
Imaging findings of Epstein-Barr Virus-positive inflammatory follicular dendritic cell sarcoma of spleen: A case report
Abstract
BACKGROUND:
Spleen Epstein-Barr Virus (EBV)-positive inflammatory follicular dendritic cell sarcoma (FDCS) is rare, and the imaging signs are unclear. The COVID-19 has been confirmed to be the cause of pneumonia and can cause a variety of diseases including myocarditis. However, it has not been reported to be the cause of the exacerbation or activation of EBV-positive inflammatory FDCS.
OBJECTIVE:
The objective is to extract the imaging features of EBV-positive inflammatory FDCS in the spleen and analyze the reasons for the special features of this case.
METHODS:
By analyzing the patient’s treatment process and imaging examinations (A 77-year-old female was admitted to the hospital due to generalized discomfort and pain symptoms. When she was admitted to the hospital a year earlier with COVID-19 pneumonia, a chest CT scan showed that she had a splenic tumor. During this admission, CT scans showed two irregularly shaped and unevenly dense soft tissue density masses within the spleen, with uneven enhancement on contrast-enhanced im-aging within the solid components and along the edges. PET/CT scans revealed elevated glucose metabolism in the masses. Postoperative pathological diagnosis confirmed splenic EBV-positive inflammatory FDCS.), reading the literature, sorting out the disease cognitive process, epidemiology, and pathological data of EBV-positive inflammatory FDCS, we discussed the imaging manifestations and possible differential diagnosis of the disease.
RESULTS:
The patient was finally diagnosed with splenic EBV-positive inflammatory FDCS.
CONCLUSIONS:
Imaging features of EBV-positive inflammatory FDCS in the spleen include a high incidence of hemorrhage and necrosis, persistent moderate enhancement of the solid portion, a “capsular-like enhancement” structure at the tumor edge, and possibly active glucose metabolism with high Standardized Uptake Values (SUVs). COVID-19 infection and long-term COVID-19 sequelae may exacerbate and activate EBV-positive inflammatory FDCS in the spleen, and the mechanism remains to be further studied.
1.Introduction
Epstein-Barr Virus (EBV)-positive inflammatory follicular dendritic cell sarcoma (FDCS) is a rare low-grade malignant tumor. The total number of cases reported worldwide is less than 200. Most reports focus on clinical and pathological research, with relatively less emphasis on imaging findings, leading to inadequate understanding of the disease among radiologists. Clinical symptoms in most cases are nonspecific, and diagnosis relies on pathological examination. Previous reports of EBV-positive inflammatory FDCS have not documented multiple splenic lesions, and most lack tumor demonstration of Positron Emission Tomography/Computed Tomography (PET/CT). Here, we present a case of multiple splenic EBV-positive inflammatory FDCS in an elderly woman. The distinctiveness resides in the tumours’ multiplicity or activity, which makes it easier to extract additional imaging features and raises radiologists’ awareness of this illness. Making decisions on preoperative patient care and clinical management may be aided by the recognition of these aspects. Further research is needed to determine whether the etiology of multiple and active tumors is related to the patient’s history of previous COVID-19 pneumonia infection.
2.Materials and methods
A 77-year-old female patient, previously diagnosed with COVID-19 pneumonia based on chest Computed Tomography (CT) findings one year ago, was incidentally found to have splenic masses. She had a splenic mass puncture biopsy at 960 People’s Liberation Army General Hospital about two months ago, and the results indicated proliferative lymphoid lesions that might be lymphomas. She was hospitalized due to nonspecific discomfort and exhaustion six weeks prior to admission. Upon inspection, her abdomen showed no signs of rebound discomfort and was smooth and flat. She did not experience fever, chills, nausea, vomiting, diarrhea, or melena. Nor did she describe any radiating discomfort in her lower back or right shoulder. She had lost 2.5 kg of weight in the last month, along with having a bad mood, decreased appetite, and trouble sleeping since the symptoms first appeared. Upon admission, her vital signs were as follows: blood pressure was 102/68 mmHg; heart rate was 86 beats per minute; respiratory rate was 17 breaths per minute; temperature was 36.7∘C. Initial laboratory findings: hemoglobin was 98 g/L (normal range 115–150), serum albumin was 87 mg/L (150–380), serum globulin was 30.6 g/L (40–55), albumin/globulin ratio was 0.5 (1.2–2.4), and C-reactive protein was 50.2 mg/L (0–8). Imaging findings were as follows: CT scans showed significant splenomegaly with two irregular soft tissue density masses in the spleen, measuring 5.6 cm
Figure 1.
