
Joint moment loading interplay between the shoulders and the low back during patient handling in nurses
Abstract
BACKGROUND:
Manual patient handling completed by nurses can include unexpected or strenuous exertions, potentially leading to injury. Lifting guidelines focus on mitigating primarily limiting low back exposures, and the influence of these techniques on the shoulder is unknown.
OBJECTIVE:
To quantify shoulder loading during manual patient handling tasks and determine whether approaches intended to limit low back exposures negatively affect shoulder demands.
METHODS:
Twenty novice university-aged females completed five manual patient handling tasks before and after a training session. Participants simulated handling a partial weight bearing patient, and joint load magnitudes were calculated. Strength demands were interpreted in the context of available population capability ranges.
RESULTS:
Using recommended techniques decreased peak low back loading in most scenarios (
CONCLUSIONS:
Recommended manual patient handling techniques mitigate low back exposures but likely transfer demands to other body regions, specifically the shoulder.
1.Introduction
Manual materials handling is often associated with manufacturing and warehousing, but non-traditional load handling scenarios exist in other workplaces, and are accompanied by the same musculoskeletal overexertion potential. Indeed, the manual patient handling completed by nurses requires transferring or repositioning substantially more complicated, unmodifiable, and often heavier objects.
Differences in anthropometrics, ability to assist, or combative and uncooperative patients can result in unexpected or strenuous exertions, leading to injury risk [1, 2, 3]. Health care and social services are second only to manufacturing sectors in Ontario for lost time injury claims [4], and musculoskeletal disorders are the cause for
Injury rates led to extensive research and creation of standardized lifting practices, but adoption of these practices can be slow, and practices focus almost exclusively on the low back. Specific tasks, including turning, repositioning or transferring a patient are recognized as high-demand activities, producing greater than recommended spinal compression forces [6, 7, 8, 9]. The dangers associated with manual patient handling have led many health units to adopt safe lifting policies, and in some cases banning certain patient handling tasks [3]. Mechanical lifting devices and lifting techniques have effectively reduced low back injuries and lost days from work [2, 9, 10]. Despite these advances, manual patient handling continues to be completed by nurses who cite a lack of time, unfamiliarity with the manual devices and a lack of available equipment as reasons for favouring manual transfers [11, 12, 13]. Widespread adoption of these techniques can be slow; previous research has indicated that up to 46% of registered nurses either were not informed or aware of national safe patient handling and mobility standards [14]. While nurses receive training throughout their undergraduate careers as well as on the job training, they often mimic the lifting techniques performed by more experienced persons [15, 16]; which may result from the new nurse wanting to assimilate and avoid confrontation. Thus, new nurses may continue to use suboptimal techniques and promote these strategies amongst subsequent nursing generations [17, 18].
While developed strategies have reduced low back injury in nurses, the influence of these techniques on the shoulder is unknown. As these ergonomic interventions have focused chiefly on the low back, concerns exist regarding potential physical demand transfers between joint in manual patient handling [19, 20, 21]. Some tasks, such as shifting the patient up or down the bed or turning the patient to one side, are highly demanding of the shoulder [20]. Other intended ergonomics interventions reduced perceived exertion at the low back while increasing it at the shoulder [2, 10]. Shoulder injuries in manual patient handling remain common among nurses. The focus of this work is to quantify shoulder loading during manual patient handling tasks and determine whether approaches intended to reduce low back exposures concomitantly increase shoulder demands. We hypothesized that trained manual patient handling techniques would decrease low back loading, but would increase peak joint moments observed at the shoulders.
