
Effectiveness and safety of thoracic manipulation in the treatment of neck pain: An updated systematic review and meta-analysis
Abstract
BACKGROUND:
The purpose of this meta-analysis was to evaluate the effectiveness and safety of thoracic manipulation (TM) in patients with neck pain (NP).
OBJECTIVE:
The purpose of this meta-analysis was to evaluate the effectiveness and safety of thoracic manipulation (TM) in patients with neck pain (NP).
METHODS:
Seven electronic databases were searched from their inception through October 2023 by two authors. The methodological quality assessments were performed with the Physiotherapy Evidence Database (PEDro) scale. Pain, cervical range of motion (ROM), disability, and quality of life (QOL) were estimated for TM treatment in patients with NP.
RESULTS:
Eighteen randomized controlled trials (RCTs) with 914 patients were included with a PEDro score of 6.923
CONCLUSIONS:
TM provides short-term effect on relieving neck pain, increasing cervical ROM, and disability in patients with NP without serious side effects. Continuous therapy and distraction therapy are recommended as optimal choice on reducing pain and improving cervical ROM, especially in patients with chronic NP (
1.Introduction
Neck pain (NP) is a common disease and a potential cause of disability. The annual prevalence of NP is approximately 15%–20% in general population and 15%–60% in the workforce. Based on the duration of the symptoms, NP is divided into acute NP (less than 7 days), subacute NP (between 7 days and 3 months) and chronic NP (more than 3 months) [1]. The main symptom of NP is cervical pain and stiffness which usually radiate to the occiput, nuchal muscles, shoulders and upper limbs [2]. These symptoms affect patients’ daily life and work, cause disability, increase social burden, and even affect patients’ mood, leading to anxious or depression. According to the Global Burden of Disease 2010 Study, NP is the fourth leading cause of disability, rank behind back pain, depression, and arthralgias [3].
NP management may be applied using a different treatment approach’s like; acupuncture, massage therapy, exercise therapy, traction, yoga and spinal manipulation. Although these interventions have some effects on patients with NP, the evidence for these methods is insufficient [4]. Furthermore, the use of cervical manipulation can cause side effects, such as neurological deficits, and headache. Due to the safety of thoracic mobilization or manipulation (TM), the use of TM has gradually increased [5, 6]. TM is defined as the mobilization or manipulation technique acting on any segment of the thoracic spine, including the cervicothoracic junction. TM include both passive and skilled manual therapy techniques that are applied to joints and associated soft tissues at different speeds and amplitudes using interactive physiological or assistive movements to achieve therapeutic purposes [7]. TM is commonly used in the treatment of pain near to thoracic vertebrae, especially in patients with NP [8]. A meta-analysis pointed out that thoracic manipulation has short term effect on the treatment of specific neck pain [9]. However, less previous meta-analysis evaluated the long-term effect and improvement of cervical range of motion (ROM) of TM [10, 11, 12]. The Neck Pain Guidelines (2017) recommended TM as Grade B or C evidence for the treatment of NP [13]. While, a lot of new research have published since 2017 which may change the results. Therefore, an updated meta-analysis is needed to re-evaluate the effect of TM. Hence, the aim of this review was to reassess the long - and short-term effects of TM on pain, disability and ROM in the management of NP.
2.Method
2.1Search strategy
An electronic search of the databases PubMed, Ovid, Embase, Medline, Cochrane Library, Wiley Online Library, and Science Direct was performed from their inception to October 1, 2022. We have registered in the PROSPERO database as (CRD42023426480) accessed at https://www.crd.york.ac.uk/PROSPERO.
The search was restricted to published articles written in English. The keywords for Science Direct were as follows: (“cervical vertebra” OR “neck pain” OR “spondylosis” OR “cervical spondylopathy”) AND (“thoracic manipulation” OR “thoracic spine manipulation” OR “thoracic thrust manipulation” OR “thoracic spine mobilization” OR “thoracic spine mobility”). The keywords used in the other databases were (“cervical vertebra” OR “neck pain” OR “spondylosis” OR “cervical spondylosis” OR “cervical spondylopathy” OR “cervical vertebra disease”), (“thoracic manipulation” OR “thoracic spine manipulation” OR “thoracic thrust manipulation” OR “thoracic nonthrust manipulation” OR “thoracic spine mobilization” OR “thoracic spine mobility” OR “thoracic nonthrust mobilization” OR “thoracic spine joint mobilization”) and (“randomized controlled trial” OR “RCT” OR “randomized” OR “controlled” OR “trial” OR “clinical”). The Boolean operator “AND” linked the three phrases. Titles and abstracts found in searches from the above databases were examined by two authors, and full texts of potentially eligible studies were subsequently screened.
To be as comprehensive as possible, reference lists of relevant reviews were manually searched by two separate authors to identify additional randomized controlled trials (RCTs). Final eligibility was determined through discussion when a discrepancy existed.
2.2Selection criteria
Two authors came to a consensus regarding the selection criteria applied independently. Studies were included if they met the following criteria: (1) Patients complained of NP or were diagnosed with NP; (2) The ages were between 18 and 60 years; (3) The articles were randomized controlled trials (RCTs); (4) The treatment group received treatment that included TM, and the comparison group received treatment that included manipulations/mobilization in other regions, sham TM, exercise or physiotherapy; (5) There was at least one measurement of pain or cervical ROM; (6) NP caused by cervical spinal disorder.
Studies were excluded if they met the following criteria: (1) Diagnosed with a specific NP, such as cervical radiculopathy, myelopathy, and fibromyalgia syndrome, or had a history of whiplash or cervical surgery; (2) The purpose of comparison between the experimental group and the control group was not to test the effectiveness of TM; (3) The language was not English; (4) The full text was not available; (5) Data were not extracted. A consensus was reached by the authors through discussion if a discrepancy existed.
2.3Data collection and quality assessment
Data extracted independently by two authors included characteristics of the study and population, details of the interventions for the experimental group and control group separately, outcomes, and side effects. Outcomes for this review were pain, cervical ROM, neck disability, and QOL. Pain was assessed by Numeric Pain Rating Scale (NPRS) or the Visual Analog Scale (VAS), disability was assessment by Neck Disability Index (NDI) or the Northwick Park Pain Questionnaire (NPQ), while, QOL were assessed via the SF36 health-related quality of life questionnaire (SF36). As one of a main outcome, cervical ROM were collected in all planes. The data we needed that were not mentioned are represented by “no report” (NR).
The 11-item Physiotherapy Evidence Database (PEDro) scale was used to assess the methodological quality of the articles, with sufficient reliability for evaluating the physical therapy RCT quality based on consensus judgments [14]. The scores of eligible RCTs were cited as the available scores from the PEDro database or were assessed manually by two authors separately. The PEDro scale score item consisted of random allocation, concealed allocation, baseline similarity, blinding of subjects, therapists and assessors, measures of key outcomes from more than 85% of subjects, intention-to-treat analysis, between-group statistical comparisons, point measures and measures of variability. An article that scored seven or above was considered high quality, a score of five to six was considered fair quality, and a score of four or below was considered poor quality [9].
2.4Statistical analyses
For continuous data, the standard mean difference (SMD) with 95% confidence interval (CI) was used. The I2 statistic was used to assess statistical heterogeneity in the included studies, while
Statistics Data Analysis Special Edition software (Stata SE, V.12.0; Stata Corp LP, College Station, Texas, USA) was applied in the statistical analysis.
