patients and unrelated controls are compared, and the comparable low values for family members ignored, the results could be misinterpreted as evidence for a diagnostic biomarker. The similarity of diseased and non-diseased family members is telling! There is no disease-specific biomarker in Fig. 2B. When both the patients and family members differ from the unrelated controls as illustrated in Fig. 2B, the measurements can reflect a risk factor. This risk factor could be due to Mendelian genetics, epigenetics or environmental factors. A good example of diagnostic biomarker vs. risk factor discrimination occurs with type 1A autoimmune diabetes [35]: lack of insulin is a diagnostic biomarker while auto-antibodies to pancreatic proteins are risk factors. The autoantibodies can be found in individuals who may never progress to disease, including family members who share genetic risk factors with the patients.
Fig. 2
A guide for detection of diagnostic biomarkers vs. risk factors when there is inclusion of unaffected family members as a second group of controls. Asterisks indicate expected statistically significant differences, with P < 0.05. A. Expected data consistent with potential as a biomarker. The differences between patients vs. the first degree relatives without ME/CFS must be significant, as are the differences between patients vs. matched unrelated healthy controls. B. Expected data eliminating consideration as a disease-specific biomarker but consistent with potential as a risk factor. To be a strong candidate as a risk factor, the differences between patients and the first degree relatives can be marginal (as indicated) or in the same direction (higher or lower than unrelated controls). The differences between all family members (patients plus unaffected family members) vs. unrelated healthy controls should be significant.
3.2ME/CFS patients, their family members, and unrelated healthy donors had similar blood total monocyte counts
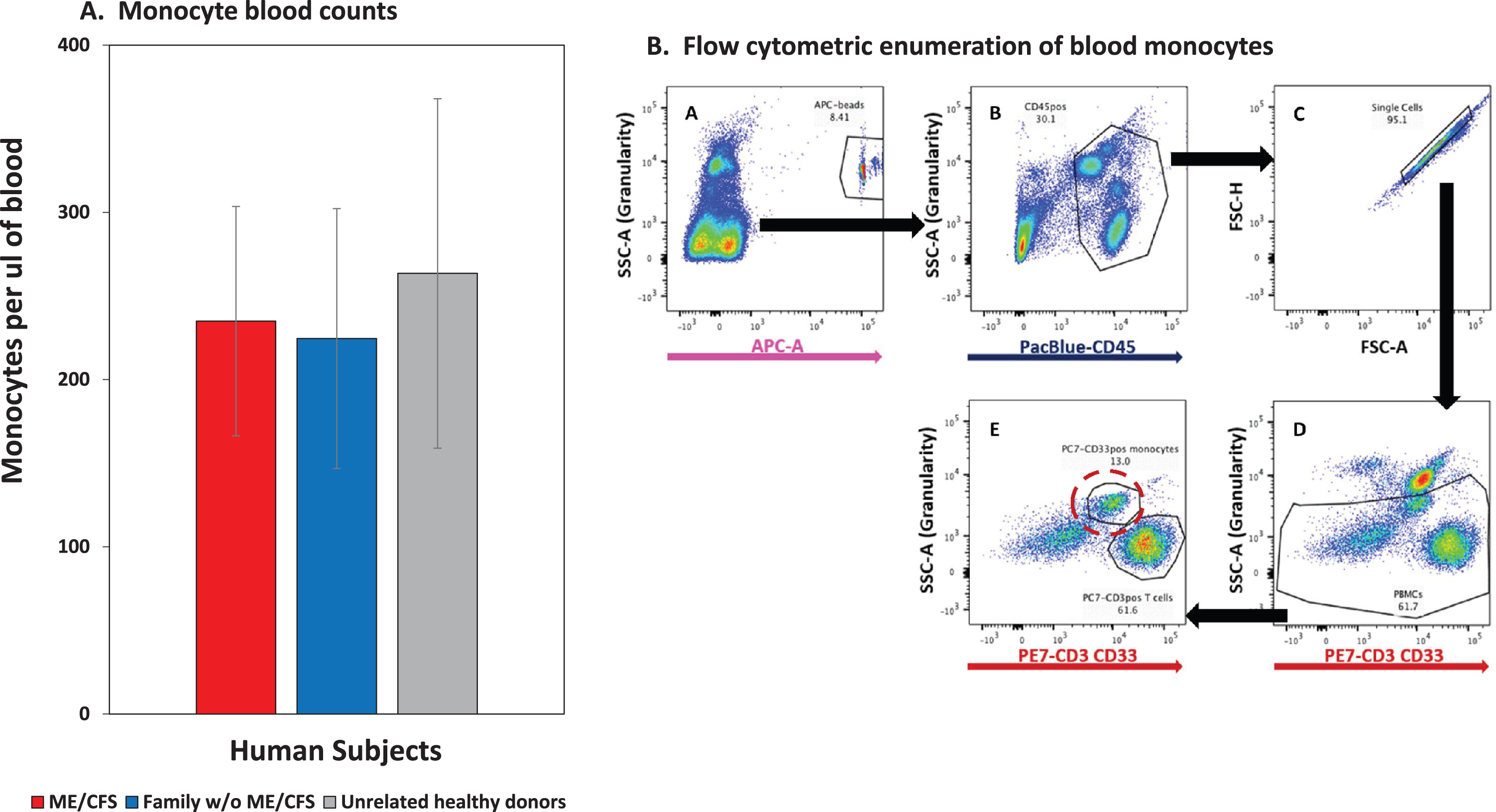
