
Analysis of behavioral disability and construction of a disability scale for the elderly in Shanghai
Abstract
BACKGROUND:
With the gradual aging of China’s population development, the number of disabled elderly has increased significantly.
OBJECTIVE:
In order to better solve the problem of life care for these elderly people, it is necessary to conduct in-depth and detailed research on the specific conditions of disabled elderly people, in order to differentiate different conditions for care and set appropriate insurance provisions.
METHODS:
Based on the detailed analysis of the basic behavioral ability of the elderly, and referring to the International Disability standards, this paper refines the three basic living ability indicators of physiological behavior, cognitive behavior and interpersonal behavior, and integrates the cultural elements of assimilation, continuity, fusion and cohesion with Chinese characteristics. A more systematic and perfect five-level disability scale which conforms to the national conditions of China is designed.
RESULTS:
The disability of the elderly in Shanghai was investigated with the newly constructed scale, and a detailed analysis and five-level division were made.
CONCLUSION:
Experiments show that the results of this study can more effectively establish the disability level of the elderly in China.
1.Introduction
In 2001, the World Health Organization (WHO) defined disability in the International Classification of Functions (ICF) as “a general term for impairment, limitation of activity and limitation of social participation, which denotes the negative aspects of interaction between situational, environmental and personal factors under certain health conditions” [1]. According to statistics from the Ministry of Civil Affairs, China has the highest disabled elderly population in the world, and is currently the only country in the world with a population of more than 10 million disabled elderly [2]. At the end of 2007, the disabled elderly population in urban and rural areas was 13.5 million, almost equal to the total population of three times Norway. If we add in the semi-self-care elderly, which are about 35 million people, almost equal to the total population of five times Switzerland, it becomes a serious social problem. In 2010, the disabled elderly, the most difficult group among the elderly, accounted for 16.5% of the total number of elderly people in China, accounting for about 33 million people. About 10.843 million of them were severely disabled and unable to take care of themselves. In 2015, China’s population reached a peak of 38.5 million, and the proportion of disabled elderly further increased. It is predicted that by 2020, the disabled elderly population in China will reach 21.85 million. Other professionals expect that China will enter a period of full-scale outbreak of various contradictions of population aging from 2030, and the rapid growth of disabled elderly is the most difficult problem to solve. At that time, the problem of the disabled in China will become an important challenge for the whole society [3].
The problems and difficulties caused by the disabled are serious, especially the heavy financial burden on the disabled families. Therefore, this issue needs attention from all sectors of society, and then a corresponding social security system must be established to solve this problem. Among the social security system, the most important one is the insurance system. With the support of the state, insurance companies have designed and developed various suitable insurance policies for the disabled, so as to provide timely compensation for the disabled and their families. In order to design and develop the insurance coverage for the disabled, the key is to determine the level and standard of the disabled reasonably and accurately so as to realize the best economic compensation.
At present, the study of disability level and disability standard in China has not yet formed a systematic and complete system [4], so it can only be carried out according to the internationally accepted standards. The ability of the elderly can be roughly divided into six aspects and three disability levels according to the number of disabilities. However, the situation in China is different from that of other countries, as the number of disabled elderly is very high. In order to provide effective care for the disabled and to facilitate the classification of insurance types, it is necessary to consider the detailed classification of disability ability and standard according to the actual situation, and to differentiate the disability levels at different levels.
Therefore, this study carried out the research on the level and standard of disability, and aimed to solve a key problem in the design and development of insurance categories related to the disabled. On the basis of the International Disability standards, this paper refines the basic living ability indicators: we selected 23 physiological and behavioral indicators, 6 cognitive and behavioral indicators, and 7 interpersonal behavioral indicators. At the same time, we integrated the cultural elements of Tonghua force, continuity, fusion and cohesion with Chinese characteristics, and then constructed a more systematic, perfect, five-level disability standard scale which conforms to the national conditions of China.
2.Methods
2.1Analysis of the constitution of the basic living behavior ability of the elderly
In general, disability means physical or mental impairment caused by accidental injury or illness, resulting in a partial or total lack of working ability, unable to complete the work equivalent to training, education and experience [5]. For the elderly, it mainly refers to the lack of basic living ability caused by disease and aging, unable to live independently and needing the care of others. We made a thorough and detailed analysis of the old people’s basic physiological and behavioral abilities, cognitive and behavioral abilities, and interpersonal behavioral abilities, which can be found in Fig. 1.
