
The value of multimodality MR in T staging evaluation after neoadjuvant therapy for rectal cancer
Abstract
BACKGROUND:
Surgery is the preferred treatment for rectal cancer, but surgical treatment alone sometimes does not achieve satisfactory results.
OBJECTIVE:
To explore the value of multimodal Magnetic Resonance (MR) images in evaluating T staging of rectal cancer after neoadjuvant therapy and to compare and analyze with pathological results.
METHODS:
This study retrospectively analyzed 232 patients with stage T3, T4 rectal cancer between January 1, 2017 and October 31, 2022. MR examination was performed within 3 days before surgery. Different MR sequences were used for mrT staging of rectal cancer after neoadjuvant therapy and compared with pathological pT staging. The accuracy of different MR sequences in evaluating T staging of rectal cancer was calculated, and the consistency between the two was analyzed by kappa test. The sensitivity, specificity, negative predictive value and positive predictive value of different MR sequences in evaluating rectal cancer invading mesorectal fascia after neoadjuvant therapy were calculated.
RESULTS:
A total of 232 patients with rectal cancer were included in the study. The accuracy of high-resolution T2 WI in evaluating T staging of rectal cancer after neoadjuvant therapy was 49.57%, and the Kappa value was 0.261. The accuracy of high-resolution T2WI combined with diffusion weighted imaging (DWI) in evaluating T staging of rectal cancer after neoadjuvant therapy was 61.64%, and the Kappa value was 0.411. The accuracy of high-resolution combined with DCE-MR images in evaluating T staging of rectal cancer after neoadjuvant therapy was 80.60%, and the Kappa value was 0.706. The sensitivity and specificity of high-resolution t2-weighted imaging (HR-T2WI) combined with dynamic contrast-enhancement magnetic resonance (DCE-MR) in evaluating the invasion of mesorectal fascia were 83.46% and 95.33%, respectively.
CONCLUSION:
Compared with HR-T2WI combined with DWI images for mrT staging of rectal cancer after neoadjuvant chemoradiotherapy (N-CRT), HR-T2WI combined with DCE-M has the highest accuracy in evaluating mrT staging of rectal cancer after neoadjuvant therapy (80.60%), and has a high consistency with pathological pT staging. It is the best sequence for T staging of rectal cancer after neoadjuvant therapy. At the same time, the sequence has high sensitivity and specificity in evaluating mesorectal fascia invasion, which can provide accurate perioperative information for the formulation of surgical plan.
1.Introduction
The incidence of rectal cancer increases year by year, with an average growth rate of about 2.2% [1]. Surgery is the preferred treatment for rectal cancer, but surgical treatment alone sometimes does not achieve satisfactory results. Locally advanced rectal cancer (LARC) has a local recurrence rate of 35–44% [2, 3]. Neoadjuvant chemoradiotherapy (N-CRT) has become an important method to improve the therapeutic effect of rectal cancer [4]. The National Comprehensive Cancer Network (NCCN) points out that patients with T3, T4 and locally unresectable rectal cancer need neoadjuvant therapy [5]. A number of studies have shown that neoadjuvant therapy can make local advanced rectal cancer retreat and downstage, reduce the proportion of postoperative recurrence and metastasis of rectal cancer, improve the complete resection rate and sphincter preservation rate, and even 3%–30% of rectal cancer patients can achieve pathologic complete response (pCR) after neoadjuvant therapy [6, 7].
Rectal cancer needs to be re-evaluated after neoadjuvant therapy. The reassessment of tumor staging after treatment determines whether patients can undergo surgical treatment and surgical design, which can significantly improve the surgical treatment effect and postoperative quality of life. At present, rectal MRI is the preferred method for imaging examination of RC local staging. In conventional MR imaging, it is difficult to distinguish the infiltration around rectal cancer from inflammatory edema and fibrosis after neoadjuvant therapy [8], and there are sometimes large errors in evaluation. The sensitivity and specificity of conventional MR examination sequence in evaluating the invasion of mesorectal fascia after rectal cancer N-CRT were also low [9, 10].
Since the routine application of MRI in rectal cancer staging, people have been exploring some new imaging techniques to further improve MRI-based rectal cancer staging. Multiparametric MRI means adding functional sequences to conventional protocols, namely dynamic contrast-enhanced magnetic resonance imaging (IVIM-DWI) and diffusion-weighted imaging (DCE-MRI). DCE-MRI can evaluate the microcirculation vascular characteristics of tumors, provide valuable parameters such as blood supply, invasiveness and microvascular density (MVD) of tumors, and may contribute to the re-staging of rectal tumors [11]. High resolution T2 weighted imaging (T2WI) and other technologies have significant advantages in the diagnosis of soft tissue lesions, which can bring more valuable information for the accurate diagnosis of lesions [12, 13]. In this study, MR functional imaging (DWI, DCE-MRI) and high-resolution T2WI were used to evaluate the re-staging of rectal cancer after neoadjuvant therapy, and the results were compared with pathological results to find the most accurate MR sequence to provide the basis for the formulation of surgical plan.
2.Materials and methods
2.1Study objects
Using a convenient sampling method, this study retrospectively analyzed the medical records of all patients with rectal cancer who met the inclusion and exclusion criteria between January 1, 2017 and October 31, 2022. All enrolled patients received neoadjuvant therapy and underwent surgery 6–7 weeks after the end of treatment. All enrolled patients before surgery. All enrolled patients underwent MR Examination 3 days before surgery. This study has been approved by the Medical Ethics Committee of our hospital.
Inclusion criteria: ⟀ Patients with rectal cancer who were first diagnosed with rectal cancer underwent rectal endoscopy and confirmed by biopsy as rectal adenocarcinoma. ⟁ Locally advanced rectal cancer at T3/T4 with or without perirectal lymph node metastasis. ⟂ No evidence of distant metastasis. ⟃ There is no anti-tumor therapy before neoadjuvant therapy. Exclusion criteria: ⟀ Patients with rectal cancer whose neoadjuvant therapy was interrupted due to various reasons. ⟁ Incomplete MR examination or clinical data. ⟂ Poorly evaluated MR images due to various causes such as motion or metal artifacts. ⟃ Patients who could not undergo surgical treatment after MR evaluation after neoadjuvant therapy.
2.2Study method
2.2.1Neoadjuvant therapy regimen
Radiotherapy regimen: Total dose of 45Gy, 5 days a week, a total of 5 weeks, daily radiation dose of 1.8Gy, radiotherapy orientation for a posterior, two lateral.
Chemotherapy regimen: Oxaliplatin, 60 mg/m2 weekly, intravenous injection; capecitabine, 825 mg/m2 daily, orally; a total of 5 weeks.
2.2.2Scanning equipment and scanning method
Scanning equipment: 1.5T magnetic resonance instrument (Avanto; Siemens Medical Systems, Erlangen, Germany), MR dedicated high pressure syringe (Accutron MR; MEDTRON, Germany).
