
Effect of virtual reality-based mindfulness training model on anxiety, depression, and cancer-related fatigue in ovarian cancer patients during chemotherapy
Abstract
BACKGROUND:
Although the prognosis of ovarian cancer can be significantly improved through standardized surgery and chemotherapy, 70% of epithelial ovarian cancer (EOC) patients would suffer from drug resistance and recurrence during the long chemotherapy cycle.
OBJECTIVE:
To explore the impact of a training mode based on the integration of virtual reality technology and mindfulness on anxiety, depression, and cancer-related fatigue in ovarian cancer patients during chemotherapy.
METHOD:
Through virtual reality technology, a mindfulness training software was designed and developed, and a mindfulness training mode based on virtual reality technology was constructed. Using a self-controlled design, 48 ovarian cancer patients undergoing chemotherapy who were hospitalized in a tertiary hospital in Beijing from August 2022 to May 2023 were conveniently selected as the research subjects. The patients were subjected to four weeks of mindfulness training based on virtual reality technology, and the acceptance of the mindfulness training mode using virtual reality technology was evaluated. The Hospital Anxiety and Depression Scale (HADS) and Cancer Related Fatigue Scale (CRF) were used to evaluate the anxiety, depression, and fatigue of patients before and after intervention.
RESULTS:
The virtual reality based mindfulness training mode includes four functional modules: personalized curriculum, intelligent monitoring, emotion tracking, and Funny Games. 48 patients had a high acceptance score (139.21
CONCLUSION:
Ovarian cancer patients during chemotherapy have a high acceptance of virtual reality based mindfulness training mode. The application of this mode can reduce the psychological problems of anxiety, depression, and cancer-related fatigue in ovarian cancer patients during chemotherapy, and is worth promoting and using.
1.Introduction
Epithelial ovarian cancer (EOC) has the highest mortality rate among all other gynecological malignant tumors [1]. Although the prognosis of ovarian cancer can be significantly improved through standardized surgery and chemotherapy [2], 70% of EOC patients would suffer from drug resistance and recurrence during the long chemotherapy cycle, which severely undermines women’s health [3]. According to the guidelines of the National Comprehensive Cancer Network (NCCN), anxiety and depression are the most common psychological disorders for cancer patients, and cancer-related fatigue (CRF) would exert a great impact on the ability of cancer patients to cope with their disease as the sixth most important vital sign, and may aggravate the progression of EOC and affect disease prognosis [4]. Mindfulness training (MT), a “mindfulness”-based psychotherapy that has been widely applied in the treatment of depression, anxiety, and insomnia [5, 6], encourages trainees to be consciously aware of their thoughts and actions without making any judgments, and focus on reality [7]. With advantages such as immersion, interactivity, and conceptualization, virtual reality (VR) is a safe and effective technology that could help reduce anxiety and depression in patients with breast cancer and lung cancer [8, 9]. In foreign countries, VR-based mindfulness training has achieved positive results in alleviating the anxiety, depression, pain, and menopausal symptoms of patients [10, 11, 12]. However, in China, no study has ever been conducted to investigate the effect of VR-based mindfulness training in EOC treatment. In this light, this study plans to construct a Mindfulness Training Virtual Reality (MTVR) model to improve anxiety, depression, and cancer-related fatigue in EOC patients accepting chemotherapy by taking advantage of the immersive experience of VR as well as traditional mindfulness training.
2.Research subjects and methods
2.1Research subjects
48 EOC patients who were hospitalized in the gynecology department of a tertiary hospital in Beijing for chemotherapy from August 2022 to May 2023 were selected through convenience sampling as the research subjects. With anxiety and depression being the main observation indexes, the sample size was determined according to the sample size calculation formula. However, considering a release rate of 10%, 50 patients should have been recruited. Inclusion criteria: (1) The age of the patient is 18–69 (including 18 years old); (2) The pathological diagnosis is ovarian cancer (stage II–IV) and the patient is aware of the disease; (3) The patient has accepted ovary tumor debulking surgery and the first postoperative chemotherapy, and has been hospitalized for 14d; (4) The patient voluntarily cooperates with researchers in the clinical study. Exclusion criteria: (1) Patients who cannot wear VR kit; (2) Patients with mental illness; (3) Patients with hypertension and heart disease; (4) Patients with serious complications, including systemic co-infections. The study was approved by the hospital medical ethics committee (approval no. 2022-KY-0062-01) and all participating patients signed the informed consent form.
