
The development and impact of an app for a smart drug interaction reminder system
Abstract
BACKGROUND:
Improved access to media and medical knowledge has elicited stronger public health awareness.
OBJECTIVE:
This study developed a smart drug interaction reminder system for patients to increase knowledge and reduce nurse workload.
METHODS:
This study used a single-group pre-test/post-test design and applied mining techniques to analyze the weight and probability of interaction among various medicines. Data were collected from 258 participants at a teaching hospital in northern Taiwan using convenience sampling. An app was used to give patients real-time feedback to obtain access to information and remind them of their health issues. In addition to guiding the patients on medications, this app measured the nurses’ work satisfaction and patients’ knowledge of drug interaction.
RESULTS:
The results indicate that using information technology products to assist the app’s real-time feedback system promoted nurses’ work satisfaction, improved their health education skills, and helped patients to better understand drug interactions.
CONCLUSION:
Using information technology to provide patients with real-time inquiring functions has a significant effect on nurses’ load reduction. Thus, smart drug interaction reminder system apps can be considered suitable nursing health education tools and the SDINRS app can be integrated into quantitative structure-activity relationship intelligence in the future.
1.Introduction
The World Health Organization (WHO) has advocated for patient safety improvement and medical error reduction in recent years [1]. With developing information technologies, the public has moved beyond simply seeking medical advice from physicians; they are now becoming increasingly aware of health-related matters. Through access to accurate medical and health information, the public now seeks to better understand the treatments provided for various diseases so that they can adopt the most appropriate forms of medical and healthcare for themselves and their family members. Access to accurate medical and health information is another aspect of healthcare-related needs that have arisen. While the last few years have seen increased integration of information technology into home healthcare, a dearth of information regarding healthcare-related issues associated with medications, including drug interactions, pharmacopeias with drug images, dietary considerations, and medication management remains [2, 3]. The present study primarily involved developing an app-based instant feedback system that provides prompt guidance regarding the relevant issues to consider to avoid improper medication use. This study posits that developing a drug warning system could improve nursing guidance tools to enhance a patient’s knowledge of drug use.
1.1Background
Improved access to media and medical knowledge has elicited a stronger awareness of health among the public. An increase in disease affluence and chronic diseases has also contributed to the frequency with which medical care is utilized. These trends have brought the objective of achieving patient safety improvement and medical error reduction to the forefront of medical care. This situation is relevant not just for the WHO and in Western countries but also in Taiwan, making these factors essential drivers of medical system reforms across various nations [1, 4]. In some countries, pharmacists are legally required to perform a check when a public member is taking five or more types of medications to address the dangers of medication use. In contrast, Taiwan has no similar mechanism for monitoring medication use. According to a study conducted as part of an ambulatory medicine quality improvement project in the U.S., 18% of outpatients complained about receiving the wrong medications [5].
A survey of the general public’s knowledge regarding medication use found that more than 50% of surveyed patients were taking medication for long-term disease control. Most people within this group (55%) failed to take their medication following their physicians’ instructions, with the most common reason cited (25%) being “the perception that one’s medical condition has stabilized” [6, 7, 8]. These survey results indicate that medication use knowledge among patients is lacking. As such, medication-use safety can only be achieved through collaboration between medical teams and the public. Recently, raising public participation in patient safety has become an annual patient safety objective under Taiwan’s Ministry of Health and Welfare (MOHW). Therefore, understanding public awareness of medication-use experience and safety can contribute to formulating strategies to improve public participation and exploring relevant behavior [1, 9].
Due to recent technological advancements, smart 3C (computer, communication, and consumer electronics) products have become ubiquitous virtually worldwide. Thus, developing home health medication safety should move toward utilizing information technology assistance to improve the public’s medication use and home-care quality. It should also seek to enhance the public’s implementation of self-care and dietary considerations, and prevent drug interactions, thus boosting the public’s autonomy and self-worth. This would provide the public with convenient, immediate access to assistive medical guidance [10]. Medication-use safety improvement has become a primary objective and component of the medical evaluation indices used in Taiwan and other regions with significant Chinese populations. In 2012, Taiwan added another objective: improving the ability of patients and primary caregivers to safely engage in medication use. The results from a survey highlight that accuracy in medication use among older adults was 73.6%, indicating the importance of medication-use safety for this age group [3]. The public now typically seeks answers to medical questions by accessing medical information online. However, medical information found online is often written by individuals without a professional medical background. Many articles are written based on personal experiences; some even propagate erroneous medical knowledge, which results in the public learning incorrect medication-use concepts [11].
