
Self-directing return-to-work: Employees’ perspective
Abstract
BACKGROUND:
Dutch legislation stimulates active participation of employees in their own return-to-work (RTW). In addition, RTW professionals encourage sick-listed employees to self-direct RTW. It remains unclear, however, how employees give meaning to and shape their self-direction.
OBJECTIVE:
This study aims to conceptualize self-direction using the components of Self-Determination Theory (autonomy, competence, and relatedness) as a framework.
METHODS:
Semi-structured interviews were conducted with three long-term sick-listed employees. These results were combined with 14 existing transcripts of semi-structured interviews with long-term sick-listed employees and employees who experienced long-term sick leave during the previous calendar year. All interview transcripts were analyzed thematically.
RESULTS:
Employees generally think of self-direction as making their own decision regarding RTW. They wish to decide by themselves how to shape their RTW-process. Several environmental factors play a role in employees’ self-direction. Proximal factors are satisfaction of the need for autonomy, competence, and relatedness. Distal factors are legislation regarding RTW, organizational culture and clarity regarding the roles of various stakeholders in the process of sickness absence and RTW.
CONCLUSIONS:
Exercising self-direction in RTW seems to contribute to a personalized RTW-process that takes into account individual needs and wishes. Preconditions for effective self-direction are a supportive environment and good cooperation between employee, employer, and occupational physician.
1Background
Early return-to-work (RTW) after sickness absence is important because work is considered to support the employee’s well-being and quality of life [1]. Therefore, it is important for sick-listed employees to RTW as soon as possible. Employees benefit from early RTW since it supports their independence and provides a daily rhythm [2]. Early RTW is important for employers as well, particularly for financial reasons. In the Netherlands, employers generally are obliged to pay at least 70% of the employee’s salary in the first two years of sickness absence [3].
To further encourage early RTW, the Dutch Improved Gatekeeper Act prescribes that sick-listed employees and their employers should participate actively in the employee’s RTW process. This Act stipulates that the sick-listed employee and the employer have to follow a compulsory procedure which includes meeting regularly, developing an action plan for RTW, and evaluating the RTW process regularly [3, 4]. The aim of this Act is to decrease the appeal on the social security system after two years of sick leave. The Act also assumes that employees take responsibility for their RTW process [3, 4].
Practice professionals such as occupational physicians (OPs) have pointed out the need for employees to self-direct their own work resumption [5]. Although professionals have different ideas of what exactly self-direction by sick-listed employees means, they generally consider it to be a form of intrinsically motivated behavior [5].
However, in practice, employees may experience barriers to self-direct their return to work. Cooperation between employees and their employers tends to be difficult and minimal [6]. For example, employees should be motivated to contribute to their own RTW. Also they need to have a positive perception about the job [7]. For employers, it is unclear what they can expect and demand from their sick-listedemployees [6].
Sick-listed employees may also experience difficulties due to problematic cooperation between other stakeholders in the RTW process such as OPs and curative healthcare professionals [6]. For example, a lack of adequate curative treatment of health complaints and a lack of mutual agreement between the general practitioner and the occupational physician can complicate an employee’s RTW process [3].
To date, it remains unclear what sick-listed employees themselves consider to be ‘self-direction’ and which factors support their self-direction. This research aims to understand what sick-listed employees consider to be 1) self-direction in a RTW context, 2) their experiences with self-directing RTW, and 3) factors that play a role in their self-direction. Ultimately, the study results can be helpful for developing interventions to encourage self-direction in RTW. Insights from this study can raise awareness among RTW professionals such as OPs about practices that support employees’ self-direction in RTW.
1.1Theoretical underpinnings
If we assume that self-direction is a form of intrinsically motivated behavior, it conforms to Self-Determination Theory (SDT) [8]. SDT is an approach to describe human motivation by assessing innate psychological needs. The three core concepts of SDT are the needs for autonomy, competence, and relatedness [8]. It has been shown that these three innate psychological needs contribute to optimal functioning and fully stimulate personal growth [8]. If these three basic psychological needs are not fulfilled, intrinsically motivated behavior (proactive behavior such as voice behavior) and well-being will be diminished or not shown [8–10].
Fig.1
Basic needs of the Self-Determination Theory.
