
Research and development of 3D printing orthotic insoles and preliminary treatment of leg length discrepancy patients
Abstract
BACKGROUND:
Leg length discrepancy (LLD) can cause abnormal posture, muscle and/or joint pains, which leads to walking difficulties. The common treatment is to use a shoe lift on the shorter leg side, but this has unsatisfying results.
OBJECTIVE:
Through research and development, we created 3D printing orthotic insoles for LLD patients and aimed to improve their symptoms.
METHODS:
1. Research and development of 3D printing orthotic insole: (1) foot scan and data acquisition; (2) insole software modeling; (3) 3D printing insole using TPU materials, and (4) post-processing. 2. Clinical observation: we customized insoles for LLD patients and required them to wear them while walking. We conducted general inquiries and a functional evaluation before and after 12 weeks of wearing insoles.
RESULTS:
There are seven complete cases. The joint and lower back pains were alleviated. The stride frequency, stride and pace were improved in all seven cases. Patients’ overall health condition improved significantly.
CONCLUSIONS:
The 3D printing orthotic insoles are made with clear procedures and practical operability. By wearing insoles, patients’ muscle and/or joint pains were relieved and their gaits were improved.
1.Introduction
Leg length discrepancy (LLD) is defined as the unequal length of bilateral lower legs [1]. There are two common types of LLD, namely structural and functional LLD. LLD can cause abnormal postures, muscle joint pain and difficulty in walking. The treatment of LLD depends on the degree of LLD difference. Often a shoe lift is used on the side of the shorter lower limb, but most scholars have found that although the use of the above insole has some effects, it is still unsatisfactory in the clinical application [2].
The 3D printing orthotic insole fits patients’ foot type and are comfortable because they are customized [3]. They are processed by computer software to change the height of the arch and the thickness of the heel according to the treatment needs. In theory, it can more accurately set the right abnormal body strength line when the patient is standing and walking, and correct abnormal postures and reduce pain. This paper introduces in detail the production process of 3D printing orthotic insoles and preliminary application to seven LLD patients. The innovation lies in the application of 3D printing technology to produce orthotic insoles for LLD treatment. To our knowledge, no relevant reference report has been published.
2.Materials and methods
2.1Participants
The patients visited the Shanghai No. 4 Rehabilitation Hospital between January and June 2018.
2.1.1Selection criteria
1) Age 10–60 years old, can communicate normally. 2) LLD difference is bigger than 5 mm (direct measurement method: the distance from anterior superior spine to malleolus medialis). 3) With lower back pain or hip, knee or ankle pain when standing or walking, the duration lasts longer than 3 months. 4) Can walk more than 30 meters in the community without a walking stick. 5) Willing to sign an informed consent form.
2.1.2Exclusion criteria
1) Used a shoe lift or other foot orthopedic device within the last three months. 2) Have ischialgia, lumbar disc herniation, vertebra slip or severe osteoarthritis of the spine. 3) Have acute lower back pain, injury on the back, surgery, compression fracture or ankle ligament tear. 4) Have systemic diseases (e.g. gout, rheumatoid arthritis).
2.2Production of the 3D printing orthotic insole
2.2.1Data collection
We used a 3D foot scanner (LSR 3D Laser Foot Scanner, Shanghai Zuyue Foot Supplies Co., Ltd., China) to collect the data. The procedure is outlined below.
Foot scan of neutral calcaneal sitting position. (1) Mark 3 middle points in the 1/3 posterior side of the patient’s lower leg, the Achilles tendon and the heel, and draw a line. (2) The patient is seated, put a foot into the scanning area, keep the second phalanx aligned with the black mark line in front, two feet should be separated and keep the same width with the shoulder, naturally place hands on thighs, and look ahead. (3) When placing the calcaneus in a neutral position, the patient is required to adjust the position of the ankle joint so that it is vertically aligned with the knee; the patient adjusts the posterior line position of the calcaneus and the tibia through the entropion or ectropion of the ankle, and observe whether the back line of the calf coincides with the red line of the scanner laser. If it is coincident, it should be judged as the calcaneus neutral position, and the patient should maintain this posture and start scanning. (4) Save the scanned file (A.obj), as shown in Fig. 1.
Figure 1.
Foot scan of the neutral calcaneal sitting position.

Insole scanning. (1) Take out the equipped insole in the patient’s shoe and place it in the scanning area for scanning. (2) Save the scanned file (B.obj).
2.2.2Software modeling
We used 3D MAX software as the modeling software of the 3D orthotic insole. The procedure is outlined below.
Import file. Import the foot model file (A.obj) and insole model file (B.obj) into the 3D MAX software, adjust the model view and save it as A.max and B.max file respectively (see Figs 2 and 3).
Figure 2.
Foot model file (A.max). Points A and B are markers with a vertical distance of 2 cm from the first and fifth metatarsophalangeal joints. Point C is the midpoint of the line that connects the first metatarsophalangeal joint to the center of the heel, which is the marker of the arch height.
