
Effects of infant care posture and weight on static postural balance
Abstract
BACKGROUND:
Studies investigating postural balance during various infant care postures have not been reported yet.
OBJECTIVE:
The aim of this study was to measure static postural balance when holding an infant dummy in-arms and carrying an infant dummy on back according to different infant dummy weights.
METHODS:
Sixteen healthy young subjects participated in a balance test. Infant dummies with weights of 4.6 kg (1-month) and 9.8 kg (12-month) were used in this study. All subjects were asked to naturally stand on a force platform in two infant care postures (holding an infant in-arms and carrying an infant on one’s back). Center of pressure (COP) was measured from the force platform. Quantitative variables were derived from the COP. Two-way repeated measure analysis of variance (ANOVA) was performed to determine main effects of infant care postures, infant weight, and their interactions on COP variables.
RESULTS:
Back carrying a 12-month infant dummy had the greatest amplitude in all COP variables. Back carrying posture showed significantly greater mean distance and peak power, faster mean velocity, and wider COP area compared to holding posture (
CONCLUSIONS:
Our results could contribute to the prevention of musculoskeletal diseases or prevention of fall due to various infant care activities by developing an assisting device to improve postural balance.
1.Introduction
Lifting, holding, and carrying an infant in-arms are typical care activities in parent’s daily life. Repetitive strain and inefficient postures during such infant care activities cause biomechanical loads on the musculoskeletal system [1, 2]. Especially, inappropriate postures that are biomechanically stressful [3, 4, 25] caused by an infant’s constant and unpredictable motions can induce various musculoskeletal diseases. Specifically, 49% of back injuries are related to infant care activities such as lifting an infant [5]. Some studies have reported that inefficient postures during infant care for a long period time can induce lower back pain [6]. Furthermore, repetitive infant carrying motion can lead to lumbar lordosis [7, 8]. Therefore, understanding biomechanical risk factors of infant care motions is important to prevent the onset of musculoskeletal diseases and suggest effective motion strategies or ergonomic interventions.
Therefore, some studies have performed quantitative motion analysis during sling-based infant carrying or carrying in-arms. Schmid et al. have demonstrated that carrying a dummy in front can induce lumbar lordosis and suggested that carrying an infant alternating on both sides using a sling could effectively prevent musculoskeletal diseases [9]. Additionally, some studies have compared ankle, knee, and hip joint moments between wearing a mannequin infant with a baby carrier and carrying a mannequin infant in arms. A baby carrier is useful for decreasing the loading knee abduction moment and the loading knee extension moment [10]. Kim et al. have investigated peak joint moments at the shoulder, lumbar, ankle, knee, and hip joints during lifting-up of infant dummies [11]. They found that the lumbar extension moment was the greatest during lifting-up of an infant dummy compared to other joints.
It has been reported that an altered posture during lifting motion can cause back pain [12] and increase the risk of falls [13]. Actually, some studies have investigated postural balance during lifting motion [12, 13]. However, no studies have investigated postural balance during various infant care motions yet. A previous study has suggested that falls during infant care activities might be associated with postural imbalance [20]. It is important to provide quantitative indicators of postural balance risk factors during infant care activities for suggesting an effective infant care strategy. Therefore, the aim of this study was to investigate COP (center of pressure) based measures during holding an infant dummy in-arms and carrying an infant dummy on back according to different infant dummy weights.
2.Method
2.1Subjects
Sixteen healthy young subjects (8 men and 8 women) participated in our study (Table 1). They were recruited from a general student population of Konkuk University for this study. Subjects with any diseases such as musculoskeletal disease or limb injury that might affect their infant care activities and balance test were excluded. This study was approved by the ethics committee of Konkuk University. Written informed consent was obtained from each subject prior to experiments following the Declaration of Helsinki.
Table 1
Subject demographics
| Variables | Mean | SD |
|---|---|---|
| Age (years) | 22.6 | 2.0 |
| Height (cm) | 167.7 | 7.3 |
| Weight (kg) | 63.7 | 10.0 |
| BMI (kg/m2) | 22.5 | 2.2 |
SD, standard deviation.