Taiwan’s MOHW was surveyed in 2012 to examine the public’s awareness and education of the terms used in correct medication use education. The survey results indicate that the public lacks an understanding of terms typically used in health education by pharmacists, including the Chinese terms for “prescription,” “package insert,” and “symptom relief.” This problem was found to be more pronounced among elementary school students. Hence, there is an urgent need for the government to establish an online platform that provides professional, accurate medical knowledge to improve the public’s medication-use knowledge and ensure people’s health concerning medication use [3]. The increasing popularity of smartphones has revolutionized most information industries and led to the creation of various daily living applications. However, it has also increased the spread of medical information. Some people have even started to experience symptoms of phone addiction and are more likely to leave their homes without their wallets or ID cards than without their phones [12]. Research also suggests that a rising number of older adults are increasingly using their phones while waiting to see their physicians. This highlights the potential for app users to be extended to people aged 60 to 70 and older [13].
To improve medication-use safety and health knowledge, the Joint Commission of Taiwan (JCT) expanded its execution strategy for improving medication-use safety in 2010. The Joint Commission of Taiwan (JCT) is an accreditation body in healthcare established in 1999. JCT was founded by the Department of Health at the time (renamed the Ministry of Health and Welfare in 2013), the Taiwan Hospital Association, the Taiwan Non-Government Hospitals and Clinics Association, and the Taiwan Medical Association. This Strategy for improving medication-use safety has involved the strengthening of medication-use safety for chronic patients. It focuses on recording and utilizing medical history about drug allergies and adverse drug reactions, patient medication guidance to improve the ability of patients and caregivers to safely engage in medication use, and the use of information technology to increase medication-use safety [3, 14, 15]. Medication safety objectives have remained primarily unchanged over the years. Development trends emphasize the public’s understanding of and participation in patient safety and the transition from passivity to active participation to ensure medication-use safety. These initiatives involve good physician-patient communication, active medication checks, an understanding of personal medication, proper medication administration (i.e., a patient does not independently change dosage levels or stop using a medication), drug response observations, adequate medication storage and management, refusal to take other patients’ medications, medication from unverified sources, expired medication. Improving medication safety focuses on enhancing personal medication knowledge and applying communication technology. A survey investigating the knowledge and experiences of outpatients concerning medication-use safety found that there is much room for improving the public’s general awareness and behavior about correct medication use [2], particularly regarding medication-taking behavior and storage. Adverse drug events may occur if an individual lacks adequate knowledge about medication storage, usage habits, and medication awareness or fails to monitor the changes in their reactions to medication use. Communication technology, which is becoming increasingly universal, can be incorporated into healthcare products to assist medical teams to monitor medication-use safety from a hospital setting to an individual’s daily life activities. This will become a significant future development trend [3, 16].
A medical center in Taiwan tracked outpatients and found that the incidence of potential drug interactions was 25.6%, where 53,624 cases of potential drug interactions occurred during the period in question [13]. Another medical center in southern Taiwan examined 8,160 prescriptions with potential Grade I drug interactions selected via MOHW’s Drug Interaction Database Management System. The significance rating of clinical drug interaction results confirmed by literature reports can be divided into (1) Grade 1 major or high risk: The interaction results in this grade can be a serious threat to life or may cause permanent injury, in which the crisis is always higher than the beneficial effect. Medications must be immediately discontinued to avoid simultaneous use or hospitalization treatment. A preliminary analysis of these 8,160 prescriptions revealed that most were long-term prescriptions. Further, some patients, owing to their medical conditions, were required to take these medications with potential interactions over the long term under close supervision of their physicians. The study proposed that physicians could closely monitor their patients’ conditions after medication use by conducting patient interviews and physical examinations or cross-referencing the relevant test data. Subsequently, they could carefully adjust dosage and frequency, stagger medication administration, and improve patient education to prevent adverse reactions [2].
Research conducted by several teaching hospitals in Taiwan shows that the highest rates of potential interactions and warnings were reported by cardiology departments. The most common warnings were issued for the combined use of aspirin and Plavix (510 times, or 22.5% of Grade I interaction warnings). Other combinations, such as digoxin and lasix, are classified as Grade I interactions based on the MOHW’s Drug Interaction Database Management System. However, the interaction grading may differ across various databases. For example, regarding the combined use of aspirin and clopidogrel, the National Health Insurance’s Guidelines and the U.S. ACC/AHA Guidelines clearly state that patients with non-ST-segment-elevation acute coronary syndrome (unstable angina and non-Q wave myocardial infarction) can take clopidogrel and aspirin together (for up to 9–12 months) to reduce cardiovascular disease complications.