Figure 3A illustrates similarity in the circulating blood monocytes among the patients, their family members without ME/CFS, and the unrelated healthy controls. These monocyte counts are within the normal range of 250–840 cells/ul [36] and below the levels elevated in sepsis [37]. Figure 3B indicates the flow cytometric approach used to count the TrucountR calibration beads and the monocytes. The beads indicated the blood volume that was sampled and the method prevented inaccuracies associated with variable cell losses if the blood cells had been washed to remove unbound antibodies. The monocyte counts are consistent with absence of major pathological bacterial infections in all the subjects.
Fig. 3
Monocyte blood counts of ME/CFS patients are similar to counts of their family members without ME/CFS and to the counts of unrelated healthy controls. A. Monocytes per ul of blood; average and SD values for families #3, 10 & 28, 16 unaffected family members and 16 unrelated healthy controls. B. Flow cytometric methodology with TruCountR beads for the monocyte blood counts. The blood cells were labeled with a panel of antibodies in tubes containing TruCountR beads, and the cells were analyzed without washing in order to avoid selective cell losses that can be caused by washes to remove unbound antibodies. Each sequential step of cell gating, that was used to detect the beads and the CD33positive & high side scatter monocytes, is indicated by letters with arrows to indicate the cells selected for each sequential gate. The monocytes are circled in dashed red in step E.
3.3ME/CFS patients and unrelated controls differed significantly in their percentages of CD16Apositive “non-classical” monocytes
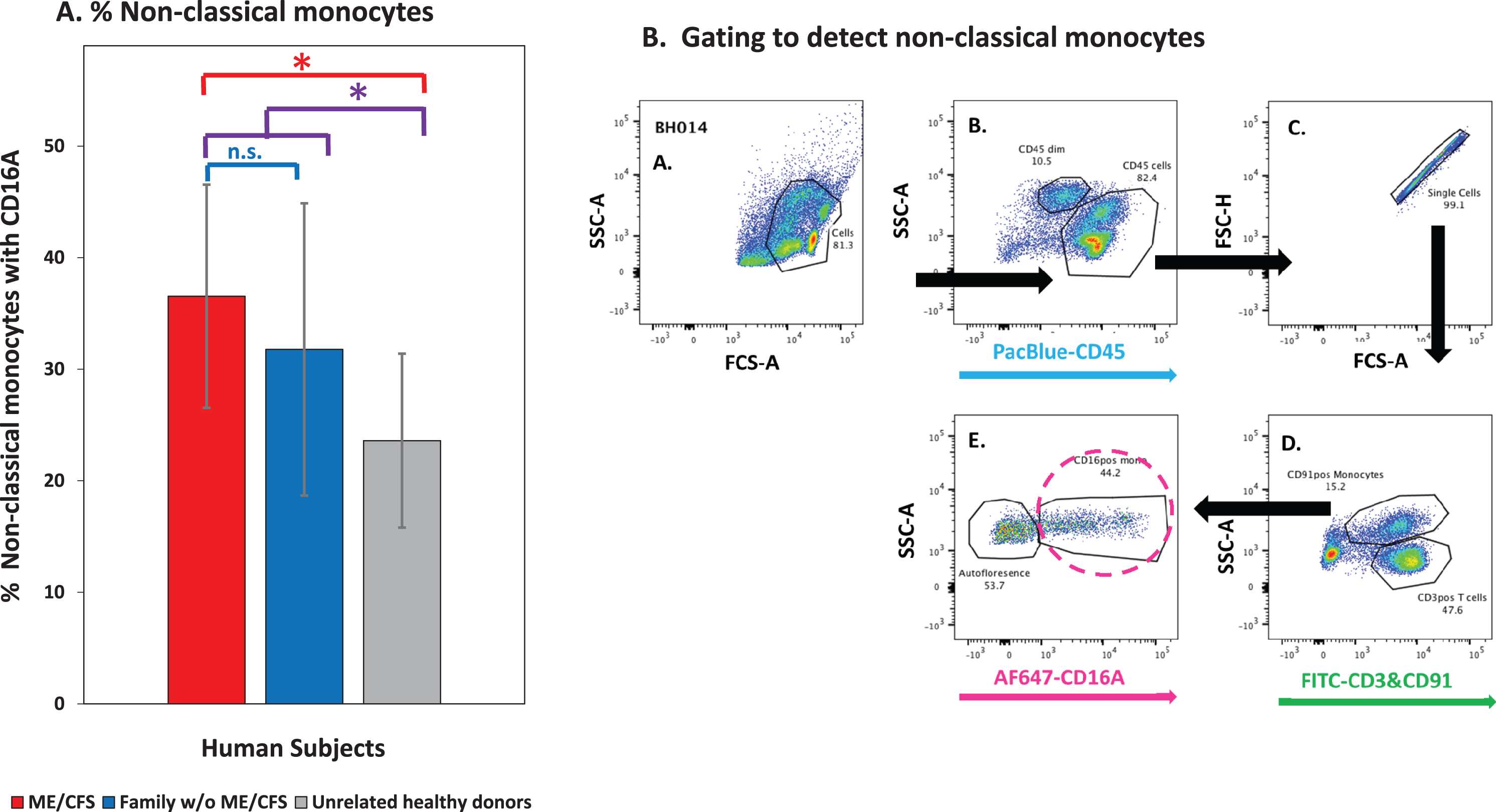
The percentage of non-classical monocytes was 55% higher for the CFS patients than for their unrelated controls (Fig. 4A) and the difference was statistically significant, P < 0.05. Thus there was evidence for non-classical monocyte polarization. In contrast to the patients vs. the unrelated controls, there was no significant difference between the patients vs. the unaffected family members (P = 0.51) and the percentage of non-classical monocytes for the family members was intermediate between those of the patients and the unrelated controls. The lack of a significant difference between the patients vs. their family members rules against diagnostic biomarker potential