2.2Experiments and analysis
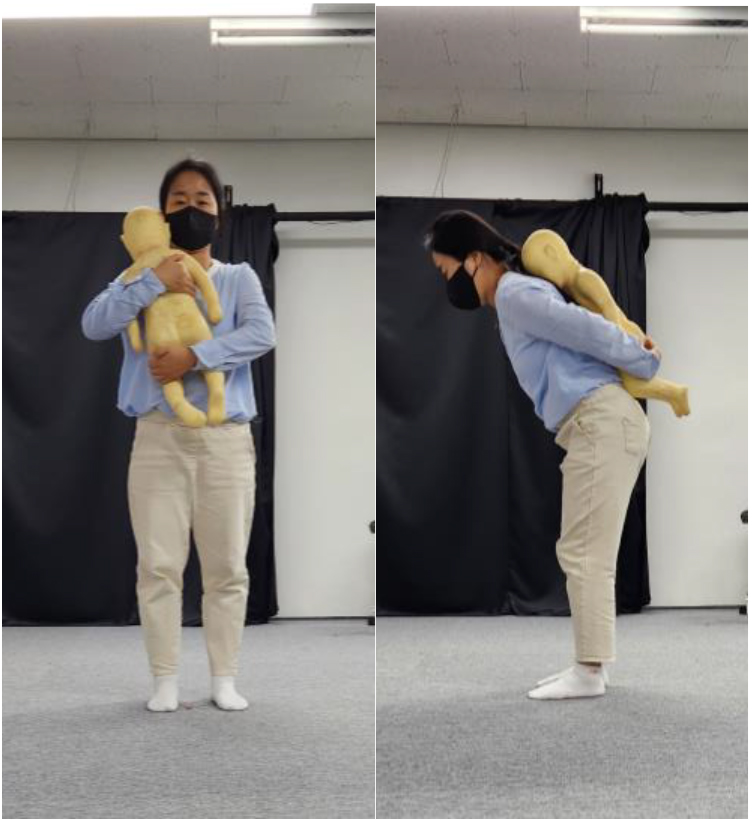
In this study, self-developed infant dummies instead of real infants were used as shown in Fig. 1. Actually, some studies have also used infant dummies for analysis of infant care [9, 10]. Moreover, it has been suggested that carrying infant dummy is not significantly different from carrying a real infant [9]. In this study, two weights (4.6 kg and 9.8 kg) of infant dummies were used according to average weights of 1-month and 12-month infants in Korea [14]. Head circumference was 43.3 cm and height was 67.6 cm as mentioned in our previous study [11].
Figure 1.
Two postures in for measuring postural balance during infant care. Two postures include holding an infant dummy in subject’s arm (left) and carrying an infant on subject’s back.
A force platform (OR-7-2000, 464
The COP was recorded for 60 s. The sampling frequency was 120-Hz. COP data were low-pass filtered with a zero-phase Butterworth filter of fourth-order and a 5 Hz cutoff frequency [16]. The mean value was subtracted from each time series for removal of the offset of anterio-posterior (AP) and medio-lateral (ML) COP data. COP time series were calculated as the COP displacement from averaged COP in the ML and AP. Many quantitative postural sway variables such as mean distance, COP area, mean velocity, and