
Development of sarcopenia assessment system using balance and gait ability: Preliminary tests in the elderly
Abstract
BACKGROUND:
Sarcopenia is a disease that has recently become an issue, and research on various assessment methods is being conducted based on guidelines published for the diagnosis of sarcopenia. However, most assessments are complex because the inspector must measure each device to collect data, or the elderly must directly manipulate and get assessment.
OBJECTIVE:
In this study, we developed an sarcopenia assessment system to assess and analyze various sarcopenia in one system.
METHODS:
The system consists of a scaffold sensor for balance ability assessment, a chair sensor for assessing the walking and lower extremity function, and a hand-held dynamometer for assessing grip strength. The balance pad consists of 326 FSR (Force Sensitive Resistor) sensors, and the accuracy is 10 kg/
RESULTS:
The average value of the total SPPB test scores, including the balance test, gait speed test, and chair stand test, of all participants was 9.06
CONCLUSIONS:
A preliminary assessment was conducted on the elderly in their 60 s or older with the developed system, and its performance confirmed that the assessment and result analysis were conducted well without any errors in software or hardware. Future studies intend to verify the reliability and accuracy of the assessment results compared to the existing direct measurement methods. In addition, we would like to conduct a study to establish data on the muscle reduction index by age group of Koreans.
1.Introduction
Sarcopenia is a disease in which muscle mass decreases with aging and physical function such as muscle strength, and walking speed decreases. Sarcopenia was classified as a disease in 2021 after the United States and Japan. Sarcopenia is a disease that can lead to hospitalization and death by increasing the risk of falls and fractures due to decreased daily life function caused by decreased physical activity ability [1, 2]. Currently, as many countries enter an aging society, the elderly population and the average age of survival are increasing. Therefore, active research and efforts are needed to prevent and manage Sarcopenia. Recently, various studies have been conducted to assess sarcopenia.
In 2010, the European Working Group on Sarcopenia in Older People (EWGSOP) developed a sarcopenia diagnostic algorithm. It was challenging to apply this algorithm to Asians because they, including Koreans, generally have smaller bodies and more body fat and activity than Westerners [3]. Since then, the Asian Working Group on Sarcopenia (AWGS) has been formed, and they published new guidelines for diagnosing patients with sarcopenia that can be used in local society or hospitals in 2019 [4]. In the assessment of sarcopenia, various musculoskeletal function assessments are performed using muscle mass estimation of the limbs (arms and legs), muscle strength estimation, and physical function assessment [5]. In addition, Yun et al. (2022) developed a deep-learning algorithm for diagnosing sarcopenia using a mobile device [6]. Lee (2020) proposed using ultrasound to assess sarcopenia by analyzing muscle thickness, Fascicle length, Pennation angle, Echo intensity, and Cross-sectional area [7]. Teixeira (2022) developed a mobile monitoring system for diagnosing and screening sarcopenia by linking Hand grip and Lipowise (subcutaneous fat meter) based on EWGSOP2 [8].
Most studies on the assessment of sarcopenia are conducting DXA, measurement of limb muscle mass using Multi-frequency bioelectrical impedance analysis (MF-BIA), Gait speed test, chair stand test, hand grip strength test, and then analyzing the results. These assessments have the inconvenience of requiring the tester to perform measurements on each device, collect the data from each device, and analyze data. The method using such a mobile device has the advantage of being easy to assess, but it is difficult for the elderly to perform it directly. In addition, despite the various inconveniences and problems of the existing method, research on developing a system that integrates, assesses, and analyze in one system is insignificant. Therefore, this study aims to develop a sarcopenia and functional assessment system for sarcopenia assessment.
2.System configuration
2.1Configuration of hardware
Figure 1 is the hardware configuration of the sarcopenia assessment system developed in this study. It consists of a scaffold sensor for evaluating balance ability, a chair sensor for evaluating lower extremity function, and a grip dynamometer for measuring the strength of grip. The balance pad was manufactured in a size of 660 mm(L)
The chair sensor for measuring walking and lower limb function was manufactured in a size of 430(L)
Figure 1.
