
Analysis of the application effect of continuous care for patients with viral keratitis
Abstract
BACKGROUND:
In recent years, the incidence of viral keratitis has been on the rise.
OBJECTIVE:
This study explored the application effect of continuous care for patients with viral keratitis.
METHODS:
A total of 148 patients with viral keratitis admitted to the ophthalmology department of the authors’ hospital from January 2019 to December 2020 were selected and divided into the observation group and the control group via the random number table method, with 74 cases in each group. Continuous care was conducted following routine discharge guidance for patients in the observation group, while routine discharge guidance only was provided for the control group. The patients in both groups were continuously observed for one year. The medication compliance, return visit rate, recurrence rate, nursing satisfaction, and quality of life between the two groups were compared and analyzed after one year.
RESULTS:
The medication compliance was higher in the observation than in the control group and the difference was statistically significant (
CONCLUSION:
Continuous care had a good application effect on patients with viral keratitis, which could potentially effectively improve medication compliance and the rate of return visits, reduce recurrence rate, and improve patient satisfaction and their quality of life. Accordingly, the results of this study present high clinical value.
1.Introduction
In recent years, with the development of society, the increase in life pressures, and the application of computers, the incidence of viral keratitis has been on the rise. The statistical results of the national multi-center epidemiological survey, “Research on the Social Harm and Intervention Strategies of Infectious Keratopathy in China” (Project of the Chinese Academy of Engineering 2009–77) revealed that the prevalence of bacterial, fungal, and viral keratitis was 0.075%, 0.007%, and 0.110%, respectively, among which viral keratitis ranked first [1]. Viral keratitis, as a common ophthalmic disease, is caused by a variety of viruses and is accompanied by ocular symptoms, e.g., lacrimation and photophobia. The condition has a long treatment duration and can easily recur, thereby seriously impacting vision and presenting the risk of blindness. In most cases, the lack of medication and inappropriate treatment can exacerbate inflammation and prolong healing, when the virus enters the incubation period, which may again stimulate the inflammatory process and cause keratitis to relapse [2]. As such, improving compliance and achieving active cooperation among patients with treatment is an important guarantee for achieving improvement in clinical therapeutic effects.
In general, patient discharge means the end of treatment and the end of nurse-patient relationship [3]. In recent years, the clinical application of the hospital-based continuous care model has greatly improved the therapeutic follow-up of patients after discharge and has been widely adopted with good outcomes [4]. Since the 1990s, more and more attention has been paid to the application of continuous care in discharged patients in developed countries. To date, professional nursing teams have been established in these countries with extensive research contents and relatively mature continuous care nursing model [5]. However, the continuous care in China is still at its initial stage, and no mature management mechanism has been established yet [3]. There are not many reports on the continuous care for discharged ophthalmic patients in China, and less than 10 relevant literatures were retrieved from major Chinese databases such as CNKI, Wanfang and Vip database during 2005–2015 [6]. Therefore, the improvement of continuous ophthalmic care needs to cause our attention.
This study through the continuous nursing intervention of viral keratitis patients, after the discharge of nursing intervention as a research focus, establish the standardized continuous care team, develop unified scientific implementation plan, not only to provide direct nursing services for viral keratitis patients after discharge, more important is to help patients and their families to participate in disease management, attaches importance to the self-management of the disease, form good disease management behavior, improve patients’ self-management ability, delay the progress of the disease, promote the outcome of the disease, truly achieve the purpose of benefit patients. In this study, the influences of continuous care on medication compliance, return visit rate, recurrence rate, nursing satisfaction, and the quality of life of patients with viral keratitis were analyzed.
2.Participants and method
2.1Study participants
A total of 148 patients with viral keratitis admitted to the ophthalmology department of the authors’ hospital from January 2019 to December 2020 were enrolled as the study subjects and were divided into the observation and control groups, respectively, using the random number table method, with 74 cases in each group.
The study’s inclusion criteria were: (1) patients who met the diagnostic criteria for viral keratitis according to Practical Ophthalmology (3
The study’s exclusion criteria were: (1) patients with severe heart, liver, kidney, and other vital organ insufficiencies; (2) patients complicated with other eye diseases; (3) pregnant and lactating women.
2.2Study methods
2.2.1Intervention methods in the observation group
2.2.1.1 Routine discharge guidance
With the discharge order issued by a doctor, discharge guidance was provided for the patients by the responsible nurse as follows.
(1) Visual guidance. The eye and surrounding skin should be kept clean, and these areas should be cleaned every morning. To avoid eye infections, the eyes should not be rubbed by the hands or wiped with an unclean handkerchief. Visual fatigue and strong light stimulation should be avoided; visual activities should be limited, including screen time on mobile phones, computers, and other electronic products, to no more than 1 h per session. Work/rest balance should be observed and the eyes should not be overused. When washing the face and hair, sewage and shampoo should not enter the eyes as this may cause adverse irritation.
