
A deep learning approach for acute liver failure prediction with combined fully connected and convolutional neural networks
Abstract
BACKGROUND:
Acute Liver Failure (ALF) is a critical medical condition with rapid development, often caused by viral infections, hepatotoxic drug abuse, or other severe liver diseases. Timely and accurate prediction of ALF occurrence is clinically crucial. However, predicting ALF poses challenges due to the diverse physiological differences among patients and the dynamic nature of the disease.
OBJECTIVE:
This study introduces a deep learning approach that combines fully connected and convolutional neural networks for effective ALF prediction. The goal is to overcome limitations of traditional machine learning methods and enhance predictive model performance and generalization.
METHODS:
The proposed model integrates a fully connected neural network for handling basic patient features and a convolutional neural network dedicated to capturing temporal patterns in patient data. The combination allows automatic learning of complex patterns and abstract features present in highly dynamic medical data associated with ALF.
RESULTS:
The model’s effectiveness is demonstrated through comprehensive experiments and performance evaluations. It outperforms traditional machine learning methods, achieving 94.8% accuracy and superior generalization capabilities.
CONCLUSIONS:
The study highlights the potential of deep learning in ALF prediction, emphasizing the importance of considering individualized medical factors. Future research should focus on improving model robustness, addressing imbalanced data, and further exploring personalized features for enhanced predictive accuracy in real-world clinical scenarios.
1.Introduction
Acute Liver Failure (ALF) is a critical medical condition typically caused by viral infections, hepatotoxic drug misuse, or other severe liver diseases [1]. As the liver functions as a central organ in metabolism, detoxification, and synthesis of essential proteins, any impairment to its normal functioning can lead to cascading effects with severe consequences for the entire body. Its rapid and critical progression underscores the utmost clinical significance of timely and accurate prediction of whether a patient is at risk of developing acute liver failure.
Acute Liver Failure stands as a formidable global health challenge, exerting a profound impact on populations across the world. In an era where health challenges transcend borders, ALF emerges as a poignant illustration of the interconnectedness of global health. Its intricate web extends beyond individual patient experiences, intertwining with broader public health concerns. The consequences of inadequate ALF management reverberate far beyond individual healthcare systems, making it imperative to approach this condition with a global perspective. As we delve into a comprehensive exploration of ALF prediction, it is with the understanding that our endeavors are integral to the broader tapestry of global health.
The prediction of acute liver failure has consistently posed a highly challenging task in the medical field. The development of acute liver failure is influenced by various chronic diseases such as hypertension and diabetes, resulting in complex and diverse physiological differences among patients [2]. Additionally, acute liver failure itself presents with multiple clinical symptoms, including decreased cardiac contractile function, fluid retention, and fatigue [3]. This diversity complicates the prediction task, where features to be considered exhibit both temporal and dynamic characteristics. Modern medicine, emphasizing personalized healthcare, further increases the adaptation difficulty of predictive models to data complexity by necessitating a comprehensive consideration of patients’ basic physiological characteristics, medical history, and medication usage [4]. The interplay of these complex factors presents a significant challenge to the accurate prediction of acute liver failure [5]. Therefore, constructing an efficient and accurate predictive model under the consideration of physiological differences, clinical diversity, and personalized healthcare becomes an urgent and formidable task in the medical field. Patients grappling with this critical medical condition not only seek accurate predictions but also harbor expectations for more personalized and effective healthcare services. The importance of our research lies not only in advancing predictive models but also in directly impacting patient outcomes and quality of life.
Traditional machine learning methods face limitations in dealing with the prediction of acute liver failure [6]. These methods often rely on manually extracted features, making it challenging to capture dynamic changes and underlying patterns between different features. Due to the highly dynamic and temporal nature of acute liver failure data, traditional approaches may struggle to effectively mine this information, subsequently affecting the accuracy of predictive models.
To address these challenges, this paper introduces deep learning methods, specifically a combination of fully connected neural networks and convolutional neural networks. Fully connected neural networks handle patients’ basic feature information, while convolutional neural networks are specialized in capturing temporal patterns within patient data. Through this deep learning model, we can automatically learn complex patterns and abstract features from the highly dynamic medical data associated with acute liver failure.
Our paper aims to propose an effective predictive model to more accurately identify patients at risk of acute liver failure. By introducing deep learning methods, we aim to overcome the limitations of traditional approaches, enhancing the performance and generalization capability of predictive models. Our research aims to provide robust support for early diagnosis and intervention in acute liver failure, offering more precise guidance for patient health and medical care.
