
The association between protein consumption from animal and plant sources with psychological distress in older people in the Mediterranean region
Abstract
BACKGROUND:
The potential for diet to prevent and treat mental health conditions is an exciting area of investigation; however, the impact of different protein sources on mental health outcomes is unclear.
OBJECTIVE:
To evaluate the association between dietary protein intake and psychological distress, in people aged >50 years of age, living in Greece.
METHODS:
A combined data set of older people living in the Athens metropolitan area and 20 Greek islands, from the ATTICA (n = 1,128) and MEDIS (n = 2,221) population-based cross-sectional studies was developed. Anthropometric, clinical and socio-demographic and lifestyle characteristics, and protein consumption (total, animal, plant) consumed based on validated FFQ, were derived through standard procedures and questionnaires. “Psychological distress” (PDS) was assessed as a combined variable representing symptoms of depression and anxiety using Item Response Theory methodology and fitting a Graded Response Model.
RESULTS:
Animal protein, but not plant protein intake, was associated with higher PDS following adjustment for age, sex, education level, Mediterranean diet adherence and physical activity (b±SE: 0.399±0.090, p = 0.003). Following analysis by Mediterranean diet adherence level, among low adherers, animal protein intake was positively associated with PDS (b±SE: 1.119±0.174, p = 0.003), and no associations were observed in moderate or high adherence groupsin regards to plant protein intake and PDS.
CONCLUSIONS:
Animal protein intake is associated with PDS, suggesting a bi-directional relationship, which may be influenced by Mediterranean diet adherence.
1Introduction
Of the large cluster of psychological disorders, depression and anxiety, are the most widely and frequently studied conditions. They have both been linked to the health status and several risk factors predisposing the development of chronic diseases, such as cardiovascular disease (CVD). These conditions are influenced by socioeconomic inequalities and adoption of unhealthy lifestyles [1]. Depression affects over 300 million people worldwide and just under 10% of the global population experience anxiety, posing a considerable financial, economic and health burden on society [2, 3].
Many epidemiological studies and clinical trials have attempted to link psychological factors with morbidity and mortality across a range of health conditions [1, 4]. However, it has long been recognised that the strong interaction between psychological disorders, such as depression and anxiety, arise serious methodological issues (i.e., multicollinearity) that can further complicate the study of their impact on health. An additional layer of complexity in research is that the putative psychological risk factors for physical disease are analysed in most cases by a single psychological construct at a time. This leads to the potential for ignoring clustering of psychosocial risk factors for disease, which may act synergistically or concomitantly. Furthermore, this approach makes it difficult to evaluate and compare the prognostic importance of these different concepts and whether one or more hidden underlying dimensions influence their relationships [5]. As such, there is an increasing interest in the influence of lifestyle, in particular diet and nutrition, to prevent, treat or delay the onset of depression and anxiety.
As part of a relatively new field termed nutritional psychiatry, dietary intake and patterns have emerged as having strong influence on symptoms of depression and anxiety, yet the specific components and the underlying mechanisms are unclear [2]. To date, several dietary nutrients have been investigated for their effects depression and anxiety including B-vitamins [6–8], omega-3-fatty acids [9], and minerals including iron, zinc and selenium [10]. However, despite some benefits of supplementation with individual nutrients, it is now widely recognised that the overall quality of the dietary pattern represents a more robust and substantial influence on overall health [11]. A relatively recent meta-analysis of 21 observational studies has shown dietary patterns high in red and processed meat, refined grains, and low intake of fruits and vegetables are associated with increased risk of depression [12]. Similarly, another meta-analysis recently identified 16 randomised controlled trials (RCTs) of various dietary interventions investigating changes in symptoms of depression and anxiety in 45,826 individuals [2]. The findings indicated reduced depressive symptoms, but not for anxiety, with benefits for both observed in females only. Therefore, diet-disorder relationships may potentially be used as a predictor of chronic disease risk; however, it is exceptionally challenging to interpret underlying mechanisms.
Three studies [13–15] included in the aforementioned meta-analysis [2] incorporated a Mediterranean style diet, with the most recent of these reporting a reduction in depressive symptoms following a twelve-week modified Mediterranean diet compared to social support [14]. The Mediterranean diet is purported to be one of the healthiest dietary patterns, characterised by frequent consumption of fruits, vegetables and spices, olive oil, unrefined grains, seafood, and low to moderate amounts of dairy and meat [16]. Benefits of this dietary pattern are often attributed to large quantities of fresh, high-quality plant-based foods, and a relatively lower amount of animal foods compared to a western dietary pattern. There exists a paradoxical relationship between protein consumption and longevity and morbidity, and protein is essential for the prevention of sarcopenia. Despite this, some of the longest-lived populations consume dietary patterns low in overall protein, suggesting that the quality and bioavailability of the protein is more important than the quantity [17]. Protein can be acquired from a number of different food sources, and its quality is dependent on the amino-acid composition which may represent implications on the psychobiological aspects related to the anxiety and depression.
The effects of animal protein on overall human health remain one of the most controversial issues in nutrition science to date [18]. Moreover, the relationship between animal and plant-based proteins with depression and anxiety is similarly controversial [19]. Therefore, the aim of this study was to investigate the association of dietary animal and plant protein intake on combined depression and anxiety symptomatology (named “psychological distress” (PDS)) and to explore the role of the Mediterranean diet on the tested hypothesis, among older adults from the general population.
2Methodology
2.1Sample
For the purposes of this work, two cross-sectional, population-based, large-scale epidemiologic studies, i.e., the ATTICA [20] and the MEDIS (MEDiterranean Islands Study) [21] conducted in Greece, were combined. The ATTICA study is a population-based, observational survey conducted in Athens greater area, Greece, during 2001–2002, and with a follow-up during 2012. At baseline, all n = 3,042 men and women participants (18+ years) were free of CVD and cancer, as assessed through a detailed clinical evaluation by the study’s physicians. The MEDIS study is a population-based, observational survey that enrolled n = 3,138 older people from 26 Mediterranean islands of 5 countries, during 2005-2017.Individuals who resided in assisted-living centres, had a clinical history of CVD or cancer, or had left the island for a considerable period of time during their life (i.e., >5 years) were excluded from the sampling. From the original sample of the ATTICA and MEDIS studies, a subgroup of n = 1,906 Greek men and women, aged >50 years old with depression and anxiety data were studied for the purposes of the present work. No differences as regards age, gender, CVD risk factor or nutritional profile were observed when the aforementioned sub-group of participants was compared with the entire sample. For both studies, a group of trained health scientists (cardiologists, general practitioners, dietitians, and nurses) collected all information using standard, validated questionnaires and clinical procedures.
2.2Bioethics
The ATTICA study was approved by the Bioethics Committee of Cardiology Department, University of Athens Medical School and was carried out in accordance with the Declaration of Helsinki (1989) of the World Medical Association. The MEDIS study was approved by the Institutional Ethics Board of Harokopio University (16/19-12-2006) and followed the ethical recommendations of the World Medical Association (52nd WMA General Assembly, Edinburgh, Scotland, October 2000). In both studies, participants were informed of the study aims and procedures and provided written informed consent for study participation prior to enrollment.