2.Methods
2.1Participants
Twenty healthy university-aged females (21.6
2.2Instrumentation
Motion capture data was collected for all experimental trials. Three-dimensional motion was tracked using an 8-camera Vicon MX20 system (VICON, Oxford, UK). Individual markers were placed over anatomical landmarks: bilaterally over the 2
To quantify resultant joint moments at the shoulders and low back, forces generated at the hand were estimated following each set of manual patient handling trials. Two ErgoFet 300
2.3Experimental design
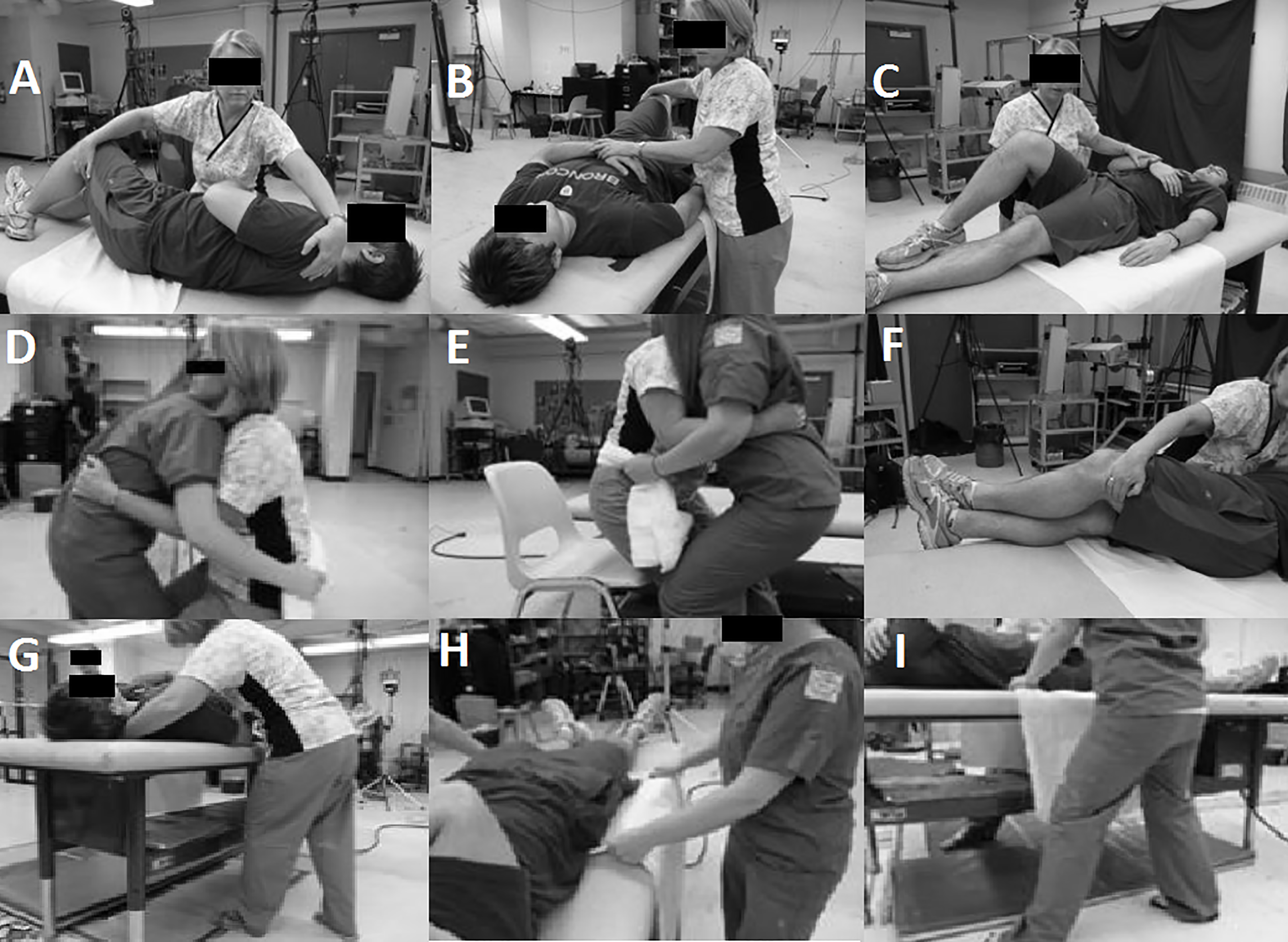
Participants performed defined manual patient handling tasks in two sessions on the same day, before and after a training session. The training session included a self-paced computer presentation of recommended techniques (described graphically and verbally) and videos of recommended lifting strategies for each task. Each video included a practicing nurse with 15 years of experience demonstrating the recommended techniques. The training session finished with physical familiarization and practice with the techniques, including manipulating the patient and feedback from the instructor. Task-specific recommended techniques were extracted from the literature [9, 24] (Fig. 1).
Figure 1.
