
Effect of lower limb resistance exercise with abdominal draw-in on stroke survivors: A pilot study
Abstract
BACKGROUND:
Evidence-based guidelines are needed to inform rehabilitation practice including the effect of non-paralytic lower limb resistance exercise with abdominal drawing-in technique (ADIM) on recovery of trunk control, balance and daily living after stroke survivors.
OBJECTIVE:
The purpose of this study was to compare the effects of trunk control strengthening performed in non-paralytic lower limb resistance exercise with ADIM on trunk control, balance, daily living in stroke survivors.
METHODS:
The 24 participants with stroke were randomly divided into three groups: lower limb resistance exercise group (LRAG; n = 8), lower limb exercise group (LAG; n = 8), and control group (CG; n = 8). The training sessions were conducted three times a week for four weeks. Outcome measures included the Korean version Trunk Impairment Scale (K-TIS), Postural Assessment Scale of Stroke (PASS), Modified Functional Reach Test (mFRT), Berg Balance Scale (BBS), Foot print and Modified Barthel’s Index (MBI).
RESULTS:
The results showed that the LRAG had a significant effect on the K-TIS, PASS, mFRT, Foot print and MBI than the LAG and CG (p < 0.05). The BBS results showed a significant difference the CG (p < 0.05).
CONCLUSION:
This study showed that repeated non-paralytic lower limb resistance exercises with ADIM can be used clinically as a training method for general physiotherapy in patients with reduced postural control, balance and daily living.
1Introduction
Stroke survivors experience balance impairments due to hemiparesis and trunk muscle weakness, which decrease stability for movement (Lattouf et al., 2021). For these reasons, most stroke survivors have balance disorders, and trunk control training is conducted for sensory re-education and to address imbalance and limited functional recovery in the trunk, arms, and legs (Lee et al., 2020).
Trunk muscle weakening leads to less control over the lower back, highlighting the importance of early exercises targeting these muscles in the rehabilitation process for stroke survivors (Hodges, 2005). If the trunk muscles are not strengthened, abnormal contractions of the arm and leg muscles due to trunk muscle weakness can lead to spinal deformities and excessive stress on the soft tissues. This can greatly reduce posture control, balance, and daily life abilities (Choi & Jung, 2017), increasing the risk of falls and further impairing daily life functioning (Haruyama et al., 2017).
Many exercises have been studied for trunk muscle strengthening (Smrcina et al., 2022). The abdominal drawing-in maneuver technique (ADIM) is being applied to improve and strengthen the contraction time of the transverse abdominal and internal oblique muscles, promoting trunk stabilization through anticipatory postural adjustments, and reducing anterior pelvic tilt and lumbar lordosis, aiming to enhance trunk muscle strength and postural control in patients with stroke (Macedo, 2009). Combining the ADIM with various exercises may not only result in greater improvement in trunk control ability (Rasheed et al., 2021), it can induce forced pelvic movements if accompanied by lower limb movements, resulting in increased activation of trunk muscles (Yoder et al., 2019). Leg lifting exercises have been shown to have a positive effect on strengthening the rectus abdominis and external oblique muscles due to the distant movement (Cheon et al., 2020). Moreover, the surrounding muscles around the abdomen automatically contract efficiently in response to pelvic movements, improving trunk control and enhancing daily life abilities (Dubey et al., 2018). Leg lifting exercises can induce automatic weight-bearing on the opposite limb, thereby influencing sensory improvement and muscle strengthening in the paralyzed limb (An & Kang, 2020).
The movements on the non-paralyzed side of stroke survivors can be expected to improve the function of the paralyzed side (Sakamoto, 2014). Exercise utilizing movements on the non-paralyzed side can lead to early recovery in hemiplegic patients (Harjpal, 2022). Additionally, planning aerobic exercise can yield benefits such as blood pressure management, endurance enhancement, improvement in the affected lower limb step length, and prevention of muscle atrophy (Nemchek, 2021). Therefore, aiming to reduce musculoskeletal injuries, it is believed that combining leg lifting exercises with ADIM in a seated position may have an impact on improving posture control, balance, and daily life abilities.
Positive literature exists on the application of resistance training on the non-paralyzed lower limb combined with the ADIM in patients with stroke, aiming to improve posture control, balance, and daily life abilities. However, the number of studies is limited, with most conducted in a supine position. Moreover, research investigating the effects of non-paralyzed limb exercises on the stroke survivor’s plantar pressure during seated movements is lacking. Therefore, the purpose of this study is to compare the effects of resistance training on the non-paralyzed lower limb combined with the ADIM in a seated position among patients with stroke, aiming to provide better rehabilitation strategies for stroke survivors to return to daily life more effectively.