The hardware configuration of sarcopenia assessment system.

TAKEI hand grip dynamometer was used to measure the strength of grip force, to which a weight sensor (Loadcell) was applied. The measurement range is 5 to 100 kgf
Figure 2.
The software of sarcopenia assessment system.
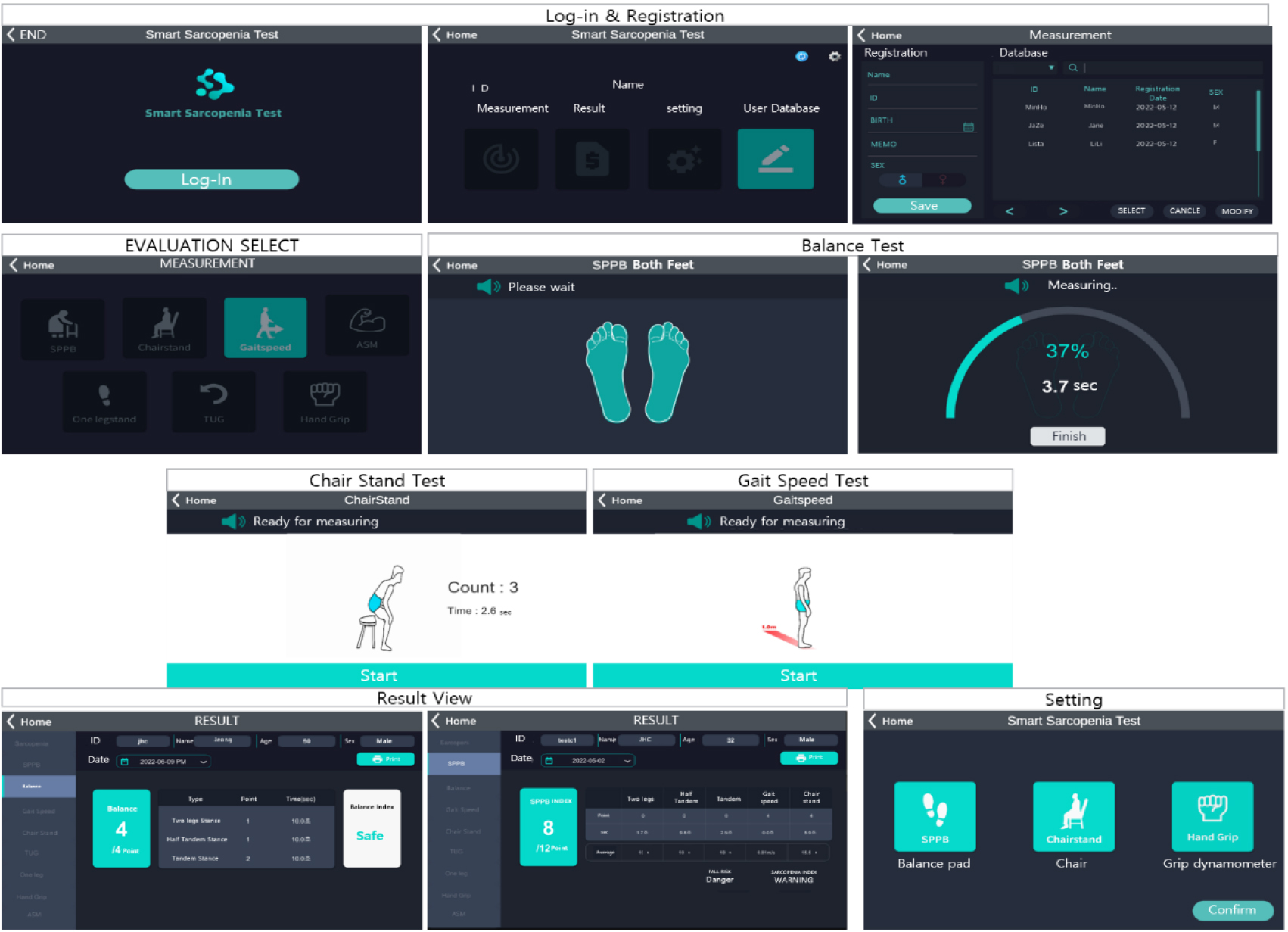
2.2Configuration of software
Figure 2 is the software of the sarcopenia assessment system developed in this study. A database was established to manage data for each user. The SPPB test assesses the degree of muscle loss by scoring a “Balance Test (4 points)”, “Gait Speed Test (4 points)”, and “Chair Stand Test (4 points).” The balance test consists of a “Side-by-side Stand,” “Semi-tandem Stand,” and “Tandem Stand.”