2.3Measurements
The basic sociodemographic characteristics studied in this work were age (years), gender (male/female) and years of school, while anthropometric characteristics, i.e., weight (kg) was measured using standard procedures.
2.4Dietary habits assessment
In both studies, dietary habits were evaluated based on the participants’ responses on validated semi-quantitative food-frequency questionnaires (FFQ). Among the ATTICA study participants, evaluation of dietary habits was based on a semi-quantitative FFQ, originally developed for the European Prospective Investigation into Cancer and Nutrition (EPIC) study [22]. The Greek version of the EPIC questionnaire was provided by the Unit of Nutrition of University of Athens Medical School, after being translated according to standard literature guidelines. Similar to the ATTICA study, dietary habits in the MEDIS study were assessed through a semi-quantitative, validated, and reproducible FFQ developed for the study [23]. Then, and for both studies, information about dietary habits of the participants was harmonised and recorded as the average intake (“per week” or “per day”) of several food items and beverages (i.e., meat and meat products, fish, milk and other dairy products, fruits, vegetables, greens and salads, legumes, cereals, pasta, olive oil, other added fat) that they have been consuming during the last 12 months. Specifically, information regarding frequency of intake based on “daily”, “weekly” (i.e., 1–2, 3–5 times per week), “monthly” basis (i.e., 2–3 times per month), “rare”, or “never” was collected. Based on food composition tables (USDA), as well as using previously described categorisation’s of protein-containing foods [24], protein intake was grouped into animal- and plant-based sources in the harmonised dataset. Particularly, animal protein intake was measured based on the assessment of the frequency of meat, poultry-, fish-, and dairy- consumption, whereas plant protein intake was assessed based on the frequency of cereal-, potato-, vegetable- and legume consumption. It was not possible to harmonise data relating to nut and seed intake or processed and unprocessed meats.
The Med Diet Score (range 0–55) evaluated the level of adherence to the Mediterranean diet; the higher the score, the greater the adherence to the traditional dietary pattern [25].
2.5Psychological distress evaluation
Depressive symptomatology was assessed using the validated Greek translation of the Zung Self-Rating Depression Scale (ZDRS) for the ATTICA study participants [26]. The time window was the preceding 4-week period before the administration. The ZDRS’ total score range was 20–80; with higher score values indicating more severe depressive symptoms. Depressive symptomatology for the MEDIS study participants was assessed using the validated Greek version of the shortened, self-report Geriatric Depression Scale (GDS) with range 0–20 [27]. For this work, GDS transformed into a score of 20–80 (20: when actual GDS was 0, and 80: when actual GDS score was 20). Anxiety levels were assessed using the validated Greek translation of the State Anxiety subscale of the Spielberger State-Trait Anxiety Inventory (STAI) [28]. The total score of the 20-item STAI ranges from 20 to 80, with higher score values being indicative of more severe anxiety symptoms.
The estimated latent dimension of psychological distress, i.e., the combined measure of depression and anxiety, the Psychological Distress Score (PDS), has been previously presented in detail [29]; it was developed using Item Response Theory (IRT) methodology and fitting a Graded Response Model using the abovementioned psychometric tools. Briefly, for the total of the 40 items of the ZDRS, GDS and STAI scales, exploratory factor analysis was first conducted to ensure unidimensionality. The loadings of the first extracted factor (29 items) were used to estimate the PDS score. The PDS ranges from 0 to 100, with higher values indicating more distress symptoms.
2.6Statistical analysis
Continuous variables are presented as mean±standard deviation, and categorical variables as frequencies. Associations between continuous variables and distress categories were evaluated with analyses of variance (ANOVA), while associations between categorical variables and distress categories were performed using the Chi-squared test. Spearman’s rho correlation coefficient was used to evaluate the relationships between protein intake (total, animal, plant) and psychological distress score. Linear regression analysis was used to assess the association between daily plant or animal protein intake (evaluated as continuous variables, i.e., “g per day”) (independent variables) and the psychological distress score, PDS (outcome), after adjusting for age and sex, years of education and level of adherence to the Mediterranean diet (using the Med Diet Score). The rationale of the models’ selection was: a) at first, to evaluate the association of the type of protein older adults consumed with psychological distress without any covariates (model 1, 1a & 1b), b) to evaluate the aforementioned association, accounting only for age and sex (model 2, 2a & 2b), c) to evaluate the before-mentioned association accounting also for level of education (model 3, 3a & 3b), and then to further evaluate this association with lifestyle factors, i.e., the level of adherence to the Mediterranean diet (model 4, 4a & 4b) and physical activity (model 5, 5a & 5b). Results are presented as unstandardized beta coefficients±standard error and p-value. The linearity of the models’ fitting was tested through scatter plots of standardised residuals against fitted values; normality of regression residuals was evaluated through P-P plots; dependency was tested using Durbin-Watson test and homoscedasticity using the variance inflation index. Stratified analysis by Med Diet Score tertile was also applied, as the interaction term between protein intake-by-Med Diet Score on PDS was significant (p = 0.003). The Locally Weighted Scatterplot Smoothing (LOWESS) was also applied to evaluate the association between animal protein intake (g/day) and standardised predicted value of PDS, as well as the association between plant protein intake (g/day) and standardised predicted value of PDS, among females and males. STATA software version 15 (M. Psarros & Associates, Sparti, Greece) was used for all calculations.
3Results
Various socio-demographic, lifestyle and nutritional characteristics of the ATTICA and MEDIS study participants based on PDS are presented in Table 1. Animal protein was different across PDS tertiles (p = 0.046) and participants with low PDS (i.e., PDS≤13) were more likely to have lower mean protein intake (p < 0.001) compared to those with moderate PDS. Participants with low PDS were also more likely to have higher adherence to the Mediterranean diet (p < 0.001) compared to those with moderate (p = 0.001)or high (p < 0.001) PDS.
Table 1
Socio-demographic, lifestyle and nutritional characteristics of the n = 1,906 participants from the ATTICA and MEDIS epidemiological studies
| Psychological Distress Score (PDS) | |||||
| Overall | Low PDS ≤13 | Moderate PDS 13–34 | High PDS ≥34 | p | |
| N | 1906 | 813 | 442 | 651 | |
| Age (yrs) | 73±9 | 73±7 | 74±9 | 72±12 | 0.001 |
| Male % (n) | 57 (1110) | 60 (488) | 64 (283) | 48 (314) | < 0.001 |
| Ever smokers % yes (n) | 42 (754) | 41 (357) | 45 (217) | 42 (180) | 0.5 2 |
| Physically active % yes (n) | 43 (828) | 42 (384) | 53 (285) | 35 (159) | < 0.001 |
| Years of education | 7.02±4.25 | 7.28±4.08 | 7.82±3.93 | 6.73±3.78 | 0. 17 |
| BMI (kg/m2) | 28.1±4.4 | 28.2±4.4 | 28.3±4.2 | 28.0±4.3 | 0. 59 |
| MedDietScore (0–55) | 32±6 | 33±5 | 31±6 | 30±6 | < 0.001 |
| Energy intake (kcal/day) | 1624±583 | 1646±539 | 1497±562 | 1731±700 | < 0.001 |
| Protein intake (% total energy intake) | 19±4 | 19±3 | 21±4 | 18±3 | < 0.001 |
| Animal Protein (g/day) | 35±6 | 35±5 | 37±5 | 36±5 | 0.046 |
| Plant Protein (g/day) | 41±6 | 42±6 | 42±6 | 41±6 | 0.1 4 |
Values are presented as percent (%) or mean±standard deviation. p: p-values derived from analysis of variance (ANOVA) for continuous variables or the chi-square test for the categorical variables.
