
Patients with pacemakers or defibrillators do not need to worry about e-Cars: An observational study
Abstract
BACKGROUND:
Electric cars are increasingly used for public and private transportation and represent possible sources of electromagnetic interference (EMI). Potential implications for patients with cardiac implantable electronic devices (CIED) range from unnecessary driving restrictions to life-threatening device malfunction. This prospective, cross-sectional study was designed to assess the EMI risk of electric cars on CIED function.
METHODS:
One hundred and eight consecutive patients with CIEDs presenting for routine follow-up between May 2014 and January 2015 were enrolled in the study. The participants were exposed to electromagnetic fields generated by the four most common electric cars (Nissan Leaf, Tesla Model S, BMW i3, VW eUp) while roller-bench test-driving at Institute of Automotive Technology, Department of Mechanical Engineering, Technical University, Munich. The primary endpoint was any abnormalities in CIED function (e.g. oversensing with pacing-inhibition, inappropriate therapy or mode-switching) while driving or charging electric cars as assessed by electrocardiographic recordings and device interrogation.
RESULTS:
No change in device function or programming was seen in this cohort which is representative of contemporary CIED devices. The largest electromagnetic field detected was along the charging cable during high current charging (116.5
CONCLUSIONS:
Electric cars produce electromagnetic fields; however, they did not affect CIED function or programming in our cohort. Driving and charging of electric cars is likely safe for patients with CIEDs.
1.Introduction
Cardiac implantable electronic devices (CIEDs) such as permanent pacemakers (PMs), implantable cardioverter-defibrillators (ICDs) and cardiac resynchronization therapy (CRT) devices are standard of care for treatment of certain bradycardias, tachycardias, and heart failure [1, 2, 3, 4]. The prevalence of CIEDs is increasing [5, 6, 7].
Exposure to electromagnetic fields generated by everyday electrical equipment is ubiquitous; for example, communication and office equipment (e.g. cellular phones), household appliances (e.g. washing machines, dishwashers), power tools and industrial machines (e.g. welding equipment), and security devices (e.g. metal detectors) [8, 9]. In vitro studies demonstrate the potential for electromagnetic fields generated by electronic devices to be sensed by CIEDs and erroneously attributed to intrinsic intra-cardiac signals [10, 11]. This electromagnetic interference (EMI) can affect CIED function; resulting in pacing inhibition, delivery of inappropriate anti-tachycardia therapy (due to oversensing), or changes to programmed CIED parameters [12, 13]. CIED manufacturers are aware of potential risks and, in addition to providing patient education [14, 15], they mitigate EMI risk through improved noise-detection algorithms, shielding and filters for problematic frequencies. Adverse events are rare, but still occur [16, 17, 18, 19, 20].
Electric cars are a potential, emerging EMI source. The popularity of electric cars has grown and growth is predicted to continue aided by superior fuel efficiency and incentives to operate low-emission vehicles [21, 22, 23]. Therefore, increasing numbers of patients will be exposed to EMI via private vehicles and public transport. However, there is no data regarding the safety of electric cars for patients with CIEDs, nor is there evidence whether restrictions on patients with CIEDs are required. Device manufacturers recommend patients with CIEDs maintain a distance of at least 30 cm from engine ignition systems and electric boat motors [14, 15]. The engines of modern electric cars have outputs significantly larger than average ignition systems (60–310 kW vs 1–2 kW, respectively) [24, 25, 26]; however, there are no specific recommendations for electric car use.
The potential for EMI increases with the strength of electromagnetic field, which is proportional to the power of the electric motor. To assess this potential risk, we conducted in vivo evaluation of CIED function during exposure to driving and charging the four most popular electric cars in Europe [27]. The primary results of this study have been previously published as a brief research report in Annals of Internal Medicine, but the methodological details and specific device and leads characteristics are reported here [28].
2.Methods
2.1Statistics and sample size calculation
At the time of the study, there was no data on potential EMI between CIEDs and electric cars. Therefore, we based our sample size on the number required to detect common events; i.e., 1–10% [29]. Hence, we calculated 100 patients were required to observe at least one EMI event with a probability of 99.4% if the EMI event rate was 5%. With an estimated drop-out rate of 10%, the target sample size was 110 patients. Data are presented as numbers and percentage and mean
2.2Participants
Consecutive patients presenting for routine follow-up of PM, ICD or CRT function at our institution, between May 2014 and January 2015 were assessed for eligibility. Of 150, 40 declined to participate and two withdrew consent. Hence, we studied 108 patients. This cohort was predominantly male (83%) with a mean age of 58
Table 1
Patient and device characteristics
| Patient | |
|---|---|
| Total number | 108 |
| Men | 90 (83%) |
| Age (years) | 58 |
| Indication | |
| Indication for anti-bradycardia therapy (PM) | 34 (31%) |
| Sinus-node dysfunction | 16 (15%) |
| Atrioventricular block | 17 (16%) |
| Carotid sinus syndrome | 1 (1%) |
| Indication for anti-tachycardia therapy (ICD) | 74 (69%) |
| Primary prevention of SCD | 40 (37%) |
| Secondary prevention of SCD | 34 (31%) |
| Pacing mode | |
| VVI or VVIR | 37 (34%) |
| VVIRV | 2 (2%) |
| DDD or DDDR | 48 (44%) |
| DDD0V or DDDRV | 21 (19%) |
Values given as number with percentage in parentheses except age.