Scanning method and sequence: MR examination before dinner after a liquid diet, fasting for at least 8 hours. Clean enema before examination. The patient was instructed to lie on the examination bed in a supine position with an advanced head. The upper limbs were naturally placed on both sides of the limbs. The ear plugs were implanted in both ears to reduce noise, and the patient was instructed to keep braking. The specific MR scan sequence and parameters are as follows: High-resolution Fast Spin Echo T2 Imaging Weighted imaging (HR-FSE T2WI) includes, repetition time/echo time (TR/TE): 5600/90 ms, slice thickness: 3 mm, interval: 05 mm, matrix: 224 * 320, field of view (FOV): 220 mm * 220 mm (axial).
DWI: Single-shot echo planner imaging (SS-EPI). TR/TE: 5000/70.6 ms, matrix: 224 * 135, visual field: 350 mm * 220 mm. Two groups of b value combination (0.800) s/mm2 and (0.1000) s/mm2, layer thickness: 5 mm, interval: 1.5 mm.
DCE-MRI: Volumetric interpolated breath-hold examination (VIBE), field of view (FOV): 360 mm * 360 mm (axial), slice thickness 4 mm, interval 0 mm. DCE-MRI Scan using MR dedicated high-pressure syringe, through the elbow vein injection paramagnetic contrast agent, injection dose of 0.2 ml/kg, rate of 2.5 ml/s, contrast agent after injection, immediately through the elbow vein injection of 20 ml saline, so that the contrast agent sufficient injection into the body circulation system. A total of double arterial phase, venous phase, delayed phase four scan. Double arterial phase scanning was performed 17 s after contrast injection, venous phase scanning 60 s later and delayed phase scanning 150 s later.
2.3Standard criteria
MR rectal cancer T staging criteria: All images were evaluated on SIEMENS Syngo.via (Siemens Medical Systems, Erlangen, Germany) post-processing workstation. Two radiologists with 6 and 7 years of experience in abdominal MR respectively evaluated the T staging of rectal cancer based on MR images of different sequences. When the opinions were not consistent, consensus was reached after negotiation. During the evaluation, the two radiologists knew the diagnosis of rectal cancer, but did not know the pathological staging. MR evaluation criteria for mesorectal fascia involvement: the shortest distance between the tumor and the mesentery is less than 1 mm. The reference standard for T staging of rectal cancer is the content of magnetic resonance T staging of rectal cancer in the 8th edition of the ‘American Joint Committee on Cáncer Staging Manual’. The specific T staging criteria are as follows: ⟀ mrT0: No abnormal signals were found in the rectal wall and surrounding structures; ⟁ mrTI-2: Tumor signal is not beyond the muscular layer or confined to the submucosa; ⟂ mrT3: tumor signal beyond the muscle layer, into the surrounding adipose tissue; ⟃ mrT4: Tumor signal significantly involved in the surrounding organs.
Pathological T staging criteria: Surgical specimens were first fixed with formalin for 24 hours, then cut along the longitudinal axis, embedded in paraffin, stained and observed under a microscope. The pathological staging of rectal cancer was based on the tumor node metastasis (TNM) staging of the American Joint Committee on Cancer. The staging criteria are as follows: ⟀ No primary tumor was found at pT0; ⟁ pTl tumor invasion submucosa; pT2 tumor invaded muscular layer; ⟂ pT3 tumor penetrated the muscular layer; ⟃ pT4 tumors invade other organs directly.
2.4Statistical methods
After N-CRT, T staging of rectal cancer was evaluated by different sequences (high-resolution T2WI, high-resolution T2WI combined with DWI, T2WI combined with DCE) and compared with pathological results. Kappa was used to test the consistency between mrT staging and pathological T staging, and the accuracy of different MR sequences in evaluating T staging was calculated. Kappa
3.Results
3.1Basic information and characteristics
From January 1,2017 to October 31,2022, there were 460 cases of rectal cancer confirmed by pathology and MR examination, 198 patients with T0-2 rectal cancer were excluded, 11 patients with locally advanced rectal cancer who did not reach the course of neoadjuvant therapy in patients with T3-4 rectal cancer were excluded, 19 patients with rectal cancer who could not be treated by surgery after neoadjuvant therapy were excluded, and 232 patients were finally enrolled in the study. The ratio of male to female was 3:1, including 32 cases of low colon cancer, 151 cases of median rectal cancer, 49 cases of high rectal cancer, 181 cases of mrT3 stage and 51 cases of mrT4 stage before treatment.
3.2Consistency analysis of multimodal MR image mrT staging and pathological pT staging
The consistency analysis of mrT staging after N-CRT and pathological pT staging of rectal cancer by HR-T2WI was shown in Table 1, and the accuracy of mrT staging after N-CRT was 49.57%. There were 110 cases MR staging higher than pathological staging., mainly in ypT 1-2 and ypT3 (Fig. 1). Kappa value was 0.261.
Table 1
HR-T2W1 to evaluate the consistency of T stage and case results after neoadjuvant therapy
| Pathology | Total | |||||
|---|---|---|---|---|---|---|
| pT0 | pT1-2 | pT3 | pT4 | |||
| HR-T2WI | mrT0 | 4 | 1 | 0 | 0 | 5 |
| mrT1-2 | 6 | 48 | 1 | 0 | 55 | |
| mrT3 | 0 | 45 | 51 | 5 | 101 | |
| mrT4 | 0 | 12 | 47 | 12 | 71 | |
| Total | 10 | 106 | 99 | 17 | 232 | |
Note: HR-T2WI: high-resolution t2-weighted imaging.
Figure 1.
MR image after neoadjuvant therapy. A 64-year-old female presented with hematochezia for 3 months. Postoperative pathological stage was T2. Figure 1B and D are local enlarged images of Fig. 1A and C, respectively. Figure 1A–B: The transverse axial HR-T2WI showed uneven thickening of the posterior rectal wall, clear serosa surface, and strip-like high signal in the right anterior wall. According to the HR-T2WI image, the staging was mrT3. Figure 1C–D: DCE-MR showed a vascular shadow in the right anterior wall of the rectum and a slight enhancement of the thickened posterior wall of the rectum. According to the DCE-MR image, the staging was mrT2.
