
Telehealth in physiotherapy during the COVID-19 pandemic, the perspective of the service users: A cross-sectional survey
Abstract
OBJECTIVE:
The satisfaction and acceptance of telehealth by the Irish physiotherapy service user is currently unclear. This study aims to evaluate the Irish service users’ experience of physiotherapy delivered totally or partially via telehealth, using a cross-sectional self-reported anonymous postal survey.
METHODS:
Service users (n = 250) of the Cavan Monaghan physiotherapy department, Health Service Executive (HSE), Republic of Ireland were surveyed. Data was collected on demographics, experience with technology, experience and satisfaction with physiotherapy delivered via telehealth. Qualitative thematic analysis of the free-text responses was completed.
RESULTS:
A response rate of 40% was achieved. Participants attended physiotherapy for an average of 2.65 months. Upper limb complaints comprised 29% of participants, 27% had a back complaint, 21% had a lower limb complaint and 14% attended for a women’s health issue. Those who received their physiotherapy consultation over the phone comprised 78%, while 15% received it virtually and 85% were highly or somewhat satisfied with the telehealth physiotherapy they received. However, 49% prefer blended care (combination of telehealth and face-to-face), 41% prefer face-to-face consultations only and 10% are satisfied with telehealth solely.
The recipients of virtual calls were all satisfied. In the future, 60% of these participants would prefer blended care, 20% would prefer face-to-face care only and 20% would be satisfied with telehealth solely.
CONCLUSION:
The physiotherapy telehealth services were well received. There was a greater acceptance of future telehealth usage by video call recipients compared to those who received a phone call only. Engagement with appropriate service users and their needs will be required to ensure the longevity and success of telehealth.
1Introduction
There has been a rapid transition to telehealth applications as a mode of intervention delivery since the onset of the COVID-19 pandemic. At times it was the only mode of intervention available to physiotherapy at the Cavan Monaghan physiotherapy department in agreement with public health advice. Until the onset of the COVID-19 pandemic the widespread uptake of telehealth was slow [1, 2]. Digital health care is supported globally as the way forward with many countries worldwide formally recognising the benefits and value of using digital modes of care delivery [3].
The term digital practice, telehealth, telerehabilitation and telemedicine can be used interchangeably as there is no agreed terminology for digital healthcare [4]. For the purpose of this research the term telehealth will be used. Telehealth is the distribution of health-related services and information via electronic information and telecommunication technologies [5]. It allows long-distance patient and clinician contact, care, advice, reminders, education, intervention, monitoring, and remote admissions [6, 7].
During the COVID-19 pandemic there were periods of nil and limited access to out-patient physiotherapy departments for the public. Physiotherapists introduced telehealth to continue physiotherapy provision. This was a relatively new work method adopted by physiotherapy. Telehealth modes adopted included telephone consultations and real-time virtual consultations. Different applications, programs and platforms were used. Hybrid/blended telehealth were then adopted, in agreement with public health advice, which combines face-to-face consultations and telehealth services to the patient [8]. Will telehealth usage continue when physiotherapists and service users have a choice on the medium of healthcare delivery? Some organisations have a considered approach to telehealth, others have rapidly adopted services without consideration for important factors [9]. However, the momentum is such that telehealth will almost certainly find a stronger place in health service frameworks beyond the pandemic and is likely to have increased acceptance among service users and providers [10, 11]. The experience of the practitioner and the patient will shift views of this service delivery method [9] and may determine its long term acceptability among service users.
A rapid evidence synthesis of paediatric telehealth reported high service user acceptance and satisfaction with telehealth and there was a tendency to favour face-to-face care of those who had not yet tried telehealth [12]. A pre COVID-19 study explored the older person’s acceptance of telehealth; perceived ease of use, usefulness and security were identified as predictors of acceptance in Slovenia [13]. Telerehabiliation demonstrated comparable pain relief and better functional recovery compared to face-to-face intervention following total knee arthroplasty [14]. A recent Australian study [11] of physiotherapy service users reported moderately or extremely positive perceptions of satisfaction of management (92%), satisfaction with privacy/security (98%) and effectiveness (83%) with physiotherapy via virtual consultation during COVID-19. Almost half (47%) of their participants indicated they were moderately or extremely likely to choose virtual consultation in the future. These studies demonstrate an acceptance of telehealth in the paediatric population and their caregivers, the older person, the musculoskeletal patient and in other countries. To date no research has been conducted, since the onset of the COVID-19 pandemic, on the Irish physiotherapy service user. Therefore, this study aims to investigate the telehealth experience of the Irish physiotherapy service user. It aimed to evaluate their satisfaction and acceptance with this service now, during COVID-19 and for the future.
