
Evaluating dose distributions of normal organs for patients undergoing VMAT therapy of nasopharyngeal carcinoma using Rando phantom and TLD-100H
Abstract
BACKGROUND:
The routine radiation therapy treatment planning does not include secondary radiation and peripheral doses resulting from radiotherapy exposure in patients with nasopharyngeal carcinoma (NPC) undergoing Volumetric Modulated Arc Therapy (VMAT) using an linear accelerator (linac) of Axesse (Elekta 2538).
OBJECTIVE:
VMAT has a better dose conformity of the tumor and is also operated by adjusting the shapes of mulileaf collimator. However, such treatment is potentially important to improve the accuracy of estimated health risks.
METHODS:
This study aimed to evaluate the equivalent dose of organ or tissue (
RESULTS:
The thyroid dose (
CONCLUSIONS:
This study can be referred to practical guidance regarding radiation protections of the public.
1.Introduction
Reported from the statistics of the Ministry of Health and Welfare for 2019 [1], nasopharyngeal carcinoma (NPC) is the 12
2.Method
2.1Volumetric Modulated Arc Therapy (VMAT) via an Axesse linear accelerator (linac)
For oncology therapy, many different linear accelerator (linac) are used worldwide. The VMAT was designed by Axesse linac of Chung Shan Medical University Hospital (CSMUH). VMAT can associate with better dose conformity to the tumor, superior dose distribution, fewer monitoring units, and faster delivery time [2, 3, 5]. It employs linac to conduct dynamic modulated rotation of intensity-modulated radiation therapy (IMRT). It can operate by adjusting the shapes of multileaf collimator, dose rate, and gantry rotation speed to benefit patients [1].
The Rando weighs 73.5 kg and is 175 cm tall. The Rando comprised 35 numbered sections. These could make phantom suitable for oncology dose calculations [7, 10]. The Rando was embedded in the anthropomorphic material. The densities (g cm
2.2CT simulation and treatment plan
All of VMAT simulations for CT examination of NPC of phantom were carried by a 16-slice CT sim. The CT-based simulation was carried with the Rando lying supine with a thermoplastic shell. The Philip Pinnacle Planning System 9.0 was adapted for VMAT planning [3, 10].
Figure 1.
The NPC treatment of for VMAT (a) axial, (b) sagittal, and (c) coronal of 5
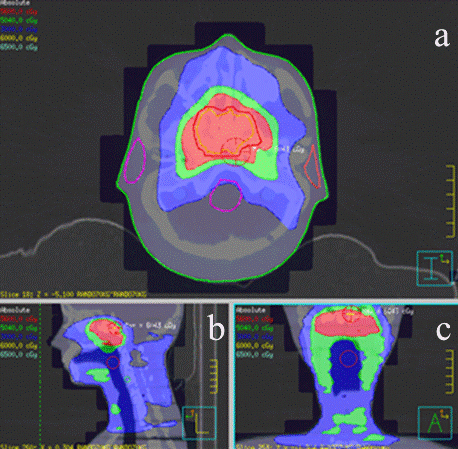
An NPC tumor size of the nasopharyngeal (NP) area of the Rando, 3
2.3Assessment of E and DT
A senior radiologist (H. C. Lin) who had a least 10 years of experience conducted the routine NPC treatment. Only the skin, salivary gland, and brain were directly irradiated during NPC treatment.