A significant positive correlation was observed between total protein intake (grams per day) and PDS (Spearman’s Rho = 0.127, p < 0.001), plant protein intake (grams per day) and PDS (Spearman’s Rho = –0.049, p = 0.04), as well as between animal protein intake (grams per day) and PDS (Spearman’s Rho = 0.052, p = 0.05).To further evaluate the research hypothesis and account for potential confounding factors, multiple linear regression analysis was then applied. The linear regression models (Table 2) revealed that total protein consumption was associated with higher levels of PDS (b±SE: 0.139±0.004, p< 0.001) (Model 1a), as was higher animal protein consumption (b±SE: 0.301±0.182, p = 0.04) (Model 1b), whereas no association was observed between plant protein intake and PDS (p = 0.07) (Model 1c). After adjusting only for age and sex, higher total protein intake was still positively associated with PDS (b±SE: 0.091±0.04, p = 0.02) (Model 1b), as was animal protein intake (b±SE: 0.377±0.178 p = 0.03) (Model 2b),whereas no association was observed with plant protein intake (p = 0.18) (Model 2c). Moreover, accounting for participants’ years of education, i.e., a factor that could help to manage PDS, the aforementioned association concerning animal protein intake and PDS became even more prominent (b±SE: 0.608±0.199, p = 0.002) (Model 3b), but not with plant protein intake (p = 0.09) (Model 3c); however, no association was observed for total protein intake (p = 0.24). After adjustment for age, sex, education level and level of adherence to the Mediterranean diet, animal protein intake was still associated with higher level of PDS and this association was even more eminent (b±SE: 0.608±0.199, p = 0.002), in contrast with plant protein intake which remained non-significant (p = 0.14). Total protein intake was also positively associated with PDS in this model (b±SE: 0.096±0.04 p = 0.022) (Model 3a). Furthermore, when physical activity was included in the models no changes on the effect size of protein intake and PDS level association was observed. Moreover, although, a non-significant interaction was observed between animal (p for interaction = 0.315), plant protein (p for interaction = 0.107) by gender, stratified analysis by gender was performed revealing no differences between gender as regards the effect size associations of protein on PDS (data not presented).
Table 2
Results from linear regression models that evaluated the association between daily animal or plant protein consumption (independent variables) and psychological distress (outcome, PDS), among ATTICA and MEDIS study participants
| B±SE | p | |
| Model 1: Protein (per g/day) | 0.139±0.04 | <0.001 |
| Model 2: Protein (per g/day)* | 0.091±0.04 | 0.02 |
| Model 3: Protein (per g/day)** | 0.051±0.04 | 0.24 |
| Model 4: Protein (per g/day)*** | 0.096±0.04 | 0.022 |
| Model 5: Protein (per g/day)**** | 0.095±0.041 | 0.022 |
| Model 1a: Animal protein (per g/day) | 0.301±0.182 | 0.04 |
| Model 2a: Animal protein (per g/day)* | 0.377±0.178 | 0.03 |
| Model 3a: Animal protein (per g/day)** | 0.479±0.188 | 0.01 |
| Model 4a: Animal protein (per g/day)*** | 0.608±0.199 | 0.002 |
| Model 5a: Animal protein (per g/day)**** | 0.399±0.090 | 0.003 |
| Model 1b: Plant protein (per g/day) | –0.171±0.097 | 0.07 |
| Model 2b: Plant protein (per g/day)* | –0.126±0.096 | 0.18 |
| Model 3b: Plant protein (per g/day)** | –0.170±0.103 | 0.09 |
| Model 4b: Plant protein (per g/day)*** | 0.096±0.118 | 0.41 |
| Model 5b: Plant protein (per g/day)**** | 0.099±0.115 | 0.39 |
B: unstandardized B-coefficient, SE: Standard Error, p: p-value. Adjusted for *age & sex, **age, sex & years of education, ***age, sex, years of education & Med Diet Score, ****age, sex, years of education, Med Diet Score & physical activity.
At this point it should be noted that for the aforementioned analyses, the association between dietary protein intake on PDS was tested; however, the opposite relationship was also evaluated (i.e., psychological disorders status on protein consumption, data not reported), revealing similar findings with PDS symptomatology and animal, but not plant protein, intake level by the participants.
3.1Adherence to Mediterranean diet, protein intake and “Psychological distress”
Further analyses revealed a significant association between Med Diet Score and PDS (Spearman’s Rho = –0.187, p < 0.001). Moreover, a highly significant interaction was observed between protein intake and Med Diet Score on PDS (p < 0.001); thus, stratified analysis based on Med Diet Score tertiles was applied (i.e., Low Med Diet Score i.e., score < 30, Moderate Med Diet Score i.e., score 30–37 and High Med Diet Score i.e., score > 37).