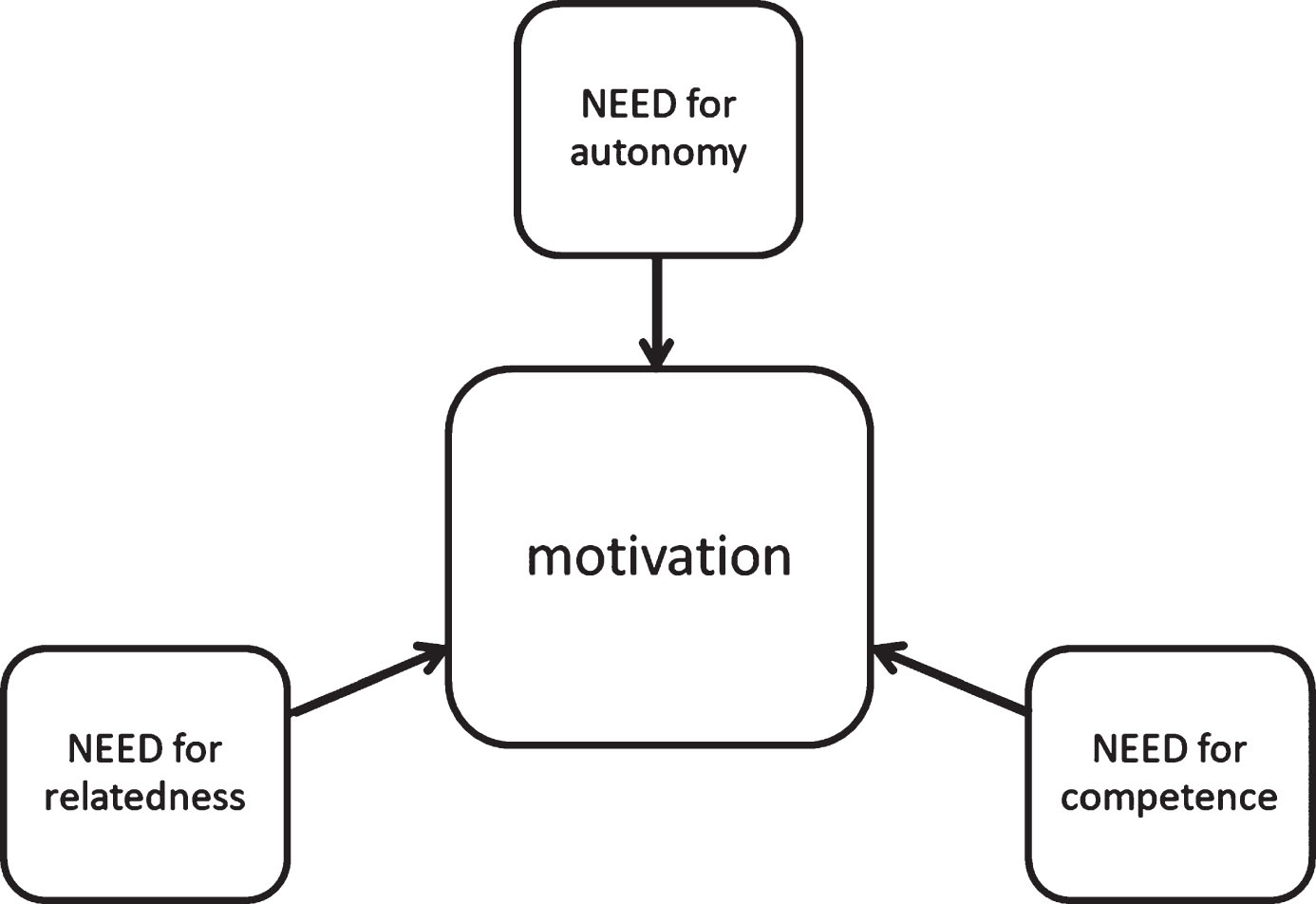
Describing RTW in terms of SDT, we assume that employees need to be motivated to self-direct their RTW process. SDT defines the need for autonomy as the need for feeling psychologically free and acting with feelings of ownership regarding their behavior [11]. Satisfaction of the need for autonomy contributes to the active involvement of employees since autonomy allows them to self-direct their RTW process [12].
Satisfaction of the need for relatedness concerns the need for feeling connected (in the sense of loving and caring) to others [13, 14]. In the context of sickness absence, the need for relatedness may be satisfied when an employee perceives adequate personal support, co-worker interactions, but also interactions with other stakeholders in the RTW process. According to Kirsch, these relations are needed for successful reintegration [15]. Satisfaction of the need for competence concerns the need for the development of new skills and feeling mastery of the environment [13, 16]. Satisfaction of the need for competence can partially be facilitated by the employer by lowering the threshold to RTW. For example, workplace adaptations and arrangements can be made [17, 18]. Still, sick-listed employees need to feel competent in performing RTW-related behavior when interacting with the workenvironment [19].
The satisfaction of the need for competence can also be considered from the perspective of self-efficacy as described by Bandura [20]. Both Self-Efficacy Theory (SET) and SDT try to understand and explain human behavior. According to SET, people behave in a certain way if they feel competent to do so (a high self-efficacy). In SDT, satisfaction of the need for competence has a direct relationship to motivation rather than behavior. Sweet, Fortier, Strachan and Blanchard [19] mention that the integration of the two theories is possible. Incorporating constructs from both will lead to a better understanding of the underlying mechanisms, especially competence (self-efficacy) and behavior. Self-efficacy is a predictor for motivation, which is the major concept in SDT. A higher self-efficacy will also result in overcoming some barriers that could hinder RTW and being able to perform RTW behavior [21]. Both theories are relevant for this research since they support and complement each other and will be used to categorize and interpret study findings.
2Study objectives
This research aims to yield insight into the employees’ perspectives on self-direction in a RTW context and the factors underlying employees’ self-direction.
In this study, self-direction is addressed from the employees’ point of view using basic psychological needs and the concept of intrinsic motivation (parts of SDT [7]) as a framework. Better insight into what employees consider to be self-direction and its supportive factors in the RTW process is relevant for all stakeholders involved in RTW, such as employers, employees, and professionals in vocational healthcare [5]. A more general description of self-direction can inform intervention participants about how to improve cooperation in the RTW process [6]. Healthcare providers, for example OPs or physiotherapists can use knowledge about the meaning of self-direction in RTW to better understand their clients (sick-listed employees) and enable workers’ self-direction in order to improve their treatment and their support.
3Methods
3.1Design, participants, and procedure
We performed a qualitative study using semi-structured interviews in order to gain in-depth information about employee experiences regarding their RTW-process and the role of self-direction in this process. These interviews took place in Spring 2017. The ethical committee of the Dutch Open University approved this study (correspondence dated 24 March 2017, registration number: U2017/02139/FRO).
Multiple HR officers, OPs, physiotherapists, and psychologists from the southern part of the Netherlands were approached by e-mail. This e-mail contained a recruitment letter to be handed out to employees from several companies and organizations who met the inclusion criteria: being long-term sick-listed (>6 weeks) or having experienced long-term sick leave less than one year before the planned interview. This group has been targeted because these employees have recently experienced or were still in an RTW-process. Additionally, two OPs were contacted by telephone, and one HR officer was contacted in person. These professionals were asked to give the recruitment letter to employees who might be eligible for participation in this study. Employees who were interested in participation could contact a member of the research team by e-mail or phone. In total, three employees participated in an interview. They all signed informed consent forms. Additionally, transcripts of 14 interviews that were conducted as part of previous research by Hoefsmit [6] regarding sickness absence, cooperation with healthcare providers, and RTW were included in this study.
