
TLD environmental monitoring of new scanner facilities at the Nuclear Medicine Department of the Taiwan Medical University Hospital
Abstract
OBJECTIVE:
Single-photon emission computed tomography (SPECT) as well as dual energy X-ray absorptiometry (DXA) scanners were designed in July 2018 at the Nuclear Medicine Department (NM), of the Taiwan Medical University Hospital. These scanners emit substantial X-rays from the target, which are tungsten, iron. Therefore, patients undergoing SPECT and DXA diagnosis, in addition to medical personnel, are exposed to undesirable photon leakage.
METHODS:
Following administration of radiopharmaceuticals, patients become radioactive sources; thus, it is necessary to evaluate a possible increase in the environmental gamma exposure rates in the NM as a result of the operation of the new scanners. A three month evaluation of environmental radiation in the NM was performed using the accurate and sensitive TLD-100H approach, which gives an error rate less than 10%.
RESULTS:
Detected exposure radiation rates in the NM ranged from 0.12
CONCLUSION:
Recommendations were sent to the authorities of AEC-ROC to implement actions that could reduce doses at these high-dose locations to meet the ALARA principle.
1.Introduction
Nuclear medicine could be widely used in applications for a variety of diagnostic tests and disease treatments, and its use has increased dramatically over the past decade [1, 2, 3, 4, 5, 6, 7, 8, 9]. The Nuclear Medicine Department (NM) of Chung Shan Medical University Hospital (CSMUH) at Taichung designed two scanners: The new Single Photon Emission computed tomography, SPECT, 670 DR, Discovery, and the dual energy X-ray absorptiometry, DXA scanner, Hologic, Discovery, and were operated in July 2018. In addition, Positron Emission Tomography with Computed Tomography, PET/CT, Philips GEMINI GXL PET/CT, as well as Single Photon Emission computed tomography accompanied with computed tomography, SPECT/CT, Symbia T2, Siemens, Illinois, USA, were installed at NM in 2007 and 2011, respectively. A few studies evaluating extra environmental radiation dose rates for PET/CT technologists working at PET/CT have been reported in the literature. This study measured the environmental radiation in the NM of the Taiwan Medical University Hospital. The target made of tungsten, iron of these scanners emit substantial X-ray emissions, and the public and patient are therefore exposed to extra radiation within these facilities, although in a much lower dose than environmental background radiation. However, this exposure cannot be ignored for health reasons [1, 2, 3, 4, 5, 6, 7, 8, 9, 10]. Furthermore, following administration of radiopharmaceuticals, patients become radioactive sources. When radionuclides decay,
A few photons emitted from these radionuclides can penetrate the reinforced concrete (RC) and lead (Pb) shielding wall, further scattering into the vicinity outside the imaging room. This environmental radiation, however minor, causes health concerns for medical personnel. The controlled area includes four imaging and control rooms, exclusive toilets for patients, three activation boxes, an injection room, and a radioimmunoassay laboratory in the NM.
In addition, CSMUH is in the process of building a new Isotope Therapy Center (ITC), which commenced operation on 1 May 2019. The new ITC, SPECT, and DXA must meet with a limit of 100 mSv per 5 years and 50 mSv per year in the controlled area [1, 8, 10]. The lack of data about a possible increase in environmental radiation rates in the new scanners also motivated this study. Figure 1 shows a plane view of the basement 1 layout at the CSMUH (including the NM, Radiation Oncology Department, and cyclotron), with all dimensions quoted in centimeters. In addition, the areas are classified into free (uncontrolled) and controlled areas, and the dose restriction levels should be 1 mSv per year and 50 mSv per year, respectively [1, 10].
Figure 1.
A layout of basement 1 of at CSMUH, which was included the NM, RO and cyclotron. These locations were labeled with letters from A to T where TLDs were placed. Each point was selected based on its occupation by workers and general individuals. TLDs were suspended at SPECT, DXA, PET/CT and SPECT/CT control rooms (A, B, C, and D) on the walls at one meter height above the floor. In addition, TLDs were tapped at the ceiling directly “O” ring above the scanner in the imaging room (A1, B1, C1, and D1).