2Methods
2.1Participants
This study selected 32 participants who met the criteria for patients with stroke as the subjects for the experiment. The sample size of the experimental subjects was calculated using the G-Power software (version 3.1.9.7; Heinrich Heine University, Düsseldorf, Germany) based on data from previous studies. The F-test was utilized with an effect size of 0.5, a statistical power of 0.8, an alpha level of 0.05. As a result, the total sample size was determined to be 27 individuals. However, considering a dropout rate of 20%, the sample size was increased to 32 participants. Subject recruitment was conducted in rehabilitation hospitals located in Seoul and participants were recruited on a voluntary basis. The inclusion criteria for participants were as follows: individuals diagnosed with stroke (infarction or hemorrhagic) by a neurologist or a specialist in physical medicine and rehabilitation, those diagnosed with stroke (infarction or hemorrhagic) and 6 months post-diagnosis, those with a TIS score of 19 or lower, those with an MMSE-K score of 21 or above, indicating no difficulty in communication, those with no musculoskeletal issues in the legs, those with an MAS score of less than 2.The exclusion criteria for participants were as follows: those with communication impairment, musculoskeletal issues in the legs, and high muscle tone. Before the experiment, participants were provided with sufficient explanation about the purpose and procedures of the study and signed informed consent forms to participate. This study received approval from the Bioethics Committee of Sahmyook University (approval no. 2022-07-018-008). Registered with the Clinical Research Information Service, this study adheres to the World Health Organization International Clinical Trials Registry Platform (WHO-ICTRP) guidelines (registration no. KCT0008967).
2.2Study procedure
This study was a randomized controlled trial using random allocation, double-blind methodology, control group (CG) comparison, parallel-group design, and multi-center clinical trial methodology. Participants were randomized using a computer-generated ladder randomizer to one of the following groups: the lower limb resistance exercise with abdominal draw-in group (LRAG), the lower limb exercise with abdominal draw-in group (LAG), or the CG. Training sessions were conducted for 30 minutes, 3 times a week, following the specific methods of each group, and the entire intervention spanned over 4 weeks with a total of 12 sessions. All groups received tailored conventional physical therapy. Additionally, the LRAG underwent lower limb resistance exercise with ADIM training, the LAG underwent lower limb exercise with ADIM training, and the CG received conventional physical therapy.
The LRAG was set up by placing the pressure biofeedback unit (PBU), set to 40 mmHg, under the lower back after sitting on a Bobath table with the hip and knee joints bent at 90° and the soles of the feet touching the ground, then securing it with straps to prevent movement. The participant performed the ADIM while observing the pressure gauge connected to the PBU, aiming to raise and maintain it at 10 mmHg. Upon successful completion, they proceeded with non-paralyzed side leg lifting exercises. The non-paralyzed side leg lifting exercise involved maintaining 90° of knee flexion while flexing, abducting, and internally rotating the hip joint. Upon achieving the correct position, they held it for 3 seconds before slowly returning to the starting position. Resistance was provided using elastic bands, loosely tied around the knees and ankles. The intensity of the elastic bands was set to a level allowing for 12 repetitions per set. A total of 5 sets were conducted, with a 2-minute rest period between each set to prevent muscle fatigue. To prevent any potential risks during the experiment, one therapist was positioned behind the patient (Fig. 1).
Fig. 1
Lower limb resistance exercise with abdominal draw-in technique.

The LAG was set up by placing the PBU, set to 40 mmHg, under the lower back after sitting on a Bobath table with the hip and knee joints bent at 90° and the soles of the feet touching the ground, then securing it with straps to prevent movement. The participant performed the ADIM while observing the pressure gauge connected to the PBU, aiming to raise and maintain it at 10 mmHg. Upon successful completion, they proceeded with non-paralyzed side leg lifting exercises. The non-paralyzed side leg lifting exercise involved maintaining 90° of knee flexion while flexing, abducting, and internally rotating the hip joint. Upon achieving the correct position, they held it for 3 seconds before slowly returning to the starting position. A total of 5 sets were conducted, with a 2-minute rest period between each set to prevent muscle fatigue. To prevent any potential risks during the experiment, one therapist was positioned behind the patient (Fig. 2).
Fig. 2
Lower limb exercise with abdominal draw-in technique.

The control group received conventional physical therapy exercises, including seated trunk rotation and lateral weight-shifting exercises, with the goal of enhancing trunk control, balance, and activities of daily living. For trunk rotation exercises, the participant sat on a Bobath table with the hip and knee joints bent at 90°, then slowly rotated the trunk towards the paralyzed side. For lateral weight-shifting exercises, the participant sat with hip and knee joints bent at 90°, ensuring a comfortable position of the feet and ankles, then gradually shifted their weight towards the paralyzed side. The intervention duration was the same as the experimental group.
2.3Outcome measures
The participants completed the Korean version of the Trunk Impairment Scale (K-TIS), Postural Assessment Scale for Stroke (PASS), Modified Functional Reaching Test (mFRT), Berg Balance Scale (BBS), Foot print of BioRescue (RM Ingénierie, Marseille, France) and the Korean version of the Modified Barthel Index (K-MBI). assessments both at baseline and after completing the intervention.
2.3.1Korean version of the trunk impairment scale (K-TIS)
The TIS consists of three components: static sitting balance (7 points), dynamic sitting balance (10 points), and coordination (6 points), totaling up to 0 to 23 points. It demonstrates high validity and reliability in assessing patients with stroke, multiple sclerosis, and Parkinson’s Disease (Verheyden et al., 2006). The test-retest reliability of the K-TIS used in this study was ICC = 0.09, while the inter-rater reliability was ICC = 0.95 (Seo et al., 2008).
2.3.2Postural assessment scale for stroke (PASS)
Modified from the Fugl-Meyer Motor Assessment, the PASS includes items with varying difficulty levels, allowing for a sensitive evaluation of postural control in patients with stroke. It is a clinically useful tool due to its ease of use, simplicity, and short administration time of less than 10 minutes. There are a total of 12 items that assess static and dynamic postural control in lying, sitting, and standing positions, consisting of 5 items for maintaining posture and 7 items for transitioning between postures (Benaim et al., 1999; Mao et al., 2002). It demonstrates very high reliability, with a coefficient of 0.97 (An & Lee, 2009).