The absorbed doses (
For calculation of
(1)
In order to evaluate the effective dose,
(2)
Table 1 lists explicitly some organs and tissues. In addition, others are “remainder tissues”. To make doses evaluations for these tissues or organs those were near to as well as within the radiation field. From the head to the gonads, including the remainder organs, could be used to evaluate
Table 1
Measurement locations of the 52 points, the weighting factors (
| Section of rando | Organ/tissue |
| Numbers of TLD |
|---|---|---|---|
| 1 | Skin | 0.01 | 96 |
| 1 | Brain | 0.01 | 15 |
| 3 | Lens | 0.017 | 6 |
| 4,5,24,30 | Bone surface | 0.01 | 39 |
| 6 | Oral mucosa | 0.017 | 3 |
| 6,7 | Salivary glands | 0.01 | 12 |
| 8,31 | Lymph nodes | 0.017 | 3 |
| 8,25,26,27 | Bone marrow | 0.12 | 12 |
| 9 | Esophagus | 0.04 | 6 |
| 10 | Thyroid | 0.04 | 6 |
| 11 | Lungs | 0.12 | 21 |
| 16 | Heart | 0.017 | 3 |
| 18 | Breast | 0.12 | 3 |
| 18 | Stomach/Spleen | 0.12 | 3 |
| 19 | Pancreas | 0.017 | 3 |
| 20 | Liver | 0.04 | 3 |
| 21,29 | Colon | 0.12 | 6 |
| 22 | Kidney | 0.017 | 3 |
| 23 | Small intestine | 0.017 | 3 |
| 28 | Bladder | 0.04 | 3 |
| 32 | Gonads | 0.08 | 3 |
| Total | 1.000 | 252 |
In addition, 42 TLDs were inserted into the H&N of the patients. The background radiation was measured by 9 TLDs. Finally, total errors could be effectively suppressed by conducting 3 independent trials. This is 32 bags of TLDs attached to the Rando’ skin. The measured points on these organs were recommended by ICRP 103. The corresponding values of
2.4Calibrate TLDs via 6 MV beams
These TLDs of photon dose measurement and linearity were calibrated via Axesse linac (6 MV). (1) The distance from source-to-surface is 100 cm. (2) At a field size of 10
The TLDs were used because of their small dimensions, and the lower dependence of its response on dose rate, photon energy, as well as the direction of any incidence of X-rays from Axesse linac. A calibrated TLD readout system of Harshaw 3500 reader could be useful to measure extra X-rays radiations, and evaluate specific doses with better reliability. After 1 day of exposure, these irradiated TLDs were measured by an automated Harshaw 3500 reader. The readout was (1) the TLD was heated up to 50
2.5In vivo experiment undergoing NPC treatment
OAR in and nearby the NP where the primary irradiated were mainly measured, then throughout the entire body. Totally, 252 TLDs were placed in the Rando at each section, then directly used to evaluate
3.Results and discussion
The NPC treatments exposure several organs via many radiation sensitivities. The
3.1Calibration and uncertainty of TLD-100H
The TLD-100H represented linearly of radiation doses ranging 10–400 cGy.
The conversion factor of the TLD-100H was Y(cGy)
Table 2
Random and systematic errors coming from the practical evaluation of radiation
| Source | One standard deviation |
|---|---|
| Measurement: | |
| TLD counting statistics | 3% |
| Others: | |
| 5% | |
| VMAT output photon dose | |
| TLD-100H calibration | 3% |
| Inserting positions of phantom organ or tissue | 5% |
| Density effects of PMMA phantom | 1.5% |
| Variation of Harshaw 3500 reader | 3% |
|
| 9.00% |
These accuracy and precision of the
3.2The equivalent doses (D T
This study measured the
Figure 2.
Equivalent doses (mSv/treatment) of organs of Rando during NPC treatment.
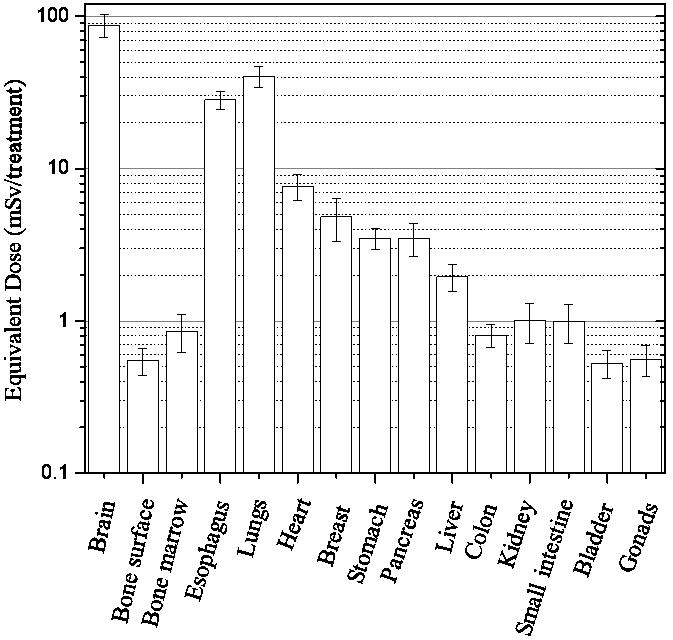
Parts of the oral mucosa, lymph nodes, and skin were also scanned. In addition, these organs had relatively low
The
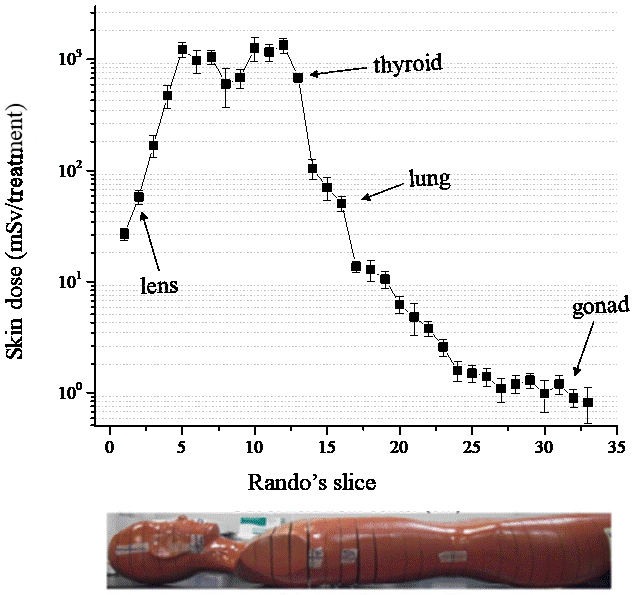
3.3Skin dose (D 𝑠𝑘𝑖𝑛
Figure 3 plots 32 measurements, data reflected the skin dose (
Figure 3.