Figure 1.
Composition of basic living behavior ability of the elderly.
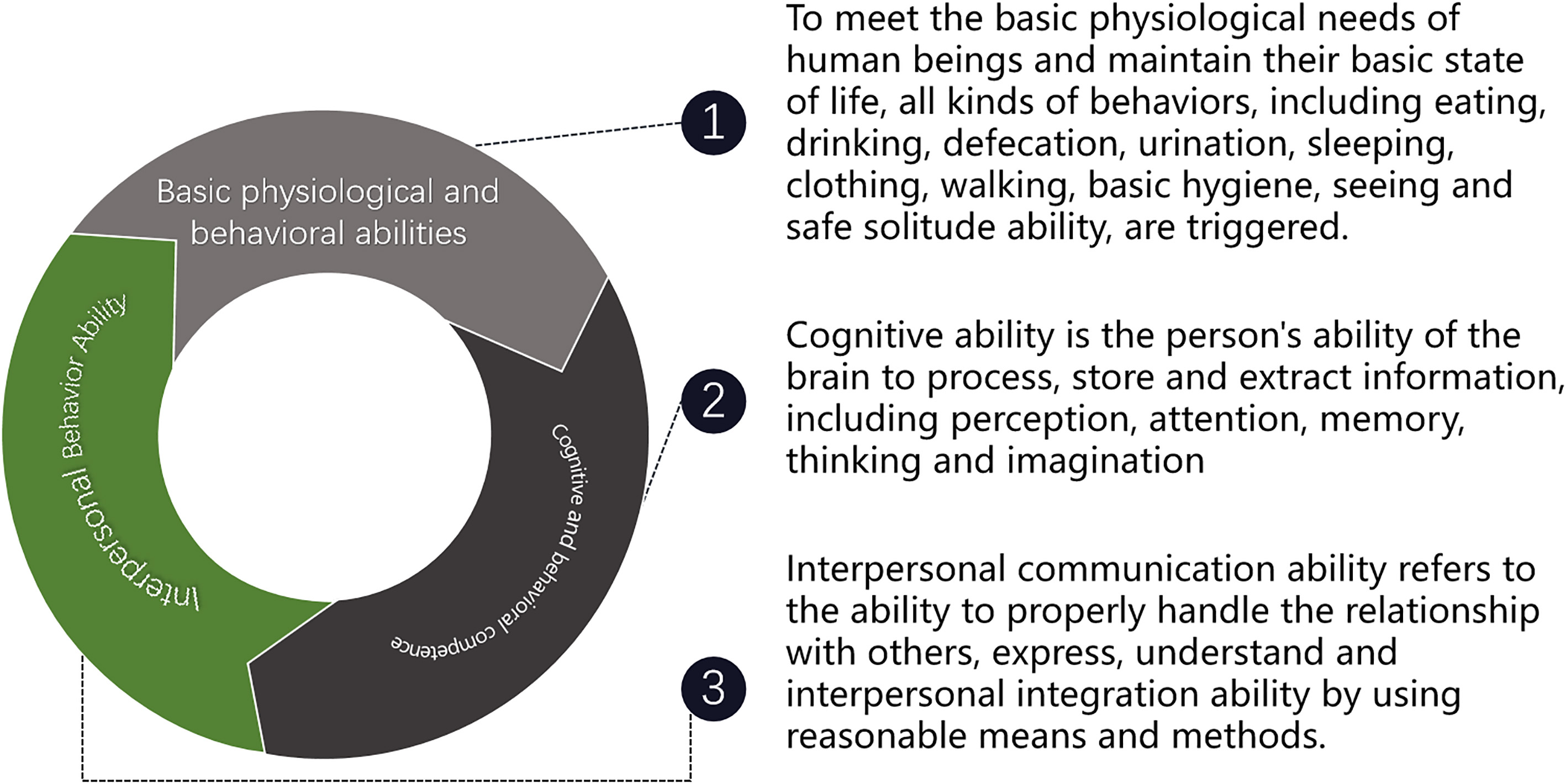
The three levels of basic physiological ability, cognitive ability and interpersonal ability, from low to high, form the basic living ability of the elderly. Only with these abilities the elderly can independently maintain a good state of life [6, 7].
