
Comparing digital and traditional guides in first molar implant surgery: A randomized clinical trial
Abstract
BACKGROUND:
There are few studies on the differences in clinical outcomes with implant guides made by different methods in cases with a single tooth loss and adjacent tooth support
OBJECTIVE:
To compare the use of digital and traditional implant guides in patients whose first molars are absent and who are undergoing implant restoration.
METHODS:
This study included 42 patients with first molars missing who were randomly divided into two groups: the digital group (
RESULTS:
The impression time and implant surgery time in the digital group were less than in the traditional group. The intraoral first fit of the guide in the digital group was higher than in the control group (
CONCLUSIONS:
In a first molar implant, the digital implant guide can effectively reduce the clinical operative time and the screw access deviation and improve efficiency. The clinical results with the digital guide provide a basis for its use in implant therapy for single missing teeth.
1.Introduction
With the improvement of medical technology, implant repair has become the preferred method for clinicians and patients to treat missing teeth [1, 2]. The use of an implant guide plate can help achieve accurate positioning in the operative process and guarantee the correct position, angle, and depth of the implant [3, 4, 5].
At present, digital technology is becoming widely used in the field of oral implantation [6, 7]. The accuracy of the implant position and depth after using the implant guide plate positioning is the subject of much research worldwide [8]. At present, there is a consensus that the accuracy of the tooth-supported implant guide is higher than that of the mucosa-supported implant guide and the mixed supported implant guide [9, 10, 11]. The main reason is that the tooth support is relatively stable, which can effectively avoid the micromotion of the guide plate caused by the stress sinking in the mucosa [12]. The implant accuracy is better with the tooth-support type guide plate for a single missing tooth [13]. However, there are few studies on the differences in clinical outcomes with implant guides made by different methods (such as the traditional impression pattern implant guide and the digital CAD/CAM implant guide) in cases with a single tooth loss and adjacent tooth support [14].
Therefore, in this study, we compared the outcomes of two different methods (intraoral digital impression and conventional impression) in the treatment of missing first molars, including time to make the impression and to do the surgery, fit of intraoral guide, and deviation of the screw access channel position. The purpose of this study is to find a more suitable implant guide for single-tooth implant restoration and to provide a more comprehensive theoretical basis for oral surgeons to choose the operation.
2.Materials and methods
2.1Study individuals
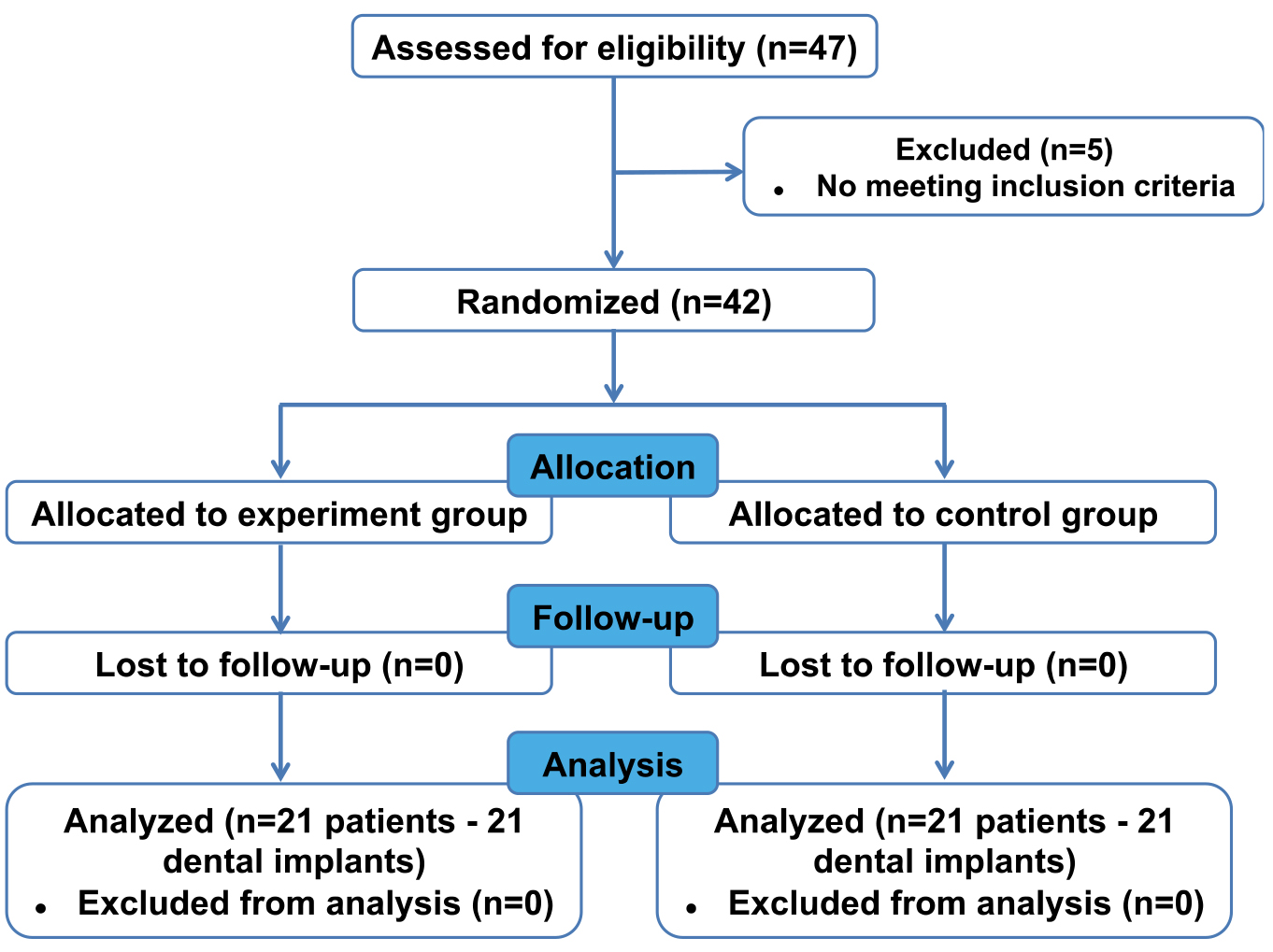
This study was conducted between January 2019 and December 2020 in the Department of Dentistry of Nanfang Hospital, Southern Medical University. The research was approved by the Ethics Committee of Nanfang Hospital, Southern Medical University (NFEC-2017-072). Forty-two patients with missing first molars were enrolled in the study. Written informed consent was obtained from every individual. The enrolled individuals were randomly divided into two groups, digital and control (Fig. 1).