CT images of EBV-positive inflammatory FDCS. (a) and (e) represent non-contrast images, revealing two cystic-solid soft tissue masses. (b)–(d) and (f)–(h) correspond to contrast-enhanced arterial, venous, and delayed phase images, illustrating moderately uneven enhancement along the edges and within the solid components of the masses. Patchy non-enhanced areas are observed internally.
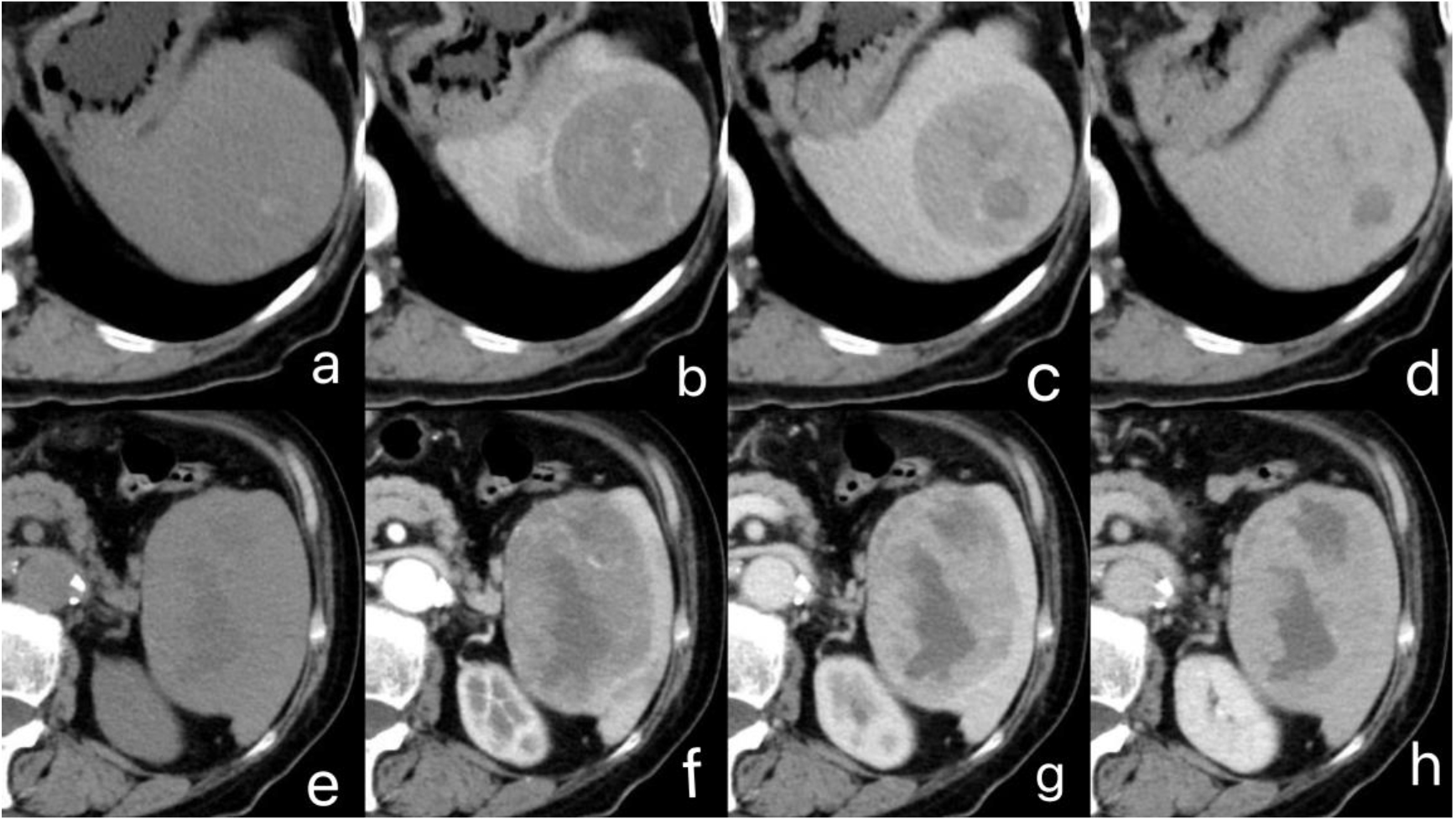
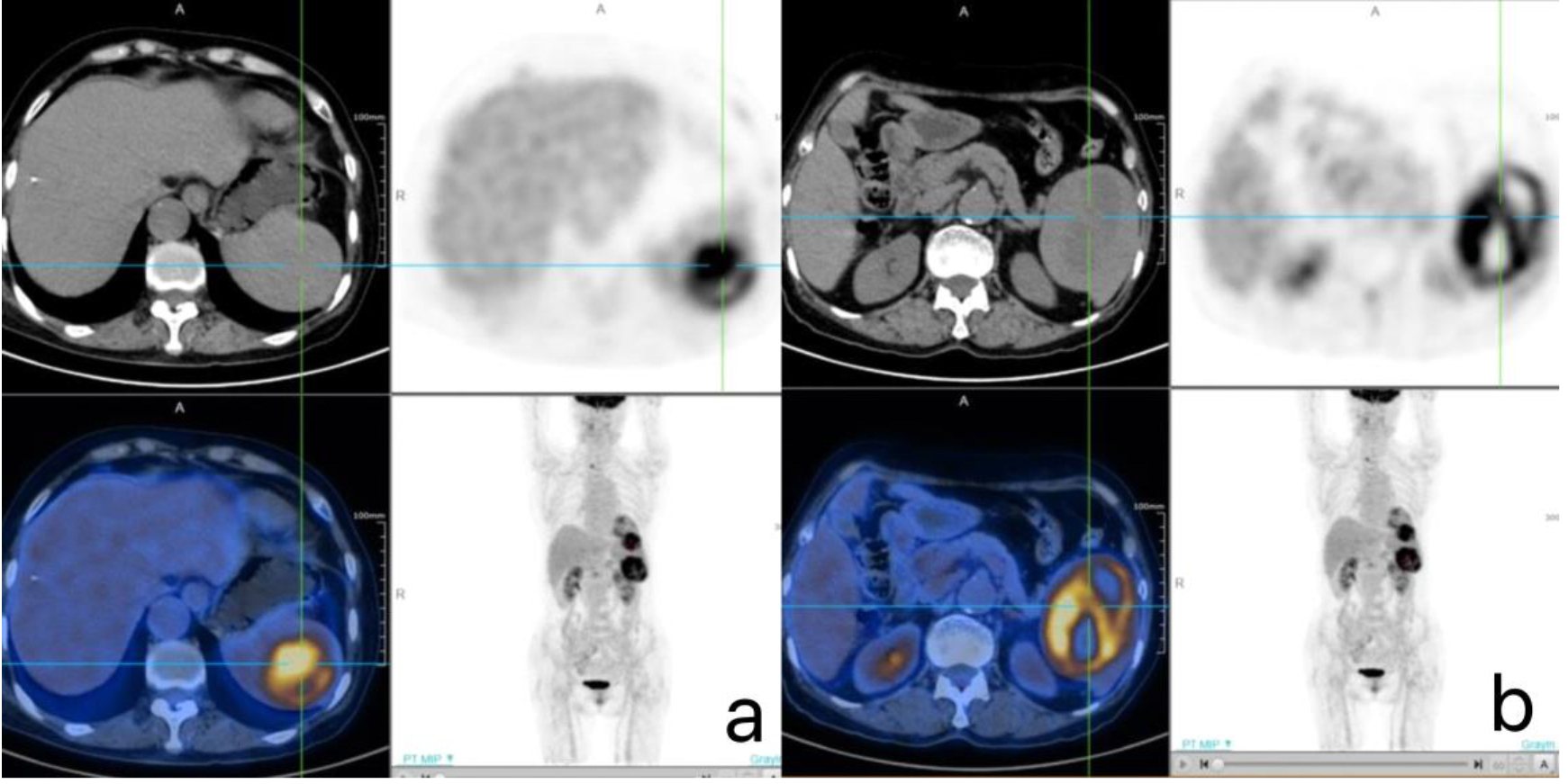
Figure 2.
PET/CT images of EBV-positive inflammatory FDCS, which reveal increased metabolic activity within the masses. (a) The tumor SUV is 10.8, (b) The tumor SUV is 8.3.