Example manual patient handling pictures that would accompany detailed descriptions on how to properly perform the recommended techniques. A: Turn Toward initiation; B: Turn Toward; C: Turn Away; D: Sit-to-Chair lift; E: Sit-to-Chair lower; F: Lie-to-Sit hand position; G: Lie-to-Sit foot position; H: Reposition hand position; I: Reposition foot position.
2.4Protocol
The protocol involved application of reflective markers and hand force calibration, a pre-training session, training of recommended techniques, then a post-training session. Within each session, five tasks were block-randomized and performed three times each for a total of 30 trials (15 pre- and post-training), with rest breaks of up to 5 minutes between tasks. The five tasks analysed were: turning the patient toward and away from the nurse (Turn Toward and Turn Away, respectively), moving the patient upward on the bed (Reposition), moving the patient from supine to sitting on the edge of the bed (Lie-to-Sit), and transferring the patient from sitting on the bed to sitting on an adjacent chair (Sit-to-Chair).
Task conditions were consistent across participants. Each trial was completed on an electrically adjustable cushioned table (56–88 cm above the floor) covered in a slider sheet similar to those found in hospitals. Table height was placed at any height the participant chose during untrained trials, while participants used their waist height in post-training trials, except for the Sit-to-Chair task when the height of the table was moved to match the height of the seat pan of the chair. A 92-kg male was used as the “patient” throughout data collection, and was 87
Each trial commenced when the participant moved toward the patient after a starting signal. Participants had 15 seconds to complete the Turn Away, Turn Toward, and Reposition tasks and 25 seconds for the Lie-to-Sit and Sit-to-Chair trials. Trials lengths were established through pilot testing to provide sufficient time to perform each transfer at a typical self-selected pace. Once three repetitions of each task were completed, hand force estimations immediately followed. Participants verbally reported how hard they were working as a percentage of their maximum, in addition to verbally reporting how their exertion was distributed between their hands (e.g. 70% left vs 30% right). They then used the hand force dynamometers against a secured bar to replicate estimated hand forces, with hand force direction relative to the hand, task performance height and orientation relative to the participant takin into consideration.
2.5Data analysis
Kinetic analysis consisted of data filtering, marker reconstruction, local joint coordinate system construction, and external joint moment calculations. Static calibration trials were completed prior to experimental trials, allowing reconstruction in subsequent frames. All raw kinematic data were low-pass filtered with a frequency of 6 Hz [26], and segment lengths and orthogonal coordinate systems were completed using ISB standards [27]. Locations of joint centres, along with participant weight, stature and estimated hand forces were used as inputs in a top-down inverse quasi-static model (similar to that of Dickerson et al. [28]) to determine time series moment data of the left and right shoulder as well as the low back. The recorded force from the hand force estimations was used throughout the trials. In order to prevent non-task movements from being considered, each trial was visually examined, and analysis was only completed on relevant frames. Peak resultant (vector norm) moments from each shoulder and the low back were then extracted for analysis.
Michigan’s 3D static strength prediction program (3DSSPP, University of Michigan, Ann Arbor, MI, USA) was used to compare median (50
2.6Statistical analysis
All statistical analyses were performed using JMP 8.0 software (SAS Institute, North Carolina, USA). Statistical significance was set at
3.Results
Training had differential responses on shoulder and low back loading and strength requirements, and typically resulted in decreased low back loading and variable responses at the shoulder. Required strength fractions generally decreased at the low back, but was variable at the shoulder (Table 1). The results are divided by task in the following sections.