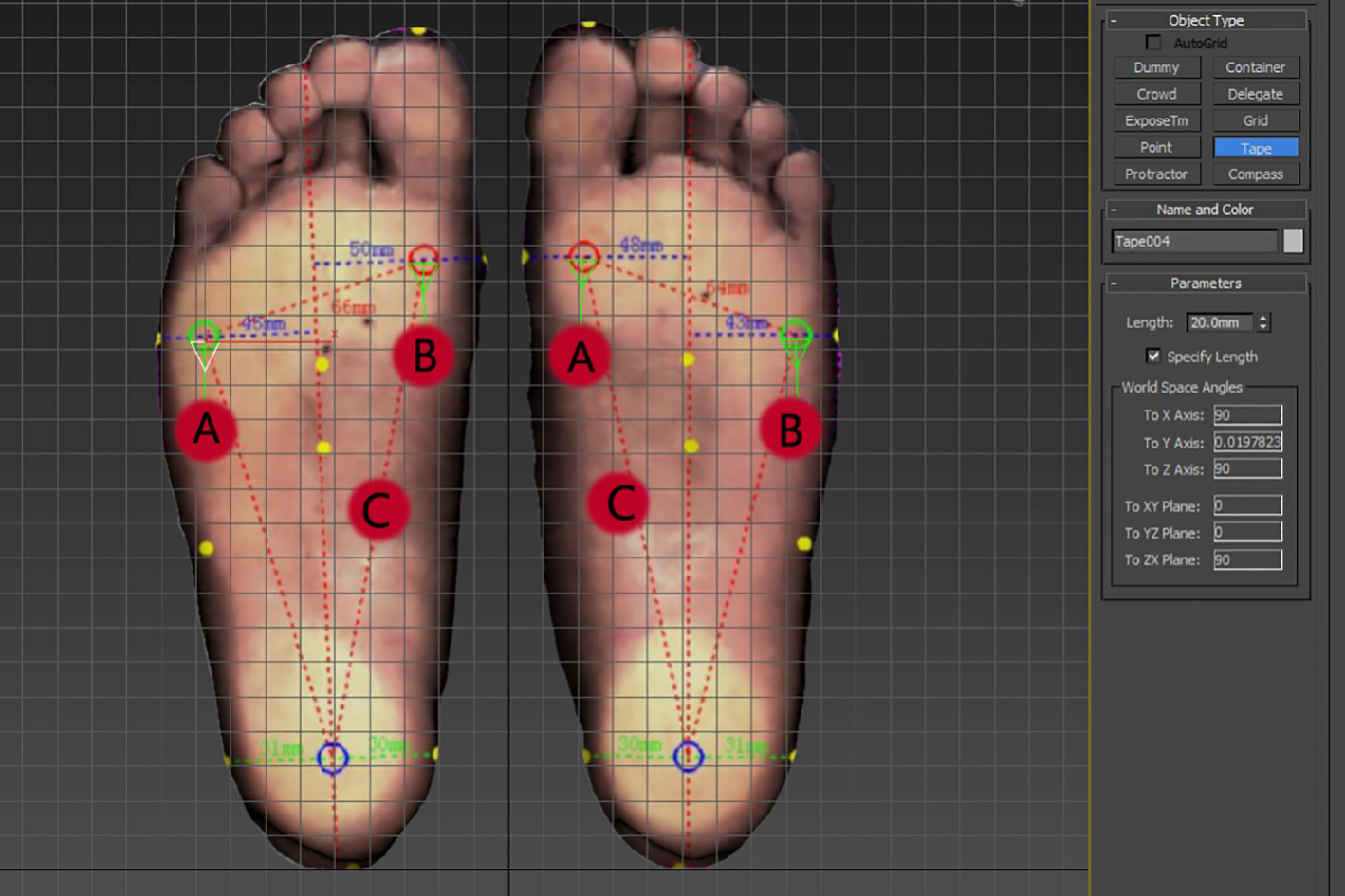
Figure 3.
Patient’s insole model file (B.max).