An overview of participant characteristics is displayed in Table 1.
Table 1
Characteristics of study participants
| Participant | Interview/transcript | Gender | Age | Job* |
| P1 | Transcript | M | < 45 | Technical maintenance |
| P2 | Transcript | M | ≥45 | Administration |
| P3 | Transcript | M | ≥45 | Administration |
| P4 | Transcript | M | ≥45 | HR advisor |
| P5 | Transcript | F | ≥45 | Coordinator |
| P6 | Transcript | M | ≥45 | ICT |
| P7 | Transcript | M | < 45 | Administration |
| P8 | Transcript | M | < 45 | Production → administration |
| P9 | Transcript | M | ≥45 | Process operator → administration |
| P10 | Transcript | F | ≥45 | Secretary |
| P11 | Transcript | F | < 45 | Tutor/coach |
| P12 | Transcript | F | < 45 | Management assistant → secretary |
| P13 | Transcript | F | ≥45 | Warehouse employee → receptionist |
| P14 | Transcript | F | ≥45 | Sales assistant |
| P15 | Interview | F | ≥45 | Coordinator |
| P16 | Interview | F | < 45 | Coordinator |
| P17 | Interview | F | < 45 | Anonymous |
*When asked: “old job → new job during/after sickness absence”.
3.2Data collection
Data were collected using semi-structured interviews. The three interviews were conducted by JS at the workplaces of the participants. The average duration of an interview was one hour, and the interviews were held in Dutch (researcher’s native language). Topic lists for the interviews were based on concepts of SDT and Social Cognitive Theory. The main topics were: satisfaction of the employee’s need for autonomy, the role of the environment (satisfaction of the need for relatedness), responsibility for RTW, the added value of self-direction for a person, competence to self-direct RTW (satisfaction of the need for competence), and the need for self-direction in their RTW process. The data collection for these 14 interviews is described in the original research by Hoefsmit [6]. The topic lists for these interviews covered topics regarding the actions of sick-listed employees to achieve RTW as well as their cooperation with their employers. In addition, topics concerned the employees’ contact with multiple other stakeholders in the employees’ RTW process such as OPs. As such, the vast majority of the topics relevant to this study were addressed in the interviews conducted by Hoefsmit [6] as well.
3.3Data analysis
All interviews were transcribed verbatim. Data were analyzed thematically following the six steps by Braun and Clarke [for more details about these steps, see 22]: familiarization, collecting ideas and developing codes, clustering codes (axial coding), reviewing the themes discussed and the need for new codes, thematic analysis, and connecting themes to the data. Ultimately, this way of processing interviews provided sufficient information to draw conclusions.
In order to prevent interpretation bias, peer reviewing was used to enhance the validity and reliability of the data. Co-researchers and peers read the manuscripts and were involved in the discussion about codes and themes (IH, NH, EW).
4Results
Section 4.1 describes the results regarding the meaning of self-direction in RTW. Sections 4.2 and 4.3 describe several environmental factors that can play a role in employees’ self-direction in RTW. A distinction is made between proximal factors (satisfaction of the employees’ need for autonomy, competence, and relatedness, see section 4.2) and distal factors (legislation and organizational culture, see section 4.3).
4.1Self-direction: Employee decision making about RTW
The interviewees considered themselves to be the key stakeholder in their own RTW process. Most employees wanted to resume work as early as possible: “I always tell them I hope to be there tomorrow”; “I am impatient and I want to go back as soon as possible” (P15). These employees generally thought of self-direction in RTW as making their own choice regarding the way in which they resume work: “To choose for yourself whether you can do or just cannot do a task/job” (P16). Such self-direction particularly concerns making a decision regarding tasks to do and the working schedule. Self-direction is experienced when an employee can choose which tasks s/he wants to do or thinks s/he can carry out, taking into account the ultimate goal of achieving total work resumption: “It [multiple jobs, JS] was offered to me. But I made it clear that I want to combine two positions” (P6).
Self-direction behaviors can be accompanied by a “...positive feeling” (P5). By choosing which work activities they would like to do during their recovery, employees can feel positive about work participation and employability, and feel more valuable and useful. All interviewed employees considered self-direction as contributing to a suitable, personalized RTW-process that takes into account individual needs and wishes: “more freedom will be beneficial for a lot of people” (P16). For example, it would be easier for employees to work part-time at home, to achieve a better work-life balance: “If I could work at home a couple of days per week, that would be very beneficial for my work-life balance” (P16). They feel that this would contribute to their recovery and RTW.
Older employees (≥45 years) in particular self-directed their own work resumption frequently: “...The funny thing is, we are still working on it, that I probably will become a fulltime ICT employee. And I have initiated that completely” (P6). They generally dared to speak up to their supervisors. Younger employees were more likely to follow the preferences of their employer: “What they say goes” (P17).
Another employee mentioned that the situation changes over time. “Interviewer: So, can we say that your need for self-direction has grown since your illness took more and more time? Participant: Yes” (P17); “Yes, because she [supervisor] asked me last week about how long I thought it would take, a couple of weeks, months, years?” (P16). This employee reported that as a sickness absence extends, the need for self-direction increases as colleagues and supervisors tend to lose their patience. The employee’s first priority is to get better and then resume work (partially): “I dropped out for a good reason, and I have to work on that, to get better, to recover, healthy, cured … I am focused too much on work resumption, and I am not occupied with my own recovery” [participant expressed her dissatisfaction] (P15). Many interviewed employees mentioned that they were dissatisfied with their degree of autonomy. All study participants agreed that an autonomous choice, based on their abilities, competences, and skills, could possibly have resulted in a better and faster RTW.
