
A study of the effects of hydroxyapatite bioceramic extract on Ang/Tie2 system of umbilical vein endothelial cells
Abstract
OBJECTIVE:
We aimed to investigate the effects of hydroxyapatite bioceramic extract on Ang/Tie2 system and cell proliferation of umbilical vein endothelial cells.
METHODS:
Human umbilical vein endothelial cells (HUVECs) were used in this research. There are two induvial groups, control group and hydroxyapatite bioceramics extract treatment group. Cell Counting Kit-8 (CCK-8) was used to evaluate cell proliferation. Western blot and real time quantitative PCR (Q-PCR) were used to evaluate the protein and mRNA expression levels of Ang1, Ang2 and Tie2 in Ang/Tie2 system, respectively. All the results were statistically analyzed by Spss19.0. All data were presented as mean
RESULTS:
Hydroxyapatite bioceramics extract showed no effect on the cell morphology and cell proliferation of HUVECs. Interestingly, we found that both Ang2 and Tie2 protein and mRNA level were markedly increased by hydroxyapatite bioceramics extract.
CONCLUSIONS:
Hydroxyapatite bioceramic extract showed no cytotoxicity to HUVECs, and might regulate vascular remodeling by mediating Ang/Tie2 system.
1.Introduction
Bone defect repair is a major and important issue in the clinical work of oral cavity. The alveolar bone of adult orthodontic patients is thin, which causes the maxillary sinus easily perforating through the maxillary sinus bottom wall. Bone regeneration is need to be taken in the bone defect site of the implant area and the alveolar bone absorption place which are caused by multiple reasons [1]. Additionally, bone regeneration allows clinicians to place implants or miniscrews with greater diameter and length, thus allowing better clinical performance and durability over time [2, 3]. With the development of materials science, clinicians gradually use bone graft materials instead of autologous bone for small-scale bone grafting, and have achieved good bone regeneration effect [4].
Hydroxyapatite bioceramics is one kind of widely used bone graft materials. The main component of Hydroxyapatite bioceramics is hydroxyapatite (HA) that is similar to inorganic materials in biological bone tissue [5]. It has been reported that hydroxyapatite bioceramics, as a bone graft material and with certain biocompatibility, could increase the bone thickness and density of alveolar bone [6].
The vascular system can provide oxygen and nutrition for the regenerated tissue and maintain the growth of the tissue. Therefore, vascular remodeling is an essential procedure during the formation of bone tissue. Tissue necrosis and poor tissue formation can be caused by the insufficient blood supply or slow angiogenesis [7]. Vascular tissue reconstruction is closely related to the proliferation of vascular endothelial cells. It has been found that angiopoietin/tyrosine kinase receptors 2 (Ang/Tie2) system plays a critical role in maintaining vascular maturity and stability, as well as repairing microcirculation after vascular injury [8]. Until now, the effect of hydroxyapatite bioceramics on the proliferation and Ang/Tie2 system of human umbilical vein endothelial cells (HUVECs) has not been reported yet. Here, in this study, firstly, we found that hydroxyapatite bioceramic extract showed no cytotoxicity to HUVECs, and might regulate vascular remodeling by mediating Ang/Tie2 system.
2.Materials and methods
2.1Reagents and instruments
Hydroxyapatite bioceramics (synthetized by Beijing Yihuajian science and Trade Co., Ltd., China), endothelial cell culture medium ECM (1001, ScienCell, USA), Potassium phosphate buffer (PBS) (SH30256 01B, Hyclone, USA), clean bench (sw-cj-ifd, Suzhou Antai, China), low-speed centrifuge (sc3614, Zhongjia, China), inverted optical microscope (CKX41, Olympus, Japan), cell incubator (Heracell 150i, Thermo Scientific, USA) and CCK-8 solution (Kga317, Jiangsu Kaiji, China), plate reader (Multiscan MK3, Thermo Fisher Scientific, USA ), Ang1 and Tie2 antibody (251671, Beijing Zen bio, China), Ang2 antibody (24613-1-ap, Proteintech, USA), RIPA buffer (P0013B, Shanghai Beyotime, China), secondary antibody (111-035-003, Jackson ImmunoResearch, USA), luminescent solution (wbkls0500, Millipore, USA), BCA Protein Assay Kit (PA115, Beijing Tiangen, China), PVDF membrane (ipvh00010, Millipore, USA), TRIzol reagent (1556018, Invitrogen, USA), SYBR GREEN qPCR Super Mix (C11733046, Invitrogen, USA), fluorescent PCR (1725274, ABI, USA).
