
Femoral condyle configuration and its impact on anterior cruciate ligament reconstruction
Abstract
BACKGROUND:
Rupture of the anterior cruciate ligament (ACL) is one of the most common knee injuries and has substantial impact on knee function. Beside primary ruptures, an increasing number of re-(re-)ruptures occur, representing a therapeutical challenge for the treating surgeon. Several risk factors for re-ruptures have been previously identified, including an increased tibial slope.
OBJECTIVE:
In this study, we investigated the effect of femoral condyle configuration on ACL-ruptures and re-ruptures.
METHODS:
In-vivo magnetic resonance imaging scans of three different groups of patients were compared. Group 1 included patients with an intact ACL on both sides, group 2 included patients with primary, unilateral ACL-rupture, while group 3 included patients with an ACL-re-rupture or re-(re-)rupture. Fourteen different variables were obtained and analyzed regarding their impact on ACL-re-(re-)rupture.
RESULTS:
Overall, 334 knees were investigated. Our data allowed us to define parameters to identify anatomical configurations of bones associated with an increased risk of ACL-re-rupture. Our results show, that patients with ACL-re-rupture show increased radii of the extension facet of the lateral femoral condyle (
CONCLUSION:
We conclude that a spherical femoral condyle form does influence the clinical outcome after ACL-reconstruction.
1.Introduction
Rupture of the anterior cruciate ligament (ACL) is one of the most common knee injuries, with an incidence between 32–38/100.000 person-years [1, 2, 3]; however, some studies report higher incidences of up to 68.6/100.000 person-years [4]. Contrasting with primary tears, re-rupture after ACL-reconstruction is quite rare, but still reaches a 5-year prevalence of around 6% [5]. ACL-ruptures are severe injuries, especially in patients performing sports-related activities. Despite reported return-to-sport rates to preinjury level of between 13–69% [6], treatment often requires surgery and strict rehabilitation. In particular, re-ruptures can be career-ending in professional athletes. Because of the relatively high incidence, especially in younger people, ACL-tears are socioeconomically relevant due to the need for surgeries and lengthy rehabilitation. Based on the abovementioned facts, ample research regarding surgical-techniques [7], graft-choice [8, 9], and post-surgery rehabilitation [10] has been published. While the surgical technique was the main topic in the beginning of ACL research, arthroscopically assisted ACL-reconstruction represents the golden standard today. Today, several grafts are available for ACL-reconstruction, whereby the autologous semitendinosus-, patella- and quadriceps-tendon can be considered as equally good, with several pros and cons for each graft [11]. In theory, preconditioned grafts should be advantageous [12]. Moreover, drilling of the femoral tunnel, which was performed transtibial in the early years, is commonly performed through the anteromedial portal now [13]. Additionally, possible risk factors for ACL-rupture have become a popular research target. Several authors have investigated the influence of anatomical configurations and structures of the knee on ACL-function and stability. Park et al. found that in both males and females with ACL-rupture, the notch width (NW) appeared smaller on magnetic resonance imaging (MRI) scans, compared to controls [14]. Similar results were reported by two other studies which found an anterior outlet-stenosis of the notch on computed tomography (CT) scans that showed significant association with ACL-tears [15, 16]. Besides the notch, the influence of several other anatomical variants of various knee structures on ACL-stability have been investigated. A follow-up study of 100 patients with ACL-tears reported that conservative treatment of ACL-tears led to less satisfying results in patients with a more spherical shape of the femoral condyles [17]. It has been postulated that patients who underwent surgery reached higher subjective scores when they had a smaller intercondylar notch and a smaller width of the intercondylar eminence. Notably, conservatively treated patients scored better when a more pyramidal shaped notch was present [18]. Moreover, a significant smaller height of the lateral femur condyle seems to be a risk factor for ACL-rupture [19]. One study reported that a smaller tibial plateau length relative to the femur comes with a higher risk for ACL-tears. The authors argue that this could be one reason for the higher incidence of ACL-tears in females, since this anatomical relation was more often detected in female participants, even when no ACL-rupture was evident [20]. The morphometry of the femoral condyles seems to not only influence ACL-stability but also the risk for injuries associated with ACL-rupture. One study noted that an increased anteroposterior length of the medial/lateral femoral condyle relative to the medial/lateral tibial plateau was associated with an increased risk of meniscal lesions when combined with ACL-rupture [21]. Beside the notch and femoral condyles, tibial parameters also seem to influence ACL-stability. Another study reported that an increase of the posterior tibial slope (PTS) increased the risk for non-contact ACL-tears in females [22]. These results are supported by those of a meta-analysis, which analyzed the cumulative data of 12 studies. The analysis indicated that an increased medial and lateral tibial slope is associated with ACL-injuries [23]. Moreover, an increased PTS is associated with ACL-re-rupture [24]. This resulted in the option of tibial slope correction, which aims to reduce the posterior tibial slope and thereby to reduce the risk for ACL-re-tear [25]. Moreover, the combination of slope correction and varus correction could show reduced forces on ACL grafts in biomechanical analysis [26].
A study concluded that their results show no evidence that knee-stability can be derived from its radiographic surface geometry [27]. Another study also reported no significant differences between the shape of the femoral condyles in ACL-reconstructed knees compared to those with native ACL. One of the major limitations of this study, however, was that bilateral knees of the same patients were compared; thus, no relevant difference in the shape of the condyle between the knees of the same patient would be expected, even if one knee suffered from ACL-rupture while the other did not [28].