Figure 1.
The flowchart of the study.
2.2Inclusion and exclusion criteria
Individuals over 18 years old with good mental health and ability to fully understand and sign the consent form were included in the study. The inclusion criteria included good general health (healthy or with well-controlled chronic disease) with no contraindications for implant surgery; willing to receive the dental implant treatment and comply with the follow up; and normal mouth opening. The exclusion criteria included chronic oral inflammation such as periodontal disease that would affect implant surgery; poor oral hygiene; systemic diseases that affect implant surgery; and pregnancy or nursing.
2.3Design and manufacture of the surgical template
In the digital group, the 3Shape Trios scanning (3Shape, Copenhagen Denmark) probe was used to obtain the surface morphology of the teeth, gingiva, and other tissues. Cone beam computed tomography (CBCT) was performed before the operation to construct a three-dimensional model of the jaw. Then, CBCT image data and intraoral scanning data were imported into the digital guide software to simulate the implant position, direction, and depth.
In the control group, the intraoral model was made with silicone rubber (DMG Silagum, Hamburg, Germany). After the model was disinfected, the diagnostic wax was made in the missing tooth area, and a plaster model was turned over. After arranging the missing tooth on the plaster model, a transparent resin mold was used to press the guide plate prototype into the vacuum molding machine. The rudimentary guide plate was placed on the model to remove the diagnostic wax. A low-speed turbine handpiece (NSK, Tokyo, Japan) was used to open a hole in the corresponding implantation site. A metal catheter was inserted into the hole and fixed with resin material.
The implant guides were used to complete the implant surgery in both groups. Three months after surgery, silicone rubber implant impressions and screw retention of the permanent prosthesis were evaluated. During the whole treatment process, the same nurse completed the model preparation and perfusion. The same dentist carried out implant (Astra Tech, Dentsply, USA) surgery and prosthesis insertion, and the same technician made the digital guide plate and prostheses.
2.4Outcome measurements
The labor time evaluated in this study included time for making impressions, surgery, and occlusal adjustments. In the digital group, time for making impressions included the time taken to obtain the surface morphology of teeth, gums, and other tissues in the oral cavity. In the control group, the impression time included the selection of the tray, mixing of silicone rubber, preparation of the intraoral mold, and the time for plaster model perfusion.
After preparing the guide, the guide plate was placed in the mouth to check the placement, prying fit, and stability.
Figure 2.
The deviation length and direction of the screw access channel position. The orange circle indicates the planed screw access channel, and the blue circle indicates a placed screw access channel. The deviation length was the diameter between the center of the orange and blue circles. Taking the midpoint of an orange circle as the origin, the X and Y axes (red lines) of quadrants were drawn along the proximal, distal, buccal, and lingual regions, respectively. The four quadrants are mesial lingual, mesial buccal, distal lingual, and distal buccal, which are abbreviated as ML, MB, DL and DB quadrants.