2.3.3Modified functional reaching test (mFRT)
The mFRT is one of the most commonly used assessment methods for sitting balance, particularly in older adults and patients with stroke. The starting position of the participant involves sitting with both feet shoulder-width apart on a fixed support surface, shoulder flexed at 90°, and fists clenched. A horizontal bar was installed at the height of the acromion, and the participant extended their arms to maintain balance, keeping their arms horizontal. The distance between the first and last points of the third metacarpal head was measured three times, and the average value was recorded (Arsh et al., 2021; Choi et al., 2017). The reliability of the mFRT ranges from r = 0.90 to 0.97, demonstrating high reliability (Katz-Leurer et al., 2009).
2.3.4Berg balance scale (BBS)
The BBS consists of 14 items: “Sitting to standing”, “Standing unsupported”, “Sitting unsupported”, “Standing to sitting”, “Transfers”, “Standing with eyes closed”, “Standing with feet together”, “Reaching forward with outstretched arm”, “Retrieving object from floor”, “Turning to look behind”, “Turning 360°”, “Placing alternate foot on stool”, “Standing with one foot in front”, and “Standing on one foot”. Each item is scored from 0 to 4 points, with a total possible score of 56 points if all items are performed perfectly. The assessment typically takes approximately 15 to 20 minutes, and higher scores indicate better balance abilities (Berg et al., 1992).
2.3.5Footprint of BioRescue (RM Ingénierie, Marseille, France)
The Footprint (BIORESCUE) consists of a square force plate with 1600 pressure sensors, a computer for data analysis, and a monitor providing visual feedback. It also features a ruler to help position the feet accurately. In this study, we evaluated the plantar pressure of the paralyzed limb in a seated position using this device. The participants sat on a Bobath table with hip and knee joints bent at 90°, placing their bare feet on the footplates. They were then comfortably seated with their legs spread about 30° apart, maintaining their gaze forward and centering themselves. Plantar pressure was measured once every minute under these conditions (Giagazoglou et al., 2012). The test-retest reliability of Biorescue shows a high reliability with an intraclass correlation coefficient (ICC) of 0.84 or higher (Hwang et al., 2019).
2.3.6The Korean version of the Modified Barthel Index (K-MBI)
The K-MBI assesses 10 items including ‘Bowels’, ‘Bladder’, ‘Grooming’, ‘Toilet Use’, ‘Feeding’, ‘Transfer (bed to chair and back)’, ‘Mobility’, ‘Dressing’, ‘Stairs’, and ‘Bathing’, with a total score of 100 points. Scores are categorized as follows: 0–24 points indicate total dependence, 25–49 points indicate severe dependence, 50–74 points indicate moderate dependence, 75–90 points indicate mild dependence, 90–99 points indicate minimal dependence, and 100 points indicate complete independence. Patients scoring above 60 are considered to have independent living abilities (Zheng et al., 2018). The inter-rater reliability of the K-MBI used in this study ranged from r = 0.93 to 0.98, demonstrating high reliability (Kim et al., 2016).
2.4Statistical analysis
This study was analyzed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA), and the normality test was conducted using the Shapiro-Wilk test. The participants underwent homogeneity testing for general characteristics and dependent variables using the one-way ANOVA before the experiment. Within-group changes before and after the experiment were analyzed using paired t-tests. Between-group differences in post-experimental changes were analyzed using the one-way ANOVA, followed by post-hoc tests using Tukey HSD (Honestly Significant Difference) test. The statistical significance level for all data was set at p < 0.05.
3Results
Initially, 32 participants were selected for the study. However, due to sudden discharges and refusals to participate in the experiment, 8 individuals were excluded, resulting in a final participation of 24 individuals (Fig. 3). Demographic characteristics are shown in Table 1. There was no significant differences in the baseline value among the three groups (Table 2).
Fig. 3
Experimental diagram.