2Methods
2.1Study design
A cross-sectional self-reported anonymous postal survey.
2.2Survey instrument
The survey was designed based on two sources. Firstly, an extensive literature search was conducted to identify previous validated surveys which focus on the perceptions of service users about telehealth. The Telehealth Usability Questionnaire [15], the Telemedicine Satisfaction Questionnaire [16] and the Service User Technology Acceptability Questionnaire [17] are the most frequently utilised questionnaires in the literature [18]. The Technology Acceptance Model [19, 20] was also considered. However COVID-19 presented specific circumstances that was not addressed by these survey tools. The researchers opted to design their own survey and this is recommended to ensure comprehensiveness in terms of the issues studied [18]. Elements of the aforementioned surveys were considered during the survey development.
The second source was the results of unpublished research investigating the physiotherapist’s perspective of telehealth during the COVID-19 pandemic within the same geographical location and published research investigating the physiotherapist’s perspective of telehealth during the COVID-19 pandemic within Republic of Ireland [21]. These two pieces of research contained surveys designed by the same authors, investigating physiotherapists’ experience and satisfaction with telehealth. Some of the questions on these surveys were transferable to the service user population studied here.
The questionnaire for this study contained 17 questions. The first questions ascertained demographics, their presenting clinical complaint and prior experience with technology. The next section included questions on method and purpose of communication with their physiotherapist, their satisfaction with that communication and any difficulties encountered. Satisfaction with the technology was established using a Likert scale (e.g. very satisfied, somewhat satisfied, neither, somewhat dissatisfied and very dissatisfied). The final part asked to comment freely on their overall experience of telehealth and their preference for physiotherapy services in the future. This survey was pilot tested on a small sample (n = 4) of respondents to establish readability and ensure anonymity. Grammatical changes and extra answer choices were included as a result of this pilot.
2.3Sample
The study population eligible to participate were all Cavan and Monaghan HSE physiotherapy service users, over the age of eighteen, who had received at least one physiotherapy intervention via telehealth between March 2020 and January 2021 and had adequate spoken and written English. This is a predominantly rural area with small urban towns. Potential participants were identified from the online booking system, www.swiftqueue.com. A sample of approximately 2205 participants was identified, an independent administrator screened the list removing duplicates and selecting every 15th name of the list, obtaining a systematic sample of 476 service users.
2.4Procedure
Ethical approval was obtained from the Health Service Executive’s North East Area Research Ethics Committee. The independent administrator contacted the services users identified in the sample to screen them against the eligibility criteria and gained their consent to post the survey and its information to them. The survey, information leaflet and prepaid self-addressed envelope were posted to the consenting service users between March and September 2021. The survey took ten minutes to complete. A return date of three weeks was given.
2.5Data analysis
Data was analysed descriptively using Microsoft Excel 2010. Descriptive statistics, including frequencies (percentages) and means were used to summarise the data from those who completed the survey. The data included categorical, continuous and ordinal level of measurement. The two open ended questions to discuss overall experience underwent thematic analysis. This involved two researchers (AR, NS) independently reading all responses and coding the data to identify initial patterns. Codes were organised into categories by the two researchers together and agreed larger themes were formed. Themes with the highest number of individual data points were identified and reported alongside the quantitative data on satisfaction.