2.3Electric cars
The four electric cars with the largest market-share in Europe at the time of the study were evaluated: Nissan LEAF, Tesla Model S P85, BMW i3 and VW eUp [27]. All are full electric cars, but with different motor power, torque, battery-size and charging properties (Table 2). Hybrid electric vehicles, combining electric propulsion with conventional powertrain were excluded, because pure electric mode of operation (with associated maximal electromagnetic field) could not be ensured during testing.
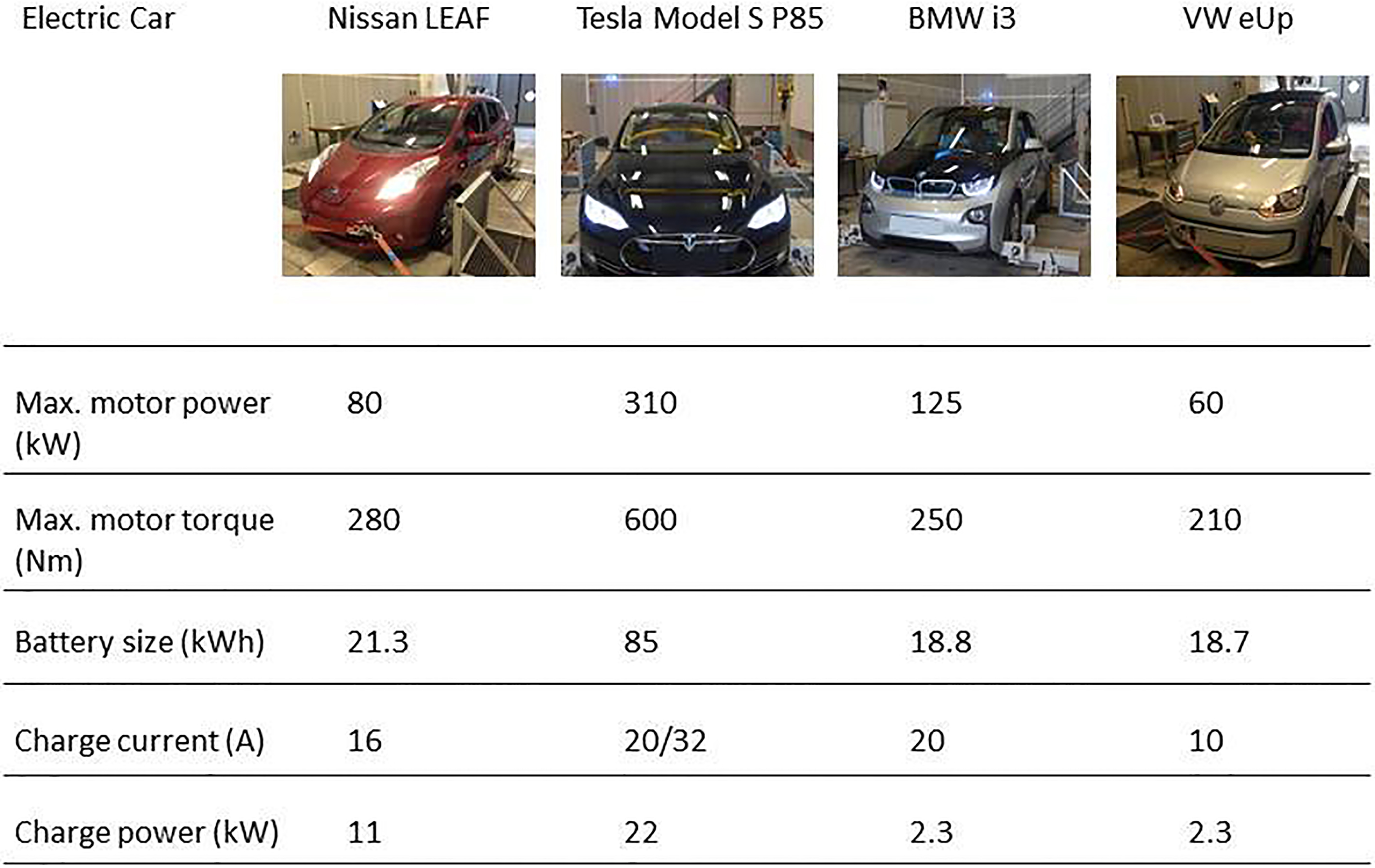
Table 3
Test protocols
| Test drive number | Protocol |
|---|---|
| 1 | Maximal acceleration to 30 km/h followed by braking to a full stop |
| 2 | Maximal acceleration to 50 km/h followed by braking to a full stop |
| 3 | Maximal acceleration to 80 km/h followed by braking to a full stop |
| 4 | Maximal acceleration to 120 km/h followed by braking to a full stop |
Table 4
CIEDs tested for EMI from electric cars
| Manufacturer | Device | Number of device tested | Type of device |
|---|---|---|---|
| Biotronik | |||
| Cylos | 1 | PM | |
| Ecuro | 1 | PM | |
| Effecta | 1 | PM | |
| Iforia | 3 | ICD | |
| Lumax | 8 | ICD | |
| Philos | 1 | PM | |
| Talos | 1 | PM | |
| Boston scientific | |||
| Advantio | 1 | PM | |
| Altrua | 1 | PM | |
| Cognis | 3 | ICD | |
| Dynagen | 1 | ICD | |
| Energen | 1 | ICD | |
| Incepta | 1 | ICD | |
| Ingenio | 2 | PM | |
| Inogen | 1 | ICD | |
| Punctua | 1 | ICD | |
| Guidant | |||
| Altrua | 1 | PM | |
| Vitality | 2 | ICD | |
| Medtronic | |||
| Adapta | 1 | PM | |
| Cardia | 1 | ICD | |
| Entrust | 2 | ICD | |
| Maximo | 2 | ICD | |
