
A comparison of the effects of green tea and cocoa on glycaemic control and insulin sensitivity in patients with type 2 diabetes mellitus: a systematic review and meta-analysis
Abstract
BACKGROUND:
Type 2 Diabetes Mellitus (T2DM) is among the most frequent chronic diseases in virtually all countries, posing a global health threat. Therefore, Preventive interventions are critical for reducing the enormous burden of diabetes. Flavanols may assist people with metabolic disorders to maintain glucose homeostasis by inhibiting digestive enzymes and glucose transporters. Green Tea (GT) and cocoa have gotten much attention since their flavanols are high.
OBJECTIVES:
To investigate the effects of polyphenols from GT and cocoa (>4 weeks) on reducing the incidence of complications and improving glycaemic control and insulin sensitivity in adult patients with T2DM through outcomes Fasting Blood Glucose (FBG), Fasting Blood Insulin (FBI), Haemoglobin A1c (HbA1c) and Homeostatic Model Assessment of Insulin Resistance (HOMA-IR).
METHODOLOGY:
An electronic research programme was applied, using different databases (including Web of Science, PubMed/Medline, Scopus, and Cochrane Reviews) to find studies that have evaluated the impact of polyphenols from GT and cocoa on reducing the incidence of complications and improving glycaemic control and insulin sensitivity in adult patients with T2DM. Articles published between 2005 and 2021 in English were selected.
RESULTS:
15 and 7 studies involved 738 participants on GT (348 male/390 female). In contrast, the ones focused on cocoa had 331 participants (83 male/ 248 female) with T2DM aged 18–65 years, and a BMI range of 25–34.9 kg/m2 was identified and included in the present review. 43 and 27% of studies were low-risk bias in cocoa and GT, respectively. The results of the meta-analysis showed no significant difference in FBG levels following GT and cocoa consumption compared to the control group (SMD: –0.08; 95% CI: –0.43 to 0.28; P = 0.68 and SMD: –0.65; 95% CI, –1.40 to 0.10; P = 0.09, respectively). Also, the results showed no significant difference for GT and cocoa intervention (SMD: 0.18; 95% CI: –0.27 to 0.64; P = 0.43 and SMD: –0.80; 95% CI: –1.92 to 0.31; P = 0.16, respectively). In addition, the results of the HbA1c analysis showed no significant reduction after GT and cocoa consumption (SMD: –0.41; 95% CI: –0.85 to 0.03; P = 0.07 and SMD, –0.37; 95% CI, –0.77 to 0.04; P = 0.08, respectively). There was no evidence that GT and cocoa interventions effectively improved HOMA-IR (SMD: 0.02; 95% CI: –0.16 to 0.20; P = 0.80 and SMD, –1.65; 95% CI, –3.77 to 0.46; P = 0.13, respectively
CONCLUSION:
The evidence shows that the short-term administration of cocoa and GT did not significantly reduce the FBG, FBI, HbA1c, and HOMA-IR levels in adult patients with T2DM.
1Introduction
1.1Diabetes management strategies and dietary flavonoids
Type 2 diabetes mellitus (T2DM) are among the most frequent chronic diseases in virtually all countries, posing a global health threat [1]. As of 2017, T2DM affected more than 8.4% of individuals globally; by 2045, this percentage is expected to climb to 9.9% [2]. Preventive interventions are critical for reducing the enormous burden of diabetes. Although drugs may help postpone the onset of diabetes complications, long-term use can be expensive and have various adverse effects [3]. Therefore, diabetic patients and doctors contemplate alternative and complementary treatments, such as herbal medications with anti-diabetic effects [4]. Indeed, plants have traditionally been a valuable source of pharmaceuticals, and many currently accessible medications are produced directly or indirectly from plants [5]. The herbal remedies may be promising for controlling diabetes.
Lifestyle changes can slow the evolution of T2DM in prediabetic people with impaired glucose tolerance or fasting glucose [6–10]. For example, Flavanols, a subset of plant-derived phytochemicals known as flavonoids, have recently received increased attention after epidemiological studies found a negative relationship between flavanol consumption and the development of diabetes [11, 12] Flavanols may assist people with metabolic disorders in maintaining glucose homeostasis by inhibiting digestive enzymes and glucose transporters, a strategy that assists people with metabolic disorders in maintaining glucose homeostasis [10;13]. In vitro studies have demonstrated that flavanols help inhibit carbohydrate digestive enzyme activity, enhance insulin sensitivity, inhibit hepatic gluconeogenesis by reducing gluconeogenic genes, and improve oxidative stress [14–17].
GT and cocoa have gotten much attention since they’re high in flavanols. Cocoa, GT, grapes, and apples are among the highest sources of flavonols [18]. After the consumption of flavanol-rich food, including cocoa, and tea, various polyphenol-derived phenolic acids, for example, m-hydroxyphenyl acetic acid, m hydrox-yphenylpropionic acid, m-hydroxybenzoic acid, and phenyl-g-valerolactones are generated [19–21]. Furthermore, cocoa may have a favourable effect on insulin signalling, possibly by increasing the incretin response or reducing oxidative stress and inflammation in the insulin-signalling pathways [22]. According to systematic reviews and meta-analyses, chocolate/cocoa improves FBI and insulin resistance in healthy adults [23–29]. The analysis of RCTs included in the review by [10] shows that cocoa consumption lowered FBG.
Catechins, flavonoid-like polyphenols, are primarily responsible for GT’s beneficial effects on human health [3]. These catechins include epigallocatechin-3-gallate (EGCG), as well as quercetin, theaflavins, theanine, caffeine, chlorogenic acid, and gallic acid [30–32]. Epicatechin (EC), epigallocatechin (EGC), epicatechin gallate (ECG), and epigallocatechingallate are the four primary catechins present in green tea extract (GTE) [33;34]. Moreover, epidemiological studies in humans have suggested that long-term use of GT is related to a lower risk of diabetes [35, 36]. Several randomised controlled studies (RCTs) have found that consuming GTE regularly can improve oral glucose tolerance in healthy persons and lower FBG and HbA1c levels in people at risk of diabetes [37–40].
However, systematic studies and meta-analyses on the link between GT intake, insulin resistance, and glycaemic control have produced conflicting results. For example, GT has been shown to enhance glycaemic control in some trials [41], whereas others have found no link between GT consumption and glycaemic management [42, 43]. According to a meta-analysis of seven RCTs by [44], the consumption of GT does not decrease FBG, FBI, HbA1c or HOMA-IR levels in populations at risk of T2DM. Another meta-analysis of 22 RCTs showed that the administration of GT with or without caffeine significantly reduced FBG. Still, the results did not support a positive effect on FBI, HbA1c or HOMA-IR in adults with [45]. In 27 RCTs, short-term GT supplementation significantly reduced FBG but did not significantly affect FBI or HbA1c in T2DM patients [3]. In the results of six RCTs, no evidence supports the suggestion that consuming GT/GTE could reduce HbA1c, HOMA-IR, FBG or FBI levels in adults with prediabetes and T2DM [31]. However, this survey study concluded that the benefits of GT ingestion were due to caffeine and not catechins [46]. The meta-analysis indicated that the supplementary intake of GT had no significant effect on FPG, FBI, HbA1c or HOMA-IR in patients with T2DM [47].
1.2Rationale for the review
Even among researchers that advocate polyphenol consumption, GT and/or cocoa consumption for T2DM is debatable. For example, according to [48, p. 303], “Indeed, tea, red wine and cocoa are good sources of flavanols (a class of polyphenol), but it is not completely established whether these foodstuffs exert a beneficial effect against diabetes.” In addition, [3, p. 2], ‘findings from randomized controlled trials (RCTs) on GT supplementation and glycaemic control or insulin sensitivity in individuals with preclinical diabetes or T2DM are debatable’. The focus was on consuming green tea and cocoa compared to other types reported to contain more abundant flavonoids because tea and cocoa consume more than other foods. For example, Cocoa and its product, chocolate, is a primarily consumed food worldwide [49]. Furthermore, according to the 2013 World Tea Market Report, tea is the most consumed beverage in the world [50]. Cocoa and GT are rich sources of various polyphenol compounds [3, 51]. We want to investigate what the most beneficial for diabetics, which are considered well available. Therefore, this research systematically reviews all existing studies that have evaluated the outcomes of GT and cocoa supplementation in adults with T2DM to assess the effectiveness of polyphenol supplementation in improving glycaemic control and insulin sensitivity. According to [52], FBG measurements do not adequately indicate glycaemic management because they do not reflect what happens after meals and during the day in free-living situations. Therefore, this systematic review and meta-analysis aimed to investigate the effects of polyphenol supplementation (GT and cocoa) on improving glycaemic control and insulin sensitivity in adult patients with T2DM through outcomes FBG, FBI, HbA1c and HOMA-IR.
2Methodology
Existing studies that have assessed the long-term positive effect of GT and cocoa on glycaemic control and insulin sensitivity in patients with T2DM were reviewed after assessing their quality.
2.1Types of studies
This study included every pertinent experimental study (including randomized controlled trials with either a parallel or crossover design), regardless of whether a double-blind method was used. Furthermore, reviews, papers and meeting abstracts were examined to obtain more evidence. The inclusion and exclusion criteria were applied as described below.
2.1.1The inclusion criteria
Previous studies among adult patients aged 18 years or older with T2DM, regardless of gender or ethnicity or the number of participants, with interventions that are relevant to GT (beverage or capsule) and/or cocoa (beverage or capsule or solid chocolate) and published in the English language from 2005 onwards (this date span was common to all sampled databases) were included in this review. The outcome of the studies was at least one of the following: (1) fasting glucose, (2) fasting insulin, (3) HbA1c and (4) HOMA-IR. Therefore, studies with paediatric participants were excluded from this review. The main objective of this systematic review was to compare the effect of GT and cocoa on glycaemic control and insulin sensitivity in patients with T2DM; therefore, only words related to this objective were used when searching the databases.
2.1.2The exclusion criteria
Studies that had the following criteria were excluded from this review –
(1) studies that included adult patients without T2DM, (2) studies that used an unclear number/rate of any intervention was relevant to GT and/or cocoa, (3) a review or a meeting abstract, (4) ongoing studies, (5) studies that lacked detailed information on baseline results or follow-up, (6) studies that lacked information on the study design, (7) nonhuman-based studies, (8) studies with limited access to the full text, (9) studies were ongoing when this review was conducted, (10) studies that lacked an appropriate control group in the research design, (11) studies on GT and/or cocoa but not type 2 diabetes or that did not focus on examining fasting glucose, fasting insulin, HbA1c and/or HOMA-IR, (12) studies on T2DM but did not include interventions assessing the effect of GT or cocoa, (13) studies not on T2DM or GT or cocoa or fasting glucose or fasting insulin or HbA1c or HOMA-IR, (14) studies that did not meet the outcome variables, (15) studies that used combination intervention, (16) studies that assessed type 1 diabetes or insulin-dependent diabetes, (17) studies not published in the English language and (18) repeated studies.
2.2Participants
Adult patients with T2DM were included in this study regardless of ethnicity.
2.3Intervention/Exposure types
The included studies conducted interventions that were relevant to the effect of GT and/or cocoa on T2DM, and some had information regarding the intensity and/or duration of their studies. The sources of this information were included where available.