4.2Proximal factors that play a role in self-direction
This section describes three proximal factors that may play a role in employees’ self-direction in RTW, involving the satisfaction of employees’ need for autonomy (section 4.2.1), competence (section 4.2.2), and relatedness (section 4.2.3).
4.2.1Autonomy: Decision latitude granted to absent employees by high-power stakeholders
During the interviews, hierarchical power during RTW and difference in power between the employee and the supervisor were frequently mentioned. Imposing influence by high-power stakeholders (the employer) appeared to be detrimental to satisfying the need for autonomy of sick-listed employees. Besides employers, multiple other stakeholders can influence the employees’ choice regarding RTW: “My supervisor, occupational physician, my parents, my friends, everyone has an opinion” (P16). In particular, high-powered stakeholders played an important role in the employees’ possibilities to self-direct their RTW. Several interviewees mentioned that high-power parties controlled their decision latitude concerning their work resumption.
First, because of a power imbalance between employees and their supervisors, employees reported feeling vulnerable in the relationships with their supervisors. The majority of employees reported being forced to return to work early by their supervisor or employer. Often, the RTW process went much faster than they would have wished. Employees first wanted to recover from their illness and then resume work. Unless they were not fully able to perform a task, they still reported to show up because they felt pressure from their supervisor: “They keep insisting … you are just pushed to that side” (P16). It seemed from our data analysis that pressure from supervisors to return to work diminished the participants’ general work motivation. Several interviewees suffering from mental health complaints reported to experience an episode of repeated sickness absence because they returned to work too early after their initial sickness absence or were saddled with too much work: “I have been saying that for almost a year. Till the moment I had to say no” (P16).
In almost every case, the supervisor asked the sick-listed employee about preferences regarding work resumption. Most participants reported that their supervisors told them that most of their preferences were unrealistic and that they just had to accept what their employer/supervisor wanted: “You have to do what everybody wants”; “In the end, it is just what they want” (P17). Some employees reported that their supervisors did not allow any personal input to facilitate work resumption. These employees noted that it was very hard and sometimes impossible for them to self-direct their work resumption.
Second, employees mentioned the varying degree of autonomy that their OPs allowed them to have. For example, an employee noted, “In the end it is the occupational physician who decides” (P7). Another employee mentioned, “The occupational physician thought that I should decide when I wanted to resume work” (P9). This suggests that stakeholders in the RTW process can influence the degree of autonomy an employee can express and experience.
Third, several employees thought that their medical specialist should allow more room for their perspectives: “Listen more to people. Do not draw conclusions for yourself. That is what I find the most important. That counts for the employer, but also for the orthopedic” (P9). The majority of the interviewed sick-listed people feel that they have to make conflicting decisions between work resumption and recovery. In many cases they need additional guidance and support with that. In general, sick-listed persons first want to recover and then resume work: “You can only resume work when you are done with all the medical processes” (P9). Guidance from medical professionals could be improved by supporting the employee more to find a better balance between recovery and work resumption.
Overall, many employees mentioned a need for more autonomy, particularly in relation to their supervisors. Some deliberately asked for help from their psychologist, relatives, or close friends regarding the balance between work resumption and recovery. The diversity of advice could make the situation for an employee worse: “Every person has an idea about what is good for you. And then it is quite hard to set your own course because you do not know it at all” (P16). Paradoxically, such employees needed some support with decision-making: “I needed a person who would slow me down, such a brake, someone who took over my direction” (P15). In some cases, the employees felt a lack of guidance. They experienced a lot of autonomy in their RTW process but were not able to use it properly. “I do not know, I just could not… I dropped out, but I have not recognized that that could be called a disease. Nobody has told me about that” (P6). This lack of guidance turned out to be a bottleneck for self-directing their RTW. In sum, employees reported a need to self-direct their RTW, but some expressed a lack of competence and knowledge to do so, which hampered them in actually self-directing their RTW.
4.2.2Competence: (un)certainty about recovery and health-related competences for work
Experiencing a sufficient degree of competence appeared to be a pre-condition for self-directing RTW. Many interviewees felt that they had insufficient knowledge and skills to self-direct their RTW process. In particular, employees who suffered from mental health conditions such as burnout or stress sometimes reported experiencing little competence to self-direct RTW. They mentioned many uncertainties; it was not clear when they would feel better and would be able to return to work. “Partially, eh, because … you cannot oversee the results of your choices. How will such a burnout develop? You cannot focus and that makes it hard to make decisions, especially when they are about yourself” (P16). It was impossible to schedule the work resumption, which made it very hard to develop an adequate work resumption plan.
It seemed from our data analysis that for persons with physical health complaints, it was less complicated to adapt their work tasks. For employers, it was clear that when an employee has a physical injury, s/he could not do the job. Usually, they were given another task: “They asked if I would like to do some adapted work, administration, and yes, that was fine” (P9). It seems that it is less complicated to guide employees with physical injuries. One reason might be the employers’ better understanding of the situation and what is involved.
4.2.3Relatedness: The availability of adequate support and feeling guilty towards colleagues
All interviewed employees had been in contact with several stakeholders during their sick leave and RTW, such as their supervisors, OPs, and/or general practitioners. Employees considered support by other stakeholders important for their RTW process: “I think it is a combination of occupational care, HR, the manager, and myself who have to discuss reintegration” (P15). However, our analysis showed that in some cases cooperation between stakeholders did not run smoothly, which resulted in a less than optimal RTW process.
For employees who experienced a lack of support by other stakeholders in the work resumption process, it remained unclear who should have given more advice or guidance. During the interviews, participants were hesitant to indicate who was responsible for that: their employer, their OP, or themselves. Interviewer: “Who is responsible for your work resumption?” Participant: “…[silence]…eh, my manager and the OP … [and I] eh, also, a bit”. This might also be due to differing health complaints and situations.