Therefore, it is necessary to re-examine the classifications of interaction severity. The quality of warning content should also be emphasized over quantity; otherwise, it will be impossible to genuinely prevent the occurrence of adverse interactions arising from the combined use of medications. These findings motivated us to re-examine drug interaction warnings to ensure medication-use safety [17, 18]. Information technology helps eliminate written errors and can enable the issuance of reminders concerning the correct time to take medication, recommendations for routes of administration, recommendations for dosage adjustments in response to liver and kidney function levels, and reminders regarding food-drug interactions [19, 20, 21, 22]. Patients’ awareness of medication use is crucial. Knowledge of medication-use safety is not the exclusive domain of medical personnel. Medical knowledge is something that all people taking medication must understand. This knowledge can reduce the occurrence of medical negligence, strengthen medication-use safety for chronic patients, prevent duplicate medications, and allow for a medical care model that centers on patient safety [1, 21].
2.Materials and methods
2.1Design
This study used an observational single-group pre-test and post-test design. The study sample was selected using convenient sampling, with a sample size of 258 subjects. A smart drug interaction reminder system was established and developed to explore and observe the changes in knowledge improvement after using SDINRS in individual cases. This study was conducted at a teaching hospital in northern Taiwan over six months. It explored the effectiveness of SDINRS on patient self-care. We established a consultation station in the outpatient department to provide individual consultations with SINDRS regarding any side effects experienced during home care. We collected data with paper and cloud questionnaires before and after three months. We recommended that clients use APP at least twice a week. This study’s inclusion criterion was patients over the age of 20 and under the age of 80 who were receiving chronic medications. The exclusion criterion was patients who were unconscious and do not habitually use smartphones or tablets.
The single-group observational study was used to avoid the interaction of individual cases. This study method was employed because people tend to share personal resources during the waiting period for outpatient service in Taiwan’s waiting area.
Background information regarding the study population was collected in addition to demographic variables, including the participants’ health status, medication use, care-related habits, experience using smart 3C products, and experience with using the Internet to access information on home medication use and home care. After the experiment, we conducted a survey to further examine the participants’ experiences. The procedures involving experiments with human subjects were conducted in accordance with the ethical standards of the Committee on Human Experimentation of the institution in which the experiments were performed; this study was also conducted in accordance with the Declaration of Helsinki of 1964 and its later amendments or comparable ethical standards. The research plan was approved by the research ethics committee of the medical department of the researchers’ institution (IRB number: (866)110-12). Before participating in the study, participants were provided with a detailed explanation of the research content, after which their written informed consent was obtained.
2.2Participants
Participants were selected through convenience sampling. A knowledge test and usability survey were performed to understand the ease of using SDINRS and its effectiveness in enhancing the knowledge of chronic patients. The 258 participants had an approximately equal gender distribution and comprised patients with chronic diseases (such as metabolic syndrome). Participants were recruited from a teaching hospital in northern Taiwan. Before the experiment, researchers verified the basic health status (such as visual acuity) of each potential study participant and whether they were long-term users of cardiac medications. Those who met the criteria were allowed to participate. The study was conducted using a quasi-experimental approach, where all participants were assigned manipulated variables and underwent each experiment. Arrangements were made to enable each participant to effectively report on the experiment’s results two weeks after it commenced. General hospitals dominate Taiwan’s medical environment. Since people often have high-risk groups of multiple chronic diseases (such as metabolic syndrome), the APP developed in this study focused on medication required for common chronic diseases. Therefore, no specific chronic disease was targeted for recruitment and convenience sampling was used in the outpatient area for announcing test results to allow the public to actively participate in this study’s clinical test.
2.3Data collection
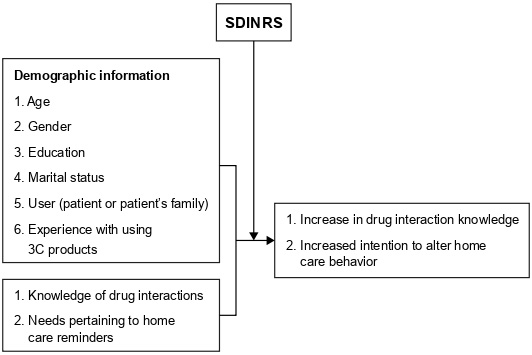
The present study was conducted from September 2016 to September 2017. After obtaining sufficient information about the study in the outpatient department and indicating their intention to participate, participants completed the informed consent form, the demographic questionnaire, and the related questionnaire regarding the smart drug interaction reminder system. After completing the pre-test questionnaire, participants used the smart drug interaction reminder system as an intervention measure. A post-test questionnaire survey was conducted, including knowledge about drug use and the participants’ satisfaction with the application after six months of using the mobile application. The research framework is shown in Fig. 1.