2.4Types of outcome measures
In this review, the effectiveness of GT and/or cocoa on glycaemic control and insulin sensitivity in patients with T2DM was assessed using the following: (1) fasting glucose, (2) fasting insulin, (3) HbA1c and/or (4) HOMA-IR.
2.5Search strategy
To identify original research articles, Web of Science, PubMed/MEDLINE, Scopus, and Cochrane were used. Retrieved references and reviews were also examined to select relevant articles. First, the keywords/terms used for green tea were ‘ tea’ OR ‘green tea’ OR ‘green tea extract’ OR ‘tea polyphenols’ OR ‘green tea catechins’ OR ‘catechin’ OR ‘epigallocatechin’ OR ‘epicatechin’ OR ‘tea component(s)’ OR ‘epigallocatechin gallate’ AND ‘glycated protein’ OR ‘insulin sensitivity’ OR ‘hyperglycemia’ OR ‘insulin resistance’ OR ‘diabetes’ OR ‘glucose’ OR ‘glycaemic control’ OR ‘HbA1c’ OR ‘fructosamine’ OR ‘insulin’ OR ‘type 2 diabetes’. Second, the keywords/terms used for cocoa were ‘Cocoa’ OR ‘Cacao’ OR ‘Chocolate’ OR ‘dark chocolate’ OR ‘Cocoa powder’ OR ‘dark chocolate’ OR ‘cocoa flavanols OR ‘cocoa polyphenols’ AND ‘glycated protein’ OR ‘insulin sensitivity’ OR ‘hyperglycemia’ OR ‘insulin resistance’ OR ‘diabetes’ OR ‘glucose’ OR ‘glycaemic control’ OR ‘Hb A1c’ OR ‘fructosamine’ OR ‘insulin’ OR ‘type 2 diabetes’.
2.6Identification of relevant studies
Studies were selected for close examination based on the abstracts of the articles in the studies that were examined to ensure their eligibility for inclusion. Subsequently, these studies were evaluated and verified for inclusion or exclusion based on a thorough review of the full texts. The last search for data was performed on January 3, 2022.
2.7Data extraction
Related findings were derived from the selected studies, and the data extracted from the studies include the name of the author (including the year of publication), country where the study was conducted, study design, study period, population number (total enrolled/completers) and participants’ characteristics, exclusion criteria, intervention type, dose, and duration (intervention/control group), main/other outcomes and p-value.
2.8Risk of Bias assessment
The Risk of Bias 2 (RoB 2) tool is an update to the original risk of bias tool launched in 2008 [53]. RoB 2 tool was used to appraise the risk of bias in the randomized controlled trials included in this review. Bias is assessed as a high, low or some concerns judgment. The following criteria were considered in the evaluation: (1) Randomisation process, (2) Deviations from the intended interventions, (3) Missing outcome data, (4) Measurement of the outcome, and (5) Selection of the reported result. In addition, we used RoB 2 to create a funnel chart to analyse the bias of the studies in this systematic review.
2.9Statistical analysis
To supplement the systematic review, a meta-analysis was performed. We used Review Manager 5.4 software to assess the heterogeneity of indicators between the GT group and the control group, as well as the cocoa group and control group. The mean difference (MD) between the baseline and final measurements of fasting glucose, fasting insulin, HbA1c and HOMA-IR was calculated, and the indexes between the GT, cocoa, and control groups were compared. In this review, heterogeneity was evaluated by the index of inconsistency (I2), and the statistical value of I2 reflected the level of heterogeneity. The result was considered heterogeneous if I2 was more than 50%. A random-effects model was employed; otherwise, a fixed-effects model was used. In this review, a P-value<0.05 was considered statistically significant. Some studies did not mention the standard deviation of change. In this case, previous systematic reviews were checked, and the data was obtained. The study [38] from [44] as well as [54] A, [55] and [56] from [31]. [54, 57–62] by calculating S.D. [63]:
3Results
3.1Study selection
A total of 3329 and 1723 studies that evaluated the effect of GT and cocoa, respectively, on glycaemic control and insulin sensitivity in patients with T2DM were identified by searching the literature, as shown in Fig. 2. A total of fifteen articles on GT [38, 40, 46, 54–56, 61, 62, 64–67] and seven on cocoa [57–60, 68–70], which were published between 2005 and 2021, met the inclusion criteria.
Fig. 1
Flowchart of study selection and exclusion in detail.
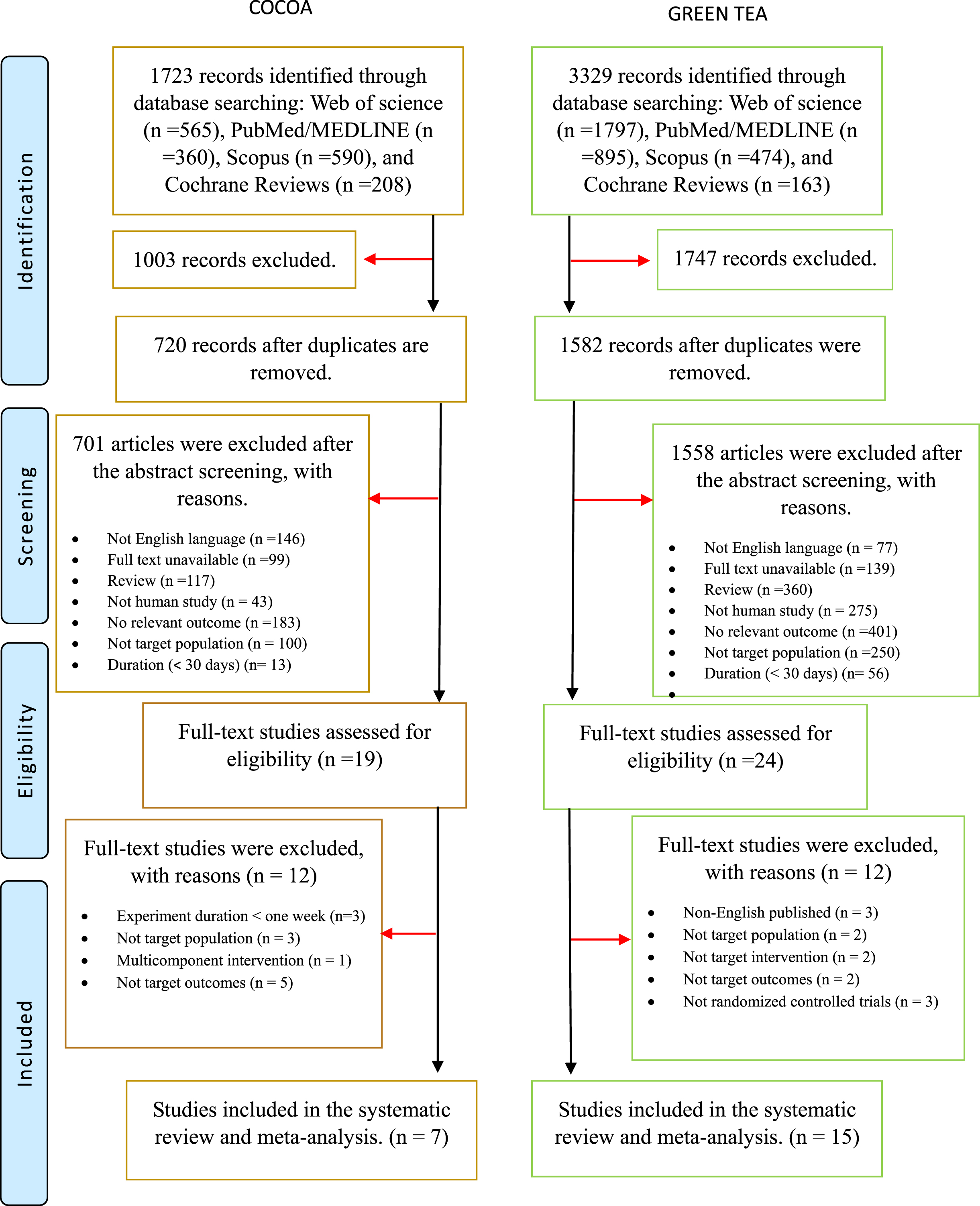
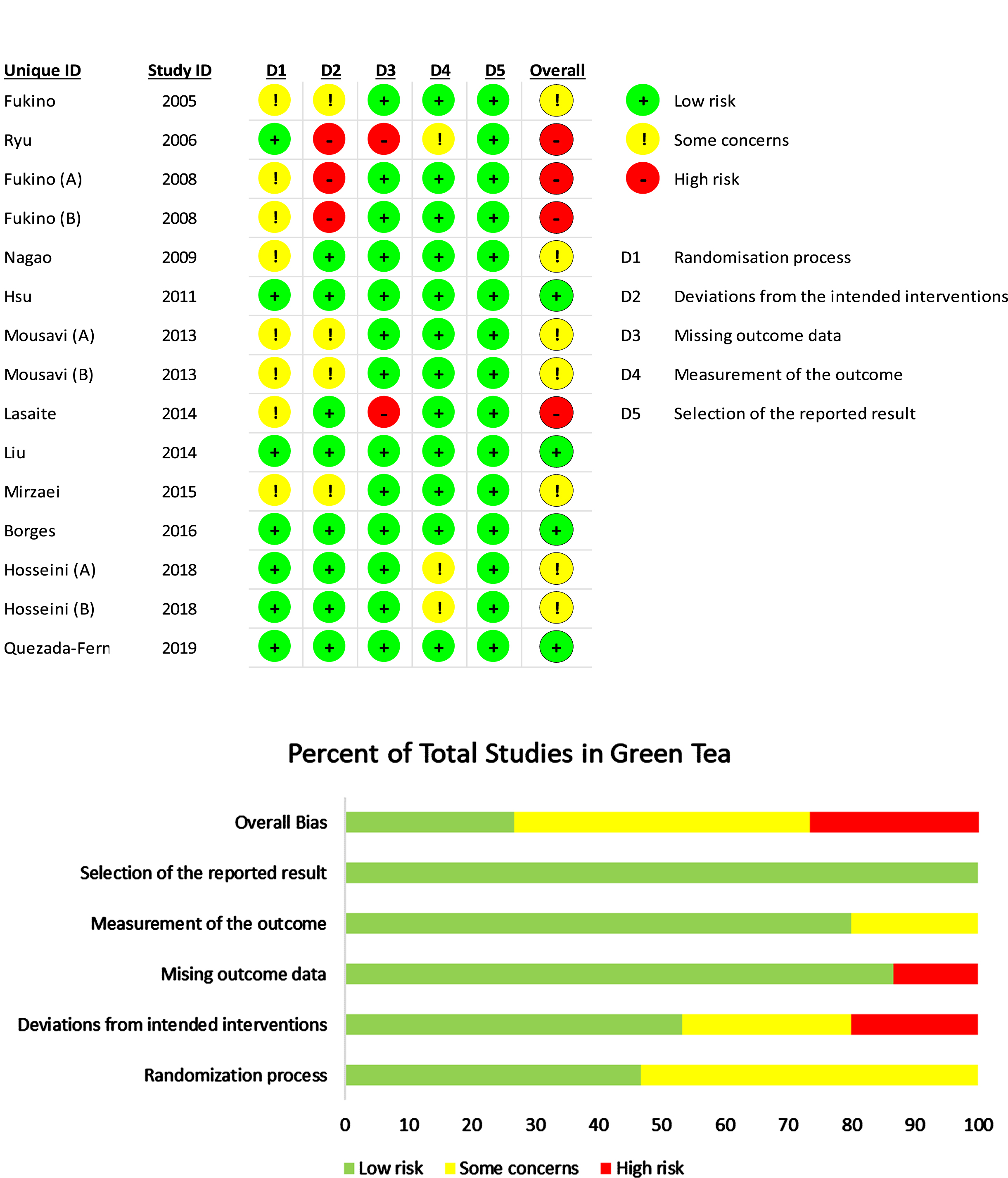
Fig. 2
Risk of bias summary: review authors’ judgements about each risk of bias item for each included study in green tea.