Some employees felt inhibited by the multitude of stakeholders and the amount of waiting time that elapsed between their request and the stakeholder’s answer (usually employer, OP, or other caregiver). As a result, employees reported they did not feel heard, which enhanced their feeling of being without guidance: “they should listen better to employees, what their needs are” (P17); “But they (employer) do not listen to that” (P3). As many employees expressed their need for guidance, and thus for relatedness, it is evident that the cooperation between stakeholders and the employee is an important contributor to self-direction. Employees also expressed complaints about a lack of communication and consultation between caregivers.
Most employees had good relationships with colleagues. Colleagues usually understood the situation and sometimes asked how the absent employee felt: “of course people understand it all” (P15). Some employees appreciated the attention received from colleagues during their episode of full sickness absence, while others did not want any contact with colleagues. The longer an employee had been absent from work (and particularly when an employee resumed work part-time), the more they experienced a growing exasperation from colleagues. In that time, many participants noted a rising incomprehension among colleagues. “And, but, the ease colleagues ask, “Could you just do this and that”, “It only takes ten minutes”, “hellooo, I am here for only four hours a day. In that time I cannot do that and that” (P15).
Another frequently mentioned issue was feeling guilty towards colleagues. Most employees felt guilty when on sickness absence: “I feel very guilty towards my colleagues because they have to bear all my work” (P15). Most interviewed employees wanted to do their best: “So then I did my best to inform people from home” (P16), to show their relatedness: “Only for my colleagues” (P2), and to cooperate in the RTW process: “You drop out because you are ill, and you have to get better of course, therefore you have to work hard on that!” (P16).
Besides autonomy and competence, relatedness is the third basic psychological need to stimulate a person’s motivation. To satisfy all three needs, employees are dependent on other people; therefore, we can state that the environment, or context, is important.
4.3Distal factors that play a role in self-direction: Legislation and organizational culture
Two contextual factors are relevant for employees’ self-direction in RTW: Return-To-Work legislation (section 4.3.1) and organizational culture (section 4.3.2).
4.3.1Legislation regarding return-to-work
Most participants reported knowing that Dutch legislation requires both employee and employer to contribute actively to the employees’ RTW. Study participants were most satisfied with the obligation to meet regularly with their employer. These meetings were a possibility for employees to discuss their RTW process and come up with ideas and express their preferences regarding work resumption. However, one employee found that the Gatekeeper Act inhibited self-direction in the RTW process because she thought that “Legislation stipulates this and this, and you have to work more and more hours, and you have to re-integrate” (P17). Another employee specifically mentioned the legal obligation to establish an action plan to achieve RTW. She experienced having a lot of influence in establishing her own plan and noted, “the action plan about reintegration is how I shape it. Now we use that as a kind of guideline” (P11). This refers to using the action plan to structure the RTW process. The difference between both quotes suggests differences in employees’ interpretation and understanding of the improved Gatekeeper Act. Some employees considered the legislation to be more useful than others.
4.3.2Organizational culture
Organizational culture can be described as “a pattern of basic assumptions, invented, discovered, or developed by a given organizational unit as it learns to cope with its problems of external adaptation and integral integration, that has worked well enough to be considered valid and, therefore, is to be taught to new members as the correct way to perceive, think, and feel in relation to those problems” [23]. Organizational culture may influence the possibility to self-direct RTW and therefore influence the quality and pace of work resumption.
One participant explicitly mentioned the bad culture in her department and the way she and her team suffered from that. “Eh, about five years ago, the culture was very stiff. Our manager was very harsh and dismissed people regularly. We had to work in a culture of fear” (P16). She also admitted that “my sickness absence had something to do with that [the culture/climate at the job]” (P16). The atmosphere among colleagues was tense; the participant particularly mentioned occasions of naming and shaming directed towards her. That was the major barrier for resuming work at the workplace. To fulfil her duties, she decided to work from home. But after six months of recovery and four months of work, she felt pressure from the director and the OP to resume her job in the office. “They thought the time has come [to go back to the office J.S.]. I have expressed my doubts. But at a certain moment you have to...” (P16). As this quote shows, she seemed to feel forced to comply, and after half a year, she reported ill and went on sick leave again.
In conclusion, employees from our study think of self-direction as making their own decision about RTW. Several proximal and distal environmental factors play a role in employees’ self-direction. Proximal factors involve satisfaction of the needs for autonomy, competence, and relatedness. Distal factors are organizational culture, legislation regarding RTW and clarity (or lack of it) regarding the roles of various stakeholders in the process of sickness absence and work resumption.
4.3.3Cooperation between stakeholders and the lack of clarity about their roles
All interviewees had been in contact with several stakeholders during their sick leave and RTW process. At first, this was their supervisor and in most cases also an OP, general practitioner, and a psychologist or social worker in the case of mental disorders. The majority of the participants considered themselves to be mainly responsible for their own RTW: “You have to put some effort into it [work resumption], you cannot just lean back… you must want to do it out of yourself” (P16). Nonetheless, other stakeholders are important people who can facilitate and improve the RTW process: “I think it is a combination of occupational care, HR, the manager, and myself who have to discuss reintegration” (P15). In some cases, the cooperation between stakeholders was problematic (e.g. power differences, lack of communication among caregivers, OP and the employer). This resulted in a less than optimal RTW process: Different caregivers provided different advice, specific to their profession and not adjusted to the employee’s situation: “They only think about a solution from their own expertise” (P12). As a result, employees felt a lack of guidance and did not know what to do or choose. They did not feel heard, which is detrimental to the satisfaction of their need for relatedness and competence: “they should listen better to employees, what their needs are” (P17); “But they (employer) do not listen to that” (P3). This underlines the poor cooperation among stakeholders; if a stakeholder does not listen to employees, their needs for autonomy and relatedness may not befulfilled.
In Fig. 2, the relationships between the most important concepts and their contribution to self-direction are presented.
Fig.2
Self-direction regarding work resumption and its underlying factors.