In the balance test, if the subjects hold their balance for 10 seconds in a side-by-side and semi-tandem stand, they will each get one point. If the subjects hold a tandem stand for 10 seconds, they will get 2 points. If they hold between 3 to 9.99 seconds, they will get 1 point, and those under 3 seconds will get 0 points. The risk of posture control is assessed according to the sum of the scores, and it is classified as “Good” if the score is 4 points, “Caution” if the score is 3 points, and “Warning” if the score is 2 points or less. The Gait speed test measures the time the subject walks a 4-meter course straight to the front of the chair sensor at their usual speed. Subjects score 4 points if their average speed is 0.83 m/sec or more, 3 points for 0.83
The chair stand test starts with the subject sitting on the chair sensor and repeating the stand-up from a chair without using their arms five times. Subjects score 4 points if the total time is less than 11.19 seconds, 3 points for 11.20 to 13.69 seconds, 2 points for 13.70 to 16.69 seconds, 1 point for 16.70 to 59.99 seconds, and 0 points for subjects who do not attempt or more than took 60 seconds. The SPPB test results are assessed according to the total score, and if the total score is 10 or more, it is classified as “Good,” if the total score is 9 to 3, it is classified as “Caution,” and if the score is 2 or less, it is classified as “Warning.”
For the hand grip strength test, which is an additional function, hold the grip dynamometer and measure the right and left hands alternately three times for three seconds. If the average value is 28 kgf or more for men and 18 kgf or more for women, it is classified as 1 point, otherwise 0 point. These assessment results are stored or printed in reports and can be classified by date to observe the change. The SPPB test criteria applied in this study were developed based on the SPPB criterion table proposed by the National Institute of Aging (NIA) in the United States and the Korean Geriatrics Society’s assessment index of sarcopenia [9, 10].
3.Methods
A preliminary test was conducted to verify the hardware and software performance of the Sarcopenia assessment system developed in this study. The participants were 36 senior citizens in Gwangju Metropolitan City, aged 60 years and over, with no medical history of the musculoskeletal or nervous system in the past 6 months (men,
Table 1
Characteristics of the participants
| Age (years) | Height (cm) | Weight (kg) | BMI (kg/2) | |
|---|---|---|---|---|
| 60 s Average (SD) ( | 65.77 ( | 161.77 ( | 65.58 ( | 24.89 ( |
| 70 s Average (SD) ( | 74.92 ( | 161.15 ( | 64.81 ( | 24.98 ( |
| 80 s Average (SD) ( | 81.70 ( | 160.20 ( | 60.21 ( | 23.48 ( |
Table 2
Result of sarcopenia assessment system
| SPPB test | |||||
|---|---|---|---|---|---|
| Subject No. (SEX) | Balance (sec) /score | Gait speed (m/s) /score | Chair stand (sec) /score | SPPB score (Total: 12) | |