3.2Study characteristics
3.2.1Study design and country
All the studies were parallel randomized controlled trials (studies on GT –[40, 46, 54–56, 61, 62, 65–67, and studies on cocoa –57, 59, 60, 68–70], except for three that were cross-over randomized controlled trials –two on GT [38, 64] and one on cocoa [58].
The majority of the included studies that focused on GT were conducted in Asia: three in Iran [54, 56, 67], three in Japan [38, 46, 61], two in Taiwan [40, 65], one in Lithuania [55], and one in South Korea [64], except for two, which were conducted in Mexico [62] and Brazil [66]. While for cocoa, three of the studies were conducted in Asia [60, 69, 70], two in the United Kingdom [58, 68], one in the United States [57] and one in Germany [59]. Table 1 shows the basic study characteristics of each study included in this review.
Table 1
Characteristics of the included trials of the effects of green tea intake in T2D patients
| Author | Study design | Duration | No. of participants (M/F) | Intervention | Outcome | |
| GT group (flavanols) | Placebo group (flavanols) | |||||
| Fukino et al. (2005) | Parallel RCT | 2 mo. | 66 (53/13) | 544 mg of GT (456 mg of catechins) | NR | =FBG,=FBI,=HbA1c,=HOMA-IR |
| Ryu et al. (2006) | Cross-over RCT | 4 wk. | 55 (31/24) | 900 ml of GT (1200 mg) | water | =FBG,=FBI,=HOMA-IR |
| Fukino et al. (2008) (A) | Cross-over RCT | 2 mo. | 29 (25/4) | GTE (456 mg of catechins) | No intervention | =FBG,=FBI, ↓HbA1c,=HOMA-IR |
| Fukino et al. (2008) (B) | Cross-over RCT | 2 mo. | 31 (26/5) | GTE (456 mg of catechins) | No intervention | =FBG,=FBI, ↓HbA1c,=HOMA-IR |
| Nagao et al. (2009) | Parallel RCT | 12 wk. | 50 (19/31) | 340 ml of GT (582.8 mg of catechins) | (96 mg catechins) | ↓FBG,=FBI, ↓HbA1c |
| Hsu et al. (2011) | Parallel RCT | 16 wk. | 68 (24/44) | GTE (856 mg of EGCG) | cellulose | ↓HbA1c, ↓HOMA-IR |
| Mousavi et al. (2013) (A) | Parallel RCT | 8 wk. | 39 (16/23) | 4 x2.5 g of GT (1000 mg) | No intervention | =FBG |
| Mousavi et al. (2013) (B) | Parallel RCT | 8 wk. | 38 (17/21) | 2 x2.5 g of GT (500) | No intervention | =FBG |
| Lasaite et al. (2014) | Parallel RCT | 18 mo. | 56 (21/35) | 200 mg of GTE (140 mg) | cellulose | =HbA1c |
| Liu et al. (2014) | Parallel RCT | 16 wk. | 77 (32/45) | 1500 mg of GTE (856 mg of EGCG) | cellulose | =FBG,=HbA1c, ↓HOMA-IR |
| Mirzaei et al. (2015) | Parallel RCT | 8 wk. | 82 (16/66) | 500 mg of GTE (80 mg) | cellulose | ↓FBG, ↓FBI, ↓HbA1c |
| Borges et al. (2016) | Parallel RCT | 12 wk. | 47 (27/20) | GT (800 mg of EGCG) | NR | =HbA1c |
| Hosseini et al. (2018) (A) | Parallel RCT | 8 wk. | 40 (15/25) | GT (300 mg of EGCG) TT genotype | NR | =FBG,=HOMA-IR |
| Hosseini et al. (2018) (B) | Parallel RCT | 8 wk. | 40 (16/24) | GT (300 mg of EGCG) AA+AT genotype | NR | =FBG,=HOMA-IR |
| Quezada-Fern
| Parallel RCT | 12 wk. | 20 (10/10) | 400 mg of GTE (≥360 mg) | NR | =FBG,=HbA1c |
The arrow indicates a decrease (↓) in the levels or activity of the different parameters analysed. (=) symbol designates unchanged parameters. RCT, randomized controlled trial; FBG, fasting blood glucose; FBI, fasting blood insulin; HbA1c, glycated haemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; GT, green tea; GTE, green tea extract; EGCG, epigallocatechin gallate; wk., week; mo., month; M, male; F, female; NR; no report.
Table 2
Characteristics of the included trials of the effects of cocoa intake in T2D patients
| Author | Study design | Duration | No. of participants (M/F) | Intervention | Outcome | |
| Cocoa group (flavanols) | Placebo group (flavanols) | |||||
| Balzer et al. (2008) | Parallel RCT | 30 days | 51 (20/31) | cocoa drink (963 mg) | cocoa drink (75 mg) | =FBG,=HbA1c |
| Mellor et al. (2010) | Cross-over RCT | 8 wk. | 12 (7/5) | 45 g of CP (16.6 mg) | 45 g of CP (<2 mg) | =FBG,=FBI,=HbA1c |
| Curtis et al. (2012) | Parallel RCT | 12 mo. | 93 (0/93) | 27 g of DC (850 mg) | NR | =HbA1c, ↓HOMA-IR, ↓FBI |
| Rostami et al. (2015) | Parallel RCT | 8 wk. | 60 (24/36) | 25 g of DC (450 mg) | 25 g of WC (0) | ↓FBG, ↓FBI, ↓HbA1c |
| Dicks et al. (2018) | Parallel RCT | 12 wk. | 35 (18/17) | 2.5 g of Cocoa capsules (207.5 mg) | cocoa-free capsules | ↓FBG, ↓FBI,=HbA1c, ↓HOMA-IR |
| Jafarirad et al. (2018) | Parallel RCT | 8 wk. | 44 (14/30) | 30 g of DC (540 mg) | NR | ↓FBG,=FBI, ↓HbA1c |
| Fakhari et al. (2021) | Parallel RCT | 8 wk. | 36 (0/36) | 3x25 g / per week of DC (450 mg) | 25 g of WC (0) | =FBG |
The arrow indicates a decrease (↓) in the levels or activity of the different parameters analysed. (=) symbol designates unchanged parameters. RCT, randomized controlled trial; FBG, fasting blood glucose; FBI, fasting blood insulin; HbA1c, glycated haemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; DC, dark chocolate; WC, white chocolate; CP, Cocoa powder; h, hour; wk., week; mo., month; M, male; F, female; NR; no report.
3.2.2Duration of study and follow-up
The follow-up period for most of the studies was less than three months, except for three studies (which focused on GT) [40, 55, 65] and one study (which focused on cocoa) [68]. [55] follow-up period was 18 months (study period: none-mention), [38] four months (study period: late February and early March 2003), [65] four months (study period: December 2007 to November 2008), [40] four months (study period: April 2011 to March 2012), [46] three months (study period: May 2004 to November 2004), [66] three months (study period: November 2013 to December 2014), [62] (study period: January to December 2016), [68] three months (study period: none-mentioned) and [59] three months (study period: September 2016 to April 2017). Four studies that focused on GT ([61] [study period: late February to early March 2003]; [54] [study period: none-mentioned]; [56] [study period: January to June 2008]; [67] [study period: August 2017 to March 2018]) and four studies focused on cocoa ([58] [study period: January 2008 to October 2008]; [69] [study period: March 2011 to February 2012]; [70] [study period: none-mention]; [60] [study period: none-mentioned]) were carried out with a follow-up period of two months. One study on GT ([64 study period: none-mention]) and one study on cocoa ([57 study period: none-mentioned]) were carried out with a follow-up period of one month.
3.3Participants’ characteristics
The studies that focused on GT had 738 participants (348 male/390 female), while the ones that focused on cocoa had 331 participants (83 male/248 female) with T2DM, aged 18–65 years. All the participants were overweight/obese (BMI: 25–34.9 kg/m2), except for the participants in [64] study (which focused on GT) and [68 and 70] studies (which focused on cocoa) (BMI < 25 kg/m2).
Most of the included studies did not report the duration of the diagnosis of T2DM, except for six studies on GT [55, 56, 62, 65–67] and five studies on cocoa [58, 59, 68, 69, 70]. The duration of the diagnosis of diabetes reported by these studies was less than eight years, except for one study on GT that reported a duration > 12 years [66].
3.4Quality assessment and publication bias
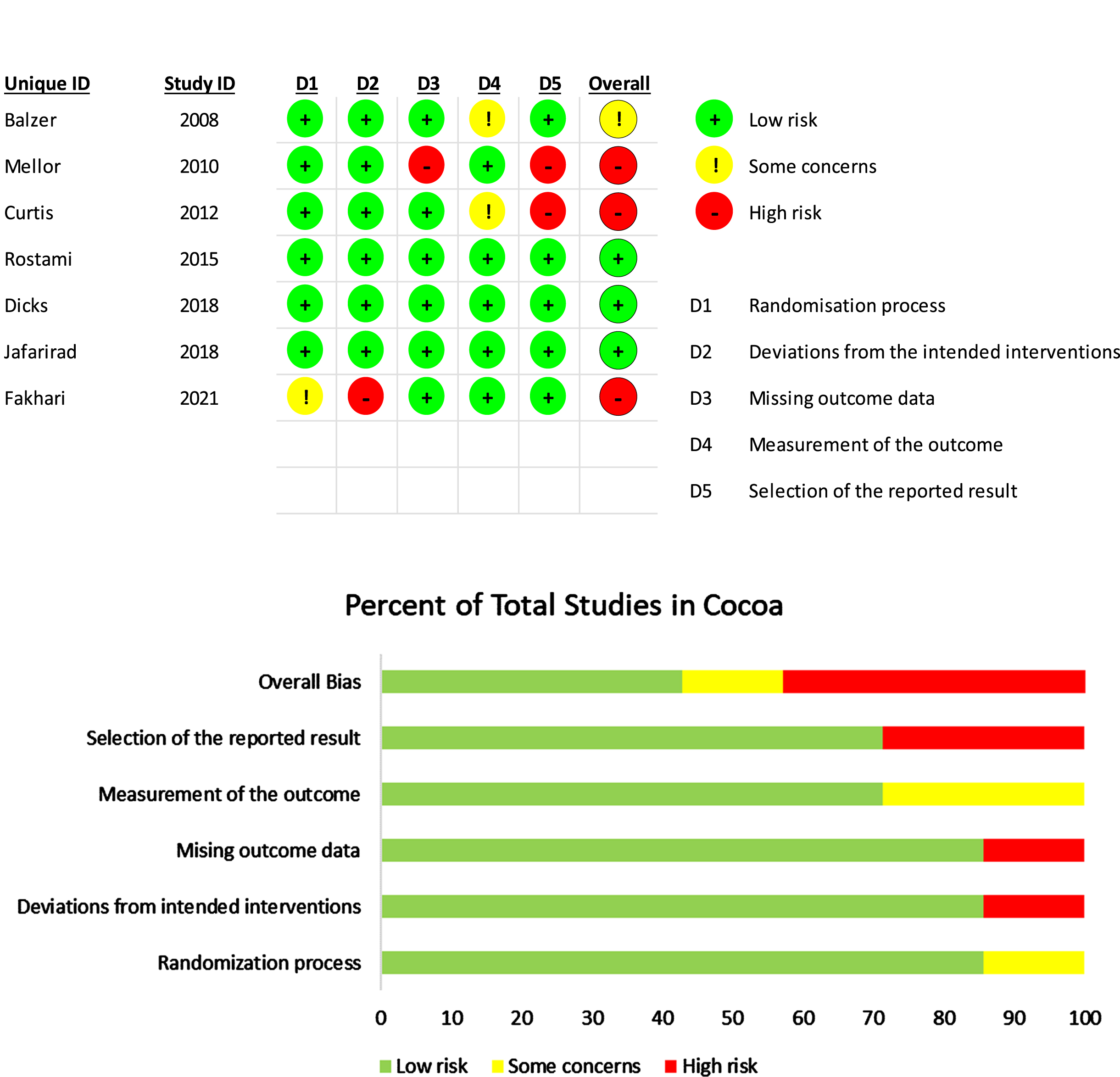
Based on the assessment tool, only four studies on GT were of low risk [40, 62, 65, 66]. In contrast, just two studies among studies on cocoa were of low risk [59, 69]. Five studies on GT [46, 54, 56, 61, 67] and only two studies on cocoa [57, 70] had some concerns. Only three studies on GT [38, 55, 64] and three studies on cocoa [58, 60, 68] had high risk, as shown in Figs. 2 and 3.