(2) Medication guidance. Clinically, combined medications were commonly adopted, and systemic medication was also prescribed for those with severe keratitis. Concurrently, the side effects of the medication were to be observed. The patients were informed to closely follow their doctor’s instructions and to not stop taking or reducing medications without authorization to avoid recurrence. Where the alternating application of multiple eye drops was implemented, antibiotic eye drops had to be applied first, followed by eye drops for epithelial nutrition and eye ointment, with reasonable intervals in-between. The patients were instructed to apply eye drops correctly and to do so gently to avoid pressure on the eyeball. Eye drops were to be kept refrigerated or away from sunlight according to the medication instructions.
(3) Diet guidance. It was suggested to patients that they eat foods high in vitamins and protein, easily digestible foods, as well as lighter foods, such as milk, eggs, and fish; they were instructed to eat less beef and mutton and more fruits and vegetables to supplement vitamin C for the promotion of corneal epithelial cell recovery. It was suggested that they avoid smoking and consuming alcohol, and not eat spicy or otherwise stimulating foods. These instructions aimed to keep stool smooth and avoid corneal perforation caused by increased intra-abdominal pressure resulting from constipation.
(4) Rest and exercise guidance. Patients were instructed to pay attention to their work and rest schedules and to keep this regular, engage in proper exercise to enhance their physical fitness and try to avoid getting a cold. They were also advised to get enough sleep and avoid fatigue. They were instructed to protect the affected eye, wear tinted glasses when outside in sunlight, and avoid sandy and dusty areas to protect their eyes from foreign objects that may cause discomfort.
(5) Psychological guidance. Knowledge concerning the treatment and prognosis of viral keratitis was provided to the patients, who were informed that the disease was prone to relapse and that active cooperation with the treatment was required. Patients were encouraged to communicate with healthcare providers, ask questions, and remain aware of their psychological status. Questions that were asked by the patients were answered patiently to help reduce psychological pressure and to help them establish confidence in overcoming the disease.
2.2.1.2 Continuous care
(1) A continuous care team was set up in the department comprising 8 members, including the head nurse, the corneal team doctor, and the responsible nurses. All members of the group received relevant knowledge training and fully understood the content of the continuous care program.
(2) Program implementation. A WeChat group was created for patients with viral keratitis, which they were instructed to join once discharged. Designated members of the care team delivered voice reminders to the group related to applying eye drops every morning, noon, and evening to prevent missing doses in the medication schedule. How to apply the eye drops was announced in the group using a combination of text, images, voice, video, and other methods to facilitate repeated viewing. Knowledge related to viral keratitis, such as diet, exercise, medication, and psychology was sent regularly each week. Every Friday, members of the healthcare team answered questions proposed by the patients in the group at a scheduled time and encouraged patients to leave feedback in the WeChat group once this was completed. The responsible nurse instructed each patient to download the HealthLe application, helped them to use it proficiently and asked them to complete a discharge follow-up form at discharge from the hospital. The disease-related knowledge, possible adverse reactions linked to medication, precautions during treatment, and regular review message reminders were regularly sent to the patient. A designated nurse checked whether patients reviewed messages promptly; phone call reminders were made to patients who failed to check messages regularly to help improve their understanding of the disease. Patients were called regularly at 1 week, 1 month, 3 months, 6 months, and 1 year following discharge to inquire about their eye condition, medication, and any effects brought on by their medication, as well as whether timely return visits had been completed, their quality of life and psychological status, and social adaptation ability. Any questions the patients asked were answered and they were instructed to return to the hospital for follow-up if necessary.
2.2.2Intervention methods in the control group
Routine guidance was provided for the patients in the control group at discharge.
2.2.3Evaluation indicators and data collection methods
2.2.3.1 Medication compliance
Using the medication adherence measurement scale for chronic diseases patients compiled by Xu et al. [7], there are 17 items, which are divided into medication adherence behavior performance and health beliefs (barriers and benefits). The higher the score of the scale, the better the compliance. A score of
2.2.3.2 Return visit rate
The return visit rates at 1 week, 1 month, 3 months, 6 months, and 1 year after discharge were compared between the two patient groups. The number and time of return visits due to viral keratitis were collected at 1 week, 1 month, 3 months, 6 months, and 1 year follow-up after discharge.
2.2.3.3 Recurrence rate
Where photophobia, lacrimation, sore eyes, a corneal epithelial defect with the manifestation of punctate, dendritic, or geographic defect, corneal stroma edema, opacity, positive fluorescein staining, and decreased corneal sensation, together with the exclusion of bacterial, fungal, and other infectious keratitis types were observed, the recurrence of viral keratitis had to be determined. The number of cases with recurrence was recorded and compared between the two groups at 1 week, 1 month, 3 months, 6 months, and 1 year follow-up after discharge.
2.2.3.4 Nursing satisfaction
A self-designed nursing satisfaction questionnaire was adopted with a total of 10 items and a total score of 100 points. A higher score indicated a higher degree of satisfaction. Questionnaires with a score below 80 points were considered to reflect an “unsatisfied” outcome, and those with a score between 80 and 100 points indicated a “satisfied” result. The questionnaire was completed by the patient or by the follow-up nurse during the phone interview 1 year after discharge.