2.2Construction of the disability rating scale
For the classification and confirmation of disability levels of the elderly, there are universal methods as well as different scales and determination methods used in specific countries. The universal scale for assessing the disability status of the elderly is the Activity of Daily Life Scale (ADLs) [8]. However, this scale is somewhat simplistic and contains only six basic physiological activities: bathing, going to the toilet, getting up from a chair, getting up, dressing and eating. Later, with the further understanding of disability, Lawton and Brody expanded the scale, and came up with the Barthel Index for Activities of Daily Living [9]. Specific indicators cover 14 items, in addition to the six items of ADLs, it also includes eight other activities necessary for an individual to live independently which are shopping, food preparation, laundry, housework, transportation, telephone, medication and financial management. Different countries have different understandings of international identification methods, and most countries have changed the scale by adding their own unique components, which reflects the humanistic characteristic of the country as well as its humanistic care. For example, the British think that making a cup of tea independently plays a greater role in their personal life, so they added this indicator to the calorimeter. Canada’s approach is more autonomous, allowing the subjects to determine the indicators they agree with, so their measurement is more personal, but the shortcomings are more obvious. It has been shown that this approach can ensure the relevance of indicators, but cannot ensure the effectiveness. Based on the above analysis, it is necessary to consider both the international standards as well as the special situation of China to determine the level of disability.
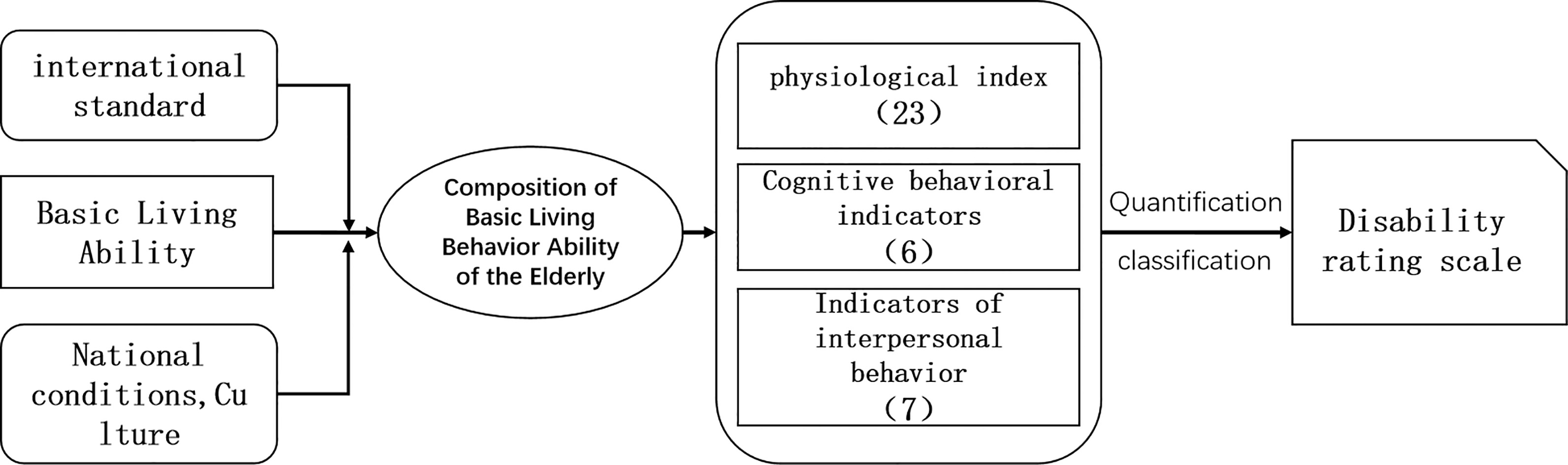
As shown in Fig. 2, we aimed to determine the indicators of the scale by taking the international standards, the basic living ability of the elderly and the special situation of China into account. Among these, the basic living ability of the elderly is the main line, and international standards are added. On the basis of in-depth and detailed analysis of the composition of the basic living ability of the elderly, from the perspective of the composition and subdivision of the basic living ability, the various indicators for determining the living ability of the elderly are gradually studied, thus forming a disability scale based on the basic living ability. In addition, the most important characteristics of Chinese culture should be taken into account when determining the indicators of the scale, which are mainly manifested in four aspects which are assimilation, continuity, fusion and cohesion. Therefore, China takes the family as the core and forms a ‘family doctrine’ culture. The elderly are the main force to cohere many members of the family. The care and care of family members play an important role in the life of Chinese people. Another Chinese characteristic derived from familialism is pragmatism. In order to realize the prosperity of the family, the Chinese should work diligently [10]. In order to better highlight the Chinese characteristics, i.e. ‘familialism’ and ‘pragmatism’, in determining the disability level of the elderly in China, this topic adds indicators reflecting the characteristics of these two aspects on the basis of international standards.