Figure 1.
Research framework.
2.3.1Patient and public involvement
This study designated gender, age, whether one habitually uses the Internet to access information on medication use and care, and whether medication care was implemented regularly as the independent variables. First, we performed an evaluation to identify differences between male and female participants, between participants above and below the average age, and in age-related preferences regarding the habitual use of the Internet to access information on medication use and care. Second, we examined the effects of various reminders that provided information on medication care. In addition to gender, age, and whether one habitually used the Internet to access information on medication use and care, the effects linked to the regular implementation of medication care were also explored.
SDINRS was designated as a manipulated variable to examine the effectiveness of its use. The effect of SDINRS use on the public refers to the transition of the participants from understanding knowledge to the execution of healthcare behaviors, as well as from understanding healthcare content to the execution of an action. Regarding the number of times SDINRS was used, a higher number indicates that the system produces a stronger effect and consequently improves the ability of members of the public to perform self-care. The study explored the impact of SDINRS use on each participant by examining the number of times each participant used SDINRS and the increase in self-care knowledge that each participant achieved.
2.3.2SDINRS development process
First, 2,368 nursing matters concerning drug interactions and after-drug use were extracted from the Hospital Health Information System (HIS) based on the Cross-Industry Standard Process for Data Mining (CRISP) program. According to the relevant literature, factors affecting the choice of nursing and the situation that should be paid attention to after drug use were discussed. After comparing the clinical and literature data, the main discriminant factors were selected from the nursing record data set; the smart drug interaction reminder system was established using the smart decision-making tree algorithm. The two tests’ most commonly used nursing methods were suggested to be displayed on the screen.
Second, we used data concerning medication use and common side effects for chronic diseases (such as cardiovascular disease and diabetes) to develop the first and bottom layers of the knowledge framework. Information on hypertension accounted for the largest proportion (25.6%) of the data, followed by diabetes (9.4%) and heart disease (9.1%). The second layer comprised common side effects. The third and upper layers comprised potential drug interactions. The association rule was used to generate minimum support and confidence. In the algorithm section, the quantitative structure-activity relationship (QSAR) design concept was referenced to obtain feedback from the real-time care gathered from the patient’s responses [23].
Regarding other nursing guidance-oriented systems, the academic terms used in the precautionary content were replaced by more vernacular terms (such as “irregular heartbeat” in place of “hypokalemia”). We conducted a correlation comparison of the two knowledge bases. The app was developed to be compatible with the two major device platforms currently used in the market: Android and iOS operating systems. The Android app was developed using Android Studio. A personal homepage program was used to send and receive data via a MySQLdb connection (MySQLdb is a multi-participant, multi-threaded SQL database server that enables effective editing, filing, and tabulation for database software so that queries and collation can be performed more effectively). The iOS app was developed using the programming languages Objective-C and Swift. Its app interface was designed using basic Xcode and UIKit components.
2.3.3Research tools
This study’s research tools included SDINRS and a knowledge-oriented questionnaire with knowledge-related items. The questionnaire was developed based on the mobile application rating scale proposed by Stoyanov, comprising eight 5-point Likert scale items [8]. Three experts (an expert on nursing information systems, an engineering professor, and a pharmacist) were invited to verify the appropriateness and clarity of the questionnaire content, which was determined to have a total CVI of 0.86. The internal consistency of the scale’s Cronbach’s
The questionnaire contained pre- and post-test components administered before and after the intervention. The pre-test questionnaire included the participants’ basic information, health status, habits related to medication use and care, and participant experience with smart 3C products. The post-test questionnaire included the participants’ perceptions of SDINRS regarding the system’s convenience, its role in enhancing their healthcare knowledge, and their satisfaction with the system. The post-test questionnaire was administered to the participants two weeks after using SDINRS. Participants were instructed to complete the questionnaire and provide feedback on how they accessed the information.