2.2Research methods
2.2.1Development process of MTVR model
A mindfulness intervention team was established. Members of the team include a master’s supervisor in the field of nursing, a psychological counselor, a nurse with a master’s degree in the department of gynecological oncology, a psychologist, and two investigators. The main researchers are masters in gynecologic oncology nursing who have systematically learned about mindfulness together with the team members by attending a 10-week mindfulness course training (once a week; 60 minutes/training). The whole training process was guided by the psychological counselor. The mindfulness intervention program took mindfulness stress reduction therapy (MBSR) and mindfulness cognitive therapy (MBCT) as the basic. After reading relevant books, the psychological counselor and psychologists who have been certified by the Canadian Professional Counselling Association (CCPA) stipulated the intervention methods according to the characteristics of EOC patients and recorded videos and audio for mindfulness training [13, 14]. Based on the consensus reached among the team members, 360∘ 3D natural scenes, video, and audio content are organically integrated with VR to achieve various goals, including scene rendering, video and audio outputting, user interaction, and interface setting. A pilot version of the mindfulness training model was designed and developed by engineers to realize the following 4 main functions: personalized course, intelligent monitoring, emotion tracking, and funny games. Tests and modifications of videos, audio, and music for different scenarios were conducted according to the suggestions of medical staff and patients before sending to medical staff for trial use. Finally, after repeated modifications and debugging, the final version of the mindfulness training software was developed. The software was then installed on the Pico Neo4 (all-in-one; consisting of a helmet and somatosensory grips; manufacturer: ByteDance) to build the MTVR model. Pico Neo4 As a VR all-in-one machine, with the help of mouse, head display, rocker and other equipment to obtain the desired perspective and moving line, the introduction of sports and health applications can be data monitoring, and can clearly present the content to patients. A random number table was used to select 10 patients who met the inclusion criteria for the preliminary experiment.
2.2.2Functional modules of MTVR model
The MTVR model contains four functional modules: personalized course, intelligent monitoring, emotion tracking, and funny games (refer to Figs 1 and 2).
Figure 1.
Functional module of MTVR model.
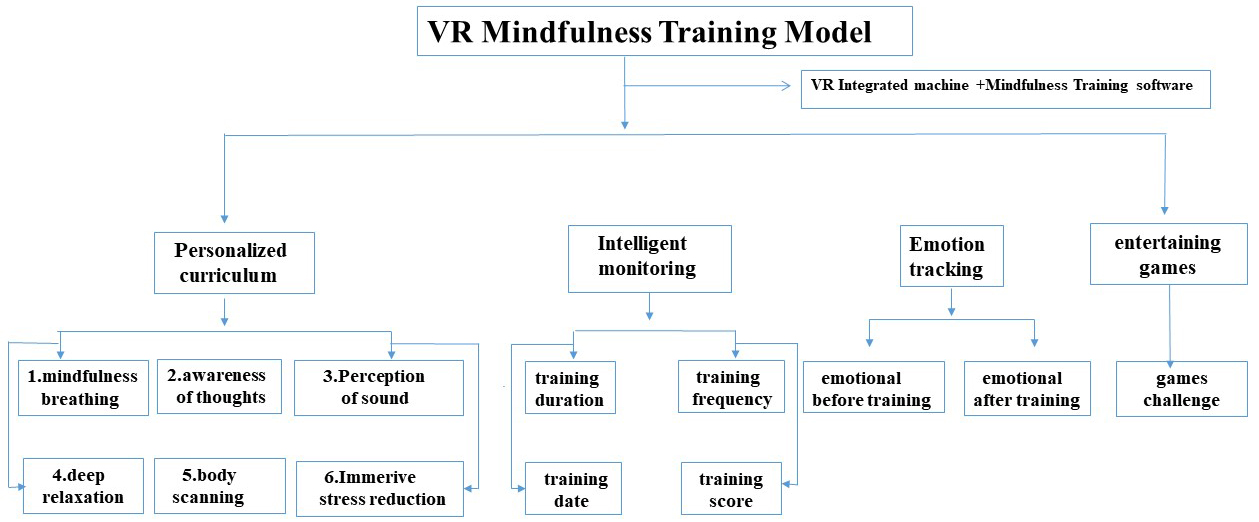
Figure 2.
Screenshots of the VR training.

2.2.2.1 Personalized course
The personalized course module is made up of 7 sub-modules, including mindfulness breathing, awareness of thoughts, perception of sound, body scanning, immersive stress reduction, and deep relaxation. In the first week, the user shall study one module a day, with the content to be studied in the second and fourth weeks being the same as that in the first week. (1) Each sub-module has a text version of the course introduction: course purpose, training duration (15 minutes/time/day); (2) course features: 360∘ 3D panorama; multi-sensory stimulation (including visual and auditory): ⟀ Over 20 kinds of 360∘ multi-directional natural landscape and tourist attractions are provided for the patients, including natural forests, sea, parks and museums; ⟁ Diverse natural sounds are also provided, including the sound of high mountains and running water, the chirping of birds in forests, and the chirping of crickets in the grass. Meanwhile, a one-on-one voice guidance course with soft music was also provided.
2.2.2.2 Intelligent monitoring
The system can automatically monitor the date, duration, times, and records of exercises for the patient, give a score for every mindfulness training, and upload the data.