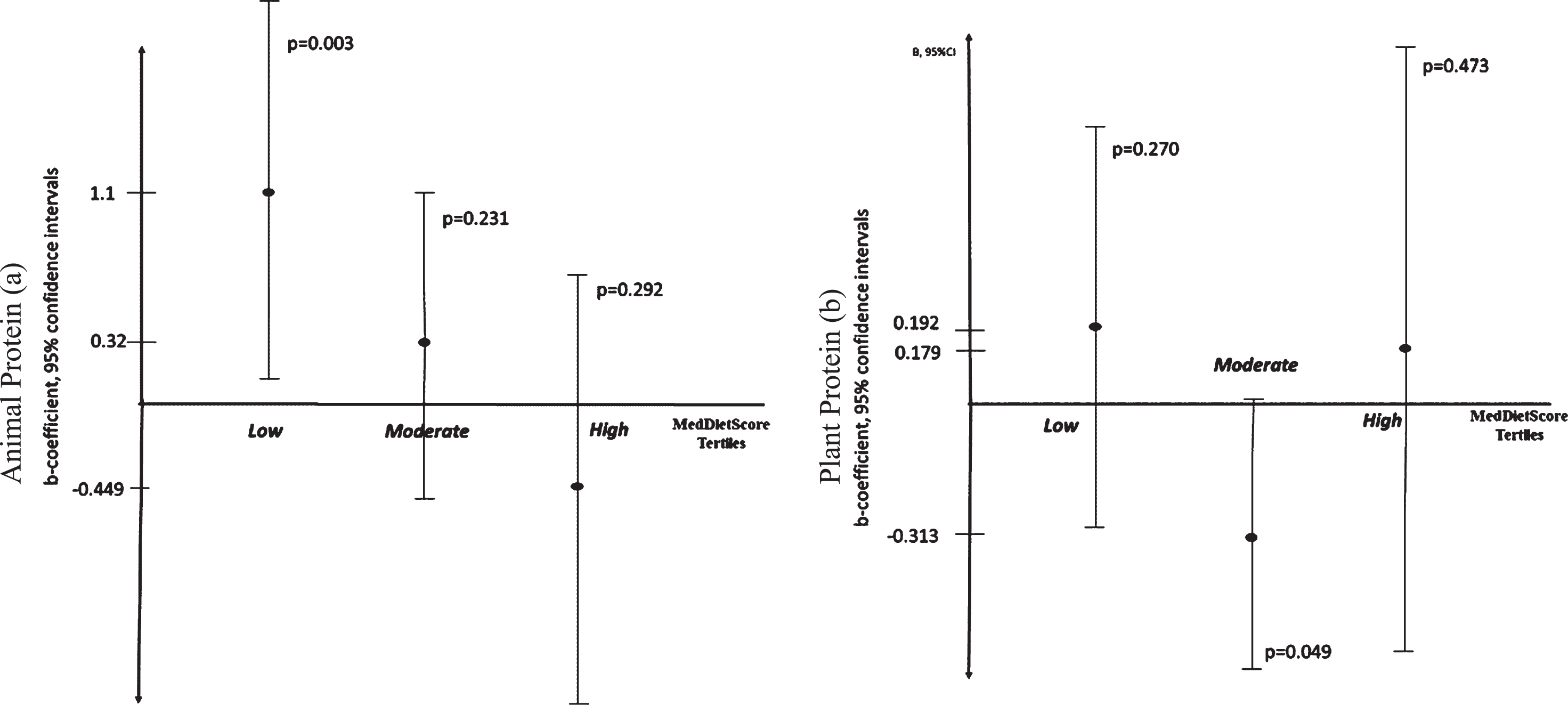
The scatter plots presented in Fig. 1 illustrate the association between animal or plant protein intake and psychological distress among women and men. It was revealed that a quadratic U-shape function better characterised the association between plant protein intake and psychological distress among women (R2 = 0.018) and men (R2 = 0.023). A positive relationship was found between animal protein intake and psychological distress among men (R2 = 0.139) whereas a J-shape association was observed among women (R2 = 0.061), meaning that for women higher animal protein intake was associated with higher psychological distress. As shown in Fig. 2, participants with lower adherence to the Mediterranean diet and higher levels of animal protein intake were associated with higher PDS levels (b±SE: 1.119±0.174, p = 0.003). However, no significant associations were observed for medium or higher Mediterranean diet adherents (all p’s > 0.05). In contrast, participants with moderate adherence to the Mediterranean diet and higher levels of plant protein intake had lower psychological distress levels and vice versa (b±SE: –0.313±0.159, p = 0.04). Still, no significant associations were observed for low or high Mediterranean diet adherents (all p’s > 0.05).
Fig.1
Scatter plots with quadratic lines corresponding to the relationship between a) animal protein intake (g/day) (X-axis) and standardised predicted value of distress (Y-axis) among females, b) animal protein intake (g/day) (X-axis) and standardised predicted value of distress (Y-axis) among males, c) plant protein intake (g/day) (X-axis) and standardized predicted value of distress (Y-axis) among females and, d) plant protein intake (g/day) (X-axis) and standardised predicted value of distress score, PDS (Y-axis) among males.
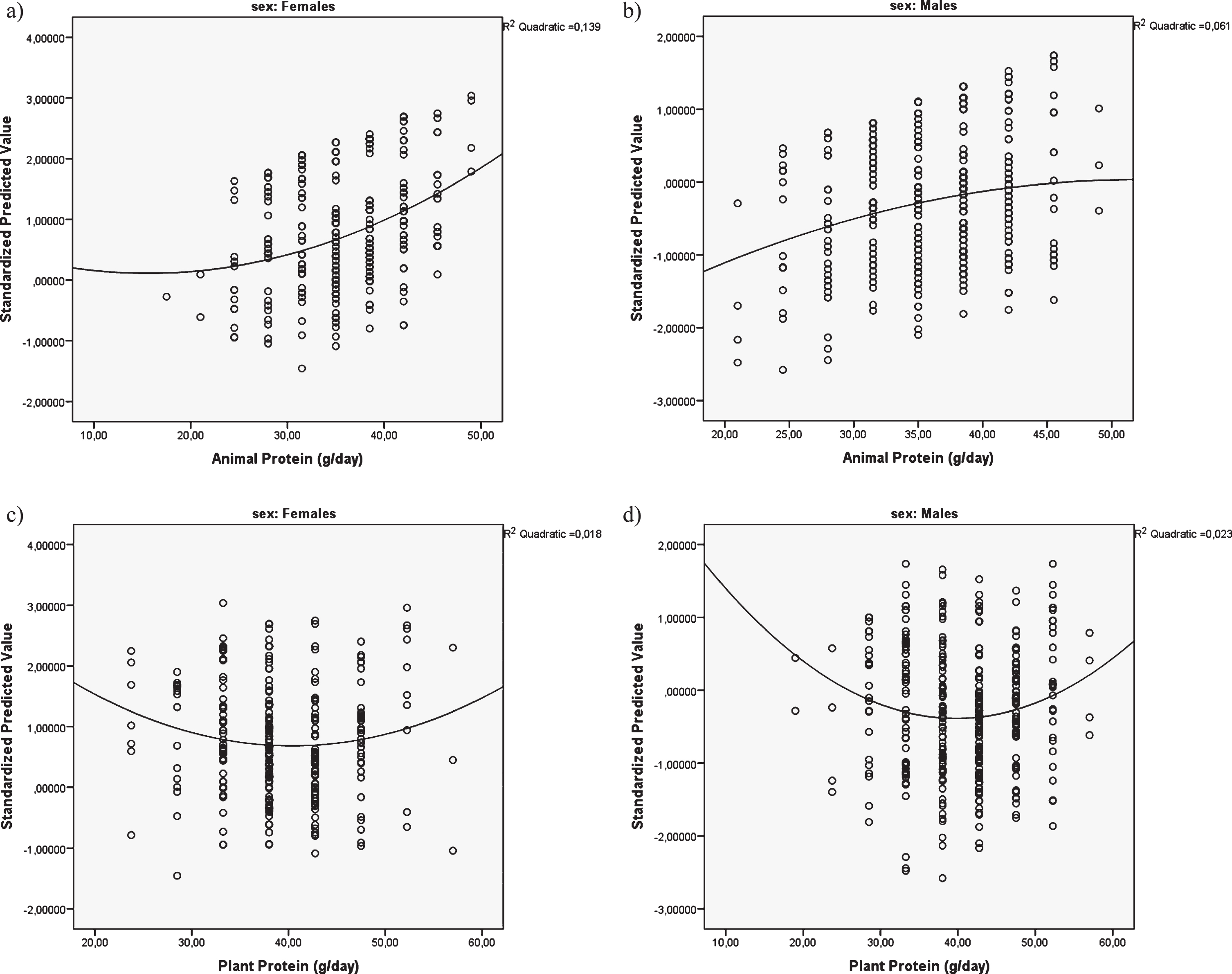
Fig.2
Error-plots illustrating the association of a) animal protein intake (in g/day) on psychological distress (PDS) and b) plant protein intake on psychological distress. Results are from linear regression models and presented by the level of adherence to the Mediterranean diet (i.e., Med Diet Scoretertiles: <30, 30–37, >37), as b-coefficient and 95% confidence interval.