3Results
3.1Survey response
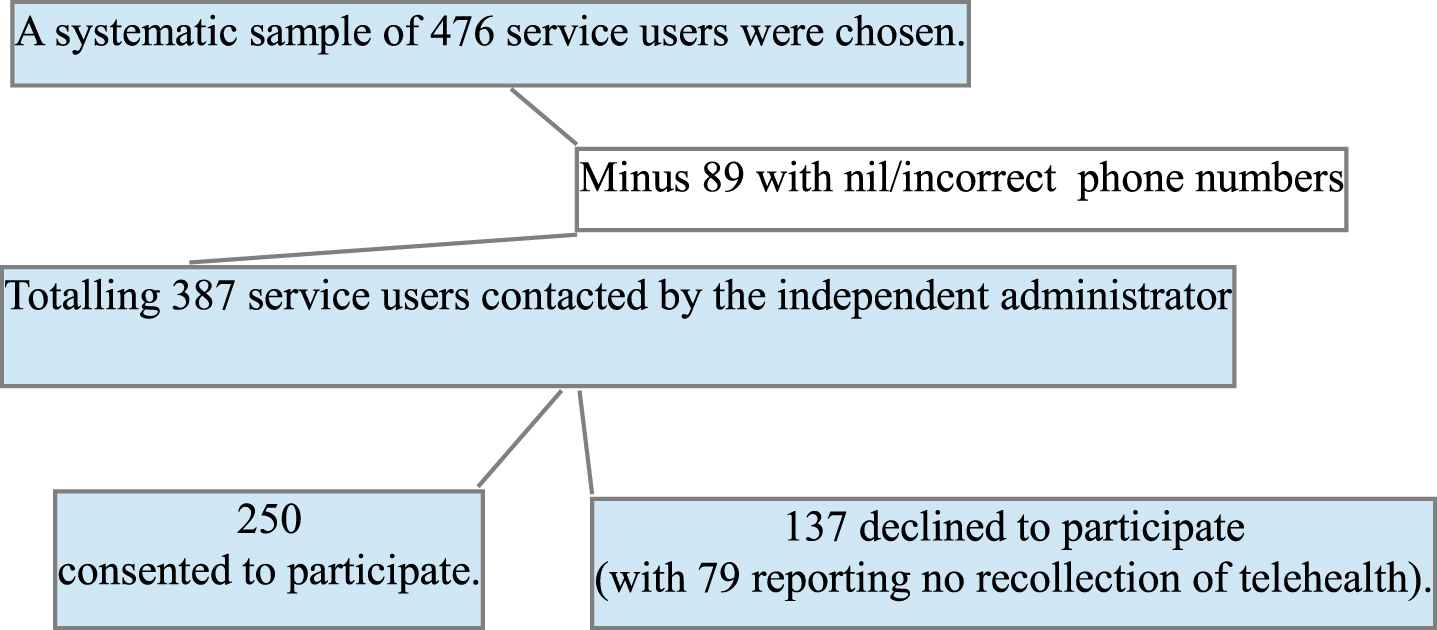
Two hundred and fifty participants consented to participate from a sample of 387. Completed surveys were returned by 100 participants, providing a response rate of forty per cent. Reasons for participant exclusion and non-participation are presented in Fig. 1.
Fig. 1
Reasons for participant exclusion and non-participation.
3.2Service user profile
Seventy-six (76%) of respondents were female and twenty-four (24%) were male. The average minimum age was 47 years and the average maximum age was 57 years. Thirty five per cent rated their I.T. skills as above average, 45% rated them as average and 17% rated their skills as below average. The average number of months the participants attended physiotherapy was answered by 94 respondents and was 2.65 months, with a standard deviation of 1.6. Twenty nine per cent attended physiotherapy for one or more upper limb symptoms. Twenty seven per cent required physiotherapy for their back with thirteen per cent of these receiving treatments for another complaint simultaneously. Twenty one per cent received physiotherapy for one or lower limb symptoms. Fourteen per cent required physiotherapy for a women’s health issue. Details of participant’s profile are available in Table 1.
Table 1
Survey participants’ sociodemographic data (n = 100)
| n | % | |
| Gender | ||
| Male | 24 | 24 |
| Female | 76 | 76 |
| Age | ||
| 18–30years | 10 | 10 |
| 31–40 years | 14 | 14 |
| 41–50 years | 20 | 20 |
| 51–60 years | 24 | 24 |
| 61–70 years | 19 | 19 |
| 71–80 years | 13 | 13 |
| 81 or older | 0 | 0 |
| mean minimum age = 47.4 years | ||
| mean maximum age = 56.7 years | ||
| The number of months attending physiotherapy mean (SD) = 2.65 (1.6)* | ||
| Complaint requiring physiotherapy | ||
| Back symptoms | 14 | 14 |
| Neck symptoms | 2 | 2 |
| Shoulder symptoms | 10 | 10 |
| Elbow, Arm or hand symptoms | 10 | 10 |
| Hip or Knee symptoms | 7 | 7 |
| Ankle or foot symptoms | 11 | 11 |
| Women’s health issue | 13 | 13 |
| Mobility issues, Balance issues, Neurological condition | 3 | 3 |
| Other: | 30 | 30 |
| 2 of the following; neck, shoulder, arm or hand | 8 | 8 |
| Back and 1 or 2 other complaints (hip, neck, shoulder, arm, hand, mobility, balance) | 13 | 13 |
| Arm or hand and 1 other complaint (knee, ankle or foot, mobility) | 4 | 4 |
| Ankle or foot, knee, mobility, balance | 2 | 2 |
| Women’s health and knee | 1 | 1 |
| Secondary lymphoedema, Bell’s palsy | 2 | 2 |
| Self-rated I.T. Literacy** | ||
| Far above average | 9 | 9.27 |
| Above average | 26 | 26.8 |
| Average | 45 | 46.4 |
| Below average | 11 | 11.34 |
| Far below average | 6 | 6.19 |
*n = 6 missing data **n = 3 blank responses.