Clinically, a study reported that at three months post-trauma, a positive pivot-shift test is the strongest predictor of the future need for ACL-reconstruction in patients with ACL-rupture [29].
Against this background, we investigated whether different shapes of the femoral condyles are associated with a higher incidence of ACL-ruptures, re-ruptures, and re-(re-)ruptures. Papers recently focused on the PTS, but beside the PTS, several anatomical variants affect the ACL. Our hypothesis was that an elliptical shape of the femoral condyles offers better bony congruency and comes along with better intrinsic stability, thereby decreasing the risk for ACL-rupture or re-rupture after ACL-reconstruction.
2.Materials and methods
This study was performed in accord with the Declaration of Helsinki of 1964 and its later amendments Ethical approval was obtained from the local ethics committee (Approval number: VT- 21-1310).
In-vivo MRI scans of three different patient groups were compared. Group 1 (
Figure 1.
Variables 1–4 are shown in sections A–D. A: Variable 1 (depth of the lateral femoral condyle). B: Variable 2 (depth of the femoral shaft lateral). C: Variable 3 (depth of the medial femoral condyle). D: Variable 4 (depth of the medial femoral shaft).
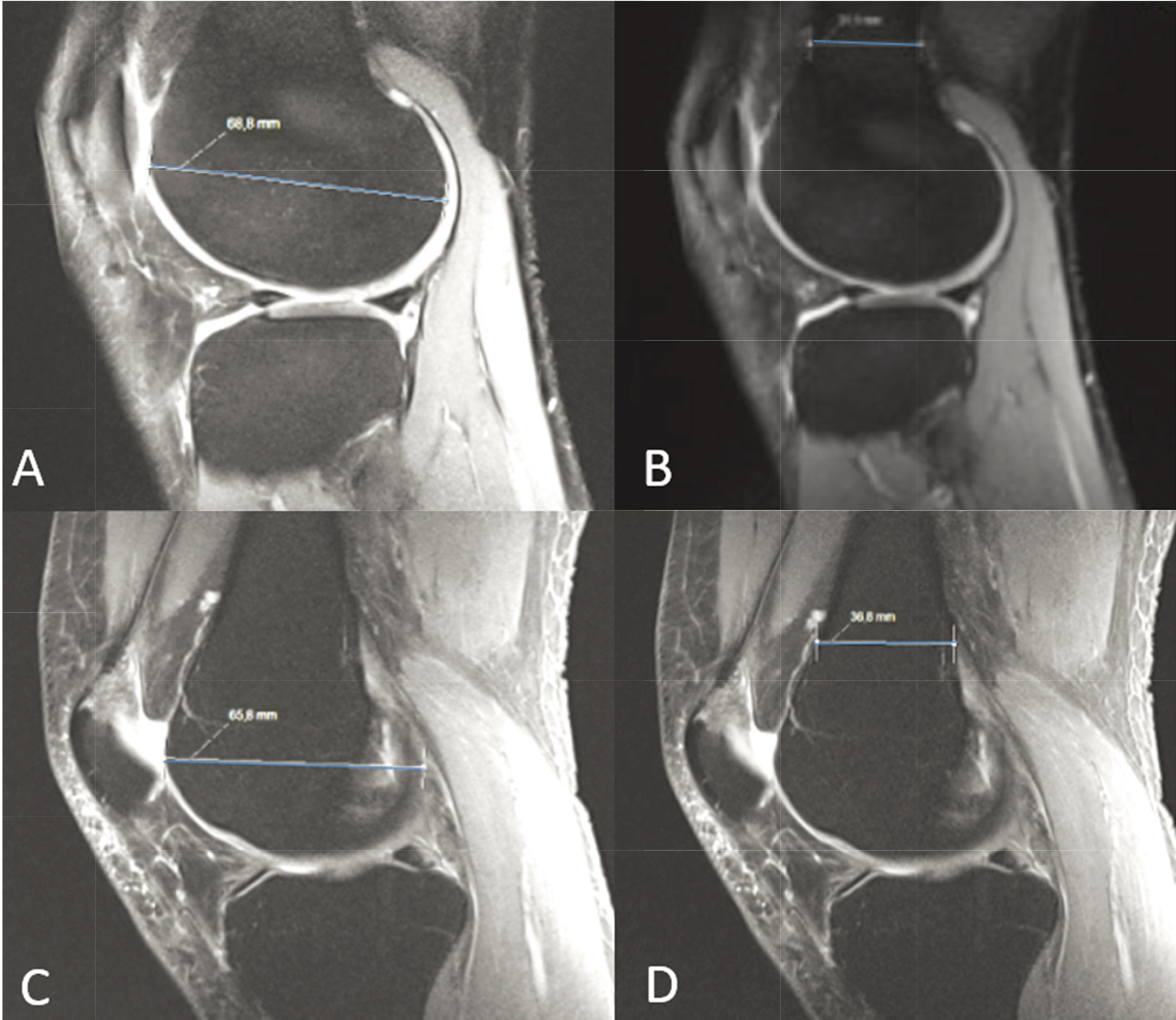
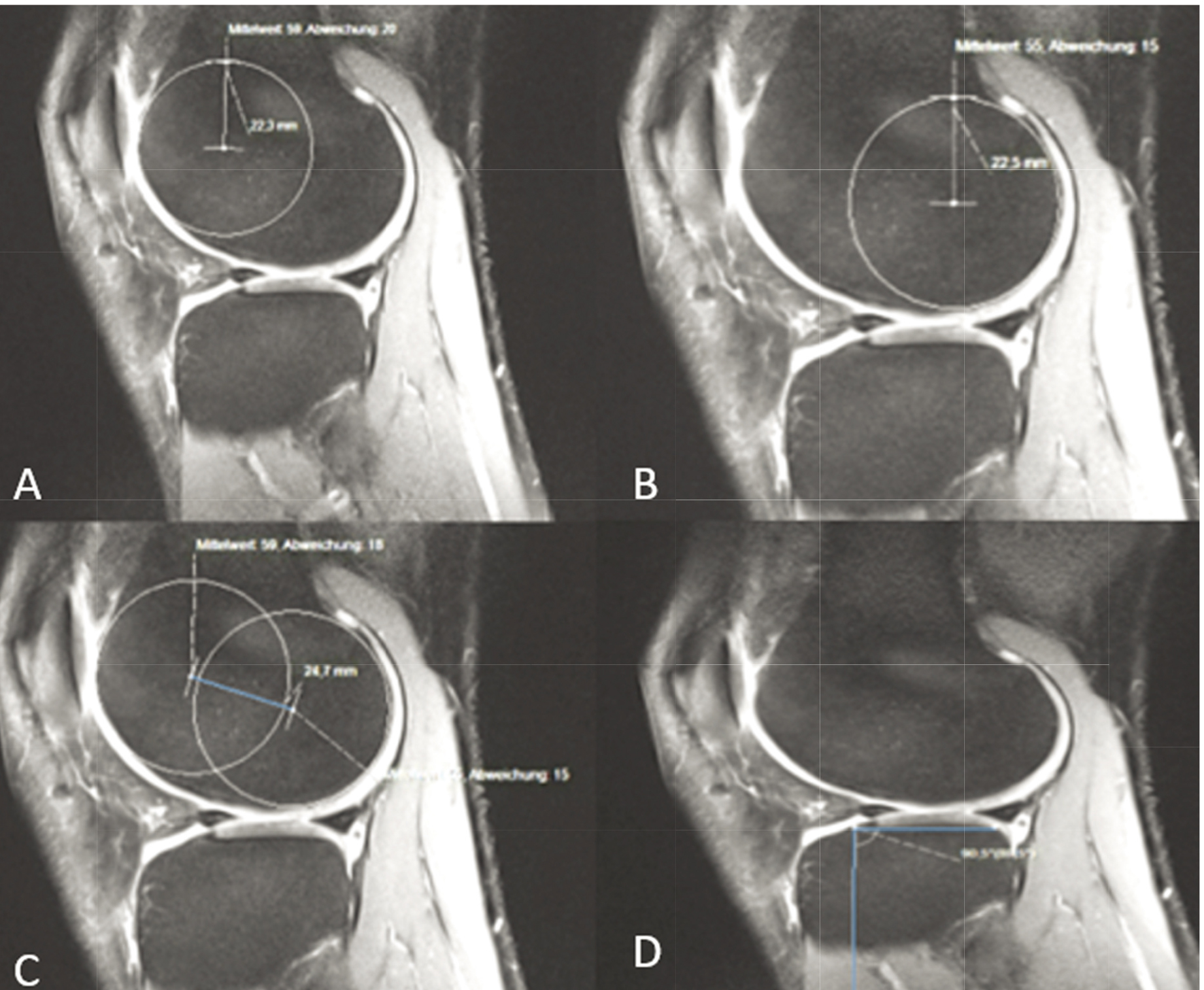
Figure 2.
Variables 5–7 and 11 are shown in section A–D. A: Variable 5 (extension facet of the lateral femoral condyle). B: Variable 6 (flexion facet of the lateral femoral condyle). C: Variable 7 (distance between the circle-centers of the lateral femoral condyle). D: Variable 11 (angle between tibial plateau and tibial shaft lateral). Determination of the extension and flexion facet of the medial femoral condyle as well as the distance between the circle-centers was performed according to the demonstrated technique on the lateral side. Same applies to the determination of the medial tibial slope.
Factors affecting image-quality were mainly related to image-quality due to moving artefacts, metal or implant artefacts, or massive joint effusion-including hemarthrosis, which can cause issues with the assessment of the anterior part of the condyles. Only images which allowed clear assessment of all relevant structures were used in this study.