2.2Methods
2.2.1Groups
There are two induvial groups, control group and hydroxyapatite bioceramics extract treatment group. Control group is HUVECs alone, and hydroxyapatite bioceramics extract treatment group is defined as experimental group.
2.2.2Hydroxyapatite bioceramics extract preparation
The concentration of hydroxyapatite bioceramics extract solution was prepared according to the protocol in part 12 of iso10993.12-2008 biological evaluation of medical devices. Briefly, 0.2 g hydroxyapatite bioceramics was dissolved into 1 ml complete culture medium and extracted in an inert container at 37
2.2.3Cell STR identification
Umbilical vein endothelial cell line was purchased from Shanghai FUHENG Biotechnology Co., Ltd. Briefly, total DNA was extracted by axygen genomic extraction kit and amplified according to 21-str amplification protocol. The STR locus and sex gene amelogenin were detected by using genetic analyzer (ABI 3730xl, Thermo Scientific, USA). The results showed that there were no multiple alleles which indicates the good quality of cell typing.
Table 1
RT-PCR primer sequences for target genes and reference gene
| Gene name | Primer sequence |
|---|---|
| Ang1 | F:5’-TGCTGATAATGACAACTGTA-3’ |
| R:5’-AAGGTCGAATCATCATAGTT-3’ | |
| Ang2 | F:5’-GAGAATATTGGCTGGGAAAT-3’ |
| R:5’-CCTGTAAGTCCTTTAAGGTG-3’ | |
| Tie2 | F:5’-TTATGAGAGGCCATCATTTG-3’ |
| R:5’-CTCATAAAGCGTGGTATTCA-3’ | |
| GAPDH | F:5’-GGGAAACTGTGGCGTGAT-3’ |
| R:5’-GAGTGGGTGTCGCTGTTGA-3’ |
2.2.4Cell culture
HUVECs were cultured in endothelial cell culture medium ECM. Under normal conditions, cells were cultured at 37
2.2.5Cell viability assay
HUVECs cells were plated at 8,000/well in 96-well plates, and cell viability assay was assessed on the indicated time points (Day1, Day3, Day5 and Day7) according to the manufacturer’s instructions (Kga317, Jiangsu Kaiji, China). Cell viability was expressed as the percentage of viable cells relative to untreated cells using the absorbance at 450 nm and absorbance was measured using auto microplate reader. All experiments were performed in three individual experiments.
2.2.6Western blot
Total proteins were extracted from HUVECs by using cell lysis buffer and passed the tissue through a 21-gauge needle more than 30 times. The cell lysate was centrifuged at 4
2.2.7Real-time PCR
Total mRNA of HUVECs was extracted by using TRIzol reagent according to the manufacturer’s protocols. The concentration of mRNA wad detected by BioPhotometers plus (Eppendorf, Germany). The quantitative real-time PCR using SYBR GREEN qPCR Super Mix was performed in ABI one step Plus (1725274, ABI, USA). All experiments were performed in nine individual experiments. All primers are listed in Table 1.