Table 1
The methodological quality of the included studies
| ID | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Score | Eligibility criteria |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [1] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 | Y |
| [15] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 | Y |
| [16] | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8 | Y |
| [17] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 | N |
| [18] | Y | N | Y | N | N | N | N | N | Y | Y | 4 | Y |
| [19] | Y | N | Y | N | N | N | Y | N | Y | Y | 5 | Y |
| [20] | Y | N | Y | N | N | Y | Y | N | Y | Y | 6 | N |
| [21] | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 | Y |
| [22] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 | Y |
| [23] | Y | Y | Y | N | N | N | Y | N | Y | Y | 6 | Y |
| [24] | Y | Y | Y | Y | N | Y | Y | N | Y | Y | 8 | Y |
| [25] | Y | Y | Y | Y | N | Y | Y | Y | Y | Y | 9 | Y |
| [26] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 | Y |
| [27] | Y | Y | Y | N | N | Y | N | N | Y | Y | 6 | Y |
| [28] | Y | Y | Y | N | N | N | Y | Y | Y | Y | 7 | Y |
| [29] | Y | Y | Y | N | N | Y | N | Y | Y | Y | 7 | Y |
| [30] | Y | Y | Y | N | N | Y | N | Y | Y | Y | 7 | Y |
| [31] | Y | Y | Y | N | Y | Y | Y | N | Y | Y | 8 | Y |
Notes: 1, Random allocation; 2, Concealed allocation; 3, Baseline similarity; 4, Blinding of subjects; 5, Blinding of therapists; 6, Blinding of assessors; 7, Measures of key outcomes from more than 85% of subjects; 8, Intention to treat analysis; 9, Between-group statistical comparisons; 10, Point measures and measures of variability.
3.Computer simulation and results
3.1Statistical analyses study selection
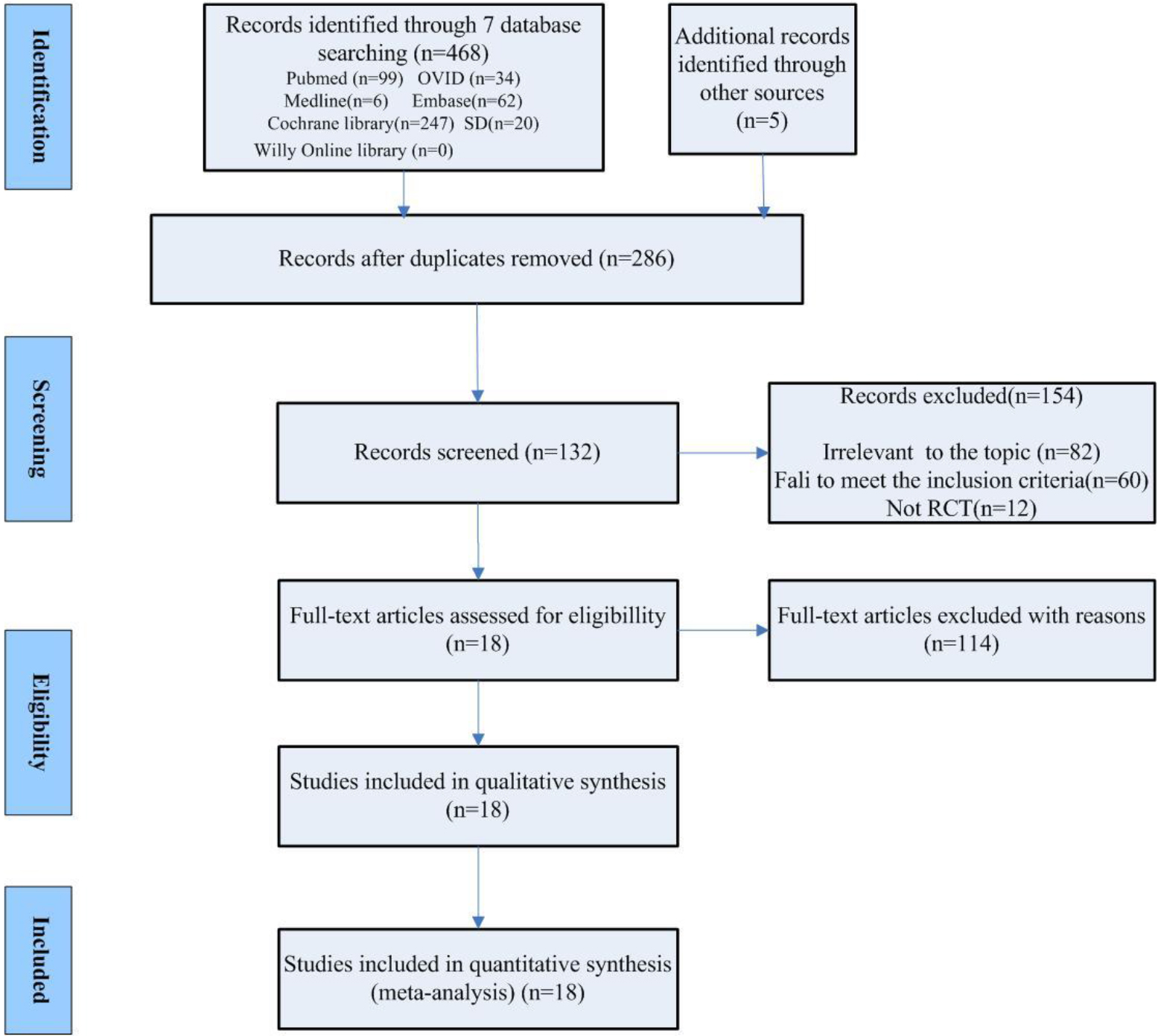
A total of 468 articles retrieved from 7 electronic databases and manual searches were identified based on the predefined search strategy. After removing duplicates and ineligible articles by screening titles and abstracts, 132 potentially eligible articles were identified. The full texts of these articles were scrutinized, leading to the final inclusion of 18 eligible studies included in this review [1, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31]. The search flowchart is shown in Fig. 1.
Figure 1.
Search flowchart of the meta-analysis. Flow diagram illustrating search strategy.
3.2Methodological quality
All eligible articles assessed the methodological quality according to the PEDro scale. The quality score ranged from 4 [18] to 9 [25] points (6.923
3.3Study characteristics
This review involved 18 studies with 914 subjects (471 in the experimental group, 443 in the control group). The characteristics of the population, interventions, comparison and outcomes are presented as follows, and more details are given in Table 2.