2.2.3.5 Quality of life
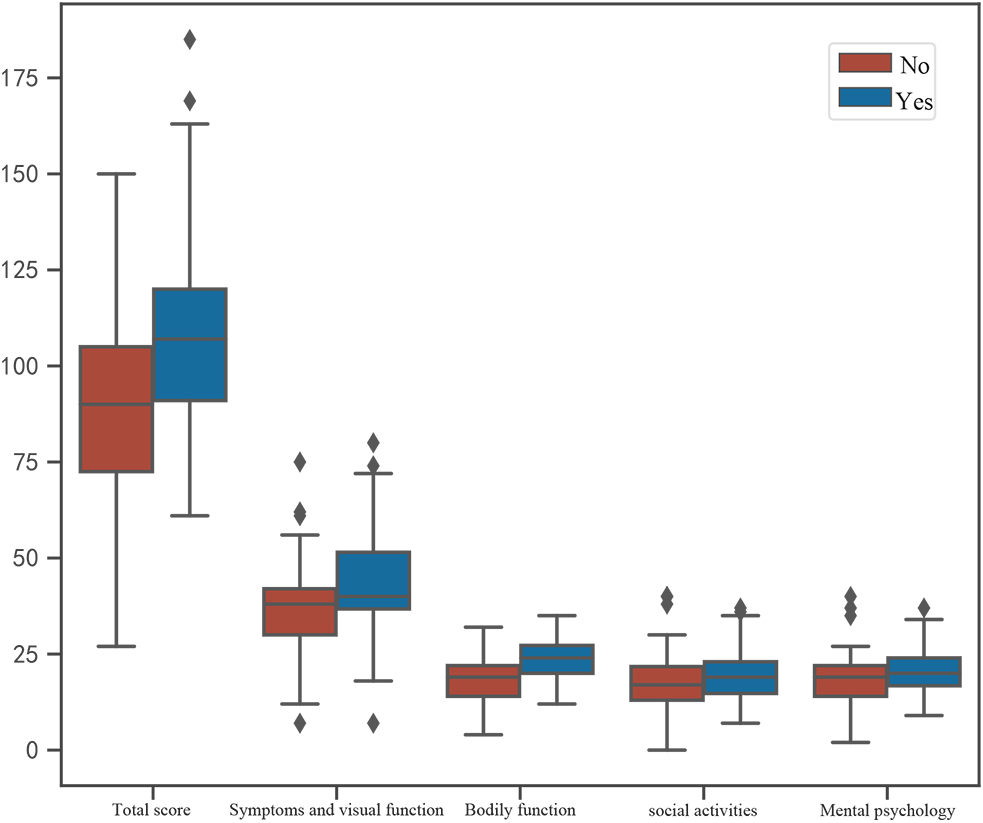
The quality of life scale for Chinese patients with visual impairment and ophthalmopathy, developed by Yu et al. [8], was adopted to compare the scores of the quality of life scores between the two patient groups. The scale included four aspects, i.e., symptoms and visual function, physical function, social activity, and mental psychology, with a total of 20 indicators. A higher score indicated a better quality of life. The scale was completed by the patient or by the follow-up nurse during the phone interview 1 year after discharge.
2.2.4Statistic methods
The measurement data that satisfied normal distribution were expressed as means
3.Results
3.1Analysis of the general data
The baseline data: There were 74 cases in the control group; in the observation group, 2 cases were lost during follow-up, leaving 72 effective cases in this group. There were 42 male and 30 female cases in the observation group. The control group included 45 male and 29 female cases. The median age in the observation and control groups was 51 and 49 years, respectively. The educational backgrounds in the observation group were as follows: 20 primary school and below, 23 junior high school, and 29 high school and above cases. The educational backgrounds in the control group were as follows: 20 primary school and below, 28 junior high school, and 26 high school and above cases. The differences in the general data between the two groups were not statistically significant (
Table 1
Comparison of the information between the two groups of patients
| Variable | Grouping 0 | Grouping 1 | Statistics |
| |
| Gender | – | – | 0. | 093 | 0.760 |
| Male | 45 (60.811) | 42 (58.333) | – | – | |
| Female | 29 (39.189) | 30 (41.667) | – | – | |
| Age | 49.000 [32.000, 68.000] | 51.000 [31.000, 68.000] | 0. | 388 | 0.700 |
| Educational background | – | – | 0. | 627 | 0.731 |
| Primary school and below | 20 (27.027) | 20 (27.778) | – | – | |
| Junior high school | 28 (37.838) | 23 (31.944) | – | – | |
| High school and above | 26 (35.135) | 29 (40.278) | – | – | |
| Course of disease | 6.000 [6.000, 8.000] | 6.000 [5.000, 8.000] | 0. | 710 | 0.473 |
| Medication compliance | – | – | 64. | 025 | |
| Poor | 58 (78.378) | 9 (12.500) | – | – | |
| Moderate | 14 (18.919) | 51 (70.833) | – | – | |
| Good | 2 (2.703) | 12 (16.667) | – | – | |
| Return visit at 1 week | 44 (59.459) | 56 (77.778) | 5. | 675 | 0.017 |
| Return visit at 1 month | 44 (59.459) | 61 (84.722) | 11. | 532 | |
| Return visit at 3 months | 33 (44.595) | 45 (62.500) | 4. | 702 | 0.030 |