Table 1
Indicators and contents of basic physiological ability
| Index | Content |
|---|---|
| Eating, drinking | Do they need help to eat or drink? |
| Defecation, urination | Do they need help to use the toilet? |
| Do they have urinary incontinence? | |
| Do they have defecation incontinence? | |
| Sleeping | Do they need help to turn over in the recumbent position? |
| Do they need help from sitting up to standing up? | |
| Do they easily fall sleep and have a good rest at night? | |
| Dressing | Do they need help wearing or taking off their jacket? |
| Do they need help to wear or take off their pants? | |
| Acting | Do they need help to seat themselves in the chair? |
| Do they need help to walk 45 meters on flat ground? | |
| Do they need help to keep the body in balance? | |
| Do they have a reason to feel tired? | |
| Basic hygiene | Do they need help to brush their teeth or gargle? |
| Do they need help to wash their face and hands? | |
| Do they need help to comb their hair and put simple makeup on? | |
| Do they need help to take a bath (including a shower and body scrub)? | |
| Safety alone | Do they have an obsessive-compulsive disorder? |
| Do they have any destructive behavior? | |
| Do they have aggressive behavior? | |
| Are there are any private outings? | |
| Do they have suicidal tendencies? |
Figure 2.
Construction process of the disability rating scale for the elderly.
2.2.1Determination of the index system of basic physiological ability
The determination of basic physiological ability indicators should be based on the ability to eat, drink, pull, scatter, sleep, clothes, travel, basic hygiene, safety and solitude to meet people’s basic living needs (see Table 1).
Table 2
Cognitive ability indicators and contents
| Index | Content |
|---|---|
| Perception | Are they still interested in what they are usually interested in? |
| Memory | Can they remember and repeat three things? |
| Can they see clearly what time it is now? | |
| Do they know where they are? | |
| Attention and thinking | Cash and bank account management |
| Do they have a basic judgment ability of daily life? |
2.2.2Determination of the cognitive ability index system
The corresponding assessment indicators are determined from the perspective of the ability of perception, memory, attention, thinking and imagination necessary for the life of the elderly (see Table 2).
2.2.3Determination of the indicator system of interpersonal ability
Relevant assessment indicators were determined from the ability of expression, understanding, interpersonal integration and communication needed by the elderly to maintain their basic living conditions (see Table 3).
Table 3
Indicators and contents of interpersonal competence
| Index | Content |
|---|---|
| Communication (expression and understanding) | Ability to express one’s will |
| Ability to understand other people’s intentions | |
| Interpersonal fusion | Do they need help to go upstairs and downstairs? |
| Do they need help to buy bus tickets? | |
| Do they think they are useful persons? | |
| Do they more easily get angry or excited? | |
| How supportive are families and children? |
2.2.4Construction of the disability rating scale for the elderly in China
The basic physiological ability index, cognitive ability index and interpersonal ability index are combined to form the disability rating scale for the elderly in China. The scale is formed by the determination of three indicators, and classified according to the scale. The scale includes 23 basic physiological competence indicators, 6 cognitive competence indicators and 7 interpersonal competence indicators.
3.Results
3.1Classification of the disability level
The classification of the disability level is usually divided into the score method and ratio method. The score method needs to fully describe the different scoring basis of each index, which regards the workload and is subjective. The scoring method is based on a clear scoring range to determine the category of failure, which is easy to operate, and can clearly determine whether the respondents have the ability of a certain index. In this study, three groups of indicators (physiological, cognitive and interpersonal behavior) were examined. It was found that the quantitative indicators were more suitable for conversion into ratios, so the ratio analysis method was chosen for the classification of the disability levels. The results are shown in Table 4.