Assessing the skin dose (
3.4Comparison of results with those of other studies
Notably, the
3.5Limitations
This study had many limitations. (1) Lack of female breast phantom could be used, so the
4.Conclusions
This study evaluated the
Acknowledgments
The authors want to thank the staff of Chung Shan Medical University Hospital for their efficient support.
Conflict of interest
None to report.
References
[1] | Statistics of General Health Welfare of 2019, Ministry of Health and Welfare, 2019. (https://dep.mohw.gov.tw/DOS/cp-1735-3242-113.html). |
[2] | Lai WH. Evaluating Dose Distributions and Minimum Detectable Dose of TLD-100H Approach for Nasopharyngeal Carcinoma Based on Rando and SDM Phantoms undergoing VMAT. Ms Thesis, Chung Shan Medical University Taiwan. (2015) . |
[3] | D’Agostino E, Bogaerts R, Defraene G, et al. Peripheral doses in radiotherapy: A comparison between IMRT, VMAT and Tomotherapy. Radiat Meas. (2013) ; 57: : 62-67. |
[4] | Lin HC, Lai TJ, Tseng HC, et al. Radiation doses with various body weights of phantom in brain 128-slice MDCT Examination. J Radiat Res. (2019) ; 60: (4): 466-475. |
[5] | International Commission on Radiological Protection, Recommendations of the International Commission on Radiological Protection. Publication 103, Annals of ICRP Vol. 37 (2/4), Pergamon Press, Oxford; (2007) . |
[6] | Lee FKH, Yip CWY, Cheung FCH, Leung AKC. Dosimetric difference amongst 3 techniques: TomoTherapy, sliding-window intensity-modulated radiotherapy (IMRT), and RapidArc radiotherapy in the treatment of late-stage nasopharyngeal carcinoma (NPC). Med Dosim. (2014) ; 39: : 44-49. |
[7] | Lee TF, Ting HM, Chao PJ, Fang FM. Dual arc volumetric-modulated arc radiotherapy (VMAT) of nasopharyngeal carcinomas: a simultaneous integrated boost treatment plan comparison with intensity-modulated radiotherapies and single arc VMAT. Clin Oncol. (2012) ; 24: : 196-207. |
[8] | Lu SH, Cheng JCH, Kuo SH, Lee JJS, Volumetric modulated arc therapy for nasopharyngeal carcinoma: a dosimetric comparison with TomoTherapy and step-and-shoot IMRT. Radiother Oncol. (2012) ; 104: : 324-330. |
[9] | Tseng HC, Liu WS, Tsai HH, et al. Radiation dose for normal organs by helical tomotherapy for lung cancer. Appl Radiat Isot. (2015) ; 102: : 35-41. |
[10] | Chen LF, Tseng HC, Pan LK, et al. Evaluating environment radiations at Axesse linac undergoing NPC treatment of VMAT. Comput. Aided Surg. (2016) ; 21: (S1): 79-83. |
[11] | Chung Shan Medical University, Available from: http://english.csmu.edu.tw/bin/home.php. (2021) . |
[12] | Mutic S, Low D. Whole-body dose from tomotherapy delivery. Int J Radiat Oncol Biol Phys. (1998) ; 42: : 229-232. |
[13] | Betta DE, Fariselli L, Bergantin A, et al. Evaluation of the peripheral dose in stereotactic radiotherapy and radiosurgery treatments. Med Phys. (2010) ; 37: : 3587-3594. |