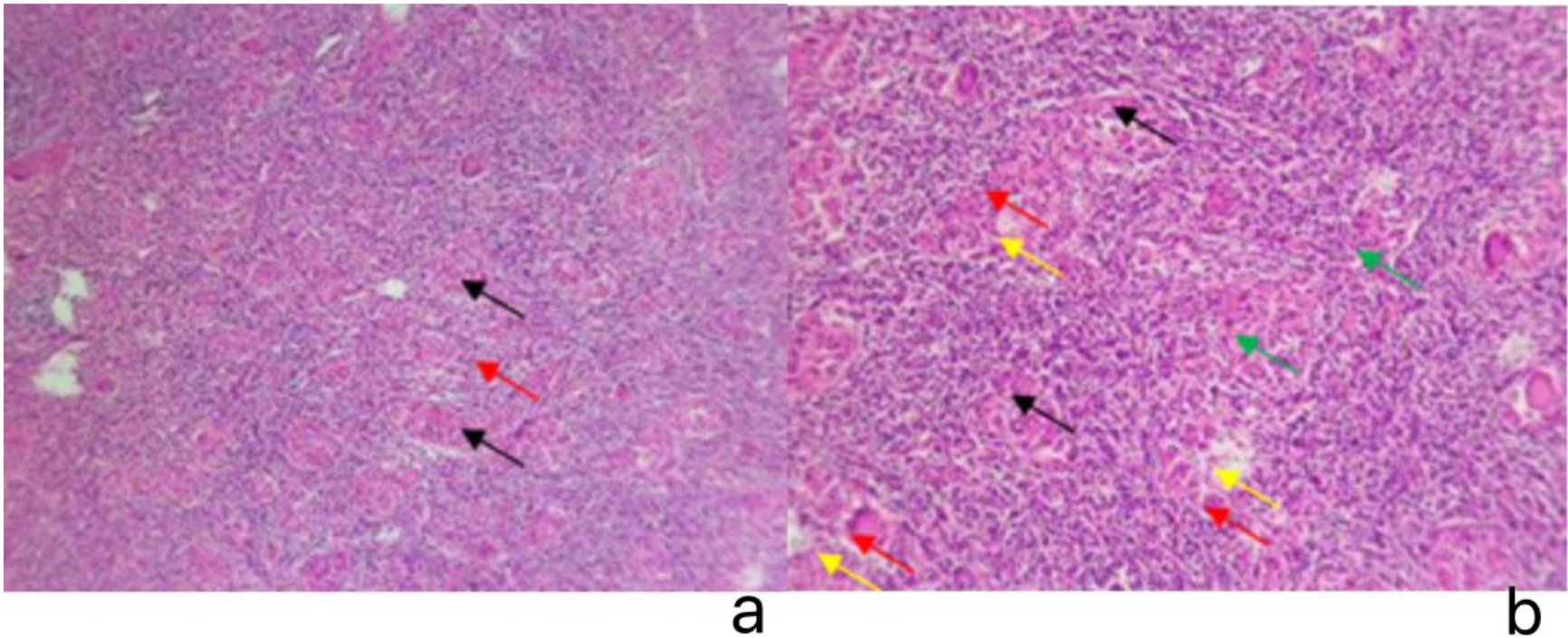
The patient underwent laparoscopic total splenectomy, a minimally invasive procedure for spleen removal. The tumor exhibited a fish-flesh appearance with areas of necrosis and hemorrhage, along with a soft consistency. Microscopic examination revealed two regions of tumor tissue with similar histomorphology, characterized by a biphasic cellular pattern. The tumor comprised spindle and oval-shaped cells mixed with numerous small lymphocytes, forming sheet-like and interwoven fascicles, with some areas showing palisading structures. Additionally, there were granulomas, multinucleated giant cells, and sheet-like coagulative necrosis in certain regions. At high magnification, the tumor cells displayed indistinct borders resembling syncytial cells, with round or oval nuclei, marked pleomorphism, and notable mitotic activity (5–8 signals/50 High Power Field (HPF)). Some areas exhibited interstitial infiltration of tissue cells and eosinophils (Fig. 3(a–b)). Immunohistochemistry showed positive expression of Vimentin (3+), Lysozyme (3+), CD68 (3+), CD163 (3+), HLA-DR (3+), CD31 (3+), CD43 (+), and Ki-67 (+, 35%–40%). Limited positive B lymphocytes in the interstitium for CD20, CD79a, and MUM1, and abundant positive T lymphocytes for CD3, CD4, and CD5 were observed. In situ hybridization detected Epstein-Barr virus-encoded small RNA (EBER) in the tumor cells, with 50–70 signals per high-power field, and positive control tissues were also positive. The pathological diagnosis confirmed the presence of EBV positive inflammatory FDCS in the spleen.
Figure 3.
Tumor pathology images under microscope. (a) HE
3.Results and discussion
In situ hybridization results showed: EBER (positive, with 50–70 signals/HPF in dense areas; positive control tissue also positive). The pathological diagnosis for this patient is EBV-positive inflammatory FDCS of the spleen. Based on the comprehensive clinical presentation, laboratory tests, imaging examinations, intraoperative findings, and postoperative pathological examination of the tumor, the patient was ultimately diagnosed with multiple EBV-positive inflammatory follicular dendritic cell sarcomas of the spleen.