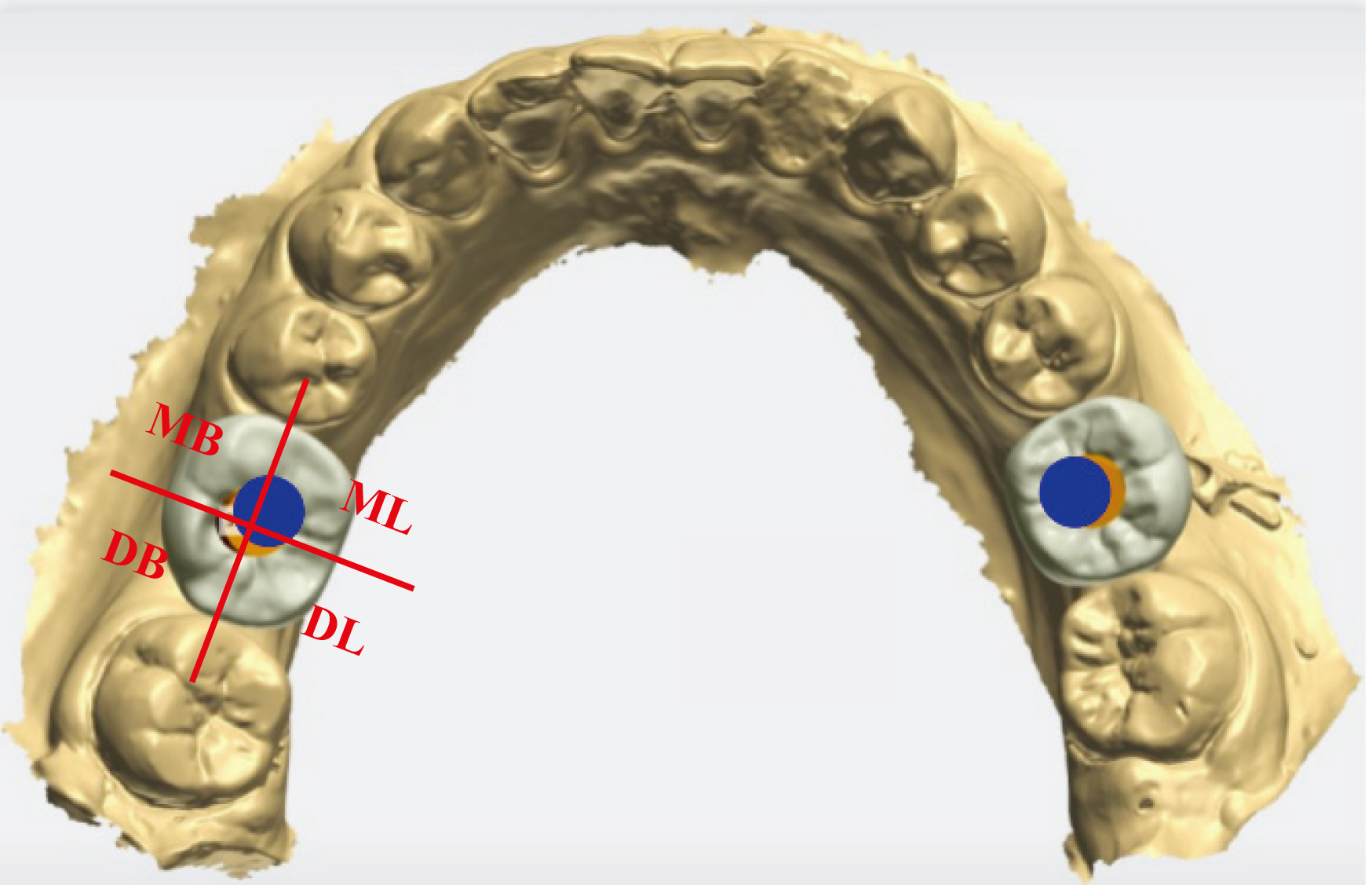
The deviation length and direction of the screw access channel position were evaluated and compared in the two groups. In Fig. 2, the orange circle indicates the planed screw access channel, and the blue circle indicates a placed screw access channel. The deviation length was the diameter between the center of the orange and blue circles. Taking the midpoint of an orange circle as the origin, the X and Y axes (red lines) of quadrants were drawn along the proximal, distal, buccal, and lingual regions, respectively. The four quadrants are mesial lingual, mesial buccal, distal lingual, and distal buccal, which are abbreviated as ML, MB, DL and DB quadrants (Fig. 2). The quadrant where the midpoint of the blue circle falls was recorded. The number of cases in each quadrant was recorded.