| Protecta | 5 | ICD | |
| Secura | 4 | ICD | |
| Sensia | 5 | PM | |
| Viva | 2 | ICD | |
| Sorin | |||
| Ovatio | 2 | ICD | |
| Paradym | 11 | ICD | |
| Reply | 3 | PM | |
| St. Jude Medical | |||
| Accent | 2 | PM | |
| Current | 3 | ICD | |
| Ellipse | 3 | ICD | |
| Fortify | 11 | ICD | |
| Identity | 1 | PM | |
| Promote | 2 | ICD | |
| Sustain | 2 | PM | |
| Unify | 5 | ICD | |
| Verity | 2 | PM | |
| Victory | 2 | PM | |
| Zephyr | 2 | PM | |
| Vitatron | |||
| C 20 | 1 | PM | |
| C 60 | 3 | PM |
ICD
Table 5
Leads tested for EMI from electric cars
| Manufacturer | Lead |
|
|---|---|---|
| Biotronik | ||
| Corox | 4 | |
| Linox | 9 | |
| Safio | 3 | |
| Selox | 1 | |
| Sentus | 2 | |
| Setrox | 7 | |
| Siello | 20 | |
| Solia | 4 | |
| Synox | 1 | |
| Y-53 | 1 | |
| Boston Scientific | ||
| Easytrak 3 | 1 | |
| Endotak Reliance | 4 | |
| Flextend | 3 | |
| Reliance 4-Front | 1 | |
| Guidant | ||
| Easytrak 2 | 2 | |
| Endotak Endurance | 1 | |
| Endotak Reliance | 6 | |
| LivaNova/Sorin | ||
| Beflex | 2 | |
| Tilda | 1 | |
| Vigila | 2 | |
| Volta | 1 | |
| Medtronic | ||
| 4057 | 3 | |
| 4598 | 1 | |
| Attain | 2 | |
| Attain StarFix | 1 | |
| CapSureEpi | 2 | |
| CapSureFix Novus | 12 | |
| CapSure Sense | 2 | |
| CapSure SP | 3 | |
| CapSure SP Novus | 4 | |
| Sprint | 1 | |
| Sprint Fidelis | 4 | |
| Sprint Quattro | 5 | |
| Sprint Quattro Secure | 5 | |
| St. Jude Medical | ||
| Durata | 26 | |
| IsoFlex | 1 | |
| OptiSense | 3 | |
| QuickFlex | 8 | |
| QuickSite | 1 | |
| Riata | 6 | |
| Tendril | 34 | |
| Vitatron | ||
| IMD49B Excellence | 2 | |
| Unknown | ||
| 4 |
Figure 1.
Magnetic field strength during testing.