Follicular dendritic cell sarcoma (FDCS) is a rare, low-grade malignant tumor that arises from follicular dendritic cells (FDC), which are specialized immune cells in the germinal center of lymphoid follicles. FDCS can occur in lymph nodes or extranodal sites, such as the head and neck, gastrointestinal tract, and retroperitoneum. FDCS was first reported by Shek et al. in 1996 [1]. It was further classified into classic FDCS and inflammatory pseudotumor-like FDCS by Cheuk et al. in 2001 [2], with the latter showing a certain correlation with EBV infection and being rarer, thus introducing the concept of inflammatory pseudotumor-like follicular dendritic cell sarcoma. In 2008, the fourth edition of the WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues categorized it as an inflammatory pseudotumor-like variant of FDCS. However, in the 2016 revised fourth edition of the WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, it was separately classified from follicular dendritic cell sarcoma and named inflammatory pseudotumor-like follicular/dendritic cell sarcoma. Considering its association with EBV, the 2019 fifth edition of the WHO Classification of Digestive System Tumours renamed it EBV-positive inflammatory follicular dendritic cell sarcoma [3]. The latest fifth edition of the WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues in 2022 [4] maintains this name and classifies EBV-positive inflammatory FDCS, follicular dendritic cell sarcoma, and fibroblastic reticular cell tumor under the category of interdigitating dendritic cell sarcoma. The 2022 International Consensus Classification (ICC) named it as EBV-positive inflammatory follicular/dendritic cell sarcoma [5]. The evolution of the disease’s nomenclature reflects the deepening understanding of the medical community regarding this condition. Providing additional information from an imaging perspective would undoubtedly aid in the comprehension and treatment of the disease.
EBV-positive inflammatory FDCS is rare, with the majority of reported cases occurring in individuals of Asian descent, suggesting a potential racial predisposition. It primarily manifests in young to middle-aged adults, with a median age ranging from 50 to 58 years and exhibits a notable female predominance. EBV-positive inflammatory FDCS primarily occurs in the liver or spleen, with occasional simultaneous or asynchronous involvement of both organs [6, 7]. It is rare in the colon, tonsils, bronchi, pancreas and mesentery [8]. Clinical presentation is often asymptomatic or may include abdominal distension, abdominal pain, accompanying anemia, and occasionally systemic symptoms such as discomfort, weight loss, and low-grade fever [9]. Laboratory investigations reveal decreased albumin, elevated gamma-globulin, and increased C-reactive protein. Tumor marker testing may show elevated CA125 levels, and peripheral eosinophilia may be observed. In the case of this elderly female patient, the condition was incidentally discovered during a routine health examination, presenting with mild abdominal distension and pain. Apart from these symptoms, there were no other clinical manifestations. Laboratory findings showed a hemoglobin level of 98 g/L, prealbumin level of 87 mg/L, albumin level of 30.6 g/L (measured by the bromocresol green method), and a C-reactive protein level of 50.2 mg/L. Some aspects of the patient’s clinical course and laboratory parameters align with the literature on EBV-positive inflammatory FDCS. However, the correlation between clinical presentation, laboratory indicators, and EBV-positive inflammatory FDCS, as well as any pathological and physiological basis, warrants further research for confirmation.
Although the precise pathogenic mechanisms behind EBV-positive inflammatory FDCS are yet unknown, it is thought that the illness may have its roots in Epstein-Barr virus-infected stromal cells that are differentiating along the follicular dendritic cell line. Histopathologically, EBV-positive inflammatory FDCS usually manifests as a well-defined mass, frequently nodular in nature, with the possibility of bleeding and necrosis on the surface of the thin fibrous capsule. Under a microscope, the tumor displays a noticeable background of inflammatory cells, such as plasma and lymphocytes, with sporadic tumor cells arranged in a loose manner within this inflammatory context. Reactive lymphoid follicles can occasionally be seen. Tumor cell-dense areas typically exhibit a pattern of growth characterized by bundles or layers. Inconsistent cell boundaries, little to moderate amounts of cytoplasm, vesicular nuclei, punctate chromatin, tiny central nucleoli, variable nuclear atypia, and infrequent mitotic figures are all common characteristics of tumor cells. Li et al. [10] and Song et al. [11] have found that D240 exhibits high sensitivity to FDCS, serving as a novel diagnostic marker. Additionally,
Radiologically, EBV-positive inflammatory FDCS often presents as a well-defined solid or cystic-solid mass. Persistent moderate enhancement is a common finding on CT scans. Larger tumors may also show other characteristics such necrosis, bleeding, calcification, and scarring [16]. The solid portions of the tumor often exhibit sustained moderate enhancement, which may be attributed to the tumor cell-dense areas’ pattern of growth characterized by bundles or layers. Such structures may impede the entry of contrast agents while also prolonging their retention within the tumor tissue. Larger masses show focal areas of hemorrhage, and contrast-enhanced scans reveal the characteristic “capsule-like enhancement” at the periphery of both masses, with a progressive and sustained enhancement in the solid part of the tumors. Similar SUVs are seen in PET/CT scans of both masses, indicating enhanced aberrant glucose metabolism and similar biological activity.