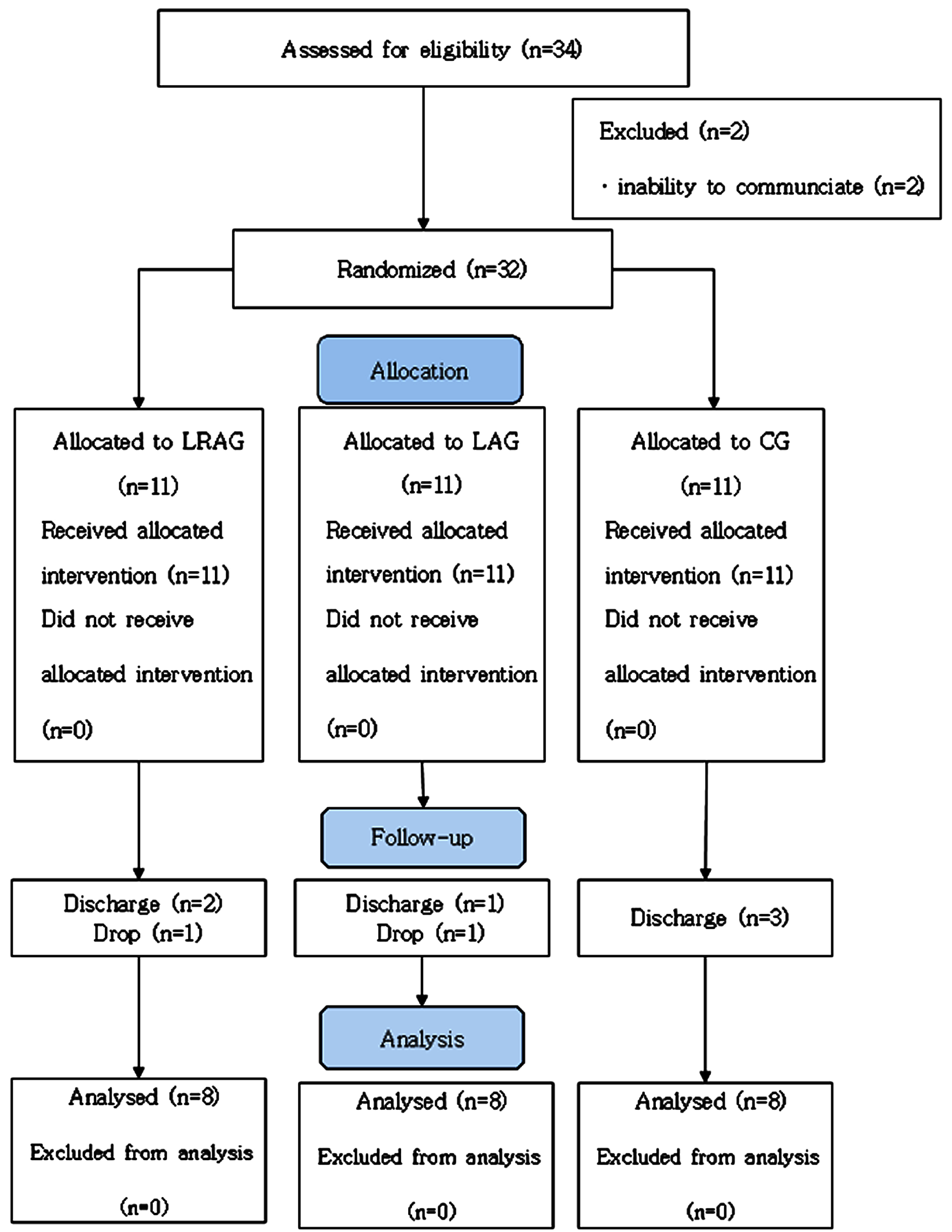
Table 1
General characteristics of subjects
| (n = 24) | ||||
| LRAG | LAG | CG | p | |
| Gender | ns | |||
| Male | 3 | 3 | 5 | |
| Female | 5 | 5 | 3 | |
| Age (years) | 62.63±8.47 | 67.5±15.05 | 60.13±5.46 | ns |
| Weight (kg) | 67.75±6.78 | 65.13±22.88 | 59.75±10.85 | ns |
| Height (cm) | 163.25±7.67 | 159.88±11.97 | 164.38±9.72 | ns |
| Onset (months) | 12.38±5.6 | 12.86±4.76 | 13.13±5.56 | ns |
| MMSE-K (score) | 20.88±6.81 | 22.56±6.93 | 25.25±6.27 | ns |
| MAS (score) | 0.75±0.71 | 0.88±0.64 | 0.75±.71 | ns |
| Affected side | ns | |||
| Right | 4 | 3 | 4 | |
| Left | 4 | 5 | 4 |
Values are mean±standard deviation or number. LRAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; MMSE-K: Mini-Mental State Examination-Korea; MAS: Modified Ashworth Scale; ns: no significance.
Table 2
Pre-assessment and homogeneity of subjects
| (n = 24) | ||||
| LRAG (n = 8) | LAG (n = 8) | CG (n = 8) | F (p) | |
| K-TIS (score) | 11±2.45 | 10±2.98 | 12.25±2.32 | 1.509 (0.244) |
| PASS (score) | 24.88±2.64 | 25.13±5.84 | 26.13±6.2 | 0.123 (0.877) |
| mFRT (cm) | 17.58±5.56 | 10.53±3.37 | 13.67±7.95 | 2.847 (0.081) |
| BBS (score) | 28±10.13 | 20.25±14.63 | 28.38±16.4 | 0.853 (0.44) |
| Foot print (%) | 56.75±15.03 | 57.38±16.61 | 51.63±16.01 | 0.315 (0.733) |
| MBI (score) | 61.13±21.07 | 54.25±23.47 | 63.38±30.47 | 0.282 (0.757) |
Values are mean±standard deviation or number. RAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; K-TIS: Korean Version Trunk Impairment Scale; PASS: Postural Assessment Scale of Stroke; mFRT: Modified Functional Reach Test; BBS: Berg Balance Scale; MBI: Modified Barthel Index.
Trunk control ability was assessed with the K-TIS and PASS. The K-TIS results is presented in Table 3 and the PASS in Table 4. In the K-TIS, the LRAG showed a statistically significant improvement compared to the LAG and CG after training (p < 0.001). However, there was no significant difference between the LAG and CG after training. In the PASS, the LRAG showed a statistically significant improvement compared to the LAG and CG after training (p = 0.004). However, there was no significant difference between LAG and CG after training.