2.5Statistical analysis
A pilot study (
All the data were analyzed by the SPSS 20.0 software package (IBM, New York, USA). The quantitative data of the two groups were compared by an independent sample
3.Results
3.1Characteristics of the study individuals
Characteristics including gender, age, and number of missing teeth were compared in the digital and conventional groups, and no significant differences were found between the two groups (Table 1).
Table 1
Characteristics of digital and control groups
| Digital group | Control group |
|
| |
|---|---|---|---|---|
| Age | 43.95 | 42.95 | 0.415 | 0.618 |
| Gender (male/female) | 11/10 | 9/12 | 0.318 | 0.537 |
| Number of left-side first molar | 10 | 11 | 0.095 | 0.758 |
| Number of right-side first molar | 11 | 10 |
3.2Labor time
Time required for making impressions and operative time in the digital group were less than those in the control group, and the difference was statistically significant. There was no difference in occlusal adjustment time between the two groups, and the results are shown in Table 2.
Table 2
Labor time in digital and control groups
| Digital group | Control group |
|
| |
|---|---|---|---|---|
| Impression time | 8.13 | 10.96 | 0.000 | |
| Occlusal adjustment time | 8.19 | 8.75 | 0.112 | |
| Surgery time | 8.03 | 10.31 | 0.002 |
Table 3
Satisfaction with the guide during fitting
| Digital group ( | Control group ( |
|
| |
|---|---|---|---|---|
| The degree of satisfaction during first fitting | 21 | 16 | 5.676 | 0.017 |
3.3Satisfaction with the guide during fitting
The degree of satisfaction during the first fitting in the digital group was 100 percent. In the control group, there were five individuals for whom the guides did not fit. After modifications and adjustments of the guides, the degree of satisfaction during the second fitting in control group was 100 percent. A significant difference was observed between the two groups regarding the satisfaction with the guide during first fitting.
3.4The deviation length of screw access channel position
Due to the effect of the position of missing teeth, the digital and control groups were divided into two subgroups (left- and right-side implants). In the digital group, there was no significant difference in the deviation of the screw access channel position between the left- and right-side subgroups. In the control group, the deviation of the screw access channel position in the right-side subgroup was significantly lower than in the left-side subgroup. Meanwhile, the deviation of the screw access channel position was significantly lower in the digital group than the control group (Table 4 and Fig. 3).
Table 4
The deviation length of the screw access channel position
| Digital group ( | Control group ( | |||
|---|---|---|---|---|