| Return visit at 6 months | 23 (31.081) | 42 (58.333) | 10. | 973 | |
| Return visit at 1 year | 22 (29.730) | 36 (50.000) | 6. | 262 | 0.012 |
| Recurrence at 1 week | 36 (48.649) | 27 (37.500) | 1. | 849 | 0.174 |
| Recurrence at 1 month | 37 (50.000) | 20 (27.778) | 7. | 572 | 0.006 |
| Recurrence at 3 months | 30 (40.541) | 11 (15.278) | 11. | 532 | |
| Recurrence at 6 months | 23 (31.081) | 12 (16.667) | 4. | 160 | 0.041 |
| Recurrence at 1 year | 21 (28.378) | 7 (9.722) | 8. | 194 | 0.004 |
| Nursing satisfaction | – | – | 7. | 606 | 0.006 |
| Unsatisfied | 26 (35.135) | 11 (15.278) | – | – | |
| Satisfied | 48 (64.865) | 61 (84.722) | – | – | |
| Symptom and visual function | 38.000 [30.000, 42.000] | 40.000 [37.000, 51.000] | | 084 | 0.002 |
| Physical function | 18.203 ( | 23.667 ( | 038 | ||
| Social activity | 17.000 [13.000, 22.000] | 19.000 [15.000, 23.000] | 986 | 0.047 | |
| Mental psychology | 19.000 [14.000, 22.000] | 20.000 [17.000, 24.000] | 855 | 0.063 | |
| Total score | 89.581 ( | 108.486 ( | 659 | ||
3.2Comparison of the medication compliance between the two patient groups
Twelve cases in the observation group and 2 cases in the control group had good medication compliance; 15 cases in the observation group and 14 cases in the control group had moderate medication compliance; 9 cases in the observation group and 58 cases in the control group had poor medication compliance. The above differences between the two groups were statistically significant (
3.3Comparison of the return visit rate between the two patient groups
The return visit rate at 1 week in the observation and control groups was 77.778% (56/72) and 59.459% (44/74), respectively, and the difference was statistically significant (
3.4Comparison of the recurrence rate within one year between the two patient groups
The recurrence rate at 1 week in the observation and control groups was 37.500% (27/72) and 48.649% (36/74), respectively, and the difference was not statistically significant (
3.5Comparison of the nursing satisfaction between the two patient groups
The nursing satisfaction in the observation and control groups was 84.722% and 64.865%, respectively (higher in the observation than the control group), and the difference was statistically significant (
3.6Comparison of the quality of life between the two patient groups
The total score of quality of life in the observation group was higher than in the control group and the difference was statistically significant (
Figure 1.
Boxplot of the quality of life scores in two groups of patients.
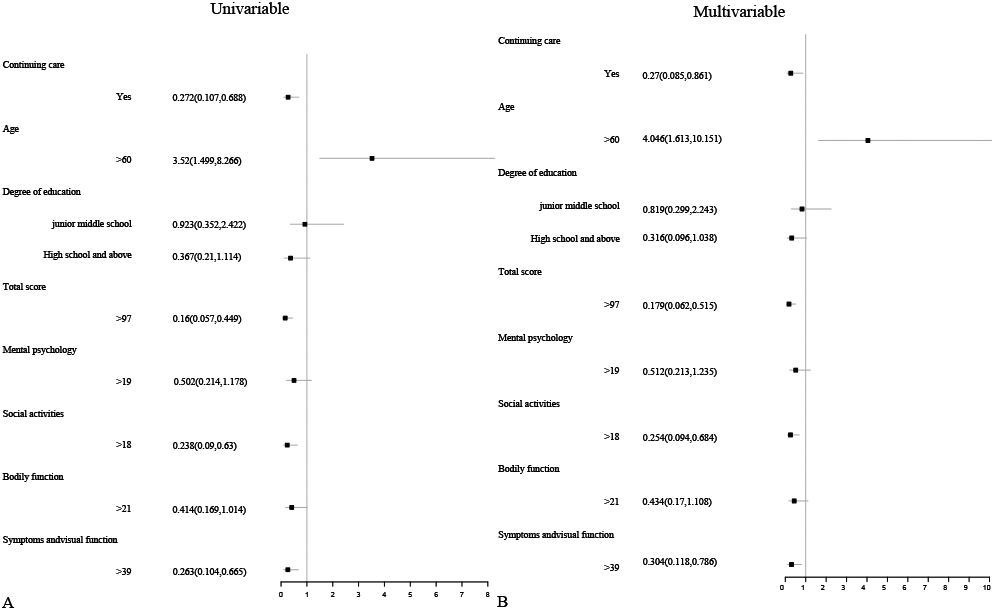