Fig. 3
Risk of bias summary: review authors’ judgements about each risk of bias item for each included study in cocoa.
3.4.1Risk of bias
The risk of bias assessment was carried out with RoB2 tool, as shown in Figs. 2 and 3. The studies by [40, 62, 64–67] on GT and the studies of [57–59, 68–70] on cocoa provided comprehensive explanations of the randomisation process. Seven studies on GT [40, 46, 55, 62, 65–67] and six studies on cocoa [57–59, 68–70] had a low risk of bias regarding deviations from the intended interventions. Ten articles on GT [38, 40, 46, 54, 56, 61, 62, 65–67] and six studies on cocoa [57, 59, 60, 68–70] had a low risk of bias regarding missing outcome data. Ten studies on GT [38, 40, 46, 54–56, 61, 62, 65, 66] and only four studies on cocoa [58–60, 69] had a low risk of bias regarding the measurement of the outcome. The majority of the studies on GT [38, 40, 46, 54–56, 61, 62, 64–67] and five studies on cocoa [57, 59, 60, 69, 70] had a low risk of bias concerning the selection of the reported result.
3.5Meta-analysis and data synthesis
In total, data from fifteen studies [38, 40, 46, 54–56, 61, 62, 64–67] that compared GT with placebos were included in these meta-analyses. On the other hand, seven studies [57–60, 68–70] that compared cocoa supplements with placebos were included in these meta-analyses. Forest plots depicting the results of the meta-analysis for each assessed outcome are shown in Figs. 4, 5.
Fig. 4
Meta-analysis results of green tea for each assessed outcome.
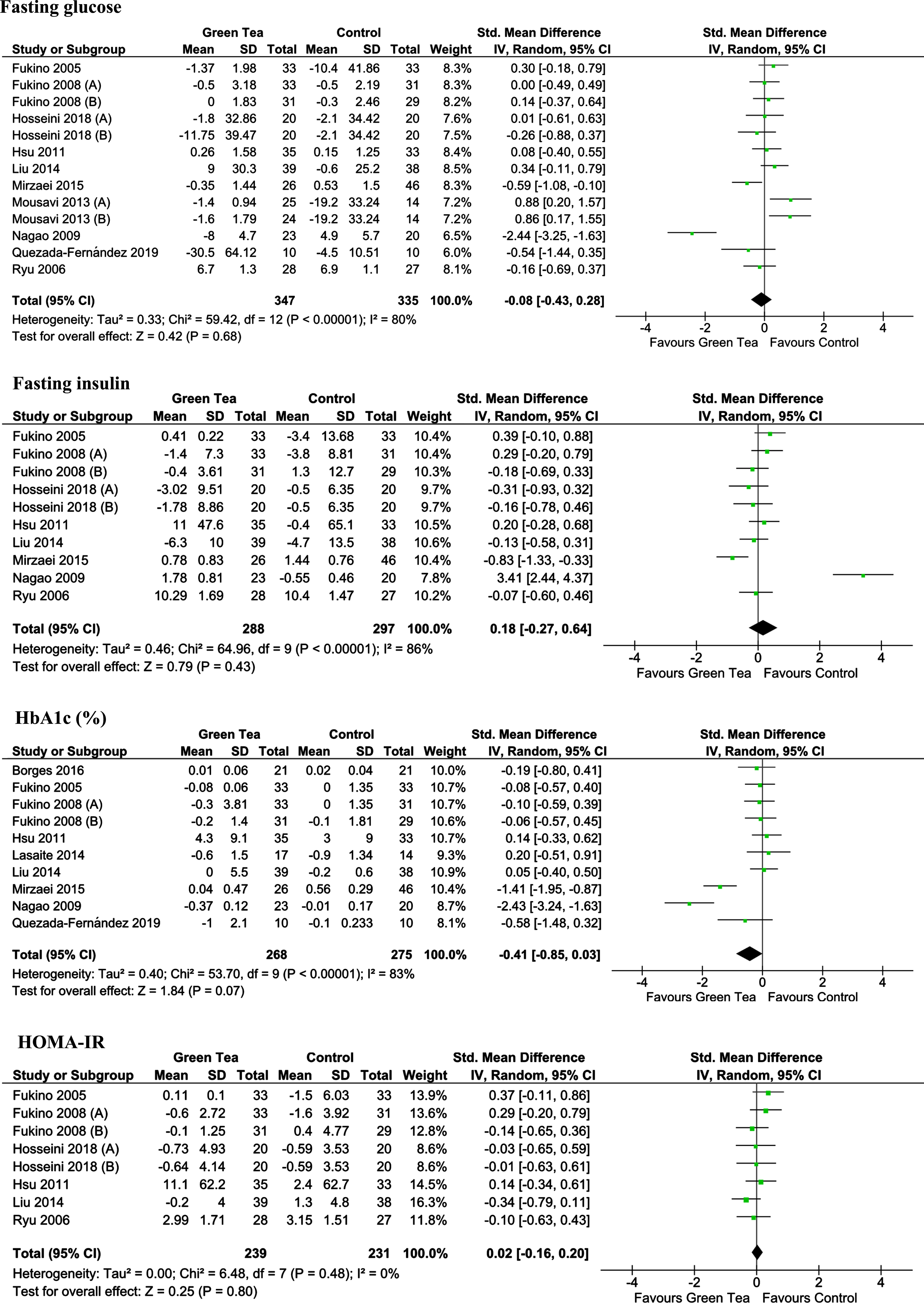
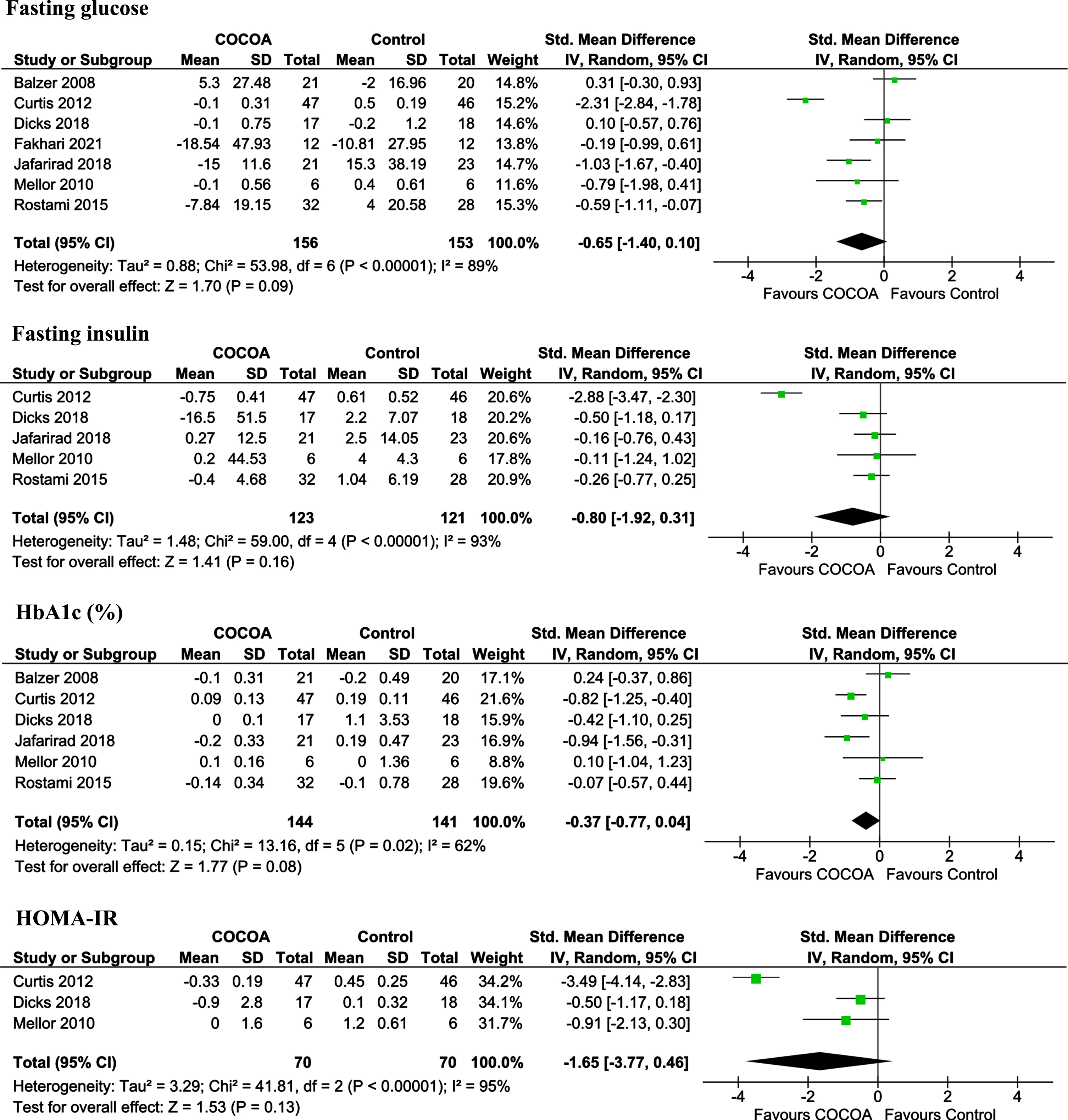
Fig. 5
Meta-analysis results of cocoa for each assessed outcome.