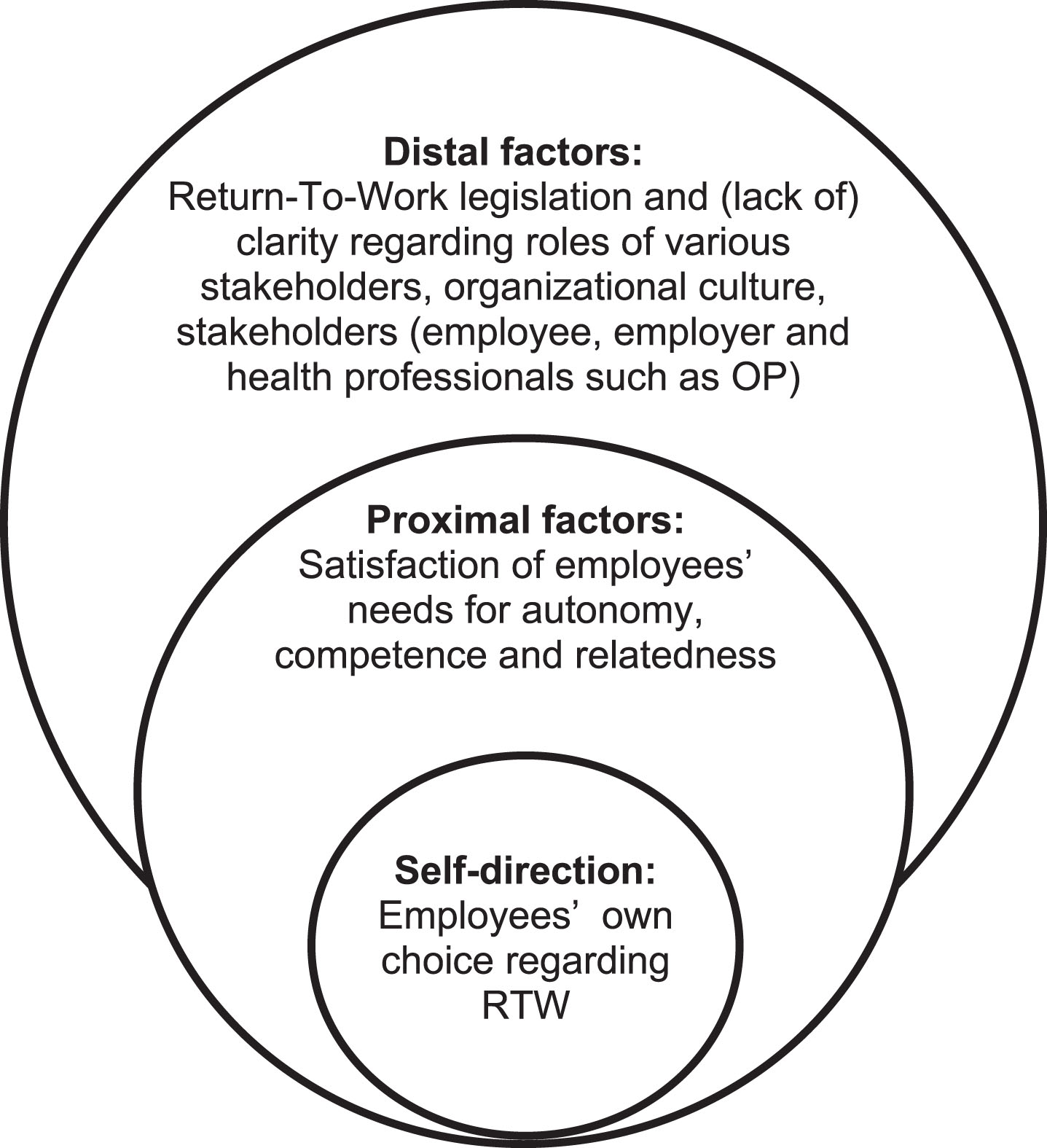
Self-direction is the core of the framework. Proximal factors influencing self-direction are the basic psychological needs of SDT. More distal factors are for example: legislation, organizational culture, and stakeholders involved in the RTW process.
5Conclusions
This study aimed to enhance our understanding of what sick-listed employees consider to be self-direction in a RTW context; and which factors may play a role in their self-direction. Interviews with 17 employees were analyzed thematically. Our results show that employees generally think of self-direction as being able to proactively decide about their RTW process regarding timing and tasks to do in an autonomous way, to reach intrinsically motivated decisions they are/feel responsible for. In addition, we found several proximal and distal environmental factors that may play a role in employees’ perceived self-direction. Proximal factors for self-directing RTW involve satisfaction of the need for autonomy, competence, and relatedness. Autonomy appears to be most salient to experiencing self-direction in RTW, and is likely to be supported by a context (environment) in which the opportunity to perform autonomous behavior is present. Feeling sufficiently competent may further enhance the motivation to self-direct RTW.
Relatedness seems to be a reflection of the organizational culture. When an employee has a good relationship with his/her employer, it is likely that the employer will provide some space and allow the employee to self-direct his/her own return to work. Distal factors are legislation regarding RTW and clarity (lack of it) regarding the roles of various stakeholders in the process of sickness absence and work resumption.
5.1Discussion
Overall, our study shows that for absent employees, self-direction means “making my own decision regarding RTW”. This general description of self-direction in RTW shows similarities to proactive goal generation [24]. Moreover, employees emphasized the importance of speaking up to their supervisors. This aspect of employees’ self-direction is somewhat similar to concepts such as “voice behavior” and “taking charge” [25, 26].