![Magnetic field strength during testing. *Values displayed as maximal field strength and as a percentage (normalized by frequency) of the maximum recommended exposure by ICNIRP [36]. Adapted from Ann Intern Med with permission [28].](https://ip.ios.semcs.net:443/media/thc/2020/28-1/thc-28-1-thc191891/thc-28-thc191891-g001.jpg)
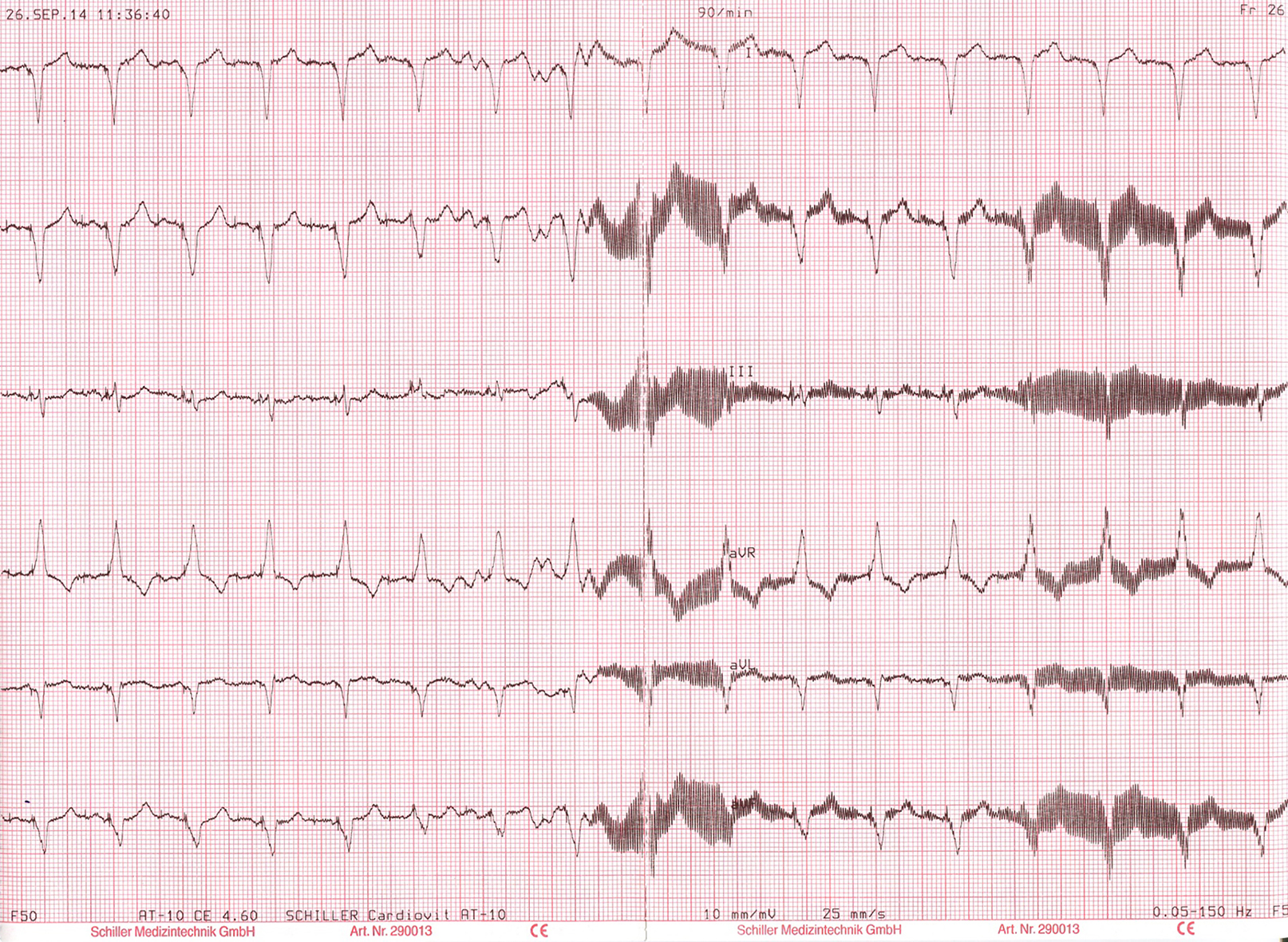
Figure 2.
High frequency, low amplitude EMI seen during testing.
2.4Roller dynamometer test-bench
Driving simulation took place on a roller dynamometer test-bench at the Institute of Automotive Technology, Department of Mechanical Engineering, Technical University of Munich, Germany. The roller test-bench enabled programmed simulation of dynamic driving resistances encountered in real life. Additionally, the roller-bench facilitates safe, standardised and reproducible test cycles with maximal acceleration and deceleration protocols; essential to obtain maximal engine torque and subsequent maximal electromagnetic field generation [32].