2.2.2.3 Emotion tracking
Patients are allowed to record their emotional state before and after the mindfulness training from the following six dimensions: physical and mental pleasure, full of energy, inner peace, sometimes sad, restless, and angry. Meanwhile, they record through the device’s software and can choose a score (1–5) corresponding to the mood: 1 means not very good, while 5 means very good.
2.2.2.4 Entertaining games
After mindfulness training, patients were free to play simple stress-relieving games (3
Table 1
Content of the MTVR model (the intervention lasted for 4 weeks. The following table just offers an example of the training content for one week)
| Time | Theme | Content |
|---|---|---|
| Day 1 | Mindfulness Breathing | The patients can see the instructor explaining the theoretical knowledge of mindfulness breathing through the VR kit, and follow the instructions to practice mindfulness breathing in silent mountains and forests. Method: Inhale slowly with the nose and exhale with the mouth; focus the strength of the body on the head, face, neck, chest, abdomen, and other parts by following the breathing rhythm; breathe smoothly and evenly to realize the natural flow of air in the nasal cavity and thereby enter the mindfulness state. |
| Day 2 | Awareness of Thoughts | Follow the instructions to breathe and become aware of thoughts on a calm lake. Method: Think in an inclusive and non-judgmental state; observe the thoughts come and go, and move toward the distance with a train carriage like observing a train. |
| Day 3 | Perception of Sound | Follow the instructions to practice mindfulness breathe in the energy forest to sense the direction of the source of sound (including the sound of high mountains and running water, the chirping birds and crickets) as well as the direction of the source of light. If you get distracted, pull your thoughts back gently. With more training, the patients would not be troubled by wandering thoughts gradually. |
| Day 4 | Deep Relaxation | Follow the instructions to practice mindfulness breathing, become aware of the body, and percept the sound; the patients would be guided to understand and face negative emotions based on mindfulness thinking. It is stressed that mindfulness training is a good way to maintain healthy emotions and patients are encouraged to stick with the practice. |
| Day 5 | Body Scanning | Patients can see the instructor teaching the methods of body scanning in a meditation room. Method: Place the back of your hands on both sides of the body; practice relaxing muscles according to the rhythm of breathing; concentrate your attention on the back, hips, feet, and the bed surface; scan your body from the head to the feet to sense the muscles and check whether the muscles are relaxed or tightened, |
| Day 6 | Immersive Stress Reduction | Follow the instructions to breathe deeply in the forest and then enjoy an immersive journey of press reduction in mountains and forests, oceans, the sky, and the ground; observe the trees on both sides of the river, the ripples on the water, the rocks at the bottom of the clear river, the downstream of waterfalls, etc. When you are flowing down by a boat, pay attention to the sky, clouds, sun, strength, color, etc. |
| Day 7 | Deep Relaxation | Follow the instructions to practice mindfulness breathing; be aware of the body and scan it; the patients would be guided to understand and face negative emotions based on mindfulness thinking. It is stressed that mindfulness training is a good way to maintain healthy emotions and patients are encouraged to stick with the practice. |
2.2.3Implementation of the MTVR model
The intervention based on the MTVR model lasted for 4 weeks. Since the chemotherapy interval of patients is 3 weeks (the treatment process can be divided into the chemotherapy period and chemotherapy interval), the intervention was performed by combining “face-to-face” and “home-based” training.
(1) Chemotherapy period
The intervention, performed one-on-one in a private room under the guidance of a nurse, started 1 week before chemotherapy and lasted for one week (1 time/day, 15 min/time). Before the training, patients were instructed to empty their bladders and wear comfortable clothes, with the room temperature maintained at 25∘C. Specific steps: ⟀ Team members told patients the purpose of VR-based mindfulness training and the operation methods of the all-in-one VR machine, and that any discomforts occur during the training should be reported to the nurse immediately; ⟁ The patients sat or laid down in a comfortable position, put on the VR kit with the help of the nurse, and were told to follow the instructions to watch and experience. As for detailed training content, please refer to Table 1; ⟂ After the training, the patients, instead of standing up immediately, followed the instructions to slowly move both shoulders, upper limbs, and lower limbs, rub both palms to make them warm, gently stroke eyes and face, and then relax both legs; ⟃ In the end, the system automatically uploaded the duration and score of the training, and the patients recorded their emotional state with the handle.
(2) Chemotherapy interval
There are four weeks from the first chemotherapy to before the second chemotherapy. During this period, the training was performed 1 time/day (15 min/time). Before the patients were discharged, a trained nurse set up a WeChat group and instructed the patients to accept training at home. The nurse urged the patients to accept the training and upload the training time screenshots to the WeChat group via the WeChat group and phone calls. If the patients had encountered any problems during the training process, the nurse could have offered guidance to ensure the continuity and quality of home-based training.
