
Vanishing bone tumor (Gorham-Stout syndrome): A case report
Abstract
Gorham-Stout syndrome/Vanishing bone tumor also known by a dozen other eponyms is an extremely rare disorder of the musculoskeletal system reported first in 1938 by Jackson and later detailed description was given by Gorham and Stout. Since then about 200 cases of this disorder have been reported. Gorham-Stout syndrome is a poorly understood disorder of abnormal lymphovascular proliferation resulting in a localized bone loss, usually painless unless complicated by a pathological fracture and usually involving the proximal humerus (most common),shoulder girdle, pelvis, skull and mandible.
In our case, a 50 year old female presentedwith a 2 year history of pain and restriction in movements involving the left shoulder for which a skiagram revealed marked bone loss. Further investigations including MRI and Tc 99 bone scan were also affirmative. Biopsy revealed lymphovascular ectasia. The patient, diagnosed as a case of Stout syndrome, was managed with removal of the involved portion of proximal humerus and shoulder hemiarthroplasty. Post operatively the patient was put on bisphosphonates and recovered remarkably well. A high index of suspicion is required while managing a case of osteolytic lesions of bone. However due to limited available literature regarding this entity the prognosis and treatment protocols are yet to be established.
1Introduction
Gorham-Stout syndrome is a very rare disorder characterized by uncontrolled proliferation of vascular or lymphatic capillaries within bone and surrounding soft tissue. It was first described by Jackson and detailed description was given by Gorham and Stout [1] in 1955. Since then about 200 cases have been reported.The disease is usually found afflicting the proximal humerus [2], the shoulder [3] and pelvic girdle [4], skull [5] and mandibular region [6]. Most cases occur in children and young adults (usually less than 40 years of age). No definite inheritance pattern has been