
Effects of an 8-week basketball-specific proprioceptive training with a single-plane instability balance platform
Abstract
BACKGROUND:
To avoid injuries in basketball players, they are recommended to pay more attention to improve their body balance. Therefore new training methods and equipment need to be devised. This study examined the effects of an 8-week basketball-specific proprioception training program while using a new developed one plane instability balance board during warm-up for improving balance ability in basketball players. Players who obtained basketball-specific balance training were compared to a control group.
METHODS:
Thirty-one male university basketball players (age: 21.35, SD
RESULTS:
The results indicate significant improvements in the overall YBT for both legs in BTG, but not in CG. However, no group differences were found for dynamic balance performance, but static balance (i.e., postural stability) differed between groups after 8 weeks. A statistically significant moderate inverse correlation was computed between the total score of YBT and the total score of the overall stability index (
CONCLUSIONS:
An 8-week basketball-specific proprioception training program with a single-plane instability balance platform improved balance ability (Y balance test and postural stability test) of basketball players.
1.Introduction
The International Basketball Federation (FIBA) estimates that about 11% of the general population plays basketball as amateurs or professionals [1]. Lithuanians are avid basketball players across all ages and genders [2]. Basketball is a high contact sport that challenges balance and stability (e.g., during accelerations and decelerations, changes in direction, penetrating the defensive perimeter, boxing out, dribbling and defense position recovery) [3]. Basketball players often experience imbalances due to the lack of neuromuscular control, compromised strength, and flexibility which may lead to injuries [4, 5, 6, 7]. Within the motor domain, balance is seen as the ability to maintain the body’s center of gravity over the base of support. Balance results from neuromuscular actions in response to continuous visual, vestibular and somatosensory feedback [8, 9]. Neuromuscular control is the ability of the central nervous system (CNS) to regulate the muscles in the execution of multi-limb functional movements. Related to this proprioception is a complex neuromuscular process pertaining to the internal kinesthetic awareness of body position and movement. Proprioception facilitates joint stability and prevents injury and thus has a significant role on the structural integrity of the body [10]. This is important because sport injuries typically result from the loss of body function or structural integrity that occurs throughout the activities [11].
Consequently, it is plausible that optimizing dynamic balance in players can help improve injury rates [6]. Currently, there are a number of multi-factorial neuromuscular training strategies targeting injury prevention in a variety of sports and across athletic levels [12]. Nevertheless, given the specific challenges of basketball, coaches and physical therapists could benefit from more individualized and supervised training approaches [13]. To that end, training approaches that target injury prevention by optimizing proprioception and dynamic stability can prove particularly beneficial.
Prevention in sport injuries is important to the extent that sport injuries are often misunderstood as an isolated, single body parts’ ‘problem’ [6] and a special emphasis is placed on the moment when the injury occurred (i.e., 42.7% during contact and 23.1%. in non-contact situations) [14]. Consequently, the notion of multiple constraints acting at multiple levels and timescales in repeated micro injuries is often overlooked. This is concerning because micro injuries can result in a macroscopic non-linear effect which can in turn lead to severe or terminal injuries [15].
A recent report has suggested reduced injury rates based on data drawn from the FIFA 11+ program in elite-level European basketball players [16]. In general however, the effectiveness of injury prevention programs for sports and basketball in particular are limited [17]. Of relevance to this study, some have argued that in addition to internal (i.e., age, sex and body composition) or external (i.e., rules, equipment and environment) factors for injury prevention [15], there is a need to maintain proprioception at optimal levels in order to improve static and dynamic balance and reduce injury rate.
The purpose of this study was to investigate the effects of an 8-week basketball-specific proprioception training program using a new developed one plane balance board during warm-up for improving balance ability in basketball players. We hypothesized that the warm-up training program using a one plane balance board would improve proprioception and enhance dynamic and static balance in basketball players. On a practical level, results from this study could help further shape proprioception trainings (while using one plane balance board) for preventing injuries in basketball players as well as other similar sports with high contact and high balance requirements.