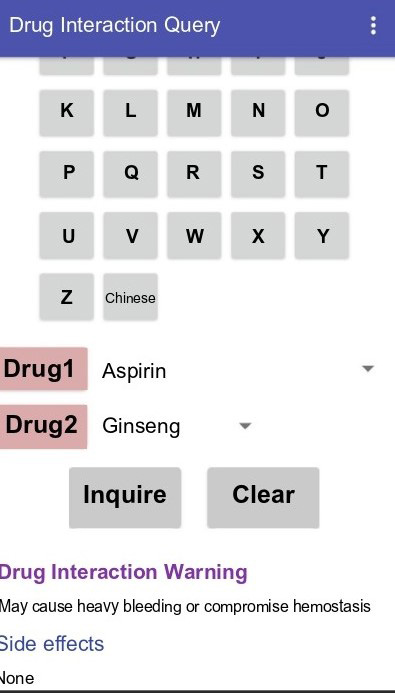
SDINRS was primarily designed to provide the public with a convenient, immediately accessible source of healthcare knowledge. It was also designed to assist in their understanding of healthcare reminders related to medication use, drug interactions, daily essentials, and dietary considerations to promote medication-use safety. This system allows the public to understand their medication use, enhance healthcare knowledge and identification methods regarding self-medication, and improve their medication adherence and participation. Moreover, families can also use the system to understand the medication precautions that apply to family members who are ill. As such, people can increase their knowledge regarding essentials and family guidance and reduce the pressure they feel due to a lack of care-related knowledge. The research schematic diagram of the app is shown in Fig. 2.
Figure 2.
Schematic diagram of the system.
2.3.4Clinical measurements
The study experiment began with the participants (recruited from a teaching hospital in northern Taiwan) undergoing a pre-test questionnaire interview. After completing the interview, participants were introduced to the SDINRS functions and operations. This system boasts two functions. The first function enables participants to independently access medication and health information. Regarding the second function, a patient who has seen a physician and collected their medication pack can enter the relevant medication names and pack numbers or QR codes into the system.
Next, a patient can set the medication time so that an alarm reminder will sound, and the system will display previous query results when it is time for the patient to take their medication. The patient is reminded about their medication time and the relevant self-care and safety precautions before and after medication use. Two weeks after the 258 participants began using the system, we conducted a post-test questionnaire-based satisfaction survey, and related knowledge tests. The clinical tests were conducted at a medical center and a regional teaching hospital in northern Taiwan between September 2016 and September 2017. A single-group intervention was performed, with pre- and post-test surveys conducted before and after participants used the system. The surveys examined the participants’ satisfaction and the system’s role in improving their healthcare knowledge.
2.4Data analysis
The collected data were processed using computers. Data analysis was conducted using statistical software IBM SPSS for Windows 25.0 and IBM Molder 18.0. We used statistical methods such as mean, standard deviation, and percentage to analyze the basic data. Correlation analysis was used to compare personal traits with consumer electronic products. A paired-samples
3.Results
This study found that participants used the APP average 5 to 31 times in six months, with an average frequency of 17 times. Particularly, participants used the APP more frequently within the first three days after attending the outpatient clinic. The 258 participants had an average age of 58.76
Table 1
Basic information of the study participants (
| Variable item ( | Mean | No. of people (%) |
|---|---|---|
| Age | 58.76 | |
| Gender | ||
| Male | 124 (48.0) | |
| Female | 134 (52.0) | |
| Educational degree | ||
| High School | 117 (51.5) | |
| College | 89 (34.4) | |
| University | 49 (18.9) | |
| Graduate and above | 3 (1.1) | |
| Married | ||
| Yes | 156 (60.4) | |
| No | 88 (34.1) | |
| Single | 28 (10.8) | |
| Participant | ||
| Patient | 210 (81.3) | |
| Family | 48 (18.7) | |
| Basic computer skills | ||
| Poor | 26 (10.0) | |
| Good | 208 (80.6) | |
| Excellent | 24 (9.3) |
3.1Usability of the care reminder system
In total, 67 common medications for chronic diseases were selected. The 67 common medications were based on the patients’ prescriptions and frequently consulted types. These medications were primarily from the information provided by the patients and their physicians. We used a decision tree algorithm to sort the potential interactions into 15 major categories (blood, systemic matters, mental state, oral cavity, respiratory tract, gastrointestinal tract, cardiovascular system, peripheral circulation, musculoskeletal system, skin, liver function, urinary tract, visual acuity, hormones, and inflammation) including 75 side effects or interactions. Two supportive care reminder guidelines were provided for each interaction. For example, the guidelines covering systemic effects such as nausea and dizziness were as follows: (1) Blood pressure was measured one hour before and after the medication time. If it fell below 90/60 mmHg, the medication was stopped or the person rested in a sitting or lying position for five minutes before taking another measurement. (2) When getting out of bed or moving around, patients did it slowly and refrained from performing hazardous work. Most participants used the system themselves with assistance. Approximately 80.7% perceived themselves to have good basic computer skills. The relationship between age and educational level and the level of experience using 3C products was determined using Pearson’s correlation coefficient. Age was negatively correlated with educational level in 3C product use (
Table 2
Correlation analysis of the participants’ demographic variables (
| Age | Educational level | Basic computer skills | ||
|---|---|---|---|---|
| Age | Correlation coefficient, r | 1 | ||
| 0.020 | 0.04 | |||
| Educational level | Correlation coefficient, r | 1 | 0.128* | |
| 0.020 | 0.003* | |||
| Basic computer skills | Correlation coefficient, r | 0.128* | 1 | |
| 0.04 | 0.003* |
*P< 0.05.