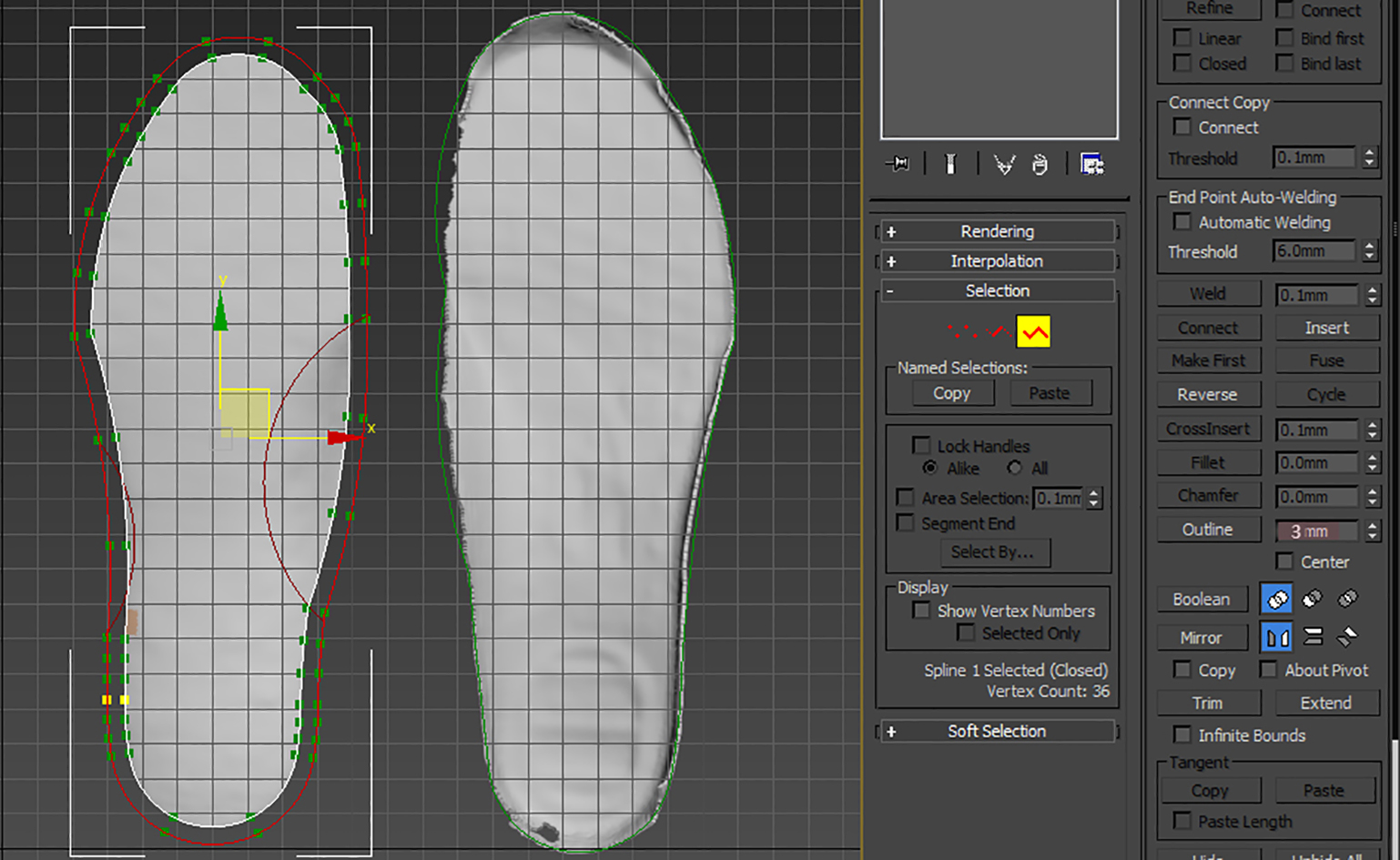
Figure 4.
The green area is a 2/3 long foot model area file (D.max).

Figure 5.
The insole file (E.max) after the adjustment of the arch height. Point C is the ‘point height value’ based on the scan result, which decides the arch height.
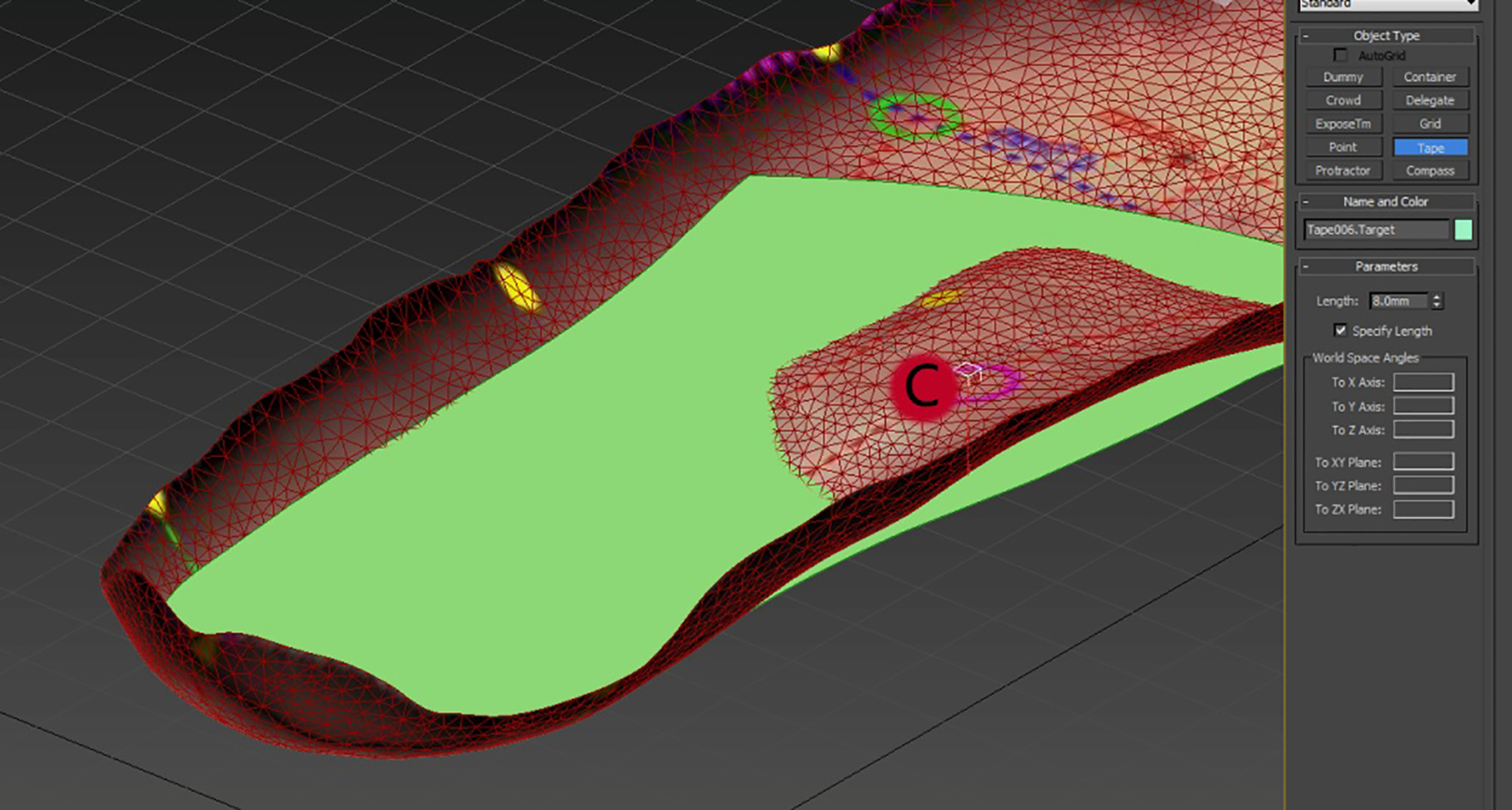
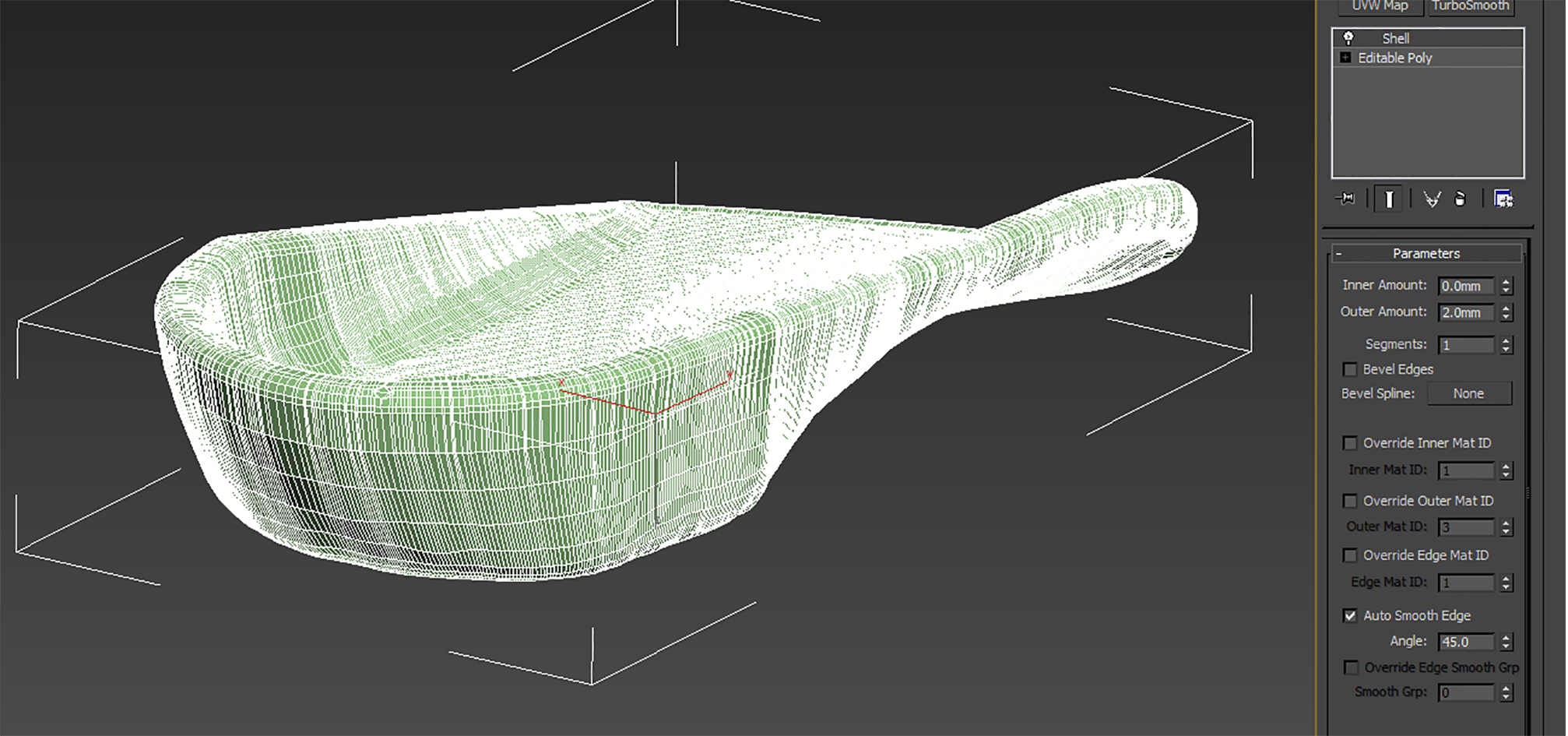
Edit file. (1) Determine the foot model area: select the insole model file (B.max) to outline, draw the outline of the insole with the spline, and the outline is inwardly retracted by 3 mm. Then map it onto the foot model file (A.max) to obtain the foot model area file (C.max). (2) Adjust the insole length: The insole is 2/3 length type, use the two points A and B of the foot model file (A.max) to make the arc and cut off the foot model area file (C.max), get a 2/3 length foot model area file (D.max), see Fig. 4. (3) Adjust the height of the insole arch (D.max): refer to point C of the foot model file (A.max), use the foot scan results “point height value” to decide the height of the arch and generate an insole file (E.max), see Fig. 5. (4) Adjust the thickness of the insole (E.max): select an insole file (E.max), according to the treatment needs, select the thickness command, and input the outer amount values of the subcommand, generate an insole file (F.max), see Fig. 6. Then conduct smooth processing to insole file (F.max) to avoid burrs.