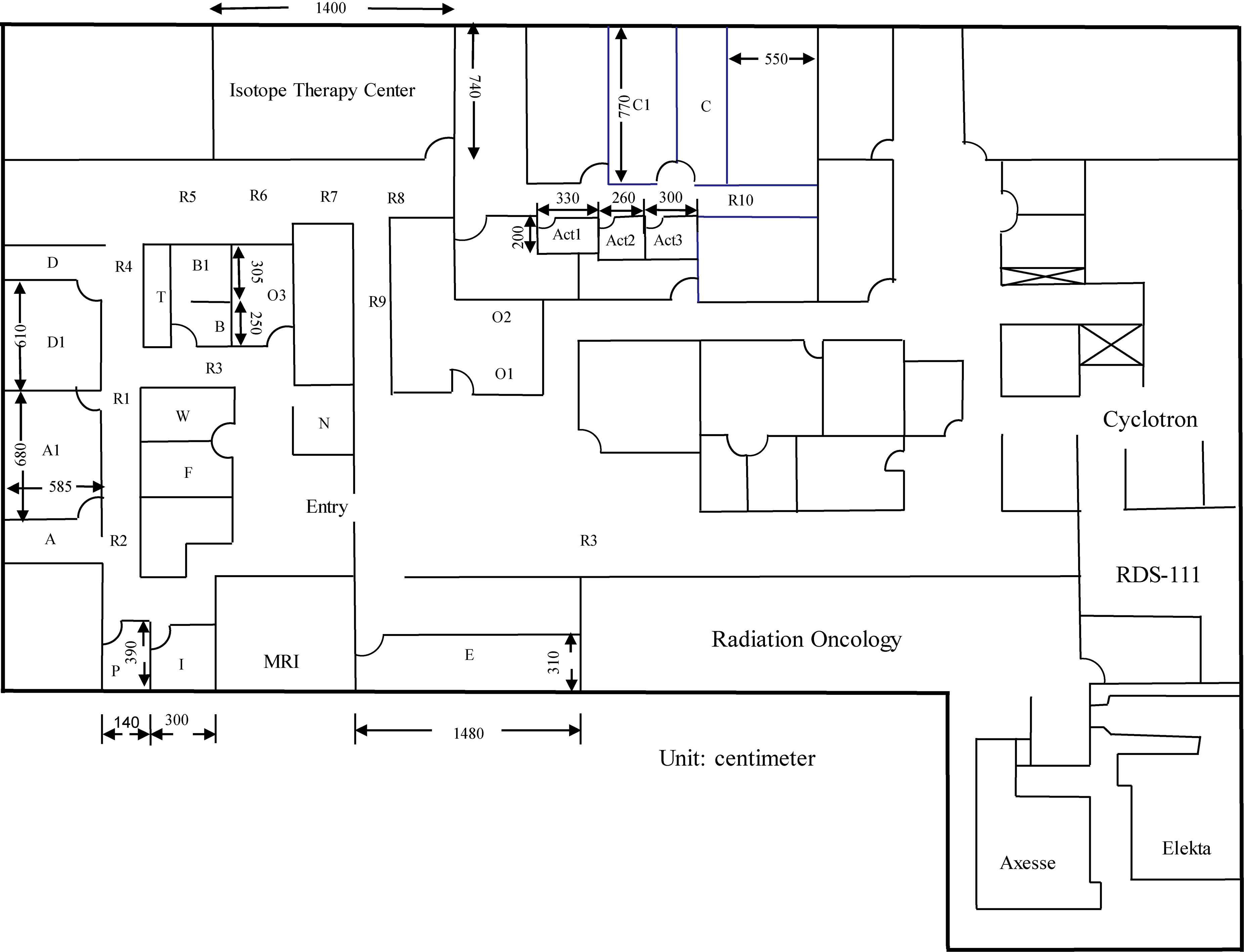
The PET/CT facility (C, C1, R10, and Act1-3) is surrounded by a shielding wall which consists of 30 cm thick RC and 3 mm thick Pb equivalent. RC, Pb are generally the most cost-effective shielding materials to protect against the leakage of
Table 1
| Radio- nuclide | Half life | Abundance (%) | Administered dose (mCi) | Patients per month | Waiting time | First scan time (min) | Waiting time (hr) | Second scan time (min) | |
|---|---|---|---|---|---|---|---|---|---|
| 110 min | 511 | 194 | 6–8 | 110 | 45–60 min | 20 | 3–4 | 20 | |
| 78.2 hr | 184 | 20 | 5 | 20 | 1 days | 30 (WB)15 (Organ) | – | – | |
| 6.0 hr | 140 | 90 | 20–25 | 150 | 20 min-4 hrs | 15 | – | – | |
| 8.0 day | 364 | 81 | 2 | 3 | 3–7 days | 30 (WB)15 (Organ) | – | – | |
| 8.0 day | 364 | 81 | 29.5 | 3 | 7 days | 30 (WB)15 (Thy) | – | – | |
| 73 hr | 167 | 9.4 | 2 | 4 | 5–10 mins | 15 | 3–6 hrs | 15 |
Fourteen staff members of NM, including radiologists, nurses, and medical doctors, contacted the relatives, patients and the public. Table 1 lists the properties of the commonly used radionuclides [6, 8]. An average of 300 patients per month were diagnosed in the NM. In addition, 150 patients received 20 mCi (74 MBq)
The evaluation of extra environmental radiation dose rates for PET/CT technologists working at PET/CT facilities has been reported in the literature. The present study measured the environmental radiation within the NM of the Taiwan Medical University Hospital.
1.1PET/CT facility
2-deoxy-2-[
Prior to diagnosis using
The patient was positioned on the PET/CT camera bed of the facility (C1) for the transmission scan. The PET/CT scans took 20 minutes and were performed twice in each patient. The second scan was performed almost 3–4 hour after the first, and the patient was asked to wait in the activation box during the interval. PET/CT scans took 20 minutes in the PET/CT imaging room (C1), and the patient spent more time inside the PET/CT facility. Finally, the patient could leave the NM of CSMUH.
1.2SPECT/CT facility
Consequently, new occupational radiation safety problems had to be resolved. The most widely used radionuclide in the NM is