2.Materials and methods
2.1Participants and experimental design
Thirty-one male university basketball players (age: 21.35, SD
A two-group, experimental design was used in this study. One team (17 participants) served as the balance training group (BTG) and practiced their balance on a new developed unstable platform entitled Abili Balance Trainer (Abili, Kaunas, Lithuania). The other team (14 participants) kept their routine team practice and served as the control group (CG). At pre- and post-training levels, players’ balance was tested by means of the Y balance test (YBT; Functional Movement, Danville, VA, USA) and postural stability test (PST) with the Biodex Balance System (BBS; Shirley, NY, USA).
All the procedures were carried out in accordance with ethical standards and were approved by the local research ethics committee (BEC-KN(B)-57). The Helsinki Declaration (1964) and its later amendments were also followed. All participants were informed about the procedures of the study and signed a written informed consent form prior to participation.
2.2Apparatus
The newly developed Abili Balance Trainer is a one plane instability platform used for training and rehabilitation (see Fig. 1). The platform comes with a balance analyzer app that determines individuals’ balance ability and helps guide the training. The platform moves in one plane with regards to task difficulty. The platform incorporates a range of levels (i.e., basic level, medium level, advanced level). For the purpose of this study, when a participant completed a balance task accurately on a given level, they were moved to the next level.
Figure 1.
One plane instability platform entitled Abili Balance Trainer.

2.3Procedure
The study was conducted during in-season with three team training sessions a week and lasted for a total of 8 weeks for both BTG and CG. Training sessions lasted 2 hours for CG and 2 hours and 20 min in total for BTG. In the initial warm-up phase, prior to training, each player from BTG performed 20 min additional BT on the Abili Balance Trainer. Besides the team training sessions, the players also completed 2 games a week. One physical therapist trained and observed all participants and mediated the move between the balance difficulty levels.
The program consisted of a basketball-specific BT program with a balance platform. It was supervised by a physical therapist that specialized in basketball. The program included three series of exercises. The initial series involved 5 exercises without any special gears. During the second series participants performed 3 exercises using an elastic band. Finally, during the last series of 5 exercises, participants used a basketball (see Fig. 2).
Figure 2.
A, First training series that was repeated 8 times for each leg separately. B, Second training series that was repeated 8 times for each leg separately. C, Third training series that was repeated 8 times for each leg separately.
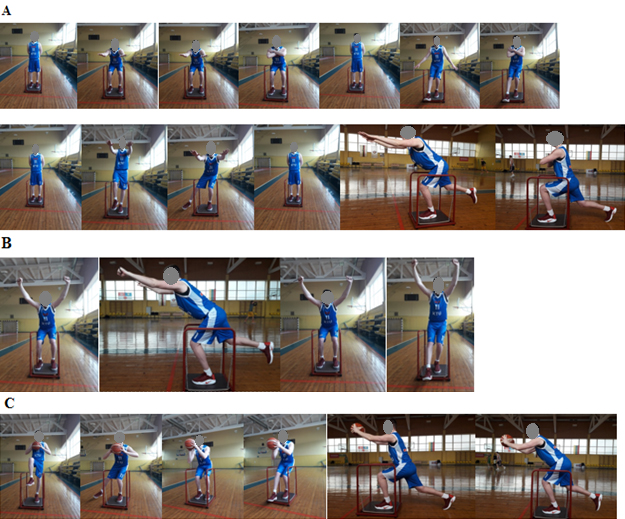
During the BT, all three series of exercises were performed, and each exercise was repeated 8 times for each leg separately. Initially, participants completed all exercises on the balance trainer at the basic difficulty level. The difficulty level for each participant was determined individually, i.e., based on participants’ capacity to maintain balance.