2.3Evaluation tools and data collection methods
2.3.1General information questionnaire
The general information questionnaire was designed independently by referring to relevant literature and related materials after being modified repeatedly by experts. General information included e.g. age, marital status, education, family income and VR use experience.
2.3.2MTVR model use and acceptance questionnaire
Under the theoretical guidance of the Technology Acceptance Model (TAM) [15] widely used at home and abroad, the researchers read relevant literature and materials and independently designed an MTVR model use and acceptance questionnaire for EOC patients during chemotherapy. The questionnaire was repeatedly discussed by experts of the research team, covering the following seven dimensions: perceived usefulness, perceived ease of use, perceived ease of learning, perceived applicability, perceived safety, perceived satisfaction, and intention of use. Each dimension involves 5 items. Therefore, there were 35 items in the questionnaire in total, with each item allocated with a score of 1–5, representing strongly disagree, disagree, unsure, agree, and strongly agree, respectively. The scores of each dimension were divided into 3 levels: ⟀ 5–10 points: low acceptance; ⟁ 10–20 points: medium acceptance; ⟂ Over 20 points: high acceptance. The score of the questionnaire ranged from 35 to 175, with the score of each dimension ranging from 5 to 25. The total score can be divided into three classes: (i) 35–70 points: low applicability; (ii) 71–140 points: moderate applicability; and (iii) 141–175 points: high applicability. The higher the score is, the higher the acceptance is. The questionnaire was reviewed by experts of the hospital and modified according to the suggestions received to ensure that it could accurately reflects the user’s evaluation of the applicability of the model. The content validity index of the questionnaire is 0.820, with the Cronbach’s alpha coefficient being 0.915.
2.3.3Hospital anxiety and depression scale (HADS)
HADS was used to evaluate the anxiety level of patients. The scale was established by Zigmond et al. [16] and converted to the Chinese population by Zhenxiao et al. [17]. Concerning 14 items, the scale involves two dimensions: anxiety and depression, with each dimension involving 7 items. The Likert 4-point scale (0 to 3 points) is used for scoring, with the score ranging from 0-21 for each dimension. A total score of 0-7 indicates symptomless, a total score of 8-7 indicates mild anxiety and depression, while a total score of 11-21 indicates obvious anxiety and depression. As for the Chinese version of the HADS scale, Cronbach’s a coefficient is 0.88, the retest reliability is 0.95, and the calibration correlation validity is 0.60, which demonstrates sound reliability and validity.
2.3.4Cancer-related fatigue scale (CRF)
The Chinese version of the CRF scale [17], a scale that is widely used at home and abroad, was used to assess the fatigue of cancer patients from 3 dimensions (physical fatigue, emotional fatigue, and cognitive fatigue) and 15 items, with items 1, 2, 3, 6, 9, 12, 15 under the dimension of physical fatigue, items 5, 8, 11, 14 under the dimension of emotional fatigue, and items 4, 7, 10, 13 under the dimension of cognitive fatigue. Linkert 4-point scale was used to assess the subjective feeling of patients from the previously mentioned three dimensions, with 0–4 indicating “never”, “rarely”, “sometimes”, “most of the time”, and “almost always” respectively. A higher score indicates severer fatigue. The score allocated for the dimension of emotional fatigue and cognitive fatigue is 0–16, and the score allocated for the dimension of physical fatigue is 0–28. The total score is 0–60. The higher the score is, the severer the fatigue is and the worse the living quality is. With relatively robust reliability and validity, CFS is widely used at home and abroad, with an internal consistency coefficient of 0. 88. The scale has been verified among different cancer patients, showing a retest reliability of 0.55–0.77 and an internal consistency of 0.88. Domestic and foreign studies have all justified their reliability and validity.
2.4Data collection method and quality control
Data were collected using a paper questionnaire, while general information, HADS, and CRF were collected on the day of admission. The MTVR model use and acceptance questionnaire was collected 1 w after intervention with the MTVR model, while HADS and CRF were collected 1 w and 4 w after intervention with the MTVR model, respectively. As for patients who could not fill out the questionnaire, the team members read out the items one by one for them and recorded the answer. The inclusion criteria were strictly followed, and all data collectors had accepted unified training concerning how to use and fill out the scales to provide unified guidance and supervision for the patients. The collected data were checked and recorded by two team members.