| 60 s ( | 60_A(M) | 10/4 | 1.2/4 | 14/2 | 10 |
| 60_B(M) | 0/0 | 1.6/4 | 16.5/1 | 5 | |
| 60_C(M) | 10/4 | 0.4/1 | 14.3/3 | 8 | |
| 60_D(M) | 10/4 | 1.2/4 | 15.6/2 | 10 | |
| 60_E(M) | 2.2/0 | 1.1/4 | 26.5/1 | 5 | |
| 60_F(F) | 10/4 | 1.2/4 | 10.7/4 | 12 | |
| 60_G(F) | 10/4 | 1.2/4 | 15.4/2 | 10 | |
| 60_H(F) | 10/4 | 1.2/4 | 14.4/4 | 12 | |
| 60_I(F) | 10/4 | 1.6/4 | 9.6/4 | 12 | |
| 60_J(F) | 10/4 | 0.9/4 | 17.1/1 | 9 | |
| 60_K(F) | 10/4 | 1.3/4 | 9.9/4 | 12 | |
| 60_L(F) | 0/0 | 1.06/4 | 6.43/4 | 8 | |
| 60_M(F) | 10/4 | 1.2/4 | 13.8/3 | 11 | |
| 70 s ( | 70_A(M) | 10/4 | 0.9/2 | 12.4/3 | 9 |
| 70_B (M) | 10/4 | 1.0/4 | 17/1 | 9 | |
| 70_C (M) | 7.8/3 | 1.1/4 | 17.4/1 | 8 | |
| 70_D (M) | 7.1/2 | 1.1/4 | 18.1/1 | 7 | |
| 70_E (M) | 10/4 | 0.3/1 | 18.6/1 | 6 | |
| 70_F (M) | 10/4 | 1.1/4 | 23.9/1 | 9 | |
| 70_G (M) | 10/4 | 1.1/4 | 21.5/1 | 9 | |
| 70_H (F) | 10/4 | 1.0/4 | 16.3/2 | 10 | |
| 70_I (F) | 7.1/3 | 1.1/4 | 17.5/1 | 8 | |
| 70_J(F) | 9.7/3 | 1.0/4 | 11.9/3 | 10 | |
| 70_K(F) | 10/4 | 0.9/4 | 17.7/1 | 9 | |
| 70_L(F) | 6.6/2 | 0.8/3 | 23.6/1 | 6 | |
| 70_M(F) | 3.5/1 | 0.9/4 | 22.8/1 | 6 | |
| 80 s ( | 80_A(M) | 10/4 | 1.0/4 | 14.7/2 | 10 |
| 80_B(M) | 8.4/3 | 1.2/4 | 14.4/2 | 9 | |
| 80_C(M) | 10/4 | 0.8/3 | 15.3/2 | 9 | |
| 80_D(M) | 7.3/3 | 0.8/3 | 26.6/1 | 7 | |
| 80_E(M) | 8.4/3 | 1.2/4 | 14.4/2 | 9 | |
| 80_F(F) | 7.1/3 | 1.0/4 | 18.1/1 | 8 | |
| 80_G(F) | 10/4 | 1.0/4 | 15.3/2 | 10 | |
| 80_H(F) | 10/4 | 0.9/4 | 13.3/3 | 11 | |
| 80_I(F) | 10/4 | 1.0/4 | 12.6/3 | 11 | |
| 80_J(F) | 10/4 | 1.4/4 | 10.3/4 | 12 | |
4.Result
Table 2 shows the results of sarcopenia evaluation of subjects in their 60 s, 70 s, and 80 s using sarcopenia assessment system. The average value of the total SPPB test scores of all participants was 9.06
The average value of the balance test scores of all participants was 8.48
The average value of the Gait speed test scores of all participants was 1.05
The average value of the chair stand test scores of all participants was 16.05
Table 3
Result of handgrip strength test
| 60 s ( | 70 s ( | 80 s ( | |
| Hand grip strength (kgf) | 28.97 | 26.45 | 30.88 |
Table 3 shows the average value of hand grip test of all participants was 28.57
5.Discussion
Recently, research for the assessment of sarcopenia has been conducted in various fields, such as engineering and medicine. However, research on the development of devices for the assessment of sarcopenia is insignificant. In addition, the method using mobile devices developed in previous studies has the advantage of being easy to assess. However, it is difficult for the elderly to collect accurate data or perform it themselves. Therefore, this study attempted to develop Sarcopenia assessment system for assessing sarcopenia and the lower extremity function. A chair-type device that assesses walking and lower extremity functions using Loadcell and LiDAR sensors was developed, and a balance board for balance assessment was developed using FSR sensors.