Regarding their knowledge of common side effects and interactions, the 258 participants’ average score increased from 50 to 80 after using SDINRS for six months. However, they still faced difficulties in fully understanding the academic terms used to describe drug interactions. Furthermore, the system’s app usability score (including participant convenience and satisfaction) increased from 45.0 to 90.0. After the six-month intervention, the knowledge score at the post-test increased by 30 points compared to the pre-test. The differences between the pre-and post-intervention scores were significant for all questionnaire items (
Table 3
Comparing SDINRS effectiveness
| ( | ||||
|---|---|---|---|---|
| Knowledge | Satisfaction |
|
| |
| Score before using SDINRS | 50.0 | |||
| Score after using SDINRS | 80.0 | 34.599 | 0.003* | |
| Usability before use | 45.0 | |||
| Usability after use | 90.0 | 11.223 | 0.001* | |
*P < 0.05.
3.2Participants’ subjective evaluation
Regarding the nursing guidance mobile application, we analyzed participants’ open-ended responses to the drug reminder system questionnaire to understand their experiences, feelings, and thoughts about post-medication precautions. A total of 178 text data sets were generated through text mining to analyze keywords from the responses. The results indicate that the most frequently used terms in the user feedback of the post-test were “simple” and “convenient.” Participants expressed a desire to include information on drug types and more image-based videos in the nursing content guidance. Attendees also suggested adding a counseling platform. Moreover, descriptive terms presented more than five times in the text mining analysis extraction were used. The participants’ subjective evaluations of SDINRS indicated the following system advantages: Its ability to help participants better understand the meaning of the academic terms used to describe side effects and interactions; The role that nursing care reminders play in reducing individual concerns and motivating behavioral change. Regarding the interface design, participants expressed their desire to include information on medication types and more image-based videos in the nursing guidance content. The participants also recommended the addition of a consultation platform.
4.Discussion
4.1Changes related to misconceptions about basic information
Since people of all ages now use many 3C products, and, middle-aged and elderly people seem interested in using apps [21, 24]. The SDINRS app used in the present study improved the middle-aged and elderly participants’ understanding of specific academic terms that describe medication side effects; it used easy-to-understand terms that allowed participants to better comprehend the precautions related to medication use. After the questionnaire was completed and collected in this study, the open data on the participants’ feelings about using the smart drug reminder system were analyzed with text exploration. A total of 186 questionnaires were used for keyword analysis with the free “HTML5 text analysis cloud platform” provided by the Internet.
4.2Effectiveness of the SDINRS app intervention
We performed a pre-test at the time of this study’s data collection. We performed a post-test at least two weeks after use and followed up with the participants for six months. Six months after implementing the SDINRS intervention, participants achieved higher scores concerning their knowledge of common medication-related side effects and interactions. They exhibited a better understanding of basic home-care concepts [24]. These results differ from previous studies that used healthcare apps only for recording purposes [25, 26]. Since the present study did not include a long-term follow-up, it is unclear if delayed effects resulted from the study. However, the app allowed for direct queries regarding patients’ medication side effects and healthcare reminders. Furthermore, the participants’ subjective evaluations indicate that they spent more time using the SDINRS app than other healthcare apps. Participants also used other search engines (e.g., Google) to a lesser degree when accessing relevant information. This study also found that using digital products for care counseling provides real-time, convenient responses. This is more effective than fixed-time medication counseling, similar to Brucker-Kley and Tang’s findings. The speed and convenience of 3C products are gradually replacing the traditional care model [27, 28].