2.5Measurement of electromagnetic fields
Magnetic field strength was measured as a surrogate for electromagnetic field strength. There is a direct relationship between magnetic and electromagnetic field strength which permits the use of this surrogate measurement. The magnetic field meter used was a calibrated ELT 400 (Narda-STS, Pfullingen, Germany) and a B-field probe (three orthogonal coils; total sensing area
2.6Test protocol
Patients underwent routine device interrogation following our standardized device follow-up protocol including evaluation of battery status, pacing and sensing thresholds, lead impedances and review of CIED event monitors. In all patients, ventricular pacing was ensured by increasing the basic pacing rate or by adjusting the atrio-ventricular delay in dual chamber devices. Pre-programmed sensitivity levels were unchanged. In ICDs, tachyarrhythmia detection algorithms were set to the minimum number of intervals to enhance the probability of inappropriate arrhythmia detection. ICD shocks were disabled during the study where applicable. This optimized CIED programming for identification of EMI have been established in other EMI-studies [33, 34, 35].
Patients sat in the front seat of the cars while on the test-bench and the electromagnetic field strength within 5 cm of the CIED was recorded. Under continuous 6-lead ECG recording patients were instructed to perform pre-defined maximal accelerations and decelerations (Table 3). Patients then charged the car; this included plugging in, holding and unplugging the charger cable under continuous ECG-monitoring. Each patient performed this protocol with a single car.
All ECGs were analyzed for abnormal CIED function; e.g. inhibition of pacing, loss of capture, tracking to the upper rate limit or inappropriate mode switch. Device event monitors were interrogated for ventricular over-sensing resulting in inappropriate tachyarrhythmia detection. After each test, the device settings were compared with the initial settings to identify spontaneous reprogramming and the CIED subsequently reprogrammed to the settings specific for that patient.
All ECG recordings were independently analyzed by two cardiologists blinded to patient and car.
The study was approved by the ethics committee of Technical University of Munich, Munich, Germany and registered with clinicaltrials.gov (NCT02252575).
3.Results
3.1Device types
One hundred and eight CIEDs comprising 42 different CIED families from 7 manufacturers were tested (Table 4). Of the 108 CIEDs 46 (42.6%) were dual chamber or CRT-ICDs, 28 (26%) were single chamber ICDs, 31 (28.7%) were dual chamber PMs, and 3 (2.7%) were single chamber PMs. One hundred and eighty-three leads (75 atrial and 108 ventricular) comprising 42 lead families from 7 manufacturers were tested (Table 5). The mean sensitivity was 0.43
3.2Magnetic field
The magnetic fields measured in and around the cars while driving on the test-bench and charging are shown in Fig. 1. The International Commission on Non-Ionizing Radiation Protection (ICNIRP) recommended exposure to magnetic fields for the general population varies with the magnetic field frequency and so field strengths are presented as absolute values (inclusive of all frequencies) and as a percentage of recommended exposure normalized for frequency [36]. The largest magnetic field measured was along the cable during charging; 116.5
The magnetic field of the test-bench measured in stand-by and with full-load torque was 1
3.3Functional device interference
We observed no evidence of EMI when driving nor when plugging in and charging. There were no episodes of over- or under-sensing, no inappropriate pacing or inhibition of pacing and no spontaneous device re-programming occurred. Pacing thresholds, sensing and lead impedance remained unchanged on post-test examination.
3.4Electromagnetic interference with ECG-machine
The only EMI detected was with the ECG-machine. An example of the high-frequency EMI signal is shown in Fig. 2. The underlying pacemaker rhythm was not influenced as demonstrated by the constant, paced R-R intervals (CL 667 ms) and there was no functional effect on the CIED when interrogated.
4.Conclusions
To our knowledge, this is the first study to evaluate the effect of electromagnetic fields and potential EMI produced by fully electric cars on CIEDs. We found no effect on CIED functional or programming during driving or charging.
Though our group have previously published the primary safety outcome of this study here we report the full methodological details and importantly the complete details of devices tested. This demonstrates the wide selection of devices studied and thus the generalisability of our results. Furthermore, it facilitates industry, physicians and patients to assess whether a particular device has been evaluated.
We aimed to maximise observation of detectable EMI by reducing tachyarrhythmia detection to minimal settings and placing patients in several locations in and around the car during maximal engine output and during charging.
Fully electric cars were selected because the electromagnetic field of hybrid vehicles varies due to concurrent internal combustion engine use. Moreover maximal power is usually higher in pure electric than in hybrid vehicle. Our results are consistent with a smaller study that investigated EMI in a single hybrid vehicle [37]. Nevertheless, important differences in our study include the testing of multiple models; all fully electric. This enabled evaluation of more powerful electric motors and their associated electromagnetic fields than is possible in hybrid vehicles. Furthermore, use of a resistive roller-bench rather than a suspended car for test drives allows maximal engine power output to be achieved and thus generation of maximum electromagnetic fields; circumstances impossible with a suspended car.