EBV-positive inflammatory FDCS is considered an indolent malignant tumor. In this case, PET/CT shows active and vigorous glucose metabolism in the tumor. Whether this is a characteristic of the individual or a feature of the disease as a whole requires further research supported by more cases. Therefore, it is important to differentiate it from the following diseases:
1. Splenic Lymphoma: Lymphoma, a common malignancy, frequently involves the spleen in systemic lymphoma. It includes Hodgkin lymphoma and non-Hodgkin lymphoma, categorized by cell type and pathology. When splenic lymphoma presents as solitary or multiple nodules, it can be challenging to distinguish from the presented case. Typically, lymphomas have less water content, uniform histological texture, minimal necrosis, hemorrhage, and cystic changes. Blood supply is less abundant, and contrast-enhanced scans show mild to moderate homogeneous delayed enhancement, with enhancement levels lower than the normal splenic parenchyma. The presence of necrosis, hemorrhage, enhancement capsule, and enhancement levels at various stages can aid in distinguishing it from EBV-positive inflammatory FDCS.
2. Inflammatory Myofibroblastic Tumor (IMT) of the Spleen: IMT is a rare intermediate-grade mesenchymal tumor with potential for recurrence. Pathologically, IMT consists mainly of spindle-shaped myofibroblastic cells often infiltrated by plasma cells or lymphocytes. IMT typically manifests as poorly defined masses with locally increased fat density at the tumor edge, adjacent thickening, and adhesion of the peritoneum and intestinal wall [17]. Non-uniform delayed enhancement is seen on CT scans in cystic or mucinous low-density lesions inside IMT, which indicates the presence of mucinous collagenized tissue within the lesion. Distinct borders, delayed enhancing patterns, and a low necrosis rate set IMT apart from inflammatory FDCS that is positive for EBV.
3. Littoral Cell Angioma (LCA) of the Spleen: LCA is a benign vascular tumor specific to the spleen, characterized by proliferative vessels with a mixed endothelial-cell phenotype. LCA is often associated with clinical symptoms such as splenomegaly, hypersplenism, fever, chills, weakness, fatigue and pain. Typically, LCA presents as multiple lesions on CT with scattered pinpoint low-density shadows, showing no significant enhancement after contrast administration. This appearance is referred to as “Freckle sign,” caused by iron deposition within the lesion. Due to their dual nature, which combines characteristics of endothelium and tissue cells, LCA tumor cells are distinguished from EBV-positive inflammatory FDCS by their intracellular hemosiderin deposition and phagocytic activity [18].
4. Splenic hamartoma: splenic hamartoma represents a rare and benign tumor that can manifest at any age, displaying no gender predilection. Pathologically, gross specimens typically portray well-defined and non-encapsulated nodules. These nodules, often solitary, consist of an anomalous amalgamation of red pulp, the predominant component of the normal spleen, occasionally incorporating mixtures of both red and white pulp. Splenic hamartomas are commonly incidentally discovered during routine physical examinations, mirroring the presentation of various other benign lesions within the spleen. Radiologically, on CT scans, splenic hamartomas typically present as slightly low-density or iso-density lesions on non-contrast images. Contrast-enhanced scans reveal early enhancement within the tumor parenchyma, displaying a pattern of progressive enhancement in subsequent phases. Notably, this enhancement pattern closely resembles that of the normal splenic parenchyma. The rich vascularization, particularly the abundant blood sinuses constituting the tumor, contributes to this characteristic enhancement pattern. This distinct enhancement pattern proves invaluable in differentiating splenic hamartomas from other entities such as EBV-positive inflammatory FDCS. The ability to discern these radiological features enhances the accuracy of diagnosis and contributes to effective clinical decision-making [19].