Table 2
The characteristics of the included studies
| Author year | Cases E/C | NPT | Duration | D | Course of treatment | E vs C | Measures |
|---|---|---|---|---|---|---|---|
| Paulo 2015 | 32 16/16 | Pain or fatigue | NR | a single session | TM vs placebo | VAS | |
| Gonzalez 2009 | 45 23/22 | AMNP | E, 18 d | Distraction | TM: 1 session/w, Electro/thermal: 2 session/w; 3 w | TM | NPRS; NPQ ROM |
| Herman 2011 | 120 60/60 | CMNP | AP | 15 min/session, 2 sessions/w, 4 w | TM | NPRSROM NPQ SF36 | |
| Suvarnnato 2013 | 26 13/13 | CMNP | Screw thrust | A single session | TM vs placebo | VAS; ROM | |
| Aslak 2004 | 41 24/17 | Neck shoulder | NR | NR | 4 sessions/1 w | TM vs exercise | VAS |
| Jinmo 2015 | 30 15/15 | CMNP | AP | 30 min/sessions, 3 sessions/w, 6 w | TM | VAS | |
| Kwan- 2016 | 31 16/15 | CMNP | NR | 35 min/d, 3 d/w, 10 w | TM | VAS;NDI; ROM NDI | |
| Joshua 2010 | 140 70/70 | NP | E, 62.5 d | Distraction AP | 2 session/w, 1 w 1 session/w, 3 w | TM | NPRS; |
| Raquel 2012 | 62 33/29 | Bilateral CMNP | E, 3.8 y | AP | A single session | TM vs cervical thrust | NPRS; ROM |
| Rob Sillevis 2010 | 100 50/50 | CMNP | E, 23.3 m; C, 25.3 m | AP | A single session | TM vs placebo | sVAS |
| Joshua 2005 . | 36 19/17 | MNP | E, 12.2 w | AP | A single session | TM vs placebo | VAS |
| Cheryl L 2017. | 24 12/12 | MNP | Less than 6 w | AP | A single session | TM vs placebo | NPRS |
| González 2009 | 45 23/22 | MNP | E, 19.5 d | Distraction | 2 session/w; 5 session | TM | VAS, NPQ ROM; |
| John 2008 | 32 22/10 | MNP | NR | AP | A single session | TM vs placebo | ROM |
| Masaracchio 2013 | 66 34/32 | MNP | E, 37.3 d | AP | 3 sessions | TM | NPRS; NDI |
| Puentedura 2011 | 24 10/14 | MNP | 18.8 d | distraction; AP | 1–3 sessions, 1 w 4–5 sessions, 1 w | TM | NPRS; NDI |
| Khoja 2015 | 18 10/8 | MNP | NR | 2 sessions /1 w; 6 w | TM | NPRS, NDI ROM | |
| Shriya 2020 | 4221/21 | MNP | NR | NR | A single session | TM VS CT junction mobilization | NRS ROM |
Notes:; D, duration; HEP, home exercise program; M, month; NDI, neck disability index; NPQ, the Northwick Park Neck Pain Questionnaire; NPRS, numeric pain rating scale; NR, no reported; ROM, range of motion; VAS, visual analogue scale; W, week; NPT,neck pain Type; P, position; MNP, mechanical neck pain; NP, neck pain; CM,cervical mobilization; AP, anterior-posterior; D, distraction.
3.3.1Patients
The age of the participants ranged from 18 to 65 years. Only two articles explicitly stated gender differences, one of which consisted of all female patients and the other of which had more female patients than male patients [1, 27]. In terms of duration, the participants in 3 articles [15, 26, 29] were in the acute phase, and those in 3 articles [25, 28, 31] were in the acute and subacute phases. Seven articles reported the chronic phase [1, 16, 17, 19, 20, 22, 23]. Participants in 2 articles [21, 30] were in all three phases, and the phase was not clearly mentioned in 3 articles [18, 24, 27].