All participants were tested in the same week prior to the training and within 7 days following the completion of the last training session. For pre- and post-testing, all participants were tested at the same time during the day to ensure the control of circadian fluctuations in performance. Once the participants were familiar with the procedure, the tests were recorded. YBT was used for assessing dynamic balance, and the Biodex Balance System helped to evaluate the features of the static balance. Each test was carried out three times and the highest of the three scores was included in the analysis of YBT, while the obtained values from Biodex Balance System were averaged.
2.3.1Y balance test
Participants performed the dynamic balance test using a commercially available device. The YBT is a screen of dynamic balance requiring stance leg balance while the contralateral leg reaches in anterior (ANT), posteromedial (PM), and posterolateral (PL) directions. The rater for the YBT had 5 years of experience in performing and evaluating the test.
Initial instructions for administering the YBT were provided to the evaluators. These verbal instructions included information regarding the number of repetitions and moves that participants were instructed to perform, along with directions and prohibitions for administering the assessment. The test began once all the instructions were provided [4, 18]. These instructions to the participants prior to testing were:
“Remove your shoes and socks and place the most distal end of the longest toe of the left stance leg at the red line on the platform on the test kit. The attempts will not be counted if you commit the following infractions: loss of balance on the stance leg that would result in movement off the platform or if the contralateral leg has a touchdown as well as if you lose contact with the reach indicator during a reach attempt. Also, if you fail to return to the starting position without loss of balance, kicking or pushing the indicator to increase distance. You will perform four to six trials as part of your training process in order to become familiar with the procedure and to reach the learning plateau. Initially, you will perform the test in the ANT direction. Then, you will switch to the right foot on the platform. Once again performing four to six trials. You will repeat the same procedure again for PM, alternating left and right, followed by PL.”
All participants underwent the training and received identical instructions. At the completion of the trial practices, right leg length was measured in centimeters from the inferior aspect of the anterior superior iliac spine to the distal medial malleolus. The weight had to be equally distributed between the right and left legs. Finally, all participants performed three attempts, following the same protocol from the practice trials. The maximal reach distance of these three trials was recorded for analysis. Reaches during the final three attempts were discarded and repeated if any of the aforementioned infractions were committed.
2.3.2Postural stability test
Each participant took PST by means of the Biodex Balance System. PST were measured in 20 sec trials with 1 min intervals in between and simulated particular movement patterns by the fixed platform. The platform stability was set to a moderately stable level and in each session participants’ sway was used to assess the postural stability. The platform provided an objective assessment of balance using three indices: the overall stability index (OSI), the anteroposterior stability index (APSI), and the mediolateral stability index (MLSI). These indices were calculated according to the degree of platform oscillation. Smaller values indicated higher stability rates for the individual [19]. Prior to testing, participants received the following instructions:
“Remove your shoes and socks and remain on one foot. Your hands should be parallel to the body and eyes should be open and fixed on the horizon.”
The protocol was performed with participants in an unipodal stance. A training test was given to minimize the effects of learning, followed by three consecutive tests with 10 sec intervals. The average of the three tests was considered the participants’ OSI.