Table 3
Comparison of trunk control abilities measured by the K-TIS
| (n = 24) | ||||
| LRAG (n = 8) | LAG (n = 8) | CG (n = 8) | F (p) | |
| K-TIS (score) | ||||
| Pretest | 11±2.45 | 10±2.98 | 12.25±2.32 | 1.509 (0.244) |
| Posttest | 21.63±3.82 | 16.13±2.59 | 16±3.67 | |
| Pre-Post | 10.63±2.83a,b | 6.13±2.1 | 3.75±1.83 | 18.579 (<0.001*) |
| t (p) | –10.625 (<0.001*) | –6.125 (<0.001*) | –3.75 (<0.001*) | LRAG > LAG, CG |
Values are mean±standard deviation or number. LRAG: RAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; K-TIS: Korean Version Trunk Impairment Scale. a: Significant difference compared to LAG. b: Significant difference compared to CG. *p < 0.05.
Table 4
Comparison of trunk control abilities measured by the PASS
| (n = 24) | ||||
| LRAG (n = 8) | LAG (n = 8) | CG (n = 8) | F (p) | |
| PASS (score) | ||||
| Pretest | 28±10.43 | 20.25±14.63 | 28.38±16.40 | 0.123 (0.877) |
| Posttest | 40.75±11.97 | 27.5±16.94 | 33.25±16.06 | |
| Pre-Post | 12.75±8.65a,b | 7.25±4.4 | 4.88±3.4 | 9.198 (0.001*) |
| t (p) | –12.75 (0.004*) | –7.25 (0.002*) | –4.875 (0.005*) | LRAG > LAG, CG |
Values are mean±standard deviation or number. RAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; PASS: Postural Assessment Scale of Stroke. a: Significant difference compared to LAG. b: Significant difference compared to CG. *p < 0.05.
Balance ability was assessed with mFRT and BBS. The mFRT is presented in Table 5 and the BBS in Table 6. In the mFRT, the LRAG showed a statistically significant improvement compared to the LAG and CG after training (p < 0.001). However, there was no significant difference between the LAG and CG after training. In the BBS, the LRAG did not show a statistically significant difference compared to the LAG after training, but showed a significant improvement compared to the CG after training (p = 0.004). However, there was no significant difference between the LAG and CG after training.
Table 5
Comparison of balance abilities measured by the mFRT
| (n = 24) | ||||
| LRAG (n = 8) | LAG (n = 8) | CG (n = 8) | F (p) | |
| mFRT (cm) | ||||
| Pretest | 17.58±5.56 | 10.53±3.37 | 13.67±7.95 | 2.847 (0.081) |
| Posttest | 39.36±5.07 | 24.41±5.46 | 24.66±9 | |
| Pre-Post | 21.78±5.22a,b | 13.89±5.27 | 10.99±5.33 | 8.978 (0.002*) |
| t (p) | –21.78 (<0.001*) | –13.886 (<0.001*) | –10.99 (<0.001*) | LRAG > LAG, CG |
Values are mean±standard deviation or number. RAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; mFRT: Modified Functional Reach Test. a: Significant difference compared to LAG. b: Significant difference compared to CG. *p < 0.05.
Table 6
Comparison of balance abilities measured by the BBS
| (n = 39) | ||||
| LRAG (n = 8) | LAG (n = 8) | CG (n = 8) | F (p) | |
| BBS (score) | ||||
| Pretest | 28±10.43 | 20.25±14.63 | 28.38±16.4 | 0.853 (0.44) |
| Posttest | 40.75±11.97 | 27.5±16.94 | 33.25±16.06 | |
| Pre-Post | 12.75±8.65b | 7.25±4.4 | 4.88±3.4 | 3.705 (0.042*) |
| t (p) | –12.75 (0.004*) | –7.25 (0.002*) | –4.875 (0.005*) | LRAG > CG |
Values are mean±standard deviation or number. RAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; BBS: Berg Balance Scale. b: Significant difference compared to CG. *p < 0.05.
ADL ability was assessed with the Foot print by BioRescue and K-MBI. The Foot print values are presented in Table 7, MBI in Table 8. In the Foot print assessment, the LRAG showed a statistically significant improvement compared to the LAG and CG after training (p = 0.003). However, there was no significant difference between the LAG and CG after training. In the K-MBI, the LRAG showed a statistically significant improvement compared to both the LAG and CG after training (p = 0.002). However, there was no significant difference between the LAG and CG after training.
Table 7
Comparison of daily life abilities measured by the Foot print
| (n = 24) | ||||
| LRAG (n = 8) | LAG (n = 8) | CG (n = 8) | F (p) | |
| Foot print (%) | ||||
| Pretest | 56.75±15.03 | 57.38±16.61 | 51.63±16.01 | 0.315 (0.733) |
| Posttest | 73.88±23.81 | 66.25±21.47 | 57.75±17.64 | |
| Pre-Post | 17.13±11.25a,b | 8.88±6.58 | 6.13±4.22 | 3.645 (0.044*) |
| t (p) | –17.125 (0.003*) | –8.875 (0.007*) | –6.125 (0.005*) | LRAG > LAG, CG |
Values are mean±standard deviation or number. RAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; a: Significant difference compared to LAG. b: Significant difference compared to CG. *p < 0.05.
Table 8
Comparison of daily life abilities measured by the MBI
| (n = 24) | ||||
| LRAG (n = 8) | LAG (n = 8) | CG (n = 8) | F (p) | |
| MBI (score) | ||||
| Pretest | 61.13±21.07 | 54.25±23.47 | 63.38±30.47 | 0.282 (0.757) |
| Posttest | 76.25±16.41 | 60.75±19.58 | 67.25±29.14 | |
| Pre-Post | 15.13±8.59a,b | 6.5±5.53 | 3.88±2.53 | 7.502 (0.003*) |
| t (p) | –15.125 (0.002*) | –6.5 (0.013*) | –3.875 (0.003*) | LRAG, LAG > CG |
Values are mean±standard deviation or number. RAG: lower limb resistance exercise with abdominal draw-in group; LAG: lower limb exercise with abdominal draw-in group; CG: control group; MBI: Modified Barthel Index. a: Significant difference compared to CG. *p < 0.05.