2.5Statistical methods
Epidata 3.1 software was used to enter the data and SPSS version 26.0 was used for statistical analysis. Normally distributed measurement data were described with (
3.Results
3.1General information comparison of patients in the two groups
50 patients were recruited in this study. Excluding the two patients who dropped out of the study due to changes in their condition, 48 patients aged from 25–60 (43.56
Table 2
Comparison of patients’ general information (
| Item | Case (%) |
|---|---|
| Marital status | |
| Married | 35 (72.91) |
| Divorced/widowed | 13 (27.08) |
| Educational background | |
| Below junior high school | 14 (29.16) |
| Senior high school | 16 (33.33) |
| Junior college and above | 18 (37.51) |
| Monthly income per family member | |
| | 15 (31.25) |
| 3000–5000 yuan | 21 (43.75) |
| Over 5000 yuan | 12 (25.00) |
| VR use experience | |
| Never | 39 (81.25) |
| Use occasionally | 9 (18.75) |
Table 3
Evaluation of patients’ acceptance of the MTVR model (
| Dimension | Score range | Score | High acceptance rate (%) |
|---|---|---|---|
| Perceived usefulness | 5–25 | 24.00 | 89.58 |
| Perceived ease of use | 5–25 | 23.60 | 89.58 |
| Perceived ease of learning | 5–25 | 22.90 | 85.42 |
| Perceived applicability | 5–25 | 23.40 | 89.58 |
| Perceived safety | 5–25 | 23.30 | 91.67 |
| Perceived satisfaction degree | 5–25 | 23.80 | 91.67 |
| Intention of use | 5–25 | 23.90 | 91.67 |
| Total | 35–175 | 164.81 | 89.58 |
3.2Evaluation of patients’ use and acceptance of the MTVR model
During the survey, the failure number of the MTVR model was 0. All subjects believed that the MTVR model was safe, and did not suffer from any uncomfortable symptoms or adverse events (e.g. dizziness, nausea). The total score of patients’ use and acceptance of the MTVR model was (164.81
3.3Comparison of patients’ HADS scores before and after intervention
After intervention 1W, the anxiety and depression scores were 3.85, 3.46; the anxiety and depression scores were 2.92, 3.13, respectively, with significant differences before and after intervention (
Table 4
Comparison of patients’ HADS score before and after intervention
| Item | Before intervention ( | After 1w of intervention ( | After 4w of intervention ( |
|
|
|---|---|---|---|---|---|
| Score | Score | Score | |||
| Anxiety | 5.27 | 3.85 | 2.92 | 45.029 | |
| Depression | 4.96 | 3.46 | 3.13 | 26.553 |
Table 5
Comparison of CRF scores of patients before and after intervention
| Item | Before intervention ( | After 1w of intervention ( | After 4w of intervention ( |
|
|
| Score | Score | Score | |||
| Total CRF score | 31.98 | 26.54 | 23.31 | 70.60 | |
| Physical fatigue | 14.96 | 12.21 | 10.67 | 61.22 | |
| Cognitive fatigue | 8.56 | 7.21 | 6.38 | 24.05 | |
| Emotional fatigue | 8.46 | 7.13 | 6.27 | 28.50 |
Figure 3.
Comparison of CRF scores of patients before and after intervention.
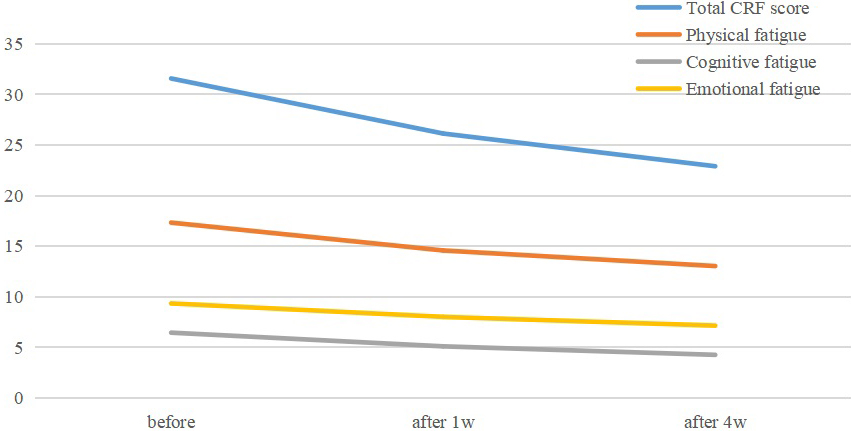
3.4Comparison of patients’ CRF scores before and after intervention
After 1w of intervention, the total CRF scores, physical fatigue, cognitive fatigue and emotional fatigue scores were 26.54, 12.21, 7.21 and 7.13, respectively, and after 4w intervention, the CRF, physical fatigue, cognitive fatigue and emotional fatigue scores were 23.31, 10.67, 6.38 and 6.27, respectively. The difference was statistically significant before and after the intervention (
4.Discussion
In recent years, cancer-based VR [18] and mindfulness training studies [19] in China have been widely applied among breast cancer patients, with EOC patients having a relatively high level of depression and anxiety, that is, 25% and 27%, respectively [20], however, with a high incidence of the psychosocial disorder, this type of patients is facing a limited number of studies on effective intervention measures. Therefore, it is necessary to conduct further study [3]. This study is based on the degree of anxiety relief in EOC patients in the Chinese health system, but the VR combined with mindfulness is equally applicable to other countries. In 2019, Cancer Research UK [21] pointed out that more attention should be paid to the psychological needs of EOC patients. In foreign countries, VR-based mindfulness training has achieved positive results in retarding anxiety and depression, and improving the living quality of EOC and breast cancer patients [3]. After reviewing previous domestic studies, it was found that up to now no study was conducted on the application of VR technology and mindfulness in intervening psychological problems of cancer patients [22, 23]. In this light, based on the immersive and interactive features of VR technology, the present study combined VR with a traditional mindfulness training model to form a VR-based mindfulness training model, with the purpose of maintaining mindfulness ability and improving the anxiety, depression, and fatigue of EOC patients.