3.7Univariate and multivariate analysis
Table 2
Univariate/multivariate analysis of 1-year recurrence
| Variable | Univariable | Multivariable | |||
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | ||||
| Continuous care | 0.272 [0.107, 0.688] | 0.006 | 0.270 [0.085, 0.861] | 0.027 | |
|
Age ( | 3.520 [1.499, 8.266] | 0.004 | 4.046 [1.613, 10.151] | 0.003 | |
| Educational background | Junior high school | 0.923 [0.352, 2.422] | 0.871 | 0.819 [0.299, 2.243] | 0.698 |
| High school and above | 0.367 [0.121, 1.114] | 0.077 | 0.316 [0.096, 1.038] | 0.058 | |
|
Total score ( | 0.160 [0.057, 0.449] | 0.001 | 0.179 [0.062, 0.515] | 0.001 | |
| Mental psychology ( | 0.502 [0.214, 1.178] | 0.113 | 0.512 [0.213, 1.235] | 0.136 | |
|
Social activity ( | 0.238 [0.090, 0.630] | 0.004 | 0.254 [0.094, 0.684] | 0.007 | |
| Physical function ( | 0.414 [0.169, 1.014] | 0.054 | 0.434 [0.170, 1.108] | 0.081 | |
|
Symptom and visual function ( | 0.263 [0.104, 0.665] | 0.005 | 0.304 [0.118, 0.786] | 0.014 | |
Note: The groupings were conducted as follows with group 0 as the reference, Age: 0 (
As shown in Table 2, the univariate analysis indicated that continuous care, total score (
The results of multivariate analysis showed that continuous care (odds ratio [OR], 0.270; 95% confidence interval [CI], 0.085–0.861;
Figure 2.
Forest plot of univariate/multivariate analysis of 1-year recurrence.
3.8Multivariate stratified analysis of the relationship between continuous care and recurrence after one year
Table 3
Multivariate stratified analysis of the relationship between continuous care and 1-year recurrence
| Variable |
| OR (95% CI) | |
|---|---|---|---|
| Educational background | |||
| Primary school and below | 40 | 0.084 [0.006, 1.113] | 0.060 |
| Junior high school | 51 | 0.201 [0.026, 1.567] | 0.126 |
| High school and above | 55 | 0.621 [0.030, 12.944] | 0.759 |
| Total score | |||
| | 73 | 0.152 [0.023, 1.005] | 0.051 |
| | 73 | 2.282 [0.177, 29.455] | 0.527 |
| Age | |||
| | 93 | 0.348 [0.051, 2.374] | 0.281 |
| | 53 | 0.046 [0.005, 0.420] | 0.006 |
| Mental psychology | |||
| | 74 | 0.227 [0.047, 1.102] | 0.066 |
| | 72 | 0.330 [0.051, 2.134] | 0.244 |
| Social activity | |||
| | 77 | 0.134 [0.026, 0.687] | 0.016 |
| | 69 | 2.031 [0.157, 26.226] | 0.587 |
| Physical function | |||
| | 80 | 0.041 [0.004, 0.462] | 0.010 |
| | 66 | 3.930 [0.387, 39.953] | 0.247 |
| Symptom and visual function | |||
| | 73 | 0.173 [0.031, 0.968] | 0.046 |
| | 73 | 0.198 [0.020, 1.943] | 0.165 |