reported.The patients usually present with history of prolonged dull aching pain of the involved area often associated with some signs of associated disuse atrophy of muscles. Diagnosis is often delayed in most cases due to its rarity. A high index of suspicion is required and radiological and laboratory parameters combined with histopathological examinations is required to make an early accurate diagnosis, ruling out all other possible diagnoses as the disease itself is a diagnosis of exclusion. Due to limited available literature regarding the entity, treatment concensus has not been established. Some authors have advocated excision with sturt grafting/prosthesis, others advocate medical management in the form of anti resorptive therapy like bisphosphonates [7], radiation therapy [8] and alpha interferon. Spontaneous resolution of the lesion is also seen [9]. The prognosis of the disease is variable. While some lesions heal on their own, others may progress to involve the whole bone. In this report, informed written consent for print and electronic publication was obtained.
Fig.1
Clinical picture showing flattening of left shoulder contour.

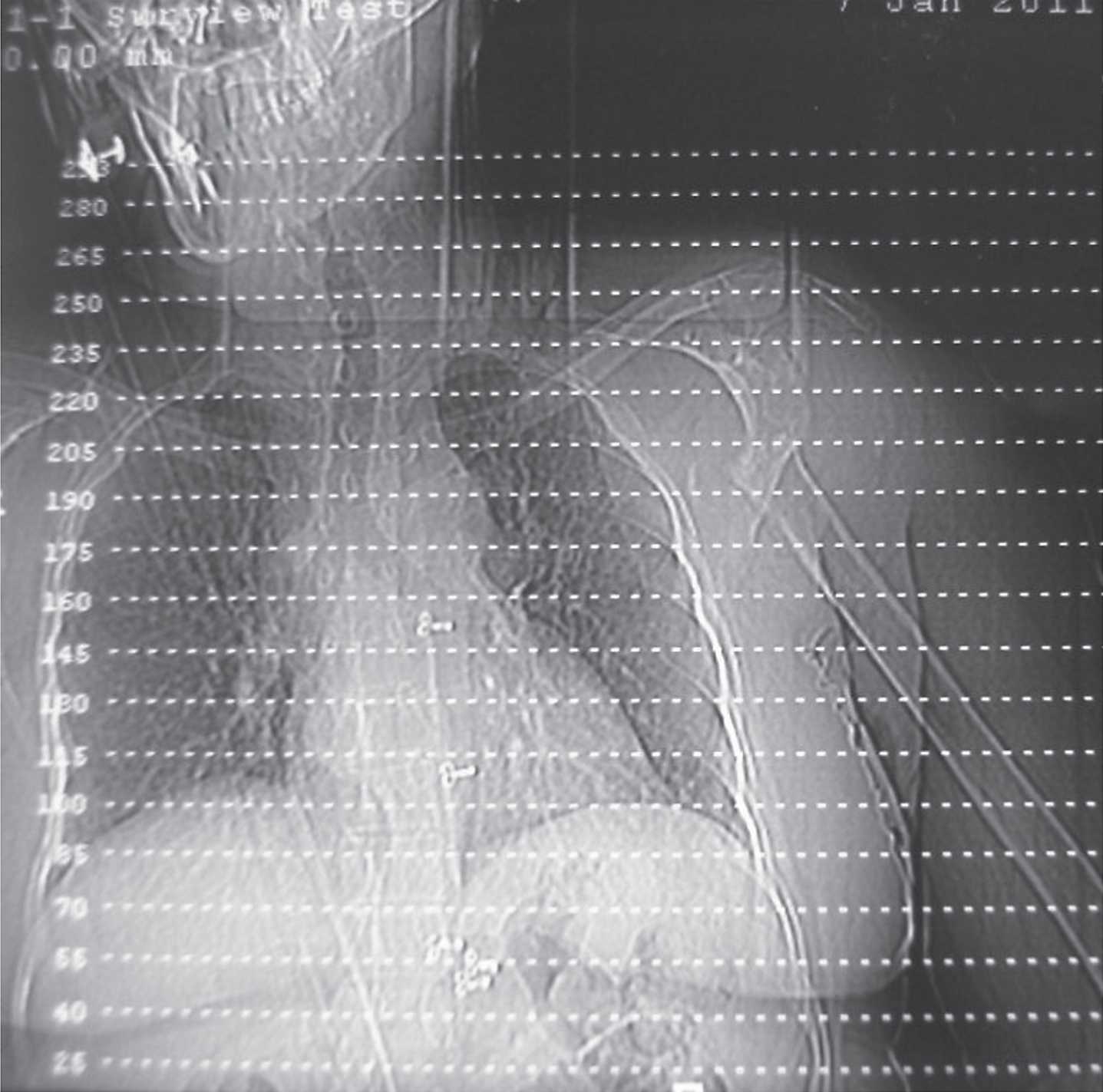
Fig.2
Xray showing bone resorption over the proximal humerus area.
2Case report
A 50 year-old woman presented with a history of vague dull aching pain involving the left shoulder and a feeling of grittiness on left shoulder movements for 2 years with no antecedent history of trauma, fever, weight loss, or loss of appetite. The patient was unable to do her daily chores and received treatment from many doctors in the form of oral analgesics. Local examination revealed significant muscle wasting. Instability of the shoulder joint was present and active movements were limited in all planes, more so in abduction which was restricted to less than 30 degrees.
Fig.3
3D- CT Reconstruction of the left shoulder showing absorption of the proximal humeral head globally with proximal migration of the shaft of humerus.