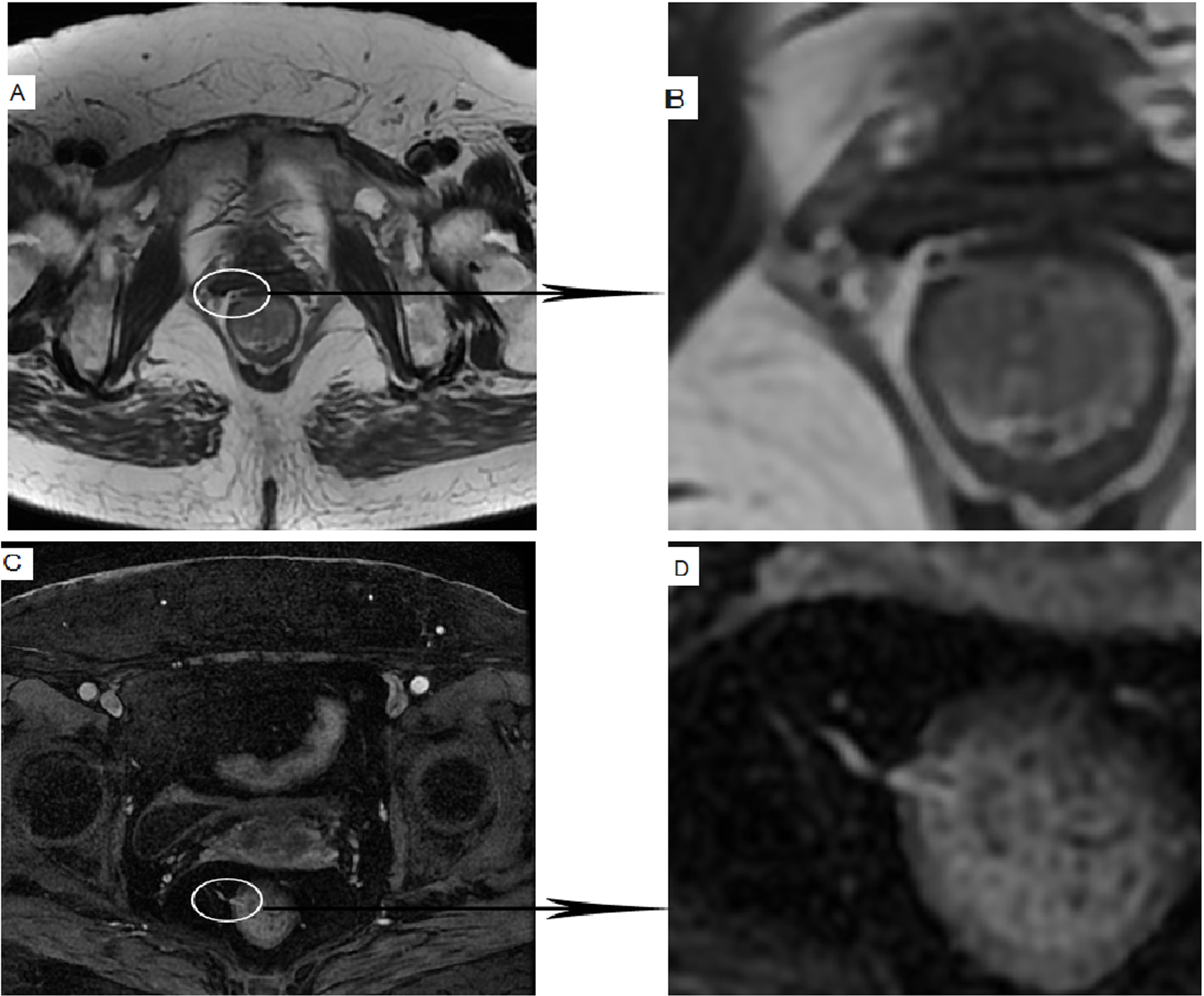
Table 2
HR-T2WI combined with DWI to evaluate the consistency of T staging and case results after neoadjuvant therapy
| Pathology | Total | |||||
|---|---|---|---|---|---|---|
| pT0 | pT1-2 | pT3 | pT4 | |||
| HR-T2WI combined with DWI | mrT0 | 3 | 0 | 0 | 0 | 3 |
| mrT1-2 | 7 | 66 | 8 | 0 | 81 | |
| mrT3 | 0 | 28 | 61 | 4 | 93 | |
| mrT4 | 0 | 12 | 30 | 13 | 55 | |
| Total | 10 | 106 | 99 | 17 | 232 | |
Note: HR-T2WI: high-resolution t2-weighted imaging. DWI: diffusion weighted imaging.
The consistency analysis of HR-T2WI combined with DWI images for mrT staging and pathological pT staging of rectal cancer after N-CRT is shown in Table 2. The accuracy of high-resolution T2WI combined with DWI in evaluating mrT staging after N-CRT was 61.64%. There were 77 cases MR staging higher than pathological staging., mainly in ypT 1-2 and ypT3 (Fig. 1), with a Kappa value of 0.411.
The consistency analysis of HR-T2WI combined with DCE for mrT staging and pathological pT staging of rectal cancer after N-CRT is shown in Table 3. The accuracy of HR-T2WI combined with DCE for mrT staging after N-CRT was 80.60%. There were33 cases MR staging higher than pathological staging., mainly in ypT 1-2 and ypT3 (Fig. 1). The Kappa value was 0.706, and the consistency was good.
Table 3
HR-T2WI combined with DCE to evaluate the consistency of T staging and case results after neoadjuvant therapy
| Pathology | Total | |||||
|---|---|---|---|---|---|---|
| pT0 | pT1-2 | pT3 | pT4 | |||
| HR-T2WI combined with DCE | mrT0 | 6 | 0 | 0 | 0 | 6 |
| mrT1-2 | 4 | 86 | 6 | 0 | 96 | |
| mrT3 | 0 | 15 | 84 | 6 | 106 | |
| mrT4 | 0 | 5 | 9 | 11 | 25 | |
| Total | 10 | 106 | 99 | 17 | 232 | |
Note: HR-T2WI: high-resolution t2-weighted imaging. DCE: dynamic contrast-enhancement magnetic resonance.
3.3Multimodal MR image evaluation of rectal cancer invading mesorectal fascia
The mesorectal fascia showed a circular low signal ring on T2WI (Fig. 1). The shortest distance between the tumor and the mesentery was less than 1 mm, which was diagnosed as rectal fascia invasion. Pathological results showed that mesorectal fascia was invaded in 25 cases (Fig. 2). The results of different MR sequences in the diagnosis of mesorectal fascia invasion are shown in Table 4. HR-T2WI combined with DCE had higher sensitivity (83.46%) and specificity (95.33%).
Table 4
Multimodal MR image evaluation of rectal cancer invading mesorectal fascia
| HR-T2W1 | HR-T2WI combined with DWI | HR-T2WI combined with DCE | |
|---|---|---|---|
| Sensitivity | 52.71% | 68.16% | 83.46% |
| Specificity | 59.38% | 76.81% | 95.33% |
| Positive prediction value | 30.68% | 54.78% | 17.67% |
| Negative prediction value | 21.07% | 30.47% | 69.21% |
Note: HR-T2WI: high-resolution t2-weighted imaging. DWI: diffusion weighted imaging. DCE: dynamic contrast-enhancement magnetic resonance.
Figure 2.