5. Sclerosing Angiomatoid Nodular Transformation (SANT): SANT is a rare benign vascular proliferative lesion that occurs in the spleen. Recent research suggests that SANT is a multiclonal reactive lesion rather than a true neoplasm. It is believed to develop in response to vascular injury or insufficient blood supply, representing a healing reaction associated with increased vascular proliferation. Radiologically, on CT-enhanced scans, SANT lesions typically exhibit clear borders and demonstrate centripetal, progressively nodular enhancement. In the arterial phase, a distinctive “spoke-wheel” or “radiating” pattern is observed with central non-enhancing areas resembling clefts or cleft-like spaces. This appearance is often referred to as the “spoke-wheel sign.” As time progresses, the enhancement range gradually expands, but it may not completely fill the lesion. Additionally, a central “starburst” pattern, known as the “stellate scar,” may be visible within the lesion. The tumor’s expansive growth can lead to compression of the surrounding splenic parenchyma, creating a pseudo-capsule. Although SANT may share some imaging features with EBV-positive inflammatory FDCS, the presence of the “spoke-wheel” and “stellate scar” patterns in the central region can help differentiate SANT from other lesions [20].
The elderly patient sought medical attention more than a year after being diagnosed with splenic lesions during a routine check-up, after experiencing symptoms like exhaustion and nonspecific pain. Abnormalities were found in the laboratory, including 98 g/L of hemoglobin, 87 mg/L of prealbumin, 30.6 g/L of albumin (measured using the bromocresol green method), and 50.2 mg/L of C-reactive protein. In this instance, a few laboratory signs matched those documented in the literature. This patient, however, showed more severe clinical symptoms, mostly systemic, in contrast to earlier findings. Larger and more numerous splenic masses were present, along with active glucose metabolism. The two splenic masses were clearly distinguished from one another, but their imaging characteristics were nearly the same; they presented as cystic-solid masses with widespread internal necrosis, with the bigger masses exhibiting focal bleeding. The distinctive “capsule-like enhancement” surrounding both masses was seen on enhanced scans, and the solid parts of the tumors had increasing, sustained enhancement. PET/CT scans showed aberrant glucose metabolism in both masses, and the SUVs were identical, indicating that the two masses behaved biologically similarly. In this instance, the characteristics of multiplicity and activity are indicative of an EBV-positive inflammatory FDCS. According to research like Jeffrey et al. [21] in Pathogens (2021) and Su et al. [22] in Cell (2022), there may be a connection between COVID-19-induced inflammation and EBV reactivation. The patient was first identified with COVID-19 pneumonia during a CT scan. The multiplicity and activity seen in this instance of EBV-positive inflammatory FDCS, according to the author, may be related to the activation of EBV as a result of inflammation brought on by COVID-19 infection and its long-term aftereffects. However, more clinical information and investigation are needed to determine the magnitude of the relationship between COVID-19 pneumonia infection and EBV-positive inflammatory FDCS.
4.Conclusions
In conclusion, splenic EBV-positive inflammatory FDCS is a relatively rare low-grade malignant tumor that predominantly affects middle-aged to elderly women. The medical imaging features of splenic EBV-positive inflammatory FDCS include a high incidence of hemorrhage and necrosis, sustained moderate enhancement of solid portions, a “capsule-like enhancement” structure at the tumor margin, and potentially active glucose metabolism with high SUVs. The infection and long-term sequelae of COVID-19 pneumonia may exacerbate and activate splenic EBV-positive inflammatory FDCS. The mechanisms behind this association require further investigation.
Conflict of interest
None to report.