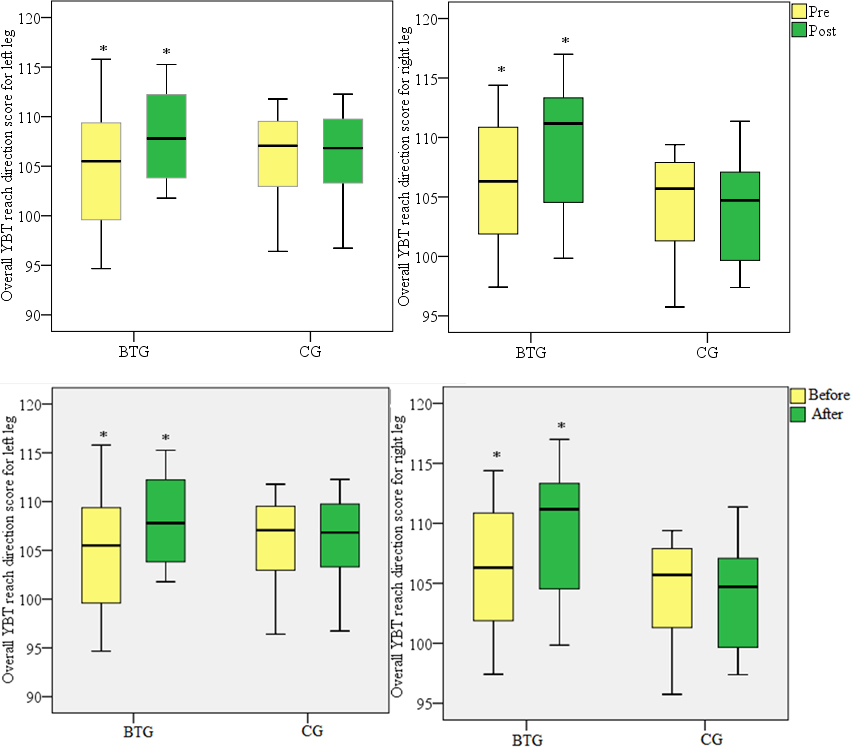
Figure 3.
Overall YBT reach direction score for left and right legs in BTG and CG pre- and post- 8-week training (
2.4Data analyses
Statistical results are shown as median Xme (minimum value (Xmin) – maximum value (Xmax)) unless otherwise noted. Significance of pre- and post-values between the groups was assessed by means of non-parametric Mann-Whitney U matched pairs test. Pairwise comparisons were performed with a non-parametric Wilcoxon test. In terms of the relationship between quantitative variables, Spearman’s correlation coefficient (r) was computed. A correlation coefficient of
3.Results
3.1Y balance test
The overall YBT reach direction score was obtained by averaging the three normalized maximal YBT scores for each direction. Prior to the 8-week training session for left and right legs, in BTG these values were 105.5 (94.67–115.79; 104.84) and 106.31 (97.42–114.39; 106.17), respectively (see Fig. 3). In CG, the overall YBT scores were 105.89 (96.41–111.78; 105.17) for the left and 104.28 (95.75–109.4; 104.28) for the right leg. At the completion of the 8-week training, BTG groups’ overall YBT score was 107.79 (101.78–115.56; 108.09) and 111.17 (99.84–117; 109.08) for the left and right legs, respectively. In CG, the scores were 106.82 (96.73–112.27; 106.15) for the left and 104.71 (97.39–111.36; 104.37) for the right leg. In BTG, significant changes were observed in both the left (
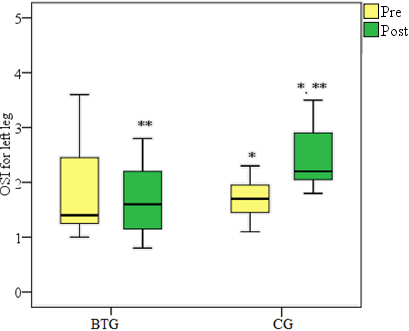
3.2Postural stability test
At the pre-training levels, in BTG the OSI for the left leg was 1.4 (1–3.6; 1.85). At the post-training levels, OSI became 1.6 (0.8–2.8; 1.69), but the changes were not significant (
Figure 4.