MR images after neoadjuvant therapy. A 71-year-old male presented with bloody and emaciation stool for half a year. Pathological examination revealed invasion of mesorectal fascia. Figure 2A axial T2WI showed that the rectal wall was unevenly thickened, and the limitation was prominent outside the contour of the intestinal wall. The T2 signal of the thickened intestinal wall was slightly higher, and the internal spotted higher T2 signal was visible. The mesorectal fascia (white arrow) was seen around it. According to the HR-T2WI image, the tumor did not invade the mesorectal fascia. Figure 2B axial DWI showed increased signal in the thickened rectal wall. According to HR-T2WI combined with DWI, the tumor did not invade the mesorectal fascia. Figure 2C–D axial and coronal DCE-MR showed that the thickened rectal wall was significantly thickened and significantly enhanced. The right side of the rectum was accompanied by patchy enhancement. The enhancement mode was consistent with the main body of the tumor. Combined with HR-T2 WI, it was suggested that the tumor invaded the mesorectal fascia.
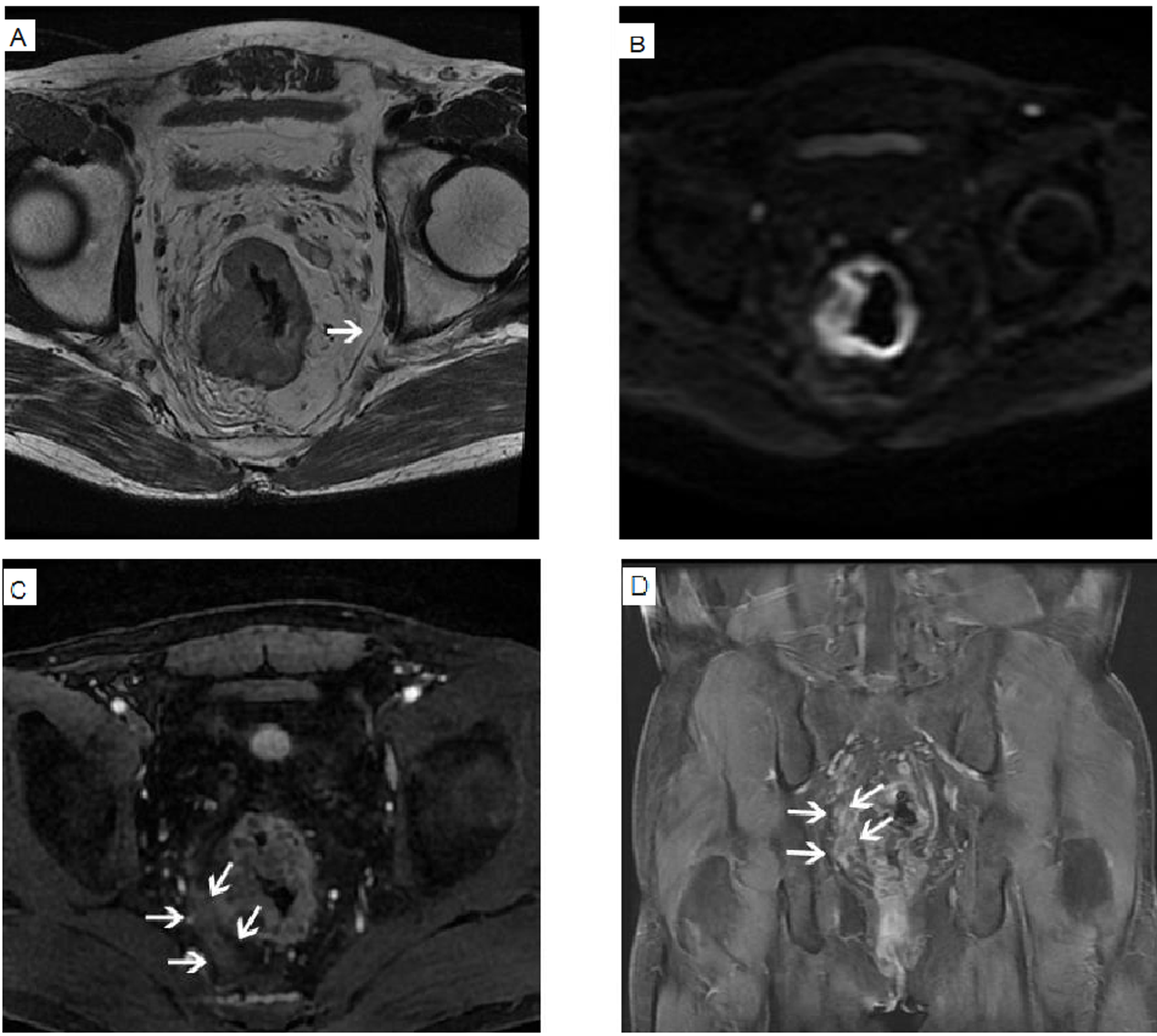
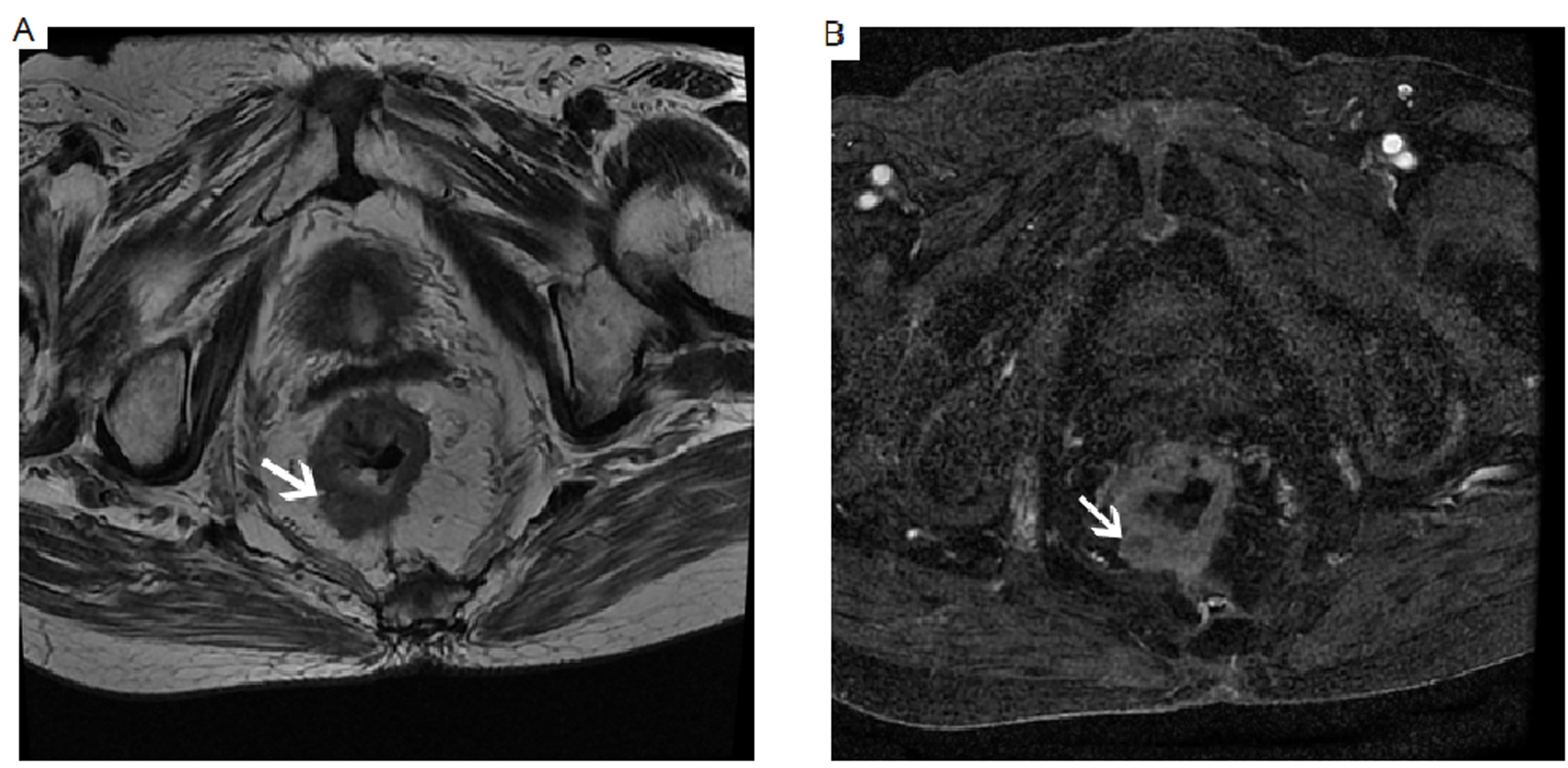
Figure 3.