| Left ( | Right ( | Left ( | Right ( | |
| Deviation length | 0.749 | 0.696 | 1.755 | 0.979 |
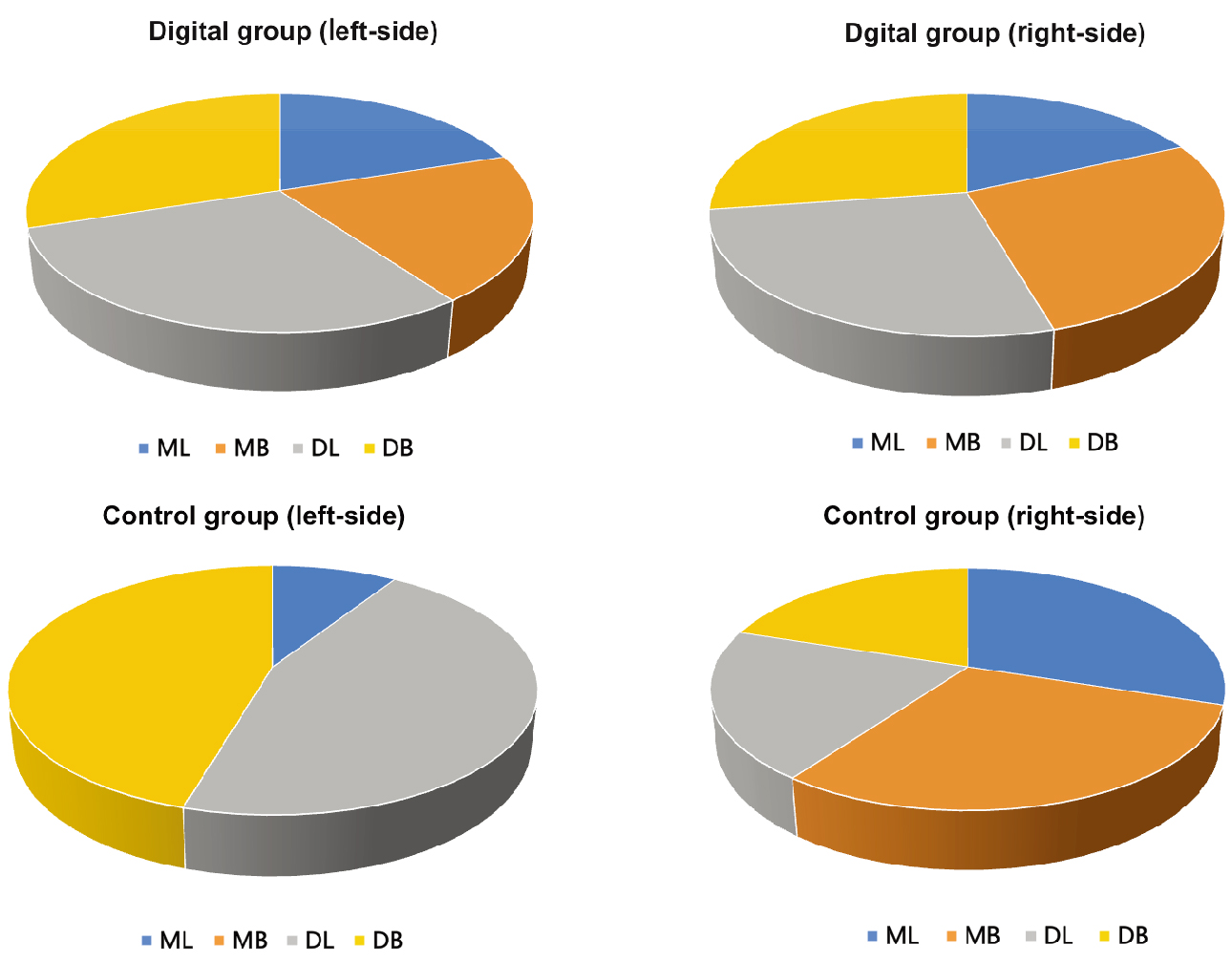
3.5The deviation direction of screw access channel position
In the digital group, there was no difference in the direction of left-side and right-side deviation. In the control group, there was a statistical difference in the deviation direction between the left and right sides, and the left side direction deviated distally (Table 5 and Fig. 4).
Table 5
The deviation direction of screw access channel position
| Digital group ( | Control group ( | |||||||
|---|---|---|---|---|---|---|---|---|
| ML | MB | DL | DB | ML | MB | DL | DB | |
| Left deviation | 2 | 2 | 3 | 3 | 1 | 0 | 5 | 5 |
| Right deviation | 2 | 3 | 3 | 3 | 3 | 3 | 2 | 2 |
Figure 3.
The deviation of the screw access channel position in the digital group and the control group.
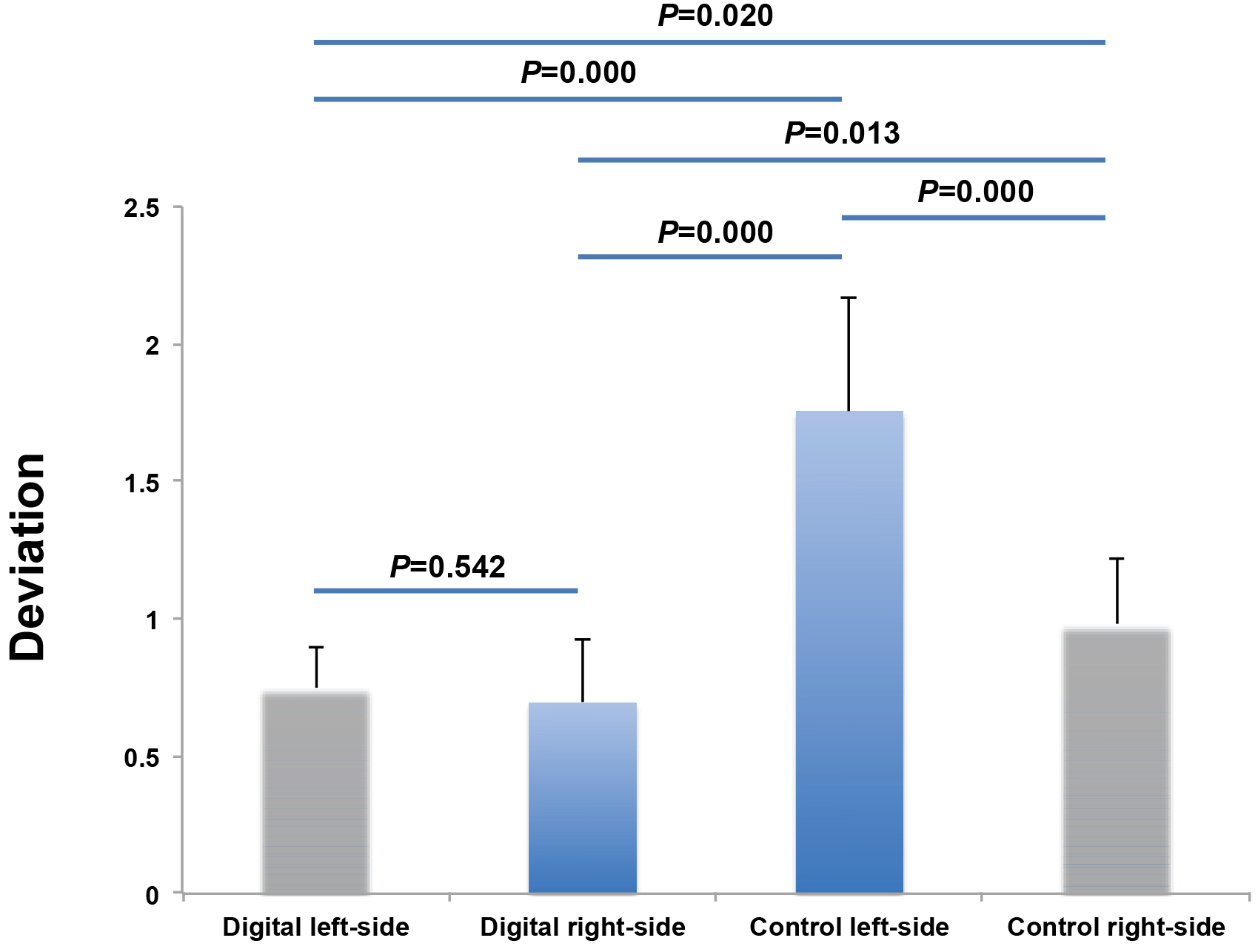
Figure 4.
The deviation direction between the left and right sides.
4.Discussion
Implant guides can be prepared by the traditional impression method and by the CAD/CAM method [15, 16]. The use of the traditional guide made by resin has some limitations [17]. When it is applied to complicated cases with poor soft and hard tissue conditions, implantation accuracy is lower than with the digital implant guide, and it may even cause implant failure [18]. So far, there is no research concerning the differences in the clinical effects between these two kinds of guide plates when they are used in cases of good bone conditions and a single missing tooth.
In our research, digital and traditional impression methods were carried out in patients with a single first molar missing. The impression time and surgery time in the digital group were less than in the control group, and the difference was statistically significant. This is because using alginic acid or silicone rubber in the traditional guide plate to make models takes more time. The digital guide plate was made by intraoral scanning, which not only reduced the surgical time but also simplified the treatment process [19, 20, 21]. Therefore, the time for making a guide plate and impression in the digital group was less than that in the control group. At the same time, because of the good retention force and intraoral fit of the digital implant guide, repeated adjustment of the position of the guide and the subsequent patient discomfort were avoided, thus shortening the operative time [22].
