
Occupational radiation exposure of orthopedists at different locations during pedicle screw insertion: An anthropomorphic phantom study
Abstract
BACKGROUND:
The purpose of this work was to evaluate orthopedic surgeons’ exposure to occupational radiation doses from scattering using a mobile flat panel C-arm X-ray machine at different standing positions during an intraoperative pedicle screw implantation.
OBJECTIVE:
Evaluate the radiation dose received by medical staff, by applying flat X-ray machine in surgical room during an intraoperative pedicle screw implantation.
METHODS:
A mobile flat-panel C-arm X-ray machine at a dedicated orthopedic operating room was used to image an anthropomorphic female phantom which was set in a prone position on the operating table. The X-ray was projected horizontally, and 1 minute continuous fluoroscopy was used for lumbar spine and thoracolumbar spine during pedicle screw implantation. Scattering radiation doses to orthopedic surgeons were measured at different standing positions and body heights (50, 100, 150 cm above the ground) with and without limited collimations.
RESULTS:
The dose area product (DAP) in this experiment is normalized as 343
CONCLUSIONS:
Using a mobile flat-panel C-arm X-ray machine during a pedicle screw implantation, the minimum scattering radiation to surgeons was found to be at the terminal DF area based on the analysis of the scattering doses orthopedic surgeons were exposed to.
1.Introduction
The mobile C-Arm fluoroscopy is frequently used in orthopedic surgeries. X-ray is applied to ensure the accuracy of pedicle screw insertion (PSI) and percutaneous vertebroplasty (PVP) [1]. During PSI, the screw is inserted along the pedicle and kept away from spine cord and vertebrae. As a pedicle is surrounded by blood vessels and nerves, the screw may be mistakenly inserted to the intervertebral foramen and result in cerebrospinal fluid leakage, if without X-ray fluoroscopy [2]. Previous researches have pointed out that the error rate of PSI without X-ray is 12.7% to 16.7 [3, 4], and the rate of nerve damage reaches up to 40% [4]. To improve the accuracy of PSI, fluoroscopy becomes a necessity, which will cause an increase in occupational radiation exposure of orthopedists.
With the development of medical imaging, X-ray is more widely used, and accompanying cancer risk on doctors is also increasing, which has aroused debates [5]. Thanks to fluoroscopy X-ray, the accuracy on spinal surgeries is improved [6], and spinal surgeries are easier to be conducted [7, 8, 9, 10, 11]. However, the risk of radiation exposure on orthopedist increases. To decrease the occupational radiation exposure and possible cancer risk on doctors, operators of X-ray machines should lower the necessary dose for examination, and doctors should obey As Low as Reasonably Achievable (ALARA) [12] during surgeries using fluoroscopy X-ray.
In this article, the Alderson Radiation Therapy (ART) phantom is used to simulate clinical scattered radiation impact in PSI. The doses of radiation exposure in TH, TF, DH and DF sides are measured and discussed. The examine points are 50, 100 and 150 cm above the ground, representing the knees, chest, and thyroid of orthopedist respectively.
2.Materials and methods
2.1ART anthropomorphic phantom
The ART anthropomorphic female phantom is used to simulate a female lying on her stomach. The weight and height are 155 cm and 50 kg respectively. The legs are not counted. The density structure of phantom is highly similar to human bone and soft tissue [13, 14]. Thus, the phantom experiment can reflect the real clinical scattered radiation impact.
2.2Ion chamber dosimeter
The dosimeter adopted is Fluke Biomedical model 660-5DE 400-cc (Everett, USA), and the display unit is
2.3Experiment design and X-ray machine settings
This study was approved by the Chang Gung Memorial Hospital, Taiwan and approval was granted by the Chang Gung Hospital Institutional Review Board under numbers 201601278B0 and 201900121B0. All the data was collected in one surgery room at Kaohsiung Chang Gung Hospital, Taiwan.