MR images after neoadjuvant therapy. Woman, 71, bloody stool June. Figure 3A: After neoadjuvant therapy, small patchy slightly longer T2 signal was seen, and the boundary with the surrounding residual tumor was blurred. There was a round unenhanced lesion, which was pathologically confirmed as a mucous lake. HR-T2WI image showed that Fig. 3B: DCE-MR showed nodular thickening of the rectal wall, and the image showed obvious enhancement of the thickened intestinal wall, with round unenhanced lesions, which was pathologically confirmed as mucus lake.
4.Discussion
Although neoadjuvant therapy for rectal cancer can reduce the tumor burden to varying degrees, reduce the tumor stage, reduce the local recurrence rate after rectal cancer surgery, and improve the resection rate and 5-year survival rate of surgery, the inflammatory response, fibrosis, and mucus-like changes after neoadjuvant therapy for rectal cancer (Fig. 3) pose a huge challenge to the evaluation of re-staging after neoadjuvant therapy for rectal cancer.
Huh et al. [14] analyzed the T staging of 219 rectal cancer patients after neoadjuvant therapy by T2WI, and compared it with pathological results. The results showed that the accuracy of T2WI in evaluating rectal cancer staging after neoadjuvant therapy was poor. Although the specificity can reach 85%, the sensitivity is only 45%. In this study, the accuracy of HR-T2WI in the re-staging of rectal cancer after neoadjuvant therapy was 49.57%, and 115 patients (49.56%) had excessive staging, which was similar to the previous study. There are still some deficiencies in T2WI evaluation of N-CRT rectal cancer re-staging. Excessive staging of rectal cancer patients is mainly concentrated in pTl-2 and pT3. The main reason for the decrease of T staging accuracy of HR-T2 WI after N-CRT for rectal cancer is that the inflammatory response, fibrosis, mucus-like changes and other factors accompanied by neoadjuvant therapy increase the difficulty of distinguishing the depth of tumor invasion, and the inflammatory edema and infiltration around the tumor on T2 WI show similar slightly higher signal [15]. Even with the application of high-field high-resolution magnetic resonance T2-weighted sequence, it is still difficult to distinguish the inflammatory response and peritumoral infiltration caused by neoadjuvant therapy. MR examination 6–7 weeks after the end of neoadjuvant therapy, there will still be some patients with inflammatory response is not fully absorbed. This study showed that the kappa coefficient of high-resolution T2WI in evaluating the consistency of mrT staging and pathological pT staging after neoadjuvant chemotherapy for rectal cancer was only 0.261, and the consistency was poor.
DWI makes up for the deficiency of T2WI in evaluating the re-staging of rectal cancer after N-CRT only from morphology. The histopathological features of rectal cancer are that the number of atypical cells is large, they have a large volume and are closely arranged, which leads to a decrease in the intercellular space and the diffusion of water molecules is limited [16]. The rectal cancer showed characteristic high signal on DWI, and the normal intestinal wall showed low signal. The signal difference between the two was obvious. This study found that HR-T2WI combined with DWI sequence for rectal cancer after neoadjuvant therapy T staging, the effect is still unsatisfactory. The reasons are as follows: Firstly, due to the existence of T2 relaxation process, the distance between EPI echoes and the length of echo chain are relatively short, so the signal-to-noise ratio and spatial resolution of DWI images are poor [17]; Secondly, due to the use of fast switching coding gradient and unique phase coding method, the magnetic field uniformity is very high, and it is easy to be affected by equipment and other environmental problems during scanning. Especially when the rectal cancer patients are not fully prepared before the examination and there is a large amount of intestinal air in the intestine, the magnetic sensitive high signal artifacts are prone to occur [18]. Thirdly, for inexperienced physicians, it is easy to put this unreal high signal, wrongly judged as residual tumor of rectal cancer. Especially when this high signal artifact is superimposed on the fibrosis formed after neoadjuvant therapy, it is more likely to cause excessive staging of rectal cancer after neoadjuvant therapy. Fourthly, the sampling time is longer, which will lead to excessive attenuation of the T2 signal and reduce the signal-to-noise ratio of the reconstructed image. In addition, due to the limitation of DWI resolution, for a small amount of extraintestinal tumor infiltration, the signal change on DWI is not obvious, and it will not show characteristic high signal [19], in this case, the staging will be too light. In this study, there were 8 cases of ypT3 stage rectal cancer due to the surrounding tumor tissue infiltration is lighter (Fig. 2), retrospective analysis of the HR-T2WI and DWI found that the 8 cases of rectal cancer patients although in T2WI appeared patchy slightly low signal shadow, but the corresponding DWI, the signal is not high, so that the two imaging experts mistaken these patchy high signal shadow as inflammatory edema after neoadjuvant therapy.