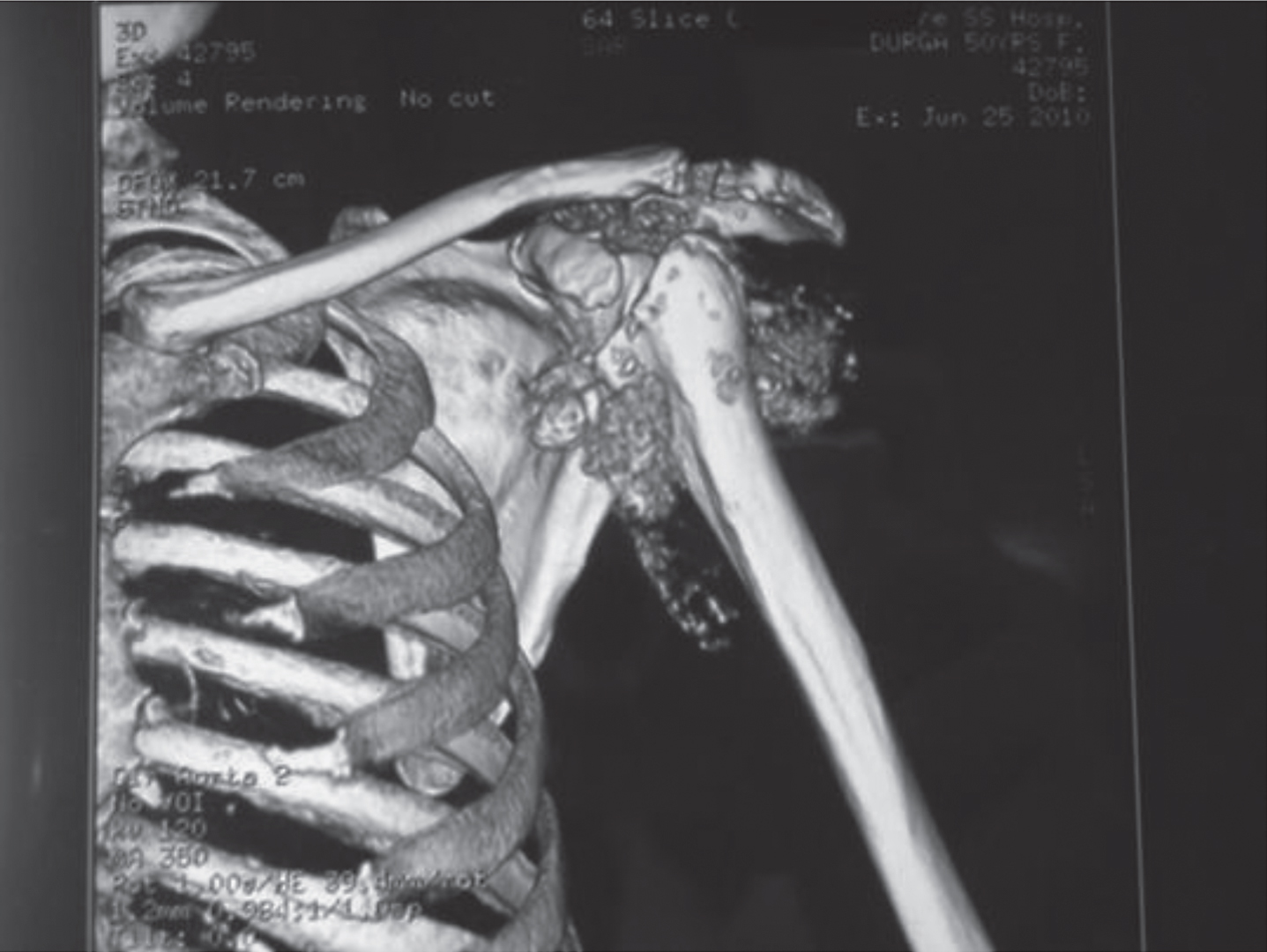
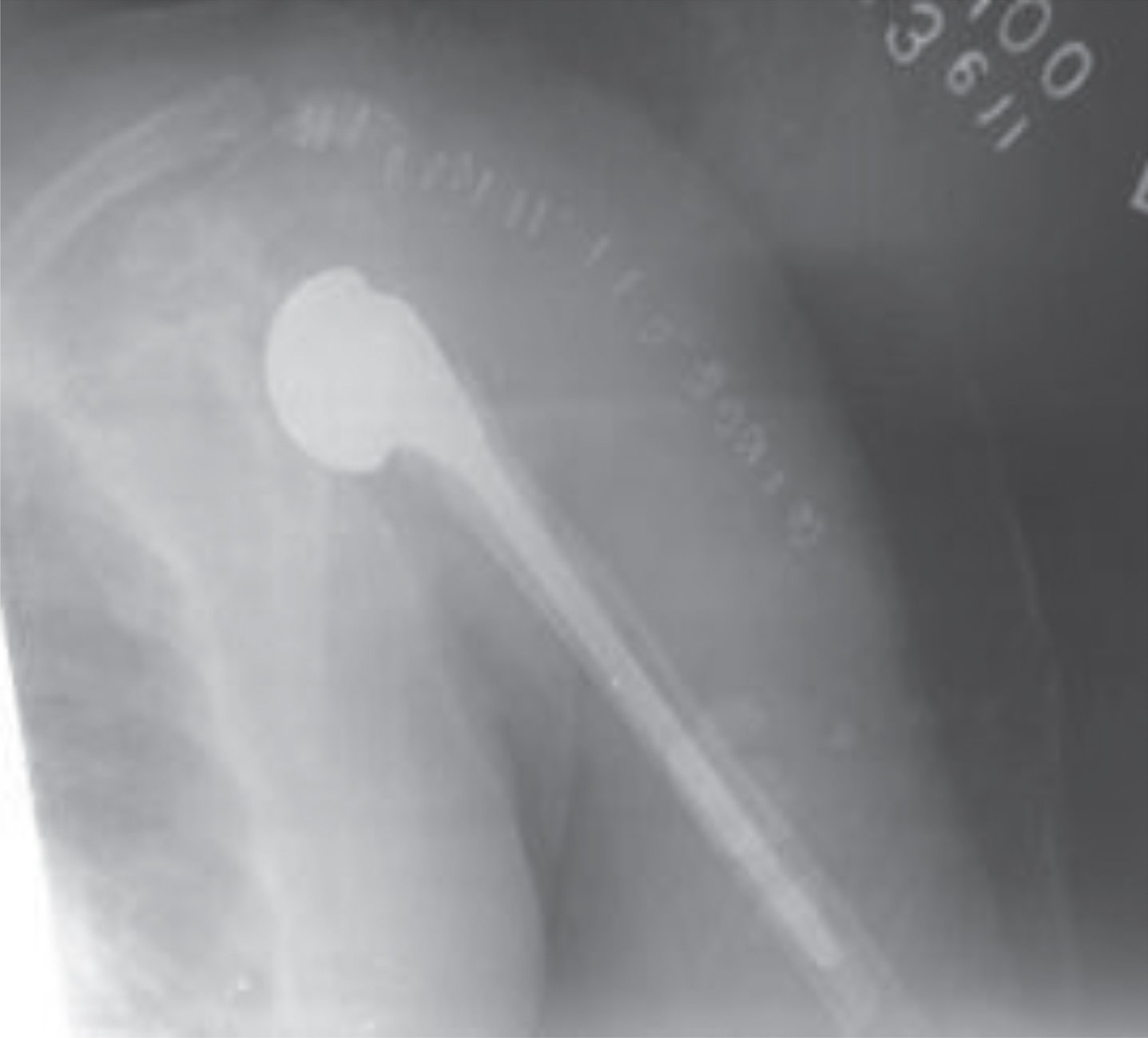
Fig.4
Post-op xray showing cemented proximal humerus prosthesis.
A skiagram was done which revealed absorption of the proximal humerus along with parts of the glenoid and acromion. This is one of the few characteristic of this lesion i.e. it has no respect for boundaries but unlike a metastatic lesion, has fewer clinical manifestations. This skiagram prompted us to investigate the patient further. A CT was done which revealed similar osseous bone loss. An MRI revealed low intensity signals on T1 signifying bone loss and hyperintensity on T2 signifying vascular proliferation. A Tc 99 labelled bone scan revealed increased uptake in the initial images signifying vascularity followed by decreased uptake in remaining phases of the scan corresponding to the bone loss. Biopsy of the lesion revealed proliferative fibrous tissue with areas of increased vascularity and few dead bony fragments along with skeletal muscle and hemorrhage, without evidence of any hereditary, metabolic, neoplastic or infectious etiology.