for non-classical monocytes, as indicated in the guide Fig. 2B. When the family members were combined into one group to evaluate potential for familial association and/or risk (Fig. 4A, purple bar), the P was 0.04, indicating that there may be shared genetic or environmental factors that distinguish ME/CFS families from unrelated controls.
Fig. 4
The percentages of non-classical (CD16Apositive) monocytes vs. unrelated healthy controls contra-indicate biomarker potential, but could reflect a disease risk factor. A. Percentages of the non-classical group of total monocytes; average and SD values for ME/CFS patients from families #3 & 28, with their unaffected family members and unrelated healthy controls. Even with low sample sizes of 4 ME/CFS patients and 11 unrelated healthy controls with flow cytometric data for monocytes, the difference between the patients vs. the unrelated controls was statistically significant. It was the similarity of the patients vs. their 14 family members that countered biomarker potential. B. Non-classical monocytes were detected by their CD16A expression (dashed circle, panel E). The cells were cultured overnight and then stained with a panel of fluorescent antibodies and washed. FITC anti-CD3 and anti-CD91 mAb’s were used for multiplex staining of T cells and monocytes, respectively. The monocytes are distinguished by their CD91staining & side scatter and are circled in dashed pink.
3.4There is an additional way to utilize data from unaffected family members
Their data can be pooled with that of the unrelated controls to form a single, larger control group of individuals without ME/CFS. In the case of the percentage of non-classical monocytes, with this combination there were 27 subjects to compare vs. the ME/CFS patients, with means of 28.2% and 36.5%, respectively. The P value was 0.19, also consistent with a low probability of non-classical monocytes being a diagnostic biomarker for ME/SFS. The 95% confidence ranges overlapped extensively: 21-53% for the CFS patients and 23-33% for all the unaffected donors. This combination increased the statistical power of the control group, but still may have left an under-powered clinical group in this pilot study.