The thyroid uptake and whole-body retention of
Additionally, prior to SPECT/CT scans using
In this study, thermoluminescence dosimetry (TLD) was used to measure environmental radiation among the NM areas. This high energy radiation poses different radiation hazard problems. Therefore, it became necessary to evaluate a possible increase in environmental radiation rates due to the operation of the new ITC, SPECT, and DXA. Special attention is necessary to optimize radiation safety among these facilities of NM to minimize environmental radiation for the safety of personnel and the public.
2.Materials and methods
2.1TLD-100 system
TLD-100H has been widely used to detect environmental radiation, since it indicates long-term accumulation during the last 30 years [7]. The TLD-100H was composed of LiF: Mg, Cu, P, 3.2
The TLDs were calibrated using known activities, 10 mCi (37 MBq)
2.2Statistical analysis and weighting factor
In order to compare the fluctuations of the TLDs, three TLDs were put in one bag, so that 120 TLDs could be represent 40 measured locations. To ensure batch homogeneity, the sensitivity of each TLD (
(1)
where
These radiation rates can be evaluated from various measured locations under the same conditions. The weighted mean (
(2)
Standard error (
(3)
The weighting factor (
(4)
The weighted standard error of each bag
(5)
2.3Surveying environmental radiation at the NM center
To evaluate environmental radiation, TLD was randomly suspended at one meter above the floor to represent exposure doses for a person standing among the NM [10]. The measurements were taken for a one month survey and were repeated three times from 1 October to 31 December 2018. Two bags (six TLDs) were used to monitor the environmental radiation rates in Taichung, 750 meters and 3000 meters away from NM, respectively, which were labeled TC1 and TC2. Four bags (12 TLDs) were used to monitor background radiation in the low background lab of CSMU [3, 7]. The results for each bag were averaged. The fluctuations, calibration, and counting statistics of the Harshaw 3500 reader for the calibrated TLD-100H were within 10% [7, 12].