The radiation doses received by the orthopedist while using fluoroscopy X-ray in lumbar vertebrae PSI are measured in the same operating room. The phantom is lying on stomach side on operating table with lumbar vertebrae exposed. The position of phantom is fixed despite the change of exposure areas. The position where orthopedist most often stand is shown in Fig. 1. Suppose orthopedist wears 0.5 mmPb lead aprons and lead thyroid shied, and stands as close as possible to the patient. The mobile X-ray machine adopted is Cios Alpha (Siemens AG, Healthcare Sector, Erlangen, Germany). The X-ray is horizontally projected to achieve lateral image of lumbar vertebrae. Orthopedist stands by patient foot side. The X-ray is projected from left to right. The cathode side of the X-ray tube points to ceiling and the anode side of X-ray tube points to the ground. The center of the X-ray projector is 109 cm above the ground. Image plate is 30*30 cm. Anode target angle is 10 degree. Focal length is 0.3 and the original filter is 3 mmAl/0.1 mm Cu. Detector pulse is 40 nGy. The fluoroscopy is under automatic dose rate control (ADR) and automatic exposure control (AEC). The system automatically adjusts the kV/mA and kV/mAs value. The X-ray protects continuously for 10 seconds. And the scattered radiation doses in TH, TF, DH and DF are measured.
Figure 1.
The X-ray machine settings.

2.4The measure points of scattered radiation
To measure the scattered radiation dose on orthopedist during surgery, we chose the measure point 50 cm away from patient skin, and 80 cm away from tube shell and plate. As shown in Fig. 2, a square of 40*40 cm on the ground is marked as the orthopedist standing point during surgery. The scattered radiation measure section is from TH to TF and DH to DF. The observer stands by the patient foot side. The X-ray is horizontally projected from left to right. The red point is the measure point.
Figure 2.
Scattered radiation experiment using ART phantom.
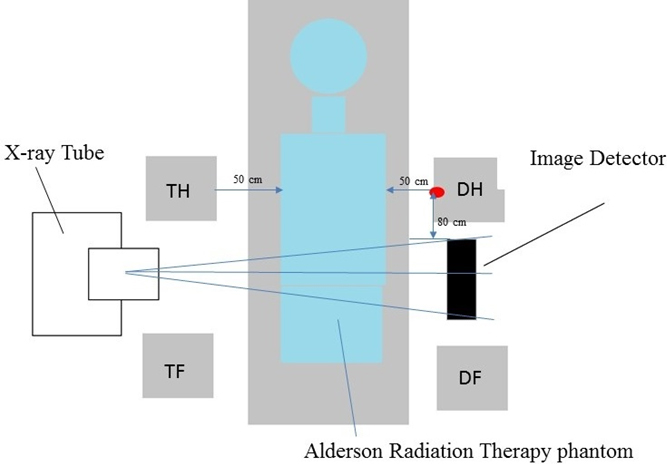
Figure 3.
The orthopedic surgeon’s standing positions during surgery.