4.3SDINRS app integrated into QSAR intelligence
This study focused on the development and clinical application of the SDINRS app in reminding patients about home care. Furthermore, the QSAR application focused on basic calculation and feedback while using the prediction model of a single algorithm only. Kwon and Zdrodowska found that using a single model did not elicit impressive results when the response characteristics of each subject were collected; however, the most important predictors could be identified by combining multiple models [23, 29]. This study’s main algorithm was a basic artificial neural network. The results can be combined with the design concept of QSAR in future research [30]. More machine learning algorithms can be incorporated, such as binary logistic regression and random forest, to calculate the possible side effects of medication for specific patients. This could provide real-time warnings for home care and optimize the performance of the app.
4.4Limitations
If more research funding is available, we can track the effectiveness of use in individual cases over a longer period of time.
5.Conclusion
The present study was conducted to establish a system that provides healthcare reminders related to medication use. The app was designed considering medication, home healthcare, diets, and the queries and reminder settings for patients, family members, and the public. This study’s findings indicate that middle-aged and elderly individuals can use smart 3C products as intervention tools. SDINRS helps increase the public’s medication-use knowledge, expand their participation in the self-care process, and boost their self-confidence and self-worth. This study suggests that introducing a healthcare information technology system can allow the public to set reminders regarding critical healthcare-related matters. It can also alleviate their concerns about forgetting the care-related information provided by medical personnel or the overly complex process for obtaining information online. By simplifying and standardizing complex issues, this system for public use can increase care safety and convenience.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethics statement
The research plan was approved by the research ethics committee of the medical department of the researchers’ institution (IRB number: (866)110-12). Before participating in the study, participants were provided with a detailed explanation of the research content, after which their written informed consent was obtained.
Author contributions
Both authors were responsible for the conception and design of the research, data collection, data analysis, data interpretation, manuscript writing and final approval of the manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Acknowledgments
We thank the staff of the Teaching and Research Center, Cheng Hsin General Hospital for their assistance in the research process.
Conflict of interest
The authors declare no conflicts of interest.
References
[1] | Min JS, Bae SK. Prediction of drug-drug interaction potential using physiologically based pharmacokinetic modeling. Arch Pharm Res. (2017) ; 40: (12): 1356-1379. |
[2] | Kao CW, Chuang HW, Chen TY. The utilization of health-related applications in chronic disease self-management. J Nurs. (2017) ; 64: (4): 19-25. doi: 10.6224/JN.000050. |
[3] | Liu HY, Chen TJ. Current state and development of m-health app usage. Clin Med. (2017) ; 80: (3): 507-510. |
[4] | Boullata JI. Drug-nutrition interactions and the brain: It’s not all in your head. Curr Nutr Rep. (2019) ; 8: (2): 92-98. doi: 10.1007/s13668-019-0273-2. |
[5] | Yeh ML. Drug safeguards to ensure the ambulatory medication safety of elderly people. J Nurs. (2013) ; 60: (2): 24-31. doi: 10.6224/JN.60.2.24. |
[6] | Boullata JI. Drug and nutrition interactions: Not just food for thought. J Clin Pharm Ther. (2013) ; 38: (4): 269-271. doi: 10.1111/jcpt.12075. |
[7] | Cheng F, Zhao Z. Machine learning-based prediction of drug-drug interactions by integrating drug phenotypic, therapeutic, chemical, and genomic properties. J Am Med Inform Assoc. (2014) ; 21: (e2): e278-e286. doi: 10.1136/amiajnl-2013-002512. |
[8] | Ge B, Zhang Z, Zuo Z. Updates on the clinical evidenced herb-warfarin interactions. Evid Based Complement Alternat Med. (2014) ; 2014: : 957362. doi: 10.1155/2014/957362. |