4Discussion
The purpose of the present study was to examine the association between sources of dietary protein intake (total, plant, animal) on PDS, a combined variable of depression and anxiety, and further more to explore the role of the Mediterranean diet in this relationship among older adults living in Greece. Our results indicate protein intake was associated with PDS, and stronger associations were observed for animal compared with plant protein intake. Low adherence to the Mediterranean diet and high animal protein intake was also associated with PDS, and moderate adherence to the Mediterranean diet and high plant protein was associated with lower PDS. Interestingly, the observed findings indicate a potential bi-directional relationship between animal protein and PDS, independently of age, sex, years of education, and physical activity. However, this relationship was not observed with plant protein intake. Taken together, our results further suggest that increased animal protein intake may be moderated by PDS, and this relationship can potentially be influenced by adherence to the Mediterranean diet.
In this sample of adults living in the Mediterranean region, it appears that there is a bi-directional association between animal protein intake and PDS, which is influenced by higher adherence to a Mediterranean diet. Higher PDS was also associated with higher overall energy intake, and protein constituted a lower percentage of overall dietary intake. Therefore, consumption of animal protein may not be driving the increase in PDS as PDS may be seen as one of the reasons for higher consumption of animal protein as part of a poor overall dietary pattern. Several observational studies have indicated that consumption of higher animal protein intake is associated with poorer lifestyle habits (smoking, alcohol, sedentary behaviour) [30–32]. However, the differential effects between intake of animal and plant protein are not well understood and further complicated by studies indicating vegan and vegetarian diets are associated with higher levels of depressive symptoms and mental health disorders [33–35]. The results presented in our study indicate that low to moderate amounts of animal protein as part of a healthy dietary pattern as measured by Mediterranean diet adherence are associated with reduced PDS, showing that animal protein is to be included in an overall healthy dietary pattern.
The beneficial effects of protein consumption vary between age, sex, and physical activity levels, and the quality of protein in the diet. Animal protein represents a complete bio available source of essential amino acids; however, specific processing techniques and cooking methods may result in the production of harmful metabolites which may negate beneficial effects of specific animal protein sources [36]. The methods of preparation and poor-quality animal protein sources are often packaged or consumed with ultra-processed foods which can compound the harmful effects of these metabolites. As such, plant proteins are currently encouraged as an important component of the human diet. Plant proteins also contain fibre and plant bio actives which have beneficial effects on gut health, which is now considered a key modulator for the development and prevention of chronic disease [37]. The Mediterranean diet is regarded as the healthiest dietary pattern and has been shown to have considerable benefits to gut health. In our study, consumption of total protein was associated with PDS, while the fully adjusted model found a positive association between animal protein and PDS, moderate and high adherence to a Mediterranean diet and animal protein was not associated with higher PDS (Fig. 2). Adherence to the Mediterranean diet was negatively associated with PDS and adherence to a Mediterranean style diet, and a healthy overall dietary pattern is associated with lower risk of depression symptoms [38]. Therefore, together, it can be considered that higher animal protein intake, in our results, is an indicator of an unbalanced overall dietary pattern and the high fibre and plant bioactive content of the Mediterranean diet might offset the impact of higher meat consumption on PDS symptoms.
Several clinical trials have found benefits to dietary patterns on psychological well-being while promoting only low to moderate levels of animal protein-containing foods. The findings of the Supporting the Modification of lifestyles in Lowered Emotional States (SMILES) trial, where education was provided to individuals with depression to consume an Australian-modified Mediterranean-style diet, found reduced depressive symptoms after twelve weeks [14]. Similarly, the Med Pork study also improved cognitive function in an Australian sample, promoting inclusion of lean pork as part of a Mediterranean dietary pattern over 24 weeks [39]. The Mediterranean-DASH diet intervention for neurodegenerative delay (MIND) has been shown to reduce risk of cognitive decline recommending moderate meat consumption (2–3 servings/week, up to 2 servings from red meat) [40]. The MIND diet is associated with reduced cognitive decline and depressive symptoms, and this pattern classifies red meat as a food to be restricted [40]. However, the Mediterranean diet on its own may be more potent in the reduction of depressive symptoms [41]. All of these dietary patterns recommend increased intake from plant sources, providing additional fibre and secondary plant metabolites to promote gut health and potentially offset some of the adverse effects of red meat consumption [42, 43]. High red meat intake in the context of a poor dietary pattern is associated with increased circulating inflammatory markers such as C-reactive protein, tumor necrosis factor-a, and interleukin-6, and poorer mental health outcomes [44]. Overall animal protein intake has shown associations with increased adiposity, one of the risk factors for onset of depression and anxiety [45]. However, high protein intake in the context of a diet high in plant foods has shown benefit to promote weight loss with both high- and low-fat diets [46], and when comparing an Atkins diet with other plant-rich diets [47]. The source of the animal protein is also critical, with a stronger association with mortality identified for processed meats [48], but the overall quality of this evidence has come into question [49]. There is also evidence that pescatarian diets are associated with lower mortality compared to vegetarian diets [50]. Therefore, these findings suggest benefits to PDS symptoms from increasing the overall plant intake in the dietary pattern and reducing ultra-processed foods, such as with a Mediterranean style dietary pattern.
Animal protein is associated with benefits due to its nutrient density as it is high in zinc and iron which are both inversely associated with depression [51]. A recent meta-analysis of 36 randomised controlled trials found no difference between red meat and a range of comparator diets across a range of CVD risk factors and saw small decreases in triglycerides with red meat consumption [52]. However, high-quality plant protein sources provided greater benefit in reduction of total and low-density lipoprotein (LDL) cholesterol, but not with fish and low-quality carbohydrate sources. A clinical trial investigating CVD risk factors found higher LDL cholesterol with red or white meat consumption compared with nonmeat protein diets, independently of saturated fat content but this was due to an increase in large LDL particles [53]. Several large cohort studies have evaluated the relationship between animal and plant protein and a range of health outcomes. In Japan, higher intake of plant-based proteins, but not animal protein, was associated with lower total mortality [54]. The UK Bio bank cohort found people with no or low red meat intake were slightly more likely to be anaemic and had lower haemoglobin concentrations [55], while in the EPIC cohort, red and processed meat was positively associated with risk for ischemic heart disease [56]. Psychological distress can potentially be prevented through factors other than diet such as physical activity and exercise as these two factors possess anti-depressive effects through both biological and psychosocial mechanisms [57], and the combined effects of exercise and the type of protein in the diet warrant further investigation. These conflicting results are aligned with the difficulty in making specific dietary recommendations for all people and suggest diet quality and nutrient density should be central to dietary recommendations.
