
Identifying pain and distress in non-verbal persons with intellectual disability: Professional caregivers’ and parents’ attitudes towards using wearable sensors
Abstract
BACKGROUND:
Persons with severe intellectual disability (ID) may be non-verbal and unable to communicate pain or distress. Consequently, painful conditions may go undetected, and non-verbal persons with ID may not receive adequate care and treatment.
OBJECTIVE:
This study aims to explore how professional caregivers and parents identify pain and distress in non-verbal persons with ID, and their attitudes towards using wearable sensors to identify pain and distress in daily life situations.
METHODS:
Exploratory, mixed method study. Caregivers (83) answered an online questionnaire, and professional caregivers (18) and parents (7) were interviewed.
RESULTS:
Professional caregivers and parents recognise pain and distress from observations and behavioural signs that are often equivocal. They experience that this is inadequate to reliably detect pain and distress in non-verbal persons with ID. Professional caregivers and parents’ express frustration and fear that painful conditions may remain untreated. They are positive towards using wearable sensors on condition that sensors do not infringe on user autonomy and privacy.
CONCLUSIONS:
There is a need for sensors and methods that can objectively identify pain and distress and ensure adequate treatment, that may improve quality of life of non-verbal persons with ID.
1.Introduction
Intellectual disability (ID) is a neurological condition that affects approximately 1% of the population [1, 2]. ID is characterized by significant limitations in intellectual functioning and adaptive behaviour [3, 4]. The condition affects communicative ability and everyday social and practical skills. ID may be caused by a wide range of genetic or acquired conditions and implies IQ below 70. Among those with ID, approximately 5% have severe ID (IQ 20–34) or profound ID (IQ
Persons with ID are as sensitive to pain as the general population [7, 8], but non-verbal persons with ID may be unable to convey that they are in pain or feeling uncomfortable. Hence, there is a risk that pain is unrecognised and undertreated in this group [9, 10, 11, 12].
Use of physiological sensors to detect pain, stress, or emotions has been an area of research for decades [13, 14, 15], and correlations between acute pain or emotional arousal and increased heart rate (HR) have been demonstrated [16, 17, 18, 19]. Available sensors vary from off-the shelf devices such as HR monitors and sleep monitors for everyday use to more advanced equipment for clinical and laboratory settings. Wearable sensors monitoring physiological responses have been used to detect pain or stress in various populations, both in laboratory and daily life situations [14, 17, 20, 21, 22].
It is demonstrated that for persons with severe communication challenges, wearable sensors monitoring HR may complement caregivers’ observation of behaviours and facilitate identification of pain and distress [17]. However, to make wearable sensors useful for non-verbal persons with ID and their caregivers, possible barriers, and facilitators towards their use in real life situations must be identified.
In this study we investigate how professional caregivers and parents usually identify pain and signs of distress, and explore their attitudes towards using wearable sensors for identifying and understanding pain and distress in non-verbal persons with ID. This paper describes the initial stage of a comprehensive research study monitoring HR to identify pain and distress in the target group.
2.Methods
2.1Study design
We implemented an exploratory mixed method study design, including quantitative data from an online survey among professional caregivers (
In this study, children and adults with ID and severe speech, language, or communication difficulties are referred to as “non-verbal persons with ID” or “users” as they are users of public services at home or in assisted living facilities.
2.2Recruitment of informants
Professional caregivers were recruited by administrative leaders in three districts of Oslo city for the online survey and focus group interviews. These caregivers were working at municipal assisted living facilities providing 24-hour care for persons with ID. Parents of non-verbal children with ID, aged 7 to 17 years, living at home, were recruited for focus group interviews by The Association for Cerebral Palsy and The Norwegian Association for Persons with Intellectual Disabilities and Relatives (LUPE).
For the focus group interviews, eighteen professional caregivers caring for non-verbal persons with ID aged 10 to 70 years were selected, by administrative leaders, as key informants, due to their extensive experience with the user group. The educational background of the key informants were social educators, occupational therapists, teachers, health care workers and administrative staff; 89% were female.
Figure 1.