2.Related work
In the field of acute liver failure prediction, researchers have dedicated efforts to enhance model performance and accuracy, employing various methods including traditional machine learning and deep learning. The following is a detailed discussion of relevant work:
2.1Traditional machine learning methods
In previous studies, scholars extensively utilized traditional machine learning algorithms for predicting acute liver failure. These methods encompass logistic regression, support vector machines (SVM), decision trees, among others. By manually extracting patients’ basic features, such as physiological indicators, models undergo learning and prediction [7]. However, these methods may face limitations in handling highly dynamic and temporally strong data associated with acute liver failure [8], making it challenging to capture complex temporal relationships within the data.
2.2Deep learning methods
With the rise of deep learning, researchers started incorporating neural networks and other deep learning methods to address acute liver failure prediction. Fully connected neural networks [9] and convolutional neural networks [10] became focal points. Fully connected neural networks handle basic feature information, while convolutional neural networks are specifically designed to capture temporal patterns. This deep learning approach is better suited for the highly dynamic medical data associated with acute liver failure, allowing for automatic learning of complex patterns and abstract features [11].
2.3Model ensemble strategies
To enhance the overall performance of models, researchers adopted model ensemble strategies [12]. By integrating outputs from different models to form the final prediction result, they aimed to find a better balance amidst the various complexities in the data. This strategy aims to leverage the strengths of individual models, thereby improving overall predictive performance.
2.4Exploration of novel prediction methods
In addition to traditional methods and deep learning, researchers also explored novel prediction methods. For instance, customized models based on individualized healthcare factors [13], considering patient histories, lifestyles, and other individual differences, have enhanced the accuracy of models in predicting acute liver failure. This personalized approach introduces more precise information into predictive models, better meeting clinical practical needs.
In summary, early-stage research in the field of acute liver failure prediction has employed various methods, including traditional machine learning, deep learning, model ensemble, and exploration of novel prediction methods. This paper aims to propose a more innovative and effective acute liver failure prediction model by combining deep learning methods with individualized healthcare factors and further exploring novel prediction methods. The introduction of deep learning, the discussion of model ensemble strategies, and the focus on novel prediction methods provide new directions and insights for improving the performance of predictive models.
3.Method
Acute liver failure is often associated with various factors, prompting the collection of diverse patient indicators for prediction. These include age, gender, weight, obesity status, blood pressure, cholesterol levels, hepatitis status, and family history of hepatitis.