Table 4
Disability severity scale
| Level | Number of negative answers, ratio% |
|---|---|
| No disability | 0 |
| Mild disability | 5 |
| Moderate disability | 6 |
| Severe disability | 14 |
| Extremely severe disability | 24 |
Table 5
Statistical table of the elderly disability questionnaire data (partial data)
| Index | Rollover | Get up | Sit | Brush teeth, rinse mouth | Wash face/ hands | Comb/ makeup |
|---|---|---|---|---|---|---|
| Answered with ‘no’ | 125 | 120 | 125 | 126 | 128 | 126 |
| Can be accomplished under the guidance or care of | 22 | 19 | 15 | 6 | 7 | 5 |
| other people’s language | ||||||
| Need help from others, but mainly accomplish it by | 13 | 17 | 14 | 19 | 23 | 24 |
| oneself | ||||||
| The need to help, the elderly is only cooperate at most | 5 | 6 | 7 | 7 | 5 | 6 |
| Completely in need of help, or worse | 2 | 4 | 4 | 8 | 9 | 7 |
1. Disability rating: If the respondents’ answers to 36 questions in the disability rating scale for the elderly are all positive, it means that they have the ability, and then the respondents can be identified according to the disability rating.
2. Level of mild disability: According to medical experts, old people gradually lose some basic living ability. At first, the speed is relatively slow. According to the observations and analyses, the elderly in this group have less than five disabilities, which is between 0% and 14%.
3. Level of moderate disability: With the increase of age, the aging rate of the elderly accelerates in the later period, and the number of disabilities increases. In this stage, on the basis of the early disability, eight more disability indicators were added. Hence, up to 13 abilities is regarded as moderately disabled, which is between 15% and 36%.
4. Level of severe disability: After moderate disability, due to the distress of the disease and the aging of its organs, at this stage, 10 abilities will gradually be lost. Our team believes that 23 of the abilities are seriously impaired, which is between 37% and 64%.
5. Extremely severe disability level: At this stage, the ability will be lost. The team believes that 36 items of the ability deficiency are mild disability, which is between 65% and 100%.
Figure 3.
Six column analysis chart of indicators.
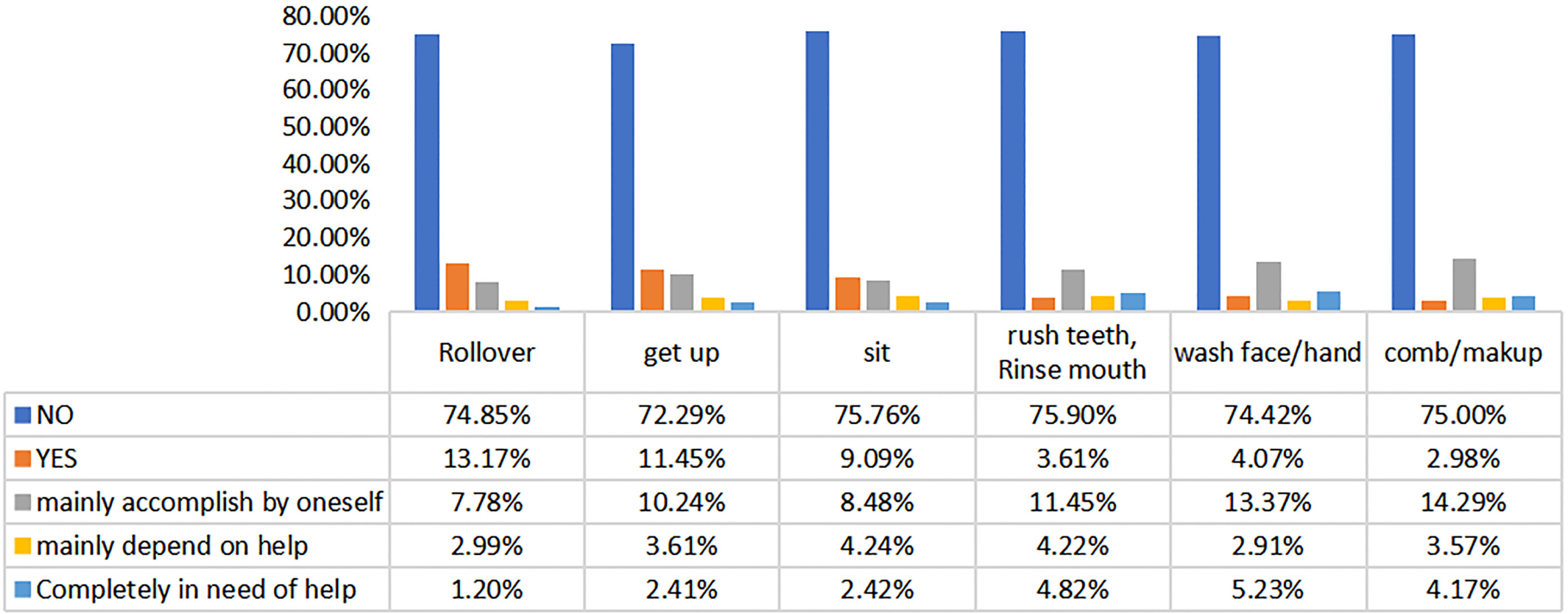
Figure 4.