Several potential mechanisms of action may be contributing to the association between animal and plant protein intake and PDS, including the overall inflammatory load of the diet and effects on the gut microbiota. Western-style diets high in animal protein are associated with increased risk of depression, while healthier dietary patterns high in fibre from fruit, vegetables and whole grains can be protective [12]. Typically, western-style diets increase production of inflammatory cytokines, and risk of cardiovascular and neurological conditions [12, 44]. Plant-based proteins possess a cluster of nutrients which are anti-inflammatory, promote gut health, and are neuroprotective, including a range vitamins, minerals, plant bio actives including polyphenols, and fibre [2, 58]. Animal proteins may displace plant foods in the diet, and when combined with processed foods can lead to poorer gut health [59]. In recent years, high trimethylamine n-oxide (TMAO) has been reported as a microbial metabolite associated with cardiovascular disease and brain health in meat-eaters [60]. However, as fish and some fruits and vegetables also increase TMAO levels, this relationship remains controversial, and it is the overall inflammatory load of the diet that is considered to contribute to its effects [61]. In addition, vegans and vegetarians have been found to have higher levels of antioxidants in the blood which are associated with lower risk of depression [62]. However, a poorly balanced diet in vegans and vegetarians can lead to lower nutritional status compared with omnivores [62]. Moreover, creatine, found in animal foods or supplement form, is considered as a potential antidepressant [63]. The relationship between animal and plant-based protein sources is complex, and measurement of inflammatory biomarkers and sampling of the gut microbiota in omnivores and vegans and vegetarians in large cohorts will strengthen future research findings observing differences between protein sources. In addition, extensive studies including plasma or urine biomarkers of amino acid sufficiency, are required to further understand how crucial plant-based protein sources are to diet quality [58].
To the best of our knowledge, this is one of the first studies to evaluate the effects of different sources of protein intake (total, animal, plant) and PDS in older people living in the Mediterranean region. A strength of the study is the combination of data from two large-scale population-based studies to minimise the effects of population bias and to augment the external validity of the findings. However, several limitations must be noted. The cross-sectional analysis does not enable the establishment of any causal association between animal protein and PDS symptoms, and we have posited the strong possibility of a reverse association. Presence of PDS symptoms is likely due to high consumption of low-quality meat sources in combination with ultra-processed foods in addition to other lifestyle factors which may accentuate the impact of animal protein [64, 65]. The use of an FFQ to examine animal and plant protein may over- or under-estimate overall dietary intake, and our analysis did not distinguish between unprocessed and processed meat sources, nor did it include plant protein sources from nuts and seeds which are health-promoting. Food Frequency Questionnaires are widely used in epidemiological research as they are cost-effective and time-saving, but are prone to under- or over-reporting bias [66]. Future studies of this kind should use new technologies which incorporate mobile phone applications and photographs, and machine learning approaches which transfer data to researchers in real-time [66]. Nevertheless, this is one of the first studies to investigate the effects of protein intake on combined depression and anxiety symptomology, and we provide evidence of the existence of non-linear trends between Mediterranean diet adherence, protein sources, and PDS which are sex-specific. Although this work can be seen as exploratory and hypothesis-generating, it is intended to expand on current evidence for an interaction between recommendations on healthy dietary patterns and mental health. Relative to PDS, future studies are required to evaluate animal protein quality and amino acid content of plant-based diets across a diverse range of population samples.
5Conclusion
The field of nutritional psychiatry is an emerging field beginning to untangle the relationship between diet and mental health conditions such as depression and anxiety. Concurrently, the limited effects of specific micronutrient supplementation to treat these conditions have led to a focus on the entire dietary pattern as a way to promote psychological well-being. The present study suggests that plant protein sources form an important part of the overall dietary pattern and that low to moderate red meat intake within a Mediterranean diet pattern may be associated with lower PDS. Similarly, PDS may be contributing to higher consumption of animal protein. Further research is needed to ascertain the interactions between PDS and other lifestyle factors which contribute to PDS and low adherence to healthy dietary patterns.
Funding
The ATTICA study is supported by research grants from the Hellenic Cardiology Society (HCS2002) and the Hellenic Atherosclerosis Society (HAS2003). The MEDIS study was funded by Research grants from the Hellenic Heart Foundation, the Graduate Program of the Department of Nutrition & Dietetics, Harokopio University and the Rutgers University, NJ, USA (GA #5884). Stefanos Tyrovolas was supported by the Foundation for Education and European Culture (IPEP), the Sara Borrell postdoctoral program (reference no. CD15/00019 from the Instituto de Salud Carlos III (ISCIII - Spain) and the Fondos Europeo de Desarrollo Regional (FEDER). Demosthenes Panagiotakos, Stefano Tyrovolas and Alexandra Foscolou have been funded for ATHLOS project to study trajectories of healthy aging (European Union’s Horizon 2020 research and innovation program, grant agreement No 635316).
ACKNOWLEDGMENTS
Authors are particularly grateful to the men and women from all areas that participated in the ATTICA and MEDIS studies, as well as to both studies investigators.
REFERENCES
[1] | Firth J , Siddiqi N , Koyanagi A , Siskind D , Rosenbaum S , Galletly C , et al. The Lancet Psychiatry Commission: a blueprint for protecting physical health in people with mental illness. The Lancet Psychiatry. (2019) . |
[2] | Firth J , Marx W , Dash S , Carney R , Teasdale SB , Solmi M , et al. The Effects of Dietary Improvement on Symptoms of Depression and Anxiety: A Meta-Analysis of Randomized Controlled Trials. Psychosomatic medicine. (2019) ;81: (3):265–80. |
[3] | World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva; 2017. |
[4] | Machado MO , Veronese N , Sanches M , Stubbs B , Koyanagi A , Thompson T , et al. The association of depression and all-cause and cause-specific mortality: an umbrella review of systematic reviews and meta-analyses. BMC Med. (2018) ;16: (1):112. |