The patient was managed by thorough surgical excision of the lesion and implantation of a cemented proximal humeral prosthesis using a prolene mesh to keep the prosthetic humeral head in place in the shallow and deformed glenoid cavity. Post operatively the patient was placed on oral bisphosphonate therapy. After one year follow-up, the patient has a pain-free, stable shoulder joint without the gritty sensation. Range of movements has improved to more than 50% of the pre-operative range.
3Discussion and conclusion
Gorham-Stout syndrome is a rare musculoskeletal disorder. Its diagnosis is usually delayed and often missed as not many physicians have the opportunity to treat this rare disease entity. The etiology of Gorham Stout syndrome is unknown. The disease affects usually young adults similar to other cystic bony lesions. Its clinical presentation is variable, largely depending upon the site of skeletal involvement. However, the disease should be kept mind while we are dealing with osteolytic lesions. One other thing to be kept in mind is the lack of respect for boundaries and contiguous spread that is its characteristic. Diagnosis is based on both radiological and histopathological investigations. Laboratory blood investigations seldom have any role. other than to rule out other differential diagnoses. Limited available literature on this condition has resulted in lack of specific treatment plans. Some manage this condition with excision and sturt grafting/prosthesis, others have opted for medical therapy in the form of bisphosphonates or alpha interferons. Radiation therapy alone has also been used. In this case report, we have employed combined surgical and medical management for this condition.
In conclusion, patients who present with osteolysis of the shoulder or pelvic girdle, skull or mandible should undergo a thorough clinical examination coupled with radiological, laboratory, and histopathological investigations to provide an accurate early diagnosis of this incompletely understood condition, to estimate its occurrence, and to ascertain its prognosis.
References
[1] | Gorham L.W. and Stout A.P. , Massive osteolysis (acute spontaneous absorption of bone, phantom bone, disappearing bone): Its relation to hemangiomatosis, J Bone Joint Surg [Am] 37-A: ((1955) ), 985–1004. |
[2] | Poirier H. and Massive osteolysis of the humerus treated by resection and prosthetic replacement, J Bone Joint Surg [Br] 50-B: ((1968) ), 158–160. |
[3] | Sacristan H.D. , Portal L.F. , Castresana F.G. and Pena D.R. , Massive osteolysis of the scapula and ribs: A case report, J Bone Joint Surg [Am] 59-A: ((1977) ), 405–406. |
[4] | Dan’ura T. , Ozaki T. , Sugihara S. , Taguchi K. and Inoue H. , Massive osteolysis in the pelvis – a case report, Acta Orthop Scand 69: ((1998) ), 197–198. |
[5] | Iyer V. and Nayar A. , Massive osteolysis of the skull: Case report, J Neurosurg 43: ((1975) ), 92–94. |
[6] | Black M.J. , Cassisi N.J. and Biller H.F. , Massive mandibular osteolysis, Arch Otolaryngol 100: ((1974) ), 314–316. |
[7] | Hagberg H. , Lamberg K. and Astrom G. , Alpha-2b interferon and oral clodronate for Gorham’s disease, Lancet 350: (9094) ((1997) ), 1822–1823. |
[8] | Dunbar S.F. , Rosenberg A. , Mankin H. , Rosenthal D. and Suit H.D. , Gorham’s massive osteolysis: The role of radiation therapy and a review of the literature, Int J Radiat Oncol Biol Phys 26: ((1993) ), 491–497. |
[9] | Campbell J. , Almond H.G. and Johnson R. , Massive osteolysis of the humerus with spontaneous recovery, J Bone Joint Surg [Br] 57-B: ((1975) ), 238–240. |