3.3Physiotherapy intervention
Ninety-nine (99%) respondents received a phone call from their physiotherapist. Seventy-seven (78%) participants received their physiotherapy consultation during this call. Eight (8%) participants received the phone call to organise a video/live streaming call and six (6%) participants received the phone call to prescribe, review or progress their exercise program. Ninety (91%) respondents reported that the information they received over the phone was clear, while seven (7%) said it was somewhat clear. (See Table 2)
Table 2
Mode of Telehealth (n = 100)
| n | % | n | % | ||
| Phone call | 99 | 99 | For physiotherapy consultation | 77 | 78 |
| To organise video/live streaming call | 8 | 8 | |||
| To prescribe, review, progress exercise plan | 6 | 6 | |||
| Blank responses | 8 | 8 | |||
| Video/live streaming call | 15 | 15 | Those who found the set-up easy | 8 | 53 |
| Those who found the set-up somewhat easy | 6 | 40 | |||
| Those who found the set-up somewhat difficult | 1 | 7 | |||
| Difficulty with video/live streaming | Poor internet connectivity | 6 | 40 | ||
| Poor picture/video quality | 2 | 13 | |||
| Poor sound quality | 1 | 1 | |||
| No issues | 6 | 6 |
Fifteen (15%) participants received their physiotherapy consultation via a video/live streaming call. Fourteen respondents reported having the necessary technology to partake in this call i.e. laptops, ipads and smart phones. Eight respondents felt the set-up of this call was very easy, six felt it was somewhat easy and one respondent felt it was somewhat difficult. Six reported problems with internet connectivity, two respondents reported poor picture/video quality between themselves and the physiotherapist, one person reported sound issues. Six respondents reported no issues. (See Table 2). Numbers do not sum to the total for some items due to unanswered questions and multiple answer choices.
3.4Service user satisfaction and overall experience
Participants reported excellent satisfaction rates with the physiotherapy services they received via phone or video call with 82 (85%) participants communicating they were highly satisfied (n = 63) or somewhat satisfied (n = 19). Participants were also asked to comment on their overall experience, please see Table 3 for themes and subthemes identified. Approximately a third commented ‘excellent, good, happy and satisfied’ and an approximate tenth mentioned ‘helpful’ and ‘sufficient’. Other commentary included ‘clear or convenient’, ‘telehealth will aid recovery’, ‘great during COVID’, ‘help reduce waiting times’ and ‘should be adopted more’. Nine (9%) were neither satisfied nor dissatisfied reporting ‘it was okay but difficult to follow over the phone’, ‘not helpful’, ‘confusing’ and ‘would prefer face-to-face or consultation’. Five (5%) were somewhat or highly dissatisfied reporting the service was ‘not entirely satisfactory’, ‘disappointing’, ‘not effective’, ‘the phone call was useless as I could not understand’, ‘I was unsure I was doing the exercises correctly’, ‘prefer personal touch’ and ‘face-to-face consultation would be more beneficial’. An unexpected theme identified in this open commentary was the positive attributes of the treating physiotherapist mentioned by the participants (see Table 3).