Table 1
Comparisons of mean population strength required for self-selected MPH techniques versus recommended MPH techniques. Percentages in Untrained and Trained rows represent percentage of mean population strength
| TASK | Condition | Right shoulder | Left shoulder | Low back |
|---|---|---|---|---|
| Lie-to-Sit | Untrained (Pull) | 215% | 171% | 199% |
| Untrained (Push) | 68% | 160% | 118% | |
| Trained | 136% | 99% | 132% | |
| % Change (Pull) | ||||
| % Change (Push) | ||||
| Reposition | Untrained (High Bed) | 151% | 157% | 175% |
| Untrained (Low Bed) | 140% | 179% | 149% | |
| Trained | 169% | 157% | 182% | |
| % Change (High Bed) | 0% | |||
| % Change (Low Bed) | ||||
| Sit-to-Chair | Untrained (Pull) | 58% | 45% | 53% |
| Untrained (Push) | 70% | 89% | 50% | |
| Trained | 109% | 88% | 56% | |
| % Change (Pull) | ||||
| % Change (Push) | ||||
| Turn Away | Untrained | 119% | 140% | 68% |
| Trained | 101% | 88% | 32% | |
| % Change | ||||
| Turn toward | Untrained | 70% | 85% | 73% |
| Trained | 94% | 102% | 35% | |
| % Change |
3.1Lie-to-Sit
Training decreased peak moments in the low back and right shoulder, but not the left shoulder. The peak resultant low back moment decreased by 42% (