Statistical analysis was performed using SPPS 22.0 (IBM, Armonk, New York, USA). A unifactorial analysis of variance (ANOVA) was used to compare mean values of the groups, while homogeneity of variances was tested using the Levene’s test. The values named above of 50 patients in group 1 were measured by three observers to test interobserver reliability. A
Table 1
Significant results regarding within group variables
| Variables | Group | Significance ( |
|---|---|---|
| 1 (depth of the lateral femoral condyle) | 3 | |
| 2 (depth of the femoral shaft lateral) | 3 | |
| 3 (depth of the medial femoral condyle) | 1 | |
| 4 (depth of the medial femoral shaft) | 3 | |
| 5 (extension facet lateral femoral condyle) | 1 | |
| 6 (flexion facet lateral femoral condyle) | 2 | |
| 7 (distance between circle-centers lateral femoral condyle) | 3 | |
| 8 (extension facet medial femoral condyle) | 1 | |
| 9 (flexion facet medial femoral condyle) | 1 | |
| 10 (distance between circle-centers medial femoral condyle) | 3 | |
| 11 (Tibial slope lateral) | 1 | |
| 13 (height area intercondylaris lateral) | 3 | |
| 14 (height area intercondylaris medial) | 3 | |
| 8:4 | 1 | |
| 5:2 | 1 |
Table 2
Values for extension facet, depth of the femoral shaft and ACL-(re-)rupture index 1 and 2 within the three groups
| Extension facet medial | Extension facet lateral | Depth shaft medial | Depth shaft lateral | ACL-(re-) rupture- index 1: Extension | ||
| facet | ||||||
| medial | ||||||
|
| ||||||
| Depth | ||||||
| shaft | ||||||
| medial | ACL-(re-) rupture- index 2: Extension facet lateral | |||||
| shaft | ||||||
| lateral | ||||||
| Group 1 Intact ACL both sides | 10.7 mm | 11.8 mm | 27.6 mm | 30.9 mm | 0.39 | 0.38 |
| Group 2 Primary unilateral ACL-rupture | 9.6 mm | 10.2 mm | 27.7 mm | 30.6 mm | 0.35 | 0.33 |
| Group 3 ACL-re-(re-)rupture | 9.3 mm | 9.9 mm | 30.9 mm | 34.7 mm | 0.3 | 0.29 |
3.Results
In total, 334 MRI scans were analyzed. Sex distribution was homogenous in all three groups: approximately 1/3 females and 2/3 males in each group without significant differences regarding the distribution between the groups (
Figure 3.
Size of the extension facet of the lateral femoral condyle in mm in groups 1 (intact ACL), 2 (unilateral ACL-rupture), and 3 (ACL-re-(re)rupture).
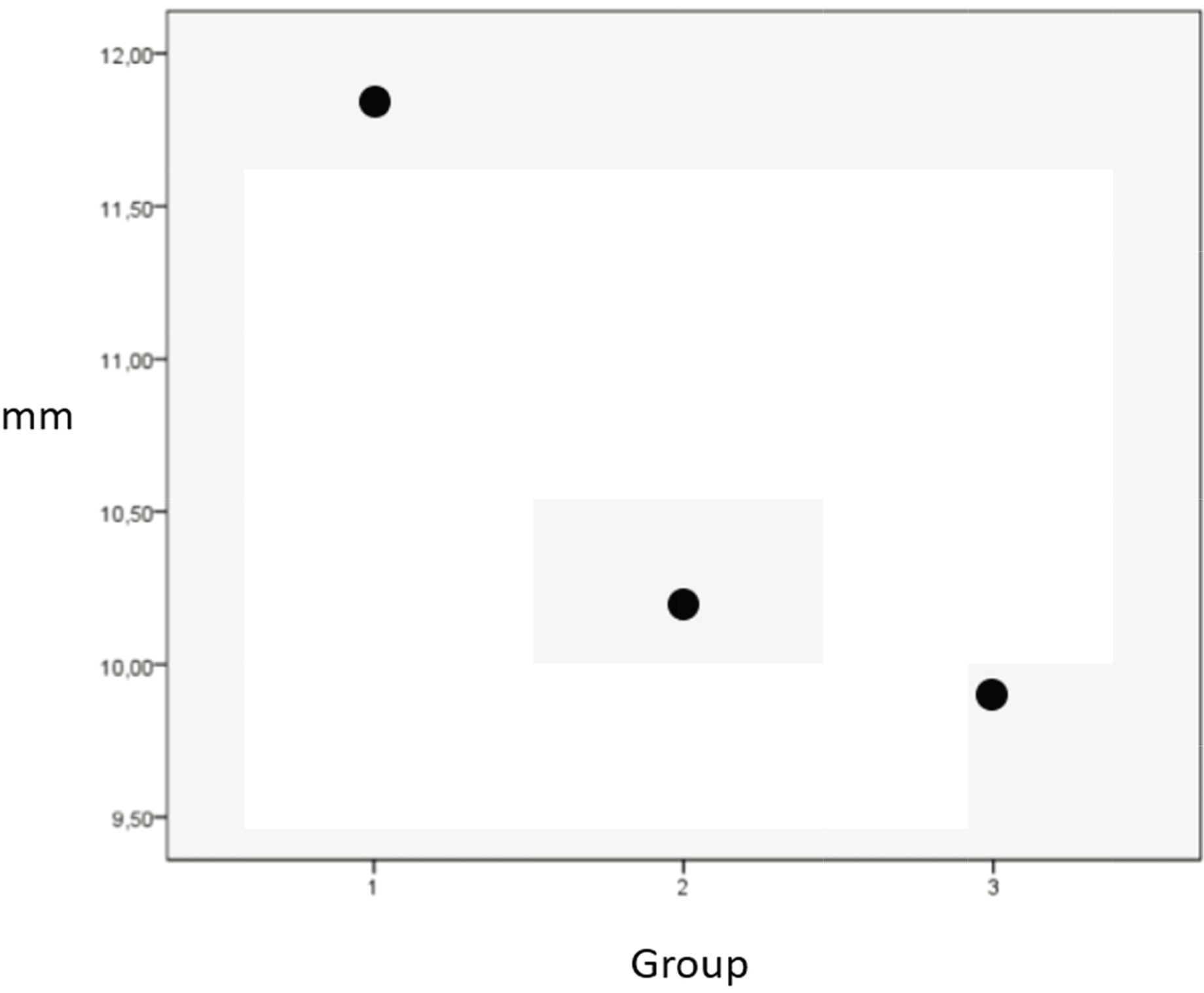