4Discussion
This study evaluated the effects of lower limb resistance exercises with ADIM on trunk control, balance, and activities of daily living in participants with stroke. In this study, the lower limb resistance exercises with ADIM showed significant improvements in trunk control, balance, and activities of daily living compared to lower limb exercises with ADIM and control exercises. Stroke survivors experience difficulty in weight-bearing and trunk control due to various reasons such as trunk muscle weakness (Hodges, 2005) and symptoms of hemiparesis (Kusoffsky et al., 2001). Unstable weight-bearing not only increases body sway, making it difficult to maintain balance, but also increases the risk of falls (Haruyama et al., 2017). Instability in trunk control arises from abnormal contractions of arm and leg muscles, leading to deformation of the spinal structure and excessive stress on soft tissues. This can result in pain, balance impairments, and reduced activities of daily living (Choi & Jung, 2017). Therefore, trunk control training is necessary exercise for achieving limited functional recovery (Lee et al., 2020).
The ADIM improves and strengthens the contraction time of muscles such as the transversus abdominis and internal obliques, enhancing anticipatory postural control ability. This contributes to trunk stabilization by increasing intra-abdominal pressure due to the inward pull of the lower abdomen without movement of the spine or pelvis, thereby improving the instability of the lumbar spine (Macedo, 2009). Furthermore, muscles that counteract lordosis of the spine and anterior pelvic tilt contract simultaneously, contributing to trunk stabilization (Teyhen et al., 2005). Leg lifting exercises create induce forced pelvic movements around the abdominal muscles, promoting efficient contraction responses and strengthening muscles necessary for postural control and balance, including those involved in hip stability. This makes it an effective exercise for improving postural control abilities (Dubey et al., 2018). Furthermore, it is effective in inducing automatic weight-bearing on the contralateral leg, leading to improvements in proprioception and muscle strengthening in the supporting leg (An & Kang, 2020). According to previous studies, combining the ADIM with various exercises is expected to have a greater effect on improving trunk control ability (Rasheed et al., 2021). Additionally, it has been reported that lower limb exercises with ADIM leads to increased activation of trunk muscles due to forced pelvic movements (Yoder et al., 2019). Based on these previous studies, lower limb exercises with ADIM can significantly contribute to improving trunk muscle strength, balance, and activities of daily living in patients with stroke.
In this study, we used the K-TIS and PASS to assess trunk control ability. Both assessment results showed significant improvements in the LRAG compared to the LAG and CG after training. However, there was no significant difference between the LAG and CG after training. High-intensity training is effective in improving trunk control ability (Ahmed et al., 2021). Furthermore, the muscles around the abdomen exhibit efficient contraction responses to pelvic movements, leading to strengthening of trunk control muscles such as the transversus abdominis and internal obliques. This results in increased segmental stability of the spine for all movements, thereby enhancing trunk control ability (Dubey et al., 2018). This study also yielded similar results to previous research.
In this study, we used the mFRT and BBS to assess balance ability. The results of the mFRT showed significant improvement after training in the LRAG compared to the LAG and CG. The BBS showed no significant difference between the LARG and LAG, but there was a significant difference between the LARG and CG. The mFRT is effective in assessing the sitting posture of patients with stroke, but it has limitations in evaluating balance in the standing position (Arsh et al., 2021). Therefore, to measure balance in the standing position, we used the BBS. Among the assessment items of the BBS, such as “Turning to look behind” and “Turning 360°”, balance is evaluated using both legs, so the paralyzed leg must be supported to achieve a high score (Berg et al., 1992). Leg lifting induces automatic step of the contralateral leg, promoting weight shifting and thus improving leg sensation and muscle strength (An & Kang, 2020). Moreover, trunk control ability and balance ability are highly correlated, so improving trunk control may also contribute to the recovery of balance ability (Lee et al., 2020). Therefore, performing trunk muscle strengthening exercises to enhance balance ability in patients with stroke can have significant effects not only on trunk control improvement but also on balance ability enhancement.
This study utilized the Foot print and MBI to evaluate activities of daily living abilities. The Foot print measured the percentage of support from the paralyzed foot during sit-to-stand tasks. This serves as an indicator to assess muscle imbalance between the left and right lower limbs during sit-to-stand. The BioRescue was used to measure Foot print. Both assessment results showed significant improvement after training in the LRAG compared to the LAG and CG. However, there was no significant difference between the LAG and CG after training. Patients with hemiparesis who have experienced falls often exhibit poor weight transfer to the paralyzed leg during the sit-to-stand movement (Liu et al., 2015). Therefore, the results from Foot print indicate a reduced risk of falls, implying a decrease in trunk sway and improvement in balance ability. This contributes to enhancing the performance of activities of daily living (Lee et al., 2020).