Characteristics of the informants (
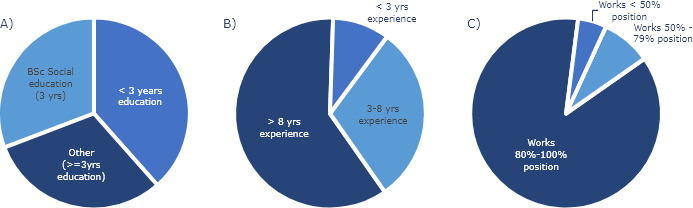
For the online survey we emailed the questionnaire to 327 professional caregivers working at assisted living facilities for persons with ID in the three districts. Of these, 102 caregivers opened the survey invitation. 83 caregivers answered the questionnaire and were included in the study; 67% were female. Most informants were highly trained and experienced in interaction with the user group: Almost two thirds of the informants had more than 3 years higher education relevant for their work, of which 31% were social educators (i.e. bachelor’s degree like the British “disability nurse”) and 31% were therapists or teachers with a bachelor’s degree or equivalent. The remaining 38% of the informants had certificate of apprenticeship in health care (see Fig. 1A). The informants were 18–65 years old; 27% were 18–30 years, 36% were 31–45 years, and 37 % were 46–65 years of age. Sixty percent of the informants had minimum 8 years of experience of interacting with non-verbal persons with ID while only 10% had worked less than three years with the user group (see Fig. 1B). The majority worked full time in close interaction with the user group (see Fig. 1C).
2.3Data collection and analysis
Initially, focus group interviews were accomplished. Interview guides were developed to facilitate three focus group interviews respectively with parents and caregivers conducted by two researchers [23]. The interview guide included open ended questions on topics as how parents and caregivers communicate with non-verbal persons with ID, how they assess pain and distress and what kind of support or technology they prefer to identifying pain and distress. Each focus group interview lasted 90–120 minutes, they were audio recorded and observational notes were taken during the interviews. Recordings were transcribed word-by-word. The transcribed data were inductively coded for content into themes with reference to the research question. After multiple readings of the text by two researchers independently, the following main themes were determined: 1) Identifying and understanding pain and distress, 2) Assessment methods and tools, 3) Attitudes towards using sensors, 4) Acceptability of different types of sensors and 5) Autonomy and privacy. Quotes from parents and caregivers highlights the results. All quotes and codes were collected in Norwegian and translated to English after coding and analysis.
The role of the researcher was discussed between the researcher after each interview, during the design of the survey and during data analysis, to be aware of any unintentional influence provided by the researcher during the research process.
An online questionnaire was developed, with reference to findings from the interviews and inspired by Wolbring and Leopatra [24]. The questionnaire asked demographic information about the informants, how they assess pain and distress in non-verbal persons with ID, if they have adequate tools for assessing pain and distress, their awareness and acceptance of sensors that may facilitate communication with the users, which sensor modalities the informants believed the users would accept, ethical issues and any concerns that may occur using wearables. The link to the online survey was distributed by email to the professional caregivers. Data collected in SurveyMonkey [25] were analysed statistically, using frequency analysis. A subset of data was analysed with the two-tailed Fisher’s exact test. The significance level was set at
3.Results
3.1Identifying pain and distress is challenging
In our study pain is described as an unpleasant sensory and emotional experience associated with actual or potential tissue damage [26]. Pain is a physical sensation, but is influenced by attitudes, beliefs, personality, and social factors, and can affect emotional and mental well-being by causing anxiety or emotional distress.
Caregivers and parents confirmed that non-verbal persons with ID often have reduced ability to communicate pain and emotional stress. Even if users were able to articulate some words, they experienced that the meaning could be equivocal. Some explained that users were screaming and expressing pain, even if the situation was not expected to be physical painful. The users may scream because they were afraid or anxious upfront of an activity or situation. Informants also reported that some users had challenges understanding speech. Five out of six children used digital devices for augmented and alternative communication (AAC). Parents reported, however, that digital AAC devices did not enable their children to adequately express pain and distress. Some adult users used pictures and symbols for communication, but caregivers experienced that this was not adequate for expressing pain and distress.
Caregivers and parents reported that they rely on visual observations and recognition of behaviour, voice, gestures, sweating, self-injury, etc. to detect signs of pain and distress in non-verbal persons with ID. They experienced that the signs are individual and not necessarily intuitively meaningful, which makes them difficult to interpret. Conflicting expressions, like screams or becoming quiet, could both indicate pain or distress, depending on the individual user and the context. Caregivers experienced that aggressive behaviour or self-injury may originate from pain and distress, and they would like to identify possible pain or distress upfront of challenging behaviour.