Predicting acute liver failure is a complex and challenging task involving multiple patient characteristics and their interrelationships. Traditional machine learning methods, such as logistic regression and decision trees, while capable of handling multidimensional features to some extent, may encounter issues like insufficient predictive performance and inadequate feature extraction when dealing with highly dynamic and temporally strong disease data like acute liver failure [14]. To address these challenges, we introduce deep learning methods, specifically employing a combination of fully connected neural networks and convolutional neural networks. Deep learning models can automatically learn complex patterns and abstract features from data, adapting better to the nonlinear and highly dynamic nature of medical data.
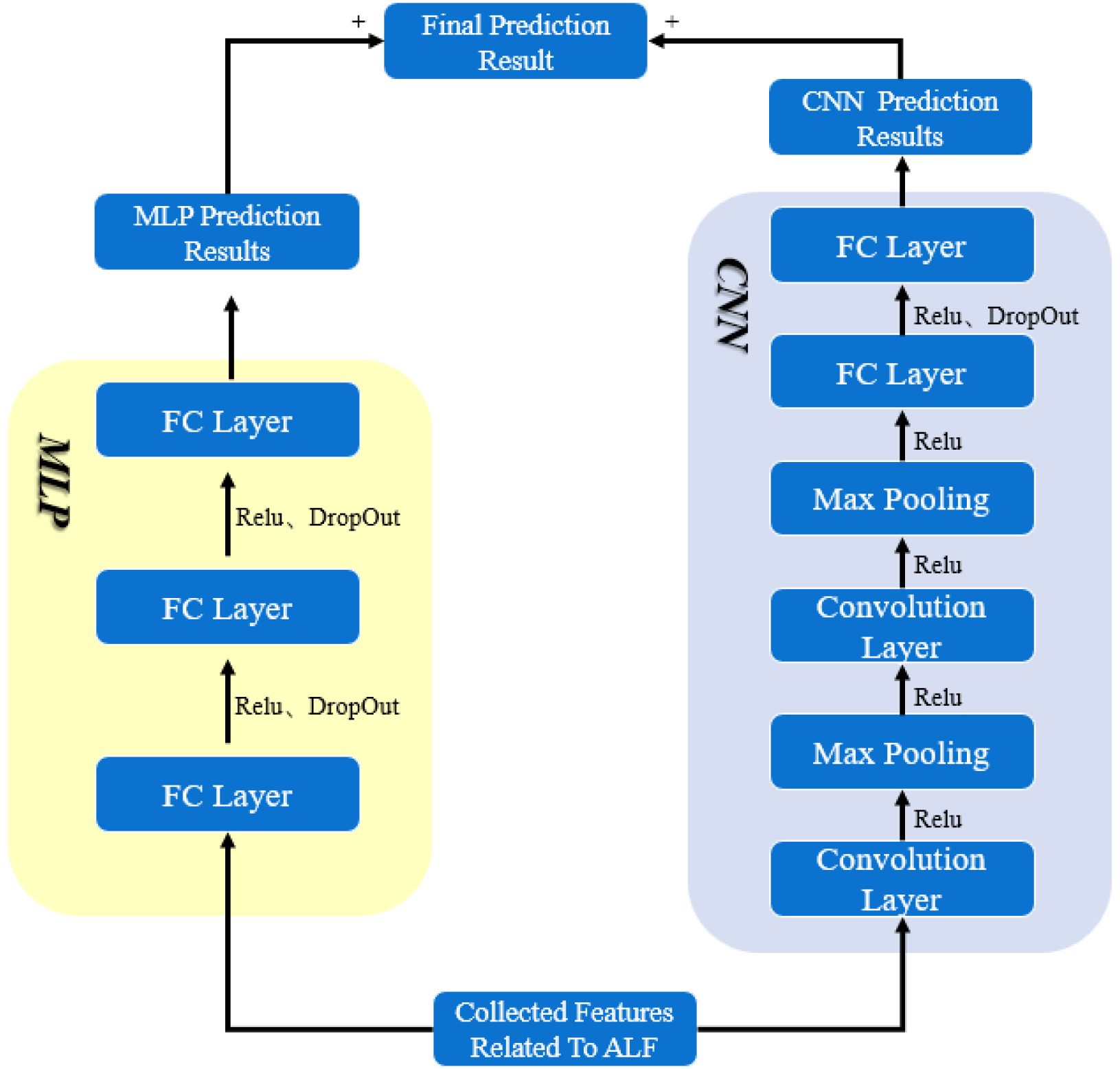
The fully connected neural network excels at processing basic patient features, providing a detailed understanding of individual characteristics. Simultaneously, the convolutional neural network specializes in capturing temporal patterns, enabling the model to discern complex and dynamic relationships within the ALF data. Operating in parallel, the fully connected and convolutional neural networks contribute unique strengths to the model. The model ensemble strategy, which averages the outputs of both networks, synergizes their interpretative and pattern-capturing advantages, mitigating errors and enhancing overall predictive performance. We leverage the advantages of both fully connected neural networks and convolutional neural networks to address the challenges encountered in predicting acute liver failure.
3.1Fully connected neural network
The fully connected neural network is a fundamental structure in deep learning, with each neuron connected to all neurons in the previous layer. In this study, we selected a fully connected layer containing 128 neurons to process basic patient feature information. This layer utilizes the Rectified Linear Unit (ReLU) activation function to map the linear combination of inputs to a nonlinear space, aiding in extracting higher-order features. ReLU is a commonly used activation function, expressed as f(x)=max(0,x), introducing nonlinearity to help the neural network better fit complex functions.
3.2Convolutional neural network
The convolutional neural network is designed specifically for processing grid-like structured data in deep learning models. In this study, a one-dimensional convolutional neural network was employed to better capture temporal patterns within patient data. The alternating arrangement of convolutional and pooling layers gradually reduces the size of feature maps and extracts important temporal features. Pooling layers, utilizing either max pooling or average pooling, progressively reduce feature map dimensions, retaining crucial information. In the final layer of the convolutional neural network, a Sigmoid activation function is applied to map the extracted advanced temporal features to a single neuron, producing a probability value between 0 and 1. Sigmoid is commonly used for binary classification problems, constraining the output within the 0 to 1 range for probability interpretation.