Figure 6.
The insole file (F.max) after adjusting the thickness of the insole.
2.2.33D printing
We used the following procedure:
1. Convert the insole file (F.max) into a printable file format (F.stl);
2. Open the slicing software Cura and import file (F.stl);
3. Set parameters: filling density 30%, print speed 30 mm/s, print temperature 226
4. The printing method adopts Fused Deposition Modeling (FDM), and the printer adopts R1000 type, FDM, produced by China Dongguan Bairen Hardware Electronic Technology Co. Ltd and the print material adopts thermoplastic urethanes (TPU) wire (specification: 1.75 mm);
5. Printing is completed after six hours.
2.2.4Post processing
Use nipper pliers to remove the support parts and use quartz sand papers of different thicknesses to polish the insole surface.
2.2.5Installation and use
Put the equipped insole inside the shoes with the 3D printing orthotic insole, adjust the position, stick the double-sided stickers between the orthotic insole and the equipped insole to avoid sliding when walking.
2.3Research methods
The selected patients who met the criteria were fully informed about the research content and agreed to sign the informed consent form. The physician asked about their general conditions (health status, medication conditions), daily activities (average daily sitting, standing, walking, working and physical activity time) before the intervention, and then LLD was further confirmed by the therapist. An initial evaluation of the patient’s pain, gait and life quality was conducted and a final evaluation would be conducted after 12 weeks.
The used intervention method was the 3D printing orthotic insole: the patient’s feet were customized on a 2/3 length type insole, the long side lower leg insole thickness was 3 mm, the short one was thicker than the long side lower limb, and the height difference was approximately 80% of the LLD discrepant distance. If there was a big difference in LLD, the height difference was adjusted multiple times, the first time was 5 mm and another 5 mm after two weeks, until it was 15 mm. When the height difference was bigger than 10 cm, then it was recommended to wear ankle-high shoes. If the patient needed to adjust the LLD difference by more than 15 mm, a shoe lift outside the shoe was added. After customizing the insole, the patient was required to wear it during the activity.
During the intervention period, all selected patients were required not to change their daily activities and habits and not to engage in other rehabilitation treatments (e.g. physical factor therapy, massage therapy). If they were engaged in another treatment, they could only be selected when they had discontinued the activities for at least two weeks. The existed drug could be taken and they were not suggested to change the dose. Patients were asked to record daily activities and wearing experience. The researchers made follow-up calls every two weeks. The research method was approved by the Ethics Committee of Shanghai No. 4 Rehabilitation Hospital.
2.4Evaluation methods
The evaluation was conducted by two therapists with more than three years of working experience.
LLD measurement: we used the indirect method. The patient kept the standing position, head up, placed hands naturally on the side of the body, kept their feet apart for 15–20 cm. Imposed a block with certain thickness under the short lower limb to heighten the short side lower limb. When anterior superior iliac spines were at the same height on both sides, the imposed block thickness was considered to be the LLD difference length. This method is considered to be the most reliable method for measuring LLD in addition to radiological diagnosis [4].
Pain evaluation: we used the visual analogue scale (VAS). VAS card was produced by Pain Society of Chinese Medical Association, the two ends of the card showed “painless” (0) and “most severe pain” (10), the patient pointed out the index that best described the degree of pain at that time.
3D gait analysis: we used the Gait Watch gait analysis system (Zhanghe Electric, Guangzhou, China). We assessed the temporal and spatial parameters and joint kinematic parameters of the subject’s gait. We collected the patient’s movement data of the pelvis, hip, knee and ankle joints in three planes. When the patient was tested, he/she walked straight by 12 m with conventional speed. This includes all data such as speed, step size, stride frequency, time, distance and foot position in real time.
Health questionnaire: We used the General Health Questionnaire-12 (GHQ-12), which could effectively evaluate the physical and mental conditions of the general population or patients. It included 12 questions, each with a score of 0-1-2-3 points: 0 points meant better than before; 1, same as before; 2, worse than before; 3, much worse than before. The higher the score, the worse the health condition. The GHQ-12 score is 0–36 points in total, the total score
3.Results
The selected patients were reconfirmed for differences in length of the lower limbs by indirect measurement, and then the 3D printing orthotic insole was customized. If the patient showed an abnormality in the foot arch and the anterior and posterior feet during the evaluation process, this was simultaneously corrected by the orthotic insole.