The magnetic fields within the cabin during road driving matched that during roller-bench testing. It is thus reasonable to assume that our measurements are representative of real-life driving.
Electric cars are designed with electromagnetic shielding to prevent interference with other on-board computer systems. Therefore, it is reasonable to anticipate the shielding also provides protection from EMI to CIEDs inside the car. Indeed, the magnetic field measured inside the cabin (2.1–3.6
The main source of the electromagnetic field generated by electric cars is the battery, though there is contribution from the power inverters, wiring, and power steering pumps [32, 38]. Differences in location of the battery and of other source components are the likely explanation for the variation of the electromagnetic field around the cars. However, the magnetic field detected around the cars is unlikely to be clinically relevant because it is only produced by moving cars and pedestrians would be exposed for a very short time.
More potentially clinically-relevant exposures occurred during charging; the observed values were consistent with previous studies [32]. A plausible explanation for the higher values is that the charging cable is less shielded. Despite this, no events were detected during charging while standing next to the cable. It should be noted that the recommended exposure limits were designed to prevent adverse health outcomes and pertain to biological systems and not electronic devices. The field strength along the charging cable increased as current increased. This is relevant because of plans to increase charging capability to deliver up to 400A (versus 32A maximum in our study) and thereby produce larger electromagnetic fields [39].
Stunder et al. demonstrated that PM with nominal sensitivity settings encountered EMI in a magnetic field starting from 300
No restrictions were placed on types of lead or device, thus increasing generalizability of our results. We did not study effects at speeds over 120 km/h, but magnetic fields are strongest with maximal acceleration and are unrelated to speed. Our results are not definitive evidence of safety; however, if there is EMI between electric vehicles and CIED, it would be a rare event. Future research should investigate potential EMI produced by super-charging cables and how to shield these cables for patients with CIEDs.
Although our sample size was too small to detect rare events (between 1 in 1,000 and 1 in 10,000) [29], other information supports the conclusion that riding in electric cars is safe for patients with CIEDs. First, magnetic fields can also be generated in gasoline-powered cars if the steel-belted tires are magnetized [41]; average values of
In summary, electromagnetic fields produced by electric cars did not affect function or programming of CIEDs in our cohort. These results suggest current electric cars are safe for patients with CIEDs and no restrictions on travelling in them are required. Nevertheless, vigilance is required to monitor for rare events, especially associated with vehicle charging and proposed super-charger technology.
Acknowledgments
The study was supported by the Karl and Lore Klein Stiftung. The funder had no role in study design, data collection and analysis, or reporting. The grant was used to rent the cars and test-bench and cover personnel costs.
References
[1] | Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Europace. (2013) ; 15: (8): 1070–118. |
[2] | Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. (2015) ; 36: (41): 2793–867. |
[3] | Tracy CM, Epstein AE, Darbar D, DiMarco JP, Dunbar SB, Estes NAM, et al. 2012 ACCF/AHA/HRS focused update incorporated into the ACCF/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities. J Am Coll Cardiol. (2013) Jan; 61: (3): e6–75. |
[4] | Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. (2016) Jul 14; 37: (27): 2129–200. |
[5] | Mond HG, Proclemer A. The 11th world survey of cardiac pacing and implantable cardioverter-defibrillators: calendar year 2009-a World Society of Arrhythmia’s project. Pacing Clin Electrophysiol. (2011) Aug; 34: (8): 1013–27. |