Table 2
Peak joint moments (in Nm) during self-selected and trained MPH techniques. Significant differences between untrained and trained conditions within regions are bold
| TASK | Condition | Right shoulder | Left shoulder | Low back |
|---|---|---|---|---|
| Lie-to-Sit | Untrained | 47.2 | 61.3 | 231.8 |
| Trained | 46.9 | 45.3 | 133.5 | |
| Reposition | Untrained | 50.6 | 62.8 | 195.1 |
| Trained | 58.3 | 50.6 | 109.5 | |
| Sit-to-Chair | Untrained | 27.3 | 29.3 | 197.0 |
| Trained | 56.7 | 57.7 | 153.5 | |
| Turn away | Untrained | 41.7 | 41.2 | 206.8 |
| Trained | 35.7 | 36.6 | 114.7 | |
| Toward | Untrained | 49.6 | 65.1 | 145.7 |
| Trained | 46.1 | 53.0 | 112.0 |
3.2Reposition
Training decreased low back, but not shoulder peak moments. Low back peak moments decreased by 43% (
Figure 2.
Joint specific peak resultant moments for the Sit-to-Chair task when considering training state as an independent factor. Significant differences between pre- and post-training are marked by an asterisk.
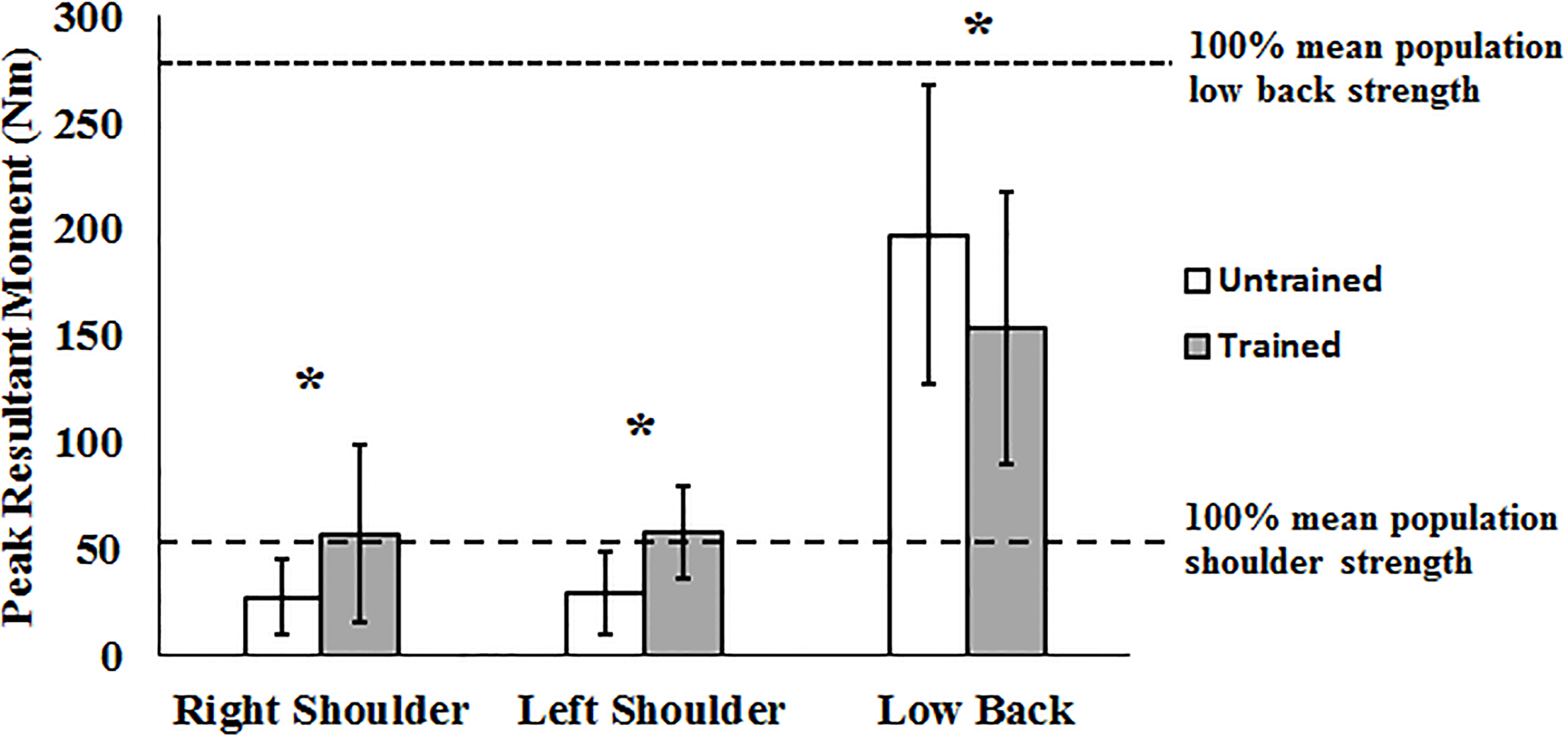
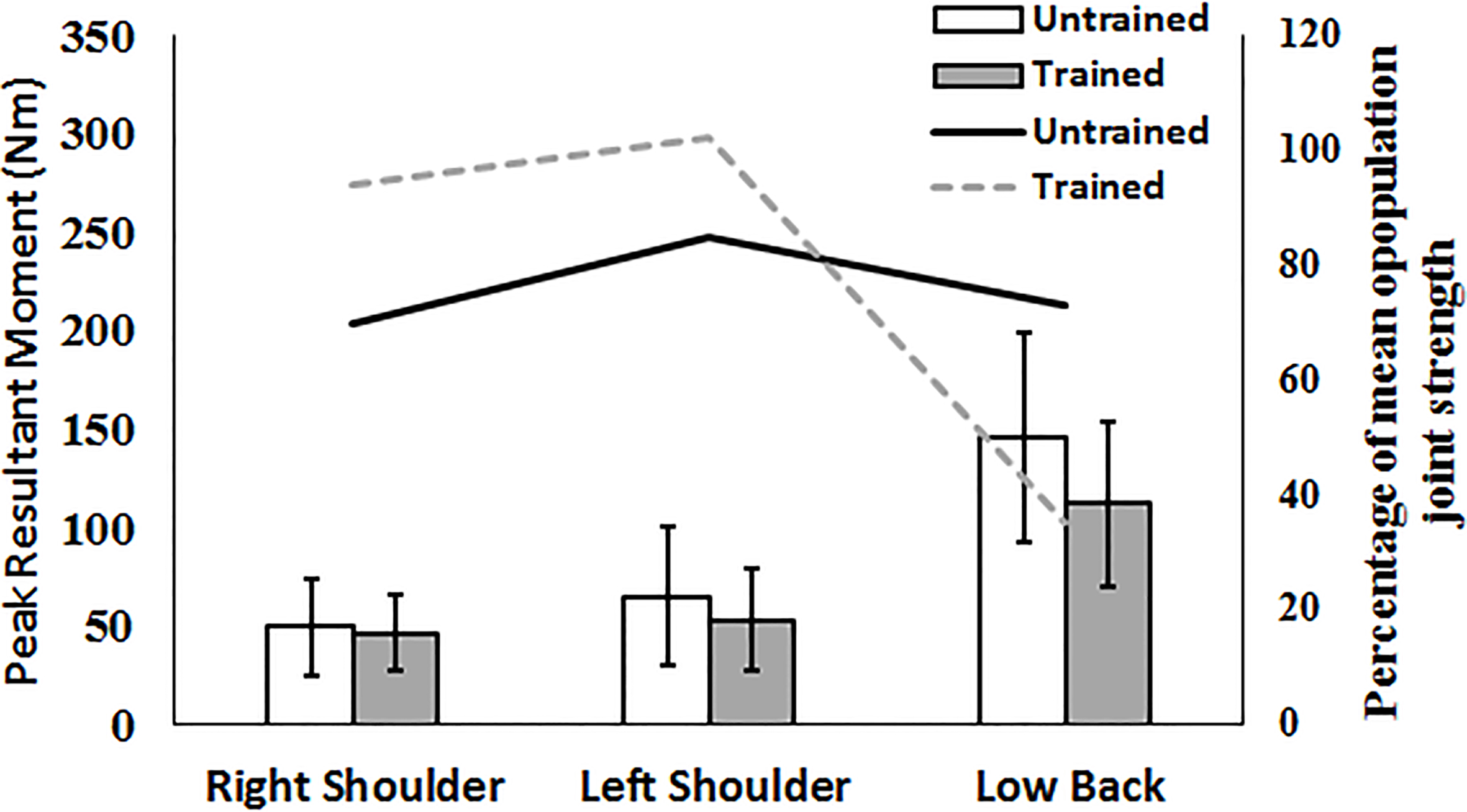
Figure 3.