Six radar analysis chart of indicators.
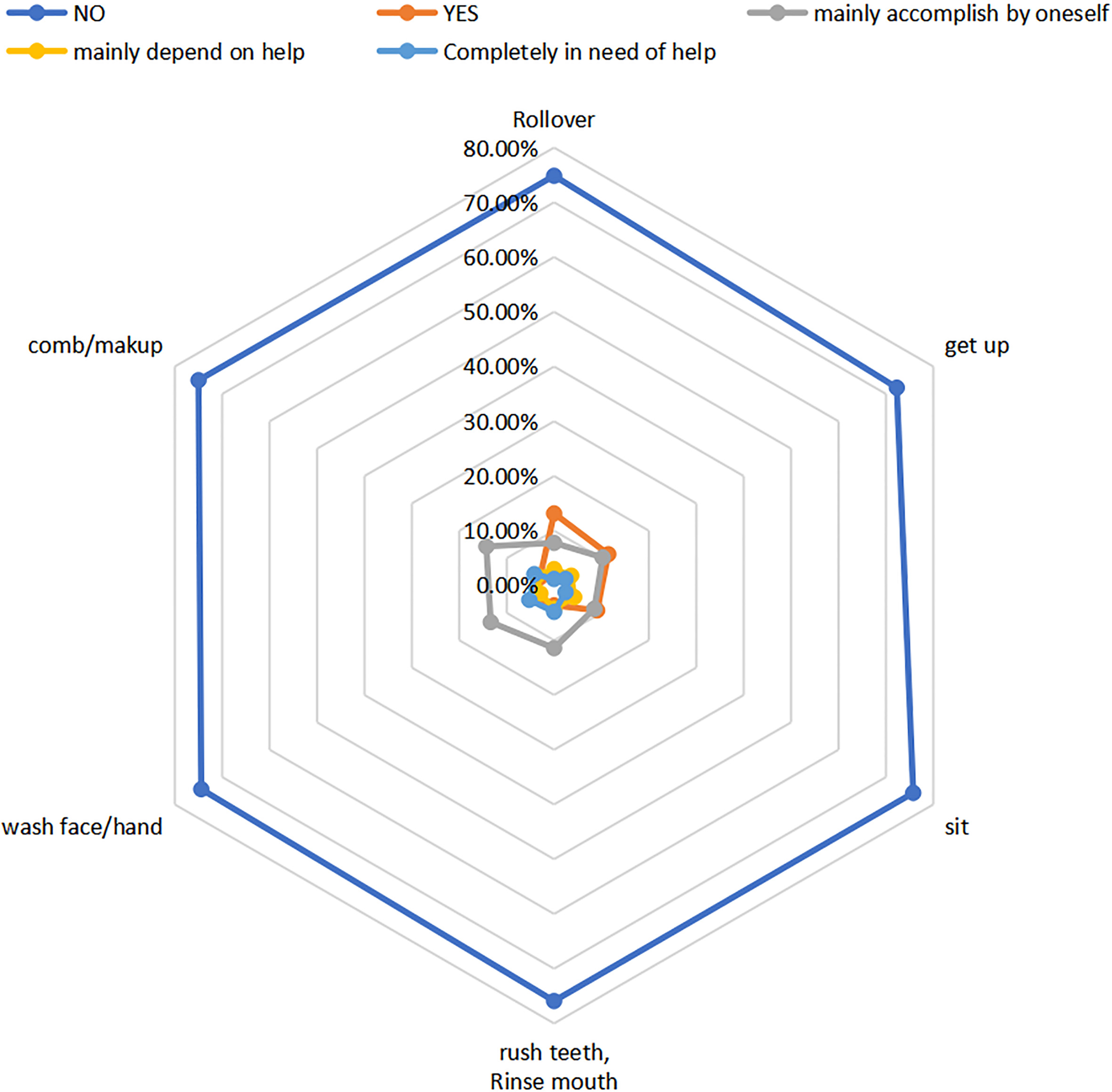