Overall stability index (OSI) results presented for the left leg in both BTG and CG pre- and post- 8-week training (*
3.3Correlations between YBT and PST
In Tables 1 and 2 correlations between the overall YBT score and OSI from PST prior to training are depicted for the left and right legs respectively. A statistically significant moderate inverse correlation was computed between the total scores of YBT and OSI (
Table 1
Correlations of YBT and PST test results prior to balance training for the left leg
| YBT | PST | ||||||
|---|---|---|---|---|---|---|---|
| PM | PL | Overall | OSI | APSI | MLSI | ||
| YBT | ANT | ||||||
| PM | |||||||
| PL | |||||||
| Overall | |||||||
| PST | OSI | ||||||
| APSI | |||||||
| * | |||||||
Table 2
Correlations of YBT and PST test results prior to balance training for the right leg
| YBT | PST | ||||||
|---|---|---|---|---|---|---|---|
| PM | PL | Overall | OSI | APSI | MLSI | ||
| YBT | ANT | ||||||
| PM | |||||||
| PL | |||||||
| Overall | |||||||
| PST | OSI | ||||||
| APSI | |||||||
| * | |||||||
4.Discussion
The purpose of this study was to determine whether an 8-week balance training could improve proprioception and consequently dynamic balance in basketball players. The main findings from this study suggested that at the completion of the 8-week balance training of 20 min, 3 times a week, dynamic balance improved. These findings are consistent with previous research that focused on training for the improvement of balance in basketball players. Boccolini et al. have shown that an equilibrium training for 30 min, 2 times a week for 12 weeks on unstable planes is effective for improving balance. [3]. Additionally, it has been shown that supervised programs (either by athletic trainers or coaches) are likely to allow higher adherence rates than unsupervised programs [13]. Our study used a brief but more ecologically sound approach, as in this players were trained on game-related exercises which in turn seemed to facilitate their balance.
In particular, drawing on the present findings, the BT on unstable planes did not reduce the dynamic balance asymmetry between the left and right leg in different directions in YBT. One potential explanation for the remaining asymmetry may be due to the fact that the experimental tasks were identical (e.g., same number of reps) for both legs. In other words, any existing original asymmetries were not considered when designing the experimental tasks for the legs. The difference between the left and right legs has been evaluated because this might be a potential determinant for lower limb injury [4]. Pliusy et al. for instance have shown that the difference in the forward direction (4 cm or more) between the left and right legs is associated with an increased risk of lower limb trauma [18]. In light of this information, the initial differences between the legs could help determine more accurately how many repetitions would be needed for each leg. This is particularly important in the present study, as administering the same amount of repetitions for both legs could have potentially inflated the differences between the legs.
The present findings associated with YBT and PST values showed moderate correlations in basketball players. In contrast to our findings, others have shown that YBT is not correlated with PST as an assessment of postural stability. Thus, these findings have implications for researchers and clinicians using YBT results as the only measure of postural stability [19]. Research has shown that YBT is a reliable measure of dynamic balance performance as 26/36 (anterior), 31/36 (posteromedial) and 33/36 (posterolateral) quantified variables demonstrated good-excellent intra-session test-retest reliability [20]. Additionally, others have indicated ANT as the main predictor of future injury from the YBT in student populations [21], while others have concluded that male collegiate athletes with greater BMI and lesser YBT anterior reach were at a greater risk of sustaining an ankle sprain injury [22].
To reiterate our initial hypothesis, in this study we expected that the 8-week training program would improve proprioception and consequently dynamic and static balance in basketball players. Our results indicated that BTG significantly improved dynamic balance in both legs. Static balance was evaluated through PST. OSI scores for the left and right legs were not significant. Nevertheless, in the post-test, BTG and CG showed differences between the groups suggesting better results for the BGT group that received additional training.
A number of limitations should be noted. First, CG did not perform a standardized warm-up routine. Each team performed its usual warm-up routine in a non-standardized fashion and this may have affected their response to the training. This said, individual athletes performing their own pre-game warm-up routine is a common practice in teams [23]. Nevertheless, the use of a vigorous and standardized warm-up protocol for CG could have enhanced the validity of our results. Second, the teams were not blinded to the training program. The use of random selection and random assignment as well as the implementation of a single or double-blind setting could have further boosted our internal validity.
Further research is needed to explore the potential link between improved proprioception and reduced injury rate via enhanced structural integrity of the body. Besides, there is a need to investigate the effectiveness of these approaches in not only basketball but also in other high contact and dynamic sports (e.g., hockey, soccer, football, lacrosse, handball). Furthermore, conceptualizing structural integrity of the body could refer to more individualized practices that account for individual capabilities, limitations, and structural asymmetries. For instance, males were shown to sense and perceive movement, position and force differently. Thus, researchers have argued that proprioception assessed by these conscious sensations is substantially genetically dependent, with heritability indexes ranging from 0.60 to 0.77, contingent on the specific task requirements [24]. These individual multifactorial factors should be taken into account by practitioners before designing training sessions.