4.1High acceptance of the MTVR model among patients
The 48 EOC patients showed a high degree of compliance. The total acceptance score was (164.81
4.2Anxiety and depression of EOC patients alleviated by MTVR model
EOC is the most malignant tumor in gynecology and leads to an increase in the depression and anxiety levels of patients due to pains brought by surgery and chemotherapy, severely damaging the psychological and physical health of patients. According to the results of the study, after 1w and 4w of intervention, the MTVR model could reduce the incidence of anxiety and depression among EOC patients, which justified the effectiveness of the MTVR model on anxiety and depression of ovarian cancer patients during chemotherapy. The main reasons include: ⟀ After being hospitalized for a long time, the activity range of patients is often limited, which makes them eager to “go back home” and visit “beautiful places”. However, affected by symptoms, patients often find it difficult to move their bodies, which means it is difficult to satisfy their desires [22, 26]. The organic combination of VR technology and traditional mindfulness training could exactly meet such demands with its immersive stress reduction module featuring virtual tourism. With VR kits, patients could enter the environment of virtual tourism, and try to relax themselves in tourism videos. In this way, patients’ anxiety and depression could be alleviated, which echoes the research results of test; ⟁ Traditional face-to-face mindfulness training requires intervention at a fixed time and place, which is not match to the needs of patients. Because fixed training sites reduce patient motivation, fixed time also tends to reduce patient enthusiasm and compliance [26, 29]. To solve this problem, the present study adopted the MTVR model, a flexible intervention method, to offer mindfulness training without influencing the daily life of patients. In addition, the MTVR model could reduce the stress patients confront in face-to-face communication with therapists. In virtual environments, therapists could achieve the same training quality as they do in traditional mindfulness training [30].
4.3CRF of EOC patients reduced by MTVR model
CRF is the most common distressing symptom and can seriously affect the living quality of patients. The results of the study showed that after 1w and 4w of intervention by the MTVR model, the CRF and symptoms in all dimensions of EOC patients were relieved. In mindfulness training, patients could notice their breath and body and could distract their attention from thinking to body perception to stay calm and strengthen their control over their body and emotions. Besides, when focusing on the present without making any judgments, patients could also grow more adaptive and endurable to uncomfortable states of their body, and thereby better control their perception of the disease [31]. By integrating VR technology with mindfulness training, MTVR created a relatively isolated mindfulness environment for patients to help them enter the mindfulness atmosphere and state within a shorter period. In addition, the model also provides the function of recording emotions before and after training to offer feedback to patients after each training and thereby strengthen their sense of achievement, which reflects the intelligent and funny side of the model. With the intervention of the MTVR model, the cortical regulation of patients’ brain limbic system could be enhanced to improve the consistency of frontal lobe EEG alpha wave, decrease the excitability of sympathetic nerves and control attention, achieve a more mentally comfortable experience, and reduce the CRF of patients from such aspects as physical condition, emotions, and cognition, which is consistent with the findings of Ma [32]. According to the study by Wu [33], to change patients’ cognition, long-term intervention is required. Cognitions are advanced activities of the cerebral cortex, including perception, recognition, memory, concept formation, thinking, reasoning, and representational processes. In this regard, the duration of intervention can be extended according to cognitive changes to cement the improvement of cognitive fatigue in ovarian cancer patients during chemotherapy.
4.4Application of artificial intelligence in medicine
In recent years, artificial intelligence (AI) has been increasingly used in various fields of medicine. AI is expected to play a key role in helping clinicians diagnose and manage respiratory diseases in the future, and it will be exciting to see the benefits it brings to patients and doctors in daily clinical practice [34]. AI can contribute to the improvement of diagnosis and treatment that can lead to an increase in the success of endodontic treatment outcomes [35]. Industrial intelligence and machine learning can achieve accurate cardiology and improve the prognosis of patients [36]. AI is revolutionizing healthcare, from medical applications to clinical engineering. However, issues of privacy, appropriate use and users, responsibility and bias, and inclusiveness need to be addressed [37].
Being a single-center study with a small number of samples, the present study has its limitations, including a lack of previous related studies, lack of scientific basis in terms of the time setting of index measurement, and failure to probe into the factors that would influence the use effect. There are still limitations in the control variables of the study participants, including the effects of different physiological stages of female age. Meanwhile, whether participants chose games and the time was not recorded may have an impact on the results of the study.