4Discussion
4.1This pilot report presents data evaluating inflammatory parameters of monocytes in ME/CFS
The results indicated that blood monocyte counts and the percentage of non-classical monocytes are unsuitable as biomarkers to diagnose ME/CFS. It was the lack of differences between the patients vs. their first degree family members without ME/CFS that was critical for these findings. The inclusion of the unaffected family members meant that relatively few ME/CFS patients were needed to donate blood and that the non-classical monocytes could be distinguished as a potential risk factor rather than a strong candidate for a diagnostic biomarker.
4.2The findings concerning monocytes indicate that a more refined study of inflammatory monocytes within the non-classical subset could be worthwhile
While the monocyte counts were similar, the groups within the monocytes differed. Similarities in monocyte cell counts have been reported previously for the severe ME/CFS patient CD14-positive blood monocyte counts [38] and the % CD14-positive monocytes within PBMCs of patients with CFS [39]. The similarities are consistent with an absence of gross infections in the patients. These classical monocytes have the CD14 receptor for bacterial lipopolysaccharides (LPS) [40] and can respond by secreting pro-inflammatory cytokines such as the fever-inducing cytokines TNFα and IL-1 [41]. The discovery of monocytes lacking CD14 led to the initial designation of non-classical CD16A-positive monocytes [42]. These CD16Apos monocytes are elevated in sepsis [21, 43]. These designations have now been updated (reviewed, [44] with additional subsets that are defined by their receptors and the different cytokines they secrete. These cytokines include TGFβ that is increased in ME/CFS [45] and associated with the severest forms of ME/CSF [18]. The CD16A-positive non-classical & intermediate monocytes are both considered as valuable markers for risks of coronary heart disease [46]. Both may be useful as indicative risk factors for ME/CFS or to distinguish patient subgroups within ME/CFS patients.
4.3This study of ME/CFS has several limitations and a potential advantage
One limitation is that the patients had moderate disease symptoms and none had extremely severe ME/CFS that leaves patients chronically bed-ridden. Another limitation is that these patients were only of northern European ancestry. As a result, the increases in CD16A-positive monocytes may not extend to all geographic or ethnic groups of CFS patients. We studied only 3 families in this pilot study so that type 2 errors are also possible due to under-powered patient numbers. Also, the families we studied here had two ME/CFS patients per family and the value of the unaffected family controls may be less when there is only one ME/CFS patient per family. The frequency of patients per family may have been an advantage. It is noteworthy that family associations are receiving attention as a new means to identify previously unrecognized potential risk factors for chronic diseases [47].
4.4Even with these limitations, inclusion of family members without disease has advantages for the screening of diagnostic biomarkers
Comparison of patients vs. family members without the specific disease offers researchers the ability to “cut to the chase” faster by early detection of false positive problems. In terms of stringency, if a biomarker fails to differentiate between the patients vs. their unaffected family members and fails in one homogenous group, it lacks universal applicability and fails. We recommend inclusion of unaffected family members regardless of whether the biomarkers being evaluated are autoantibodies [48], brain lesions [49] or intestinal microbial populations [50]. Occupational therapists, with their many hours spent with patients and family members, are in a unique position to explain to non-ME/CFS first degree family members the need for their inclusion as critical controls and the value of their time spent answering questionnaires and donating blood.
4.5Continuation of research to discover biomarkers for ME/CFS is extremely important for both patients and clinicians
A definitive biomarker would help both patients who are sometimes dismissed as having psychosomatic illnesses [1] and their doctors who struggle to treat the debilitating symptoms. The National Institutes of Health (USA) is actively pursuing diagnostic biomarkers and causes of the disease symptoms [51]. Clinical research is difficult because of the large sample sizes that are usually needed to achieve valid conclusions [52] and thus investigators have to make difficult decisions as to which hypotheses they will test. In summary, this report provides general guidance to future biomarker studies to include unaffected family members as a separate control group whenever ethically possible.