Although DWI sequence is more sensitive to detect rectal lesions than conventional MR sequence, these reasons lead to HR-T2WI combined with DWI did not show a significant advantage in assessing rectal cancer re-staging after neoadjuvant chemotherapy compared with HR-T2WI alone. At the same time, due to the low spatial resolution and signal-to-noise ratio of DWI, the structure of each layer of the rectal wall cannot be accurately distinguished, so the application of DWI alone has little significance for the T staging of rectal cancer after N-CRT.In this study, DWI was not used alone to evaluate the T staging of rectal cancer after N-CRT, but DWI was used as a supplementary sequence of T2WI to evaluate the T staging of rectal cancer after N-CRT.
Few studies have mentioned the application of DCE-MR images in evaluating T staging of rectal cancer after N-CRT. In this study, we mainly used the degree of enhancement of the tumor on DCE-MR images to determine the depth of tumor invasion, and then evaluate the T stage of rectal cancer after treatment. In this study, HR-T2WI combined with DCE-MR sequence was used to evaluate the re-staging of rectal cancer after neoadjuvant therapy. The effect was significantly better than HR-T2WI, HR-T2WI combined with DWI. During the growth of rectal cancer, itself and its nutrient vessels secrete vascular growth factors, which can promote tumor capillary formation, and the capillary endothelial permeability of malignant tumors increases [13]. After injection of contrast agents, the parenchyma of the tumor is significantly enhanced, which is significantly compared with the surrounding intestinal wall and adjacent tissues. After N-CRT, rectal cancer has different degrees of tumor response, and the number of internal capillaries is less than before. Although the degree of enhancement of the residual tumor is significantly lower than that of the tumor before neoadjuvant therapy, the enhancement mode of the residual tumor is still significantly different from that of the normal intestinal wall, so that the T staging of rectal cancer after N-CRT can be evaluated relatively correctly according to DCE-MR images. The identification of perirectal infiltration and inflammatory edema after neoadjuvant therapy has an important impact on the evaluation of T staging of rectal cancer after N-CRT. Although the surrounding infiltration of rectal cancer and the inflammatory edema after neoadjuvant therapy will show different degrees of enhancement, the enhancement methods of the two are significantly different on DCE-MR images [15]. The enhancement of the infiltration around rectal cancer is similar to that of the primary lesion, and the enhancement of inflammatory edema is basically delayed enhancement. Inflammatory edema and infiltration around rectal cancer are sometimes difficult to distinguish on T2WI and DWI, and it is easier to distinguish on DCE-MR images according to their different enhancement methods. In addition, DCE-MR images have certain diagnostic value for the identification of mucoid changes and residual cancer after N-CRT. On T2WI, myxoid lesions and residual cancer lesions showed similar slightly higher signal or equal signal (Fig. 3), which was difficult to distinguish. Although DWI can theoretically identify the two according to different signals, DWI generally has geometric distortion and low spatial resolution. In addition, the area of myxoid change is generally small and T2 penetration effect, so it is still difficult to identify the two by DWI in clinical work. On DCE-MR images, the mucus tissue was not enhanced, and the residual tumor tissue after N-CRT had different degrees of enhancement (Fig. 3B) [20].
The distance between the tumor and the mesorectal fascia determines whether the mesorectal fascia is invaded, and it is also one of the most important risk factors for postoperative recurrence of rectal cancer [21]. Currently, the criterion for mesorectal fascia involvement on MR is that the tumor is less than 1 mm from the mesorectal fascia. Taylor et al. [22] retrospectively analyzed the MR images of 374 patients with rectal cancer to study the correlation between the different distances between the tumor and the mesorectal fascia and the local recurrence of rectal cancer after surgery. Multivariate analysis showed that the distance between the rectal cancer and the mesorectal fascia less than or equal to 1 mm was an independent risk factor for postoperative recurrence of rectal cancer regardless of neoadjuvant therapy. In another prospective study with a cut-off point of 1 mm, the accuracy of MR measurement of the distance between the tumor and the mesorectal fascia to determine mesorectal fascia involvement was 88% [23]. Some literatures have reported that for rectal cancer patients without neoadjuvant therapy, MRI examination can accurately measure the distance between the tumor and the mesorectal fascia, so as to relatively accurately evaluate the invasion of rectal cancer to the mesorectal fascia. However, inflammatory edema and fibrosis after neoadjuvant therapy, especially neoadjuvant radiotherapy, greatly affect the measurement of the distance between the tumor and the mesorectal fascia. The results of this study showed that the sensitivity and specificity of HR-T2WI combined with DCE-MR images in evaluating the involvement of mesorectal fascia were significantly higher than those of HR-T2WI and HR-T2WI combined with DWI.
At present, the pathological and imaging diagnosis of tumors mainly depends on the visual assessment of pathologists and radiologists, which is susceptible to factors such as doctors ’ own subjectivity and visual perception differences, which may lead to inconsistent clinical diagnosis. Compared with traditional manual reading judgment, artificial intelligence (AI) has significant advantages in fine image recognition and rapid and accurate interpretation [24]. By suggesting positive lesion areas and excluding negative cases, it can greatly improve the diagnostic efficiency of doctors and reduce repetitive work [25, 26]. Lou et al. [27] developed a CNN-based upper gastrointestinal tract tumor endoscopic AI-assisted diagnostic system (GRAIDS) to help screen and early diagnose upper gastrointestinal tumors. The diagnostic accuracy can reach the level of expert endoscopists. The Al diagnostic system developed by McKinney et al. [28] based on breast X-ray examination of large sample size cohort can further reduce the false positive rate and false negative rate of breast cancer screening, and the diagnostic accuracy of AI system is higher than that of all 6 radiologists. Paige Prostate software (Paige.AI, USA) is an AI software that is one of the classic cases of clinical application. In a pathological AI diagnosis study based on more than 40,000 digital pathological images of more than 15,000 patients in 44 countries/regions [29], the AUC of Paige Prostate algorithm in the diagnosis of prostate cancer, basal cell carcinoma and axillary lymph node metastasis breast cancer reached more than 0.98. In addition, the Al study has shown preliminary advantages in ultrasound screening of breast cancer [30], enhanced CT differential diagnosis of liver lesions [31], differential diagnosis of benign and malignant nasopharyngeal masses [32], and bladder cancer screening under cystoscopy [33]. The AI model might aid less experienced physicians and radiologists in improving their diagnostic performance for the localisation of nasal bone fractures on CT images [34]. Artificial intelligence will be our next research focus.
There are still some limitations in this study. Firstly, due to the relatively small number of research samples, more research subjects need to be included in future studies to obtain more and more reliable evidence to prove the effectiveness of DCE-MR in evaluating T staging of rectal cancer after N-CRT. Secondly, sample selection bias, after neoadjuvant therapy is still part of the patient is not suitable for surgical treatment, no pathological results. Finally, this study only analyzed the value of multimodal MR for T staging after neoadjuvant therapy, but not for lymph node staging. However, this is due to the limitation of objective conditions at this stage, and the lymph nodes of postoperative specimens are difficult to correspond to the lymph nodes on MR images.