A total of seven patients completed the study. They were able to take notes, give timely feedback, and cooperate with the therapist’s guidance. The patients wore insoles every day, no insole rupture occurred in the final evaluation, and no damage or allergy occurred on foot skin (see Tables 1 and 2 for details).
Table 1
General conditions of the patients
| Patient | Gender | Age | Diagnosis | Disease time | LLD (heightened amount), abnormal foot type | Health condition | Medication | Daily activities |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 38 | Right tibiofibula fracture | 1 year | 10 mm short on right (heightened 8 mm) | No other chronic disease history | No long term medication history | Pain in right hip after walking for more than half an hour |
| 2 | F | 14 | Cerebral palsy, post Achilles tendon extension surgery | 2 years | 8 mm short on left (heightened 5 mm), low arch of both feet, left heel varus | No other chronic disease history | No long term medication history | Pain in left ankle after walking for 10 meters or more |
| 3 | F | 14 | Cerebral palsy, post Achilles tendon extension surgery | 2 years | 20 mm short on left (heightened 15 mm), low arch of both feet, right heel valgus | No other chronic disease history | No long term medication history | Pain in left knee joint after walking for 50 meters or more |
| 4 | F | 68 | Left femur fracture, post internal fixation surgery | 1 years | 20 mm short on left (heightened 15 mm) | No other chronic disease history | No long term medication history | Numbness in left knee, hip and back after walking for more than 100 meters, with pain in lower back |
| 5 | F | 69 | Cerebral infraction | 5 years | 15 mm short on right (heightened 10 mm), low arch of both feet, left heel mild valgus | High blood pressure | Hypotensive drug | Pain in right hip joint and lower back after walking for more than 100 meters, can’t stand and walk for long time |
| 6 | M | 34 | Hip arthroplasty, replacement surgery for loose prosthsis | 5 months | 22 mm shorter right leg (heightened for 12 mm), low arches of both feet, right heel with mild vagus, left heel with mild valgus | Post right femur osteosarcoma surgery | No long-term medication history | Pains in right hip and right knee when walking more than 100 meters |
| 7 | M | 34 | Left plantar fasciitis | 2 years | A 9 mm shorter left leg (heightened for 5 mm), right heel with mild valgus | No history of other chronic diseases | No long-term medication history | Pains in left knee joint and right navicular bone after walking for more than half an hour |
Table 2
Changes in the patients’ pain, health and gait
| Patient | Evaluation | Pain score (VAS) | Health condition (score) (GHQ-12) | Stride frequency (step/ minute) | Stride length (cm) | Pace (cm/s) | Step size (cm) (left/ | ||
|---|---|---|---|---|---|---|---|---|---|
| right) | Stance phase % (left/ right) | Swing phase % (left/ right) | |||||||
| 1 | Preliminary | 7 | 17 | 114 | 132 | 126 | 66/66 | 60/60 | 40/40 |
| Final | 1 | 5 | 122 | 140 | 142 | 71/69 | 59/59 | 41/41 | |
| 2 | Preliminary | 6 | 18 | 77 | 41 | 26 | 22/19 | 75/80 | 25/20 |
| Final | 2 | 6 | 93 | 59 | 46 | 33/26 | 64/63 | 36/37 | |
| 3 | Preliminary | 7 | 18 | 83 | 38 | 26 | 22/16 | 81/81 | 19/19 |
| Final | 2 | 7 | 103 | 57 | 49 | 36/21 | 61/63 | 39/37 | |
| 4 | Preliminary | 6 | 19 | 77 | 55 | 35 | 28/27 | 67/67 | 33/33 |
| Final | 1 | 8 | 102 | 86 | 73 | 42/43 | 62/63 | 38/37 | |
| 5 | Preliminary | 7 | 20 | 79 | 57 | 38 | 22/35 | 65/58 | 35/42 |
| Final | 2 | 8 | 83 | 79 | 54 | 34/44 | 62/60 | 38/40 | |
| 6 | Preliminary | 7 | 19 | 102 | 103 | 88 | 51/52 | 66/63 | 34/37 |
| Final | 2 | 7 | 106 | 106 | 94 | 54/52 | 63/61 | 37/39 | |
| 7 | Preliminary | 6 | 17 | 113 | 147 | 138 | 72/75 | 61/59 | 39/41 |
| Final | 1 | 6 | 113 | 154 | 145 | 78/76 | 60/59 | 40/41 |
4.Discussion
LLD patients have two adverse consequences: (1) when standing and walking, they have posture, balance and gait problems, such as pelvic tilt, scoliosis, gait abnormalities, etc. [5]; (2) musculoskeletal problems: they have limb pain after standing and walking, injury after exercise, such as back pain [6], knee arthritis [7], stress fracture [8] and so on. In terms of posture and balance, some scholars believe that if the unequal length of the lower limbs does not exceed 20 mm, because of the compensation mechanism works, there is generally no obvious limp when walking. The compensation mechanisms include increased foot pronation in the long lower limb and increased foot supination in the short lower limb during the supporting phase [9], the pelvic tilt to the short lower limb [10], scoliosis, etc. [11]. The unequal length of the lower limbs exceeds 20 mm will result in changes in the spine [12]. In a gait analysis study, Song et al. found that the LLD patient’s stride frequency and pace are reduced, and the stride time is larger than the normal value. The reason is that in order to alleviate the change of the body gravity center caused by limb asymmetry, the patient stabilizes the body gravity center during walking, resulting in a change in the support period and step time [13]. In the musculoskeletal system, LLD patients receive more impact on lower limb bones and joints than normal people while walking. Wretenberg et al. have found that when LLD reaches or exceeds 20 mm, it will result in changes in hip load in the long and short lower limbs, and bigger changes in the lower limbs [14]. Of the seven patients reported in this article, the result is consistent with the above mentioned changes in gait deviations, musculoskeletal load and joint pain after activity. Many scholars believe that LLD will also affect patient’s living ability and life quality [15]. In this article, gait deviations and joint pain are the main factors affecting their daily activities and life quality, and their health conditions have also declined (see Tables 1 and 2).