3.Results and discussion
3.1TLD-100H calibration
The irradiated TLD chips were read by Harshaw 3500 reader automatically on the following reading cycle. First, TLD is pre-heating temperature 135
3.2Environmental radiation
The TLDs measurements among the SPECT, DXA, PET/CT, and SPECT/CT facilities show a huge gradient that environmental radiation rates varied from 0.15
From the SPECT imaging room (A1), an explicit photon dose rate of 0.90
Following the three month survey, the average environmental radiation in the vicinity of the ceiling “O” ring of the SPECT ranged from 0.28
The highest environmental radiation rates came from patient
Table 2
Environmental radiation (mSvper month) measured at the NM from Oct. 1
| Locations | Area classification* | Environmental radiation |
|---|---|---|
| SPECT facility | A | |
| SPECT control room (A) | A | 0.12 |
| SPECT imaging room (A1) | A | 0.28 |
| Corridor (R1) | A | 0.15 |
| Corridor (R2) | A | 0.15 |
| DXA facility | A | |
| Control area (B) | A | 0.12 |
| Treatment area (B1) | A | 0.16 |
| Corridor (R3) | A | 0.16 |
| PET/CT facility | A | |
| PET/CT control room (C) | A | 0.15 |
| PET/CT imaging room (C1) | A | 0.32 |
| Corridor (R10) | A | 0.16 |
| SPECT/CT facility | A | |
| SPECT/CT control room (D) | A | 0.13 |
| SPECT/CT imaging room (D1) | A | 0.76 |
| Corridor (R4) | A | 0.16 |
| Activation box (Act 1) | A | 0.14 |
| Activation box (Act 2) | A | 0.15 |
| Activation box (Act 3) | A | 0.16 |
| Radioimmunoassay laboratory (E) | A | 0.13 |
| Consultation room (F) | B | 0.15 |
| Injection room (I) | A | 0.18 |
| Nursing station (N) | B | 0.16 |
| Medical office (O1) | B | 0.14 |
| Medical office (O2) | B | 0.15 |
| Medical office (O3) | B | 0.14 |
| Waiting room (W) | B | 0.16 |
| Toilet (T) | A | 0.16 |
| Taichung (TC1) | B | 0.17 |
| Taichung (TC2) | B | 0.13 |
*A: Controlled, B: Free.
Table 2 lists the environmental radiation in the NM at the 40 measured points. The highest radiation was obtained in the imaging room of the SPECT/CT facility (D1). The individual environmental radiation at points in D1 ranged from 0.76
Shielding ranged from 0.13
3.3Minimum detectable dose (MDD) of TLD method
The values of radiation rates have a confidence level of 95% and were evaluated by the minimum detectable dose (MDD). When the environmental radiation rates were measured at several points at the same distance, the average environmental radiation rate at these points was used. All measurements were performed three times. These TLDs were subsequently counted and analyzed to evaluate the distribution of environmental radiation within the NM. Many of the detected points of environmental radiation rates were uncertain because the corresponding photon doses were under the MDD [12, 14]. The net counts (
(6)
(7)
Figure 2.