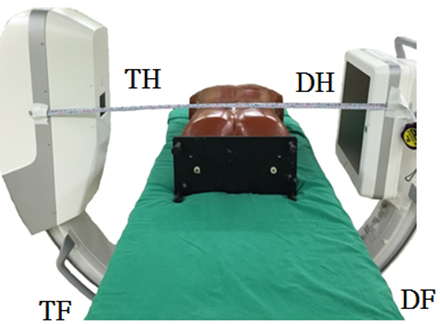
As shown in Fig. 3, the operation desk is 100 cm above the ground, which satisfies the requirement of surgery and lowest height of C-arm horizontal projection. In four sections, the scattered radiation doses are measured separately in front of lead suit and in the lead suit. The measure points are 50 cm, 100 cm and 150 cm above the ground, representing knees, chest and thyroid respectively. The measurements repeated for five times. We compared the radiation exposure differences when using the full X-ray projection area of 40 m
2.5Statistical analysis
The scattered radiation doses on the X-ray tube side and image detector side were compared using paired
3.Results
The research adopted ART phantom to simulate scattered radiation received by orthopedist during spine surgeries. The measure point is 50 cm away from patient skin, and 50 cm, 100 cm, and 150 cm above the ground, representing the knee, chest and thyroid respectively. The X-ray is horizontally projected. The radiation doses inside and outside the 0.5 mmPb lead suit are measured. The nature background radiation in operation room is 0.06
Table 1
Radiation dose in different sections
| Height | Tube voltage | Without protection of lead suit | With protection of lead suit | Attenuation rate | |
|---|---|---|---|---|---|
| Location | (cm) | ev | (%) | ||
| TH | 50 | 93 | 9.9 | 0.4 | 96.0% |
| 100 | 93 | 116.3 | 1.1 | 99.1% | |
| 150 | 93 | 68.9 | 17.8 | 74.2% | |
| TF | 50 | 93 | 4.5 | 0.2 | 95.6% |
| 100 | 93 | 128.0 | 1.4 | 98.9% | |
| 150 | 93 | 88.5 | 15.0 | 83.1% | |
| DH | 50 | 93 | 5.2 | 0.4 | 92.3% |
| 100 | 93 | 5.2 | 0.3 | 94.2% | |
| 150 | 93 | 24.7 | 3.3 | 86.6% | |
| DF | 50 | 93 | 6.6 | 0.4 | 93.9% |
| 100 | 93 | 4.7 | 0.3 | 93.6% | |
| 150 | 93 | 22.2 | 1.3 | 94.1% |
Table 2
Paired
| Location area | Paired |
|---|---|
| Tube and image detector | |
| DF–TH | |
| DF–DH | |
| DF–TF |
The estimated air kerma dose can be calculated by a simplified version of Eqs (1)–(4):
(1)
(2)
(3)
(4)
Table 3
The difference of radiation doses between full X-ray projection area and controlled X-ray projection area 150 cm above the height
| Height | Tube voltage | Without protection of lead suit | With protection of lead suit | Attenuation rate | |
|---|---|---|---|---|---|
| Location | (cm) | ev | (%) | ||
| TH | 150 | 93 | 68.9 | 17.8 | 74.20% |
| 104 | 85.2 | 19.8 | 76.80% | ||
| TF | 150 | 93 | 88.5 | 15.0 | 83.10% |
| 104 | 102.2 | 20.4 | 80.00% | ||
| DH | 150 | 93 | 24.7 | 3.3 | 86.60% |
| 104 | 25.3 | 1.3 | 94.90% | ||
| DF | 150 | 93 | 22.2 | 1.3 | 94.10% |
| 104 | 20.0 | 1.7 | 91.50% |
The controlled X-ray projection area can improve the image contrast, however the scattered radiation is increased. Table 3 shows the difference of radiation doses between the full X-ray projection area and controlled X-ray projection area at the point 150 cm above the height. If the tube voltage in controlled X-ray projection area increases, the scattered radiation is more penetrable, and radiation dose in TF is the most. The scattered radiation inside lead suit in TH section in the controlled X-ray projection is 17.8 Sv, while in uncontrolled one is 19.8 Sv; in TF the rate is 15.0:20.4 Sv; in DH the rate is 3.3:1.3 Sv; in DF the rate is 1.3:1.7 Sv. Use the paired
4.Discussion
The research studied the scattered radiation dose received by orthopedists during spinal surgery using horizontal fluoroscopy X-ray machine. The experiment adopts ART phantom to simulate real clinical exposure environment and patient posture. The observer stood by the patient’s feet, and the X-ray was horizontally projected from left to right. The scattered radiation dose may change with settings of X-ray exposure and the size of phantom. So, the experiments were conducted in the same operation room to avoid errors. This research focuses only on scattered radiation dose received by orthopedists during horizontal fluoroscopy on lumbar vertebra, because the scattered radiation in lumbar vertebra surgery is higher than surgeries on other body parts.