[6] | Greenspon AJ, Patel JD, Lau E, Ochoa JA, Frisch DR, Ho RT, et al. 16-Year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States: 1993 to 2008. J Am Coll Cardiol. (2011) ; 58: (10): 1001–6. |
[7] | Hatala R, Lunati M, Calvi V, Favale S, Goncalvesová E, Haim M, et al. Clinical implementation of cardiac resynchronization therapy-regional disparities across selected ESC member countries. Ann Noninvasive Electrocardiol. (2015) Jan; 20: (1): 43–52. |
[8] | Leitgeb N, Cech R, Schröttner J, Lehofer P, Schmidpeter U, Rampetsreiter M. Magnetic emissions of electric appliances. Int J Hyg Environ Health. (2008) Mar; 211: (1–2): 69–73. |
[9] | Gajšek P, Ravazzani P, Grellier J, Samaras T, Bakos J, Thuróczy G. Review of Studies Concerning Electromagnetic Field (EMF) Exposure Assessment in Europe: Low Frequency Fields (50 Hz–100 kHz). Int J Environ Res Public Health. (2016) Sep 1; 13: (9): 875. |
[10] | Dawson TW, Caputa K, Stuchly MA, Shepard RB, Kavet R, Sastre A. Pacemaker interference by magnetic fields at power line frequencies. IEEE Trans Biomed Eng. (2002) Mar; 49: (3): 254–62. |
[11] | Scholten A, Silny J. The interference threshold of unipolar cardiac pacemakers in extremely low frequency magnetic fields. J Med Eng Technol. (2001) ; 25: (5): 185–94. |
[12] | Beinart R, Nazarian S. Effects of external electrical and magnetic fields on pacemakers and defibrillators: from engineering principles to clinical practice. Circulation. (2013) Dec 24; 128: (25): 2799–809. |
[13] | Misiri J, Kusumoto F, Goldschlager N. Electromagnetic interference and implanted cardiac devices: the nonmedical environment (Part I). Clin Cardiol. (2012) May; 35: (5): 276–80. |
[14] | Medtronic. Answers to Questions about Implantable Cardiac Devices, electromagnetic compatability guide [Internet]. 2016 [cited (2016) Sep 5]. Available from: http://www.medtronic.com/content/dam/medtronic-com-m/mdt/documents/emc_guide.pdf. |
[15] | StJude. ICD and Pacemaker Interference: Dealing With EMI [Internet]. [cited (2017) Sep 5]. Available from: https://www.sjm.com/en/patients/arrhythmias/living-with-your-treatment/electromagnetic-interference?alert=DeepLinkSoftAlert&clset=af584191-45c9-4201-8740-5409f4cf8bdd%3Ab20716c1-c2a6-4e4c-844b-d0dd6899eb3a. |
[16] | Kolb C, Zrenner B, Schmitt C. Incidence of electromagnetic interference in implantable cardioverter defibrillators. Pacing Clin Electrophysiol. (2001) Apr; 24: (4): 465–8. |
[17] | Trigano A, Blandeau O, Dale C, Wong MF, Wiart J. Reliability of electromagnetic filters of cardiac pacemakers tested by cellular telephone ringing. Hear Rhythm. (2005) ; 2: (8): 837–41. |
[18] | Naegeli B, Osswald S, Deola M, Burkart F. Intermittent pacemaker dysfunction caused by digital mobile telephones. J Am Coll Cardiol. (1996) May; 27: (6): 1471–7. |
[19] | Hofgärtner F, Müller T, Sigel H. Could C- and D-network mobile phones endanger patients with pacemakers? DMW – Dtsch Medizinische Wochenschrift. (2008) Mar 25; 121: (20): 646–52. |
[20] | von Olshausen G, Rondak I-C, Lennerz C, Semmler V, Grebmer C, Reents T, et al. Electromagnetic interference in implantable cardioverter defibrillators: present but rare. Clin Res Cardiol. (2016) Aug; 105: (8): 657–65. |
[21] | Handelsblatt. Prognose zum weltweiten Umsatz mit Elektrofahrzeugen von 2010 bis 2030. Optional translation of article title: Forcast for global sales of electric cars from 2010 to 2030. [Internet]. [cited (2017) Aug 19]. Available from: https://de.statista.com/statistik/daten/studie/173157/umfrage/prognose-zum-weltweiten-umsatz-mit-elektrofahrzeugen/%0A. |
[22] | WirtschaftsWoche. Politisch gewünschte Anzahl der Elektroautos im Jahr 2020 nach Ländern. Optional translation of article title: Political targets for the number of electric cars in 2020 by country. [Internet]. [cited (2017) Aug 19]. Available from: https://de.statista.com/statistik/daten/studie/180290/umfrage/politisch-gewuenschte-anzahl-der-elektroautos-im-jahr-2020/. |
[23] | A European Strategy for Low-Emission Mobility – Commission to the European parliament, the council, the European economic and social committee and the committee of the regions [Internet]. [cited (2017) Oct 16]. Available from: https://ec.europa.eu/transport/sites/transport/files/themes/strategies/news/doc/2016-07-20-decarbonisation/com%282016%29501_en.pdf. |