Caregivers and parents consistently informed that observations and interpretations of body language, behaviour and sounds are insufficient to adequately understand signs of pain and distress. They feared that users being unable to communicate pain or distress adequately may suffer harm, and that necessary interventions could be delayed or not implemented. One caregiver [C-1] stated: “We interpret body language and behaviour, facial expressions, flickering looks, tears, sounds, anxiety, sweat, exhaustion, and so forth. We are guessing and guessing, which is unacceptable, and we cannot continue doing so.” While one parents [P-1] explained: “Sometimes when he is screaming a lot, I become frustrated, because I do not understand what the matter is, and nothing calms him down. I do not know why he is crying. He might have had an epileptic seizure, gas pains, a dream, or nothing? It’s frustrating.”
Caregivers and parents emphasize the importance of knowing each individual user well to recognise and interpret behavioural signs correctly. Despite daily contact and observing the user over time, caregivers and parents felt frustrated and insecure because they were left with no other option than guessing as to the cause of pain and distress.
3.2Need for assessment tools and measures
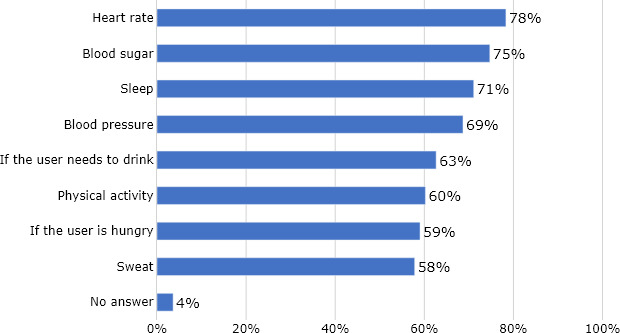
Figure 2.
Results from the online survey showing which type of sensors that professional caregivers believe non-verbal persons with ID will accept to use. Measuring HR was most acceptable. Four percent (3 persons) of the informants (
Almost three quarter of the professional caregivers (73%) in the online survey replied that they did not have adequate tools for user assessment and identifying pain and distress in non-verbal persons with ID, while a quarter (25%) reported to have adequate tools and 2% did not answer. Lack of adequate tools for pain assessment is supported by findings from the focus group interviews. Some professional caregivers used the visual analogue scale (VAS) [27] or self-designed assessment tools to subjective measure pain in persons with mild to moderate ID Others used Inventory of Potential Communicative Acts (IPCA) [28] translated into local language, to describe the communicative acts of non-verbal children with ID. However, the informants reported that these tools were not sufficient to identify pain and distress in non-verbal persons with severe ID during daily activities.
Caregivers experienced that most persons with severe ID were unable to locate pain or use self-reporting tools like VAS to measure pain. Caregivers are well trained at observing the user and carefully register daily routines like eating, drinking, personal hygiene, resting, sleeping, various behaviours, movements, perceived dissatisfaction, and various incidents. However, they still expressed the need for tools to identify pain, distress, anxiety, etc. in real life settings. Caregivers also highlighted the need for tools that would be equally well understood by caregivers, general practitioners, and specialists. A caregiver [C-2] explained: “Yes, we register (on paper/in the medical chart) when we think there is pain or distress. But it’s not at all that easy to record. Registrations made by one person may be interpreted differently by another. So, there are, yes, there are many challenges.”
Caregivers’ express concerns that non-verbal persons with ID may not receive appropriate medical treatment. General practitioners and specialists may not be aware that the target group may express pain differently from the general population. The caregiver may interpret behaviours as indicating severe pain, whereas the physician registers no pain or low levels of pain and may not administer adequate medication. The caregiver [C-6] explained: “I told the general practitioner that she (the user) expressed either pain or severe pain. When he (the general practitioner) was dictating for the medical recoding, he reported that it was weak pain, because this was his interpretation. From what I experienced; she was in severe pain because she usually does not express any pain.”
Caregivers felt that sometimes physicians do not take their statements about the users seriously, because the information was given by proxy and not by the user. A caregiver [C-2] illustrated the situation: “Sometimes we feel that the physicians do not believe us, because we are talking on behalf of the user. We have been to countless medical appointments, but because they (the users) cannot express themselves, the physician says, now you must go back and make better observations. It ended up that a user had serious illness that was not detected.” While another caregiver [C-3] added: “We want to have objective measurements to bring to the physicians.”
Caregivers and parents alike, expressed the need for adequate tools to objectively identify the origin and intensity of pain experienced by non-verbal persons with ID, instead of auditive and visual expressions that may be interpreted differently.