2.3Statistical treatment
Spss19.0 statistical software (IBM, USA) was used to analyze the data. All data were presented as mean
3.Results
3.1Hydroxyapatite bioceramics extract showed no effect on the cell morphology of HUVECs
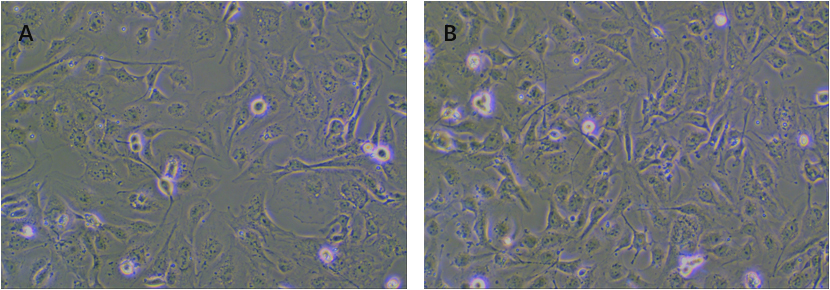
We first test the effect of hydroxyapatite bioceramics extract on the cell morphology of HUVECs. The images were captured by inverted microscope. As shown in Fig. 1A and B, the cell morphology of both control group and hydroxyapatite bioceramics extract treatment group (48 h) showed the “paving stone” shape, which was reflected by spindle shaped and small angle shaped (as shown by the white arrow).
Figure 1.
The morphology shape of HUVECs (A) the morphology of HUVECs in control group (B) the morphology of HUVECs in hydroxyapatite bioceramic extract treatment group.
3.2The effect of hydroxyapatite bioceramics extract on cell proliferation of human HUVECs
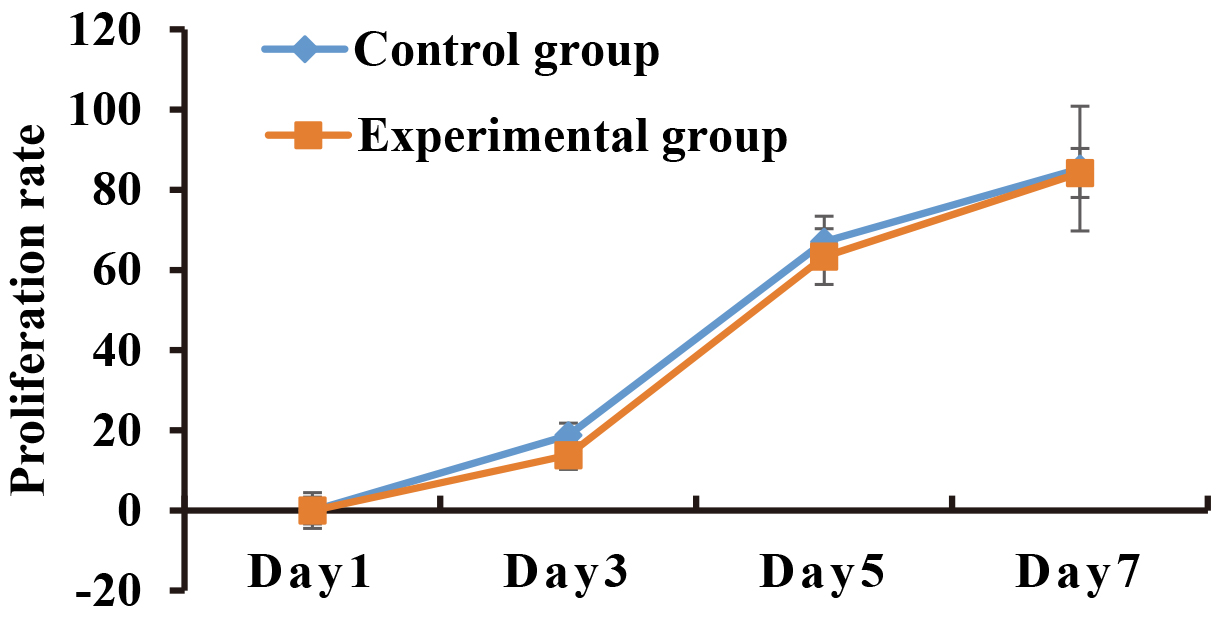
To investigate whether hydroxyapatite bioceramics extract could affect the viability of HUVECs, cell proliferation was assessed by CCK-8 assay after hydroxyapatite bioceramics extract treatment at the indicated time points (Day1, Day3, Day5 and Day7). The results in Fig. 2 showed that there was no significant difference in cell proliferation rate between control and hydroxyapatite bioceramics extract treatment group (
Figure 2.