Authors’ contributions
Ideas for the measurements of monocytes were conceptualized by DH and DR. Clinical diagnoses of ME/CFS were done by LB. The clinical arrangements, patient data and acquisition of blood samples were organized by LB and the staff at the Bateman Horne Center. Flow cytometry was done by KT, DR, DH, and MJG. Statistical analyses were guided and reviewed by JSG. Manuscript preparation was done by KT, DH, APS, and MJG.
Conflict of interest
The authors lack financial interests or potential financial benefits from this research and its publication.
Acknowledgments
We are indebted to the patients and their families who participated in this study and thankful for the leadership and staff at the Bateman Horne Center who made this study possible. The research was supported in part by NIH R21 AI117491 awarded to Dr. Dorothy Hudig as a co-investigator, by NIH P30 GM110767 (Cytometry Center), and by an anonymous generous private donor to the Bateman Horne Center who helped pay for the collection and shipment of blood samples. We would also thank the Nevada INBRE program (NIH GM103440) for an undergraduate research scholarship (to APS) and supplies which helped support the project. We thank Terry Woodin, Ph.D. for manuscript editing.
References
[1] | National Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness: National Academies Press, Washington, DC; (2015) . |
[2] | Fukuda K , Straus SE , Hickie I , Sharpe MC , Dobbins JG , Komaroff A . The chronic fatigue syndrome: a comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann Intern Med. (1994) ;121: (12):953–9. |
[3] | Rusu C , Gee ME , Lagace C , Parlor M . Chronic fatigue syndrome and fibromyalgia in Canada: prevalence and associations with six health status indicators. Health Promot Chronic Dis Prev Can. (2015) ;35: (1):3–11. |
[4] | Hickie I , Davenport T , Wakefield D , Vollmer-Conna U , Cameron B , Vernon SD , et al. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: prospective cohort study. BMJ. (2006) ;333: (7568):575. |
[5] | Reynolds KJ , Vernon SD , Bouchery E , Reeves WC . The economic impact of chronic fatigue syndrome. Cost Eff Resour Alloc. (2004) ;2: (1):4. |
[6] | Levine PH , Whiteside TL , Friberg D , Bryant J , Colclough G , Herberman RB . Dysfunction of natural killer activity in a family with chronic fatigue syndrome. Clin Immunol Immunopathol. (1998) ;88: (1):96–104. |
[7] | Daugherty SA , Henry BE , Peterson DL , Swarts RL , Bastien S , Thomas RS . Chronic fatigue syndrome in northern Nevada. Rev Infect Dis. (1991) ;13: Suppl 1:S39–44. |
[8] | Loebel M , Strohschein K , Giannini C , Koelsch U , Bauer S , Doebis C , et al. Deficient EBV-specific B- and T-cell response in patients with chronic fatigue syndrome. PLoS One. (2014) ;9: (1):e85387. |
[9] | Loebel M , Eckey M , Sotzny F , Hahn E , Bauer S , Grabowski P , et al. Serological profiling of the EBV immune response in Chronic Fatigue Syndrome using a peptide microarray. PLoS One. (2017) ;12: (6):e0179124. |
[10] | Lerner AM , Beqaj SH , Deeter RG , Fitzgerald JT . IgM serum antibodies to Epstein-Barr virus are uniquely present in a subset of patients with the chronic fatigue syndrome. In Vivo. (2004) ;18: (2):101–6. |
[11] | Beqaj SH , Lerner AM , Fitzgerald JT . Immunoassay with cytomegalovirus early antigens from gene products p52 and CM2 (UL44 and UL57) detects active infection in patients with chronic fatigue syndrome. J Clin Pathol. (2008) ;61: (5):623–6. |
[12] | Shapiro JS . Does varicella-zoster virus infection of the peripheral ganglia cause Chronic Fatigue Syndrome? Med Hypotheses. (2009) ;73: (5):728–34. |
[13] | Komaroff AL . Is human herpesvirus-6 a trigger for chronic fatigue syndrome? J Clin Virol. (2006) ;37: Suppl 1:S39–S46. |