3.3Attitudes towards the use of wearable sensors
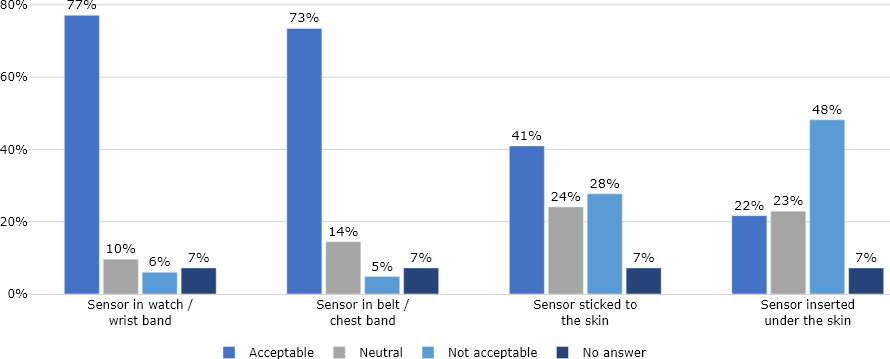
Figure 3.
Result from online survey showing how professional caregivers evaluate the ethical acceptance of using various sensor types for non-verbal persons with ID. Wearable sensors embedded in wrist band were most acceptable. Seven percent of the total number of informants (
Attitude is understood as a feeling or opinion about something or someone, or a way of behaving that is caused by this [29]. In our survey most informants (78%) replied that they would like to use sensors that facilitated communication with non-verbal persons with ID, while 13% would not like to use sensors, and 9% did not answer. A larger proportion of informants reporting that they lacked adequate tools were positive towards the use of sensors in their daily work (92%) than informants that were satisfied with today’s tools (65%) (
From interviews, caregivers and parents confirmed their positive attitudes towards using wearable sensors for communication and recognising pain in non-verbal persons with ID. A caregiver [C6] confirmed: “Sensors can be a nice tool. We need effective tools and methods to understand persons with severe disabilities, who cannot express themselves. We would like to identify illness or distress. This may increase quality of life for our users.” A parent [P-2] stated: “Using sensors sounds very interesting, and any tool or device that may help us understand our children will be useful.” In general, caregivers and parents were enthusiastic about using sensors if this may improve communication and help identify pain and distress, thereby increasing quality of life of non-verbal persons with ID.
Most informants were aware that increased HR are autonomic responses and may indicate acute pain, distress, or fear, but also joy, excitement, and physical activity. They clearly stated that the measurements need to be understood relative to the situation and with reference to behavioural and contextual observations, and one caregiver [C-8] explained: “Using sensors must always be considered in relation to the situation, and we do not want to measure more than necessary. We don’t want to measure without a specific purpose.” Caregivers also emphasised that sensors should only be utilised after individual assessment of user needs, and the purpose for using sensor should be clearly stated.
Informants with prior background information about our study on wearable sensors for non-verbal persons with ID [17] were relatively more positive towards using sensors in their daily work (97%) than the informants that were not familiar with the study monitoring HR (78%) (
3.4Type of sensors considered useful and acceptable
In the online survey, informants were asked to consider which type of sensors they believed the users would accept; sensors for measuring HR, blood sugar, sleep, blood pressure, physical activity or need for food and liquid. The majority stated that they assumed the users would accept sensors measuring HR (78%), blood sugar (75%), sleep (71%), or blood pressure (69%). Additionally, more than half of the informants answered that they expected that the user would accept sensors for measuring the need for food, liquid, physical activity, and sensors for sweat (Fig. 2).
Interviews with caregivers confirmed that sensors for HR, blood sugar and sleep were the top three sensors that they considered useful and acceptable. They expected that wearable HR sensors could provide them with an additional tool to identify pain and distress at an early stage, and thus use this insight to relieve pain and possibly avoid aggressive behaviour and self-injury, and ultimately improve daily life for non-verbal persons with ID. A caregiver [C-7] explained the objectives of using sensors: “We want to detect illness or distress that the user is unable to communicate, which can contribute to improved quality of life.”
Caregivers and parents considered HR to be useful for identifying acute pain, while monitoring sleep was considered useful for understanding and interpreting user needs and behaviour. Caregivers often register time spent in bed, but quality of sleep is usually not routinely measured. Knowledge about the quality of sleep could assist in understanding stress reactions the following day as well as planning and adjusting activities to the user’s capacity and a caregiver [C-3] stated: “Monitoring sleep may be an efficient tool, as sleep and sleep patterns have a great influence on the user’s emotions and their capacity the following day.”
Further, informants expressed interest in exploring the use of wearable HR sensors to possibly detect nightly epileptic seizures. The purpose would be to monitor seizures that are not easily detected visually, by sounds or by traditional alarms. Thus, if possible, caregivers could quickly treat and comfort the user and hopefully prevent serious incidents from epileptic seizures.