Joint specific peak resultant moments and percentage of mean population strength for the Turn Toward task. Significant differences between joint specific peak resultant moments between pre- and post-training are marked by an asterisk. Columns are for peak resultant moments (PM in legend), lines are for percentage of mean population joint strength (JS in legend).
3.3Sit-to-Chair
Training generated increases in peak moments in both shoulders, but decreases at the low back. Peak moments in the left shoulder and right shoulder increased during trained exertions by 97% and 107% respectively (
3.4Turn away
Low back peak moments decreased following training, but no changes existed in the shoulders. The low back moment decreased by 92 Nm (
3.5Turn toward
Decreases existed in the left shoulder and the low back, but not the right shoulder. The left shoulder moment decreased by 12.1 Nm or 18% (
4.Discussion
The focus of this research was to examine if techniques designed to decrease low back demands transferred these exposures to the shoulders, or if overall loading decreased holistically. Peak resultant magnitudes were reduced for the low back for every task, and reductions occurred for the shoulders in some tasks, but demands increased after training for others, indicating a spectrum of exposures. Peak moments at the low back decreased by 22–44%, depending on the task. This confirms previous reports of decreased low back exposures with recommended manual patient handling techniques [9, 24, 30]. Peak resultant moments at the right shoulder increased using the recommended techniques for two of the five tasks, with no change in a third task and increases in two tasks; left shoulder peak moments decreased in four of five scenarios. The identified moment increases suggest possible exposure transfers from the low back to the shoulder.
These changes were then converted into a common scale by replicating the postures assumed by the participants during peak force exertion were within a static strength analysis program (3DSSPP) and interpreted. This provided an estimate of how capable the study population is of performing the techniques compared to population normative strength data [29]. For several tasks, the required strength at the shoulders and low back exceeded the mean population strength while using the recommended techniques, increasing overexertion risk [31, 32]. In many cases, using the recommended techniques increased the percentage of mean population strength required to complete the tasks at the shoulders. The recommended techniques required at least 88% of the mean population strength at both shoulders for all tasks, and every scenario except Turn Away resulted in increased strength requirements compared to novice techniques in at least one shoulder.
Joint demand loading changes are readily identified in the Turn Toward and Sit-to-Chair tasks. In the Turn Toward task, the untrained technique balanced exposures nearly equally amongst all three joints, with each joint requiring approximately 75% of the mean population joint strength. Once the recommended technique was adopted, the low back mean population strength fraction decreased to 35%, while the left and right shoulders increased to nearly 100% mean joint strength fraction. This confirms previous recognition of the Turn Toward task as a stressful nursing task [33]. The largest increase occurred in the Sit-to-Chair task, with peak resultant moments at the right and left shoulders increasing by 107% and 97%, respectively, while the low back moment decreased by 22%. This task is frequently targeted for replacement with mechanical lift assists [34]. The strength requirement changes establish both the overall high demand of these MPH tasks while highlighting the potential for transfer of demand between joints for certain tasks.
Field examination of manual patient handling is challenging due to complex interaction between nurse and patient in various situations, and this generated limitations in our work. At present, there is no benchmark for recording separate hand forces in manual patient handling scenarios [35, 36]. The current research did not want to interfere with participant techniques or generate compensations through encumbrance of heavy or awkward equipment, and hand demands (such as holding dynamometers during transfers) are known to affect strategies [37, 38]. Absolute direction of the force applied was estimated, and the use of this method limits analysis to calculation of peak moments, potentially over- or underestimating peak joint moments. However, this study was primarily interested in changes related to training and task type and relative rather than absolute magnitudes. The estimated magnitudes were of similar shoulder moment magnitudes for previous reposition tasks, confirming the reasonableness of the approach [19]. Finally, the set of manual patient handling tasks was not exhaustive, and each participant was limited to approaching the left side of the bed. Approaching from the opposite side of the bed may have generated bilaterally opposite exposures, but anecdotal evidence from practicing nurses suggests that handedness is not typically considered in manual patient handling.