5.Conclusion
DCE-MR has the highest accuracy in evaluating T staging of rectal cancer after N-CRT, and has a high consistency with pathological T staging. It is the best sequence for T staging of rectal cancer after CRT. It has high accuracy, sensitivity and specificity in evaluating the invasion of mesorectal fascia, and can provide accurate perioperative information for the formulation of surgical plan.
Ethics statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the Second Hospital of Qinhuangdao. Informed consent was signed by all participants in this study.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Competing interests
None of the authors has any personal, financial, commercial, or academic conflicts of interest.
Funding
Not applicable.
Author contributions
Conception and design of the work: LB; Data collection: SC, ZXY, LLY, LS, and MHC; Supervision: LB and MHC; Analysis and interpretation of the data: SC, ZXY, LLY, LS, and MHC; Statistical analysis: LB and MHC; Drafting the manuscript: LB. All authors critically revised the manuscript and approved the final version.
Acknowledgments
Not applicable.
References
[1] | Yan YL, Ma XW, Tan L, et al. Therapeutic effects of neoadjuvant chemoradiotherapy on locally advanced rectal cancer. Journal of Xi’an Jiaotong University (Medical Sciences). (2018) ; 39: (3): 442-446. (in Chinese). doi: 10.7652/jdyxb201803030. |
[2] | Moreno CC, Sullivan PS, Kalb BT, et al. Magnetic resonance imaging of rectal cancer: Staging and restaging evaluation. Abdom Imaging. (2015) Oct; 40: (7): 2613-29. doi: 10.1007/s00261-015-0394-z. |
[3] | Hu MH, Huang RK, Zhao RS, et al. Short-term efficacy of neoadjuvant chemoradiotherapy combined with laparoscopy in the treatment of low rectal cancer. Chinese Journal for Clinicians. (2014) ; 6: : 45-49. (in Chinese). doi: 10.3969/j.issn.1008-1089.2014.06.017. |
[4] | Xu HX. Effect of neoadjuvant chemoradiotherapy on rectal cancer patients. Contemporary Medicine Forum. (2014) ; 10: : 265-267. (in Chinese). doi: 10.3969/j.issn.2095-7629.2014.10.232. |
[5] | Han KS, Sohn DK, Kim DY, et al. Endoscopic criteria for evaluating tumor stage after preoperative chemoradiation therapy in locally advanced rectal cancer. Cancer Res Treat. (2016) Apr; 48: (2): 567-73. doi: 10.4143/crt.2015.195. |
[6] | Lee SR. Factors influencing clinical cancer stage in women patients with rectal cancer. Technol Health Care. (2014) ; 22: (3): 497-503. doi: 10.3233/THC-140809. PMID: 24763204. |
[7] | Wu A, Li Y. Application status, controversy and challenge of neoadjuvant immunotherapy for colorectal cancer. Chinese Journal of Gastrointestinal Surgery. (2022) ; 25: (03): 185-192. doi: 10.3760/cma.j.cn441530-20211219-00510. |
[8] | Juresic E, Liney GP, Rai R, et al. An assessment of set up position for MRI scanning for the purposes of rectal cancer radiotherapy treatment planning. J Med Radiat Sci. (2018) Mar; 65: (1): 22-30. doi: 10.1002/jmrs.266. |
[9] | Sudarski S, Henzler T, Floss T, et al. Variability and Reproducibility of 3rd-generation dual-source dynamic volume perfusion CT Parameters in Comparison to MR-perfusion Parameters in Rectal Cancer. Sci Rep. (2018) May 2; 8: (1): 6868. doi: 10.1038/s41598-018-25307-w. |
[10] | Atkinson SJ, Daly MC, Midura EF, et al. The effect of hospital volume on resection margins in rectal cancer surgery. J Surg Res. (2016) Jul; 204: (1): 22-8. doi: 10.1016/j.jss.2016.04.041. |
[11] | Guo C. The effect of dynamic enhanced MRI and DWI in evaluating the short-term prognosis of liver malignant tumor after microwave ablation. Chinese Medical Innovations. (2022) ; 19: (35): 174-179. |
[12] | Li Y, Ding HL. Comparative analysis of the value of spiral CT and MRI in the diagnosis of preoperative T stage of rectal cancer. Zhejiang J Traumat Surg. (2020) ; 25: (3): 575-577. (in Chinese). doi: 10.3969/j.issn.1009-7147.2020.03.088. |
[13] | Kang DH, Zhang JQ, Zhao LY, et al. Application of Multimodal MR Imaging in Preoperative TN Staging of Rectal. Zhejiang Medical Education. (2021) ; 20: (1): 54-56. (in Chinese). doi: 10.3969/j.issn.1672-0024.2021.01.020. |
[14] | Huh JW, Kim HC, Lee SJ, et al. Diagnostic accuracy and prognostic impact of restaging by magnetic resonance imaging after preoperative chemoradiotherapy in patients with rectal cancer. Radiother Oncol. (2014) Oct; 113: (1): 24-8. doi: 10.1016/j.radonc.2014.08.023. |
[15] | Cao W. Application of multi-parameter magnetic resonance imaging and omics in evaluating the efficacy of neoadjuvant chemoradiotherapy for rectal mucinous adenocarcinoma. South China University of Technology. (2021) . doi: 10.27151/d.cnki.ghnlu.2021.000202. |
[16] | Peng Y, Li Z, Tang H, et al. Comparison of reduced field-of-view diffusion-weighted imaging (DWI) and conventional DWI techniques in the assessment of rectal carcinoma at 3.0T: Image quality and histological T staging. J Magn Reson Imaging. (2018) Apr; 47: (4): 967-975. doi: 10.1002/jmri.25814. |
[17] | Huh JW, Park YA, Jung EJ, et al. Accuracy of endorectal ultrasonography and computed tomography for restaging rectal cancer after preoperative chemoradiation. J Am Coll Surg. (2008) Jul; 207: (1): 7-12. doi: 10.1016/j.jamcollsurg.2008.01.002. |
[18] | Chen Y, Wu B, Liu H, et al. Feasibility study of dual parametric 2D histogram analysis of breast lesions with dynamic contrast-enhanced and diffusion-weighted MRI. J Transl Med. (2018) Nov 23; 16: (1): 325. doi: 10.1186/s12967-018-1698-x. |