Cell proliferation curve. HUVECs were treated with hydroxyapatite bioceramic extract for the indicated time points (Day1, Day3, Day5 and Day7), and then assessed by CCK-8 assay.
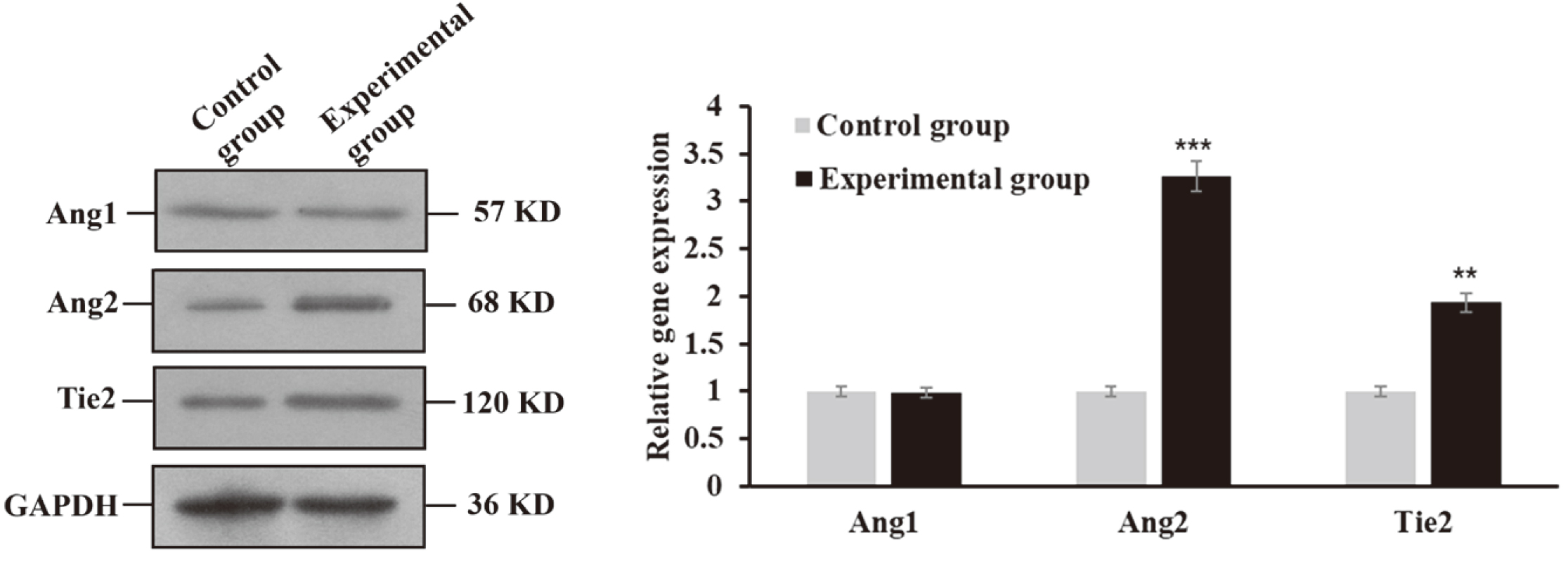
3.3The protein levels of Ang2 and Tie2 were up-regulated by hydroxyapatite bioceramic extract
Evidence suggests that the Ang/Tie2 signaling pathway is essential for maintaining vascular homeostasis, and its dysregulation is associated with several diseases [10]. Until now, the relevance between hydroxyapatite bioceramic extract and Ang/Tie2 is unkown, therefore, it is of great interest to investigate whether hydroxyapatite bioceramic extract could affect Ang/Tie2 signaling pathway. Data in Fig. 3 showed that there was no significant difference in the protein level of Ang1 (
Figure 3.