3.5Autonomy and privacy
In the online survey, the informants answered questions about ethical issues and acceptance of various sensor modalities (see Fig. 3). Most informants (77%) stated that wearable sensors embedded in a watch or wrist band were ethically acceptable, whereas a chest band was considered slightly less acceptable (73%). Less than half of the informants (41%) considered sensors glued to the skin to be acceptable, and only 22% of the informants considered invasive sensors to be acceptable. Forty-eight percent considered invasive sensors unacceptable. Sensors that can easily be taken on and off, such as wrist bands or chest bands were viewed as more ethically acceptable than sensors more permanently attached to the body.
When caregivers were asked whether they had any concerns about using sensors, user autonomy, infringement of privacy and coercion were frequently mentioned. Ethical discussions and proper assessment and documentation of the users’ needs were considered important to reduce the risk of coercion and infringement of privacy. Caregivers emphasized that the use of sensors must not cause harm and should serve a clear purpose. They brought forward their duty to balance the privacy of the user on the one hand, and the user’s improved well-being on the other.
Caregivers preferred using wearable sensors like a watch, wristband or belt that allows the user to express their disapproval by taking it off or signalling that they wanted it off. Some users may have esthetical preferences concerning the sensor. The caregivers highlighted the importance of respecting the users’ preferences and stated that if ethical dilemmas are not considered and discussed, this may infringe on the autonomy of the users: “I think it will be more accepted by the user if it is aesthetically nice and she gets to choose colours and designs on bracelets. Then I think it will be much more accepted, and she would like it better.” [C-6].
However, caregivers also commented that the way the sensor was introduced to the user could influence his/her attitudes and acceptance towards using sensors. In interviews and in the survey, caregivers emphasized the value of autonomy and privacy of the user and the importance of user participation.
4.Discussion
4.1The difficulty of identifying pain and distress in non-verbal persons with ID
In this study, we found that professional caregivers and parents of non-verbal children with ID recognise pain from observing facial expression, bodily movements, or sound, as reported previously [12, 30, 31]. However, professional caregivers and parents expressed great frustration when being unable to reliably identify pain and distress in non-verbal persons with ID despite their extensive knowledge of them. This uncertainty made identification of pain and distress difficult and frustrating. Decisions about appropriate interventions and treatment are experienced to be complex and ambiguous, as previously described [32]. Professional caregivers’ fear of overlooking pain is substantiated by previous findings that persons with IDs were less likely to be diagnosed with a painful condition and to receive adequate medication [9, 33]. But the intensity of the fear expressed by professional caregivers and parents were more explicit and profound in our study.
Observational pain tools and checklists for assessing pain in non-verbal persons with ID [31, 34] and self-reporting tool for persons with mild to moderate ID do exist [35]. In our study, most users do not have the ability to use self-reporting tools, and many caregivers reported that they do not have adequate tools for assessing and identifying pain and distress in non-verbal person with ID, and they request objective tools and measures that can be utilised in daily life situations. Previous findings have confirmed that to construct a tool that usefully determine the presence of pain in people with severe cognitive impairments is difficult [36]. Our informants described their difficulties when assessing pain, and the challenges caused by the users limited communication skills and self-reporting abilities. Breau and Burkitt [31] further confirmed that the vulnerabilities of this group require special care in assessing and managing their pain, which our findings also confirm.
4.2Positive attitudes towards sensors among parents and professional caregivers
Previous literature portray health professionals’ ambivalence towards their patients’ use of wearables [37], which are not consistent with our findings. However, given the frustration that professional caregivers and parents feel being unable to adequately identify pain and distress in non-verbal persons with ID, it is not surprising that they request new tools and sensors to help them assess and recognise pain and distress. Even so, professional caregivers felt the purpose of such sensors should be limited to aiding the understanding of non-verbal persons in terms of pain and distress; the use of sensors as a general tool for monitoring the user, was felt to infringe upon the privacy and autonomy of the non-verbal person.
These findings agree with those of Wolbring and Leopatra [24] that professional caregivers express positive attitudes towards the use of wearable sensors that may detect signs of pain and distress, but sensors were less acceptable if they infringed markedly on the integrity of the user, or if the sensor had to be inserted under the skin. Professional caregivers and parents take the privacy and autonomy of the user and the degree of physical invasiveness of the sensor into account when evaluating the ethical implications of sensors for non-verbal persons with ID. They need to be sure that the effect of the sensor in terms of better health care or quality of life outweighs any downsides in terms of infringement of privacy and autonomy, or physical invasiveness.