Note: Variables included in the multivariate stratified analysis: nursing satisfaction, surgery, gender, disease duration, medication compliance, and missed medication as an adjustment variable. The bold characters represent variables.
As shown in Table 3, a multivariate stratified analysis was conducted within the patient subgroups. The multivariate stratified analysis verified a correlated risk between continuous care and recurrence after 1 year. The OR results of the following variables were all less than 1 and were all statistically significant (
Table 4
Binary logistic regression analysis of 1-year recurrence
| Variable |
|
| OR (95% CI) |
|
|---|---|---|---|---|
| Symptom and visual function | 0.973 [0.933, 1.012] | 0.178 | ||
| Social activity | 0.902 [0.834, 0.964] | 0.005 | ||
| Age | 0.039 | 2.905 | 1.04 [1.014, 1.07] | 0.004 |
| Continuous care | 0.34 [0.115, 0.92] | 0.039 |
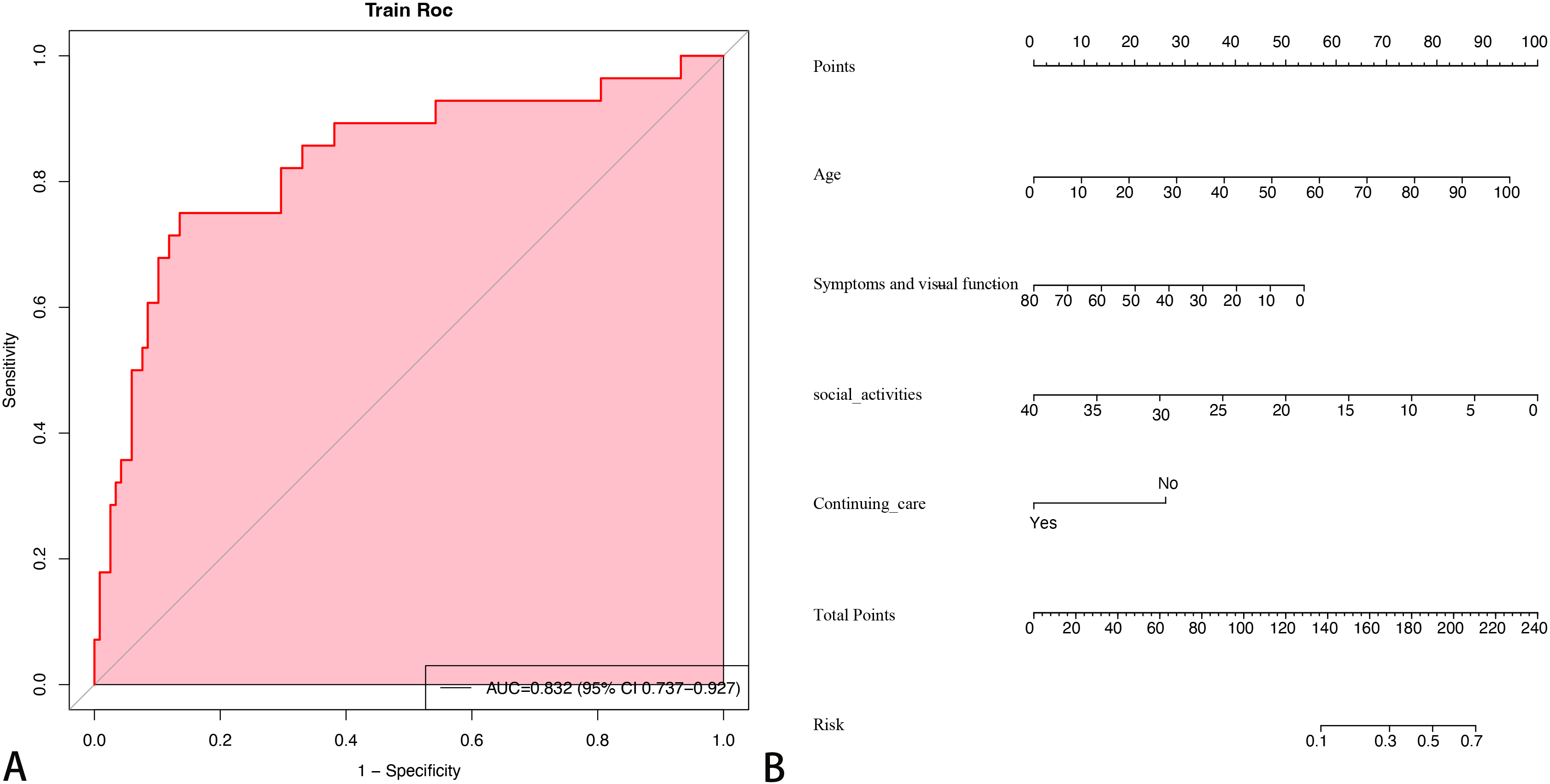
Figure 3.
Prediction results of binary logistic regression of 1-year recurrence.
3.9Logistic regression modeling
As shown in Table 4, binary logistic regression was adopted to evaluate the effects of symptom and visual function, social activity, age, and continuous care on recurrence after 1 year. The area under the curve of the model (Fig. 3A) was 0.83 (95% [0.737, 0.927]). Among the variables introduced into the model, social activity (OR, 0.902; 95% CI, 0.834–0.964;
The results of logistic regression analysis were used to construct a nomogram for predicting the probability of recurrence after 1 year (Fig. 3B). To estimate the risk of 1-year recurrence, the observed value in each predictor was assigned a specific number of points by drawing a vertical line to the vertex ruler. The sum of the points for each variable corresponded to the individual risk of recurrence after 1 year.
Figure 4.
Online interactive dynamic nomogram.
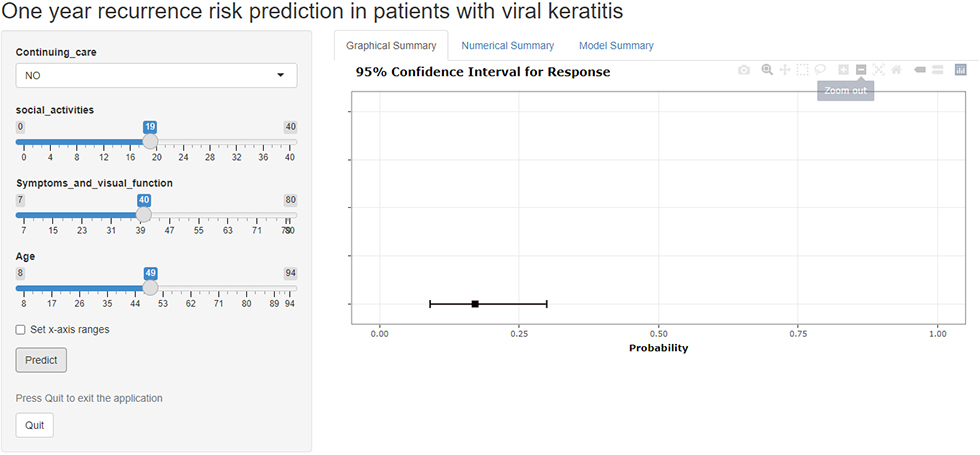
3.10Online interactive dynamic nomogram
To facilitate user access, an online risk calculator (https://ouyangxiao111.shinyapps.io/Viral_keratitis/) (Fig. 4) was constructed as part of this study, based on the nomographic atlas. This calculator may be useful for decision-making and improving clinical diagnostic efficiency. The models could also be further tested and updated, based on the availability of new clinical trial data. The user can estimate the risk of recurrence within 1 year by completing the patient information and relevant characteristics. For example, a 75-year-old patient with no continuous care and a social activity score of 10 points, as well as a symptom and visual function score of 25 points, would have a 1-year recurrence probability of 0.686 (95% CI, 0.468–0.844).