The treatment of LLD usually depends on the degree of LLD difference and the severity of the patient’s symptoms [16]. A shoe lift is one of the most common methods of treating LLD. It can improve patient’s gait and reduce the pain from LBP, hip arthritis and knee arthritis, as well as the patient’s function [17], but some scholars found that long-term use of a shoe lift of more than 10 mm will result in changes in biomechanical abnormalities such as a shortening of the Achilles tendon and lumbar lordosis [18]. The current use of a shoe lift is generally based on clinical judgment and experience [19]. A uniform standard has not been established and the reference is inconsistent with the use of the shoe lift [18, 19, 20]. Mark Campbell [2] has reviewed the studies of 10 shoe lifts in the treatment LLD which led to LBP, sciatica and hip pain, and he points out that in the above mentioned pain treatment caused by LLD, the shoe lift is effective. However, more and higher quality clinical application studies are needed, including improvements in shoe lift and observations of its effects.
In recent years, 3D printing technology has gradually been applied to the production of orthopedic braces and insoles [3, 21]. Due to the individualized and precise characteristics of 3D printing orthotic insoles, theoretically, it also has a certain effect on the treatment of LLD patients. From the seven cases reported in this article, by customizing the 3D printing orthotic insole, after 3 months of wearing, the joint pain and lower back pain were alleviated, and the gait was improved (see Tables 1 and 2). To the best of our knowledge, such research on the application of 3D printing orthotic insoles for patients with LLD has not yet been reported, which is the innovation of this research.
For the seven patients in our study, the 3D printing orthotic insole works better. In terms of the manufacturing process, the steps are clear and the operation is feasible. The 3D printing orthotic insole developed in this article has the following advantages. Compared with the commonly used prefabricated shoe lift, the foot is equipped with insoles on both sides. On the one hand, the feelings of the two foot are symmetrical, which increases the comfort of patient’s wearing perception. On the other hand, because many LLD patients have excessive pronation or supination compensation on both sides of the foot, it is often necessary to correct both feet in a neutral position at the same time. Compared with the currently used customized insoles (such as ICB and CNC machine tool insoles), 3D printing insoles can be adjusted to the density and style of different parts of the insole through modeling software. The design is very flexible and creative, the insole can be adapted according to the orthopedic needs, and the printing is done once after the design, without additional patches. In addition, since 3D printing is an additive manufacturing process, there is no corner scrap generated by cutting.
This article focuses on the production process of 3D printing insoles, as well as the preliminary application to seven LLD patients. The results show that there are better therapeutic effects and the clinical promotion is significant. The shortcomings are that the cases are fewer, the tracking time is short, the postural changes such as pelvis and scoliosis in LLD patients are not included in the study. If the topic is studied further, the comparative study, the expansion of the case and the scope of the study will be more meaningful.
3D printing is still a new technology. Although 3D printing insoles are commercially available, there are only a few reports on orthotic insoles. This might be because 3D software processing needs high professionalism, lacks printing materials, and the cost of scanning and printing equipment is still high, which limits the clinical application of 3D printing technology in orthopedic insoles. However, with the ‘fooling’ of 3D software processing, the increase of printing materials and the reduction of printing equipment cost, 3D printing orthopedic insoles will definitely gain popularity in clinical treatment.
Acknowledgments
The project was supported by the Joint Medical Research Program of Shanghai Jing’an District Science and Technology Commission and Health Commission, Shanghai, China (Grant No. 2017MS12). The authors would like to thank Ms. He Qun for editing the manuscript.
Conflict of interest
None to report.