3.5.1Dietary polyphenols (cocoa vs. green tea) and association with incidence glycaemic control and insulin sensitivity in patients with type 2 diabetes mellitus
3.5.1.1. Fasting glucose. Amongst the included studies, twelve RCTs assessed the effect of GT on FBG levels [38, 40, 46, 54, 61, 62, 64, 65, 67], while seven RCTs assessed the effect of cocoa on FBG levels [57–60, 68–70]. The GT and cocoa studies that involved 635 (300 males/335 females) and 331 (82 males/248 females) participants, respectively, were included in the FBG analysis. The results of the meta-analysis showed no significant difference in FBG levels following GT and cocoa consumption compared to the control group (SMD: –0.08; 95% CI: –0.43 to 0.28; P = 0.68 and SMD: –0.65; 95% CI, –1.40 to 0.10; P = 0.09, respectively). The forest plot of the meta-analysis for the FBG level is shown in Figs. 4, 5.
3.5.1.2. Fasting insulin. Ten studies assessed the effect of GT on the FBI level and involved 538 (257 males/281 females) participants who were included in the FBI analysis [38, 40, 46, 56, 61, 64, 65, 67]. Five studies assessed the effect of cocoa on the FBI level and involved 244 (63 males/181 females) participants who were included in the FBI analysis [58, 59, 68–70]. The results showed no significant difference for GT intervention (SMD: 0.18; 95% CI: –0.27 to 0.64; P = 0.43) also no statistical difference for cocoa intervention (SMD: –0.80; 95% CI: –1.92 to 0.31; P = 0.16). The forest plot of the meta-analysis for the FBI level is shown in Figs. 4, 5.
3.5.1.3. HbA1c. Ten studies reported the HbA1c level as an outcome after GT consumption and involved 526 (253 males/273 females) participants who were included in the HbA1c analysis [38, 40, 46, 55, 56, 61, 62, 65, 66]. Six studies reported the HbA1c level as an outcome after cocoa consumption and involved 295 (83 males/212 females) participants who were included in the HbA1c analysis [57–59, 68–70]. The results of the HbA1c analysis showed no significant reduction after GT and cocoa consumption (SMD: –0.41; 95% CI: –0.85 to 0.03; P = 0.07 and SMD, –0.37; 95% CI, –0.77 to 0.04; P = 0.08, respectively). The forest plot of the meta-analysis for the HbA1c level is shown in Figs. 4, 5.
3.5.1.4. HOMA-IR. Amongst the included studies, eight RCTs assessed the effect of GT on HOMA-IR levels [38, 40, 61, 64, 65, 67], while three RCTs assessed the effect of cocoa on HOMA-IR levels [58, 59, 68]. The GT and cocoa studies that involved 406 (222 males/184 females) and 140 (25 males/115 females) participants, respectively, were included in the HOMA-IR analysis. The results of the meta-analysis showed no significant difference in HOMA-IR levels following GT and cocoa consumption compared to the control group (SMD: 0.02; 95% CI: –0.16 to 0.20; P = 0.80 and SMD: –1.62; 95% CI, –3.77 to 0.46; P = 0.13, respectively). The forest plot of the meta-analysis for the FBG level is shown in Figs. 4, 5.
3.5.2Subgroup analysis
We stratified studies based on the type of intervention (beverage, capsule, solid chocolate in cocoa) and (beverage, capsule in GT) duration of intervention (≥12 and <12 weeks), flavanols dosage (≥500 and <500 mg/day) and baseline of FBG (high, >7.1 mmol/l and standard, 4–7 mmol/l). Subgroup analysis showed that cocoa consumption longer than three months resulted in a highly significantly reduce in HbA1c levels (SMD: –0.71; 95% CI: –1.07 to –0.35; P = 0.0001). Additionally, solid chocolate consumption resulted in a highly significant decrease in FBG and HbA1c (SMD: –1.01; 95% CI: –1.82 to –0.20; P = 0.01 in FBG) and (SMD: –0.50; 95% CI: –1.00 to –0.02; P = 0.04 in HbA1c). The dose (<500 mg/day) consumption resulted in a significant decrease in HOMA-IR (SMD: –0.60; 95% CI: –1.19 to –0.01; P = 0.05). However, It can be seen that studies who started with baseline of FBG within the normal range (4–7 mmol/l) had highly significant difference in FBG levels following GT and cocoa consumption compared to the group who started with FBG within the high range (>7.1 mmol/l) (SMD: –2.44; 95% CI: –3.25 to 1.63; P = 0.0001 and SMD: –0.62; 95% CI, –1.10 to –0.15; P = 0.01, respectively). As shown in Tables 3, 4.
Table 3
Result of subgroup analysis of included studies in the meta-analysis for green tea.
| Change in FBG | Change in FBI | Change in HbA1c | Change in HOMA-IR | ||||||||||
| Sub-grouped by | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | |
| Type of intervention | Beverage | 5 | –0.09[–0.77,0.58] | 0.78 | 4 | 0.59[–0.36,1.53] | 0.22 | 3 | –0.87[–2.15,0.42] | 0.19 | 3 | –0.02[–0.30,0.26] | 0.89 |
| Capsule | 5 | –0.05[–0.34,0.25] | 0.76 | 4 | –0.13[–0.51,0.25] | 0.51 | 6 | –0.24[–0.67,0.19] | 0.27 | 3 | 0.09[–0.19,0.36] | 0.55 | |
| Duration | ≥12 weeks | 5 | –0.34[–0.98,0.29] | 0.29 | 4 | 0.62[–0.20,1.44] | 0.14 | 7 | –0.32[–0.78,0.14] | 0.18 | 3 | –0.02[–0.30,0.26] | 0.89 |
| <12 weeks | 5 | 0.12[–0.28,0.52] | 0.56 | 4 | –0.19[–0.62,0.23] | 0.38 | 2 | –0.74[–2.04,0.56] | 0.26 | 3 | 0.09[–0.19,0.36] | 0.55 | |
| Flavanols dose | ≥500 mg/dl | 6 | –0.13[–0.77,0.52] | 0.70 | 4 | 0.43[–0.50,1.37] | 0.36 | 4 | –0.87[–1.93,0.18] | 0.11 | 3 | –0.11[–0.39,0.17] | 0.45 |
| <500 mg/dl | 4 | 0.03[–0.20,0.26] | 0.82 | 4 | 0.03[–0.20,0.26] | 0.80 | 5 | –0.10[–0.34,0.13] | 0.40 | 3 | 0.12[–0.12,0.36] | 0.32 | |
| Country | Western | 1 | –0.54[–1.44,0.35] | 0.24 | NA | NA | NA | 3 | –0.14[–0.55,0.27] | 0.50 | NA | NA | NA |
| Asian | 9 | –0.05[–0.41,0.32] | 0.81 | 8 | 0.18[–0.27,0.64] | 0.43 | 6 | –0.51[–1.08,0.06] | 0.08 | 6 | 0.02[–0.16,0.20] | 0.80 | |
| Study design | Parallel | 8 | –0.11[–0.58,0.37] | 0.66 | 6 | 0.29[–0.39,0.97] | 0.40 | 8 | –0.51[–1.07,0.06] | 0.08 | 4 | 0.02[–0.23,0.27] | 0.86 |
| Crossover | 2 | 0.07[–0.29,0.42] | 0.71 | 2 | 0.02[–0.27,0.32] | 0.88 | 1 | –0.08[–0.43,0.27] | 0.65 | 2 | 0.03[–0.27,0.32] | 0.86 | |
| Baseline FBG | High (>7.1 mmol/l) | 8 | 0.09[–0.19,0.37] | 0.53 | 6 | –0.08[–0.36,0.20] | 0.57 | 8 | –0.21[–0.54,0.11] | 0.20 | 5 | 0.04[–0.16,0.24] | 0.69 |
| Normal (4–7 mmol/l) | 2 | –2.44[–3.25,1.63] | 0.0001 | 2 | 1.65[–1.76,5.05] | 0.34 | 1 | –2.43[–3.24, –1.63] | 0.0001 | 1 | –0.10[–0.63,0.43] | 0.72 | |
| Overall bias | Low risk | 3 | 0.09[–0.31,0.49] | 0.66 | 2 | 0.02[–0.30,0.35] | 0.90 | 4 | –0.03[–0.30,0.25] | 0.85 | 2 | –0.11[–0.57,0.36] | 0.65 |
| Some concerns | 5 | –0.16[–0.85,0.54] | 0.65 | 4 | 0.44[–0.62,1.50] | 0.42 | 3 | –1.28[–2.56,0.00] | 0.05 | 2 | 0.15[–0. 17,0.48] | 0.35 | |
| High rick | 2 | 0.07[–0.29,0.42] | 0.71 | 2 | 0.02[–0.27,0.32] | 0.88 | 2 | –0.03[–0.34,0.29] | 0.87 | 2 | 0.03[–027,0.32] | 0.86 | |
FBG, fasting blood glucose; FBI, fasting blood insulin; HbA1c, glycated haemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; NA, not applicable.
Table 4
Result of subgroup analysis of included studies in the meta-analysis for cocoa.
| Change in FBG | Change in FBI | Change in HbA1c | Change in HOMA-IR | ||||||||||
| Sub-grouped by | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | Trials (n) | Std. Mean Difference IV, Random, 95% CI | P for effect size | |
| Type of intervention | Beverage | 1 | 0.31[–0.30,093] | 0.32 | NA | NA | NA | 1 | 0.24[–0.37,0.86] | 0.44 | NA | NA | NA |
| Capsule | 1 | 0.10[–0.57,0.76] | 0.77 | 1 | –0.50[–1.18,0.17] | 0.14 | 1 | –0.42[–1.10,0.25] | 0.22 | 1 | –0.50[–1.17,0.18] | 0.15 | |
| Solid chocolate | 5 | –1.01[–1.82, –0.20] | 0.01 | 4 | –0.87[–2.29,0.54] | 0.23 | 4 | –0.50[–1.00, –0.02] | 0.04 | 2 | –2.26[–4.78,0.27] | 0.08 | |
| Duration | ≥12 weeks | 2 | –1.11[–3.47,1.24] | 0.35 | 2 | –1.70[–4.03,0.63] | 0.15 | 2 | –0.71[–1.07, –0.35] | 0.0001 | 2 | –1.99[–4.93,0.94] | 0.18 |
| <12 weeks | 5 | –0.43[–0.93,0.07] | 0.09 | 3 | –0.21[–0.57,0.16] | 0.26 | 4 | –0.19[–0.74,0.35] | 0.48 | 1 | –091[–2.13,0.30] | 0.14 | |
| Flavanols dose | ≥500 mg/dl | 3 | –1.02[–2.55,0.51] | 0.19 | 2 | –1.52[–4.19,1.14] | 0.26 | 3 | –0.52[–1.21,0.17] | 0.14 | 1 | –3.49[–4.14, –2.83] | 0.0001 |
| <500 mg/dl | 4 | –0.34[–0.70,0.03] | 0.07 | 3 | –0.32[–0.71,0.06] | 0.10 | 3 | –0.16[–0.54,0.22] | 0.40 | 2 | –0.60[–1.19, –0.01] | 0.05 | |
| Country | Western | 4 | –0.68 [–2.09,0.74] | 0.35 | 3 | –1.20 [–3.03, 0.63] | 0.20 | 4 | –0.30[–0.85,0.26] | 0.30 | 3 | –1.65[–3.77,0.46] | 0.13 |
| Asian | 3 | –0.65 [–1.07,0.22] | 0.003 | 2 | –0.22[–0.61,0.17] | 0.26 | 2 | –0.48[–1.33,0.37] | 0.27 | NA | NA | NA | |
| Study design | Parallel | 6 | –0.63 [–1.46,0.19] | 0.13 | 4 | –0.95[–2.23,0.33] | 0.14 | 5 | –0.41[–0.85,0.03] | 0.07 | 2 | –1.99[–4.93,0.94] | 0.18 |
| Crossover | 1 | –0.79 [–1.98, 0.41] | 0.20 | 1 | –0.11[–1.24,1.02] | 0.85 | 1 | 0.10[–1.04,1.23] | 0.87 | 1 | –091[–2.13,0.30] | 0.14 | |
| Baseline FBG | High (>7.1 mmol/l) | 5 | –0.64[–1.68,0.41] | 0.23 | 3 | –1.19[–2.92,0.55] | 0.18 | 4 | –0.50[–1.02,0.01] | 0.05 | 2 | –1.99[–4.93,0.94] | 0.18 |
| Normal (4–7 mmol/l) | 2 | –0.62[–1.10, –0.15] | 0.01 | 2 | –0.24[–0.70,0.23] | 0.32 | 2 | –0.04[–0.50,0.42] | 0.87 | 1 | –091[–2.13,0.30] | 0.14 | |
| Overall bias | Low risk | 2 | –0.28[–0.95,0.39] | 0.41 | 2 | –0.35[–0.76, 0.06] | 0.09 | 2 | –0.20[–0.60,0.21] | 0.34 | 1 | –0.50[–1.17,0.18] | 0.15 |
| Some concerns | 2 | –0.36[–1.68,0.96] | 0.59 | 1 | –0.16[–0.76,0.43] | 0.59 | 2 | –0.35[–1.50,0.81] | 0.56 | NA | NA | NA | |
| High rick | 3 | –1.13[–2.62,0.36] | 0.14 | 2 | –1.54[–4.26,1.17] | 0.27 | 2 | –0.52[–1.37,0.33] | 0.23 | 2 | –2.26[–4.78,0.27] | 0.08 | |
FBG, fasting blood glucose; FBI, fasting blood insulin; HbA1c, glycated haemoglobin; HOMA-IR, homeostatic model assessment of insulin resistance; NA, not applicable.