There are several limitations to this study. First, the experiment was conducted with a sample size of 24 participants, making it difficult to generalize the results of this study to all stroke survivors due to the small sample size. Second, the intensity of resistance exercise was limited by the small number of intensity levels, which consisted of only six levels. Third, the recovery time from muscle fatigue induced by eccentric contractions of the calf muscles at each intensity level was not considered. Fourth, the assessment of walking ability, one of the activities of daily living, was not conducted. In future studies, it is necessary to recruit a larger number of participants and conduct research with various resistance intensities to validate the effects. Additionally, research on walking, which has a high correlation with balance ability and activities of daily living, should also be conducted.
5Conclusion
This study investigated the effects of lower limb resistance exercises with the ADIM on posture control, balance, and activities of daily living in patients with stroke while seated. The results revealed that performing lower limb resistance exercises with ADIM led to significant improvements in posture control, balance, and activities of daily living compared to lower limb exercises with ADIM alone and conventional physical therapy. Additionally, it was observed that lower limb resistance exercises with ADIM were effective in enhancing posture control, balance, and activities of daily living in patients with stroke. Therefore, it is suggested that when planning training programs for stroke survivors, one should consider incorporating methods aimed at improving posture control, balance, and activities of daily living, particularly for chronic stroke survivors who may face challenges in functional recovery.
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics statement
This study complies with the Declaration of Helsinki and was performed according to the Bioethics Committee of Sahmyook University (Approval Number: 2022-07-018-008). Registered with the Clinical Research Information Service, this study adheres to the World Health Organization International Clinical Trials Registry Platform (WHO-ICTRP) guidelines (registration number: KCT0008967).
Conflict of interest
The authors declare no potential conflicts of interest concerning this article’s authorship and/or publication.
References
1 | Ahmed, U. , Karimi, H. , Amir, S. , & Ahmed, A. ((2021) ). Effects of intensive multiplanar trunk training coupled with dual-task exercises on balance, mobility, and fall risk in patients with stroke: A randomized controlled trial. Journal of International Medical Research, 49: (11), 03000605211059413. |
2 | An, S.-H. , & Lee, J.-H. ((2009) ). Reliability and validity of the postural assessment scale for stroke in chronic stroke patients. The Journal of Korean Physical Therapy, 21: (1), 9–17. |
3 | An, S. , & Kang, S. ((2020) ). The effect of resistance exercise using elastic band on muscle strength, muscle tone, balance and gait in stroke patients. Journal of Korean Society of Integrative Medicine, 8: (1), 57–66. |
4 | Arsh, A. , Darain, H. , Rahman, M. U. , Ullah, I. , & Shakil-Ur-Rehman, S. ((2021) ). Reliability of modified functional reach test in the assessment of balance function in people with spinal cord injury: A systematic review. Journal of the Pakistan Medical Association, 71: (8), 2040–2044. |
5 | Benaim, C. , Pérennou, D. A. , Villy, J. , Rousseaux, M. , & Pelissier, J. Y. ((1999) ). Validation of a standardized assessment of postural control in stroke patients: The Postural Assessment Scale for Stroke Patients (PASS. Stroke, 30: (9), 1862–1868. |
6 | Berg, K. O. , Maki, B. E. , Williams, J. I. , Holliday, P. J. , & Wood-Dauphinee, S. L. ((1992) ). Clinical and laboratory measures of postural balance in an elderly population. Archives of Physical Medicine and Rehabilitation, 73: (11), 1073–1080. |
7 | Cheon, S. , Lee, J.-H. , Jun, H.-P. , An, Y. W. , & Chang, E. ((2020) ). Acute effects of open kinetic chain exercise versus those of closed kinetic chain exercise on quadriceps muscle thickness in healthy adults. International Journal of Environmental Research and Public Health, 17: (13), 4669. |
8 | Choi, H.-S. , Shin, W.-S. , Bang, D.-H. , & Choi, S.-J. ((2017) ). Effects of game-based constraint-induced movement therapy on balance in patients with stroke: A single-blind randomized controlled trial. American Journal of Physical Medicine & Rehabilitation, 96: (3), 184–190. |
9 | Choi, J.-D. , & Jung, K.-M. ((2017) ). The effect of active trunk training in sitting position on balance and energy consumption in early stroke patients. Journal of the Korean Society of Physical Medicine, 12: (4), 93–103. |
10 | Dubey, L. , Karthikbabu, S. , & Mohan, D. ((2018) ). Effects of pelvic stability training on movement control, hip muscles strength, walking speed and daily activities after stroke: A randomized controlled trial. Annals of Neurosciences, 25: (2), 80–89. |
11 | Giagazoglou, P. , Arabatzi, F. , Dipla, K. , Liga, M. , & Kellis, E. ((2012) ). Effect of a hippotherapy intervention program on static balance and strength in adolescents with intellectual disabilities. Research in Developmental Disabilities, 33: (6), 2265–2270. |