Grip dynamometer uses commercially available tools, and all hardware can be linked to software through a USB cable, allowing data to be automatically collected and analyzed. In order to verify the performance of the developed device, a preliminary test was conducted on 36 elderly people aged 60 or older. In the preliminary test, the SPPB test and hand grip strength test were performed, and as a result, digitized data by age group could be collected. In the case of the SPPB test, it was confirmed that the average value of the total score decreased as the age group increased, and the Gait speed test, one of the SPPB tests, showed that the walking speed decreased with age group.
These results were consistent with the findings of Kim et al. (2012) and Cho et al. (2019) that the prevalence of sarcopenia increases with age [11, 12]. Insufficient nutrition and muscle failure to adapt to nutrition, such as essential amino acids, is one of the causes of sarcopenia [13]. In old age, it was observed that sarcopenia intensifies due to a lack of skeletal muscle accumulation and a decrease in skeletal muscle as age increases [14]. A decrease in skeletal muscle mass due to aging leads to decreased physical activities such as balance ability and walking function and a decrease in daily life performance [15]. During the SPPB test, there were no peculiarities in the results of the chair stand test and the balance test. The hand grip strength test also found no peculiarities in their result. Due to the characteristics of the elderly, it is believed that the measurement environment on the day of evaluation and the subjects’ psychological and physical conditions affected the test’s performance.
There was no difficulty using the equipment developed in this study to assess the sarcopenia of the elderly by experts in related fields. It was also confirmed that collecting quantitative assessment data and analyzing the results were performed without problems. However, in the case of balance boards, there was a problem that the sensor’s sensitivity was too high that the Semi-tandem stand posture and the Tandem Stand posture were not adequately recognized, except for the side-by-side stand posture of the elderly with reduced balance ability. Sometimes, assessment was impossible for the elderly who weighed too little. In order to compensate for these problems, a function capable of adjusting sensor sensitivity should be added. In addition, there was no separate safety device to prevent the subject from falling, so the risk of falling was expected. When measuring using a balance board, it is judged that a handle or an auxiliary device for safety is required on the left and right sides or in front.
In the case of chair sensors, when performing the Gait speed test, there were cases where it could not be measured if it deviated from the left and right recognition range of the LiDAR sensor, and it could cause problems when performing the test of the elderly who could not walk in a straight line. In order to compensate for these limitations, the assessment is expected to be carried out accurately only when the software shows a pop-up of route departure information and marks the floor of the space to be inspected using tape. Through the results of this study, it was possible to confirm the muscle loss index, walking speed, and balance point of the elderly by age group on various scales. It was confirmed that as the age group increased, the muscle loss index and walking speed tended to decrease. In future studies, it is necessary to identify characteristics according to changes in physical function such as muscle loss index, Gait speed, chair stand, and balance by age group, and to study the composition of customized exercise guides to prevent and recover sarcopenia.
6.Conclusions
In this study, a chair sensor and a balance board were developed to assess sarcopenia and lower extremity function, and data measured with the equipment and grip dynamometer were automatically linked and analyzed in software. As a result, a system that can quickly check the overall measurement results and whether sarcopenia is applicable was developed. Next, through a preliminary test of the elderly, it was confirmed that hardware and software were well assessed and analyzed without errors. However, there is a limitation in that the accuracy and reliability of the product developed in this study needed to be verified compared to the existing direct assessment method. Future studies should verify the reliability and accuracy of the evaluation results compared to the existing direct assessment methods. In addition, we would like to conduct a study on the characteristics of Koreans’ muscle loss index data by age group.
Acknowledgments
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (Project no: NRF-2022R1A2C1093320 & RS-2023-00236157).
Conflict of interest
None to report.