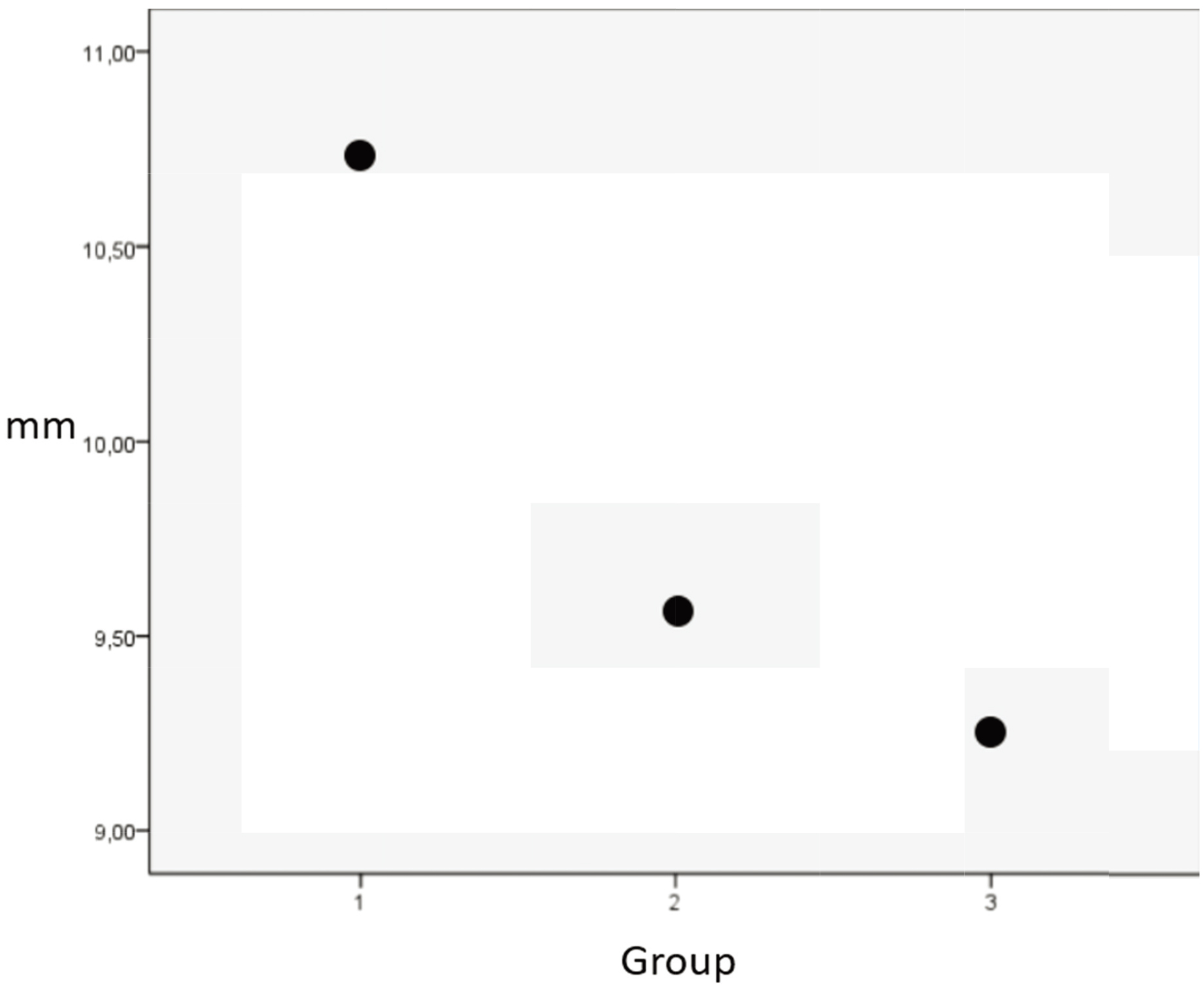
Figure 4.
Size of the extension facet of the medial femoral condyle in mm in groups 1 (intact ACL), 2 (unilateral ACL rupture), and 3 (ACL-re-(re-)rupture).
Variable 3 showed a significant difference when groups 1 and 3 were compared (
Unifactorial ANOVA was used to compare variables 5 and 6 and variables 8 and 9. For variables 5 and 6, group 3 showed a significantly smaller ratio compared to groups 1 and 2 (
ANOVA of the ratio of variables 8/4 revealed non-homogenous distribution; thus, a Games-Howell correction was performed. This was repeated for the ratio of variables 5/2. Group 1 showed significantly higher mean values than group 2 and 3 (
Regarding the variable 5/2 ratio, group 1 showed significantly higher values than groups 2 and 3 (1 vs. 2
Variables 13 and 14 were compared using a
The risk for an ACL-re-rupture increases with the decrease of the radius of the extension facet of the lateral femoral condyle (OR
4.Discussion
In this study, we measured 14 anatomical variables around the knee joint in MRI scans from patients with intact ACL (group 1); patients with primary, unilateral ACL-rupture (group 2); and patients with ACL-re-rupture or ACL-re-(re-)rupture (group 3). Two variables showed a significant difference between patients with an intact ACL and those with ruptured or re-(re-)ruptured ACLs: the extension facets of the lateral and medial femoral condyles. Group 1 showed a significantly larger radius of the medial and lateral extension facets compared to groups 2 and 3. In terms of 6 of the 14 variables, patients with ACL-re-rupture differed significantly from those in the groups with an intact ACL or an ACL-rupture. Patients in group 3 show a smaller radius of the extension facet of the lateral and medial femoral condyle. Moreover, in patients with ACL-re-rupture, the tuberculi of the eminentia are lower, and the distance between both centers of the circles in the lateral femoral condyle is larger, probably resulting in a longer running surface of the lateral condyle. Moreover, four ratios, which are significantly smaller in patients with ACL-re-rupture, can be calculated. The ratios are as follows: depth of the femoral condyle/femoral shaft both -medial and lateral- and the ratios of extension facet/flexion facet -both medial and lateral.