4.1Comparisons to other studies
Previous researches show that when the X-ray is projected up and down, the radiation exposure with thyroid shields is 1.78 Sv/min while that without thyroid shields is 16.32 Sv/min [15]. Thyroid shields can block 85% of radiation. In our experiment, the X-ray is horizontally projected, and the measure point 150 cm above the ground represents thyroid. As shown in Fig. 1, when wearing the thyroid shied, the block rate on the tube side is 79% and on the image detector side is 90%. In the study by Sung, scattered radiation dose received by the surgeon’s thyroid is 7
Suppose the experiment result is applied in clinic and the radiation in air goes directly to thyroid, orthopedist will receive radiation of 15
4.2The research limitations
In this research, only one type of lead suit is applied, so we did not compare the blocking rates of different types and different materials of protection suits. According to Scuderi et al., lead suit is too heavy to wear, so less heavy materials are proposed to be the substitutes. The blocking rate of three kinds of protection suits using un-lead materials are evaluated under the fluoroscopy X-ray (energy range 60–110 keV). When energy is less than 70 keV, the penetration rate of 0.254 mm lead aprons is 5.4%. The average penetration rate of 0.25 mmPb lead equivalent is 7.1%. When energy is less than 100 keV, the penetration rate of 0.508 mm lead aprons is 5%. The average penetration rate of 0.5 mmPb lead equivalent is 4.9% [18]. The entrance skin dose is not recorded in our X-ray exposure anthropomorphic phantom study. The patient dose can be obtained through a simple conversion formula, which is 0.065 mSv/Gy cm
The limitations in this research have been considered. Firstly, the X-ray machine is under ADR, which is more common in clinical applications. The scattered radiation under manual X-ray is not compared. The body thickness varies per patient. Although the dose can be manually adjusted, the patient will receive more doses in repeated check before the ideal setting is found, which may result in longer surgery and anesthesia duration, and increase the risk. Even though a manual X-ray can reduce the scattered radiation, it prolongs the anesthesia duration and reduces the image quality. So ADR is preferred in clinic rather than manual X-ray. Secondly, the reason why we did not use TLD to collect all scattered radiation in the first exposure is because TLD is unstable when the dosimeter is lower than 1 cGy [20], and is easily influenced by background radiation. In this research, fluoroscopy continuously works for 10 s and the lowest scattered radiation value in front of lead suit is 4.7
5.Conclusions
In this study, we used the lead apron with 0.5 mmPb lead equivalent which only covers the front part of body. The penetration rate is 6.6% at 50 cm above the ground, 3.5% at 100 cm, and 15.5% at 150 cm. At 150 cm, the average controlled fluoroscopy area is 14.2%. The average penetration rate of 0.5 mmPb lead equivalent under 100 keV is 8.2%. Horizontal fluoroscopy X-ray is adopted in spinal surgeries, and the X-ray machine is set as AEC to guarantee image quality. According to the comparison of scattered radiation doses in TH, TF, DH, and DF sections, we conclude that the dose in DF section is lowest. Thus, we suggest that orthopedists should conduct operations in DF section to minimize occupational radiation exposure. Overall, orthopedists receive the least scattered radiation dose when standing in DF section during spinal surgery.
Acknowledgments
This study was supported by the Chang Gung Memorial Hospital (grant numbers: CMRPG8G1561 and CMRPG8J0081), Taiwan. The Chang Gung Hospital Institutional Review Board, Taiwan approved the study (numbers: 201601278B0 and 201900121B0).
Conflict of interest
None to report.