[9] | Ching TT. Health information technology for quality improvement and patient safety. J Hosp Bimon. (2014) ; 47: (3): 31. |
[10] | Ching WY. The user-centric based mobile health apps to facilitate patients while receiving medical treatments. J Hosp Bimon. (2014) ; 47: (4): 25-29. |
[11] | Mehralian HA, Moghaddasi J, Rafiei H. The prevalence of potentially beneficial and harmful drug-drug interactions in intensive care units. Drug Metab Pers Ther. (2019) ; 34: (1). |
[12] | Jafari J, Moonaghi HK, Zary N, Masiello I. Exploring educational needs and design aspects of internet-enabled patient education for persons with diabetes: A qualitative interview study. BMJ Open. (2016) ; 6: (10): 1-7. |
[13] | Lin MF, Chen WJ, Chang XL, Lai YW. Drug interactions build database of clinical classification. J Med Qual. (2014) ; 8: (3): 51-53. |
[14] | Ötles S, Senturk A. Food and drug interactions: A general review. Acta Sci Pol Technol Aliment. (2014) ; 13: (1): 89-102. doi: 10.17306/J.AFS.2014.1.8. |
[15] | Qiu QR, Zhang YY, Chen WZ, Huang, JZ, Huang ZX. Evaluation of high tree village health of rural elderly. J Nurs Res. (2000) ; 8: (2): 227. |
[16] | Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. (2013) ; 12: (1): 14. doi: 10.1186/2251-6581-12-14. |
[17] | Chen CM, Hou IC, Chen HP, Weng YC. Design of an electronic reminder system for supporting the integerity of nursing records. Stud Health Technol Inform. (2016) ; 225: : 830-831. |
[18] | Wang WJ. Medical quality award series-class small hospital medical wisdom medical chapter: Preventive care tips APP. J Med Qual. (2015) ; 9: (2): 77. |
[19] | Alrabiah Z, Alhossan A, Alghadeer SM, Wajid S, Babelghaith SD, Al-Arifi MN. Evaluation of community pharmacists’ knowledge about drug-drug interaction in Central Saudi Arabia. Saudi Pharm J. (2019) ; 27: (4): 463-466. doi: 10.1016/j.jsps.2019.01.008. |
[20] | Jain S, Ecker GF. In silico approaches to predict drug-transporter interaction profiles: Data mining, model generation, and link to cholestasis. Methods Mol Biol. (2019) ; 1981: : 383-396. doi: 10.1007/978-1-4939-9420-5_26. |
[21] | Wang CJ, Chaovalit P, Pongnumkul S. A breastfeed-promoting mobile app intervention: Usability and usefulness study. JMIR Mhealth Uhealth. (2018) ; 6: (1): e27. doi: 10.2196/mhealth.8337. |
[22] | Wu LC, Chen SX, Xu YJ, Zhuang ZH. Community treatment in elderly people plagued. Changhua Nurs. (2015) ; 22: (1): 26. |
[23] | Kwon S, Bae H, Jo J, Yoon S. Comprehensive ensemble in QSAR prediction for drug discovery. BMC Bioinform. (2019) ; 20: (1): 521. doi: 10.1186/s12859-019-3135-4. |
[24] | Liao PH, Kang SJ. The mindset and realization of precision care provided by the science of ambient-assisted living. Hu Li Za Zhi. (2022) Apr; 69: (2): 19-24. Chinese. doi: 10.6224/JN.202204_69(2).04. PMID: 35318629. |
[25] | Chiou PY, Liao PH, Liu CY, Hsu YT. Effects of mobile health on HIV risk reduction for men who have sex with men. AIDS Care. (2020) Mar; 32: (3): 316-324. doi: 10.1080/09540121.2019.1668531. Epub 2019 Sep 26. PMID: 31558040. |
[26] | Shih YL, Hsieh CJ, Lee TY, Liao PH, Wu HT, Liu CY. Sex Differences between Urinary Phthalate Metabolites and Metabolic Syndrome in Adults: A Cross-Sectional Taiwan Biobank Study. Int J Environ Res Public Health. (2022) Aug 22; 19: (16): 10458. doi: 10.3390/ijerph191610458. PMID: 36012094; PMCID: PMC9407747. |
[27] | Brucker-Kley E, Kleinberger U, Keller T, Christen J, Keller-Senn A, Koppitz A. Identifying research gaps: A review of virtual patient education and self-management. Technol Health Care. (2021) ; 29: (6): 1057-1069. doi: 10.3233/THC-202665. |
[28] | Tang X, Li F, Seetharam TG, Vignesh CC. Internet of Things-assisted intelligent monitoring model to analyze the physical health condition. Technol Health Care. (2021) ; 29: (6): 1355-1369. doi: 10.3233/THC-213011. |
[29] | Zdrodowska M, Dardzińska-Głȩbocka A. Classification and action rules in identification and self-care assessment problems. Technol Health Care. (2022) ; 30: (1): 257-269. doi: 10.3233/THC-219008. |
[30] | Shayanfar S, Shayanfar A. Comparison of various methods for validity evaluation of QSAR models. BMC Chem. (2022) ; 16: (1): 63. doi: 10.1186/s13065-022-00856-4. |