[14] | Buchwald D , Cheney PR , Peterson DL , Henry B , Wormsley SB , Geiger A , et al. A chronic illness characterized by fatigue, neurologic and immunologic disorders, and active human herpesvirus type 6 infection. Ann Intern Med. (1992) ;116: (2):103–13. |
[15] | Eymard D , Lebel F , Miller M , Turgeon F . Human herpesvirus 6 and chronic fatigue syndrome. Can J Infect Dis. (1993) ;4: (4):199–202. |
[16] | Bonnem EM , Oldham RK . Gamma-interferon: physiology and speculation on its role in medicine. J Biol Response Mod. (1987) ;6: (3):275–301. |
[17] | Kerr JR , Tyrrell DA . Cytokines in parvovirus B19 infection as an aid to understanding chronic fatigue syndrome. Curr Pain Headache Rep. (2003) ;7: (5):333–41. |
[18] | Montoya JG , Holmes TH , Anderson JN , Maecker HT , Rosenberg-Hasson Y , Valencia IJ , et al. Cytokine signature associated with disease severity in chronic fatigue syndrome patients. Proc Natl Acad Sci U S A. (2017) ;114: (34):E7150–e8. |
[19] | Soto NE , Straus SE . Chronic Fatigue Syndrome and Herpesviruses: the Fading Evidence. Herpes. (2000) ;7: (2):46–50. |
[20] | Wallace HL 2nd , Natelson B , Gause W , Hay J . Human herpesviruses in chronic fatigue syndrome. Clin Diagn Lab Immunol. (1999) ;6: (2):216–23. |
[21] | Fingerle G , Pforte A , Passlick B , Blumenstein M , Strobel M , Ziegler-Heitbrock HW . The novel subset of CD14+/CD16+blood monocytes is expanded in sepsis patients. Blood. (1993) ;82: (10):3170–6. |
[22] | Hudig D , Hunter KW , Diamond WJ , Redelman D . Properties of human blood monocytes. II. Monocytes from healthy adults are highly heterogeneous within and among individuals. Cytometry B Clin Cytom. (2014) ;86: (2):121–34. |
[23] | Ziegler-Heitbrock L , Ancuta P , Crowe S , Dalod M , Grau V , Hart DN , et al. Nomenclature of monocytes and dendritic cells in blood. Blood. (2010) ;116: (16):e74–80. |
[24] | Shapouri-Moghaddam A , Mohammadian S , Vazini H , Taghadosi M , Esmaeili SA , Mardani F , et al. Macrophage plasticity, polarization, and function in health and disease. J Cell Physiol. (2018) ;233: (9):6425–40. |
[25] | Guilliams M , Mildner A , Yona S . Developmental and Functional Heterogeneity of Monocytes. Immunity. (2018) ;49: (4):595–613. |
[26] | Murray PJ . Macrophage Polarization. Annu Rev Physiol. (2017) ;79: :541–66. |
[27] | Ziegler-Heitbrock L . Blood Monocytes and Their Subsets: Established Features and Open Questions. Front Immunol. (2015) ;6: :423. |
[28] | Hanna RN , Cekic C , Sag D , Tacke R , Thomas GD , Nowyhed H , et al. Patrolling monocytes control tumor metastasis to the lung. Science. (2015) ;350: (6263):985–90. |
[29] | Hijdra D , Vorselaars AD , Grutters JC , Claessen AM , Rijkers GT . Phenotypic characterization of human intermediate monocytes. Front Immunol. (2013) ;4: :339. |
[30] | Wong KL , Tai JJ , Wong WC , Han H , Sem X , Yeap WH , et al. Gene expression profiling reveals the defining features of the classical, intermediate, and nonclassical human monocyte subsets. Blood. (2011) ;118: (5):e16–31. |
[31] | Carruthers BM , van de Sande MI , De Meirleir KL , Klimas NG , Broderick G , Mitchell T , et al. Myalgic encephalomyelitis: International Consensus Criteria. J Intern Med. (2011) ;270: (4):327–38. |
[32] | Boyum A , Lovhaug D , Tresland L , Nordlie EM . Separation of leucocytes: improved cell purity by fine adjustments of gradient medium density and osmolality. Scand J Immunol. (1991) ;34: (6):697–712. |
[33] | Langenskiold C , Mellgren K , Abrahamsson J , Bemark M . Determination of blood cell subtype concentrations from frozen whole blood samples using TruCount beads. Cytometry B Clin Cytom. 2016. |
[34] | Sung AP , Tang JJ , Guglielmo MJ , Redelman D , Smith-Gagen J , Bateman L , et al. An improved method to quantify human NK cell-mediated antibody-dependent cell-mediated cytotoxicity (ADCC) per IgG FcR-positive NK cell without purification of NK cells. J Immunol Methods. (2018) ;452: :63–72. |