Ang2 and Tie2 were up-regulated by hydroxyapatite bioceramic extract (**
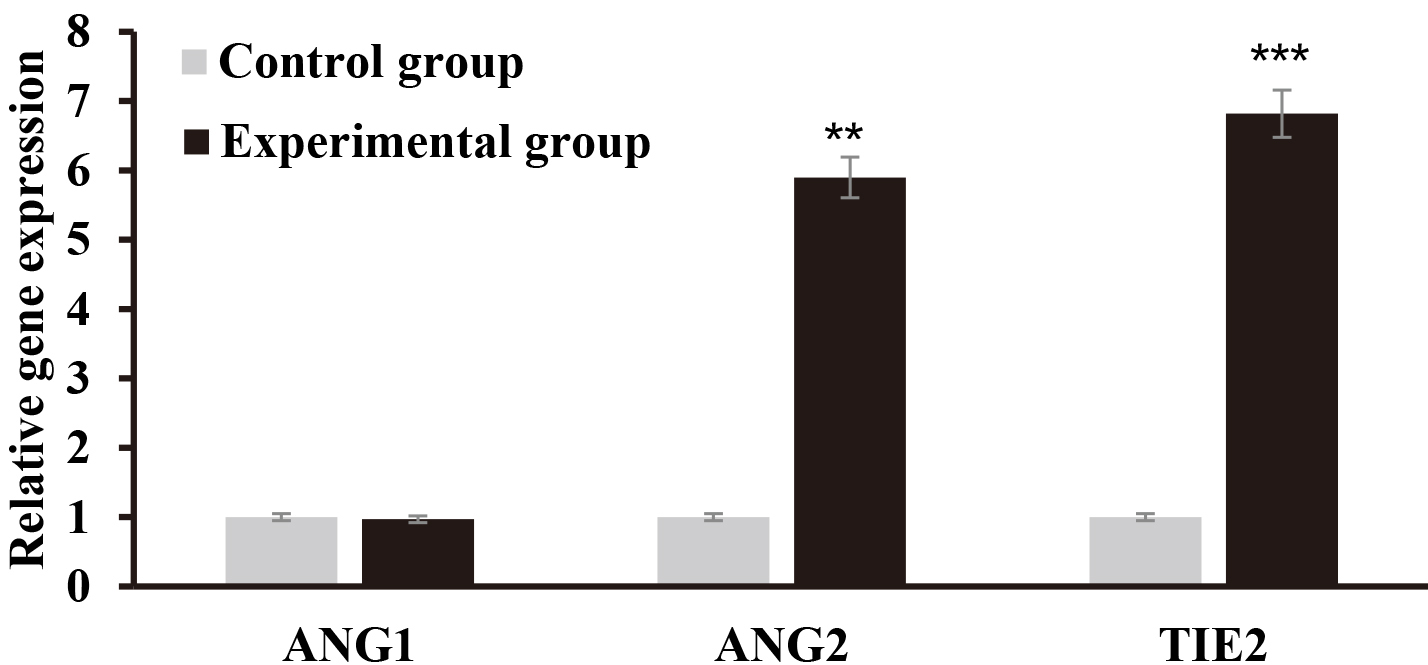
3.4The transcriptional level of ANG2 and TIE2 were up-regulated by hydroxyapatite bioceramic extract
Consistently, the results of real-time quantitative PCR in Fig. 4 showed that there was no significant difference in the transcriptional level of ANG1 (
Figure 4.
The transcriptional level of ANG2 and TIE2 were up-regulated by hydroxyapatite bioceramic extract (**
4.Discussion
Bone tissue defect, which is caused by tissue defect, maxillofacial trauma, congenital malformation, tumor or alveolar bone defect, is a very common phenomenon in stomatology [1]. Bone regeneration allows clinicians to place implants or miniscrews with greater diameter and length, thus allowing better clinical performance and durability over time [2, 3]. Recently, with the development of bone regeneration in surgery technology and bone substitute implantation, hydroxyapatite bioceramic has been widely used in clinical research. Hydroxyapatite bioceramic is mostly composed of hydroxyapatite which is about 90%, and the chemical composition it is similar to that of inorganic components in bone tissue. In oral clinic, it is commonly used in maxillary sinus elevation surgery and implantation bone defect repair. It has been reported that Fu as a bone implant material has a good effect on osteogenic [11]. Nowadays studies have demonstrated that hydroxyapatite-based biomimetic solutions are active for enamel and dentin remineralization but the reconstruction of hard tissues is still an open challenge [12, 13].