Some of the variables described in this study have been investigated by previous studies. An increase of the PTS is a well-studied risk factor for ACL-rupture [22, 23, 24]. Kapandji et al. reported that the medial tuberculum intercondylaris is higher than the lateral [30]. This is in line with our data. Kostogiannis et al. reported that a spherical configuration of the femoral condyles is an indicator that ACL-reconstruction will likely be necessary in case of ACL-rupture [31]. In our study, a spherical configuration of the femoral condyle was determined by lower values regarding the variables 1, 3, 7, 10 and the ratios 1/2 and 3/4.
Eggerding et al. postulated that a spherically shaped femoral condyle does not influence the clinical result after ACL-reconstruction [18]. Our results do not support these findings. All variables described above, which describe a spherical femoral condyle, show significant differences in patients with ACL-re-rupture compared to at least group 1, 2 or both. Thus, we conclude that a spherical form of the femoral condyle could influence the clinical outcome after ACL-reconstruction.
Several studies have noted that an increase of the tibial slope is associated with a higher risk for ACL-rupture or ACL-(re-)(re-)rupture [22, 23, 24, 32]. Normally, PTS is measured using radiography. However, some authors have used CT and MRI, which allows differentiation between a medial and lateral PTS -as we did in this study. In our study, we measured the angle between the tibial shaft and plateau, both medial and lateral. This can be converted into the PTS as described above. In our study, the mean angle between the tibial shaft and plateau was significantly higher on the lateral side. Due to the bulge of both articular surfaces, we can expect that the PTS measured in plain radiographs does not correspond with the mean value of the medial and lateral PTS. In our study, we measured the angle between the tibial shaft and plateau both medially and laterally in 50 radiographs of knees in group 3. Compared to the angle between the tibial shaft and plateau, in medial and lateral MRI scans of the same patients there were significant differences (MRI 84.2
5.Conclusion
The finding that the more significantly the re-rupture-indices decrease, the higher the degree of damage is, could lead to the conclusion that patients with the anatomical configuration described above have a higher risk for ACL-injury in the future. This knowledge could be used in postoperative physiotherapy. Patients with higher risk for re-ruptures could perform proprioceptive exercises and stabilization workouts for a longer period of time to improve the intermuscular interaction. The “loading response,” i.e., the stage during walking where the leg adopts the load during walking, should be addressed. In this stage, the knee needs maximum stability [33]. The timepoint for return-to-sport could be adjusted, especially in full-contact sports. From an economical perspective, these indices could be measured in professional athletes, especially in those who already suffered from an ACL-injury. The studies discussed focus on anatomical and biomechanical aspects of the problem, in the future, stem cell based therapies may play an increased role [34].
There are some limitations, which have to be mentioned. This study focused on the configuration of the femoral condyle and its impact on ACL-tears. However, additional pathologies -like meniscus also impact ACL-stability, which is difficult to quantify. Moreover, long-axis X-ray is the golden standard to determine the PTS. In our study, we measured the PTS in MRI-scans, which is advantageous to differentiate between the medial and lateral PTS, but can be error prone due to the short image section. We used a standardized rehabilitation protocol, however in practice, compliance may vary quiet significantly and the quality and quantity of physiotherapy may also vary, due to the fact, that patients underwent physiotherapy in many different institutions. Also, the physical and sportive activity varies within our patients, which also can influence the occurance of re-rupture.
However, the present data allow defined parameters, which identify anatomical configurations of the bone, which seem to be associated with an increased risk for an ACL-(re-)rupture. These parameters are the extension facets of the medial and lateral femoral condyles, which are significantly lower in patients with ACL-re-rupture than in patients with intact ACLs. However, our findings represent one possible factor for ACL(re-)rupture, in many cases a combination of pathologies leads to (re-)tear. It is hard to objectifiable, which proportion can be lead back to the different factors.
Funding
No funds, grants, or other support were received.
Ethical approval
All procedures performed in the study were in accordance with the Declaration of Helsinki (1964). The study was approved by the institutional ethics committee (VT-21-1310).
Informed consent
In accordance with the institutional ethics committee, informed consent was not necessary.
Author contributions
Conceptualization: Lena Riemer, David Grevenstein; Methodology: David Grevenstein, Jens Dargel, Thomas Steimel, Sönke Reineck, Peter Schäferhoff; Formal analysis and investigation: David Grevenstein, Lena Riemer; Writing – original draft preparation: Lena Riemer, David Grevenstein; Writing – review and editing: Jens Dargel, Peer Eysel, David Grevenstein; Resources: Sönke Reineck, Thomas Steimel; Supervision: David Grevenstein.
Acknowledgments
None to report.