From a practical standpoint, it appears that based on the evidence presented in this study, proprioceptive training on the Abili Balance Trainer, could be used in isolation as a safe tool to train dynamic and static balance in basketball players. This is important because there is an empirical basis for the role of proprioception for neuromuscular control and human performance but also for the improvement of balance, and injury prevention in basketball[7, 25]. Practitioners should therefore be aware of these approaches to further develop neuromuscular motor control and structural integrity in players to ultimately make the game safer and help prevent injuries.
5.Conclusions
An 8-week basketball-specific proprioception training program during warm-up with a single-plane instability balance platform improved the balance ability (Y balance test and postural stability test) of basketball players. In order to develop balance, it is sufficient to perform exercises on an unstable platform during warm-up when the level of instability is selected appropriately.
Acknowledgments
The authors would like to thank to Abili (Kaunas, Lithuania) for the technical support. This research did not receive any specific grant from funding agencies in the public, commercial, or non-for-profit sector.
Conflict of interest
None of the authors declare competing financial interests.
References
[1] | Zedde P, Mela F, Del Prete F, Masia F, Manunta AF. Meniscal injuries in basketball players. Joints. (2014) ; 2: : 192-6. doi: 10.11138/jts/2014.2.4.192. |
[2] | Cingiene V, Laskiene S. A Revitalized Dream: Basketball and National Identity in Lithuania. Int J Hist Sport. (2004) ; 21: : 762-79. doi: 10.1080/0952336042000262042. |
[3] | Boccolini G, Brazzit A, Bonfanti L, Alberti G. Using balance training to improve the performance of youth basketball players. Sport Sci Health. (2013) ; 9: : 37-42. doi: 10.1007/s11332-013-0143-z. |
[4] | Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a Predictor of Lower Extremity Injury in High School Basketball Players. J Orthop Sport Phys Ther. (2006) ; 36: : 911-9. doi: 10.2519/jospt.2006.2244. |
[5] | Foss KDB, Thomas S, Khoury JC, Myer GD, Hewett TE. A school-based neuromuscular training program and sport-related injury incidence: a prospective randomized controlled clinical trial. J Athl Train. (2018) ; 53: : 20-8. |
[6] | Barber Foss KD, Myer GD, Hewett TE. Epidemiology of basketball, soccer, and volleyball injuries in middle-school female athletes. Phys Sportsmed. (2014) ; 42: : 146-53. doi: 10.3810/psm.2014.05.2066. |
[7] | Zech A, Hübscher M, Vogt L, Banzer W, Hänsel F, Pfeifer K. Balance training for neuromuscular control and performance enhancement: A systematic review. J Athl Train. (2010) ; 45: : 392-403. doi: 10.4085/1062-6050-45.4.392. |
[8] | Raymond J, Nicholson LL, Hiller CE, Refshauge KM. The effect of ankle taping or bracing on proprioception in functional ankle instability: A systematic review and meta-analysis. J Sci Med Sport. (2012) ; 15: : 386-92. doi: 10.1016/j.jsams.2012.03.008. |
[9] | Bonato M, Benis R, La Torre A. Neuromuscular training reduces lower limb injuries in elite female basketball players. A cluster randomized controlled trial. Scand J Med Sci Sports. (2018) ; 28: : 1451-60. |
[10] | Riva D, Bianchi R, Rocca F, Mamo C. Proprioceptive Training and Injury Prevention in a Professional Men’s Basketball Team: A Six-Year Prospective Study. J Strength Cond Res. (2016) ; 30: : 461-75. doi: 10.1519/JSC.0000000000001097. |