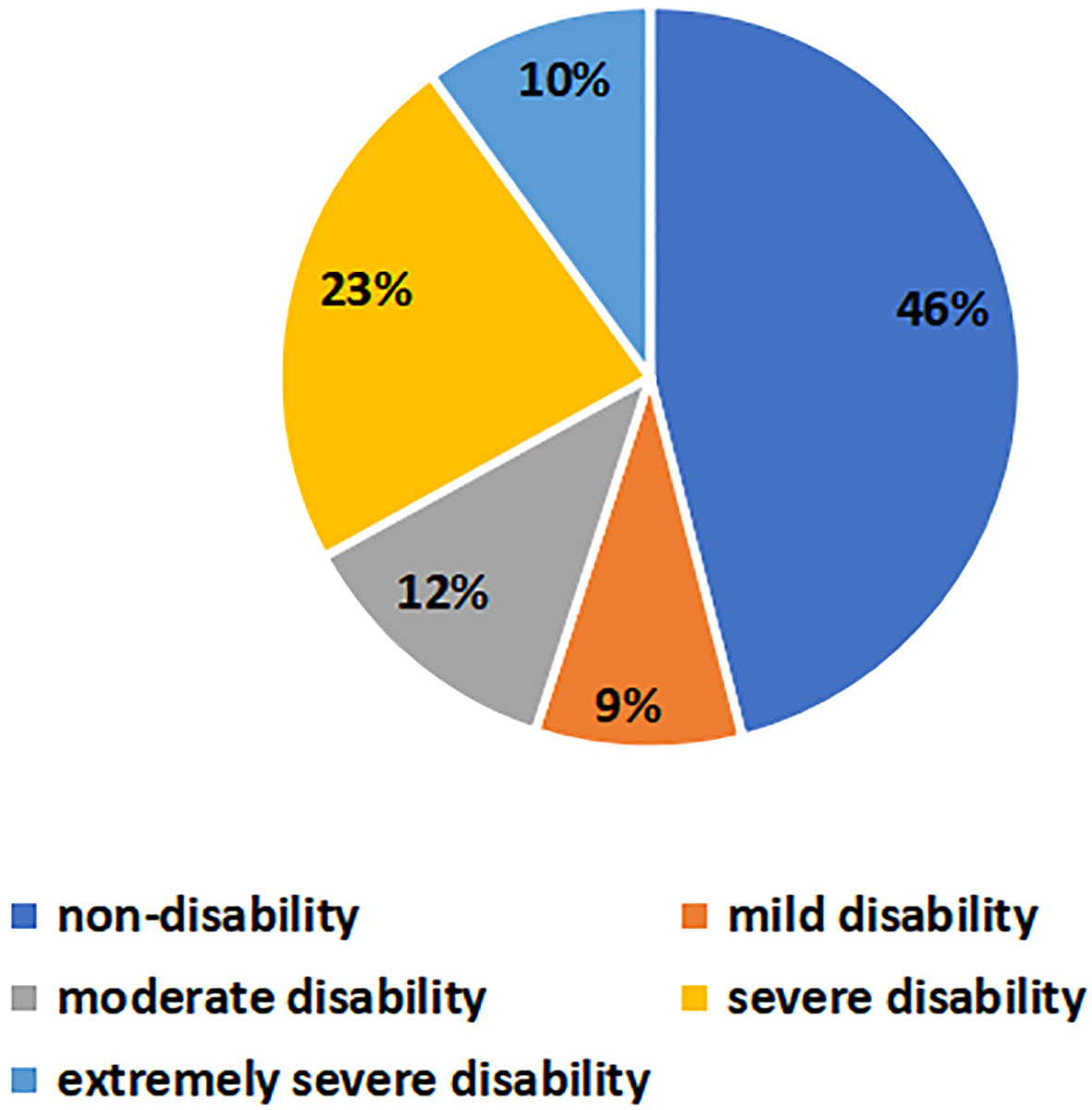
Figure 5.
Disability ratio of the elderly in Shanghai.