Table 3
Themes and subthemes for interpretation of the two open ended questions
| Themes | Subthemes |
| Overall experience of telehealth | |
| (Positive commentary) | Excellent, satisfied, convenient, efficient, informative. |
| (Negative commentary) | Not entirely satisfactory, disappointing, not effective, face-to-face consultation would be more beneficial. |
| (Neutral commentary) | Needed/prefer blended care. |
| Connectivity/Technology | |
| (Positive commentary) | Convenient, useful. |
| (Negative commentary) | Difficulty with phone call, difficulty with video call, video call would not work. |
| Physiotherapist’s attributes | Caring, supportive, pleasant, professional, informative, empathic. |
3.5Future of telehealth
Forty-five (49%) participants would be satisfied with blended care (a combination of telehealth and face-to-face), thirty-seven (41%) people would prefer face-to face consultations only and nine (10%) would be satisfied with their full care via telehealth. Nine people didn’t answer this question. ‘I found the phone/video session very good but really appreciated the hands-on expertise of the physiotherapist. It was reassuring though, to be able to receive both’. ‘The personal contact of the physiotherapist initially is important to establish trust and professionalism. Thereafter telemeeting is okay’.
3.6Recipients of physiotherapy via video call/live streaming
Of those who received physiotherapy via video call, all fifteen participants were highly (n = 13) or somewhat (n = 2) satisfied with the service they received. Twelve (80%) of these recipients commented it was ‘helpful and informative’, ‘super-efficient’ and a ‘really positive session’. Participants were ‘grateful to receive a video call’ and it was ‘reassuring during COVID-19’. Nine (60%) of these respondents would prefer a blended approach to their physiotherapy care in the future with one person commenting ‘it was reassuring to be able to receive both telehealth and face-to-face’. Three (20%) would be happy with their full care via telehealth. Benefits reported included ‘no travel, no waiting room time, video call worked well in conjunction with the phone conversations/calls, accommodating when childcare is an issue, exercises were clearly demonstrated and reassuring to get advice quickly’. Another three (20%) would prefer their care in person in totality, stating it was okay but there was no care after the video call and they would prefer face-to-face.
4Discussion
This study found that participants had an overall positive experience with their physiotherapy delivered via telehealth during the COVID-19 pandemic. Thus, telehealth should be suggested as an alternative method of healthcare delivery during a health emergency. However, despite the high satisfaction rates almost half would prefer a blended care approach in the future.
Our findings are broadly similar to recent Australian [11], Italian [22, 23] and North American [24, 25] studies investigating service users’ experience using video conferencing for physiotherapy and rehabilitation during COVID-19. Four of these five studies were also service evaluations [11, 22, 24, 25], while one study [23] was a research intervention. The studies conducted in Italy and North America reported high levels of satisfaction among service users with intervention delivered via videoconferencing. Australian participants attended physiotherapy for musculoskeletal conditions (63%) and reported positive perceptions about ease of technology use for the video call and high satisfaction with the management of their condition [11], similar to the participants in this study. However a significant proportion would not be willing to use videoconferencing for individual consultations in the future, with 28% of the Australian participants [11] and 41% of the participants in this study preferring not to engage in future telehealth.
Almost half of the participants of this study and the Australian study would be satisfied with blended care in the future. Despite this preference for blended care, a pre-pandemic study reported a high level of agreement between telehealth and in-person assessments with respect to clinical management decisions and diagnosis of patients with chronic musculoskeletal conditions managed in an advanced-practice physiotherapy screening clinic [26]. The same authors suggest that telehealth may be most suitable for observational assessments and not suitable for those requiring physical touch [9]. Blended care may allow the service provider to consider the patient preferences, circumstances and requirements.
There was a greater acceptance of future telehealth usage by video call recipients compared to those who received a phone call only. Recipients of virtual consultation are open to partial or complete telehealth physiotherapy in the future. Recipients of phone consultation are less willing to engage with telehealth in partial or full in the future. This suggests that greater exposure and experience with different modes of telehealth delivery may increase its acceptance. A 2019 study [27] suggests that virtual consultation was considered superior to telephone consultation in providing visual cues and reassurance, building rapport and improving communication. Consideration should be given when planning telehealth to the modes offered to the service user.
Telehealth has been propelled forward during COVID-19. The authors propose that as the technology evolves, and the professional and the service user become accustomed to and comfortable with telehealth, acceptance of telehealth should improve. Attention to perceived barriers, facilitators and potential safety issues may enhance the experience of the service user with telehealth [11]. Therefore regular evaluation of telehealth should be considered.
4.1Strengths
This study investigated both telephone and video consultations while a significant proportion of the most recent literature only exams videoconferencing. Participants were clearly informed that their results were anonymous to facilitate accurate and truthful responses.