peak power were derived from the COP time series. The mean distance was calculated as average value of COP time series and the mean velocity was calculated as the mean absolute value of time derivative of COP time series. The peak power was defined as the peak value in the power spectrum of COP time series. Finally, COP area was defined as the area surrounding 95% of the points in the COP time series. These quantitative variables have generally been used to assess static postural balance ability in many previous studies [15, 16, 17, 18, 19, 22, 23, 24]. Two-way repeated measure analysis of variance (ANOVA) was performed to determine main effects of infant care postures, infant weight, and their interactions on COP variables. All statistical analyses were performed using SPSS ver. 16 for Windows (SPSS Inc., Chicago, IL, USA). The significant level was defined at
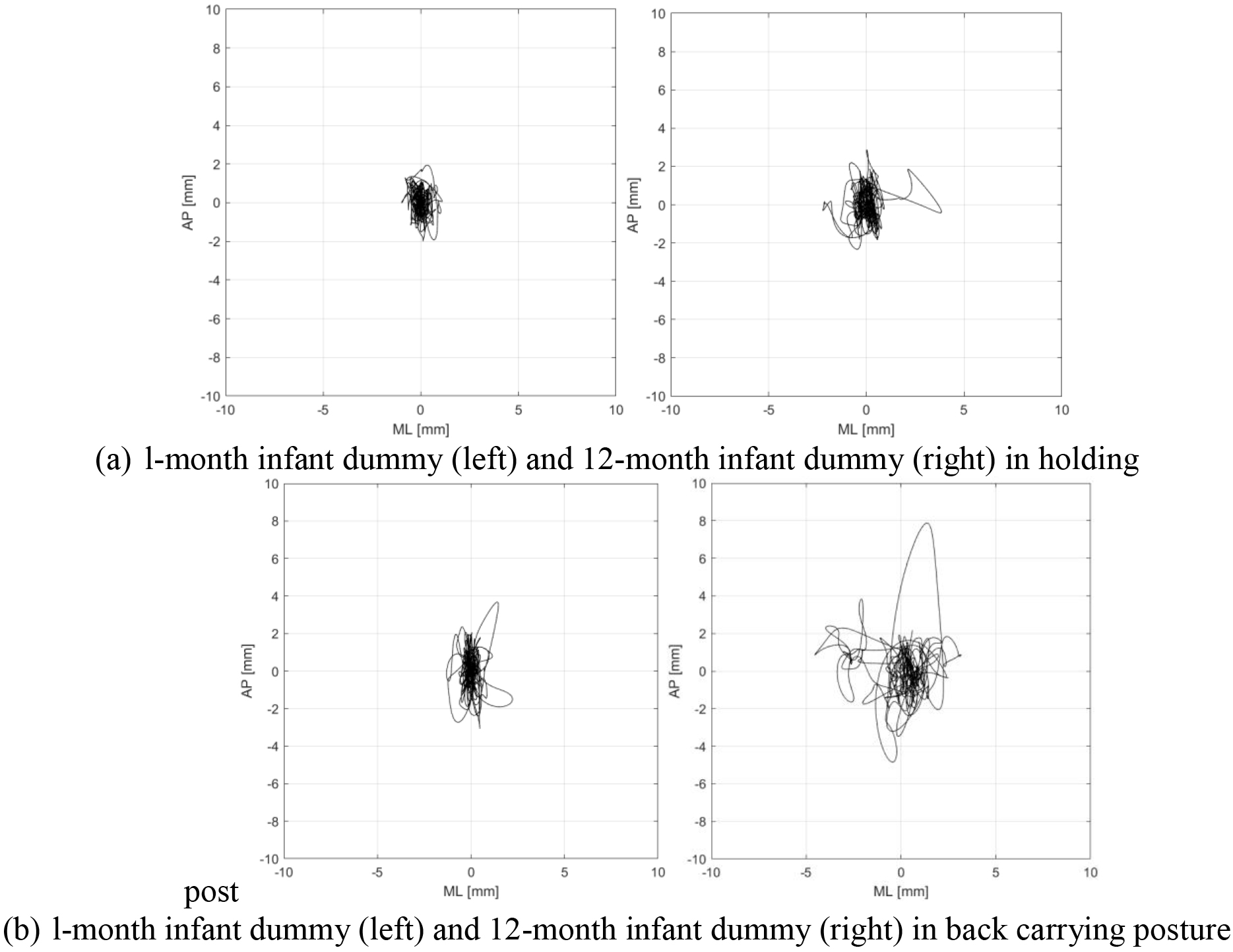
Figure 2.
Representative center of pressure trajectories according to infant weight and infant care postures. AP, anterio posterior; ML, medio lateral.
3.Results
Figure 2 shows trajectories of representative COP according to dummy weight and infant care postures. Back carrying a 12-month infant dummy (9.8 kg) showed the greatest COP trajectory. In contrast, holding a 1-month infant dummy (4.6 kg) presented the smallest COP trajectory.