[5] | Frasure-Smith N , Lesperance F . Depression and other psychological risks following myocardial infarction. Arch Gen Psychiatry. (2003) ;60: (6):627–36. |
[6] | Naumovski N , Veysey M , Ng X , Boyd L , Dufficy L , Blades B , et al. The folic acid endophenotype and depression in an elderly population. J Nutr Health Aging. (2010) ;14: (10):829–33. |
[7] | Ng X , Boyd L , Dufficy L , Naumovski N , Blades B , Travers C , et al. Folate nutritional genetics and risk for hypertension in an elderly population sample. J Nutrigenet Nutrigenomics. (2009) ;2: (1):1–8. |
[8] | Barnett H , D’Cunha NM , Kellett J , Mellor DD , McKune AJ , Naumovski N . Effect of Folate Supplementation on Inflammatory Markers in Individuals Susceptible to Depression: A Systematic Review. Explor Res Hypothesis Med. (2017) ;2: (4):86. |
[9] | Su K-P , Tseng P-T , Lin P-Y , Okubo R , Chen T-Y , Chen Y-W , et al. Association of Use of Omega-3 Polyunsaturated Fatty Acids With Changes in Severity of Anxiety Symptoms: A Systematic Review and Meta-analysis. JAMA Network Open. (2018) ;1: (5):e182327-e. |
[10] | Li Z , Wang W , Xin X , Song X , Zhang D . Association of total zinc, iron, copper and selenium intakes with depression in the US adults. J Affect Disorders. (2018) ;228: :68–74. |
[11] | Opie RS , Itsiopoulos C , Parletta N , Sanchez-Villegas A , Akbaraly TN , Ruusunen A , et al. Dietary recommendations for the prevention of depression. Nutr Neurosci. (2017) ;20: (3):161–71. |
[12] | Li Y , Lv M-R , Wei Y-J , Sun L , Zhang J-X , Zhang H-G , et al. Dietary patterns and depression risk: A meta-analysis. Psychiatry Res. (2017) ;253: :373–82. |
[13] | Hyyppa MT , Kronholm E , Virtanen A , Leino A , Jula A . Does simvastatin affect mood and steroid hormone levels in hypercholesterolemic men? A randomized double-blind trial. Psychoneuroendocrinology. (2003) ;28: (2):181–94. |
[14] | Jacka FN , O’Neil A , Opie R , Itsiopoulos C , Cotton S , Mohebbi M , et al. A randomised controlled trial of dietary improvement for adults with major depression (the ‘SMILES’ trial). BMC Med. (2017) ;15: (1):23. |
[15] | Wardle J , Rogers P , Judd P , Taylor MA , Rapoport L , Green M , et al. Randomized trial of the effects of cholesterol-lowering dietary treatment on psychological function. Am J Med. (2000) ;108: (7):547–53. |
[16] | Forsyth C , Kouvari M , D’Cunha NM , Georgousopoulou EN , Panagiotakos DB , Mellor DD , et al. The effects of the Mediterranean diet on rheumatoid arthritis prevention and treatment: a systematic review of human prospective studies. Rheumatol Int. (2018) ;38: (5):737–47. |
[17] | Kitada M , Ogura Y , Monno I , Koya D . The impact of dietary protein intake on longevity and metabolic health. EBioMedicine. (2019) ;43: :632–40. |
[18] | Johnston BC , Zeraatkar D , Han MA , Vernooij RWM , Valli C , El Dib R , et al. Unprocessed Red Meat and Processed Meat Consumption: Dietary Guideline Recommendations From the Nutritional Recommendations (NutriRECS) Consortium. Ann of Intern Med. (2019) . |
[19] | Rosenfeld DL . The psychology of vegetarianism: Recent advances and future directions. Appetite. (2018) ;131: :125–38. |
[20] | Panagiotakos DB , Georgousopoulou EN , Pitsavos C , Chrysohoou C , Metaxa V , Georgiopoulos GA , et al. Ten-year (2002-2012) cardiovascular disease incidence and all-cause mortality, in urban Greek population: the ATTICA Study. Int J Cardiol. (2015) ;180: :178–84. |
[21] | Tyrovolas S , Haro JM , Mariolis A , Piscopo S , Valacchi G , Tsakountakis N , et al. Successful aging, dietary habits and health status of elderly individuals: a k-dimensional approach within the multi-national MEDIS study. Exp Gerontol. (2014) ;60: :57–63. |
[22] | Katsouyanni K , Rimm EB , Gnardellis C , Trichopoulos D , Polychronopoulos E , Trichopoulou A . Reproducibility and relative validity of an extensive semi-quantitative food frequency questionnaire using dietary records and biochemical markers among Greek schoolteachers. Int J Epidemiol. (1997) ;26 Suppl 1: :S118–27. |
[23] | Tyrovolas S , Pounis G , Bountziouka V , Polychronopoulos E , Panagiotakos DB . Repeatability and validation of a short, semi-quantitative food frequency questionnaire designed for older adults living in Mediterranean areas: the MEDIS-FFQ. J Nutr Elder. (2010) ;29: (3):311–24. |
[24] | Song M , Fung TT , Hu FB , Willett WC , Longo VD , Chan AT , et al. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific MortalityAssociation of Protein Intake With MortalityAssociation of Protein Intake With Mortality. JAMA Intern Med. (2016) ;176: (10):1453–63. |
[25] | Panagiotakos DB , Pitsavos C , Stefanadis C . Dietary patterns: a Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr Metab Cardiovasc Dis. (2006) ;16: (8):559–68. |
[26] | Fountoulakis KN , lacovides A , Samolis S , Kleanthous S , Kaprinis SG , Kaprinis GS , et al. Reliability, validity and psychometric properties of the Greek translation of the zung depression rating scale. BMC Psychiatry. (2001) ;1: (1):6. |
[27] | Fountoulakis KN , Tsolaki M , Iacovides A , Yesavage J , O’Hara R , Kazis A , et al. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging Clin Exp Res. (1999) ;11: (6):367–72. |
[28] | Fountoulakis KN , Papadopoulou M , Kleanthous S , Papadopoulou A , Bizeli V , Nimatoudis I , et al. Reliability and psychometric properties of the Greek translation of the State-Trait Anxiety Inventory form Y: preliminary data. Ann Gen Psychiatry. (2006) ;5: :2. |
[29] | Kollia N , Panagiotakos D , Georgousopoulou E , Chrysohoou C , Yannakoulia M , Stefanadis C , et al. Exploring the path between depression, anxiety and 10-year cardiovascular disease incidence, among apparently healthy Greek middle-aged adults: The ATTICA study. Maturitas. (2017) ;106: :73–9. |
[30] | Foster HME , Celis-Morales CA , Nicholl BI , Petermann-Rocha F , Pell JP , Gill JMR , et al. The effect of socioeconomic deprivation on the association between an extended measurement of unhealthy lifestyle factors and health outcomes: a prospective analysis of the UK Biobank cohort. Lancet Public Health. (2018) ;3: (12):e576–e85. |
[31] | Key TJ , Appleby PN , Davey GK , Allen NE , Spencer EA , Travis RC . Mortality in British vegetarians: review and preliminary results from EPIC-Oxford. Am J Clin Nutr. (2003) ;78: (3):533S–8S. |
[32] | Zeraatkar D , Han MA , Guyatt GH , Vernooij RWM , El Dib R , Cheung K , et al. Red and Processed Meat Consumption and Risk for All-Cause Mortality and Cardiometabolic Outcomes: A Systematic Review and Meta-analysis of Cohort Studies. Ann Intern Med. (2019) . |
[33] | Burkert NT , Muckenhuber J , Großschädl F , Rásky é , Freidl W . Nutrition and Health – The Association between Eating Behavior and Various Health Parameters: A Matched Sample Study. PLoS One. (2014) ;9: (2):e88278. |
[34] | Matta J , Czernichow S , Kesse-Guyot E , Hoertel N , Limosin F , Goldberg M , et al. Depressive Symptoms and Vegetarian Diets: Results from the Constances Cohort. Nutrients. (2018) ;10: (11):1695. |