4.2Limitations
The response rate was low which may introduce a non-response bias. We were unable to send reminders secondary to the ethical anonymity required. We did not ask our respondents to specify if they had attended a face-to-face consultation at any point for their complaint. This would be useful to determine if they were commenting on telehealth experience alone versus comparing telehealth to face-to-face experience. This study only investigated adult service users who availed of physiotherapy in the Irish public health care system and therefore our findings cannot be generalised to other physiotherapy settings not included here, other healthcare services or other countries. A proportion of people choose not to participate and the reason for this is unknown.
5Conclusion
This study found that implementation of a telehealth physiotherapy service in this rural HSE area, during COVID-19 was widely accepted. However, a blended care approach is preferential for the future. It is proposed that further exposure to telehealth may increase its acceptance as a mode of care delivery. Cyclical evaluation of telehealth is required to guide service providers to successfully select appropriate service users for telehealth while ensuring equitable access to services.
Acknowledgments
The authors thank the Cavan and Monaghan physiotherapy service users who completed the survey, the physiotherapists who read draft copies of the survey. Ms. Louise Smith for acting as the independent administrator. Dr. Helen French and Dr. Sarah Casserley-Feeney, Royal College of Surgeons in Ireland, for their expertise and assistance during this study.
Conflict of interest
None.
Funding
This research did not receive specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
[1] | Tanriverdi H , Iacono CS , Diffusion of telemedicine: a knowledge barrier perspective, Telemed J (1999) ;5: (3):223–44. doi: 10.1089/107830299311989. |
[2] | Wade VA , Taylor AD , Kidd MR , Carati C , Transitioning a home telehealth project into a sustainable, large-scale service: a qualitative study, BMC Health Serv Res (2016) ;16: :183. doi: 10.1186/s12913-016-1436-0. |
[3] | World Confederation of Physical Therapy/INPTRA Digital Practice Final Report 2020. Available from: https://world.physio/sites/default/files/2020-06/WCPT-INPTRA-Digital-Physical-Therapy-Practice-Task-force-March2020 |
[4] | Bashshur R , Shannon G , Krupinski E , Grigsby J , The taxonomy of telemedicine, Telemed J E Health (2011) ;17: (6):484–94. doi: 10.1089/tmj.2011.0103. |
[5] | The Health Resources and Services Administration. 17/10/21. What is telehealth. [Last reviewed September 2021]. Available from: https://www.hrsa.gov/rural-health/telehealth/what-is-telehealth. |
[6] | Masson M , Benefits of TED Talks, Can. Family Phys (2014) ;60: (12), 1080. |
[7] | Shaw DK , Overview of telehealth and its application to cardiopulmonary physical therapy, Cardiopulmonary Phys, Therapy J (2009) ;20: (2):13–18. |
[8] | HealthIT.gov. [Last reviewed on April 15, 2019]. What types of telehealth services can I offer? Available from: https://www.healthit.gov/faq/what-types-telehealth-services-can-i-offer. |
[9] | Cottrell MA , Russell T , Telerehabilitation for musculoskeletal physiotherapy, Musculoskeletal Sci. Practice (2020) ;48: :102193. doi: 10.1016/j.msks2020.102193. |
[10] | Fisk M , Livingstone A , Pit SW , Telehealth in the Context of COVID- Changing Perspectives in Australia, the United Kingdom, and the United States, J Med Internet Res (1926) ;22: (6):e4. doi: 10.2196/19264. |
[11] | Bennell KL , Lawford BJ , Metcalf B , Mackenzie D , Russell T , van den Berg M , et al., Physiotherapists and patients report positive experiences overall with telehealth during the COVID-19 pandemic: a mixed-methods study, J Physiother (2021) ;67: (3):201–9. doi: 10.1016/j.jphys.2021.06.009. |