It is expected that randomized controlled studies with larger sample sizes and more research evidence be conducted in the future, and the intervention duration be extended to further verify the effect of the MTVR model as a way of psychological intervention on EOC patients during chemotherapy.
5.Conclusion
In this study, a psychological intervention model was developed for EOC patients during chemotherapy by integrating VR technology and mindfulness training. The purpose was to reduce the anxiety, depressional, and CRF state of EOC patients during chemotherapy. The results showed that EOC patients during chemotherapy had higher acceptance of the MTVR model, with their anxiety, depression and CRF state effectively improved. Moreover, given the decreasing price of VT kits and easy installation of the model, the application of the MTVR model could be extended from clinical psychological intervention to community-based or home-based psychological intervention under a reduced cost without the participation of professional medical staff.
Author contributions
All authors contributed to data analysis, drafting or revising the article, provided final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
The study was supported by the Nursing Project Foundation of Peking University International Hospital (No. YN-2022HL03).
Data availability statement
All data generated or analyzed during this study are included in this published article.
Conflict of interest
The authors declare that they have no competing interests.
References
[1] | Zhu J, Wu X. Leading research progress and the prospect of gynecological oncology in 2020. China Oncology. (2021) ; 31: (04): 250-256. |
[2] | Sarkar S, Malekshah OM, Nomani A, et al. A novel chemotherapeutic protocol for peritoneal metastasis and inhibition of relapse in drug resistant ovarian cancer. Cancer Med. (2018) ; 7: (8): 3630-3641. |
[3] | Arden-Close E, Mitchell F, Davies G, et al. Mindfulness-based interventions in recurrent ovarian cancer: A mixed-methods feasibility study. Integr Cancer Ther. (2020) ; 19: : 1534735420908341. |
[4] | Armstrong DK, Alvarez RD, Bakkum-Gamez JN, et al. Ovarian Cancer, Version 2. 2020, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. (2021) ; 19: (2): 191-226. |
[5] | Hu XS, Beard K, Sherbel MC, et al. Brain mechanisms of virtual reality breathing versus traditional mindful breathing in pain modulation: Observational functional near-infrared spectroscopy study. J Med Internet Res. (2021) ; 23: (10): e27298. |
[6] | Zhu TR, Zhou YX. The effect of mindfulness-based intervention on anxiety, depression and quality of life in patients with inflammatory bowel disease: A meta-analysis. Nursing Journal of Chinese People’s Liberation Army. (2022) ; 39: (04): 61-64, 80. |
[7] | Zhang GR, Yang L, Duan DK, et al. Effects of mindfulness relaxation training on perioperative psychological stress response and sleep quality in elderly patients with coronary heart disease undergoing PCI. Chinese Journal of Nursing. (2018) ; 53: (12): 1463-1467. |
[8] | Bani Mohammad E, Ahmad M. Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: A randomized control trial. Palliat Support Care. (2019) ; 17: (1): 29-34. |
[9] | Zeng Y, Zhang JE, Cheng A, et al. Meta-analysis of the efficacy of virtual reality-based interventions in cancer-related symptom management. Integr Cancer Ther. (2019) ; 18: : 1534735419871108. |
[10] | Horesh D, Kohavi S, Shilony-Nalaboff L, et al. Virtual Reality Combined with Artificial Intelligence (VR-AI) Reduces Hot Flashes and Improves Psychological Well-Being in Women with Breast and Ovarian Cancer: A Pilot Study. Healthcare (Basel). (2022) ; 10: (11): 2261. |
[11] | Haisley KR, Straw OJ, Müller DT, et al. Feasibility of implementing a virtual reality program as an adjuvant tool for peri-operative pain control; Results of a randomized controlled trial in minimally invasive foregut surgery. Complement Ther Med. (2020) ; 49: : 102356. |
[12] | O’Connor S, Mayne A, Hood B. Virtual reality-based mindfulness for chronic pain management: A scoping review. Pain Manag Nurs. (2022) ; 23: (3): 359-369. |
[13] | Chen C, Shi J, Stanley RM, et al. U.S. Trends of ED Visits for Pediatric Traumatic Brain Injuries: Implications for Clinical Trials. Int J Environ Res Public Health. (2017) ; 14: (4): 414. |
[14] | Bob Starr, Elisha Goldstein. Life of Mindfulness, a Way to Reduce Stress: Mindfulness Stress Reduction Workbook. 2013. Life of Mindfulness, a Way to Reduce Stress: Mindfulness Stress Reduction Workbook. |