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
References
[1] | Granan LP, Forssblad M, Lind M, Engebretsen L. The scandinavian ACL registries 2004–2007: Baseline epidemiology. Acta Orthop. (2009) Oct; 80: (5): 563-7. doi: 10.3109/17453670903350107. |
[2] | Lind M, Menhert F, Pedersen AB. The first results from the Danish ACL reconstruction registry: Epidemiologic and 2 year follow-up results from 5,818 knee ligament reconstructions. Knee Surg Sports Traumatol Arthrosc. (2009) Feb; 17: (2): 117-24. doi: 10.1007/s00167-008-0654-3. Epub 2008 Oct 31. |
[3] | Granan LP, Bahr R, Steindal K, Furnes O, Engebretsen L. Development of a national cruciate ligament surgery registry: The Norwegian National Knee Ligament Registry. Am J Sports Med. (2008) Feb; 36: (2): 308-15. doi: 10.1177/0363546507308939. Epub 2007 Nov 7. |
[4] | Sanders TL, Maradit Kremers H, Bryan AJ, Larson DR, Dahm DL, Levy BA, Stuart MJ, Krych AJ. Incidence of anterior cruciate ligament tears and reconstruction: A 21-year population-based study. Am J Sports Med. (2016) Jun; 44: (6): 1502-7. doi: 10.1177/0363546516629944. Epub 2016 Feb 26. |
[5] | Salmon L, Russell V, Musgrove T, Pinczewski L, Refshauge K. Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthroscopy. (2005) Aug; 21: (8): 948-57. doi: 10.1016/j.arthro.2005.04.110. |
[6] | Glogovac G, Schumaier AP, Grawe BM. Return to sport following revision anterior cruciate ligament reconstruction in athletes: A systematic review. Arthroscopy. (2019) Jul; 35: (7): 2222-2230. doi: 10.1016/j.arthro.2019.01.045. |
[7] | Zeng C, Lei G, Gao S, Luo W. Methods and devices for graft fixation in anterior cruciate ligament reconstruction. Cochrane Database Syst Rev. (2018) Jun 29; 2018: (6): CD010730. doi: 10.1002/14651858. |
[8] | Karpinski K, Bierke S, Häner M, Hees T, Petersen W. Quadriceps- vs. semitendinosus tendon in ACL reconstruction – a prospective study comparing autologous transplants regarding their clinical outcome. Orthop J Sports Med. (2020) May 29; 8: (5 suppl4): 2325967120S00287. doi: 10.1177/2325967120S00287. |
[9] | Horstmann H, Petri M, Tegtbur U, Felmet G, Krettek C, Jagodzinski M. Quadriceps and hamstring tendon autografts in ACL reconstruction yield comparably good results in a prospective, randomized controlled trial. Arch Orthop Trauma Surg. (2022) Feb; 142: (2): 281-289. doi: 10.1007/s00402-021-03862-8. |
[10] | Jenkins SM, Guzman A, Gardner BB, Bryant SA, Del Sol SR, McGahan P, Chen J. Rehabilitation after anterior cruciate ligament injury: Review of current literature and recommendations. Curr Rev Musculoskelet Med. (2022) Jun; 15: (3): 170-179. doi: 10.1007/s12178-022-09752-9. |
[11] | Buerba RA, Boden SA, Lesniak B. Graft selection in contemporary anterior cruciate ligament reconstruction. J Am Acad Orthop Surg Glob Res Rev. (2021) Oct 25; 5: (10): e21.00230. doi: 10.5435/JAAOSGlobal-D-21-00230. |
[12] | Dong YL, Cai CY, Jiang GY, Qian YN, Yang GJ. Femoral tunnel positioning using an anteromedial technique for ACL reconstruction: A radiographic study with a cadaveric model. Technol Health Care. (2017) Aug 9; 25: (4): 729-737. |
[13] | Blythe A, Tasker T, Zioupos P. ACL graft constructs: In-vitro fatigue testing highlights the occurrence of irrecoverable lengthening and the need for adequate (pre)conditioning to avert the recurrence of knee instability. Technol Health Care. (2006) ; 14: (4-5): 335-47. |
[14] | Park JS, Nam DC, Kim DH, Kim HK, Hwang SC. Measurement of knee morphometrics using MRI: A comparative study between ACL-injured and non-injured knees. Knee Surg Relat Res. (2012) Sep; 24: (3): 180-5. doi: 10.5792/ksrr.2012.24.3.180. Epub 2012 Sep 3. |
[15] | Anderson AF, Lipscomb AB, Liudahl KJ, Addlestone RB. Analysis of the intercondylar notch by computed tomography. Am J Sports Med. (1987) Nov-Dec; 15: (6): 547-52. doi: 10.1177/036354658701500605. |
[16] | Dienst M, Schneider G, Altmeyer K, Voelkering K, Georg T, Kramann B, Kohn D. Correlation of intercondylar notch cross sections to the ACL size: A high resolution MR tomographic in vivo analysis. Arch Orthop Trauma Surg. (2007) May; 127: (4): 253-60. doi: 10.1007/s00402-006-0177-7. Epub 2006 Jun 21. |
[17] | Fridén T, Jonsson A, Erlandsson T, Jonsson K, Lindstrand A. Effect of femoral condyle configuration on disability after an anterior cruciate ligament rupture. 100 patients followed for 5 years. Acta Orthop Scand. (1993) Oct; 64(5): 571-4. doi: 10.3109/17453679308993695. |