[35] | Zhang L , Eisenbarth GS . Prediction and prevention of Type 1 diabetes mellitus. J Diabetes. (2011) ;3: (1):48–57. |
[36] | Hubl W , Andert S , Erath A , Lapin A , Bayer PM . Peripheral blood monocyte counting: towards a new reference method. Eur J Clin Chem Clin Biochem. (1995) ;33: (11):839–45. |
[37] | Schinkel C , Sendtner R , Zimmer S , Faist E . Functional analysis of monocyte subsets in surgical sepsis. J Trauma. (1998) ;44: (5):743–8; discussion 8-9. |
[38] | Hardcastle SL , Brenu EW , Johnston S , Nguyen T , Huth T , Wong N , et al. Characterisation of cell functions and receptors in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME). BMC Immunol. (2015) ;16: :35. |
[39] | Cliff JM , King EC , Lee JS , Sepulveda N , Wolf AS , Kingdon C , et al. Cellular Immune Function in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Front Immunol. (2019) ;10: :796. |
[40] | Triantafilou M , Triantafilou K . Lipopolysaccharide recognition: CD14, TLRs and the LPS-activation cluster. Trends Immunol. (2002) ;23: (6):301–4. |
[41] | Wu Z , Zhang Z , Lei Z , Lei P . CD Biology and role in the pathogenesis of disease. Cytokine Growth Factor Rev. (2019) ;48: :24–31. |
[42] | Passlick B , Flieger D , Ziegler-Heitbrock HW . Identification and characterization of a novel monocyte subpopulation in human peripheral blood. Blood. (1989) ;74: (7):2527–34. |
[43] | Horelt A , Belge KU , Steppich B , Prinz J , Ziegler-Heitbrock L . The CD14+CD16+monocytes in erysipelas are expanded and show reduced cytokine production. Eur J Immunol. (2002) ;32: (5):1319–27. |
[44] | Wolf AA , Yanez A , Barman PK , Goodridge HS . The Ontogeny of Monocyte Subsets. Front Immunol. (2019) ;10: :1642. |
[45] | Bennett AL , Chao CC , Hu S , Buchwald D , Fagioli LR , Schur PH , et al. Elevation of bioactive transforming growth factor-beta in serum from patients with chronic fatigue syndrome. J Clin Immunol. (1997) ;17: (2):160–6. |
[46] | Idzkowska E , Eljaszewicz A , Miklasz P , Musial WJ , Tycinska AM , Moniuszko M . The Role of Different Monocyte Subsets in the Pathogenesis of Atherosclerosis and Acute Coronary Syndromes. Scand J Immunol. (2015) ;82: (3):163–73. |
[47] | Rasooly D , Ioannidis JPA , Khoury MJ , Patel CJ . Family History-Wide Association Study (“FamWAS’’) for Identifying Clinical and Environmental Risk Factors for Common Chronic Diseases. Am J Epidemiol. 2019. |
[48] | Giannoccaro MP , Cossins J , Sorland K , Fluge O , Vincent A . Searching for Serum Antibodies to Neuronal Proteins in Patients With Myalgic Encephalopathy/Chronic Fatigue Syndrome. Clin Ther. (2019) ;41: (5):836–47. |
[49] | Mueller C , Lin JC , Sheriff S , Maudsley AA , Younger JW . Evidence of widespread metabolite abnormalities in Myalgic encephalomyelitis/chronic fatigue syndrome: assessment with whole-brain magnetic resonance spectroscopy. Brain Imaging Behav. 2019. |
[50] | Nagy-Szakal D , Williams BL , Mishra N , Che X , Lee B , Bateman L , et al. Fecal metagenomic profiles in subgroups of patients with myalgic encephalomyelitis/chronic fatigue syndrome. Microbiome. (2017) ;5: (1):44. |
[51] | Komaroff AL . Advances in Understanding the Pathophysiology of Chronic Fatigue Syndrome. Jama. 2019. |
[52] | Button KS , Ioannidis JP , Mokrysz C , Nosek BA , Flint J , Robinson ES , et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci. 14. England2013. p. 365-76. |
[53] | Hays RD , Morales LS . The RAND-36 measure of health-related quality of life. Ann Med. (2001) ;33: (5):350–7. |
[54] | Bennett RM , Friend R , Jones KD , Ward R , Han BK , Ross RL . The Revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther. (2009) ;11: (4):R120. |