3.3.2Interventions
TM techniques varied substantially in the included studies in terms of the patient position, segment, range, velocity, amplitude, direction of TM and course of treatment. The patient position included seated (2 articles) [15, 26], supine (6 articles) [1, 16, 20, 22, 23, 24], prone (2 articles) [17, 31] and seated plus supine (3 articles) [19, 21, 29]. Ten articles [1, 20, 21, 22, 23, 24, 25, 28, 29, 31] mentioned that the velocity of TM was high, while other articles did not report the velocity. Six articles [1, 20, 24, 25, 28, 31] mentioned that the amplitude of TM was low, while others did not clearly report the amplitude. This review subgrouped the TM technique using the direction of TM classification into anterior-posterior [16, 19, 22, 23, 24, 25, 27, 28] distraction [15, 26] or screw thrust [17] directions and performed a subgroup analysis.
3.3.3Comparison
In the included studies, six articles [1, 17, 23, 24, 25, 27] compared TM to placebo TM, six articles [18, 19, 20, 21, 29, 31] compared TM plus exercise to exercise, and the others compared TM plus comprehensive physical therapy to comprehensive physical therapy.
3.3.4Outcomes
The outcomes included pain (VAS in 7 studies [1, 17, 19, 20, 23, 24, 26], NPRS in 9 studies [15, 16, 21, 22, 25, 28, 29, 30, 31], CROM in 9 articles) [15, 16, 17, 20, 22, 26, 27, 30, 31], disability (NPQ in 3 articles [15, 16, 26], NDI in 5 articles [20, 21, 28, 29, 30], and QOL (in 1 article, 120 patients) [16]. Eight studies [1, 17, 22, 23, 24, 25, 27, 31] assessed immediate effects after a single session, and nine articles [15, 16, 18, 19, 20, 21, 26, 28, 29, 30] examined cumulative effects. One article [18] did not describe immediate or short-term results but only follow-up results (12 months). The follow-up varied from 24 hours to 12 months in 6 included studies. The follow-up visits were more than 6 months in only 4 studies [16, 18, 21, 29].
Effect size of pain
Pain data (16 articles, 840 subjects) were assessed with the VAS and NPRS, which showed a high correlation [33]. The pooled effect size indicated significant heterogeneity (
Figure 2.
Forest plots of pain and disability. Efficacy of TM vs placebo. Forest plot was built considering
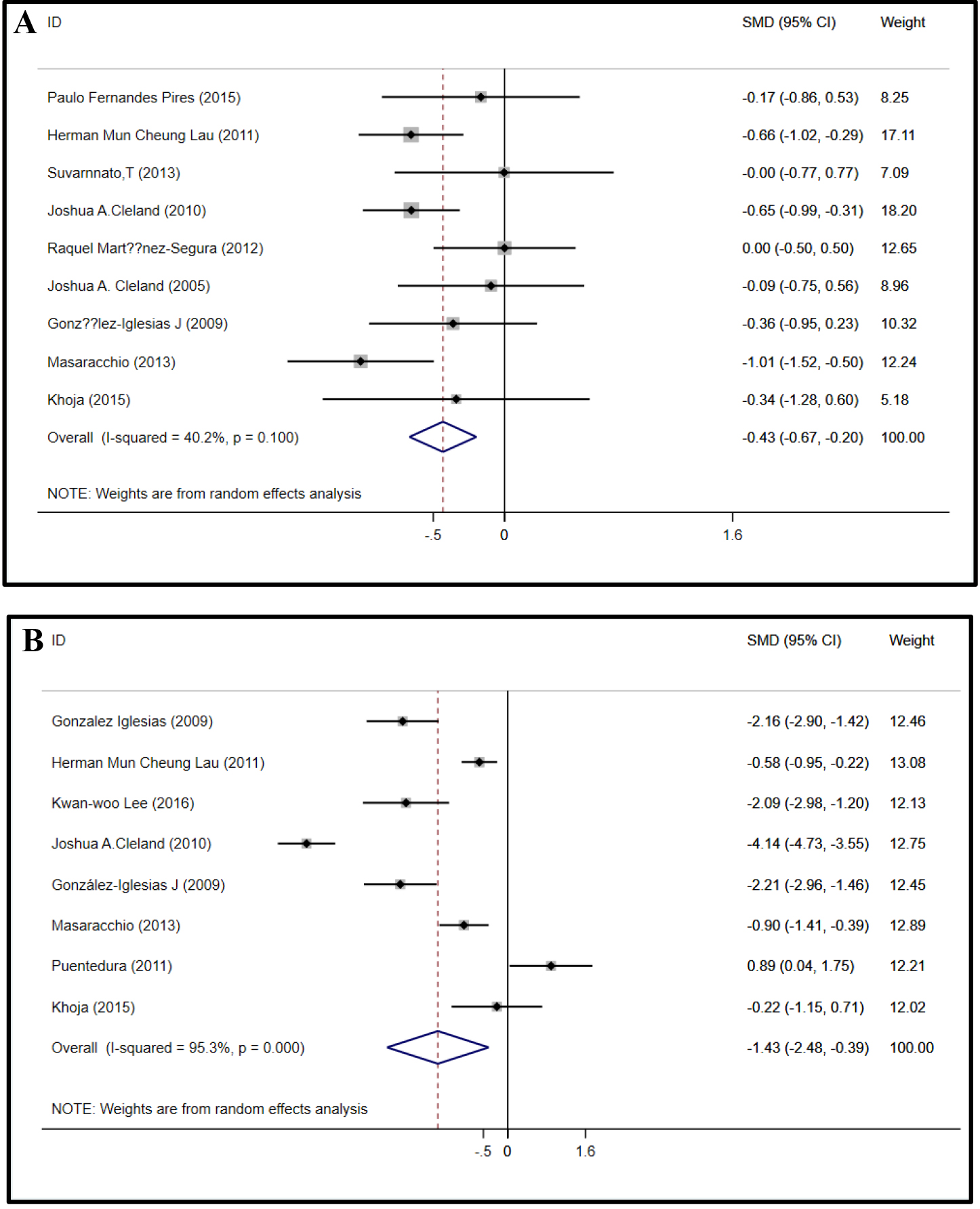
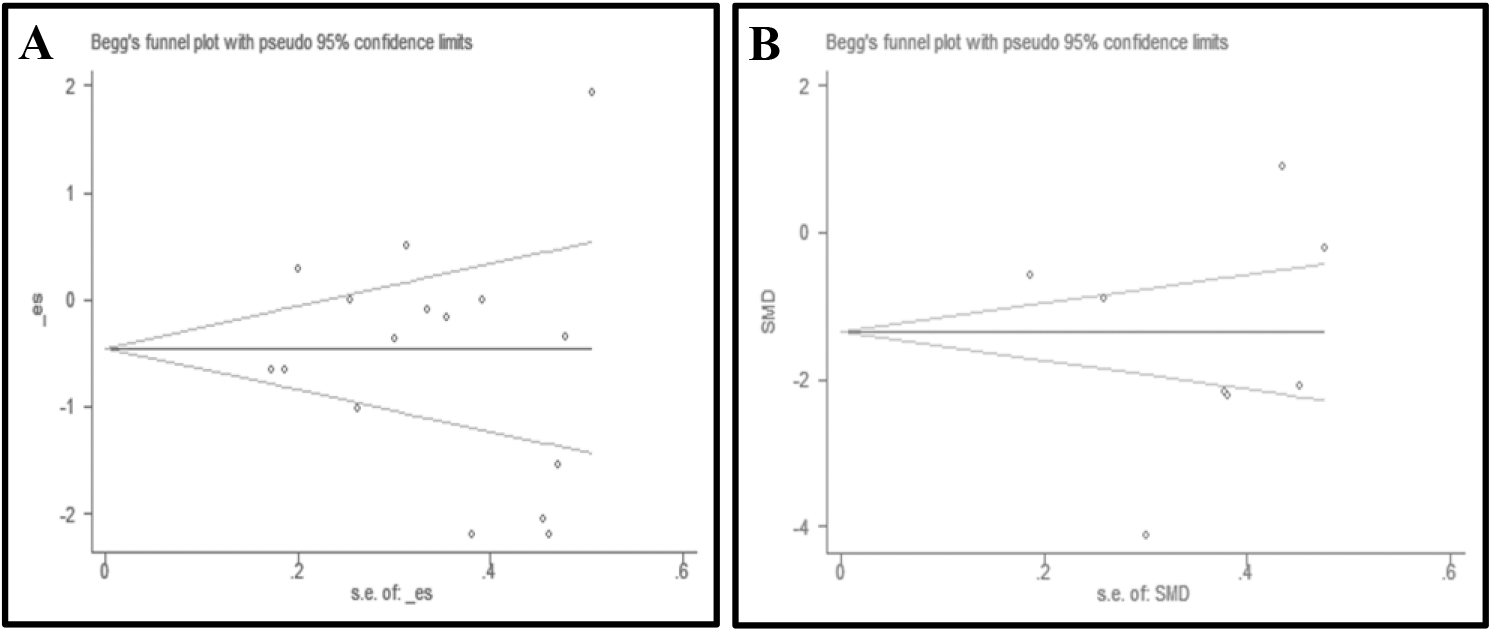
Figure 3.
Funnel plots of pain and disability.
Follow-up assessments for pain (at least six months) were reported in 4 articles with 325 subjects [16, 18, 21, 29]. The extracted data were pooled with a random-effects model and showed substantial heterogeneity and no statistical significance (
Effect size of ROM
The cervical ROM was measured across all 9 studies (421 patients) [15, 16, 17, 20, 22, 26, 27, 30, 31]. Separate meta-analyses were conducted to evaluate the changes in cervical ROM in all planes. Meta-analysis of 8 studies [15, 16, 17, 20, 22, 26, 30, 31] (
Figure 4.
Forest plots of ROM in all planes.
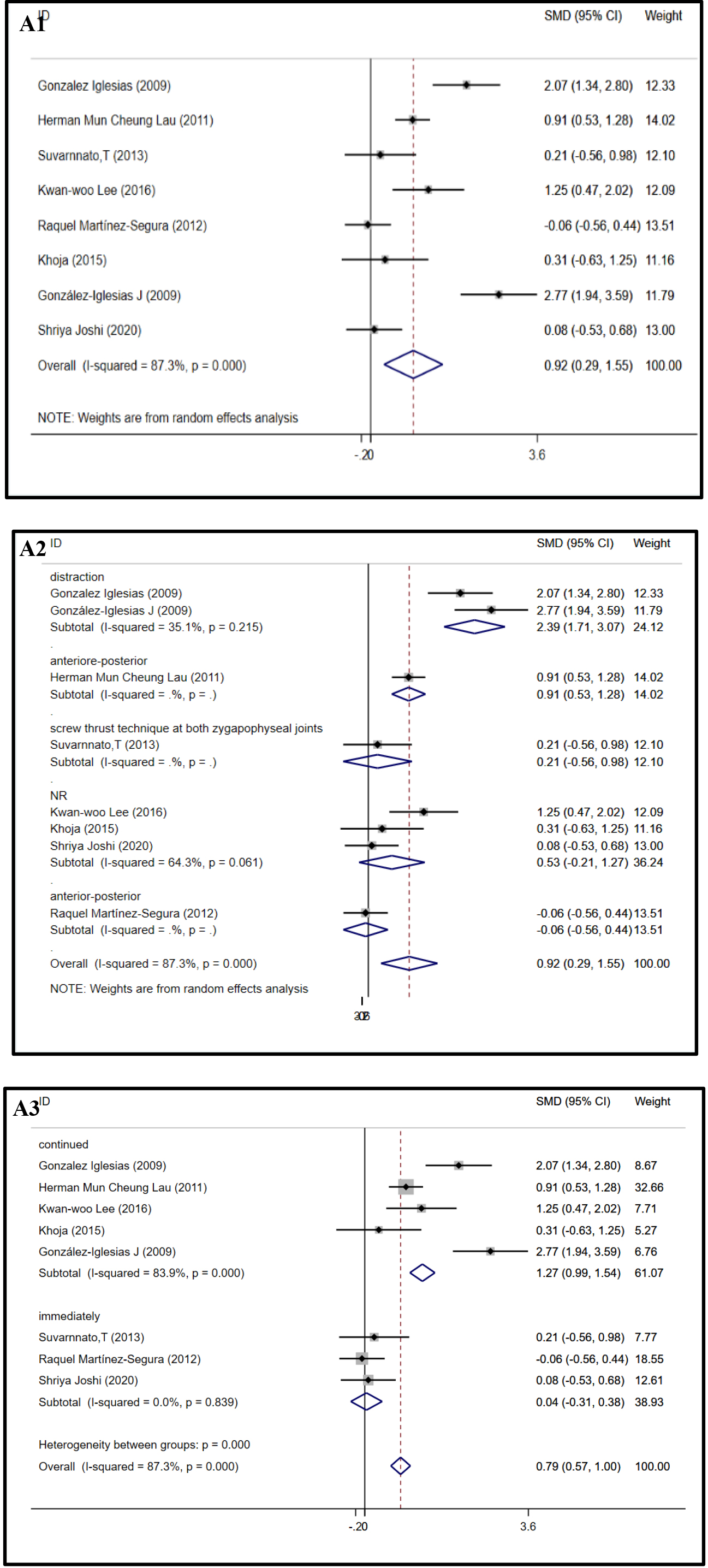
Figure 4.