References
[1] | Malmstrom TK, Miller DK, Simonsick EM, Ferrucci L, Morley JE. SARC-F: a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. Journal of Cachexia, Sarcopenia and Muscle. (2016) ; 7: (1): 28-36. |
[2] | Schaap LA, Schoor NMV, Lips P, Visser M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study Amsterdam. Journal of gerontology: medical sciences. (2018) ; 73: (9): 1199-1204. |
[3] | Chen LK, Liu LK, Woo J, Assantachai P, Auyeung TW, Bahyah KS, Chou MY, Chen LY, Hsu PS, Krairit O, Lee JSW, Lee WJ, Lee YH, Liang CK, Limpawattana P, Lin CS, Peng LN, Satake S, Suzuki T, Won CW, Wu CH, Wu SN, Zhang T, Zeng P, Akishita M, Arai H. Sarcopenia in asia: consensus report of the asian working group for sarcopenia. Journal of the American Medical Directors Association. (2014) ; 15: (2): 95-101. |
[4] | Chen LK, Woo J, Assantachai P, Auyeung TW, Chou MY, Lijima K, Jang HC, Kang L, Kim MJ, Kim SY, Kojima T, Kuzuya M, Lee JSW, Lee SY, Lee WJ, Lee YH, Liang CH, Lim JY, Lim WS, Peng LN, Arai H. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. Journal of the American medical directors association. (2020) ; 21: (3): 300-307. |
[5] | Won CW. Diagnosis of sarcopenia in primary health care. Journal of Korean Medical Association. (2020) ; 63: (10): 633-641. |
[6] | Yun YU, Sohn JW. Diagnosis of Sarcopenia in the Elderly and Development of Deep Learning Algorithm Exploiting Smart Devices. Journal of the Society of Disaster Information. (2022) ; 18: (3): 433-443. |
[7] | Lee SY. Ultrasound evaluation for sarcopenia. Geriatric Rehabilitation. (2020) ; 10: (2): 50-57. |
[8] | Teixeira E, Bohn L, Guimaraes JP, Alexio IM. Portable Digital Monitoring System for Sarcopenia Screening and Diagnosis. Geriatrics. (2022) ; 7: (1): 121-134. |
[9] | Cho BL. Physical performance measures in the elderly. Journal of Korean academy of family medicine. (2003) ; 24: (8): 689-695. |
[10] | Baek JY, Jung HW, Kim KM, Kim MJ, Park CYJ, Lee KP, Lee SY, Jang IY, Jeon OH, Lim JY. Korean Working Group on Sarcopenia Guideline: Expert Consensus on Sarcopenia Screening and Diagnosis by the Korean Society of Sarcopenia, the Korean Society for Bone and Mineral Research, and the Korean Geriatrics Society. Annals of Geriatric medicine and research. (2023) ; 27: (1): 9-21. |
[11] | Kim YS, Lee YH, Chung YS, Lee DJ, Joo NS, Hong DH, Song GE, Kim HJ, Choi YJ, Kim KM. Prevalence of Sarcopenia and Sarcopenic Obesity in the Korean Population Based on the Fourth Korean National Health and Nutritional Examination Surveys. Journal of Gerontology: Medical science. (2012) ; 67: (10): 1107-1113. |
[12] | Cho GY, Bae EJ, Kim YH. Association between Sarcopenia and Health Risk Behaviors by Age Groups in Korean Adults: Korea National Health and Nutrition Examination Survey IV to V. Journal of the Korean Data Analysis Society. (2019) ; 21: (3): 1523-1537. |
[13] | Volpi E, Mittendorfer N, Rasmussen BB, Wolfe RR. The Response of Muscle Protein Anabolism to Combined Hyperaminoacidemia and Glucose-Induced Hyperinsulinemia Is Impaired in the Elderly. Journal of Clinical Endocrinol Metabolism. (2011) ; 85: (12): 4481-4490. |
[14] | Srikanthan P, Hevener AL, Karlamangla AS. Sarcopenia Exacerbates Obesity-Associated Insulin Resistance and Dysglycemia: Findings from the National Health and Nutrition Examination Survey III. Sarcopenic Obesity and Diabetes. (2010) ; 5: (5): 1-8. |
[15] | Park CR, Kim HI, Kim MC. Analysis of Sarcopenia Using an Integrated Evaluation Tool: Targeting the elderly over 65 years of age in Korea. Journal of The Korean Society of Integrative medicine. (2023) ; 11: (1): 31-41. |