[18] | Eggerding V, van Kuijk KS, van Meer BL, Bierma-Zeinstra SM, van Arkel ER, Reijman M, Waarsing JH, Meuffels DE. Knee shape might predict clinical outcome after an anterior cruciate ligament rupture. Bone Joint J. (2014) Jun; 96-B: (6): 737-42. doi: 10.1302/0301-620X.96B6.32975. |
[19] | Fernandes MS, Pereira R, Andrade R, Vasta S, Pereira H, Pinheiro JP, Espregueira-Mendes J. Is the femoral lateral condyle’s bone morphology the trochlea of the ACL? Knee Surg Sports Traumatol Arthrosc. (2017) Jan; 25: (1): 207-214. doi: 10.1007/s00167-016-4159-1. Epub 2016 May 9. |
[20] | Wahl CJ, Westermann RW, Blaisdell GY, Cizik AM. An association of lateral knee sagittal anatomic factors with non-contact ACL injury: Sex or geometry? J Bone Joint Surg Am. (2012) Feb 1; 94: (3): 217-26. doi: 10.2106/JBJS.K.00099. |
[21] | Gaillard R, Magnussen R, Batailler C, Neyret P, Lustig S, Servien E. Anatomic risk factor for meniscal lesion in association with ACL rupture. J Orthop Surg Res. (2019) Jul 30; 14: (1): 242. doi: 10.1186/s13018-019-1281-z. |
[22] | Hohmann E, Bryant A, Reaburn P, Tetsworth K. Is there a correlation between posterior tibial slope and non-contact anterior cruciate ligament injuries? Knee Surg Sports Traumatol Arthrosc. (2011) Dec; 19: (Suppl 1): S109-14. doi: 10.1007/s00167-011-1547-4. Epub 2011 May 24. |
[23] | Zeng C, Cheng L, Wei J, Gao SG, Yang TB, Luo W, Li YS, Xu M, Lei GH. The influence of the tibial plateau slopes on injury of the anterior cruciate ligament: A meta-analysis. Knee Surg Sports Traumatol Arthrosc. (2014) Jan; 22: (1): 53-65. doi: 10.1007/s00167-012-2277-y. Epub 2012 Nov 1. |
[24] | Napier RJ, Garcia E, Devitt BM, Feller JA, Webster KE. Increased radiographic posterior tibial slope is associated with subsequent injury following revision anterior cruciate ligament reconstruction. Orthop J Sports Med. (2019) Nov 5; 7: (11): 2325967119879373. doi: 10.1177/2325967119879373. |
[25] | Dejour D, Saffarini M, Demey G, Baverel L. Tibial slope correction combined with second revision ACL produces good knee stability and prevents graft rupture. Knee Surg Sports Traumatol Arthrosc. (2015) Oct; 23: (10): 2846-52. doi: 10.1007/s00167-015-3758-6. |
[26] | Imhoff FB, Comer B, Obopilwe E, Beitzel K, Arciero RA, Mehl JT. Effect of slope and varus correction high tibial osteotomy in the ACL-deficient and ACL-reconstructed knee on kinematics and ACL graft force: A biomechanical analysis. Am J Sports Med. (2021) Feb; 49: (2): 410-416. doi: 10.1177/0363546520976147. |
[27] | Dargel J, Schmidt-Wiethoff R, Feiser J, Koebke J, Schlüter-Brust K, Eysel P, Michael JW. Relationship between human femorotibial joint configuration and the morphometry of the anterior cruciate ligament. Arch Orthop Trauma Surg. (2011) Aug; 131: (8): 1095-105. doi: 10.1007/s00402-011-1345-y. Epub 2011 Jul 8. |
[28] | Siebold R, Axe J, Irrgang JJ, Li K, Tashman S, Fu FH. A computerized analysis of femoral condyle radii in ACL intact and contralateral ACL reconstructed knees using 3D CT. Knee Surg Sports Traumatol Arthrosc. (2010) Jan; 18: (1): 26-31. doi: 10.1007/s00167-009-0969-8. Erratum in: Knee Surg Sports Traumatol Arthrosc. 2010 Apr; 18(4): 554. Li, Kanglai [corrected to Li, Kang]. |
[29] | Kostogiannis I, Ageberg E, Neuman P, Dahlberg LE, Fridén T, Roos H. Clinically assessed knee joint laxity as a predictor for reconstruction after an anterior cruciate ligament injury: A prospective study of 100 patients treated with activity modification and rehabilitation. Am J Sports Med. (2008) Aug; 36: (8): 1528-33. doi: 10.1177/0363546508317717. Epub 2008 Jun 10. |
[30] | Kapandji IA. Funktionelle Anatomie der Gelenke, 5th edn. Thieme Verlag 2008, Stuttgart, p 72–73, 80–81, 89, 162p (in German). |
[31] | Kostogiannis I, Swärd P, Neuman P, Fridén T, Roos H. The influence of posterior-inferior tibial slope in ACL injury. Knee Surg Sports Traumatol Arthrosc. (2011) Apr; 19: (4): 592-7. doi: 10.1007/s00167-010-1295-x. Epub 2010 Oct 21. |
[32] | Hendrix ST, Barrett AM, Chrea B, Replogle WH, Hydrick JM, Barrett GR. Relationship between posterior-inferior tibial slope and bilateral noncontact ACL injury. Orthopedics. (2017) Jan 1; 40: (1): e136-e140. doi: 10.3928/01477447-20161013-06. Epub 2016 Oct 18. |
[33] | Goetz-Neumann K. Gehen Verstehen-Ganganalyse in der Physiotherapie. 4rd ed. Stuttgart: Thieme 2003 (in German). |
[34] | Minervini G, Del Mondo D, Russo D, Cervino G, D’Amico C, Fiorillo L. Stem cells in temporomandibular joint engineering: State of art and future persectives. J Craniofac Surg. (2022) Oct 1; 33: (7): 2181-2187. doi: 10.1097/SCS.0000000000008771. |