5.Conclusion
This study supports a recommended of continued implementation of several of the manual patient handling techniques; however, certain cautions should be considered for some transfers. The recommended techniques were aimed specifically at lowering low back injury exposures, but may transferring demands to the shoulders. The Turn Toward and Sit-to-Chair tasks appear to adversely affect the shoulder the most, suggesting they should be avoided if possible. Future investigations may benefit from developing novel holistic patient handling techniques that do not transfer demands to other areas of the body.
Conflict of interest
The authors have no conflict of interest to report.
References
[1] | Garg A, Owen B, Beller D, Banaag J. A biomechanical and ergonomic evaluation of patient transferring tasks: bed to wheelchair and wheelchair to bed. Ergonomics. (1991) ; 34: (3): 289-312. |
[2] | Owen B, Keene K, Olson S. An ergonomic approach to reducing back/shoulder stress in hospital nursing personnel: a five year follow up. Int J Nurs Stud. (2002) ; 39: (3): 295-302. |
[3] | Nelson A, Baptiste A. Evidence-based practices for safe patient handling and movement. Orthop Nurs. (2006) ; 25: (6): 366-79. |
[4] | WSIB. 2015 Statistical Report, (2015) . |
[5] | Bureau of Labor Services. Workplace injuries and illnesses in 2007, (2008) . |
[6] | Garg A, Owen B. Prevention of back injuries in healthcare workers. Int J Ind Ergon. (1994) ; 14: (4): 315-31. |
[7] | Daynard D, Yassi A, Cooper J, Tate R, Norman R, Wells R. Biomechanical analysis of peak and cumulative spinal loads during simulated patient-handling activities: a substudy of a randomized controlled trial to prevent lift and transfer injury of health care workers. Appl Ergon. (2001) ; 32: (3): 199-214. |
[8] | Keir P, MacDonell C. Muscle activity during patient transfers: a preliminary study on the influence of lift assists and experience. Ergonomics. (2004) ; 47: (3): 296-306. |
[9] | Schibye B, Hansen A, Hye-Knudsen C, Essendrop M, Böcher M, Skotte J. Biomechanical analysis of the effect of changing patient-handling technique. Appl Ergon. (2003) ; 34: (2): 115-23. |
[10] | Fujishiro K, Weaver J, Heaney C, Hamerick C, Marras W. The effect of ergonomic interventions in healthcare facilities on musculoskeletal disorders. Am J Ind Med. (2005) ; 48: : 338-47. |
[11] | Garg A, Owen B, Carlson B. An ergonomic evaluation of nursing assistants’ job in a nursing home. Ergonomics. (1992) ; 35: (9): 979-95. |
[12] | Engst C, Chhokar R, Miller A, Tate R, Yassi A. Effectiveness of overhead lifting devices in reducing the risk of injury to care staff in extended care facilities. Ergonomics. (2005) ; 48: (2): 187-99. |
[13] | Evanoff B, Wolf L, Aton E, Canos J, Collins J. Reduction in injury rates in nursing personnel through introduction of mechanical lifts in the workplace. Am J Ind Med. (2003) ; 44: (5): 451-7. |
[14] | Vendittelli D, Penprase B, Pittiglio L. Musculoskeletal Injury Prevention for New Nurses. Workplace Health Saf [Internet]. (2016) ; 64: (12): 573-85. |
[15] | Kneafsey R, Haigh C. Learning safe patient handling skills: Student nurse experiences of university and practice based education. Nurse Educ Today. (2007) ; 27: : 832-9. |
[16] | Kneafsey R. Developing skills in safe patient handling: Mentors’ views about their role in supporting student nurses. Nurse Educ Pract. (2010) ; 7: : 365-72. |
[17] | Cornish J, Jones A. Factors affecting compliance with moving and handling policy: Student nurses‘ views and experiences. Nurse Educ Pract. (2007) ; 10: : 96-100. |