Table 2
Normalized maximum joint moment according to increased weight in each joint
| Variables | Directions | Dummy weight 4.6 kg | Dummy weight 9.8 kg | |||||
|---|---|---|---|---|---|---|---|---|
| Holding infant | Back carrying | Holding infant | Back carrying | Significance | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Posture | Weight | Interaction | ||
| Mean | Overall | 0.87 (0.22) | 1.19 (0.60) | 1.04 (0.27) | 1.27 (0.54) | * | NS | NS |
| distance | AP | 0.63 (0.16) | 0.80 (0.37) | 0.78 (0.21) | 0.92 (0.39) | * | *** | NS |
| (mm) | ML | 0.47 (0.14) | 0.68 (0.48) | 0.51 (0.17) | 0.67 (0.33) | * | NS | NS |
| Mean | Overall | 6.09 (1.32) | 8.29 (4.41) | 7.17 (1.82) | 9.46 (4.76) | * | ** | NS |
| velocity | AP | 4.80 (1.04) | 6.55 (3.47) | 5.78 (1.51) | 7.66 (3.95) | * | ** | NS |
| (mm/s) | ML | 2.75 (0.69) | 3.64 (2.10) | 3.08 (0.97) | 3.88 (2.08) | * | NS | NS |
| Peak | Overall | 45.94 (39.73) | 65.27 (56.40) | 52.17 (32.49) | 82.04 (68.09) | * | NS | NS |
| power | AP | 103.06 (64.72) | 181.72 (154.30) | 169.84 (102.73) | 248.02 (203.22) | * | ** | NS |
| (mm2/Hz) | ML | 86.69 (56.98) | 167.61 (207.53) | 103.52 (72.28) | 195.72 (190.62) | * | NS | NS |
| COP | 10.21 (5.37) | 21.26 (23.41) | 14.09 (7.04) | 26.38 (23.94) | * | * | NS | |
| area | ||||||||
| (mm2) | ||||||||
COP, center of pressure; SD, standard deviation; AP, anterio posterior; ML, medio lateral; *,
Figure 3.
Comparison of COP variables according to infant care posture and infant dummy weight. COP, center of pressure; AP, anterio posterior; ML, medio lateral; NS, non significance (*,
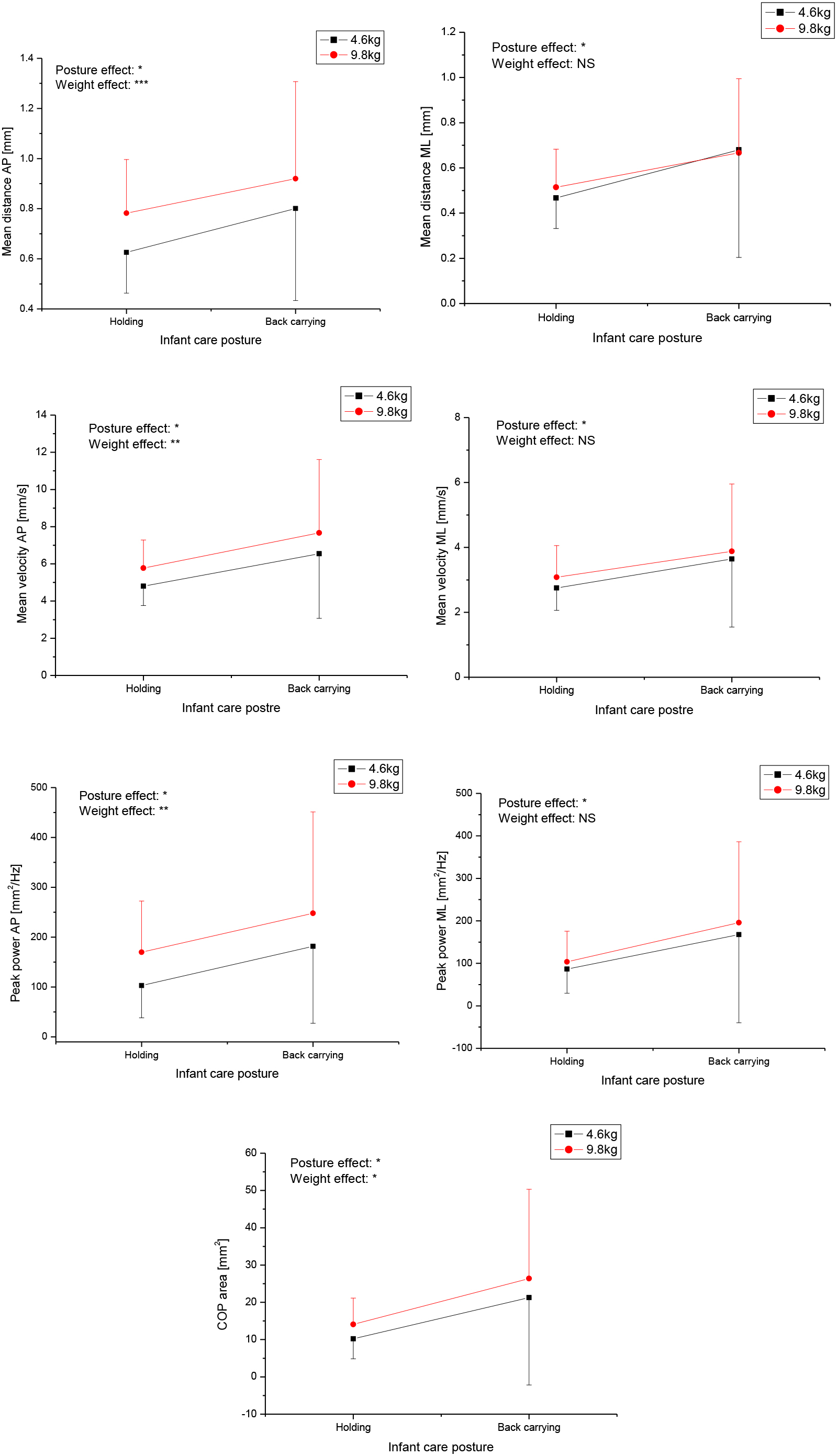
Table 2 and Fig. 3 present results of two-way repeated measure ANOVA to investigate infant care posture effect, infant weight effect, and their interactions. Back carrying a 12-month infant dummy had the greatest amplitude in all COP variables. Main effects of infant care posture were significant in all variables (
There were significant weight effects mainly in AP direction, with significantly greater mean distance, greater peak power, and faster mean velocity when holding or back carrying a 12-month infant dummy than when holding or back carrying a 1-month infant dummy (all
4.Discussion