3.3Model ensemble
The fully connected neural network and convolutional neural network operate in parallel within the model, each extracting features and generating prediction probabilities. To better leverage the strengths of both, a model ensemble strategy is employed. The final prediction result is formed by averaging the outputs of both models. This approach combines the interpretative advantage of the fully connected neural network with the temporal pattern capturing advantage of the convolutional neural network, to some extent mitigating errors from each model. During model training, the Binary Cross-Entropy Loss (BCELoss) is used to measure the difference between the model output and true labels, common for binary classification problems. The Adam optimizer, chosen for its adaptive learning rate characteristics, facilitates faster convergence in optimizing model parameters.
Through the combination of these deep learning methods, we have constructed a more intricate predictive model capable of better understanding and utilizing patient data. The specific model diagram is illustrated in Fig 1.
Figure 1.
Combined prediction model for acute liver failure using fully connected neural network and convolutional neural network.
4.Experiment
To construct and evaluate the acute liver failure prediction model, we divided the dataset into training and validation sets in a 7:3 ratio. The validation set remained unchanged throughout the entire process, not participating in any data processing or model training stages, and was solely used for the final model performance validation. Utilizing the validation set during model evaluation allows for a comprehensive assessment of the model’s generalization ability. The performance on the validation set directly reflects the predictive effectiveness of the model on unseen data.
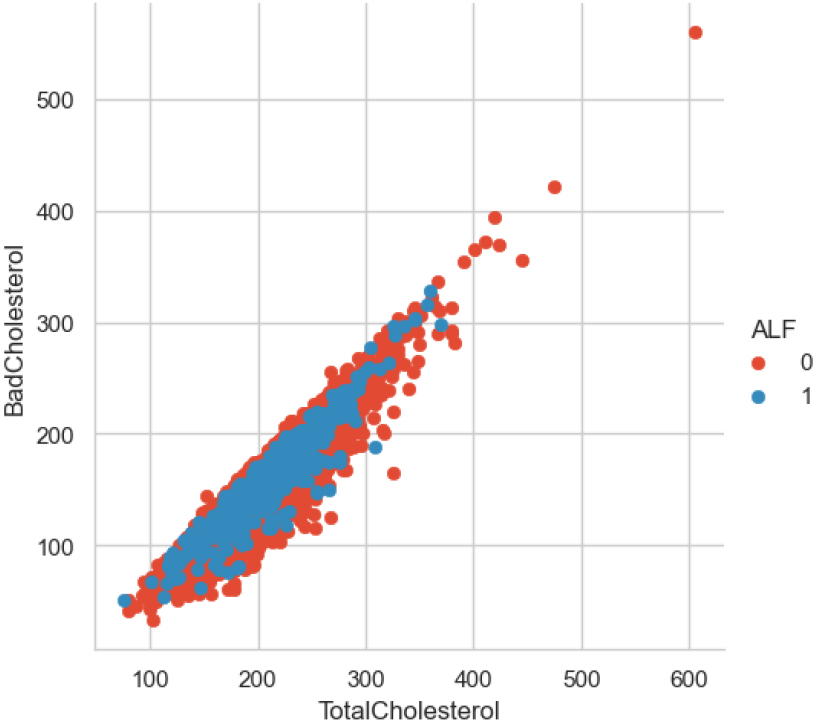
To gain a better understanding of the impact of different clinical data on acute liver failure, we conducted detailed data exploration. By plotting scatter plots for several key variables, we aimed to identify potential correlations and outliers, as depicted in Figs 2 and 3. Building upon Figs 2 and 3, we performed outlier removal to enhance data quality. By identifying and excluding noise values deviating from the normal range, we improved data quality and reduced the risk of model overfitting to abnormal data. This step contributes to enhancing the model’s robustness, enabling it to better adapt to real clinical scenarios.
Figure 2.
Scatter Plot of GoodCholesterol.