continued.
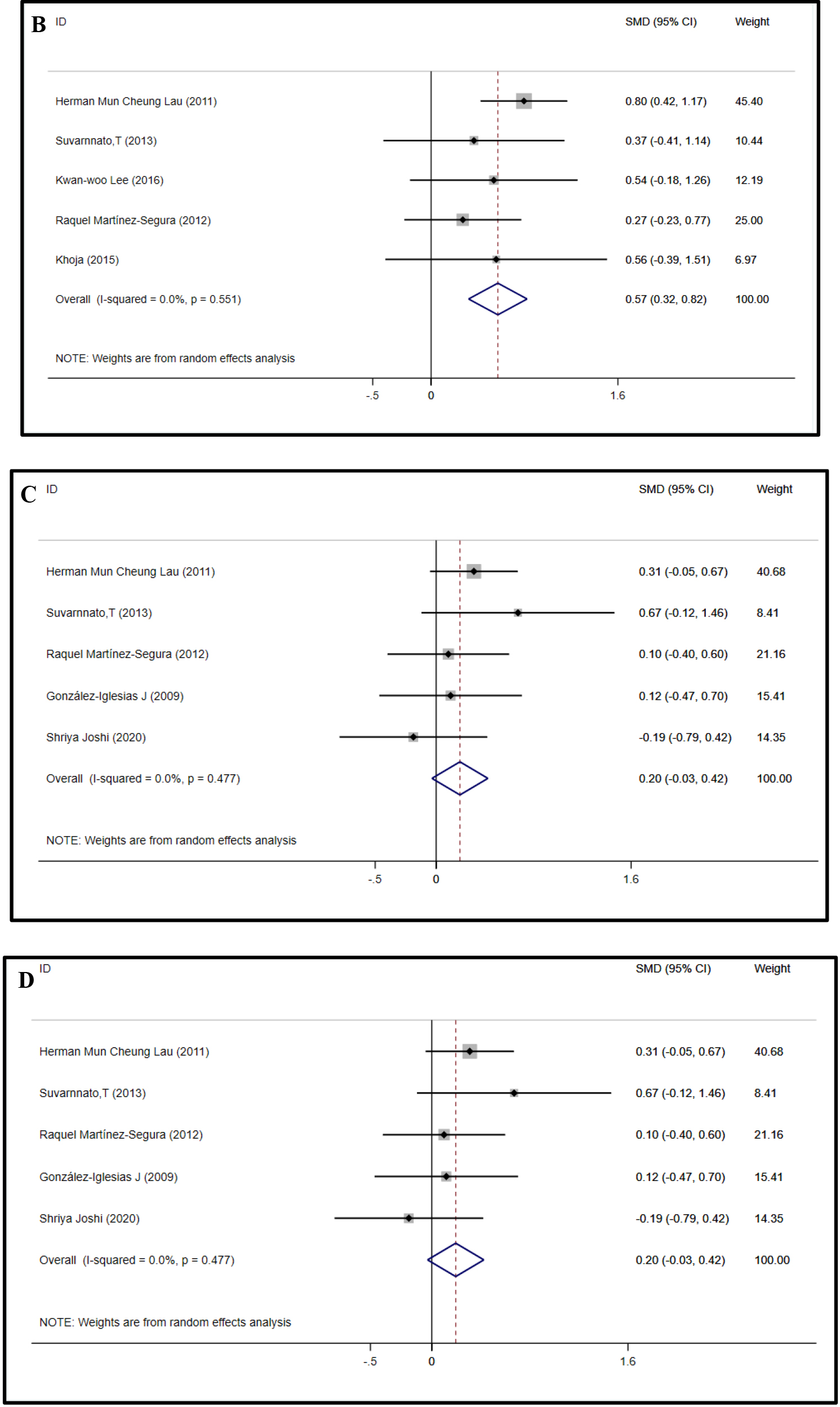
Figure 4.
continued.