Little is known about postural balance during infant care motions. This study investigated static standing posture balance during holding an infant dummy in arms and back carrying an infant according to two weights. Main findings of this study were as follows. First, standing posture during back carrying an infant dummy showed the greatest postural sway size and peak power, the fastest sway speed, and the widest sway area. Second, back carrying posture showed greater sway size and peak power, faster sway speed, and wider sway area in both AP and ML directions than holding posture. Third, effect of dummy weight was prominent in AP direction, with greater sway size, greater peak power, and faster sway size when holding or back carrying a 12-month infant than when holding or back carrying a 1-month infant.
In this study, a back carrying posture had significantly greater mean distance, greater peak power, faster mean velocity, and wider COP area than a holding posture. These results indicate that back carrying an infant can induce more unstable postural balance condition, with greater body sway and greater amplitude of main frequency component, faster sway speed, and wider sway area in both AP and ML directions. That is, back carrying posture may induce inefficient level of steadiness. Thus, greater postural balance activity might be required to achieve the level of steadiness. Moreover, back carrying posture’s balance strategy might have a greater intensity of the main COP oscillation component. Effect of infant care posture might be due to difference in trunk posture during static standing between holding and back carrying an infant dummy. Specifically, most participants tended to flex their trunk more during back carrying an infant dummy. This flexed posture might have made it more difficult to maintain postural stability.
Particularly, back carrying an increased weight showed increased values in all COP variables. That is, back carrying a 12-month infant showed the greatest sway size, the greatest amplitude of main frequency, the fastest sway speed, and the widest sway area. This means that holding an infant in one’s arms is helpful for maintaining a more stable postural balance than carrying an infant on the back. Postural imbalance is associated with the risk of fall. Many studies have shown that increased COP variables contribute to deterioration of postural balance. Actually, a previous study has reported that falls while carrying an infant might be due to postural imbalance [20]. Our study suggests that assisting aid such as commercialized back carrier should be used to maintain a stable postural balance when carrying an infant on one’s back.