References
[1] | Shek TWH, Ho FCS, Ng IOL, et al. Follicular dendritic cell tumor of the liver: evidence for an Epstein-Barr virus-related clonal proliferation of follicular dendritic cells. The American Journal of Surgical Pathology. (1996) ; 20: (3): 313-324. |
[2] | Cheuk W, Chan JKC, Shek TWH, et al. Inflammatory pseudotumor-like follicular dendritic cell tumor: a distinctive low-grade malignant intra-abdominal neoplasm with consistent Epstein–Barr virus association. The American Journal of Surgical Pathology. (2001) ; 25: (6): 721-731. |
[3] | Nagtegaal ID, Odze RD, Klimstra D, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. (2020) ; 76: (2): 182. |
[4] | Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia. (2022) ; 36: (7): 1720-1748. |
[5] | Campo E, Jaffe ES, Cook JR, et al. The international consensus classification of mature lymphoid neoplasms: a report from the clinical advisory committee. Blood, The Journal of the American Society of Hematology. (2022) ; 140: (11): 1229-1253. |
[6] | Li X, Shi Z, You R, et al. Inflammatory pseudotumor-like follicular dendritic cell sarcoma of the spleen: computed tomography imaging characteristics in 5 patients. Journal of Computer Assisted Tomography. (2018) ; 42: (3): 399-404. |
[7] | Zhang BX, Chen ZH, Liu Y, et al. Inflammatory pseudotumor-like follicular dendritic cell sarcoma: A brief report of two cases. World Journal of Gastrointestinal Oncology. (2019) ; 11: (12): 1231. |
[8] | Tao LL, Huang YH, Chen YL, et al. SSTR2a is a useful diagnostic marker for follicular dendritic cells and their related tumors. The American Journal of Surgical Pathology. (2019) ; 43: (3): 374-381. |
[9] | Yao D, Li WP, Xu HX, et al. Analysis of clinical characteristics of inflammatory pseudotumor-like follicular dendritic cell tumors of the spleen. Chinese Journal of General Surgery. (2018) ; 33: (11): 958-959. doi: 10.3760/cma.j.issn.1007-631X.2018.11.018. |
[10] | Li J, Yin WH, Yu GY, et al. Evaluation of the diagnostic value of Clusterin, CXCL13, Podoplanin(D2-40), CD21 and CD35 in follicular dendritic cell sarcoma. Journal of Clinical and Experimental Pathology. (2015) ; 31: (2): 145-150. |
[11] | Song XX, Li N, Zhang S, et al. Clinicopathological analysis of 10 cases of follicular dendritic cell sarcoma. Journal of Clinical and Experimental Pathology. (2018) ; 34: (5): 566-568. |
[12] | Zhang H, Maitta RW, Bhattacharyya PK, et al. γ-Synuclein is a promising new marker for staining reactive follicular dendritic cells, follicular dendritic cell sarcoma, Kaposi sarcoma, and benign and malignant vascular tumors. The American Journal of Surgical Pathology. (2011) ; 35: (12): 1857-1865. |
[13] | Shia J, Chen W, Tang LH, et al. Extranodal follicular dendritic cell sarcoma: clinical, pathologic, and histogenetic characteristics of an underrecognized disease entity. Virchows Archiv. (2006) ; 449: : 148-158. |
[14] | Li Y, Yang X, Tao L, et al. Challenges in the diagnosis of epstein-barr virus-positive inflammatory follicular dendritic cell sarcoma: extremely wide morphologic spectrum and immunophenotype. The American Journal of Surgical Pathology. (2023) ; 47: (4): 476-489. |
[15] | Liu XY, Li YC, Zhang Z, et al. Application of EBER in situ hybridization and CD35 double staining method in liver/spleen EBV-positive inflammatory follicular dendritic cell sarcoma. Journal of Clinical and Experimental Pathology. (2023) ; 39: (10): 1264-1265. doi: 10.13315/j.cnki.cjcep.2023.10.026. |
[16] | Yuan XD, Wang JH, Wang YT, et al. Imaging characteristics of splenic inflammatory follicular dendritic cell sarcoma. Chinese Journal of Radiology. (2019) ; 53: (5): 375-380. doi: 10.3760/cma.j.issn.1005-1201.2019.05.009. |
[17] | Wang WW, Dong Y, Wang SW, et al. A case of inflammatory myofibroblastic tumor of the spleen. Chinese Medical Imaging Technology. (2016) ; 32: (4): 577. doi: 10.13929/j.1003-3289.2016.04.025. |
[18] | Li Y, Yang WB, Ke XK. Comparative analysis of imaging manifestations and pathology of multiple nodular splenic sinus bank cell hemangiomas. Radiology Practice. (2023) ; 38: (2): 183-187. doi: 10.13609/j.cnki.1000-0313.2023.02.012. |
[19] | Liu M, Liu HL, Liu Y. Analysis of imaging manifestations of splenic hamartoma. Journal of Medical Imaging. (2012) ; 22: (7): 1161-1163. doi: 10.3969/j.issn.1006-9011.2012.07.036. |
[20] | Liu GJ, Bo XH, Ye J, et al. Clinical value of laparoscopic surgery in the treatment of sclerosing angiomatous nodular transformation of the spleen. Journal of Laparoscopic Surgery. (2022) ; 27: (3): 189-193. doi: 10.13499/j.cnki.fqjwkzz.2022.03.189. |
[21] | Gold JE, Okyay RA, Licht WE, et al. Investigation of long COVID prevalence and its relationship to Epstein-Barr virus reactivation. Pathogens. (2021) ; 10: (6): 763. |
[22] | Su Y, Yuan D, Chen DG, et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell. (2022) ; 185: (5): 881-895. e20. |