Our findings confirm that caregivers and parents expect that wearable sensors measuring physiological responses will provide valuable information about pain and distress. They also expect that the users will accept wearing sensors measuring HR. Informants with prior knowledge about sensors, were more positive towards the use of sensors. Caregivers express that measuring HR should be implemented in combination with behavioural observations, which is consistent with previous studies on implementation of sensors and multimodal information supporting assessment of pain and distress in non-verbal persons [38, 39].
4.3Strength and limitations of the study
A strength of the present study was the extensive experience of the professional caregivers. Most professional caregivers had an educational background that was relevant to care for non-verbal persons with ID. They had long and daily experience with the user group, and thus had a comprehensive understanding of the everyday challenges of communicating with non-verbal persons with ID.
Another strength was the mixed-method approach, which provide statistical findings, complemented by in depth understanding of caregivers’ and parents’ attitudes and possible barriers and facilitators towards the use of sensors in real life situations. Including data from both questionnaires and interviews, and the informants extensive experience with the user group support the credibility and trustworthiness of study findings.
A limitation might be the bias of informants who had heard about our study, as 97% of those informants were positive toward the use of sensors, compared to 78% of those who had not heard about our study prior to completing the online questionnaire. On the other hand, it may be argued that the informants who had heard about our study had more knowledge of the merits of the use of sensors and thus were better qualified to evaluate the use of sensors.
Another limitation is that online surveys are easily accessible to digitally literate informants with access to digital communication devices. Informants without digital skills or digital access were offered to fill in a paper-based version of the survey. Only one of the informants filled in a paper-based questionnaire.
5.Conclusion
This study documents that professional caregivers and parents find it challenging to reliably identify pain and distress in non-verbal persons with ID. They have experienced that pain and distress go undetected due to the users’ limited communication abilities. Consequently, non-verbal persons with ID may not receive adequate care and treatment, that may reduce their quality of life or cause serious illness.
Most professional caregivers and parents were positive towards the use of sensors that could facilitate communication and identify pain and distress in non-verbal persons with ID. Non-invasive wearable sensors for monitoring heart rate, sleep, blood sugar and epileptic seizures were considered most useful and acceptable. Professional caregivers expressed reservations if sensors infringed upon the autonomy and privacy of non-verbal persons with ID and highlighted the importance of facilitating user involvement.
Consequently, there is a need for sensors that can objectively identify pain and distress in non-verbal persons with ID in daily life situations and contribute to adequate care and treatment A follow up study monitoring heart rate in non-verbal persons with ID will add knowledge on how wearable sensors may complement subjective observations and contribute to identify pain and distress.
Author contributions
CONCEPTION: B.H., T.Ø., E.S.B., F.S., and C.M. designed the study.
PERFORMANCE OF WORK: T.Ø., E.S.B., and F.S. created the online survey; all co-authors critically revised the questions in the survey. I-L.D. provided contact information for the informants of the survey. T.Ø. and E.S.B. drafted the interview guide with important input from I-L.D.; all authors critically revised the interview guide. T.Ø. and E.S.B. performed the interviews.
INTERPRETATION OF DATA: T.Ø., and E.S.B. analysed the data form the survey. T.Ø. and E.S.B. transcribed and analysed the interview data. All authors discussed the results and interpretations.
PREPARATION OF THE MANUSCRIPT: T.Ø. drafted the manuscript. All authors critically revised the manuscript. All authors approved the final version of the manuscript.
SUPERVISION: B.H supervised the study.
Ethical considerations
Caregivers and parents received written information of the study prior to participation, and informed consent was obtained from all informants. Participation in the project was volunteer. The participants had the opportunity to withdraw from the study at any time without having to state any reason.
The study was approved by The Committee for Ethics in Medical Research for the Southern and Eastern parts of Norway, reference number 2016/1956, dated 20.12.2016 and Norwegian Centre for Research Data reference number 57131, dated 06.12.2017 The study conformed with the Declaration of Helsinki.
Acknowledgments
We would like to thank caregivers and parents who have contributed to the study with their knowledge and opinions. We would also like to thank the representatives of the two organisations of persons with disabilities; The Association for Cerebral Palsy, and The Norwegian Association for Persons with Intellectual Disabilities and Relatives (LUPE) and the individual parents of non-verbal children with ID. This research study is funded by The Research Council of Norway, project # 269348.