In most COP variables, effect of dummy weight was prominent in AP direction. This might be due to change of body center of mass (COM) caused by an increase of dummy weight. For example, back carrying an infant dummy may lead to greater sway distance and greater main COP component mainly in AP direction to maintain postural correction against gravity by body COM placed to the posterior direction with an increase of infant dummy weight. Moreover, a faster sway speed by a heavier weight means that more postural control activity in AP direction might be required to achieve the level of steadiness. In a previous joint moment study, heavier infant weight during lifting-up of an infant caused increases of lumbar and hip extension moments [11]. Particularly, the lumbar extension showed the greatest peak joint moment [11]. Our study and the previous study indicate that weight effect exists in postural sway and joint load. These results suggest that an assisting aid or device should be developed in order to prevent unstable postural balance as well as back pain by increased infant weight.
Previous studies have focused on joint moment analysis during lifting-up or carrying of infant [9, 10, 11]. They reported that various infant care activities could induce mechanical load on musculoskeletal systems. Although various biomechanical analyses during infant care motions have been performed, studies investigating postural balance considering various infant care posture or infant weight are insufficient. This study demonstrates that both infant care posture and infant weight can affect postural sway characteristics. However, this study has some limitations. Some studies have suggested that using sling or carrier can improve joint loading and prevent musculoskeletal diseases [9, 10]. Some study investigated gait variables carrying an infant dummy in a baby carrier [21]. We also should investigate if the sling or baby carrier can improve postural balance in a further study. In this study, COP was measured for 60 seconds. However, most babysitters usually stand for long time for holding or back carrying an infant. Long period standing test should be investigated to reflect real infant care situations. Additionally, a small number of young subjects participated in this study, although there might be age and gender differences. Further study should investigate larger populations including elderly subjects. Furthermore, this study only focused on static postural balance. COP based measure during dynamic situation should be investigated to reflect more real infant care conditions.
5.Conclusion
COP variables during holding an infant dummy in-arms and carrying an infant dummy on back were investigated according to the weight of the infant dummy. Posture for carrying an infant dummy on one’s back showed the greatest postural sway size and peak power, the fastest sway speed, and the widest sway area. Additionally, the back carrying posture showed greater sway size, greater peak power, faster sway speed, and wider sway area in both AP and ML directions compared to the holding posture. Effect of infant dummy weight was prominent in AP direction for most COP variables. Our results could contribute to the prevention of musculoskeletal diseases or prevention of fall due to various infant care activities by developing an assisting device to improve postural balance.
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (No. 2019R1C1C1008209 and No. 2022R1I1A3065537).
Conflict of interest
None to report.
References
[1] | Sanders MJ, Morse T. The ergonomics of caring for children: An exploratory study. American Journal of Occupational Therapy. (2005) May-Jun; 59: (3): 285-95. |
[2] | Borg-Stein J, Dugan SA. Musculoskeletal disorders of pregnancy, delivery and postpartum. Phys Med Rehabil Clin N Am. (2007) Aug; 18: (3): 459-76, ix. |
[3] | Owen BD. Intervention for musculoskeletal disorders among child-care workers. Pediatrics. (1994) Dec; 94(6 Pt 2): 1077-9. |