4Discussion
This systematic review identified the studies that evaluated the effect of GT and/or cocoa intake on improving glycaemic control and insulin sensitivity in patients with T2DM. To the best of our knowledge, this is the first systematic review and meta-analysis to compare the effects of GT and cocoa consumption on individuals with chronic T2DM for a period of more than four weeks. However, the results of the FBG, FBI, HbA1c, and HOMA-IR analyses showed no significant reduction in T2DM after GT and cocoa consumption. Though extensive studies have been conducted over the past few decades, the efficacy of polyphenols from GT and cocoa on reducing the incidence of complications and improving glycaemic control and insulin sensitivity in adult patients with T2DM has not been well-established. The findings of this systematic review are consistent with the findings of a previous systematic review and meta-analysis regarding the efficacy of polyphenols from GT and cocoa on improving glycaemic control and insulin sensitivity (see, for example, [31, 44], and [47] in green tea, and partially with [10] in cocoa). Though a [10] meta-analysis revealed that cocoa consumption significantly reduced FBG, no significant improvement was found in FBI and HbA1c. In addition, despite the inclusion criterion (studies that examined T2DM outcomes), the review’s strength may be demonstrated in the number of papers it carefully reviewed between 2005 and 2021, including RCTs with either a parallel or crossover design, which were included in this study. According to [3], because of their lower intraparticipant variability, crossover trials are typically considered more robust than parallel trials. After excluding the studies that did not meet the inclusion criteria, fifteen studies on GT and seven on cocoa were included. There were 738 participants (348 male/390 female) in the GT studies and 331 (83 male/ 248 female) in the cocoa studies with T2DM. The GT studies used a dose ranging from 80 to 1200 mg/day of polyphenols for different periods (either 30 days, three months, or≥one year); the cocoa studies used a dose ranging from 16.6 to 850 mg/day of polyphenols for different periods (30 days, two months, three months).
Even among the researchers who advocate polyphenol consumption, the effect of GT and/or cocoa consumption on T2DM remains uncertain. A meta-analysis of seven RCTs by [44] found that GT consumption did not decrease FBG, FBI, HbA1c, or HOMA-IR levels in populations at risk of T2DM. In the results of six RCTs, no evidence was found to support the suggestion that consuming GT/GTE could reduce HbA1c, HOMA-IR, FBG, or FBI levels in adults with prediabetes and T2DM [31]. The meta-analysis indicated that the supplementary intake of GT had no significant effect on FPG, FBI, HbA1c, or HOMA-IR in patients with T2DM [47]. Moreover, the systematic studies and meta-analyses that focused on the link between GT and cocoa intake, insulin resistance, and glycaemic control have produced conflicting results. Another meta-analysis of 22 RCTs revealed that the administration of GT with or without caffeine significantly reduced FBG; still, the results did not reveal a positive effect on FBI, HbA1c, or HOMA-IR in adults with T2DM [45]. In 27 RCTs, short-term GT supplementation significantly reduced FBG but did not significantly affect FBI or HbA1c in T2DM patients [3].
4.1Other factors that may influence the effectiveness of GT and cocoa on glycaemic control and insulin sensitivity
The changes in outcomes might be related to the different types of the population investigated (disease type), the clinical characteristics of patients (the severity of the disease), the type and dose of supplementation, the duration of intervention, and the sample size at the start of the study. Accordingly, several factors could help to show positive effects, including the duration of a diabetes diagnosis. This disparity might be more evident in diabetic patients who had a mean illness duration of approximately seven years. The majority of studies on cocoa reported that the duration of the disease or the time since diagnosis was less than seven years, while some studies on the effect of GT on T2DM reported the duration to be more than 12 years. For example, [70] found that cocoa led to lower levels of FBS and HbA1c compared to the control. However, while these changes were not high rates, they were considered significant compared to the control group. [40] found that GTE supplementation had a superior FBG-reducing impact in individuals with a diabetes history of fewer than five years than in those with a history of more than five years, while reduced insulin and lower HOMA-IR were only significant in people with illness for less than five years. Though a few studies have focused on the severity of T2DM (in terms of disease duration) in relation to the use of GT, the results have been difficult to ascertain. Accordingly, the clinical features of T2DM patients must be investigated in future research with a larger patient sample.
There may be a relationship between the dose amount and the extent of the effect on glycaemic control. However, the amount and type of polyphenols found in published research vary. [54] suggested that larger dosages may be required for diabetic individuals to detect clear results, such as drinking four cups of GT daily (1000 mg of flavanols). The number of polyphenols consumed, and the amount of insulin was also found to have a favourable association [61]. After 16 weeks of 856 mg EGCG, the HbA1c level and HOMA-IR index in the GTE group decreased significantly compared to the placebo group [65]. The GTE group (1344 mg of catechins) demonstrated substantial within-group alterations in the HOMA-IR index after 16 weeks of therapy, despite no significant changes in FBG or HbA1c [40]. [68] observed a significant reduction in HOMA-IR and an improvement in insulin sensitivity following a significant decrease in FBI concentrations within two months associated with 850 mg of flavanols from cocoa. [59] reported that glucose and lipid metabolism was unaffected by the regular consumption of 2.5 g of cocoa (207.5 mg of flavanols) over three months. [69] indicated that cocoa with 450 mg of polyphenols is ineffective in improving the FBG, FBI, and HbA1c levels in diabetic adults compared to WCG. Moreover, [56] demonstrated no significant differences in the intervention group’s FBG, HbA1c, and FBI levels within two months (with 240 mg of flavanols). From these studies it can be deduced that higher doses are more effective for T2DM, although researchers have reported that there were no restrictions on drinking GT in the control group. This could be the main reason for the results of the previous study.
4.2Limitations of the review
This systematic review and meta-analysis have some limitations that must be addressed. First, T2DM is influenced by several variables, including genetic, metabolic, environmental, behavioural, social, and cultural factors, all of which may diminish the link between polyphenol consumption and T2DM outcomes. The selected studies focused on the impact of GT and cocoa on improving glycaemic control and insulin sensitivity in adults who are overweight/obese with T2DM. Therefore, the effectiveness of other sources of polyphenol in patients newly diagnosed with T2DM might not be determined in this review. Furthermore, since the majority of the RCTs selected included short-term interventions (up to 12 weeks), any long-term effects of the intervention were limited to expectations. In addition, this review’s BMI range was 25–34.9 kg/m2, so it was unable to identify the efficacy of GT or chocolate for people with a BMI of≤24 kg/m2. Therefore, the difference may be due to the degree of obesity or disease intensity, which merits further investigation. Consequently, most population groups from Asia and Africa may not have similar results compared to their counterparts in United States and Europe. Many participants (67%) were adult women, which limited the popularisation of the results. Moreover, significant differences in the feeding protocols between RCTs, short follow-up periods, small sample sizes, high dropout rates, the characteristics and number of participants, and the differences in the form of intervention make it difficult to determine which polyphenols are the most effective for T2DM. There is a high degree of heterogeneity between the clinical and methodological RCTs included. For example, there was a substantial variation in macronutrient energy percentages. The probable influence of other lifestyle-related factors, which are not obvious in any of the studies included, is one of the biggest methodological challenges in any nutritional intervention. Nonetheless, the results of this meta-analysis may be limited because of the small number of eligible RCTs. Although a thorough search of the literature was conducted using limited search engines, there was bias in selecting RCTs that fit within the search engines’ limited reach.
Some limitations of the included studies should be considered as well. Most of the studies focused on adults with T2DM aged between 18 and 65; hence, the findings of these studies may not hold for those with different ages and levels of health status and are thus limited in their generalisability. Some of the studies did not use a placebo: seven focused on GT [38, 54, 61, 62, 64, 66, 67], and two focused on cocoa [68, 70]. Consequently, it may be difficult to avoid bias. [66] and [58] identified the significant discrepancies in HbA1c levels (≥9), while all the other studies had discrepancies of≤6, which could affect the validity of the findings. Furthermore, since most studies on cocoa were based on small sample sizes and a minority number of male participants, it was difficult to ensure any impact related to gender. In contrast, the sample size for the GT studies was somewhat acceptable, and the ratio of males to females was equal. However, a large number of dropouts was noted in some studies: exceeding 21% for studies by [67] and [68] and 10% for the study by [66]. Despite these limitations, [68] offered the longest intervention to date for assessing the effects of cocoa flavonoids on patients with T2DM.