[12] | Tully L , Case L , Arthurs N , Sorensen J , Marcin JP , O’Malley G , Barriers and Facilitators for Implementing Paediatric Telemedicine: Rapid Review of User Perspectives, Front Pediatr (2021) ;9: :630365. doi: 10.3389/fped.2021.630365. |
[13] | Cimperman M , Makovec Brenčič M , Trkman P , Analyzing older users’ home telehealth services acceptance behaviour-applying an Extended UTAUT model, Int J Med Inform (2016) ;90: :22–31. doi: 10.1016/j.ijmedinf.2016.03.002. |
[14] | Jiang S , Xiang J , Gao X , Guo K , Liu B , The comparison of telerehabilitation and face-to-face rehabilitation after total knee arthroplasty: A systematic review and meta-analysis, J Telemed Telecare (2018) ;24: (4):257–62. doi: 10.1177/1357633X16686748. |
[15] | Parmanto B , Lewis AN Jr , Graham KM , Bertolet MH , Development of the Telehealth Usability Questionnaire (TUQ), Int J Telerehabil (2016) ;8: (1):3–10. doi: 10.5195/ijt.2016.6196. |
[16] | Yip MP , Chang AM , Chan J , MacKenzie AE , Development of the Telemedicine Satisfaction Questionnaire to evaluate patient satisfaction with telemedicine: a preliminary study, J Telemed Telecare (2003) ;9: (1):46–50. doi: 10.1258/135763303321159693. |
[17] | Hirani SP , Rixon L , Beynon M , Cartwright M , Cleanthous S , Selva A , Sanders C , Newman SP ; WSD investigators, Quantifying beliefs regarding telehealth: Development of the Whole Systems Demonstrator Service User Technology Acceptability Questionnaire, J Telemed Telecare (2017) ;23: (4):460–9. doi: 10.1177/1357633X16649531. |
[18] | Hajesmaeel-Gohari S , Bahaadinbeigy K , The most used questionnaires for evaluating telemedicine services, BMC Med Inform Decis Mak (2021) ;21: (1):36. doi: 10.1186/s12911-021-01407-y. |
[19] | Davis FD , Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology, MIS Quarterly (1989) ;13: :319–40. doi: 10.2307/249008. |
[20] | Wikipedia 2021. 30/09/2021. Technology acceptance model. Available from: https://en.wikipedia.org/wiki/Technologyacceptancemodel. |
[21] | Reynolds A , Awan N , Gallagher P , Physiotherapists’ perspective of telehealth during the COVID-19 pandemic, Int J Med Inform (1046) ;156: :13. doi: 10.1016/j.ijmedinf.2021.104613. |
[22] | Assenza C , Catania H , Antenore C , Gobbetti T , Gentili P , Paolucci S , Morelli D , Continuity of Care During COVID-19 Lockdown: A Survey on Stakeholders’ Experience With Telerehabilitation, Front Neurol (2021) ;11: :6172–76. doi: 10.3389/fneur.2020.617276. |
[23] | Negrini S , Donzelli S , Negrini A , Negrini A , Romano M , Zaina F , Feasibility and Acceptability of Telemedicine to Substitute Outpatient Rehabilitation Services in the COVID-19 Emergency in Italy: An Observational Everyday Clinical-Life Study, Arch Phys Med Rehabil (2020) ;101: (11):2027–32. doi: 10.1016/j.apmr.2020.08.001. |
[24] | Tenforde AS , Borgstrom H , Polich G , Steere H , Davis IS , Cotton K , et al., Outpatient Physical, Occupational, and SpeechTherapy Synchronous Telemedicine: A Survey Studyof Patient Satisfaction with Virtual Visits During the COVID-19Pandemic, Am J Phys Med Rehabil (2020) ;99: (11):977–81. doi: 10.1097/PHM.0000000000001571. |
[25] | Miller MJ , Pak SS , Keller DR , Barnes DE , Evaluation of Pragmatic Telehealth Physical Therapy Implementation During the COVID-19 Pandemic, Phys Ther (2021) ;101: (1):pzaa193. doi: 10.1093/ptj/pzaa193. |
[26] | Cottrell MA , O’Leary SP , Swete-Kelly P , Elwell B , Hess S , Litchfield MA , McLoughlin I , Tweedy R , Raymer M , Hill AJ , Russell TG , Agreement between telehealth and in-person assessment of patients with chronic musculoskeletal conditions presenting to an advanced-practice physiotherapy screening clinic, Musculoskelet Sci Pract (2018) ;38: :99–105. doi: 10.1016/j.msks2018.09.014. |
[27] | Donaghy E , Atherton H , Hammersley V , McNeilly H , Bikker A , Robbins L , et al., Acceptability, benefits, and challenges of video consulting: a qualitative study in primary care, British Journal of General Practice (2019) ;69: (686):e586–e594. doi: 10.3399/bjgp19X704141. |