These similarities between employees’ self-direction in RTW and several proactivity concepts suggest that self-direction is something that employees can do on their own, without the support of other stakeholders. Yet, our findings particularly illustrate the important roles of other stakeholders (such as employers) in employees’ self-direction. For example, many interviewed employees emphasized that they wanted to resume their work as early as possible. Although this appeared to be part of their self-direction, it may also be exactly the opposite if their employers were forcing them to resume work early. Some of these employees may resume work too early and without resolving work-related bottlenecks (whether their employers pressured them into work resumption or not), which may result in recurrent sickness absence [27]. In line with Social Cognitive Theory, self-direction exists in a triadic relationship between personal factors, the influence of others (environment), and the actual RTW behavior [28]. SDT is useful for explaining proximal factors, while the Social Cognitive Theory is more helpful in explaining distal factors. Both theories might be helpful for researchers to better understand the motivation of sick-listed persons, and their (in)ability to self-direct their RTW process. Based on this understanding it may be possible for supervisors and professionals to better support employees during their RTW process.
Regarding the factors underlying employees’ self-direction, most employees emphasized the need for autonomy. This appeared to be the most salient factor contributing to their self-direction. Yet, our findings suggest individual differences in the strength of basic psychological needs. For example, employees with mental disorders such as burnout felt more vulnerable and reported needing more guidance from others (supervisors, OPs) regarding RTW due to their unpredictable medical recovery. Their need for autonomy might be less than that of employees with physical complaints, and they may need more empowerment by occupational health professionals and employers.
Older employees may be more inclined to self-direct their work resumption than younger ones. Most older participants in our study dared to speak up to their employer, while younger ones were more likely to comply with the employer’s demands even when that was contrary to their preferences. In line with socio-emotional selectivity theory, younger employees may feel particularly dependent on their employer to provide them with extrinsic rewards such as a promotion [29]. A lack of knowledge and skills may also lead to a diminished need and feeling of competence of younger employees to self-direct RTW. Older employees are likely to have more work experience and know the organization and its staff better. Having more knowledge may make them more assertive and willing to voice their preferences and ideas. This can lead to self-efficacy and greater feelings of autonomy during the RTW process.
5.2Methodological reflections
All participants lived in the southern part of the Netherlands, but they were employed in a variety of work sectors. This can be considered beneficial for the transferability of the results of this research. To enhance the quality of the data analysis, peer review was conducted. A random selection of transcripts was also peer-reviewed by other researchers (including outside the research team), who arrived at similar findings and interpretations of the data.
Another strength of this study was the interviewing method. The researcher was experienced in in-depth interviewing. Participants had the opportunity to tell their story, which provided rich data.
A limitation of this study is that we were only able to recruit three original interviewees for this study (which is why we had to use existing interviews from another research project). Explanations for this difficult recruitment could be time restrictions and the sensitive and personal nature of the topic under study. Many of the people contacted were not willing to distribute the information letter to potential participants. The existing transcripts were highly valuable, though, because similar topics were addressed. This resulted in a varied sample of 17 interviews.
5.3Recommendations for future research
We recommend conducting more qualitative research with larger and even more varied sample populations. This will provide the opportunity to study different sectors and, for instance, the role of employees’ seniority and place in the organization in exercising self-direction during return to work. It would be valuable to develop and validate a measurement scale for employees’ self-direction in RTW based on the results of this qualitative research, in order to conduct quantitative research in larger groups. This will enable the separate study of the degree of influence of every basic psychological need. Moreover, self-direction and its supporting factors could be studied further among specific populations such as employees who are on sick leave due to mental health complaints or certain chronic diseases.
5.4Recommendations for practice
Based on the results of this study, we can formulate several recommendations for RTW practice. First, high-power stakeholders such as employers need to be aware of their power over absent employees. They should enable sick-listed employees to take sufficient autonomy in order to encourage them and make room for self-directing RTW.
Interview participants with mental complaints mentioned that they sometimes needed help in making choices and taking decisions. The unpredictable nature of mental illness does not support the cooperation between employer and employee. A stumbling block for these employees is that they cannot promise anything to their employer because they do not know how the illness will develop (positively or negatively). This frequently results in a lack of understanding on the employer’s part. Therefore, it is advisable to do more research on how health professionals can support employees who suffer from mental complaints, especially in their communication with their employer.
Employees experience a need to self-direct their RTW, but some express a lack of competence to do so. These persons should be guided and empowered by external stakeholders like health professionals and OPs but also by people from their company. These stakeholders have the possibility to empower sick-listed employees and guide them during their RTW process.
With regard to cooperation between stakeholders, the employee, the employer (or its representative) and the OP were mentioned frequently. Previous research by Hoefsmit, Houkes, and Nijhuis [7] also indicated that these three stakeholders frequently work together since both employer and employee ask OPs forsupport and advice. It turned out that OPs were criticized less than employers by the employee. This indicates that in most cases the OP may be able to function as a suitable, unbiased intermediary in the regular meetings with the employee and employer.
It can be concluded that enabling employees to self-direct their RTW process and listening to their needs may be beneficial for a better work resumption. Every sickness-absence case is unique of course, but our findings are based on a varied sample of employees with different educational levels, working in a variety of jobs, and suffering from various health complaints. We therefore think this study has provided some valuable insights in the factors that may potentially support employees in taking self-direction in their RTW process. Support from health professionals and understanding from high-powered stakeholders seem to be relevant components for encouraging self-direction and facilitating better work resumption.
6Author information and contributions
JS (MSc) recently graduated from Maastricht University. He has finished the master program Work Health and Career and is still connected to Maastricht University. At the moment he is working as Safety and RTW employee at an international transport and logistics company. In this professional role, he is also involved in supporting absent employees to return-to-work.
For this study, he conducted three semi-structured interviews and made transcripts of them. He analyzed all of the transcripts used in this study. He wrote the first draft of this manuscript and adjusted it based on comments from the co-authors.