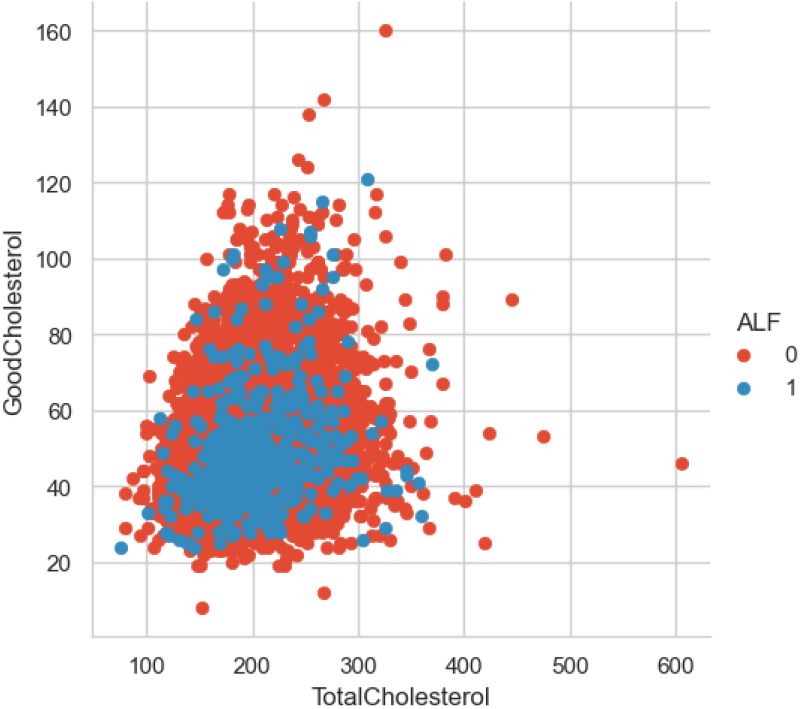
Figure 3.
Scatter Plot of BadCholesterol.
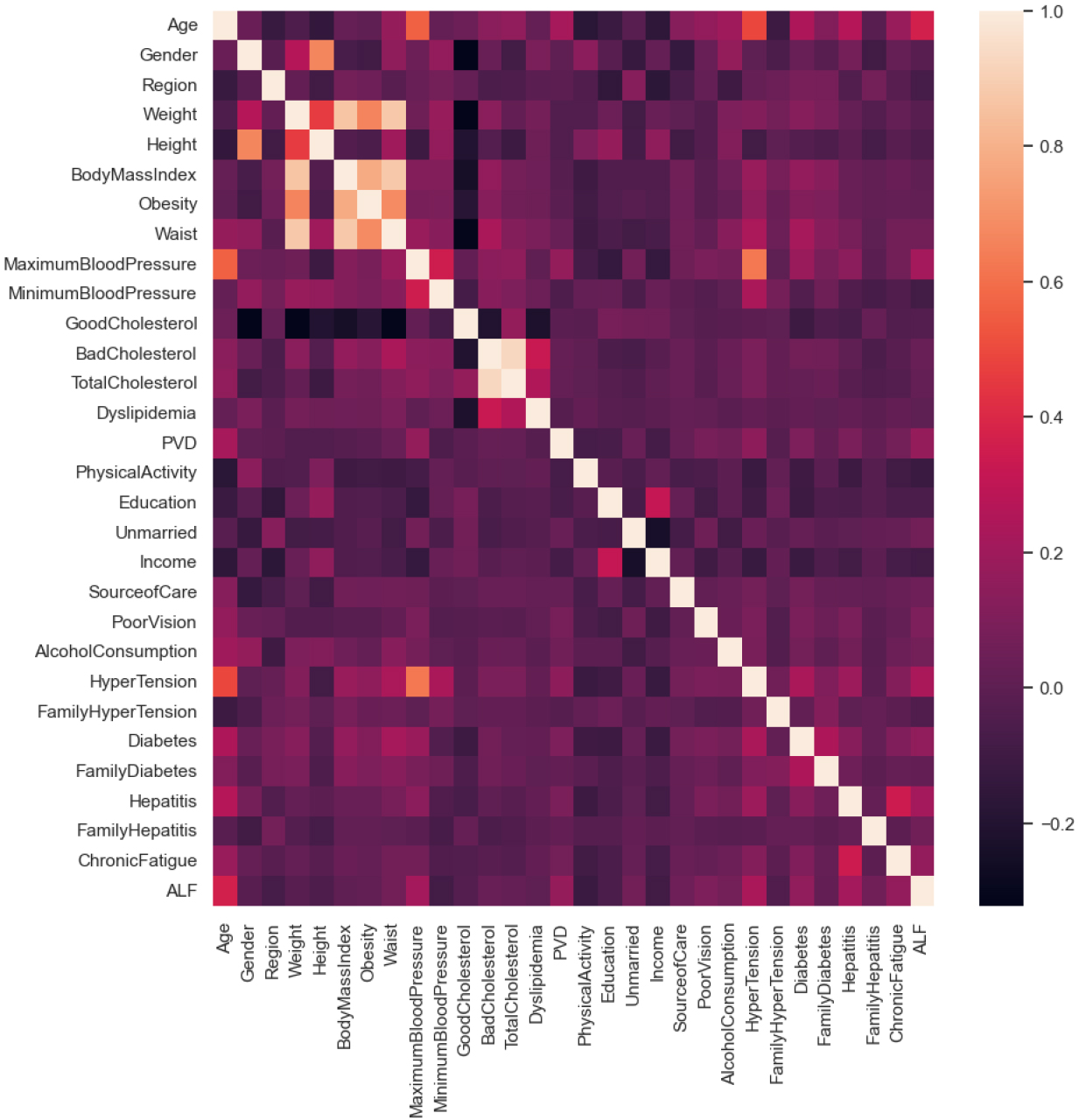
In addition to outlier handling, we conducted a correlation analysis of patient information. Figure 4 allowed us to identify data with higher correlations, facilitating data fusion. Merging highly correlated data simplifies model training, reduces feature dimensions, and enhances the model’s efficiency and generalization ability.