Both peak A or B corresponded to nearly the same gross count. The gross count is equal to background count (B) adds net count (
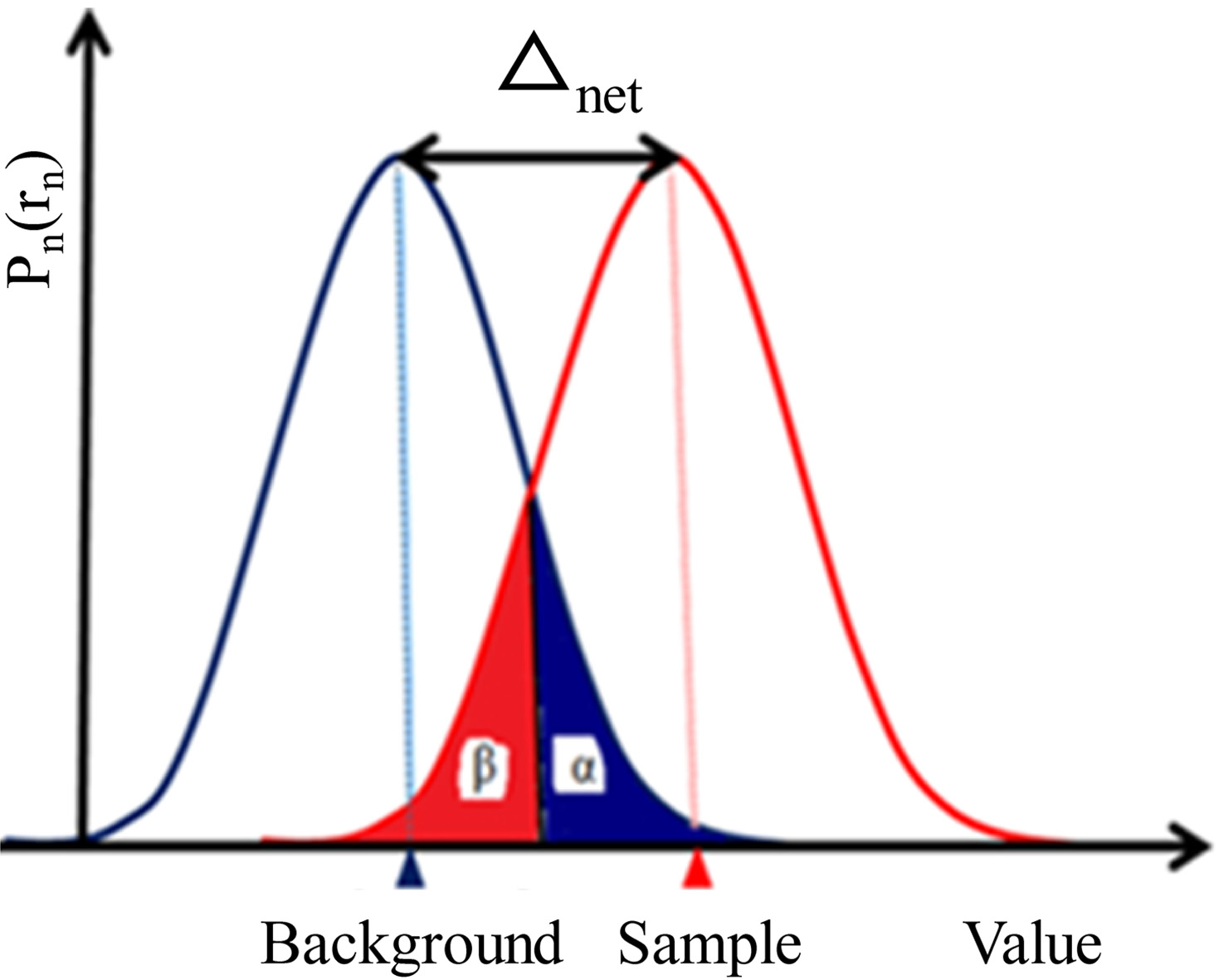
Accordingly, the
The derived measurements could be re-evaluated to obtain these MDD. A total of 82 of 120 analyzed results to identify radiation from the TLDs failed, due to the 95% confidence level. The unqualified glow curves from the TLDs were mostly around the free and controlled areas within the NM, indicating that only a negligible amount of
3.4Environmental radiation for personnel
The “hot” points in the radiology personnel control rooms were near the PET/CT control room (A). The extra environmental radiation rates a year for a radiologist who was stationed in the control room (B) of the PET/CT facility was:
(8)
This extra radiation dose rate is far lower than that of the annual limit of 50 mSv per year recommended by the ICRP 60 [10]. The results show that the RC/Pb shielding can adequately protect hospital personnel. Hence, the penetrating photons cause no health concerns for medical personnel in the CSMUH during the operation of these scanners. However, due to the ALARA principle, the actual extra radiation in the vicinity outside the NM is worth measuring in future work.