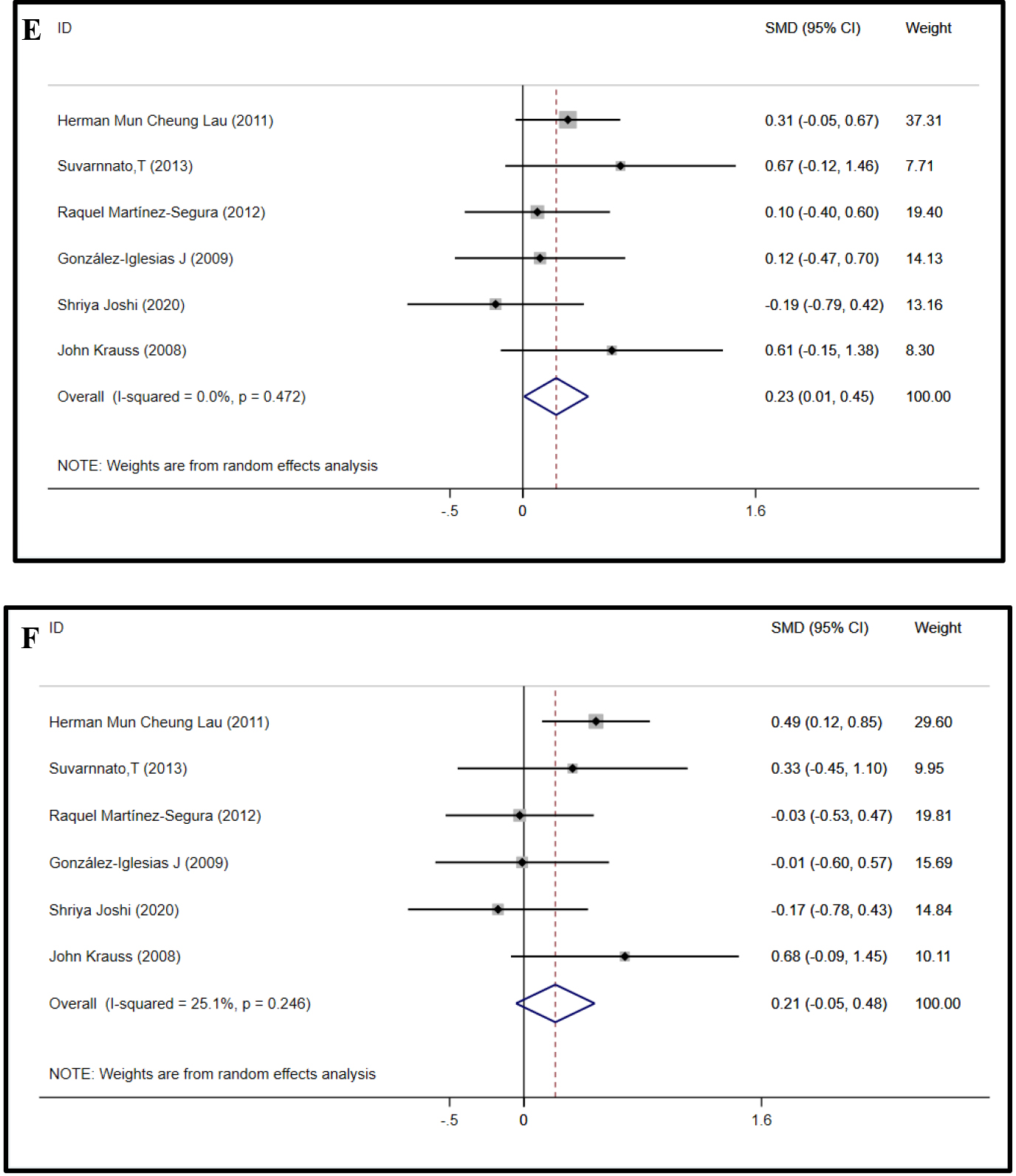
model was used for the remaining studies (5 studies, 257 subjects), and the results showed that TM improved the cervical ROM of extension (SMD
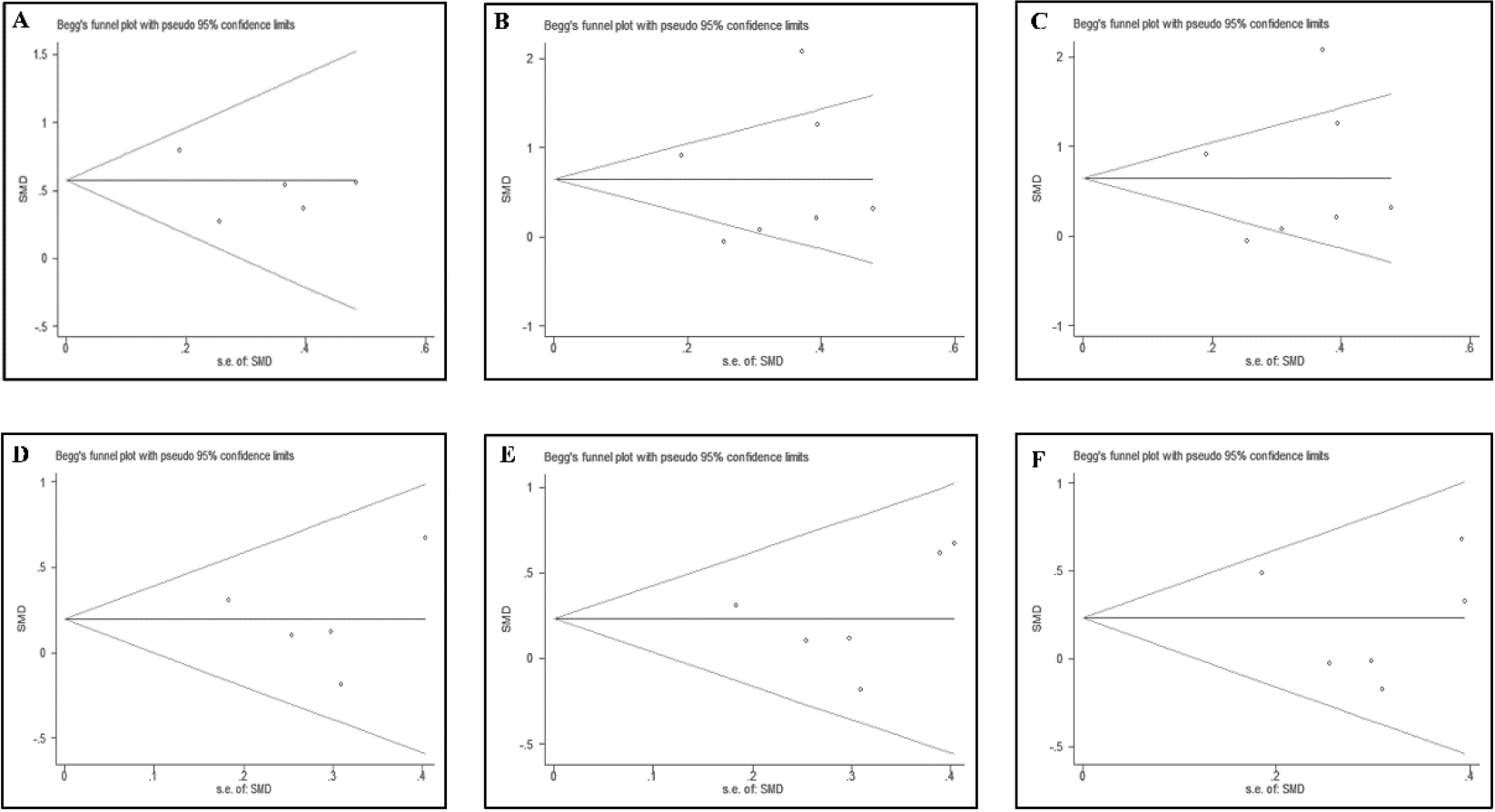
The publication bias of cervical ROM in all planes was separately performed by Begg’s tests and Egger’s tests. The results showed that publication bias of cervical ROM in all planes was not identified in Begg’s tests and Egger’s tests, which is shown in S3 Table (Fig. 5).
Figure 5.
Funnel plots of ROM in all planes.
Effect size of disability
Disability functions were assessed with NDI and NPQ in 8 articles (489 subjects) [15, 16, 20, 21, 26, 28, 29, 30]. The NDI and NPQ scores were merged due to the high correlation between them [34]. The pooled effect size of disability showed significant heterogeneity (
Meta-analysis of disability follow-up data for more than six months in 3 articles with 284 subjects showed no statistical significance (SMD
Effect size of QOL
QOL was evaluated with the health-related quality of life questionnaire (SF36) in 1 study (120 subjects) [16] which consisted of a mental component score (MCS) and physical component score (PCS) [35]. Consequently, the meta-analysis was unable to perform. The SMD (
3.4Adverse events
Only 2 articles clearly stated that patients presented adverse reactions, one [22] reported fatigue after receiving TM and the another one [29] reported headache and upper back pain. Seven articles [16, 20, 21, 24, 25, 27, 28] clearly reported that there were no adverse reactions after receiving TM. The remaining 8 articles [1, 15, 17, 18, 19, 23, 26, 30] did not report whether adverse events had occurred.
4.Discussion
This meta-analysis evaluated the effect of TM in patients with NP. To the limit of our knowledge, this is a preliminary meta-analysis study that simultaneously assesses improving effects of TM on pain, cervical ROM, QOL and disability among subjects with NP. This review included 18 RCTs with 914 patients and demonstrated that TM provide a short-term effect on improving pain, ROM, QOL-PCS and neck disability among patients with NP.