[19] | Petrillo A, Fusco R, Granata V, et al. MR imaging perfusion and diffusion analysis to assess preoperative Short Course Radiotherapy response in locally advanced rectal cancer: Standardized Index of Shape by DCE-MRI and intravoxel incoherent motion-derived parameters by DW-MRI. Med Oncol. (2017) Nov 18; 34: (12): 198. doi: 10.1007/s12032-017-1059-2. |
[20] | Horvat N, Carlos Tavares Rocha C, Clemente Oliveira B, Petkovska I, Gollub MJ. MRI of rectal cancer: Tumor staging, imaging techniques, and management. Radiographics. (2019) Mar-Apr; 39: (2): 367-387. doi: 10.1148/rg.2019180114. Epub 2019 Feb 15. PMID: 30768361; PMCID: PMC6438362. |
[21] | Mathur P, Smith JJ, Ramsey C, et al. Comparison of CT and MRI in the pre-operative staging of rectal adenocarcinoma and prediction of circumferential resection margin involvement by MRI. Colorectal Dis. (2003) Sep; 5: (5): 396-401. doi: 10.1046/j.1463-1318.2003.00537.x. |
[22] | Taylor FG, Quirke P, Heald RJ, et al. One millimetre is the safe cut-off for magnetic resonance imaging prediction of surgical margin status in rectal cancer. Br J Surg. (2011) Jun; 98: (6): 872-9. doi: 10.1002/bjs.7458. |
[23] | MERCURY Study Group. Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: Prospective observational study. BMJ. (2006) Oct 14; 333: (7572): 779. doi: 10.1136/bmj.38937.646400.55. |
[24] | Artificial intelligence for medical image processing. Technol Health Care. (2021) ; 29: (2): 361. doi: 10.3233/THC-202658. PMID: 33361623. |
[25] | Bi WL, Hosny A, Schabath MB, Giger ML, Birkbak NJ, Mehrtash A, Allison T, Arnaout O, Abbosh C, Dunn IF, Mak RH, Tamimi RM, Tempany CM, Swanton C, Hoffmann U, Schwartz LH, Gillies RJ, Huang RY, Aerts HJWL. Artificial intelligence in cancer imaging: Clinical challenges and applications. CA Cancer J Clin. (2019) Mar; 69: (2): 127-157. doi: 10.3322/caac.21552. Epub 2019 Feb 5. PMID: 30720861; PMCID: PMC6403009. |
[26] | Niazi MKK, Parwani AV, Gurcan MN. Digital pathology and artificial intelligence. Lancet Oncol. (2019) May; 20: (5): e253-e261. doi: 10.1016/S1470-2045(19)30154-8. PMID: 31044723; PMCID: PMC8711251. |
[27] | Luo H, Xu G, Li C, He L, Luo L, Wang Z, Jing B, Deng Y, Jin Y, Li Y, Li B, Tan W, He C, Seeruttun SR, Wu Q, Huang J, Huang DW, Chen B, Lin SB, Chen QM, Yuan CM, Chen HX, Pu HY, Zhou F, He Y, Xu RH. Real-time artificial intelligence for detection of upper gastrointestinal cancer by endoscopy: A multicentre, case-control, diagnostic study. Lancet Oncol. (2019) Dec; 20: (12): 1645-1654. doi: 10.1016/S1470-2045(19)30637-0. Epub 2019 Oct 4. PMID: 31591062. |
[28] | McKinney SM, Sieniek M, Godbole V, Godwin J, Antropova N, Ashrafian H, Back T, Chesus M, Corrado GS, Darzi A, Etemadi M, Garcia-Vicente F, Gilbert FJ, Halling-Brown M, Hassabis D, Jansen S, Karthikesalingam A, Kelly CJ, King D, Ledsam JR, Melnick D, Mostofi H, Peng L, Reicher JJ, Romera-Paredes B, Sidebottom R, Suleyman M, Tse D, Young KC, De Fauw J, Shetty S. International evaluation of an AI system for breast cancer screening. Nature. (2020) Jan; 577: (7788): 89-94. doi: 10.1038/s41586-019-1799-6. Epub 2020 Jan 1. Erratum in: Nature. 2020 Oct; 586(7829): E19. PMID: 31894144. |
[29] | Campanella G, Hanna MG, Geneslaw L, Miraflor A, Werneck Krauss Silva V, Busam KJ, Brogi E, Reuter VE, Klimstra DS, Fuchs TJ. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat Med. (2019) Aug; 25: (8): 1301-1309. doi: 10.1038/s41591-019-0508-1. Epub 2019 Jul 15. PMID: 31308507; PMCID: PMC7418463. |
[30] | Shen Y, Shamout FE, Oliver JR, Witowski J, Kannan K, Park J, Wu N, Huddleston C, Wolfson S, Millet A, Ehrenpreis R, Awal D, Tyma C, Samreen N, Gao Y, Chhor C, Gandhi S, Lee C, Kumari-Subaiya S, Leonard C, Mohammed R, Moczulski C, Altabet J, Babb J, Lewin A, Reig B, Moy L, Heacock L, Geras KJ. Artificial intelligence system reduces false-positive findings in the interpretation of breast ultrasound exams. Nat Commun. (2021) Sep 24; 12: (1): 5645. doi: 10.1038/s41467-021-26023-2. PMID: 34561440; PMCID: PMC8463596. |
[31] | Yasaka K, Akai H, Abe O, Kiryu S. Deep learning with convolutional neural network for differentiation of liver masses at dynamic contrast-enhanced CT: A preliminary study. Radiology. (2018) Mar; 286: (3): 887-896. doi: 10.1148/radiol.2017170706. Epub 2017 Oct 23. PMID: 29059036. |
[32] | Li C, Jing B, Ke L, Li B, Xia W, He C, Qian C, Zhao C, Mai H, Chen M, Cao K, Mo H, Guo L, Chen Q, Tang L, Qiu W, Yu Y, Liang H, Huang X, Liu G, Li W, Wang L, Sun R, Zou X, Guo S, Huang P, Luo D, Qiu F, Wu Y, Hua Y, Liu K, Lv S, Miao J, Xiang Y, Sun Y, Guo X, Lv X. Development and validation of an endoscopic images-based deep learning model for detection with nasopharyngeal malignancies. Cancer Commun (Lond). (2018) Sep 25; 38: (1): 59. doi: 10.1186/s40880-018-0325-9. PMID: 30253801; PMCID: PMC6156962. |
[33] | Wu S, Chen X, Pan J, Dong W, Diao X, Zhang R, Zhang Y, Zhang Y, Qian G, Chen H, Lin H, Xu S, Chen Z, Zhou X, Mei H, Wu C, Lv Q, Yuan B, Chen Z, Liao W, Yang X, Chen H, Huang J, Lin T. An artificial intelligence system for the detection of bladder cancer via cystoscopy: A multicenter diagnostic study. J Natl Cancer Inst. (2022) Feb 7; 114: (2): 220-227. doi: 10.1093/jnci/djab179. PMID: 34473310; PMCID: PMC8826636. |
[34] | Yang C, Yang L, Gao GD, Zong HQ, Gao D. Assessment of artificial intelligence-aided reading in the detection of nasal bone fractures. Technol Health Care. (2022) Nov 17. doi: 10.3233/THC-220501. Epub ahead of print. PMID: 36442167. |