Figure 4.
Correlation analysis chart of patient information in acute liver failure.
Finally, we performed normalization on the data. By eliminating scale differences between features, we effectively improved the training performance of the model. This preprocessing approach provides a more robust training foundation for deep learning models, aiding in better learning and adaptation to patients’ physiological characteristics.
During model training, we chose Binary Cross-Entropy Loss (BCELoss) as the metric to measure the difference between the model output and true labels. The formula is as follows:
(1)
In the formula,
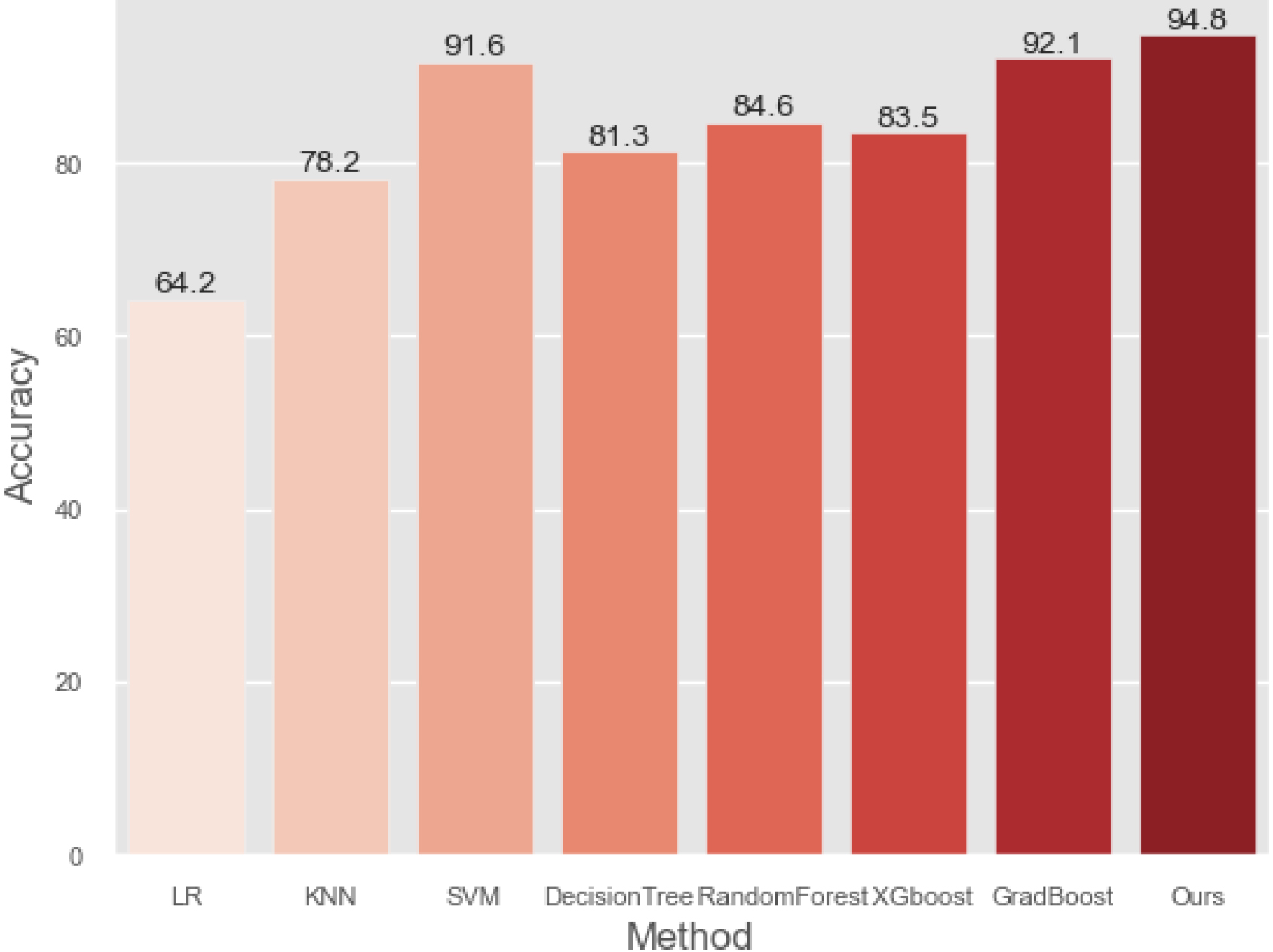
To validate the effectiveness of the model, we conducted a comprehensive performance comparison study, comparing the proposed deep learning model with traditional machine learning methods. Traditional algorithms, including Logistic Regression, K-Nearest Neighbors (KNN), Support Vector Machine (SVM), Decision Tree, Random Forest, XGBoost, and Gradient Boosting, were all included in the comparison. The results, as shown in Fig. 5, demonstrate the outstanding performance of our model, exhibiting the highest accuracy and generalization ability. Table 1 displays the accuracy of each model.
Table 1
Model results
| Model | Accuracy |
|---|---|
| LR | 64.2% |
| KNN | 78.2% |
| SVM | 91.6% |
| Decision tree | 81.3% |
| Random Forest | 84.6% |
| XGBoost | 83.5% |
| GradBoost | 92.1% |
| Ours | 94.8% |
Figure 5.
Comparison chart between our model and other traditional models.
Through these experimental steps, we thoroughly trained and evaluated the model, providing robust support for subsequent discussions and conclusions.
5.Discussion
In this study, we introduced deep learning methods, including a combination of fully connected neural networks and convolutional neural networks, to construct an acute liver failure prediction model. Through comparing the performance of traditional machine learning methods and deep learning methods, we found that deep learning methods excel in both accuracy and generalization ability. However, we still need to delve into some key issues to more comprehensively assess and understand the model’s strengths and limitations.
Firstly, we should focus on the robustness of the model and its ability to handle imbalanced data. In real medical datasets, there may be instances of sample imbalance, where there is a significant difference in the number of samples between patients with acute liver failure and non-patients. The model’s performance under such circumstances needs further evaluation to ensure its effectiveness in practical applications.