In the traditional implant guide, the mixing time for the impression material, the surgical method, the ambient temperature, the suitability of the impression tray, and the pouring of the gypsum model affect the accuracy of the model. In addition, the traditional implant guide does not exhibit the three-dimensional structure of the implant bone area, and there is no accurate positioning marker [23, 24, 25]. Additionally nowadays a completely digital workflow is possible in clinical dentistry, from digital impression, thorough manufacturing production to final framework, showing good clinical reliability [26] and excellent patients’ feedback [27] in many fields of dentistry. Therefore, the intraoral fit in the control group was not as good as that in the digital guide group.
The information provided by the guide plate made by the traditional impression method is limited. In particular, it does not consider the bone tissue. Use of the digital implant guide enables dental surgeons to fully consider the internal anatomy of the jaw, with high accuracy [28, 29]. The retention design of the prosthesis depends on the implant angle and depth. Therefore, the deviation of the screw access channel position as guided by the digital plate is less than that in the traditional method. At the same time, the left first molar with traditional guide plate was the largest. This is due to the unstable retention force in the implant area with the traditional guide plate. In addition, the operator is located on the right side of the patient, which easily causes horizontal and positioning deviation without a precise guide plate. In the digital group, the digital guide plate was used to fully expose the surgical field. The positioning hole of the guide plate was accurate and stable, so as to effectively avoid the influence of the operator’s position during surgery. When the left-side implant was placed in the digital group under the precise guidance of the digital guide plate, there was no need to repeatedly adjust the operation position, and the guide plate fixed the positioning drill in a stable position. The results showed that the deviation length and direction of the screw access channel position in the digital group were not limited by the body position, and there was no difference between the left and right sides. However, the control group was still affected by the operator’s position, and the deviation length of the screw access channel on the left side was higher than on the right, and most of them were in the far middle direction.
5.Conclusion
The results of this study showed that for the cases with good bone condition and a single tooth missing, there were advantages and disadvantages of different implant guides. The main reason is that surgery on the left and right sides is affected by body position and tooth position, and it is difficult to place an implant using a simple guide plate. However, the digital implant guide plate provides stable retention and accurate positioning, which can reduce the adverse effects of different tooth positions and body positions and obtain better clinical effects.