[15] | Davis FD. Perceived usefulness, perceived ease of use, and user acceptance of information technology. Mis Quarterly. (1989) ; 13: (3): 319-340. |
[16] | Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) ; 67: (6): 361-370. |
[17] | Sun ZX, Liu HX, Jiao LY, et al. Reliability and validity of hospital anxiety and depression scale. Chinese Journal of Clinicians (Electronic Edition). (2017) ; 11: (02): 198-201. |
[18] | Chen XM, Jin AX, Zhu H, et al. Application and effect of virtual cognitive rehabilitation training in breast cancer patients with cognitive impairment after chemotherapy. Chinese Journal of Nursing. (2019) ; 54: (05): 664-668. |
[19] | Zhang L, Du J, Zou ZY, et al. Meta-analysis of effects of mindfulness-based interventions on anxiety and depression symptoms of patients with breast cancer. Chinese Nursing Research. (2020) ; 34: (14): 2437-2444. |
[20] | Halada P, Doničová V, Práznovec I, et al. Depression, anxiety in ovarian cancer patient. Ceska Gynekol. (2019) ; 84: (4): 309-317. |
[21] | Thomas DS, Gentry-Maharaj A, Ryan A, et al. Colorectal cancer ascertainment through cancer registries, hospital episode statistics, and self-reporting compared to confirmation by clinician: A cohort study nested within the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS). Cancer Epidemiol. (2019) ; 58: : 167-174. |
[22] | Wu Y, Zhang HC, Wang NN, et al. Nursing journal of chinese people’s liberation army. Nursing Journal of Chinese People’s Liberation Army. (2022) ; 39: (05): 61-64. |
[23] | Cui MM, Xu XM, Luo XY, et al. Application progress of virtual reality technology in cancer-related pain care. Journal of Shenyang Medical College. (2023) ; 25: (01): 83-87. |
[24] | Veličković P, Milovanović M. Improvement of the interaction model aimed to reduce the negative effects of cybersickness in VR rehab applications. Sensors (Basel). (2021) ; 21: (2): 321. |
[25] | Cikajlo I, Cizman Staba U, Vrhovac S, et al. A cloud-based virtual reality app for a novel telemindfulness service: Rationale, design and feasibility evaluation. JMIR Res Protoc. (2017) ; 6: (6): e108. |
[26] | Navarro-Haro MV, López-Del-Hoyo Y, Campos D, et al. Meditation experts try Virtual Reality Mindfulness: A pilot study evaluation of the feasibility and acceptability of Virtual Reality to facilitate mindfulness practice in people attending a Mindfulness conference. PLoS One. (2017) ; 12: (11): e0187777. |
[27] | Fu WS, Song YC, Wu BA, et al. Virtual reality combined with robot-assisted gait training to improve walking ability of children with cerebral palsy: A randomized controlled trial. Technol Health Care. (2022) ; 30: (6): 1525-1533. |
[28] | Lee S, Cha H. The effect of clinical application of transcranial direct current stimulation combined with non-immersive virtual reality rehabilitation in stroke patients. Technol Health Care. (2022) ; 30: (1): 117-127. |
[29] | Bai TJ, Qin L, Dong JX, et al. Effects of mindfulness training based on WeChat live broadcast on subthreshold depressive symptoms after PCI. Chinese Journal of Nursing. (2022) ; 57: (11): 1304-1309. |
[30] | Seabrook E, Kelly R, Foley F, et al. Understanding how virtual reality can support mindfulness practice: Mixed methods study. J Med Internet Res. (2020) ; 22: (3): e16106. |
[31] | Chen YX, Li F. Analysis on the effect of mindfulness-based stress reduction training combined with empathy intervention in patients with gastric cancer. China Journal of Health Psychology. (2020) ; 28: (06): 836-840. |
[32] | Ma J, Zhao D, Xu N, et al. The effectiveness of immersive virtual reality (VR) based mindfulness training on improvement mental-health in adults: A narrative systematic review. Explore (NY). (2023) ; 19: (3): 310-318. |
[33] | Wu XL, Fang YQ, Cai YM. Effect of mindfulness meditation on cancer-related fatigue and psychological state of patients with hematological tumor undergoing chemotherapy. China Modern Medicine. (2021) ; 29: (09): 1310-1314. |
[34] | Kaplan A, Cao H, FitzGerald JM, et al. Artificial intelligence/machine learning in respiratory medicine and potential role in asthma and COPD diagnosis. J Allergy Clin Immunol Pract. (2021) ; 9: (6): 2255-2261. |
[35] | Aminoshariae A, Kulild J, Nagendrababu V. Artificial intelligence in endodontics: Current applications and future directions. J Endod. (2021) ; 47: (9): 1352-1357. |
[36] | Johnson KW, Torres Soto J, Glicksberg BS, et al. Artificial intelligence in cardiology. J Am Coll Cardiol. (2018) ; 71: (23): 2668-2679. |
[37] | Badnjevi A, Avdihodži H, Gurbeta Pokvi L. Artificial intelligence in medical devices: Past, present and future. Psychiatr Danub. (2021) ; 33: (Suppl 3): S336-S341. |