4.Discussion
Viral keratitis is caused by several viruses, and its clinical manifestation varies in severity. The degree of visual impairment is correlated with the severity of lesions, the severity of inflammation, the course of the disease, and the number of recurrences [9]. From a population health perspective, the American Care Continuum Alliance notes that, in addition to the transfer of patients within or between institutions, continuous care also includes the transfer of patients when their health status changes, and the transfer of patients between care providers [10], the ultimate goal of which is to facilitate a safe and smooth transition for patients from the hospital to their home/community and improve their outcomes after discharge [11]. Domestic and overseas investigations have been conducted on the application of continuous care involving various diseases, e.g., among elderly patients with chronic diseases, including diabetes mellitus, lumbar disc herniation, cervical cancer, and chronic obstructive pulmonary disease [12, 13, 14, 15]. In recent years, the model of hospital-based continuous care has been widely applied. The main model has responsible nurses or senior nurses carrying out health education during the hospitalization period, regularly evaluating the physical condition of discharged patients through consistent telephone follow-up calls/other follow-up methods, and educating patients by delivering knowledge related to diet, exercise, medication, and rehabilitation, in addition to answering questions on disease knowledge [4].
4.1The influence of continuous care on medication compliance in patients with viral keratitis
The results of the present study showed that, with the implementation of continuous care, medication compliance among patients in the observation group was higher than in the control group (
4.2The influence of continuous care on the return visits of patients with viral keratitis
The results of this study revealed that the return visit rate at 1 week, 1 month, 3 months, 6 months, and 1 year of patients in the observation group were higher than in the control group (
4.3The influence of continuous care on the recurrence rate in patients with viral keratitis
The results of this study showed that the recurrence rate at 1 month, 3 months, 6 months, and 1 year was lower in the observation than in the control group (
4.4The influence of continuous care on nursing satisfaction in patients with viral keratitis
The present study showed that nursing satisfaction in the observation and the control groups was 84.722% and 64.865%, respectively. Nursing satisfaction was higher in the observation group, and the difference was statistically significant (
4.5Continuous nursing may improve the quality of life of patients with viral keratitis
The results of this study showed that the total quality of life score of patients in the observation group was higher than in the control group, and the difference was statistically significant (
5.Conclusion
The application effect of continuous care showed positive outcomes for patients with viral keratitis, and continuous care could improve medication compliance and the return visit rate, reduce the recurrence rate, and improve satisfaction and the quality of life of patients with viral keratitis. The results of the present study thus hold a degree of reference value for the implementation of continuous care in patients with viral keratitis. A web-based model (https://ouyangxiao111.shinyapps.io/Viral_keratitis/) that could facilitate early detection of the risk of recurrence after 1 year in patients with viral keratitis was created as part of this study. With access to new clinical trial data, this model can be further tested and updated to provide more individualized treatment for patients in the future.
A limitation of this study was that it only selected patients with viral keratitis in the authors’ hospital as study participants, which limited the scope of the investigation due to its small sample size. As such, it does not fully reflect the overall status of continuous care for patients with viral keratitis, and further investigation is required to support the present results.
Ethics statement
The study was conducted with approval from the Ethics Committee of The Second Affiliated Hospital of Nanchang. This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
The study was funded by the Science and Technology Department of Jiangxi Province (No. 20202BBGL73074).
Availability of data and materials
All data generated or analysed during this study is included in this article. Further enquiries can be directed to the corresponding author.
Author contributions
Conception and design of the research: Yang Y; Acquisition of data: Chen L, Su R, Yang Y; Analysis and interpretation of the data: Yang Y, Su R; Statistical analysis: Xu Y, Yang Y; Obtaining financing: Yang Y; Writing of the manuscript: Su R, Yang Y; Critical revision of the manuscript for intellectual content: Yang Y. All authors read and approved the final draft.
Acknowledgments
The authors would like to thank the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.
Conflict of interest
The authors declare that they have no competing interests.