[35] | Michalak J , Zhang XC , Jacobi F . Vegetarian diet and mental disorders: results from a representative community survey. IntJ Behav Nutr Phy. (2012) ;9: (1):67. |
[36] | Kouvari M , Tyrovolas S , Panagiotakos DB . Red meat consumption and healthy ageing: A review. Maturitas. (2016) ;84: :17–24. |
[37] | Hills RD Jr , PontefractBA, MishconHR, BlackCA, SuttonSC, ThebergeCR. Gut Microbiome: Profound Implications for Diet and Disease. Nutrients. (2019) ;11: (7). |
[38] | Molendijk M , Molero P , Ortuño Sánchez-Pedreño F , Van der Does W , Angel Martínez-González M . Diet quality and depression risk: A systematic review and dose-response meta-analysis of prospective studies. JAffect Disorders. (2018) ;226: :346–54. |
[39] | Wade AT , Davis CR , Dyer KA , Hodgson JM , Woodman RJ , Keage HAD , et al. A Mediterranean Diet with Fresh, Lean Pork Improves Processing Speed and Mood: Cognitive Findings from the MedPork Randomised Controlled Trial. Nutrients. (2019) ;11: (7):1521. |
[40] | van den Brink AC , Brouwer-Brolsma EM , Berendsen AAM , van de Rest O . The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease—A Review. AdvNutr. (2019) . |
[41] | Fresan U , Bes-Rastrollo M , Segovia-Siapco G , Sanchez-Villegas A , Lahortiga F , de la Rosa PA , et al. Does the MIND diet decrease depression risk? A comparison with Mediterranean diet in the SUN cohort. Eur J Nutr. (2019) ;58: (3):1271–82. |
[42] | Feng Q , Liang S , Jia H , Stadlmayr A , Tang L , Lan Z , et al. Gut microbiome development along the colorectal adenoma–carcinoma sequence. Nat Commun. (2015) ;6: (1):6528. |
[43] | Makki K , Deehan EC , Walter J , Bäckhed F . The Impact of Dietary Fiber on Gut Microbiota in Host Health and Disease. Cell Host Microbe. (2018) ;23: (6):705–15. |
[44] | Chai W , Morimoto Y , Cooney RV , Franke AA , Shvetsov YB , Le Marchand L , et al. Dietary Red and Processed Meat Intake and Markers of Adiposity and Inflammation: The Multiethnic Cohort Study. J Am Coll Nutr. (2017) ;36: (5):378–85. |
[45] | Samaan Z , Lee YK , Gerstein HC , Engert JC , Bosch J , Mohan V , et al. Obesity genes and risk of major depressive disorder in a multiethnic population: a cross-sectional study. J Clin Psychiatry. (2015) ;76: (12):e1611–8. |
[46] | Gardner CD , Trepanowski JF , Del Gobbo LC , Hauser ME , Rigdon J , Ioannidis JPA , et al. Effect of Low-Fat vs Low-Carbohydrate Diet on 12-Month Weight Loss in Overweight Adults and the Association With Genotype Pattern or Insulin Secretion: The DIETFITS Randomized Clinical Trial. JAMA. (2018) ;319: (7):667–79. |
[47] | Gardner CD , Kiazand A , Alhassan S , Kim S , Stafford RS , Balise RR , et al. Comparison of the Atkins, Zone, Ornish, and LEARN diets for change in weight and related risk factors among overweight premenopausal women: the A TO Z Weight Loss Study: a randomized trial. JAMA. (2007) ;297: (9):969–77. |
[48] | Zheng Y , Li Y , Satija A , Pan A , Sotos-Prieto M , Rimm E , et al. Association of changes in red meat consumption with total and cause specific mortality among US women and men: two prospective cohort studies. BMJ. (2019) ;365: :l2110. |
[49] | Händel MN , Cardoso I , Rasmussen KM , Rohde JF , Jacobsen R , Nielsen SM , et al. Processed meat intake and chronic disease morbidity and mortality: An overview of systematic reviews and meta-analyses. PLoS One. (2019) ;14: (10):e0223883. |
[50] | Orlich MJ , Singh PN , Sabaté J , Jaceldo-Siegl K , Fan J , Knutsen S , et al. Vegetarian dietary patterns and mortality in Adventist Health Study 2. JAMA InternMed. (2013) ;173: (13):1230–8. |
[51] | Li Z , Li B , Song X , Zhang D . Dietary zinc and iron intake and risk of depression: A meta-analysis. Psychiatry Res. (2017) ;251: :41–7. |
[52] | Guasch-Ferre M , Satija A , Blondin SA , Janiszewski M , Emlen E , O’Connor LE , et al. Meta-Analysis of Randomized Controlled Trials of Red Meat Consumption in Comparison With Various Comparison Diets on Cardiovascular Risk Factors. Circulation. (2019) ;139: (15):1828–45. |
[53] | Bergeron N , Chiu S , Williams PT , M King S , Krauss RM . Effects of red meat, white meat, and nonmeat protein sources on atherogenic lipoprotein measures in the context of low compared with high saturated fat intake: a randomized controlled trial. Am J Clin Nutr. (2019) ;110: (1):24–33. |
[54] | Budhathoki S , Sawada N , Iwasaki M , Yamaji T , Goto A , Kotemori A , et al. Association of Animal and Plant Protein Intake With All-Cause and Cause-Specific Mortality. JAMA Intern Med. (2019) . |
[55] | Tong TYN , Key TJ , Gaitskell K , Green TJ , Guo W , Sanders TA , et al. Hematological parameters and prevalence of anemia in white and British Indian vegetarians and nonvegetarians in the UK Biobank. Am J Clin Nutr. (2019) ;110: (2):461–72. |
[56] | Key Timothy J , Appleby Paul N , Bradbury Kathryn E , Sweeting M , Wood A , Johansson I , et al. Consumption of Meat, Fish, Dairy Products, and Eggs and Risk of Ischemic Heart Disease. Circulation. (2019) ;139: (25):2835–45. |
[57] | Kandola A , Ashdown-Franks G , Hendrikse J , Sabiston CM , Stubbs B . Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. NeurosciBiobehav Rev. (2019) . |
[58] | Mariotti F , Gardner DC . Dietary Protein and Amino Acids in Vegetarian Diets—A Review. Nutrients. (2019) ;11: (11). |
[59] | Partula V , Mondot S , Torres MJ , Kesse-Guyot E , Deschasaux M , Assmann K , et al. Associations between usual diet and gut microbiota composition: results from the Milieu Intérieur cross-sectional study. Am J Clin Nutr. (2019) ;109: (5):1472–83. |
[60] | Tomova A , Bukovsky I , Rembert E , Yonas W , Alwarith J , Barnard ND , et al. The Effects of Vegetarian and Vegan Diets on Gut Microbiota. Front Nutr. (2019) ;6: (47). |
[61] | Janeiro HM , Ramírez JM , Milagro IF , Martínez AJ , Solas M . Implication of Trimethylamine N-Oxide (TMAO) in Disease: Potential Biomarker or New Therapeutic Target. Nutrients. (2018) ;10: (10). |
[62] | Gajski G , Gerić M , Vučić Lovrenčić M , Božičević S , Rubelj I , Nanić L , et al. Analysis of health-related biomarkers between vegetarians and non-vegetarians: A multi-biomarker approach. J Func Foods. (2018) ;48: :643–53. |
[63] | Kious MB , Kondo GD , Renshaw FP . Creatine for the Treatment of Depression. Biomolecules. (2019) ;9: (9). |
[64] | Gomez-Donoso C , Sanchez-Villegas A , Martinez-Gonzalez MA , Gea A , Mendonca RD , Lahortiga-Ramos F , et al. Ultra-processed food consumption and the incidence of depression in a Mediterranean cohort: the SUN Project. Euro JNutr. (2019) . |
[65] | Machado PP , Steele EM , Levy RB , Sui Z , Rangan A , Woods J , et al. Ultra-processed foods and recommended intake levels of nutrients linked to non-communicable diseases in Australia: evidence from a nationally representative cross-sectional study. BMJ Open. (2019) ;9: (8):e029544. |
[66] | Shim J-S , Oh K , Kim HC . Dietary assessment methods in epidemiologic studies. Epidemiol Health. (2014) ;36: :e2014009-e. |