Conflict of interest
The authors have no conflicts of interest to report.
References
[1] | Maulik PK, Mascarenhas MN, Mathers CD, Dua T, Saxena S. Prevalence of intellectual disability: a meta-analysis of population-based studies. Res Dev Disabil. (2011) ; 32: (2): 419-36. |
[2] | Zablotsky B, Black LI, Maenner MJ, Schieve LA, Danielson ML, Bitsko RH, et al. Prevalence and Trends of Developmental Disabilities among Children in the United States: 2009-2017. Pediatrics. (2019) ; 144(4). |
[3] | WHO. International Classification of Diseases 11th Revision. (2018) . |
[4] | AAIDD. Definition of Intellectual Disability: American Association on Intellectual and Developmental Disabilities. (2020) . Available from: https://www.aaidd.org/intellectual-disability/definition. |
[5] | Boat TF, Wu JT, editors. Mental Disorders and Disabilities Among Low-Income Children. National Academies of Sciences, Engineering, and Medicine. Washington DC, US: National Academies Press; 2015. |
[6] | van Bakel M, Einarsson I, Arnaud C, Craig S, Michelsen SI, Pildava S, et al. Monitoring the prevalence of severe intellectual disability in children across Europe: feasibility of a common database. Dev Med Child Neurol. (2014) ; 56: (4): 361-9. |
[7] | Defrin R, Pick CG, Peretz C, Carmeli E. A quantitative somatosensory testing of pain threshold in individuals with mental retardation. Pain. (2004) ; 108: (1-2): 58-66. |
[8] | McGuire BE, Defrin R. Pain perception in people with Down syndrome: a synthesis of clinical and experimental research. Front Behav Neurosci. (2015) ; 9: : 194. |
[9] | Amor-Salamanca A, Menchon JM. Pain underreporting associated with profound intellectual disability in emergency departments. J Intellect Disabil Res. (2017) ; 61: (4): 341-7. |
[10] | Beacroft M, Dodd K. Pain in people with learning disabilities in residential settings – the need for change. British Journal of Learning Disabilities. (2010) ; 38: (3): 201-9. |
[11] | Boerlage AA, Valkenburg AJ, Scherder EJ, Steenhof G, Effing P, Tibboel D, et al. Prevalence of pain in institutionalized adults with intellectual disabilities: a cross-sectional approach. Res Dev Disabil. (2013) ; 34: (8): 2399-406. |
[12] | de Knegt NC, Pieper MJ, Lobbezoo F, Schuengel C, Evenhuis HM, Passchier J, et al. Behavioral pain indicators in people with intellectual disabilities: a systematic review. J Pain. (2013) ; 14: (9): 885-96. |
[13] | Bohlin G. Delayed habituation of the electrodermal orienting response as a function of increased level of arousal. Psychophysiology. (1976) ; 13: (4): 345-51. |
[14] | Can YS, Chalabianloo N, Ekiz D, Ersoy C. Continuous Stress Detection Using Wearable Sensors in Real Life: Algorithmic Programming Contest Case Study. Sensors (Basel). (2019) ; 19: (8). |
[15] | Gonsalves S, Mercer J. Physiological correlates of painful stimulation in preterm infants. Clin J Pain. (1993) ; 9: (2): 88-93. |
[16] | Hilgard ER, Morgan AH, Lange AF, Lenox JR, MacDonald H, Marshall GD, et al. Heart rate changes in pain and hypnosis. Psychophysiology. (1974) ; 11: (6): 692-702. |
[17] | Kildal E, Stadskleiv K, Boysen ES, Oderud T, Dahl IL, Seeberg TM, et al. Increased heart rate functions as a signal of acute distress in non-communicating persons with intellectual disability. Sci Rep. (2021) ; 11: (1): 6479. |
[18] | Meesters NJ, Simons SHP, van Rosmalen J, Holsti L, Reiss IKM, van Dijk M. Acute Pain Assessment in Prematurely Born Infants Below 29 Weeks: A Long Way to Go. Clin J Pain. (2019) ; 35: (12): 975-82. |
[19] | Rathmell JP, Fields HL. Pain: pathophysiology and management. In: Longo DL, Fauci AS, Kapser DL, Hauser SL, Jameson JL, Loscalzo J, editors. Harrison’s Principles of Internal Medicine, 21e. New York: McGraw-Hill; (2012) . |