[24] | Volkswagen UK. Volkswagen eUP specifications [Internet]. [cited (2017) Oct 16]. Available from: www.volkswagen.co.uk/new/up-pa/which-model-compare/details/2800#!#tech-spec. |
[25] | Tesla Motors. Tesla Models S specifications [Internet]. [cited (2017) Oct 16]. Available from: www.tesla.com/en_GB/models. |
[26] | AC Delco 336-2060 Starter, Autoparts Warehouse [Internet]. [cited (2017) Oct 17]. Available from: http://www.autopartswarehouse.com/sku/AC_Delco/Starter/AC3362060.html. |
[27] | Bimmertoday.de. Anzahl der Neuzulassungen von Elektroautos in Europa im Jahr 2014 nach Modellen. Optional translation of article title: Number of registrations of electric cars in Europe in 2014 by model [Internet]. [cited (2017) Feb 5]. Available from: http://de.statista.com/statistik/daten/studie/431419/umfrage/anzahl-verkaufter-elektroautos-in-europa%0A. |
[28] | Lennerz C, O’Connor M, Horlbeck L, Michel J, Weigand S, Grebmer C, et al. Electric cars and electromagnetic interference with cardiac electronic implantable devices: a cross-sectional evaluation. Ann Intern Med. (2018) ; 169: (5): 350–352. https://annals.org/aim/article-abstract/2679357/electric-cars-electromagnetic-interference-cardiac-implantable-electronic-devices-cross-sectional. |
[29] | A Guideline on summary of product characteristics – Consumer goods, Pharmaceuticals – European commission for enterprise and industry [Internet]. [cited (2017) Oct 16]. Available from: https://ec.europa.eu/health//sites/health/files/files/eudralex/vol-2/c/smpc_guideline_rev2_en.pdf. |
[30] | BMW. BMW i3 Specifications [Internet]. [cited (2017) Oct 16]. Available from: www.bmwusa.com/standard/content/vehicles/2017/i3/bmwi3/features_and_specs/default.aspx. |
[31] | Nissan USA. Nissan leaf specifications [Internet]. [cited (2017) Oct 16]. Available from: www.nissanusa.com/electric-cars/leaf/. |
[32] | Vassilev A, Ferber A, Wehrmann C, Pinaud O, Schilling M, Ruddle A. Magnetic field exposure assessment in electric vehicles. IEEE Trans Electromagn Compatability. (2015) ; 57: (1): 35–43. |
[33] | Lennerz C, Pavaci H, Grebmer C, Semmler V, ier F, Haller B, et al. Electromagnetic interference in cardiac implantable electronic devices. J Am Coll Cardiol. (2017) Jan; 69: (1): 108–10. |
[34] | Kolb C, Schmieder S, Lehmann G, Zrenner B, Karch MR, Plewan A, et al. Do airport metal detectors interfere with implantable pacemakers or cardioverter-defibrillators? J Am Coll Cardiol. (2003) Jun; 41: (11): 2054–9. |
[35] | Jilek C, Tzeis S, Vrazic H, Semmler V, Andrikopoulos G, Reents T, et al. Safety of screening procedures with hand-held metal detectors among patients with implanted cardiac rhythm devices. Ann Intern Med. (2011) Nov 1; 155: (9): 587. |
[36] | ICNIRP. ICNIRP Guidelines for limiting exposure to time-varying electric, magnetic and electromagnetic fields [Internet]. [cited (2017) Sep 5]. Available from: www.icnirp.org/cms/upload/publications/ICNIRPemfgdl.pdf |
[37] | Tondato F, Bazzell J, Schwartz L, Mc Donald BW, Fisher R, Anderson SS, et al. Safety and interaction of patients with implantable cardiac defibrillators driving a hybrid vehicle. Int J Cardiol. (2017) Jan; 227: : 318–24. |
[38] | Concha P, Velez P, Lafoz M, Arribas J. Passenger exposure to magnetic fields due to the batteies of an electric vehicle. IEEE Trans Veh Technol. (2016) ; 65: (6): 4564–71. |
[39] | Foley A, Winning I, O’Gallachoir B. State-of-the-Art in Electric Vehicle Chargng Infrastructure. In: Vehicle Power and Propulsion Conf IEEE. (2010) . pp. 1–6. |
[40] | Stunder D, Seckler T, Joosten S, Zink MD, Driessen S, Kraus T, et al. In vivo study of electromagnetic interference with pacemakers caused by everyday electric and magnetic fields. Circulation. (2017) Feb 28; 135: (9): 907–9. |
[41] | Milham S, Hatfield J, Tell R. Magnetic fields from steel-belted radial tires: implications for epidemiologic studies. Bioelectromagnetics. (1999) ; 20: (7): 440–7. |
[42] | Stankowski S, Kessi A, Becheiraz O, Meier-Engel K, Meier M. Low frequency magnetic fields induced by car tire magnetization. Health Phys. (2006) Feb; 90: (2): 148–53. |
[43] | Halgamuge MN, Abeyrathne CD, Mendis P. Measurement and analysis of electromagnetic fields from trams, trains and hybrid cars. Radiat Prot Dosimetry. (2010) Oct 1; 141: (3): 255–68. |