References
[1] | Song X, Xie L, Tan X, et al. A multi-center, cross-sectional study on the burden of infectious keratitis in China. PLoS One. (2014) ; 9: (12): e113843. Published 2014 Dec 1. doi: 10.1371/journal.pone.0113843. |
[2] | Heba AS, Wael W. Management of neovascularization in recurrent herpetic keratitis. Journal of the Bahrain Medical Society. (2020) ; 32: (1): 37-40. |
[3] | Li F, Gong Q, Lu Y. Effects of continuous nursing on rehabilitation compliance, living quality and daily living ability of patients with acute ischemic stroke. American Journal of Translational Research. (2022) ; 14: (1): 381-388. |
[4] | Shi F, Xiao L, Xiao W. Research progress in continuity of care. Modern Nurse. (2017) ; (12): 6-9. |
[5] | Mora K, Dorrejo XM, Carreon KM, Butt S. Nurse practitioner-led transitional care interventions: An integrative review. Journal of the American Association of Nurse Practitioners. (2017) ; 29: (12): 773-790. doi: 10.1002/2327-6924.12509. |
[6] | Ke BH. Progress in the application of continuous nursing in patients discharged from ophthalmology. International Medicine & Health Guidance News. (2019) ; 25: (134): 2207-2208. |
[7] | Xu WH, Wang Q, Liang XW. Development of a medication compliance scale in patients with chronic diseases. Chinese Journal of Prevention and Control of Chronic Non-Communicable Diseases. (2008) ; 16: (6): 558-560. |
[8] | Yu Q, Li SZ, Chen HN, et al. The development of a scale of life quality for diseases with visual impairment. Chinese Journal of Ophthalmology. (1997) ; 33: (4): 307-310. |
[9] | Mu HD. Application of comprehensive nursing in herpetic keratitis patients. Chinese Journal of Modern Nursing. (2019) ; 25: (33): 4385-4387. |
[10] | Alliance CC. What is the care continuum? (2012-05-04). http://www.carecontinuumalliance.org/index.asp. |
[11] | Li YH, Wang X, Liu Y, et al. Reliability and validity of Chinese version of Care Transitions Measure. Chinese Nursing Management. (2014) ; 14: (9): 919-922. |
[12] | Chi S, Liu JL, Kang HC, Lv DM. Continuous nursing intervention on recovery of diabetic patients. J Biol Regul Homeost Agents. (2018) ; 32: (6): 1507-1513. |
[13] | He Q, Zhao J, Fan M, Wang F. Effect of continuous nursing based on wechat platform on postoperative rehabilitation of patients with lumbar disc herniation. Jpn J Nurs Sci. (2021) ; 18: (2): e12382. doi: 10.1111/jjns.12382. |
[14] | Han D, Wang D, Yang J, Li X. Effect of multidisciplinary collaborative continuous nursing on the psychological state and quality of life of patients with cervical cancer. Am J Transl Res. (2021) ; 13: (6): 6654-6661. Published 2021 Jun 15. |
[15] | Guo X, Men F, Han X, Wang Z. The efficacy of continuous nursing care for patients with chronic obstructive pulmonary disease: A randomized controlled trial protocol. Medicine (Baltimore). (2021) ; 100: (2): e23974. doi: 10.1097/MD.0000000000023974. |
[16] | Sanguansak T, Morley KE, Morley MG, Thinkhamrop K, Thuanman J, Agarwal I. Multimedia Appendix Removal and Editorial Warning Regarding the MMAS Scale (Two-Way Social Media Messaging in Post-Operative Cataract Surgical Patients: A Prospective Interventional Study). J Med Internet Res. (2018) ; 20: (12): e12120. Published 2018 Dec 20. doi: 10.2196/12120. |
[17] | Wan C, Zhou Y. Effect of continuous nursing intervention on the therapeutic outcome, compliance behavior and quality of life of patients with pulmonary tuberculosisInt. J Clin Exp Med [Internet]. (2020) ; 13: (3): 1528-36. |
[18] | Parik PC, Patel VJ. Health-related Quality of Life of Patients with Type 2 Diabetes Mellitus at A Tertiary Care Hospital in India Using EQ 5D 5L. Indian J Endocrinol Metab. (2019) ; 23: (4): 407-411. doi: 10.4103/ijem.IJEM_29_19. |
[19] | Ba̧k E, Nowak-Kapusta Z, Dobrzyn-Matusiak D, Marcisz-Dyla E, Marcisz C, Krzemińska SA. An assessment of diabetes-dependent quality of life (ADDQoL) in women and men in Poland with type 1 and type 2 diabetes. Ann Agric Environ Med. (2019) ; 26: (3): 429-438. doi: 10.26444/aaem/99959. |
[20] | Posadas-Collado G, Membrive-Jiménez MJ, Romero-Béjar JL, et al. Continuity of nursing care in patients with coronary artery disease: A systematic review. Int J Environ Res Public Health. (2022) ; 19: (5): 3000. Published 2022 Mar 4. doi: 10.3390/ijerph19053000. |
[21] | Geng W, Tao N, Wang T, et al. Continuous nursing reduces postoperative complications and improves quality of life of patients after enterostomies. Int J Clin Exp Med. (2019) ; 12: (5): 5895-5901. |