[18] | Cornish J, Jones A. Evaluation of moving and handling training for pre-registration nurses and its application to practice. Nurse Educ Pract. (2010) ; 7: : 128-34. |
[19] | Yassi A. Development of a method for quantifying biomechanical risk factors associated with manual and mechanically assisted patient handling. Richmond, BC, Canada: Worksafe BC, (2005) . |
[20] | Gagnon M, Smyth G. Muscular mechanical energy expenditure as a process for detecting potential risks in manual materials handling. J Biomech. (1991) ; 24: (3-4): 191-203. |
[21] | Menzel N, Brooks S, Bernard T, Nelson A. The physical workload of nursing personnel: association with musculoskeletal discomfort. Int J Nurs Stud. (2004) ; 41: (8): 859-67. |
[22] | Kingma I, Looze de M. Validation of a full body 3-D dynamic linked segment model. Hum Mov Sci [Internet]. (1996) ; [cited 2014 Sep 24]; 833-60. |
[23] | Marshall M, Armstrong T, Ebersole M. Verbal estimation of peak exertion intensity. Hum Factors. (2004) ; 46: (7): 697-710. |
[24] | Skotte J, Essendrop M, Hansen A, Schibye B. A dynamic 3D biomechanical evaluation of the load on the low back during different patient-handling tasks. J Biomech. (2002) ; 35: (10): 1357-66. |
[25] | Gordon C, Churchill T, Clauser C, Bradtmiller B, McConville J, Tebbets I, et al. 1988 Anthropometric Survey of U.S. Army Personnel: Methods and Summary Statistics. Tech Rep NATICK/TR-89/044 Natick, MA; US Army Natick Res Dev Eng Cent (AD A225 094). (1989) . |
[26] | Winter D. Biomechanics and Motor Control of Human Movement, 4th Edition, (2009) . |
[27] | Wu G, van Der Halm F, Veeger H, Maksous M, Van Roy P, Anglin C, et al. ISB recommendation on definitions for the reporting of human joint motion – Part II: shoulder, elbow, wrist and hand. J Biomech. (2005) ; 38: : 981-92. |
[28] | Dickerson C, Martin B, Chaffin D. The relationship between shoulder torques and the perception of muscular effort in loaded reaches. Ergonomics. (2006) ; 49: (11): 1036-51. |
[29] | Chaffin D. Development of computerized human static strength simulation model for job design. Hum Factors Ergon Manuf. (1997) ; 7: (4): 305-22. |
[30] | Skotte J, Fallentin N. Low back injury risk during repositioning of patients in bed: the influence of handling technique, patient weight and disability. Ergonomics. (2008) ; 51: (7): 1042-52. |
[31] | Chaffin D, Herrin G, Keyserling W. Preemployment strength testing: an updated position. J Occup Med. (1978) ; 20: (6): 403-8. |
[32] | Keyserling W, Herring G, Chaffin D. Isometric strength testing as means of controlling medical incidents on strenuous jobs. J Occup Med. (1980) ; 22: (5): 332-6. |
[33] | Zhuang Z, Stobbe T, Collins J, Hongwei H, Hobbs G. Psychophysical assessment of assistive devices for transferring patients/residents. Appl Ergon. (1999) ; 31: (1): 35-44. |
[34] | Santaguida P, Pierrynowski M, Goldsmith C, Fernie G. Comparison of cumulative low back loads of caregivers when transferring patients using overhead and floor mechanical lifting devices. Clin Biomech. (2005) ; 20: (9): 906-16. |
[35] | Radwin R, Masters G, Lupton F. A linear force-summing hand dynamometer independent of point of application. Appl Ergon. (1991) ; 22: (5): 339-45. |
[36] | Bao S, Silverstein B. Estimation of hand force in ergonomic job evaluations. Ergonomics, 48: (3): 288-301. Ergonomics. 2005; 48: (3): 288-301. |
[37] | Antony N, Keir P. Effects of posture, movement and hand load on shoulder muscle activity. J Electromyogr Kinesiol. (2010) ; 20: (2): 191-8. |
[38] | Brookham R, Wong J, Dickerson C. Upper limb posture and submaximal hand tasks influence shoulder muscle activity. Int J Ind Ergon. (2010) ; 40: (3): 337-44. |