[11] | Timpka T, Jacobsson J, Bickenbach J, Finch CF, Ekberg J, Nordenfelt L. What is a sports injury? Sports Med. (2014) ; 44: : 423-8. doi: 10.1007/s40279-014-0143-4. |
[12] | Malliaras P, Morrissey D, Herman K, Barton C, Malliaras P, Morrissey D, Herman K, Barton C, Malliaras P, et al., The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during spor. The effectiveness of neuromuscular warm-up strategies, that req. (2012) ; 1: -12. doi: 10.1186/1741-7015-10-75. |
[13] | van Reijen M, Vriend I, van Mechelen W, Finch CF, Verhagen EA. Compliance with Sport Injury Prevention Interventions in Randomised Controlled Trials: A Systematic Review. Sport Med. (2016) ; 46: : 1125-39. doi: 10.1007/s40279-016-0470-8. |
[14] | Kay MC, Register-Mihalik JK, Gray AD, Djoko A, Dompier TP, Kerr ZY. The Epidemiology of Severe Injuries Sustained by National Collegiate Athletic Association Student-Athletes, 2009–2010 Through 2014–2015. J Athl Train. (2017) ; 52: : 117-28. doi: 10.4085/1062-6050-52.1.01. |
[15] | Pol R, Hristovski R, Medina D, Balague N. From microscopic to macroscopic sports injuries. Applying the complex dynamic systems approach to sports medicine: a narrative review. Br J Sport Med. 2018bjsports-2016. |
[16] | Longo UG, Loppini M, Berton A, Marinozzi A, Maffulli N, Denaro V. The FIFA 11+ program is effective in preventing injuries in elite male basketball players: A cluster randomized controlled trial. Am J Sports Med. (2012) ; 40: : 996-1005. doi: 10.1177/0363546512438761. |
[17] | DiFiori JP, Güllich A, Brenner JS, Côté J, Hainline B, Ryan E, et al. The NBA and Youth Basketball: Recommendations for Promoting a Healthy and Positive Experience. Sport Med. (2018) ; 48: : 2053-65. doi: 10.1007/s40279-018-0950-0. |
[18] | Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, Elkins B. The reliability of an instrumented device for measuring components of the star excursion balance test. North Am J Sport Phys Ther NAJSPT. (2009) ; 4: : 92. |
[19] | Almeida GPL, Monteiro IO, Marizeiro DF, Maia LB, de Paula Lima PO. Y balance test has no correlation with the Stability Index of the Biodex Balance System. Musculoskelet Sci Pract. (2017) ; 27: : 1-6. doi: 10.1016/j.msksp.2016.11.008. |
[20] | Johnston W, Reilly MO, Coughlan GF, Caulfield B. Inter-session test-retest reliability of the quantified Y balance test Inter-session test-retest reliability of the quantified Y balance test, (2018) . |
[21] | Luan Y, Wu F, Wang WTJ. Functional Movement Screen and Y-Balance Test as Injury Predictors in UTF8min大å¸ç”ŸåŠŸèƒ½æ€§å‹•ä½œæª¢æ¸¬èˆ‡ Y å—平衡測試å°å—傷之é 測. (2018) ; 20: . doi: 10.5297/ser.201806. |
[22] | Hartley EM, Hoch MC, Boling MC. Y-balance test performance and BMI are associated with ankle sprain injury in collegiate male athletes. J Sci Med Sport. (2018) ; 21: : 676-80. doi: 10.1016/j.jsams.2017.10.014. |
[23] | Bloom GA, Durand-Bush N, Salmela JH. Pre-and postcompetition routines of expert coaches of team sports. Sport Psychol. (1997) ; 11: : 127-41. |
[24] | Missitzi J, Geladas N, Misitzi A, Misitzis L, Classen J, Klissouras V. Heritability of proprioceptive senses. J Appl Physiol. (2018) . |
[25] | Proske U, Gandevia SC. The proprioceptive senses: their roles in signaling body shape, body position and movement, and muscle force. Physiol Rev. (2012) ; 92: : 1651-97. |