[20] | Carreiro S, Chintha KK, Shrestha S, Chapman B, Smelson D, Indic P. Wearable sensor-based detection of stress and craving in patients during treatment for substance use disorder: A mixed methods pilot study. Drug Alcohol Depend. (2020) ; 209: : 107929. |
[21] | Kaczor EE, Carreiro S, Stapp J, Chapman B, Indic P. Objective Measurement of Physician Stress in the Emergency Department Using a Wearable Sensor. Proc Annu Hawaii Int Conf Syst Sci. (2020) ; 2020: : 3729-38. |
[22] | Rodrigues S, Paiva JS, Dias D, Pimentel G, Kaiseler M, Cunha JPS. Wearable Biomonitoring Platform for the Assessment of Stress and its Impact on Cognitive Performance of Firefighters: An Experimental Study. Clin Pract Epidemiol Ment Health. (2018) ; 14: : 250-62. |
[23] | Malterud K. Qualitative research: standards, challenges, and guidelines. Lancet. (2001) ; 358: (9280): 483-8. |
[24] | Wolbring G, Leopatra V. Sensors: views of staff of a disability service organization. J Pers Med. (2013) ; 3: (1): 23-39. |
[25] | SurveyMonkey. Survey. (2018) . |
[26] | IASP. Terminology. Available from: https://www.iasp-pain.org/terminology. |
[27] | Delgado DA, Lambert BS, Boutris N, McCulloch PC, Robbins AB, Moreno MR, et al. Validation of Digital Visual Analog Scale Pain Scoring With a Traditional Paper-based Visual Analog Scale in Adults. J Am Acad Orthop Surg Glob Res Rev. (2018) ; 2: (3): e088. |
[28] | Sigafoos JW, Gail W, Keen D, Tait K, Tucker M, Roberts-Pennell D, Pittendreigh N. Identifying potential communicative acts in children with developmental and physical disabilities. Communication Disorders Quarterly. (2000) ; 21: (2): 10. |
[29] | Dictionary – Attitude. Cambridge University Press; (2020) . Available from: https://dictionary.cambridge.org/dictionary/english/attitude. |
[30] | Kunz M, de Wall MWM, Achterberg WP, Gimenez-Llort L, Lobbezoo F, Sampson EL, van Dalen-Kok AH, Defrin R, Invitto S, Konstantinovic L, Oosterman J, Petrini L, van der Steen JT, Strand LI, de Tommaso M, Zwakhalen S, Husebo BS, Lautenbacher S. The Pain Assessment in Impaired Cognition scale (PAIC15): A multidisciplinary and international approach to develop and test a meta-tool for pain assessment in impaired cognition, especially dementia. European Journal of Pain. (2020) ; 24: (1): 192-208. |
[31] | Breau LM, Burkitt C. Assessing pain in children with intellectual disabilities. Pain Res Manag. (2009) ; 14: (2): 116-20. |
[32] | Findlay L, Williams AC, Baum S, Scior K. Caregiver experiences of supporting adults with intellectual disabilities in pain. J Appl Res Intellect Disabil. (2015) ; 28: (2): 111-20. |
[33] | Axmon A, Ahlstrom G, Westergren H. Pain and Pain Medication among Older People with Intellectual Disabilities in Comparison with the General Population. Healthcare (Basel). (2018) ; 6: (2). |
[34] | Lotan M, Ljunggren EA, Johnsen TB, Defrin R, Pick CG, Strand LI. A modified version of the non-communicating children pain checklist-revised, adapted to adults with intellectual and developmental disabilities: sensitivity to pain and internal consistency. J Pain. (2009) ; 10: (4): 398-407. |
[35] | de Knegt NC, Lobbezoo F, Schuengel C, Evenhuis HM, Scherder EJ. Self-Reporting Tool On Pain in People with Intellectual Disabilities (STOP-ID!): a Usability Study. Augment Altern Commun. (2016) ; 32: (1): 1-11. |
[36] | Foley DC, McCutcheon H. Detecting pain in people with an intellectual disability. Accid Emerg Nurs. (2004) ; 12: (4): 196-200. |
[37] | Watt A, Swainston K, Wilson G. Health professionals’ attitudes to patients’ use of wearable technology. Digit Health. (2019) ; 5: : 2055207619845544. |
[38] | Werner P, Lopez-Martinez D, Walter S, Al-Hamadi A, Gruss S, Picard R. Automatic Recognition Methods Supporting Pain Assessment: A Survey. IEEE Transactions on Affective Computing. (2019) . |
[39] | Picard RW. Future affective technology for autism and emotion communication. Philos Trans R Soc Lond B Biol Sci. (2009) ; 364: (1535): 3575-84. |