The traditional implant guide is mostly made of alginic acid or silicone rubber. It takes more time to mix materials, select pallets or make personalized pallets, and turn gypsum models. The digital guide conducted by the intraoral scanner not only reduces the operation time, but also simplifies the treatment process. Meanwhile, the digital impression scanning method makes the impression to avoid the nausea and vomiting caused by patients using alginate or silicone rubber impression. In addition, due to the good retention and intraoral fit of the digital implant guide, the intraoperative discomfort caused by repeatedly adjusting of the guide is avoided.
A digital implant guide is not suitable for patients with limited mouth opening and narrow gap between implant sites. However, with the application of computer technology, a digital implant guide provides a new opportunity for implant repair treatment of patients with complicated cases. The digital implant guide can effectively reduce the clinical operative time and the deviation of the screw access channel position and improve work efficiency. The digital guide is recommended for use in implant therapy for a single missing tooth.
The research only focused on the clinical effect of digital guide plate in the delayed implantation of first molar. In the future work, the research of digital guide plate can be carried out in patients with early implantation and immediate implantation in multiple centers.
Acknowledgments
The study was supported by the Science and Technology Program of Guangzhou, China (201907010032), the Clinical Research Startup Program of Southern Medical University by High-level University Construction Funding of Guangdong Provincial Department of Education (LC2016PY022), the Clinical Research Program of Nanfang Hospital, Southern Medical University (2018CR022, 2021CR016), the Courtyard’s Level Program of Hainan General Hospital (QN202012), the Medical Scientific Research Foundation of Guangdong Province of China (B2021076) and the Nursing Special Research Project of Southern Medical University (Y2018008).
Conflict of interest
None to report.
References
[1] | Guglielmotti MB, Olmedo DG, Cabrini RL. Research on implants and osseointegration. Periodontol 2000. (2019) ; 79: (1): 178-189. |
[2] | Albrektsson T, Chrcanovic B, Östman PO, Sennerby L. Initial and long-term crestal bone responses to modern dental implants. Periodontol 2000. (2017) ; 73: (1): 41-50. |
[3] | Mijiritsky E, Ben Zaken H, Shacham M, Cinar IC, Tore C, Nagy K, Ganz SD. Variety of surgical guides and protocols for bone reduction prior to implant placement: A narrative review. Int J Environ Res Public Health. (2021) ; 18: (5): 2341. |
[4] | Chen P, Nikoyan L. Guided implant surgery: A technique whose time has come. Dent Clin North Am. (2021) ; 65: (1): 67-80. |
[5] | De Santis D, Gelpi F, Zambotti T, Rossetto A, Luciano U, Zotti F, Iurlaro A, Zarantonello M, Finotti M, Alberti C, Zangani A, Capocasale G, Donadello D, Faccioni P, Nocini PF. The use of computer-guided flapless dental implant surgery (Nobel guide) and immediate function to support a fixed full-arch prosthesis in fresh frozen homologous bone grafted patients: a retrospective cohort study with 5 to 8-year follow-up. J Biol Regul Homeost Agents. (2020) ; 34: (6 Suppl 2): 49-61. |
[6] | Tanveer W, Ridwan-Pramana A, Molinero-Mourelle P, Koolstra JH, Forouzanfar T. Systematic review of clinical applications of CAD/CAM technology for craniofacial implants placement and manufacturing of nasal prostheses. Int J Environ Res Public Health. (2021) ; 18: (7): 3756. |
[7] | Kernen F, Kramer J, Wanner L, Wismeijer D, Nelson K, Flügge T. A review of virtual planning software for guided implant surgery – data import and visualization, drill guide design and manufacturing. BMC Oral Health. (2020) ; 20: (1): 251. |
[8] | Tatakis DN, Chien HH, Parashis AO. Guided implant surgery risks and their prevention. Periodontol 2000. (2019) ; 81: (1): 194-208. |
[9] | Raico Gallardo YN, da Silva-Olivio IRT, Mukai E, Morimoto S, Sesma N, Cordaro L. Accuracy comparison of guided surgery for dental implants according to the tissue of support: a systematic review and meta-analysis. Clin Oral Implants Res. (2017) ; 28: (5): 602-612. |