The results of the present review demonstrated that TM provide a short-term effect on alleviating pain, especially in patients with a long duration (
Compared with previous meta-analyses focusing on this topic [9, 12, 37, 38], although the benefits of TM on patients with NP remained similar, there were still differences from previous reviews. First, this study included more RCTs and a larger sample size. Second, the improving cervical ROM of TM on NP patients were first analyzed in this study. Third, this study analyzed the methodological quality with the PEDro scale but not the Cochrane Collaboration scale [39], which was not specifically targeted in physical therapy RCTs [12]. Finally, subgroup analyses according to the duration of NP, the course of treatment, comparison and the direction of TM were analyzed to optimize the clinical application of TM, while none of the others were analyzed.
Several limitations existed in this review. First, the influence of TM on the participation and environmental level in patients with NP was not investigated due to a lack of relevant data [40]. Second, considerable heterogeneities existed in our study due to the variations in the TM protocols and control interventions. In the included studies, the standardization of TM protocols was challenged by the treatment sessions, manipulation direction, and vertebral segment. The control interventions also varied and were diverse from each other. Moreover, two studies were proven to be the main causes of heterogeneity in sensitivity analysis when assessing cervical ROM of right lateral flexion, left rotation and right rotation, which were conducted by Gonzalez Iglesias et al. [32] and Shriya Joshi et al. [30] Compared with other studies, research led by Gonzalez Iglesias et al. [32] included patients with acute mechanical neck pain, which is different from other studies. However, a study led by Shriya Joshi et al. [30] did not demonstrate the details of duration, position, direction, segment, range velocity and amplitude. Third, the blinding of therapists and subjects was not well conducted in most of the included studies due to the nature of physical therapy [41]. Moreover, QOL was evaluated by only one article, which largely influenced our results. Therefore, future studies are strongly recommended to evaluate QOL and describe the intervention process in detail, including the operation segment, patient and therapist’s position, frequency, amplitude, direction, range, course of treatment, etc.
5.Conclusion
TM provide a short-term effect on reducing neck pain, increasing cervical ROM, and disability in patients with NP without serious side effects. Continuous therapy and distraction therapy are recommended as an optimal choice on reducing pain and improving cervical ROM, especially in patients with chronic NP (>3 months). The TM-induced improvements in the QOL of patients with NP should be verified by further high-quality RCTs.
Acknowledgments
We would like to thank associate professor Deng kai of West China Hospital, Sichuan University, for providing valuable suggestions and comments. This research was supported by the Key Research and Development Project of the Science and Technology Department of Sichuan Province (No. 2016SZ0039; No. 2018SZ0082) and the Medical Association of Sichuan Province (No. S15063), Chengdu, China.
Conflict of interest
None to report.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/THC-248034.
References
[1] | Pires PF, Packer AC, Dibai-Filho AV, Rodrigues-Bigaton D. Immediate and Short-Term Effects of Upper Thoracic Manipulation on Myoelectric Activity of Sternocleidomastoid Muscles in Young Women With Chronic Neck Pain: A Randomized Blind Clinical Trial. J Manipulative Physiol Ther. (2015) ; 38: (8): 555-563. doi: 10.1016/j.jmpt.2015.06.016. |
[2] | Binder A. The diagnosis and treatment of nonspecific neck pain and whiplash. Eura Medicophys. (2007) ; 43: (1): 79-89. |
[3] | Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet (London, England). (2016) ; 388: (10053): 1545-1602. doi: 10.1016/S0140-6736(16)31678-6. |
[4] | Cohen SP. Epidemiology, diagnosis, and treatment of neck pain. Mayo Clinic proceedings. (2015) ; 90: (2): 284-299. doi: 10.1016/j.mayocp.2014.09.008. |
[5] | Puntumetakul R, Suvarnnato T, Werasirirat P, Uthaikhup S, Yamauchi J, Boucaut R. Acute effects of single and multiple level thoracic manipulations on chronic mechanical neck pain: a randomized controlled trial. Neuropsychiatr Dis Treat. (2015) ; 11: : 137-144. doi: 10.2147/NDT.S69579. |
[6] | Salom-Moreno J, Ortega-Santiago R, Cleland JA, Palacios-Ceña M, Truyols-Domínguez S, Fernández-de-las-Peñas C. Immediate changes in neck pain intensity and widespread pressure pain sensitivity in patients with bilateral chronic mechanical neck pain: a randomized controlled trial of thoracic thrust manipulation vs non-thrust mobilization. J Manipulative Physiol Ther. (2014) ; 37: (5): 312-319. doi: 10.1016/j.jmpt.2014.03.003. |
[7] | Haleema B, Riaz H. Effects of thoracic spine manipulation on pressure pain sensitivity of rhomboid muscle active trigger points: A randomized controlled trial. JPMA The Journal of the Pakistan Medical Association. (2021) ; 71: (7): 1720-1724. doi: 10.47391/JPMA.02-256. |
[8] | Raja GP, Bhat NS, Fernández-de-Las-Peñas C, et al. Effectiveness of deep cervical fascial manipulation and yoga postures on pain, function, and oculomotor control in patients with mechanical neck pain: study protocol of a pragmatic, parallel-group, randomized, controlled trial. Trials. (2021) ; 22: (1): 574. doi: 10.1186/s13063-021-05533-w. |
[9] | Walser RF, Meserve BB, Boucher TR. The effectiveness of thoracic spine manipulation for the management of musculoskeletal conditions: a systematic review and meta-analysis of randomized clinical trials. J Man Manip Ther. (2009) ; 17: (4): 237-246. doi: 10.1179/106698109791352085. |
[10] | Tsegay GS, Gebregergs GB, Weleslassie GG, Hailemariam TT. Effectiveness of Thoracic Spine Manipulation on the Management of Neck Pain: A Systematic Review and Meta-Analysis of Randomized Control Trials. Journal of pain research. (2023) ; 16: : 597-609. doi: 10.2147/JPR.S368910. |
[11] | Gross A, Langevin P, Burnie SJ, et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. The Cochrane database of systematic reviews. (2015) (9): Cd004249. doi: 10.1002/14651858.CD004249.pub4. |
[12] | Masaracchio M, Kirker K, States R, Hanney WJ, Liu X, Kolber M. Thoracic spine manipulation for the management of mechanical neck pain: A systematic review and meta-analysis. PloS one. (2019) ; 14: (2): e0211877. doi: 10.1371/journal.pone.0211877. |
[13] | Blanpied PR, Gross AR, Elliott JM, et al. Neck Pain: Revision 2017. J Orthop Sports Phys Ther. (2017) ; 47: (7): A1-A83. doi: 10.2519/jospt.2017.0302. |
[14] | Maher CG, Sherrington C, Herbert RD, et al. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. (2003) ; 83: (8): 713-721. |