Our research emphasizes the importance of personalized medicine, yet how to better integrate individual differences information to enhance the model’s predictive accuracy remains a topic for further investigation [15]. Considering additional personalized features, such as genetic information and lifestyle factors, may be necessary to comprehensively grasp the physiological status of patients [16].
While our model has demonstrated promising results in our current dataset, external validation in a more diverse and extensive patient population is essential for assessing its generalizability. Future research should involve collaboration with multiple healthcare institutions to validate the model’s performance across various demographic groups, geographical locations, and clinical settings. This approach will ensure the broader applicability and reliability of our model in real-world scenarios.
Lastly, our model demonstrated superior performance in experiments, but real-world application will face the complexity and diversity of clinical scenarios [17]. Future research should focus on further optimizing the model and validating its feasibility and effectiveness in larger and more diverse patient populations [18] to ensure its applicability in actual medical practice. In contemplating the broader societal implications of our research, we recognize the ethical responsibility to transparently communicate the methodology and potential applications of our predictive model. This includes addressing concerns related to bias, fairness, and the responsible deployment of our model in real-world clinical scenarios. As we envision the integration of our model into healthcare practices, ethical considerations become pivotal in fostering trust, accountability, and the responsible advancement of medical research.
6.Conclusion
In conclusion, our study makes significant strides in the realm of Acute Liver Failure (ALF) prediction. By introducing a novel deep learning approach that combines fully connected and convolutional neural networks, we have achieved a robust predictive model. This model not only outperforms traditional machine learning methods but also demonstrates superior generalization capabilities, reaching an impressive accuracy of 94.8%. Our research places a spotlight on the potential of deep learning in ALF prediction, showcasing its ability to automatically learn complex patterns and abstract features from highly dynamic medical data.
Beyond the technical advancements, the practical implications of our work are paramount. Early and accurate prediction of ALF is crucial for timely interventions and improved patient outcomes. Our model, with its enhanced accuracy and generalization, stands as a powerful tool in the hands of healthcare professionals. It opens avenues for more precise and personalized guidance in patient care, potentially saving lives and improving the quality of healthcare in the context of acute liver failure.