IH (PhD) is a health scientist working as an associate professor at the Department of Social Medicine, Maastricht University, The Netherlands (Faculty of Health, Medicine and Life Sciences). Her current research interests encompass various topics in the area of work and health as well as research methodology. She supervises PhD students who perform research in these areas and is (co-)author of various articles in these fields. In addition, she is involved as a lecturer in the bachelor programs Health Sciences, European Public Health, Health Sciences and Medicine and vice-director of the master programme Work, Health and Career at Maastricht University. She was involved in the design of this study, participated in the peer review process, and commented on earlier drafts of this manuscript.
NH completed a PhD on self-direction in return-to-work after sickness absence from Maastricht University. She works as an assistant professor at the Department of Work and Organizational Psychology, Faculty of Psychology and Educational Science, Open University, Heerlen, The Netherlands. She delivered the transcripts for this research, was involved in the design of this study, participated in the peer review process, and commented on earlier drafts of this manuscript.
Conflict of interest
The authors report no conflicts of interest.
Acknowledgments
The authors thank the interviewees for their participation and in particular for their openness and for sharing their RTW stories. We would also like to thank Emilie Wouda for participating in the peer review process.
References
[1] | Waddell G, Burton AK. Is work good for your health and well-being. London; (2006) . |
[2] | Mowlam A, Lewis J. Exploring how general practitioners work with patients on sick leave: A study commissioned as part of the’Job Retention and Rehabilitation Pilot’ evaluation. (2005) . |
[3] | Overheid.nl. Wet verbetering poortwachter [Internet]. (2017) [cited 2017 Jan 25]. Available from: https://wetten.overheid.nl/BWBR0013063/2008-11-01 |
[4] | Ministerie van Sociale zaken en Werkgelegenheid. Wet verbetering poortwachter [Internet]. [cited 2019 Feb 16]. Available from: https://www.arboportaal.nl/onderwerpen/wet-verbetering-poortwachter |
[5] | Hoefsmit N, Boumans NPG, Houkes I. Eigen regie over werkhervatting bij verzuimende werknemers. Unpublished manuscript; (2017) . |
[6] | Hoefsmit N. Self-Direction in Return-to-Work: Bottlenecks, facilitators and an intervention [dissertation]. Maastricht, NL; Maastricht University; (2015) . |
[7] | Hoefsmit N, Houkes I, Nijhuis F. Environmental and personal factors that support early return-to-work: A qualitative study using the ICF as a framework. Work. (2014) ;48: (2):203–15. |
[8] | RyanR, DeciE. Self-determination theory and the facilitation of intrinsic motivation. Am Psychol. (2000) ;55: (1):68–78. |
[9] | Sheldon KM, Gunz A. Psychological needs as basic motives, not just experiential requirements. J Pers. (2009) ;77: (5):1467–92. |
[10] | Parker SK, Bindl UK, Strauss K. Making things happen: A model of proactive motivation. J Manage. (2010) ;36: (4):827–56. |
[11] | Deci EL, Ryan RM. The “ What ” and “ Why ” of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. (2000) ;11: (4):227–68. |
[12] | Deci EL, Ryan RM. Intrinsic motivation and self-determination in human behavior. New York: Plenum; (1985) . |
[13] | Van den Broeck A, Ferris DL, Chang CH, Rosen CC. A review of self-determination theory ’ s basic psychological needs at work. J Manage. (2016) ;42: (5):1195–229. |
[14] | Baumeister RF, Leary MR. The need to belong: Desire for interpersonal attachments as a fundamental the need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol Bull. (1995) ;117: (3):497–529. |
[15] | Kirsh B. Work, workers, and workplaces: A qualitative analysis of narratives of mental health consumers. J Rehabil. (2000) ;66: (4):24–30. |
[16] | White RW. Motivation reconsidered: The concept of competence. Psychol Rev. (1959) ;66: (5):297–333. |
[17] | Deci EL, Ryan RM. Facilitating optimal motivation and psychological well-being across life’s domains. Can Psychol. (2008) ;49: (1):14–23. |
[18] | UWV. Ik ben ziek (loondoorbetaling, ziektewet, WIA, WAO, WAZ) [Internet]. 2019 [cited 2019 Dec 4]. Available from: https://www.uwv.nl/particulieren/ziek/index.aspx |
[19] | Sweet SN, Fortier MS, Strachan SM, Blanchard CM. Testing and integrating self-determination theory and self-efficacy theory in a physical activity context. Can Psychol. (2012) ;53: (4):319–27. |
[20] | Bandura A. Self-efficacy: The exercise of control. New York: Freeman; (1997) . |
[21] | Lee L, Arthur A, Avis M. Using self-efficacy theory to develop interventions that help older people overcome psychological barriers to physical activity: a discussion paper. Int J Nurs Stud. (2008) ;45: :1690–9. |
[22] | Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) ;3: (2):77–101. |
[23] | Schein EH. Organizational culture. Am Psychol. (1990) ;45: (2):109–19. |
[24] | Parker SK, Bindl UK, Strauss K. Making things happen: A model of proactive motivation. J Manage. (2010) ;36: (4):827–56. |
[25] | Van Dyne L, LePine J. Helping and voice extra-role behaviors: Evidence of construct and predictive validity. Acad Manag J. (1998) ;41: (1):108–19. |
[26] | Van Dyne L, Cummings L, Parks J. Extra-role behaviors: In pursuit of construct and definitional clarity. Research in Organizational Behavior. (1995) , pp. 215–85. |
[27] | Arends I, van der Klink JJL, van Rhenen W, de Boer MR, Bültmann U. Prevention of recurrent sickness absence in workers with common mental disorders: Results of a cluster-randomised controlled trial. Occup Environ Med. (2014) ;71: (1):21. |
[28] | Bandura A. Health promotion from the perspective of social cognitive theory. Psychol Health. (1998) ;13: (4):623–49. |
[29] | Carstensen LL, Isaacowitz DM, Charles ST. Taking time seriously. Am Psychol. (1999) ;54: (3):165–81. |