Some studies measured dietary intake/adherence using food records [38, 46, 54, 59, 61, 67]. Only a few studies have studied dietary intake, and their outcomes might be incorrect. According to [71] and [72], approximately 30% of overweight people underreport their food intake. Most of the participants were overweight and obese in this review, and a lack of substantial differences between the two groups might be due to the control group’s lack of limits on GT consumption in [61]. Although dietary intake was monitored by a weekly intake questionnaire at each visit, this was not restricted in [60]. Some studies have reported that adherence to dietary restrictions was controlled by investigating nutrition status and nutritional intake, although physical activity was not assessed [38, 46, 54, 59, 61, 67]. Therefore, the research may have been underpowered due to confounding effects from the lifestyle changes that may have altered outcome factors. However, in studies by [58–60, 68, 69], the participants were instructed to maintain a normal diet and engage in regular physical activity. In addition to the long duration, this results in ideal and more realistic situations. [38, 58, 64] were crossover trial studies in which there was more/some concern that individuals might be able to distinguish between the two preparations. In its study design, [69] did not have the possibility of double-blinding, and the participants were aware of the intervention grouping type. For [68] and [69], the amounts of serum polyphenols were not assessed at the start and conclusion, which might have influenced the outcomes in both groups. [60] reported that the diet of all patients was not the same 24 h before each blood sampling; moreover, during the trial, the patient’s sleep, stress, and psychological condition were not examined as factors that could influence the findings. Moreover, some studies did not measure HbA1c and insulin resistance [46, 54–57, 59, 60, 62, 64, 66], which might have led to a less accurate evaluation of the changes in glycaemic control.
5Conclusion
The effect of polyphenol intake in patients with T2DM is still uncertain. This systematic review has attempted to explore this by reviewing several studies. With regard to improving glycaemic control and insulin sensitivity, the evidence shows clearly that the short-term administration of cocoa or GT intake did not significantly reduce the level of FBG, FBI, HbA1c, and HOMA-IR. Overall, diabetes diagnosis should be performed regularly among the population at a high risk of T2DM. Combining increased screening, lifestyle changes, and polyphenols intake alongside anti-diabetic drugs may improve results for adults with T2DM if it is initiated early.
Based on the results of the systematic review, the heterogeneity of the findings of the included studies is attributed to the variability in dose, the severity of the disease, the duration of treatment, and the tools used to diagnose the disease. Consequently, further RCTs should consider larger sample size, dosage, duration or long-term follow-up, the timing of either GT or cocoa, the generalisation of the diet, the severity of the disease, and different methods of assessing the hypotheses to investigate the effect of polyphenols on FBG, especially the long-term effects on FBI, HbA1c, and HOMA-IR.
Acknowledgments
The authors would like to acknowledge Taif University, Saudi Arabia, for its unlimited support.
References
[1] | Pittas AG , Dawson-Hughes B , Sheehan P , Ware JH , Knowler WC , Aroda VR , Brodsky I , Ceglia L , Chadha C , Chatterjee R , Desouza C . Vitamin D supplementation and prevention of type 2 diabetes. New England Journal of Medicine. (2019) ;381: (6):520–30. |
[2] | Cho N , Shaw JE , Karuranga S , Huang Y , da Rocha Fernandes JD , Ohlrogge AW , Malanda B . IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Research and Clinical Practice. (2018) ;138: :271–281. |
[3] | Xu R , Bai Y , Yang K , Chen G . Effects of green tea consumption on glycemic control: a systematic review and meta-analysis of randomized controlled trials. Nutrition & Metabolism. (2020) ;17: (1):1–13. |
[4] | Huyen VTT , Phan DV , Thang P , Hoa NK , Östenson CG Gynostemma pentaphyllum tea improves insulin sensitivity in type 2 diabetic patients. Journal of Nutrition and Metabolism. 2013;2013. |
[5] | Hou LQ , Liu YH , Zhang YY . Garlic intake lowers fasting blood glucose: meta-analysis of randomized controlled trials. Asia Pacific Journal of Clinical Nutrition. (2015) ;24: (4):575–82. |
[6] | Knowler WC , Barrett-Connor E , Fowler SE , Hamman RF , Lachin JM , Walker EA , Nathan DM , Watson PG , Mendoza JT , Smith KA , Caro J Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin; 2002. |
[7] | Diabetes Prevention Program Research GrouReduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. New England Journal of Medicine. (2002) ;346: (6):393–403. |
[8] | Huxley R , Lee CMY , Barzi F , Timmermeister L , Czernichow S , Perkovic V , Grobbee DE , Batty D , Woodward M . Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Archives of Internal Medicine. (2009) ;169: (22):2053–63. |
[9] | Polonsky KS . The past 200 years in diabetes. New England Journal of Medicine. (2012) ;367: (14):1332–40. |
[10] | Darand M , Hajizadeh Oghaz M , Hadi A , Atefi M , Amani R . The effect of cocoa/dark chocolate consumption on lipid profile, glycemia, and blood pressure in diabetic patients: A meta-analysis of observational studies. Phytotherapy Research. (2021) ;35: (10):5487–501. |
[11] | Knekt P , Kumpulainen J , Järvinen R , Rissanen H , Heliövaara M , Reunanen A , Hakulinen T , Aromaa A . Flavonoid intake and risk of chronic diseases. The American Journal of Clinical Nutrition. (2002) ;76: (3):560–8. |
[12] | Hussain T , Tan B , Murtaza G , Liu G , Rahu N , Kalhoro MS , Kalhoro DH , Adebowale TO , Mazhar MU , ur Rehman Z , Martínez Y . Flavonoids and type 2 diabetes: Evidence of efficacy in clinical and animal studies and delivery strategies to enhance their therapeutic efficacy. Pharmacological Research. (2020) ;152: :104629. |
[13] | Cao H , Ou J , Chen L , Zhang Y , Szkudelski T , Delmas D , Daglia M , Xiao J . Dietary polyphenols and type 2 diabetes: Human Study and Clinical Trial. Critical Reviews in Food Science and Nutrition. (2019) ;59: (20):3371–9. |
[14] | Collins QF , Liu HY , Pi J , Liu Z , Quon MJ , Cao W . Epigallocatechin-3-gallate (EGCG), a green tea polyphenol, suppresses hepatic gluconeogenesis through 5′-AMP-activated protein kinase. Journal of Biological Chemistry. (2007) ;282: (41):30143–9. |
[15] | Broadhurst CL , Polansky MM , Anderson RA . Insulin-like biological activity of culinary and medicinal plant aqueous extracts in vitro. Journal of Agricultural and Food Chemistry. (2000) ;48: (3):849–52. |
[16] | Sakurai N , Mochizuki K , Kameji H , Shimada M , Goda T . (-)-Epigallocatechin gallate enhances the expression of genes related to insulin sensitivity and adipocyte differentiation in 3T3-L1 adipocytes at an early stage of differentiation. Nutrition. (2009) ;25: (10):1047–56. |
[17] | Roghani M , Baluchnejadmojarad T . Hypoglycemic and hypolipidemic effect and antioxidant activity of chronic epigallocatechin-gallate in streptozotocin-diabetic rats. Pathophysiology. (2010) ;17: (1):55–9. |
[18] | Manach C , Scalbert A , Morand C , Remásy C , Jimenez L . Polyphenols: food sources and bioavailability. The American Journal of Clinical Nutrition. (2004) ;79: (5):727–47. |
[19] | Spencer JP . Metabolism of tea flavonoids in the gastrointestinal tract. The Journal of Nutrition.. (2003) ;133: (10):3255S–61S. |
[20] | Urpi-Sarda M , Monagas M , Khan N , Lamuela-Raventos RM , Santos-Buelga C , Sacanella E , Castell M , Permanyer J , Andres-Lacueva C . Epicatechin, procyanidins, and phenolic microbial metabolites after cocoa intake in humans and rats. Analytical and Bioanalytical Chemistry. (2009) ;394: (6):1545–56. |
[21] | Stockley C , Teissedre PL , Boban M , Di Lorenzo C , Restani P . Bioavailability of wine-derived phenolic compounds in humans: A review. Food & Function. (2012) ;3: (10):995–1007. |
[22] | Strat KM , Rowley IV TJ , Smithson AT , Tessem JS , Hulver MW , Liu D , Davy BM , Davy KP , Neilson AP . Mechanisms by which cocoa flavanols improve metabolic syndrome and related disorders. The Journal of Nutritional Biochemistry. (2016) ;35: :1–21. |
[23] | Buitrago-Lopez A , Sanderson J , Johnson L , Warnakula S , Wood A , Di Angelantonio E , Franco OH . Chocolate consumption and cardiometabolic disorders: systematic review and meta-analysis. Bmj. (2011) ;343: :d4488. |
[24] | Shrime MG , Bauer SR , McDonald AC , Chowdhury NH , Coltart CE , Ding EL . Flavonoid-rich cocoa consumption affects multiple cardiovascular risk factors in a meta-analysis of short-term studies. The Journal of Nutrition. (2011) ;141: (11):1982–8. |
[25] | Hooper L , Kay C , Abdelhamid A , Kroon PA , Cohn JS , Rimm EB , Cassidy A . Effects of chocolate, cocoa, and flavan-3-ols on cardiovascular health: a systematic review and meta-analysis of randomized trials. The American Journal of Clinical Nutrition. (2012) ;95: (3):740–51. |
[26] | Ellam S , Williamson G . Cocoa and human health. Annual Review of Nutrition. (2013) ;33: :105–28. |
[27] | Zamora-Ros R , Forouhi NG , Sharp SJ , Gonzalez CA , Buijsse B , Guevara M , van der Schouw YT , Amiano P , Boeing H , Bredsdorff L , Fagherazzi G . Dietary intakes of individual flavanols and flavonols are inversely associated with incident type 2 diabetes in European populations. The Journal of Nutrition. (2014) ;144: (3):335–43. |
[28] | Martín MÁ , Ramos S . Health beneficial effects of cocoaphenolic compounds: A mini review. Current Opinion in Food Science. (2017) ;14: :20–25. |
[29] | Vitale M , Masulli M , Rivellese AA , Bonora E , Cappellini F , Nicolucci A , Squatrito S , Antenucci D , Barrea A , Bianchi C , Bianchini F . Dietary intake and major food sources of polyphenols in people with type 2 diabetes: The TOSCA. IT Study. European Journal of Nutrition. (2018) ;57: (2):679–88. |
[30] | Cercato LM , White PA , Nampo FK , Santos MR , Camargo EA . A systematic review of medicinal plants used for weight loss in Brazil: Is there potential for obesity treatment? Journal of Ethnopharmacology. (2015) ;176: :286–96. |
[31] | Yu J , Song P , Perry R , Penfold C , Cooper AR . The effectiveness of green tea or green tea extract on insulin resistance and glycemic control in type 2 diabetes mellitus: a meta-analysis. Diabetes & Metabolism Journal. (2017) ;41: (4):251–62. |
[32] | Alipour M , Malihi R , Hosseini SA , Abbasnezhad A , Ghavami A , Shahmohammadi HA , Ghanavati M . The effects of catechins on related risk factors with type 2 diabetes: a review. Progress in Nutrition. (2018) ;20: (1):12–20. |