[15] | González-Iglesias J, Fernández-de-las-Peñas C, Cleland JA, et al. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial. Man Ther. (2009) ; 14: (3): 306-313. doi: 10.1016/j.math.2008.04.006. |
[16] | Lau HM, Wing Chiu TT, Lam TH. The effectiveness of thoracic manipulation on patients with chronic mechanical neck pain – a randomized controlled trial. Man Ther. (2011) ; 16: (2): 141-147. doi: 10.1016/j.math.2010.08.003. |
[17] | Suvarnnato T, Puntumetakul R, Kaber D, et al. The effects of thoracic manipulation versus mobilization for chronic neck pain: a randomized controlled trial pilot study. J Phys Ther Sci. (2013) ; 25: (7): 865-871. doi: 10.1589/jpts.25.865. |
[18] | Savolainen A, Ahlberg J, Nummila H, Nissinen M. Active or passive treatment for neck-shoulder pain in occupational health care? A randomized controlled trial. Occup Med (Lond). (2004) ; 54: (6): 422-424. doi: 10.1093/occmed/kqh070. |
[19] | Yang J, Lee B, Kim C. Changes in proprioception and pain in patients with neck pain after upper thoracic manipulation. J Phys Ther Sci. (2015) ; 27: (3): 795-798. doi: 10.1589/jpts.27.795. |
[20] | Lee KW, Kim WH. Effect of thoracic manipulation and deep craniocervical flexor training on pain, mobility, strength, and disability of the neck of patients with chronic nonspecific neck pain: a randomized clinical trial. J Phys Ther Sci. (2016) ; 28: (1): 175-180. doi: 10.1589/jpts.28.175. |
[21] | Cleland JA, Mintken PE, Carpenter K, et al. Examination of a clinical prediction rule to identify patients with neck pain likely to benefit from thoracic spine thrust manipulation and a general cervical range of motion exercise: multi-center randomized clinical trial. Phys Ther. (2010) ; 90: (9): 1239-1250. doi: 10.2522/ptj.20100123. |
[22] | Martínez-Segura R, De-la-Llave-Rincón AI, Ortega-Santiago R, Cleland JA, Fernández-de-Las-Peñas C. Immediate changes in widespread pressure pain sensitivity, neck pain, and cervical range of motion after cervical or thoracic thrust manipulation in patients with bilateral chronic mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. (2012) ; 42: (9): 806-814. doi: 10.2519/jospt.2012.4151. |
[23] | Sillevis R, Cleland J, Hellman M, Beekhuizen K. Immediate effects of a thoracic spine thrust manipulation on the autonomic nervous system: a randomized clinical trial. J Man Manip Ther. (2010) ; 18: (4): 181-190. doi: 10.1179/106698110X12804993427126. |
[24] | Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther. (2005) ; 10: (2): 127-135. doi: 10.1016/j.math.2006.02.005. |
[25] | Sparks CL, Liu WC, Cleland JA, et al. Functional Magnetic Resonance Imaging of Cerebral Hemodynamic Responses to Pain Following Thoracic Thrust Manipulation in Individuals With Neck Pain: A Randomized Trial. J Manipulative Physiol Ther. (2017) ; 40: (9): 625-634. doi: 10.1016/j.jmpt.2017.07.010. |
[26] | González-Iglesias J, Fernández-de-las-Peñas C, Cleland JA, Mdel R. Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. (2009) ; 39: (1): 20-27. doi: 10.2519/jospt.2009.2914. |
[27] | Krauss J, Creighton D, Ely JD, Podlewska-Ely J. The immediate effects of upper thoracic translatoric spinal manipulation on cervical pain and range of motion: a randomized clinical trial. J Man Manip Ther. (2008) ; 16: (2): 93-99. doi: 10.1179/106698108790818530. |
[28] | Masaracchio M, Cleland JA, Hellman M, Hagins M. Short-term combined effects of thoracic spine thrust manipulation and cervical spine nonthrust manipulation in individuals with mechanical neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. (2013) ; 43: (3): 118-127. doi: 10.2519/jospt.2013.4221. |
[29] | Puentedura EJ, Landers MR, Cleland JA, Mintken PE, Huijbregts P, Fernández-de-Las-Peñas C. Thoracic spine thrust manipulation versus cervical spine thrust manipulation in patients with acute neck pain: a randomized clinical trial. J Orthop Sports Phys Ther. (2011) ; 41: (4): 208-220. doi: 10.2519/jospt.2011.3640. |
[30] | Khoja SS, Browder D, Daliman D, Piva SR. Benefits of thoracic thrust manipulation when applied with a multi-modal treatment approach in individuals with mechanical neck pain: A pilot randomized trial. Int J Phys Med Rehabil. (2015) ; 3: (306): 2. |
[31] | Joshi S, Balthillaya G, Neelapala YR. Immediate effects of cervicothoracic junction mobilization versus thoracic manipulation on the range of motion and pain in mechanical neck pain with cervicothoracic junction dysfunction: a pilot randomized controlled trial. Chiropractic & manual therapies. (2020) ; 28: : 1-8. doi: 10.1186/s12998-020-00327-4. |
[32] | González-Iglesias J, Fernández-de-las-Peñas C, Cleland JA, Alburquerque-Sendín F, Palomeque-del-Cerro L, Méndez-Sánchez R. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial. Manual Therapy. (2009) ; 14: (3): 306-313. doi: 10.1016/j.math.2008.04.006. |
[33] | Downie WW, Leatham PA, Rhind VM, Wright V, Branco JA, Anderson JA. Studies with pain rating scales. Ann Rheum Dis. (1978) ; 37: (4): 378-381. doi: 10.1136/ard.37.4.378. |
[34] | Hoving JL, O’Leary EF, Niere KR, Green S, Buchbinder R. Validity of the neck disability index, Northwick Park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders. Pain. (2003) ; 102: (3): 273-281. doi: 10.1016/S0304-3959(02)00406-2. |
[35] | Burholt V, Nash P. Short Form 36 (SF-36) Health Survey Questionnaire: normative data for Wales. J Public Health (Oxf). (2011) ; 33: (4): 587-603. doi: 10.1093/pubmed/fdr006. |
[36] | Huisman PA, Speksnijder CM, de Wijer A. The effect of thoracic spine manipulation on pain and disability in patients with non-specific neck pain: a systematic review. Disabil Rehabil. (2013) ; 35: (20): 1677-1685. doi: 10.3109/09638288.2012.750689. |
[37] | Cross KM, Kuenze C, Grindstaff TL, Hertel J. Thoracic spine thrust manipulation improves pain, range of motion, and self-reported function in patients with mechanical neck pain: a systematic review. J Orthop Sports Phys Ther. (2011) ; 41: (9): 633-642. doi: 10.2519/jospt.2011.3670. |
[38] | Young JL, Walker D, Snyder S, Daly K. Thoracic manipulation versus mobilization in patients with mechanical neck pain: a systematic review. J Man Manip Ther. (2014) ; 22: (3): 141-153. doi: 10.1179/2042618613Y.0000000043. |
[39] | Koperny M, Leśniak W, Jankowski M, Bała M. The Cochrane collaboration – therole in the evolution of evidence-based medicine and development of cooperation in Poland. Przegl Epidemiol. (2016) ; 70: (3): 508-520. |
[40] | Arsh A, Darain H, Iqbal M, Rahman MU, Ullah I, Khalid S. Effectiveness of manual therapy to the cervical spine with and without manual therapy to the upper thoracic spine in the management of non-specific neck pain; a randomized controlled trial. JPMA The Journal of the Pakistan Medical Association. (2020) ; 70: (3): 399-403. doi: 10.5455/JPMA.300523. |
[41] | Steffens D, Maher CG, Pereira LS, Stevens ML, Oliveira VC, Chapple M, et al. Prevention of Low Back Pain: A Systematic Review and Meta-analysis. JAMA internal medicine. (2016) ; 176: (2): 199-208. doi: 10.1001/jamainternmed.2015.7431. |