References
[1] | Gurney B. Leg length discrepancy. Gait Posture. (2002) , 15: (2): 195-206. PMID: 11869914. |
[2] | Campbell TM, Ghaedi BB, Tanjong Ghogomu E, et al. Shoe lifts for leg length discrepancy in adults with common painful musculoskeletal conditions: A systematic review of the literature. Arch Phys Med Rehabil. (2018) , 99: (5): 981-993. PMID: 29229292. doi: 10.1016/j.apmr.2017.10.027. |
[3] | Cao P, Wu XG. Application of 3D printing technology in custom-made foot orthosis (review). Zhongguo Kangfu Lilun Yu Shijian. (2015) , 21: (7): 753-756. doi: 10.3969/j.issn.1006-9771.2015.07.003. |
[4] | Brady RJ, Dean JB, Skinner TM, et al. Limb length inequality: Clinical implications for assessment and intervention. J Orthop Sports Phys Ther. (2003) , 33: (5): 221-234. PMID: 12774997. doi: 10.2519/jospt.2003.33.5.221. |
[5] | Raczkowski JW, Daniszewska B, Zolynski K. Functional scoliosis caused by leg length discrepancy. Arch Med Sci. (2010) , 6: (3): 393-398. PMID: 22371777. doi: 10.5114/aoms.2010.14262. |
[6] | Defrin R, Ben Benyamin S, Aldubi RD, et al. Conservative correction of leg-length discrepancies of 10 mm or less for the relief of chronic low back pain. Arch Phys Med Rehabil. (2005) , 86: (11): 2075-2080. PMID: 16271551. doi: 10.1016/j.apmr.2005.06.012. |
[7] | Harvey WF, Yang M, Cooke TD, et al. Association of leg-length inequality with knee osteoarthritis: A cohort study. Ann Intern Med. (2010) , 152: (5): 287-295. PMID: 20194234. doi: 10.7326/0003-4819-152-5-201003020-00006. |
[8] | Guichet JM, Spivak JM, Trouilloud P, et al. Lower limb-length discrepancy. An epidemiologic study. Clin Orthop Relat Res. (1991) , (272): 235-241. PMID: 1934739. |
[9] | Resende RA, Kirkwood RN, Deluzio K, et al. Biomechanical strategies implemented to compensate for mild leg length discrepancy during gait. Gait Posture. (2016) , 46: : 147-153. PMID: 27131193. doi: 10.1016/j.gaitpost.2016.03.012. |
[10] | Gong W. The influence of pelvic adjustment on vertical jump height in female university students with functional leg length inequality. J Phys Ther Sci. (2015) , 27: (1): 251-253. PMID: 25642085. doi: 10.1589/jpts.27.251. |
[11] | Walsh M, Connolly P, Jenkinson A, et al. Leg length discrepancy-an experimental study of compensatory changes in three dimensions using gait analysis. Gait Posture. (2000) , 12: (2): 156-161. PMID: 10998613. |
[12] | Betsch M, Rapp W, Przibylla A, et al. Determination of the amount of leg length inequality that alters spinal posture in healthy subjects using rasterstereography. Eur Spine J. (2013) , 22: (6): 1354-1361. PMID: 23479027. doi: 10.1007/s00586-013-2720-x. |
[13] | Song L, Xing YH, Kang T, et al. Effects of leg length discrepancy on gait: An experimental study. Journal of Medical Biomechanics. (2016) , 31: (6): 501-505. doi: 10.3871/j.1004-7220.2016.06.501. |
[14] | Wretenberg P, Hugo A, Brostrom E. Hip joint load in relation to leg length discrepancy. Med Devices (Auckl). (2008) , 1: : 13-18. PMID: 22915902. |
[15] | Fujimaki H, Inaba Y, Kobayashi N, et al. Leg length discrepancy and lower limb alignment after total hip arthroplasty in unilateral hip osteoarthritis patients. J Orthop Sci. (2013) , 18: (6): 969-976. PMID: 23963590. doi: 10.1007/s00776-013-0457-3 |
[16] | Stanitski DF. Limb-length inequality: Assessment and treatment options. J Am Acad Orthop Surg. (1999) , 7: (3): 143-153. PMID: 10346823. |
[17] | Thakral R, Johnson AJ, Specht SC, et al. Limb-length discrepancy after total hip arthroplasty: Novel treatment and proposed algorithm for care. Orthopedics. (2014) , 37: (2): 101-106. PMID: 24679191. doi: 10.3928/01477447-20140124-06. |
[18] | Franklin ME, Chenier TC, Brauninger L, et al. Effects of positive heel inclination on posture. J Orthop Sports Phys Ther. (1995) , 21: (2): 94-99. PMID: 7711763. doi: 10.2519/jospt.1995.21.2.94. |
[19] | McCaw ST. Leg length inequality. Implications for running injury prevention. Sports Med. (1992) , 14: (6): 422-429. PMID: 1470794. |
[20] | Nakanowatari T, Suzukamo Y, Izumi SI. The effectiveness of specific exercise approach or modifiable heel lift in the treatment of functional leg length discrepancy in early post-surgery inpatients after total hip arthroplasty: A randomized controlled trial with a PROBE design. Phys Ther Res. (2016) , 19: (1): 39-49. PMID: 28289580. |
[21] | Wang K, Shi YT, He W, et al. The research on 3D printing fingerboard and the initial application on cerebral stroke patient’s hand spasm. Biomed Eng Online. (2018) , 17: (1): 92. PMID: 29941033. doi: 10.1186/s12938-018-0522-4. |