4.Discussion
The author chose eight representative districts in Shanghai: Yangpu District, Chongming District, Jiading District, Putuo District, Pudong District, Hongkou District, Zhabei District and Baoshan District, and conducted a questionnaire survey among the elderly in their homes, pension institutions and medical institutions. The questionnaire consisted of three parts of 66 questions. The first part was about the subjects and their family status, which is the foundation of the core part, and consisted of 26 questions. The second part was about the basic items of the ability of the elderly, and mainly included self-care ability, emotional status, spiritual feelings and so on. This part was the main part of the questionnaire, which consisted of 34 questions. The third part was about the general situation of the elderly, which included four problems. A total of 300 questionnaires were sent out and 272 valid questionnaires were collected. The statistical data obtained are shown in Table 5. The analysis based on the six indicators can be found in Figs 3 and 4.
From this analysis, the six indicators of the elderly in Shanghai showed that some of them had self-care ability, and the need for personal care was not very great. They could act on their own and did not need to be accompanied by a caregiver all the time. However, a small number of elderly people may be paralyzed and unable to control their own behavior and needed care all the time. Nurses are indispensable.
From Fig. 5, we can see that the behavioral indicators are directly related, so when disabled, the overall operational capacity decreases. In addition, the ratios of non-disability, mild disability, moderate disability, severe disability and extremely severe disability were 46%, 9%, 12%, 23% and 10%, respectively. This further illustrates that most of the elderly in Shanghai have strong self-care ability, better ability to live independently, better physical quality, and some of them needed the care of caregivers in order to live a normal life, but very few lost their mobility and needed constant company of caregivers.
5.Conclusion
Based on the basic living ability of the elderly, this paper classifies the disability levels, determines the disability rating scale and the disability severity rating scale, conducts a questionnaire survey, and summarizes and analyzes the current situation of the disabled elderly in Shanghai. According to the failure level and failure standard of the system studied, the design and development of insurance companies and the design of social security service system by relevant government agencies with the support of governments at all levels in China will be able to clearly define and classify the failure levels, facilitate the determination of the corresponding insurance types and service modes, and make the long-term care service system more human. Sexualization and design and provide different disability levels of life care, rehabilitation care, spiritual comfort, social interaction and hospice care services. Thus, it will effectively solve the difficulties of nursing for the disabled, and greatly promote the development of the cause of the disabled pursued by the Chinese government.
Acknowledgments
This research was supported by the National Key R&D Program of China (grant no. 2017YFE0112000), the Shanghai Municipal Science and Technology Major Project (grant no. 2017SHZDZX01), and the Major Project of Cooperative Innovation of Shanghai Medical College of Health.
Conflict of interest
The authors declare no conflict of interest.
References
[1] | Liu K, Manton KG, Aragon C. Changes in home care use by disabled elderly persons: 1982–1994. Journals of Gerontology, (2000) , 55: (4): S245. |
[2] | Baviera M, Roncaglioni MC, Tettamanti M, et al. Diabetes mellitus: A risk factor for seizures in the elderly – a population-based study. Acta Diabetologica, (2017) , 54: (2): 1–8. |
[3] | Liu X, Lu B, Feng Z. Intergenerational transfers and informal care for disabled elderly persons in China: Evidence from CHARLS. Health & Social Care in the Community, (2017) , 25: (4). |
[4] | Wei C, Fang Y, Mao F, et al. Assessment of disability among the elderly in xiamen of China: A representative sample survey of 14,292 older adults. Plos One, (2015) , 10: (6): e0131014. |
[5] | Riffin C, Van Ness PH, Wolff JL, et al. Family and other unpaid caregivers and older adults with and without dementia and disability. Journal of the American Geriatrics Society, (2017) , 65: (8). |
[6] | Lin XU. The Plight of the Home-based Care for the Disabled Elderly: Based on the Case Interview of the Disabled Elderly in Xi’an. Journal of Northwest University, (2014) . |
[7] | Zhao H, Luo D. Care feelings and influencing factors of family caregivers of disabled elderly. Chinese Journal of Gerontology, (2015) , (2): 449–451. |
[8] | Suryadevara NK, Mukhopadhyay SC. ADLs Recognition of an Elderly Person and Wellness Determination, (2015) . |
[9] | Fish J. Lawton-Brody Instrumental Activities of Daily Living Scale. Encyclopedia of Clinical Neuropsychology, (2011) . |
[10] | Pan J. Suggestions for solving the problem of care for disabled elderly in Jiangsu. Realism, (2015) (1). |