[4] | Brown MZ, Gerberich SG. Disabling injuries to childcare workers in Minnesota, 1985 to 1990. An analysis of potential risk factors. J Occup Med. (1993) Dec; 35: (12): 1236-43. |
[5] | Wu WH, Meijer OG, Uegaki K, Mens JM, van Dieen JH, Wuisman PI, et al. Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. Eur Spine J. (2004) Nov; 13: (7): 575-89. |
[6] | Phillips JA, Forrester B, Brown KC. Low back pain: prevention and management. AAOHN J. (1996) Jan; 44: (1): 40-51; quiz 2-3. |
[7] | Junqueira LD, Amaral LQ, Iutaka AS, Duarte M. Effects of transporting an infant on the posture of women during walking and standing still. Gait Posture. (2015) Mar; 41: (3): 841-6. |
[8] | Anderson AM, Meador KA, McClure LR, Makrozahopoulos D, Brooks DJ, Mirka GA. A biomechanical analysis of anterior load carriage. Ergonomics. (2007) Dec; 50: (12): 2104-17. |
[9] | Schmid S, Stauffer M, Jager J, List R, Lorenzetti S. Sling-based infant carrying affects lumbar and thoracic spine neuromechanics during standing and walking. Gait Posture. (2019) Jan; 67: : 172-80. |
[10] | Williams L, Standifird T, Madsen M. Effects of infant transportation on lower extremity joint moments: Baby carrier versus carrying in-arms. Gait Posture. (2019) May; 70: : 168-74. |
[11] | Kim JW, Eom GM, Kwon YR. Analysis of maximum joint moment during infant lifting-up motion. Technol Health Care. (2022) ; 30: (S1): 441-50. |
[12] | Jeong H, Yamada K, Watanabe S, Kido M, Nomura T, Ohno Y. Analysis of center of pressure location during asymmetric lifting. Proc. IEEE Int. Conf. Syst. Man Cybern. (2015) ; 2471-2474. |
[13] | Antwi-Afari MF, Li H, Edwards DJ, Pa¨rn EA, Seo J, Wong A. Effects of different weights and lifting postures on balance control following repetitive lifting tasks in construction workers. International Journal of Building Pathology and Adaptation. (2017) ; 35: : 247-263. |
[14] | Korean National Growth Charts for children and adolescents. Korea Centers for Disease Control and Prevention. (2017) . |
[15] | Kim JW, Eom GM, Kim CS, Kim DH, Lee JH, Park BK, et al. Sex differences in the postural sway characteristics of young and elderly subjects during quiet natural standing. Geriatr Gerontol Int. (2010) Apr; 10: (2): 191-8. |
[16] | Prieto TE, Myklebust JB, Hoffmann RG, Lovett EG, Myklebust BM. Measures of postural steadiness: differences between healthy young and elderly adults. IEEE Trans Biomed Eng. (1996) Sep; 43: (9): 956-66. |
[17] | Kwon DY, Choi YH, Kwon Y, Eom GM, Kim JW. Comparison of static postural balance in patients with SWEDDS and Parkinson’s disease. J Mech Med Biol. (2020) ; 9: : 2040013. |
[18] | Kim JW, Kwon Y, Jeon HM, Eom GM, Gender-difference in the relationship between postural sway and body factors during quiet standing in the elderly. J Mech Med Biol. (2017) ; 17: : 1740038. |
[19] | Kim JW, Kwon Y, Eom GM, Jun JH, Lee JW, Tack GR, Effects of Vision, Age and Gender on Structural and Global Posturographic Features during Quiet Standing. Int J Precis Eng Manuf. (2012) ; 13: : 969-975. |
[20] | Frisbee SJ, Hennes H. Adult-worn child carriers: a potential risk for injury. Inj Prev. (2000) Mar; 6: (1): 56-8. |
[21] | Havens KL, Goldrod S, Mannen EM. The Combined Influence of Infant Carrying Method and Motherhood on Gait Mechanics. J Appl Biomech. (2023) Nov 20: : 1-7. |
[22] | Kwon DY, Kwon Y, Choi JA, Ko J, Kim JW. Quantitative Analysis of Postural Balance in Faller and Nonfaller Patients with Parkinson’s Disease. Parkinsons Dis. (2023) ; 2023: : 9688025. |
[23] | Kwon Y, Eom GM, Kim JW, Test-retest reliability of postural sway measures during static standing balance performance in healthy elderly adults. J Mech Med Biol. (2022) ; 22: : 2240034. |
[24] | Kwon Y, Kim JW, Reliability of static balance test in faller and nonfaller Parkinson disease patients. J Mech Med Biol. (2023) ; 9: : 2340103. |
[25] | Aburub A, Darabseh MZ, Alsharman A, Hegazy MM, Hunter SM. Nursing Mothers’ Experiences of Musculoskeletal Pain Attributed to Poor Posture During Breastfeeding: A Mixed Methods Study. Breastfeed Med. (2022) Nov; 17: (11): 926-31. |