Vascular remodeling is an essential procedure during the formation of bone tissue. Lack of blood supply and reconstruction can cause tissue undernutrition and necrosis during tissue repair process [14]. Moreover, too large size of the implanted tissue, which only relies on the neighborhood blood vessels to get nutrients, will suffer insufficient blood supply and undernutrition in vivo. Therefore, good blood cell compatibility, without cytotoxicity and promoting angiogenesis are the basal requirements of the bone graft materials. Therefore it is of great interest to investigate the effect of hydroxyapatite bioceramics on angiogenesis during bone regeneration.
Vascular remodeling is initiated by multiple cytokines, including angiopoietins like Ang1 and Ang2, VEGF, as well as TNF-
5.Conclusion
In this study, we firstly found that hydroxyapatite bioceramic extract, without cytotoxicity to HUVECs, can increase both Ang2 and Tie2 protein and mRNA levels, which hints that under hydroxyapatite bioceramic extract treatment condition, Ang2, here, may act as an agonist of Tie2, which might regulate vascular remodeling through Ang/Tie2 signaling. Therefore, the underling mechanism of how hydroxyapatite bioceramic extract regulates vascular remodeling needs further to be elucidated.
Conflict of interest
The authors state that there is no conflict of interest related to this article.
References
[1] | Liu Y, Li Z, Gong J, et al. Study on the application of autogenous dental bone powder in oral and maxillofacial bone defects. Journal of Clinical Stomatology. (2018) ; 34: (6): 375-377. |
[2] | Sfondrini M, Gandini P, Alcozer R, et al. Failure load and stress analysis of orthodontic miniscrews with different transmucosal collar diameter. J Mech Behav Biomed Mater. (2018) ; 87: : 132-137. |
[3] | Cenkoglu BG, Balcioglu NB, Ozdemir T, et al. The Effect of the length and distribution of implants for fixed prosthetic reconstructions in the atrophic posterior maxilla: A finite element analysis. Materials (Basel). (2019) ; 12: (16): 2556. |
[4] | Zhao G, Yao Y, Xu G, et al. Preventive effect of BIOSs bone powder on postoperative complications and alveolar bone mineral density of mandibular horizontal impacted teeth. Chinese Journal of aesthetic medicine. (2019) ; 28: (12): 142-145. |
[5] | Liu M, Qi M. Research progress of repair materials for oral and maxillofacial bone defects. Journal of general Stomatology. (2019) ; 6: (6): 57-58. |
[6] | Shu Y. Application effect of platelet rich plasma combined with bio OSS bone powder and Hai’ao biofilm on oral implant bone regeneration in diabetic patients. Journal of Practical Clinical Medicine. (2020) ; 24: (1): 36-38. |
[7] | Wang M, Zou D, Zhou Y, et al. In vitro experimental study on angiogenesis and osteogenic differentiation of canine BMSCs induced by mir-210. Journal of Anhui Medical University. (2016) ; 51: (9): 1258-1262. |
[8] | Haase K, Gillrie MR, Hajal C, et al. Pericytes Contribute to Dysfunction in a Human 3D Model of Placental Microvasculature through VEGF-Ang-Tie2 Signaling. Adv Sci (Weinh). (2019) ; 6: (23): 1900878. |
[9] | Guo W, Hao B, Wang Q, et al. Requirement of B-Raf, C-Raf, and A-Raf for the growth and survival of mouse embryonic stem cells. Exp Cell Res. (2013) ; 319: (18): 2801-2811. |
[10] | Mirando AC, Shen J, Silva RLE, et al. A collagen IV-derived peptide disrupts α5β1 integrin and potentiates Ang2/Tie2 signaling. JCI Insight. (2019) ; 4: (4): e122043. |