4.Conclusion
In July 2018, the CSMUH built new SPECT and DXA facilities, and the new ITC began operation in May 2019. Therefore, it was necessary to calculate the extra radiation. Evaluation of exposure rates indicates that the environmental radiation rates among the NM range from 0.12
Acknowledgments
The authors thank the NM staff of CSMUH for their efficient support and co-operation of this academic research without any reservation. Financial support was given in part by the Ministry of Science and Technology of ROC (grant no. MOST 105-2314-B-040-010).
Conflict of interest
None to report.
References
[1] | Chung Shan Medical University, ((2019) ). Available from: http://english.csmu.edu.tw/bin/home.php. |
[2] | Tseng HC, Liu WS, Huang HS, et al., Spatial distributions of environmenral radiations at medical linac undergoing treatment of vmat using taguchi method. Journal of Radioanalytical and Nuclear Chemistry. (2016) ; 307: : 1635-1639. |
[3] | Tseng HC, Liu WS, Tsai HH, et al., Radiation dose for normal organs by helical tomotherapy for lung cancer. Applied Radiation and Isotopes. (2015) ; 102: : 35-41. |
[4] | Changlai SP, Tsai HH, Tsai SC, et al., Environmental radiation detected at lin shin hospital in taichung during the fukushima nuclear power plant accident. Journal of Radioanalytical and Nuclear Chemistry. (2015) ; 291: (3): 859-863. |
[5] | Avila O, Torres-Ulloa CL, Medina LA, et al., TL measurement of ambient dose at a Nuclear Medicine. Radiation Measurements. (2011) ; 46: (12): 1843-1846. |
[6] | Saha GB. et al., Fundamentals of nuclear pharmacy. 6 |
[7] | Changlai SP, Chang PJ, Chen CY. Biodistribution and dosimetry of 131I in thyroidectomy patients using semi-quantitative γ-camera imaging. Cancer Biotherapy & Radiopharmaceuticals. (2008) ; 23: (6): 759-766. |
[8] | Madsen MT, Anderson JA, Halama JA, et al., AAPM Task Group 108: PET and PET/CT Shielding Requirements. Medical Physics. (2006) ; 33: : 4-15. |
[9] | Chen CY, Chang PJ, Changlai SP, et al., Effective half life of iodine for five thyroidectomy patients using an in-vivo gamma camera approach. Journal of Radiation Research. (2007) ; 48: : 485-493. |
[10] | International Commission on Radiological Protection. ((1991) )Recommendation of the ICRP, ICRP Publication 60, Annals of the ICRP, No. 1-3; Pergamon Press, Oxford, UK |
[11] | Chen CY, Pan LK. Trace elements of taiwanese dioscorea spp. Using neutron activation analysis. Food Chemistry. (2001) ; 72: : 255-260. |
[12] | Chen LF, Tseng HC, Pan LK, et al., Evaluating environment radiations at Axesse linac undergoing NPC treatment of VMAT. Computer Aided Surgery. (2016) ; 21: (S1): 79-83. |
[13] | Chung C, Chen CY, Wei YY, et al., Monitoring of environmental radiation on the spratly island in the south china sea. Journal of Radioanalytical and Nuclear Chemistry Articles. (1995) ; 194: (2): 291-296. |
[14] | Turner JE. Atoms, Radiation, and Radiation Protection, 3rd Edn, New York USA, John Wiley & Sons, Inc. ISBN 978-3-527-40606-7; (2007) . |