[33] | Khan N , Mukhtar H . Tea polyphenols for health promotion. Life Sciences. (2007) ;81: (7):519–33. |
[34] | Katz DL , Doughty K , Ali A . Cocoa and chocolate in human health and disease. Antioxidants & Redox Signaling. (2011) ;15: (10):2779–811. |
[35] | Oba S , Nagata C , Nakamura K , Fujii K , Kawachi T , Takatsuka N , Shimizu H . Consumption of coffee, green tea, oolong tea, black tea, chocolate snacks and the caffeine content in relation to risk of diabetes in Japanese men and women. British Journal of Nutrition. (2010) ;103: (3):453–9. |
[36] | Toolsee NA , Aruoma OI , Gunness TK , Kowlessur S , Dambala V , Murad F , Googoolye K , Daus D , Indelicato J , Rondeau P , Bourdon E Effectiveness of green tea in a randomized human cohort: relevance to diabetes and its complications. BioMed Research International. 2013;2013. |
[37] | Brown AL , Lane J , Coverly J , Stocks J , Jackson S , Stephen A , Bluck L , Coward A , Hendrickx H . Effects of dietary supplementation with the green tea polyphenol epigallocatechin-3-gallate on insulin resistance and associated metabolic risk factors: randomized controlled trial. British Journal of Nutrition. (2008) ;101: (6):886–94. |
[38] | Fukino Y , Ikeda A , Maruyama K , Aoki N , Okubo T , Iso H . Randomized controlled trial for an effect of green tea-extract powder supplementation on glucose abnormalities. European Journal of Clinical Nutrition. (2008) ;62: (8):953–60. |
[39] | Basu A , Du M , Sanchez K , Leyva MJ , Betts NM , Blevins S , Wu M , Aston CE , Lyons TJ . Green tea minimally affects biomarkers of inflammation in obese subjects with metabolic syndrome. Nutrition. (2011) ;27: (2):206–13. |
[40] | Liu CY , Huang CJ , Huang LH , Chen IJ , Chiu JP , Hsu CH . Effects of green tea extract on insulin resistance and glucagon-like peptide 1 in patients with type 2 diabetes and lipid abnormalities: a randomized, double-blinded, and placebo-controlled trial. PLoS One. (2014) ;9: (3):e91163. |
[41] | Belcaro G , Ledda A , Hu S , Cesarone MR , Feragalli B , Dugall M Greenselect phytosome for borderline metabolic syndrome. Evidence-Based Complementary and Alternative Medicine. 2013;2013. |
[42] | Josic J , Olsson AT , Wickeberg J , Lindstedt S , Hlebowicz J . Does green tea affect postprandial glucose, insulin and satiety in healthy subjects: a randomized controlled trial. Nutrition Journal. (2010) ;9: (1):1–8. |
[43] | Igarashi Y , Obara T , Ishikuro M , Matsubara H , Shigihara M , Metoki H , Kikuya M , Sameshima Y , Tachibana H , Maeda-Yamamoto M , Kuriyama S Randomized controlled trial of the effects of consumption of ‘Yabukita’or ‘Benifuuki’encapsulated tea-powder on low-density lipoprotein cholesterol level and body weight. Food & Nutrition Research. 2017. |
[44] | Wang X , Tian J , Jiang J , Li L , Ying X , Tian H , Nie M . Effects of green tea or green tea extract on insulin sensitivity and glycaemic control in populations at risk of type 2 diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. Journal of Human Nutrition and Dietetics. (2014) ;27: (5):501–12. |
[45] | Zheng XX , Xu YL , Li SH , Hui R , Wu YJ , Huang XH . Effects of green tea catechins with or without caffeine on glycemic control in adults: a meta-analysis of randomized controlled trials. The American Journal of Clinical Nutrition. (2013) ;97: (4):750–62. |
[46] | Nagao T , Meguro S , Hase T , Otsuka K , Komikado M , Tokimitsu I , Yamamoto T , Yamamoto K . A catechin-rich beverage improves obesity and blood glucose control in patients with type 2 diabetes. Obesity. (2009) ;17: (2):310–7. |
[47] | Asbaghi O , Fouladvand F , Gonzalez MJ , Ashtary-Larky D , Choghakhori R , Abbasnezhad A . Effect of green tea on glycemic control in patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. (2021) ;15: (1):23–31. |
[48] | Martin MA , Goya L , Ramos S . Protective effects of tea, red wine, and cocoa in diabetes. Evidence from human studies. Food and Chemical Toxicology. (2017) ;109: :302–14. |
[49] | Kord-Varkaneh H , Ghaedi E , Nazary-Vanani A , Mohammadi H , Shab-Bidar S . Does cocoa/dark chocolate supplementation have favorable effect on body weight, body mass index and waist circumference? A systematic review, meta-analysis and dose-response of randomized clinical trials. Critical Reviews in Food Science and Nutrition. (2019) ;59: (15):2349–62. |
[50] | Türközü D , Tek NA . A minireview of effects of green tea on energy expenditure. Critical Reviews in Food Science and Nutrition. (2017) ;57: (2):254–8. |
[51] | Crozier SJ , Preston AG , Hurst JW , Payne MJ , Mann J , Hainly L , Miller DL . Cacao seeds are a. Chemistry Central Journal. (2011) ;5: (1):1–6. |
[52] | Libianto R , Batu D , MacIsaac RJ , Cooper ME , Ekinci EI . Pathophysiological links between diabetes and blood pressure. Canadian Journal of Cardiology. (2018) ;34: (5):585–94. |
[53] | Sterne JA , Savović J , Page MJ , Elbers RG , Blencowe NS , Boutron I , Cates CJ , Cheng HY , Corbett MS , Eldridge SM , Emberson JR RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366. |
[54] | Mousavi A , Vafa M , Neyestani T , Khamseh M , Hoseini F . The effects of green tea consumption on metabolic and anthropometric indices in patients with type 2 diabetes. Journal of Research in Medical Sciences: The Official Journal of Isfahan University of Medical Sciences. (2013) ;18: (12):1080. |
[55] | Lasaite L , Spadiene A , Savickiene N , Skesters A , Silova A . The effect of Ginkgo biloba and Camellia sinensis extracts on psychological state and glycemic control in patients with type 2 diabetes mellitus. Natural Product Communications.. (1934) ;9: (9):1934578X1400900931. |
[56] | Mirzaei K , Hossein-Nezhad A , Karimi M , Hosseinzadeh-Attar MJ , Jafari N , Najmafshar A , Larijani B . Effect of green tea extract on bone turnover markers in type 2 diabetic patients; a double-blind, placebo-controlled clinical trial study. DARU Journal of Pharmaceutical Sciences. (2015) ;(1):38–44. |
[57] | Balzer J , Rassaf T , Heiss C , Kleinbongard P , Lauer T , Merx M , Heussen N , Gross HB , Keen CL , Schroeter H , Kelm M . Sustained benefits in vascular function through flavanol-containing cocoa in medicated diabetic patients: a double-masked, randomized, controlled trial. Journal of the American College of Cardiology. (2008) ;51: (22):2141–9. |
[58] | Mellor DD , Sathyapalan T , Kilpatrick ES , Beckett S , Atkin SL . High-cocoa polyphenol-rich chocolate improves HDL cholesterol in Type 2 diabetes patients. Diabetic Medicine. (2010) ;27: (11):1318–21. |
[59] | Dicks L , Kirch N , Gronwald D , Wernken K , Zimmermann BF , Helfrich HP , Ellinger S . Regular intake of a usual serving size of flavanol-rich cocoa powder does not affect cardiometabolic parameters in stably treated patients with type 2 diabetes and hypertension— A double-blinded, randomized, placebo-controlled trial. Nutrients. (2018) ;10: (10):1435. |
[60] | Fakhari M , Fakhari M , BamBaeichi E . The effects of pilates and flavanol-rich dark chocolate consumption on the total antioxidant capacity, glycemic control and BMI in diabetic females with neuropathy complications. Journal of Bodywork and Movement Therapies. (2021) ;26: :294–9. |
[61] | Fukino Y , Shimbo M , Aoki N , Okubo T , Iso H . Randomized controlled trial for an effect of green tea consumption on insulin resistance and inflammation markers. Journal of Nutritional Science and Vitaminology. (2005) ;51: (5):335–42. |
[62] | Quezada-Fernandez P , Trujillo-Quiros J , Pascoe-Gonzalez S , Trujillo-Rangel WA , Cardona-Müller D , Ramos-Becerra CG , Barocio-Pantoja M , Rodríguez-de la Cerda M , Nerida Sanchez-Rodriguez E , Cardona-Muñóz EG , García-Benavides L . Effect of greentea extract on arterial stiffness, lipid profile and sRAGE inpatients with type 2 diabetes mellitus: a randomised, double-blind,placebo-controlled trial. International Journal of Food Sciences andNutrition. (2019) ;70: (8):977–85. |
[63] | “How to Calculate Standard Deviation of Change in a Data Set?” Cross Validated, stats.stackexchange.com/questions/534180/how-to-calculate-standard-deviation-ofchange-in-a-data-set. Accessed 15 Aug. 2023. |
[64] | Ryu OH , Lee J , Lee KW , Kim HY , Seo JA , Kim SG , Kim NH , Baik SH , Choi DS , Choi KM . Effects of green tea consumption on inflammation, insulin resistance and pulse wave velocity in type 2 diabetes patients. Diabetes Research and Clinical Practice. (2006) ;71: (3):356–8. |
[65] | Hua C , Liao Y , Lin S , Tsai T , Huang C , Chou P . Does supplementation with green tea extract improve insulin resistance in obese type 2 diabetics? A randomized, double-blind, and placebocontrolled clinical trial. Alternative Medicine Review. (2011) ;16: (2):157–63. |
[66] | Borges CM , Papadimitriou A , Duarte DA , de Faria JML , de Faria JBL . The use of green tea polyphenols for treating residual albuminuria in diabetic nephropathy: A double-blind randomised clinical trial. Scientific Reports. (2016) ;6: (1):1–9. |
[67] | Hosseini SA , Alipour M , Zakerkish M , Cheraghian B , Ghandil P . The Gene-Treatment Interaction of FTO-rs9939609 Gene Polymorphism and Epigallocatechin-GallateIntervention on Anthropometric Indices, Fasting Blood Sugar and Insulin Resistance/Sensitivity in Patients with Type 2 Diabetes Mellitus. Iran Red Crescent Med J. (2018) ;20: (12):e82228. |
[68] | Curtis PJ , Sampson M , Potter J , Dhatariya K , Kroon PA , Cassidy A . Chronic ingestion of flavan-3-ols and isoflavones improves insulin sensitivity and lipoprotein status and attenuates estimated 10-year CVD risk in medicated postmenopausal women with type 2 diabetes: a 1-year, double-blind, randomized, controlled trial. Diabetes Care. (2012) ;35: (2):226–32. |
[69] | Rostami A , Khalili M , Haghighat N , Eghtesadi S , Shidfar F , Heidari I , Ebrahimpour-Koujan S , Eghtesadi M . High-cocoa polyphenol-rich chocolate improves blood pressure in patients with diabetes and hypertension. ARYA Atherosclerosis. (2015) ;11: (1):21. |
[70] | Jafarirad S , Ayoobi N , Karandish M , Jalali MT , Haghighizadeh MH , Jahanshahi A Dark chocolate effect on serum adiponectin, biochemical and inflammatory parameters in diabetic patients: A randomized clinical trial. International Journal of Preventive Medicine. 2018;9. |
[71] | Nielsen BM , Nielsen MM , Toubro S , Pedersen O , Astrup A , Sørensen TI , Jess T , Heitmann BL . Past and current body size affect validityof reported energy intake among middle-aged Danish men. The Journalof Nutrition. (2009) ;139: (12):2337–43. |
[72] | Scagliusi FB , Ferriolli E , Pfrimer K , Laureano C , Cunha CSF , Gualano B , Lourenço BH , Lancha AH Jr. Characteristics of womenwho frequently under report their energy intake: a doubly labelledwater study. European Journal of Clinical Nutrition. (2009) ;63: (10):1192. |