[11] | Nazirkar G, Singh S, Dole V, et al. Effortless effort in bone regeneration: a review. J Int Oral Health. (2014) ; 6: (3): 120-124. |
[12] | Scribante A, Dermenaki Farahani MR, Marino G, et al. Biomimetic effect of nano-hydroxyapatite in demineralized enamel before orthodontic bonding of brackets and attachments: Visual, adhesion strength, and hardness in in vitro tests. Biomed Res Int. (2020) ; 2020: : 6747498. |
[13] | Bächli K, Schmidlin PR, Wegehaupt F, et al. Remineralization of artificial dentin caries using dentin and enamel matrix proteins. Materials (Basel). (2019) ; 12: (13): 2116. |
[14] | Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: a systematic review. J Clin Periodontol. (2008) ; 35: : 136-162. |
[15] | Augustin HG, Koh GY, Thurston G, et al. Control of vascular morphogenesis and homeostasis through the angiopoietin-Tie system. Nat Rev Mol Cell Biol. (2009) ; 10: (3): 165-177. |
[16] | Baluk P, Yao LC, Feng J, et al. TNF-alpha drives remodeling of blood vessels and lymphatics in sustained airway inflammation in mice. J Clin Invest. (2009) ; 119: (10): 2954-2964. |
[17] | Lee CG, Link H, Baluk P, et al. Vascular endothelial growth factor (VEGF) induces remodeling and enhances TH2-mediated sensitization and inflammation in the lung. Nat Med. (2004) ; 10: (10): 1095-1103. |
[18] | Tabruyn SP, Colton K, Morisada T, et al. Angiopoietin-2-driven vascular remodeling in airway inflammation. Am J Pathol. (2010) ; 177: (6): 3233-3243. |
[19] | Sato TN, Tozawa Y, Deutsch U. Distinct roles of the receptor tyrosine kinases Tie-1 and Tie-2 in blood vessel formation. Nature. (1995) ; 376: (6535): 70-74. |
[20] | Suri C, Jones PF, Patan S. et al. Requisite role of angiopoietin-1, a ligand for the TIE2 receptor, during embryonic angiogenesis. Cell. (1996) ; 87: (7): 1171-1180. |
[21] | Yancopoulos GD, Davis S, Gale NW, et al. Vascular-specific growth factors and blood vessel formation. Nature. (2000) ; 407: (6801): 242-248. |
[22] | Maisonpierre PC, Suri C, Jones PF, et al. Angiopoietin-2, a natural antagonist for Tie2 that disrupts in vivo angiogenesis. Science. (1997) ; 277: (5322): 55-60. |
[23] | Benest AV, Kruse K, Savant S, et al. Angiopoietin-2 is critical for cytokine-induced vascular leakage. PLoS One. (2013) ; 8: (8): e70459. |
[24] | Ziegler T, Horstkotte J, Schwab C, et al. Angiopoietin 2 mediates microvascular and hemodynamic alterations in sepsis. J Clin Invest. (2013) ; 123: (8): 3436-3445. |
[25] | Daly C, Pasnikowski E, Burova E, et al. Angiopoietin-2 functions as an autocrine protective factor in stressed endothelial cells. Proc Natl Acad Sci U S A. (2006) ; 103: (42): 15491-15496. |
[26] | Davis S, Papadopoulos N, Aldrich TH, et al. Angiopoietins have distinct modular domains essential for receptor binding, dimerization and superclustering. Nat Struct Biol. (2003) ; 10: (1): 38-44. |
[27] | Scharpfenecker M, Fiedler U, Reiss Y, et al. The Tie-2 ligand angiopoietin-2 destabilizes quiescent endothelium through an internal autocrine loop mechanism. J Cell Sci. (2005) ; 118: (Pt 4): 771-780. |
[28] | Yuan HT, Khankin EV, Karumanchi SA, et al. Angiopoietin 2 is a partial agonist/antagonist of Tie2 signaling in the endothelium. Mol Cell Biol. (2009) ; 29: (8): 2011-2022. |
[29] | Kim M, Allen B, Korhonen EA, et al. Opposing actions of angiopoietin-2 on Tie2 signaling and FOXO1 activation. J Clin Invest. (2016) ; 126: (9): 3511-3525. |