References
[1] | Kim, K.D., Li, W., and Galloway, C.L. Use of a radiopaque localizer grid to reduce radiation exposure. Annals of Surgical Innovation and Research, (2011) . 5: (1): 6. |
[2] | Ammerman, J.M., et al., A prospective evaluation of the role for intraoperative x-ray in lumbar discectomy. Predictors of incorrect level exposure. Surgical Neurology, (2006) . 66: (5): 470–473. |
[3] | Esses, S.I., Sachs, B.L., and Dreyzin, V. Complications associated with the technique of pedicle screw fixation a selected survey of ABS members. Spine, (1993) . 18: (15): 2231–2239. |
[4] | Jones, D.P.G., et al. Radiation exposure during fluoroscopically assisted pedicle screw insertion in the lumbar spine. Spine, (2000) . 25: (12): 1538–1541. |
[5] | Prime, M., et al. The use of ionising radiation in trauma and orthopaedic theatres. Journal of Perioperative Practice, (2010) . 20: (5): 165–172. |
[6] | Ciol, M.A., et al. An assessment of surgery for spinal stenosis: time trends, geographic variations, complications, and reoperations. Journal of the American Geriatrics Society, (1996) . 44: (3): 285–290. |
[7] | Haque, M.U., et al. Radiation exposure during pedicle screw placement in adolescent idiopathic scoliosis: is fluoroscopy safe? Spine, (2006) . 31: (21): 2516–2520. |
[8] | Lieberman, I.H., et al. Assessment of pedicle screw placement accuracy, procedure time, and radiation exposure using a miniature robotic guidance system. Clinical Spine Surgery, (2012) . 25: (5): 241–248. |
[9] | Eaton, D.J., et al. Radiation protection for an intra-operative X-ray device. The British Journal of Radiology, (2011) . 84: (1007): 1034–1039. |
[10] | Chiang, H.-W., et al. Scattered radiation doses absorbed by technicians at different distances from X-ray exposure: experiments on prosthesis. Bio-medical Materials and Engineering, (2015) . 26: (s1): S1641–S1650. |
[11] | Pauwels, R., et al. Effective dose range for dental cone beam computed tomography scanners. European Journal of Radiology, (2012) . 81: (2): 267–271. |
[12] | Rampersaud, Y.R., et al. Radiation exposure to the spine surgeon during fluoroscopically assisted pedicle screw insertion. Spine, (2000) . 25: (20): 2637–2645. |
[13] | Hart, D., and Wall, B. The UK national patient dose database: now and in the future. The British Journal of Radiology, (2003) . 76: (906): 361–365. |
[14] | Kim, S., et al. Kerma area product method for effective dose estimation during lumbar epidural steroid injection procedures: phantom study. American Journal of Roentgenology, (2009) . 192: (6): 1726–1730. |
[15] | Lee, S.Y., et al. Types and arrangement of thyroid shields to reduce exposure of surgeons to ionizing radiation during intraoperative use of C-arm fluoroscopy. Spine, (2013) . 38: (24): 2108–2112. |
[16] | Sung, K., et al. Measurements of surgeons’ exposure to ionizing radiation dose: comparison of conventional and mini C-arm fluoroscopy. Journal of Hand Surgery (European Volume), (2016) . 41: (3): 340–345. |
[17] | Eagan, J., John, T., and Jones, C.T. Cutaneous cancers in an interventional cardiologist: a cautionary tale. Journal of Interventional Cardiology, (2011) . 24: (1): 49–55. |
[18] | Scuderi, G.J., et al. Evaluation of non-lead-based protective radiological material in spinal surgery. The Spine Journal, (2006) . 6: (5): 577–582. |
[19] | Smans, K., Struelens, L., Hoornaert, M.-T., et al. A study of the correlation between dose area product and effective dose in vascular radiology. Radiation Protection Dosimetry, (2008) . 130: (3): 300–308. |
[20] | Gooden, D.S., and Brickner, T., Jr. The routine use of thermoluminescence dosimetry for radiation therapy. Radiology, (1972) . 102: (3): 685–690. |