This study not only represents technological progress but also offers a powerful tool for future acute liver failure prediction. By more accurately predicting the patients’ conditions, we provide healthcare professionals with finer information, aiming to improve the effectiveness of early diagnosis and treatment. This holds positive implications for personalized medicine and clinical practice. We anticipate that the findings of this research will contribute beneficial support to the health and medical care of acute liver failure patients and pave the way for new directions in future medical research.
Conflict of interest
None to report.
References
[1] | Dong V, Nanchal R, Karvellas CJ. Pathophysiology of acute liver failure. Nutrition in Clinical Practice. (2020) ; 35: (1): 24-29. |
[2] | Zaccherini G, Weiss E, Moreau R. Acute-on-chronic liver failure: definitions, pathophysiology and principles of treatment. JHEP Reports. (2021) ; 3: (1): 100176. |
[3] | Wong F, Piano S, Singh V, et al. Clinical features and evolution of bacterial infection-related acute-on-chronic liver failure. Journal of Hepatology. (2021) ; 74: (2): 330-339. |
[4] | Squires JE, Alonso EM, Ibrahim SH, et al. North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition position paper on the diagnosis and management of pediatric acute liver failure. Journal of Pediatric Gastroenterology and Nutrition. (2022) ; 74: (1): 138-158. |
[5] | Mai R, Lu H, Bai T, et al. Artificial neural network model for preoperative prediction of severe liver failure after hemihepatectomy in patients with hepatocellular carcinoma. Surgery. (2020) ; 168: (4): 643-652. |
[6] | Xie S, Yu Z, Lv Z. Multi-Disease Prediction Based on Deep Learning: A Survey. CMES-Computer Modeling in Engineering & Sciences. (2021) ; 128: (2). |
[7] | Lei L, Wang Y, Xue Q, et al. A comparative study of machine learning algorithms for predicting acute kidney injury after liver cancer resection. Peer J. (2020) ; 8: : e8583. |
[8] | Hong N, Liu C, Gao J, et al. State of the art of machine learning–enabled clinical decision support in intensive care units: literature review. JMIR Medical Informatics. (2022) ; 10: (3): e28781. |
[9] | Musunuri B, Shetty S, Shetty DK, et al. Acute-on-chronic liver failure mortality prediction using an artificial neural network. Engineered Science. (2021) ; 15: : 187-196. |
[10] | Morid MA, Sheng ORL, Del Fiol G, et al. Temporal pattern detection to predict adverse events in critical care: case study with acute kidney injury. JMIR Medical Informatics. (2020) ; 8: (3): e14272. |
[11] | Puri M. Automated machine learning diagnostic support system as a computational biomarker for detecting drug-induced liver injury patterns in whole slide liver pathology images. Assay and Drug Development Technologies. (2020) ; 18: (1): 1-10. |
[12] | Md AQ, Kulkarni S, Joshua CJ, et al. Enhanced Preprocessing Approach Using Ensemble Machine Learning Algorithms for Detecting Liver Disease. Biomedicines. (2023) ; 11: (2): 581. |
[13] | Salazar de Pablo G, Studerus E, Vaquerizo-Serrano J, et al. Implementing precision psychiatry: a systematic review of individualized prediction models for clinical practice. Schizophrenia Bulletin. (2021) ; 47: (2): 284-297. |
[14] | Mostafa F, Hasan E, Williamson M, et al. Statistical machine learning approaches to liver disease prediction. Livers. (2021) ; 1: (4): 294-312. |
[15] | Su TH, Wu CH, Kao JH. Artificial intelligence in precision medicine in hepatology. Journal of Gastroenterology and Hepatology. (2021) ; 36: (3): 569-580. |
[16] | Zhang D, Gong Y. The comparison of LightGBM and XGBoost coupling factor analysis and prediagnosis of acute liver failure. IEEE Access. (2020) ; 8: : 220990-221003. |
[17] | Dirven H, Vist GE, Bandhakavi S, et al. Performance of preclinical models in predicting drug-induced liver injury in humans: a systematic review. Scientific Reports. (2021) ; 11: (1): 6403. |
[18] | Ramspek CL, Jager KJ, Dekker FW, et al. External validation of prognostic models: what, why, how, when and where? Clinical Kidney Journal. (2021) ; 14: (1): 49-58. |