[10] | Kurbad A. Tooth-supported surgical guides for guided placement of single-tooth implants. Int J Comput Dent. (2017) ; 20: (1): 93-105. |
[11] | Layton D. A critical appraisal of the survival and complication rates of tooth-supported all-ceramic and metal-ceramic fixed dental prostheses: the application of evidence-based dentistry. Int J Prosthodont. (2011) ; 24: (5): 417-27. |
[12] | Derksen W, Wismeijer D, Flügge T, Hassan B, Tahmaseb A. The accuracy of computer-guided implant surgery with tooth-supported, digitally designed drill guides based on CBCT and intraoral scanning. A prospective cohort study. Clin Oral Implants Res. (2019) ; 30: (10): 1005-1015. |
[13] | Pozzi A, Polizzi G, Moy PK. Guided surgery with tooth-supported templates for single missing teeth: A critical review. Eur J Oral Implantol. (2016) ; 9: (Suppl 1): S135-53. |
[14] | Cosyn J, Eghbali A, Hanselaer L, De Rouck T, Wyn I, Sabzevar MM, Cleymaet R, De Bruyn H. Four modalities of single implant treatment in the anterior maxilla: A clinical, radiographic, and aesthetic evaluation. Clin Implant Dent Relat Res. (2013) ; 15: (4): 517-30. |
[15] | Zhou M, Zhou H, Li SY, Yang XB, Geng YM, Che YJ. Accuracy of implant placement guided with surgical template: an in vitro and in vivo study. Int J Periodontics Restorative Dent. (2021) ; 41: (2): e55-e62. |
[16] | Liu X, Liu J, Feng H, Pan S. Accuracy of a milled digital implant surgical guide: An in vitro study. J Prosthet Dent. (2020) ; S0022-3913: (20): 30654-5. |
[17] | Gjelvold B, Mahmood DJH, Wennerberg A. Accuracy of surgical guides from 2 different desktop 3D printers for computed tomography-guided surgery. J Prosthet Dent. (2019) ; 121: (3): 498-503. |
[18] | Bell CK, Sahl EF, Kim YJ, Rice DD. Accuracy of Implants Placed with Surgical Guides: Thermoplastic Versus 3D Printed. Int J Periodontics Restorative Dent. (2018) ; 38: (1): 113-119. |
[19] | Brandt J, Brenner M, Lauer HC, Brandt S. Accuracy of a template-guided implant surgery system with a CAD/CAM-based measurement method: An in vitro study. Int J Oral Maxillofac Implants. (2018) ; 33: (2): 328-334. |
[20] | Park SJ, Leesungbok R, Cui T, Lee SW, Ahn SJ. Reliability of a CAD/CAM surgical guide for implant placement: an in vitro comparison of surgeons’ experience levels and implant sites. Int J Prosthodont. (2017) ; 30: (4): 367-169. |
[21] | Reyes A, Turkyilmaz I, Prihoda TJ. Accuracy of surgical guides made from conventional and a combination of digital scanning and rapid prototyping techniques. J Prosthet Dent. (2015) ; 113: (4): 295-303. |
[22] | Ritter L, Palmer J, Bindl A, Irsen S, Cizek J, Karapetian VE, Zöller JE. Accuracy of chairside-milled CAD/CAM drill guides for dental implants. Int J Comput Dent. (2014) ; 17: (2): 115-24. |
[23] | Conejo J, Atria PJ, Schweitzer D, Blatz MB. Digital implant planning and surgical guides: tools for clinical success. Compend Contin Educ Dent. (2021) ; 42: (7): 400-401. |
[24] | Komuro A, Yamada Y, Uesugi S, Terashima H, Kimura M, Kishimoto H, Iida T, Sakamoto K, Okuda K, Kusano K, Baba S, Sakamoto T. Accuracy and dimensional reproducibility by model scanning, intraoral scanning, and CBCT imaging for digital implant dentistry. Int J Implant Dent. (2021) ; 7: (1): 63. |
[25] | Yeung M, Abdulmajeed A, Carrico CK, Deeb GR, Bencharit S. Accuracy and precision of 3D-printed implant surgical guides with different implant systems: An in vitro study. J Prosthet Dent. (2020) ; 123: (6): 821-828. |
[26] | Fischer CAI, Ghergic DL, Vranceanu DM, Ilas SA, Comaneanu RM, Baciu F, et al. Assessment of force retention between milled metallic and ceramic telescopic crowns with different taper angles used for oral rehabilitation. Materials (Basel). (2020) Oct 28; 13: (21): 4814. |
[27] | Sfondrini MF, Gandini P, Malfatto M, Di Corato F, Trovati F, et al. Computerized casts for orthodontic purpose using powder-free intraoral scanners: accuracy, execution time, and patient feedback. Biomed Res Int. (2018) ; 2018: : 4103232. |
[28] | Smitkarn P, Subbalekha K, Mattheos N, Pimkhaokham A. The accuracy of single-tooth implants placed using fully digital-guided surgery and freehand implant surgery. J Clin Periodontol. (2019) ; 46: (9): 949-957. |
[29] | Al Yafi F, Camenisch B, Al-Sabbagh M. Is digital guided implant surgery accurate and reliable? Dent Clin North Am. (2019) ; 63: (3): 381-397. |