12 | Harjpal, P. L. , Kovela, R. K. , Qureshi, M. I. , & Salphale, V. G. ((2022) ). Novelty in exercise regimen towards bilateral training in a patient after a cerebrovascular event. Journal of Clinical & Diagnostic Research, 16: (11). |
13 | Haruyama, K. , Kawakami, M. , & Otsuka, T. ((2017) ). Effect of core stability training on trunk function, standing balance, and mobility in stroke patients. Neurorehabil Neural Repair, 31: (3), 240–249. |
14 | Hodges, P. W. , Eriksson, A. E. , Shirley, D. , & Gandevia, S. C. ((2005) ). Intra-abdominal pressure increases stiffness of the lumbar spine. J Biomech, 38: (9), 1873–1880. |
15 | Hwang, J. , Lee, Y. , Joo, M. , & Kim, S. ((2019) ). The effect of action on the balance and the trunk control ability in the sit position of chronic stroke patients. Journal of Korean Society of Integrative Medicine, 7: (3), 1–9. |
16 | Katz-Leurer, M. , Fisher, I. , Neeb, M. , Schwartz, I. , & Carmeli, E. ((2009) ). Reliability and validity of the modified functional reach test at the sub-acute stage post-stroke. Disabil Rehabil, 31: (3), 243–248. |
17 | Kim, J. Y. , Kang, K. , Kang, J. , Koo, J. , Kim, D. H. , Kim, B. J. , et al. ((2019) ). Executive summary of stroke statistics in korea 2018: A report from the epidemiology research council of the korean stroke society. J Stroke, 21: (1), 42–59. |
18 | Kim, S. Y. , Shin, S. B. , Lee, S. J. , Kim, T. U. , & Hyun, J. K. ((2016) ). Factors associated with upper extremity functional recovery following low-frequency repetitive transcranial magnetic stimulation in stroke patients. Annals of Rehabilitation Medicine, 40: (3), 373–382. |
19 | Kusoffsky, A. , Apel, I. , & Hirschfeld, H. ((2001) ). Reaching-lifting-placing task during standing after stroke: Coordination among ground forces, ankle muscle activity, and hand movement. Arch Phys Med Rehabil, 82: (5), 650–660. |
20 | Lattouf, N. A. , Tomb, R. , Assi, A. , Maynard, L. , & Mesure, S. ((2021) ). Eccentric training effects for patients with post-stroke hemiparesis on strength and speed gait: A randomized controlled trial. NeuroRehabilitation, 48: (4), 513–522. |
21 | Lee, P. Y. , Huang, J. C. , Tseng, H. Y. , Yang, Y. C. , & Lin, S. I. ((2020) ). Effects of trunk exercise on unstable surfaces in persons with stroke: A randomized controlled trial. Int J Environ Res Public Health, 17: (23). |
22 | Liu, M. , Chen, J. , Fan, W. , Mu, J. , Zhang, J. , Wang, L. , et al. ((2016) ). Effects of modified sit-to-stand training on balance control in hemiplegic stroke patients: A randomized controlled trial. Clin Rehabil, 30: (7), 627–636. |
23 | Macedo, L. G. , Maher, C. G. , Latimer, J. , & McAuley, J. H. ((2009) ). Motor control exercise for persistent, nonspecific low back pain: A systematic review. Phys Ther, 89: (1), 9–25. |
24 | Mao, H.-F. , Hsueh, I.-P. , Tang, P.-F. , Sheu, C.-F. , & Hsieh, C.-L. ((2002) ). Analysis and comon of the psychometric properties of three balance measures for stroke patients. Stroke, 33: (4), 1022–1027 paris. |
25 | Nemchek, V. , Haan, E. M. , Mavros, R. , Macuiba, A. , & Kerr, A. L. ((2021) ). Voluntary exercise ameliorates the good limb training effect in a mouse model of stroke. Experimental Brain Research, 239: , 687–697. |
26 | Phipps, M. S. , & Cronin, C. A. ((2020) ). Management of acute ischemic stroke. Bmj, 368: . |
27 | Rasheed, H. , Ahmad, I. , Javed, M. A. , Rashid, J. , & Javeed, R. S. ((2021) ). Effects of Diaphragmatic Breathing Maneuver and Abdominal Drawing-in Maneuver on trunk stability in stroke patients. Physical & Occupational Therapy In Geriatrics, 39: (1), 1–10. |
28 | Sakamoto, K. , Nakamura, T. , Uenishi, H. , Umemoto, Y. , Arakawa, H. , Abo, M. , et al. ((2014) ). Immediate effects of unaffected arm exercise in poststroke patients with spastic upper limb hemiparesis. Cerebrovascular Diseases, 37: (2), 123–127. |
29 | Seo, H.-D. , Kim, N.-J. , & Chung, Y.-J. ((2008) ). Reliability of the Korean version of the trunk impairment scale in patients with stroke. Physical Therapy Korea, 15: (4), 87–96. |
30 | Smrcina, Z. , Woelfel, S. , & Burcal, C. ((2022) ). A systematic review of the effectiveness of core stability exercises in patients with non-specific low back pain. International Journal of Sports Physical Therapy, 17: (5), 766–774. https://doi.org/10.26603/001c.37251 |
31 | Teyhen, D. S. , Miltenberger, C. E. , Deiters, H. M. , Del Toro, Y. M. , Pulliam, J. N. , Childs, J. D. , et al. ((2005) ). The use of ultrasound imaging of the abdominal drawing-in maneuver in subjects with low back pain. Journal of Orthopaedic & Sports Physical Therapy, 35: (6), 346–355. |
32 | Yoder, A. J. , Silder, A. , Farrokhi, S. , Dearth, C. L. , & Hendershot, B. D. ((2019) ). Lower extremity Joint contributions to trunk control During Walking in persons with transtibial Amputation. Scientific Reports, 9: (1), 1–8. |
33 | Zheng, X. , Chen, D. , Yan, T. , Jin, D. , Zhuang, Z. , Tan, Z. , et al. ((2018) ). A randomized clinical trial of a functional electrical stimulation mimic to gait promotes motor recovery and brain remodeling in acute stroke. Behavioural Neurology, 2018: . |

